outpatient perineal sling in adolescent boys with neurogenic incontinence
TRANSCRIPT
Outpatient Perineal Sling in Adolescent Boys WithNeurogenic Incontinence
Gregory E. Dean*,† and David A. Kunkle
From the Department of Pediatric Urology, Temple University School of Medicine, Philadelphia, Pennsylvania
Abbreviations
and Acronyms
AUS � artificial urinary sphincter
CIC � clean intermittentcatheterization
* Correspondence: 120 Carnie Blvd., Suite 2,Voorhees, New Jersey 08043 (telephone: 856-751-7880; FAX: 856-751-9133; e-mail: [email protected]).
† Financial interest and/or other relationshipwith American Medical Systems.
Purpose: Management for urinary incontinence in boys with sphincteric incom-petence secondary to a neurogenic etiology is a challenge. Minimally invasiveapproaches have inconsistent efficacy and may require multiple treatments.Open bladder neck reconstruction requires inpatient hospitalizations and can beassociated with a high complication rate. To overcome some of these shortcom-ings we placed a polypropylene male perineal sling in male adolescents withneurogenic sphincteric incontinence. We retrospectively reviewed the outcome inour initial 6 patients.Materials and Methods: Six patients 14 to 20 years old underwent placement ofa polypropylene male perineal sling on an outpatient basis. Followup was 27 to 39months (median 33). All patients had a history of myelomeningocele and under-went urodynamics showing normal compliance, adequate capacity and sphinc-teric incompetence. A suburethral sling was placed on an outpatient basisthrough a small perineal incision. Sling tension was adjusted for maximal ure-thral compression while still permitting uncomplicated urethral catheter pas-sage.Results: All 6 patients reported immediate complete continence after sling place-ment. Two slings were removed after local infection developed and 1 was re-placed. Another sling required revision secondary to incomplete bone anchorfixation. No patients had urethral erosion. All 5 patients with a sling currently inplace were fully continent on intermittent catheterization every 3 hours and theyreported excellent satisfaction with the procedure.Conclusions: Our retrospective study suggests that the male urethral sling maybe an outpatient option for neurogenic incontinence secondary to sphinctericincompetence. Long-term followup in our initial 6 patients shows encouragingdurability. Continued study is required to determine strategies that might de-crease the complication rate of this approach.
Key Words: urinary incontinence; urinary bladder, neurogenic; urethra; male;
adolescent; suburethral slings1792 www.jurology.com
TREATMENT in children with neurogenicurinary incontinence remains challeng-ing despite the wide variety of treatmentoptions. The population with neurogenicbladder is most commonly patients withmyelomeningocele but other causes aresacral agenesis, spinal cord tumor, iatro-
genic injury and trauma.10022-5347/09/1824-1792/0THE JOURNAL OF UROLOGY®
Copyright © 2009 by AMERICAN UROLOGICAL ASSOCIATION
The introduction of CIC by Lapideset al in 1972 was a significant devel-opment for children with neurogenicbladder that has resulted in urinarycontinence in up to 81% when usedalone or combined with pharmaco-therapy.2 However, patients who do
not achieve dryness despite CIC andVol. 182, 1792-1796, October 2009Printed in U.S.A.
DOI:10.1016/j.juro.2009.04.082

PERINEAL SLING FOR NEUROGENIC INCONTINENCE 1793
pharmacotherapy represent a significant treatmentchallenge. In those with low bladder outlet resis-tance there are various procedures to increase ure-thral resistance but no consensus on optimal man-agement to achieve continence has been reached.Current treatment options are urethral lengthen-ing, bladder neck closure, fascial slings, bladderwrap slings, AUS and endoscopic injection of bulk-ing agents.
We investigated the novel application of a bone an-chored suburethral sling as a relatively noninvasivealternative in boys. The InVance™ polypropylenemale perineal sling system has been successfully usedin men with post-prostatectomy incontinence. Thispolypropylene mesh shows low morbidity and reliableimprovement in post-prostatectomy incontinence inthis patient population.3–5 To our knowledge no pub-lished reports exist in the world literature to date onthis sling in children with neurogenic sphincteric in-continence. We present our experience with a novelapplication of the polypropylene male urethral sling asoutpatient surgery in male adolescents with neuro-genic incontinence due to low outlet resistance.
MATERIALS AND METHODS
Patient SelectionFrom December 2005 through December 2006 all postpu-bertal boys followed at our clinic with urodynamic criteriaof neurogenic sphincteric incompetence, and adequatebladder compliance and capacity were offered the treat-ment options of observation, bladder neck bulking or per-ineal sling placement. Six patients self-selected placementof a polypropylene mesh perineal sling for neurogenicsphincteric incontinence. Evaluation included history,physical examination, renal/bladder ultrasound, urody-namics and cystography. All patients continued to haveurinary incontinence despite CIC and maximal oral phar-macotherapy. One patient had no history of open urolog-ical surgery, 1 underwent prior appendicovesicostomy andbladder augmentation with a Mitrofanoff channel, and 4underwent unsuccessful bladder neck bulking. Three ofthe 6 patients walk with Canadian crutches and the re-mainder are wheelchair bound.
Preoperatively urodynamics revealed adequate bladdercompliance with greater than 300 cc capacity in patientsable to fill despite the open bladder neck. All patients haddetrusor leak point pressure less than 25 cm H2O. Cys-tography or videourodynamics showed an open bladderneck. In patients with low detrusor leak point pressureprecluding adequate filling on urodynamics an occlusiveballoon used during cystography revealed a capacious,smooth walled bladder. Also, no patient had evidence ofhydronephrosis on ultrasound and all had normal serumcreatinine preoperatively.
Surgical TechniqueThe surgical procedure was similar to that described in pa-tients after prostatectomy3 with some notable modification
to achieve urinary retention. The patient was administeredbroad-spectrum antibiotic coverage perioperatively. Aftergeneral anesthetic induction the patient was positioned inan exaggerated lithotomy position. When the lithotomyposition was limited secondary to contracture, gel padswere used to promote optimal positioning. Orthopedic lim-itations never prevented the procedure but they affectedsurgical field size. The perineum was shaved and vigor-ously scrubbed with chlorhexidine preparation. A markingpen was used to delineate the inferior pubic rami and thepubis. A Foley catheter corresponding in size to that nor-mally used by the patient was placed to facilitate urethralpalpation. A 3 cm incision was made in the perineal mid-line at a point just below the scrotum. Care was taken toavoid midline dissection and in doing so the superficialtissue was left intact over the bulbospongiosus and ure-thra. Lateral dissection was performed to expose the me-dial and superior aspects of the bilateral descending pubicrami. The Lone Star Retractor System™ was used toprovide exposure. Dissection to the periosteal level en-sured satisfactory anchor placement. Titanium bonescrews 5.5 � 3.2 mm in diameter preloaded with 2, 1-zeropolypropylene sutures were prepared in the bone drill.Three screws were placed in each descending pubic ramususing the InVance bone drill. The most proximal screwswere placed at the confluence of the inferior pubic ramusand the pubis. Care was taken to avoid screw placement inthe arcuate ligament. Subsequent screws were placed se-quentially approximately 5 mm apart. Bone screws wereplaced similarly on the right side.
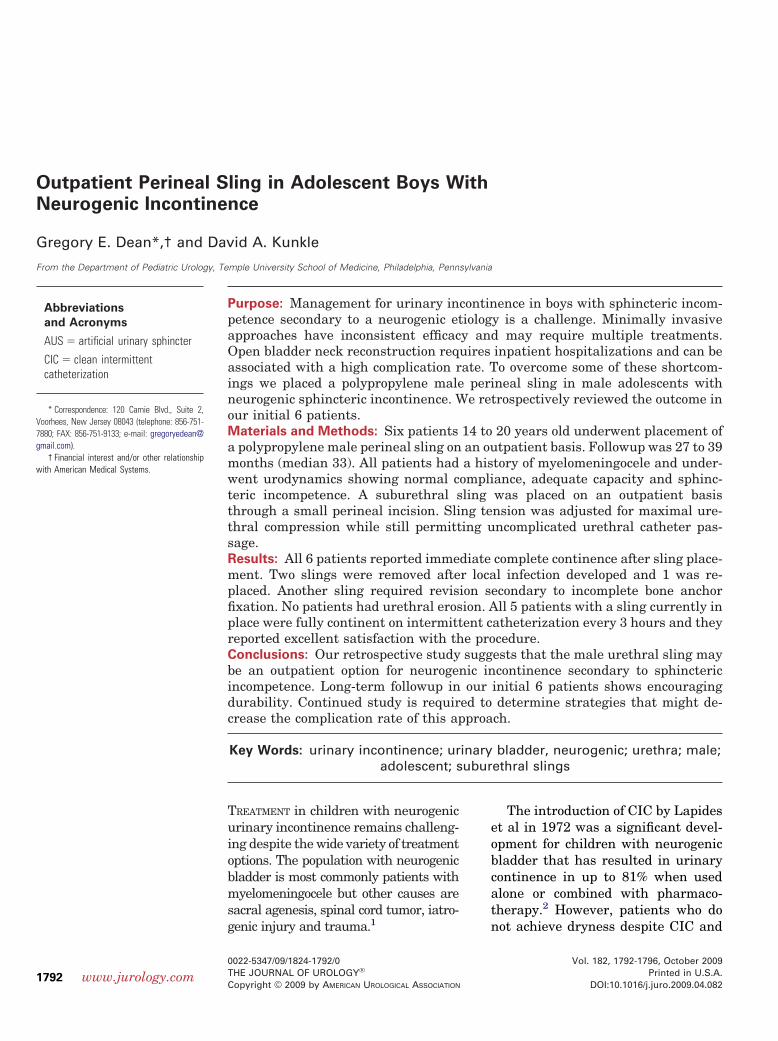
The polypropylene mesh to be implemented as the slingwas measured and cut in an elliptical configuration toapproximately 2 � 4 cm. The 2 bone anchored sutures foreach right screw were passed through the edges of themesh through separate openings and tied down (part A offigure). The left side of the mesh was held in place at thedescending pubic ramus to simulate the expected tensionto be placed over the bulbospongiosus muscle while theFoley catheter was removed and reinserted. Sling tensionwas adjusted to provide maximal urethral compressionwhile still permitting catheter passage (part B of figure).This level of compression is significantly higher than thatdescribed for post-prostatectomy incontinence, when uri-nary retention is a complication of the procedure ratherthan the goal. After optimal urethral compression wasachieved the left sutures were tied down. The superiorsuture was secured initially, subsequent sutures were pre-assessed for relative position and tension was adjustedaccordingly. The mesh was tailored in situ to avoid im-planting excess material. The most recent 2 cases wereperformed with an antibiotic impregnated mesh, whichsuperseded the older style nontreated mesh.
The wound was irrigated and closed in 2 layers. Thecatheter was removed before leaving the operating room.Patients resumed the CIC regimen immediately postoper-atively. All patients were discharged home on the day ofsurgery on a 1-week course of oral antibiotics.
RESULTS
Six adolescent boys underwent placement of a polypro-pylene perineal sling for neurogenic sphincteric incon-
tinence. Neurogenic bladder resulted from myelodys-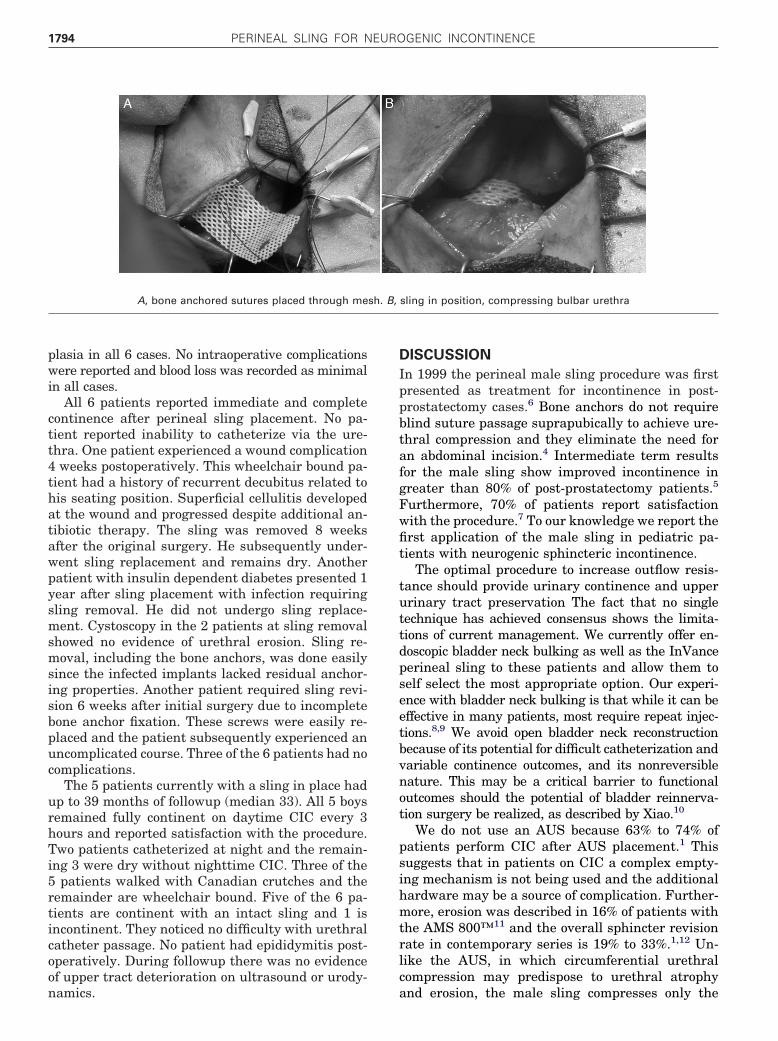
sh. B,
PERINEAL SLING FOR NEUROGENIC INCONTINENCE1794
plasia in all 6 cases. No intraoperative complicationswere reported and blood loss was recorded as minimalin all cases.
All 6 patients reported immediate and completecontinence after perineal sling placement. No pa-tient reported inability to catheterize via the ure-thra. One patient experienced a wound complication4 weeks postoperatively. This wheelchair bound pa-tient had a history of recurrent decubitus related tohis seating position. Superficial cellulitis developedat the wound and progressed despite additional an-tibiotic therapy. The sling was removed 8 weeksafter the original surgery. He subsequently under-went sling replacement and remains dry. Anotherpatient with insulin dependent diabetes presented 1year after sling placement with infection requiringsling removal. He did not undergo sling replace-ment. Cystoscopy in the 2 patients at sling removalshowed no evidence of urethral erosion. Sling re-moval, including the bone anchors, was done easilysince the infected implants lacked residual anchor-ing properties. Another patient required sling revi-sion 6 weeks after initial surgery due to incompletebone anchor fixation. These screws were easily re-placed and the patient subsequently experienced anuncomplicated course. Three of the 6 patients had nocomplications.
The 5 patients currently with a sling in place hadup to 39 months of followup (median 33). All 5 boysremained fully continent on daytime CIC every 3hours and reported satisfaction with the procedure.Two patients catheterized at night and the remain-ing 3 were dry without nighttime CIC. Three of the5 patients walked with Canadian crutches and theremainder are wheelchair bound. Five of the 6 pa-tients are continent with an intact sling and 1 isincontinent. They noticed no difficulty with urethralcatheter passage. No patient had epididymitis post-operatively. During followup there was no evidenceof upper tract deterioration on ultrasound or urody-
A, bone anchored sutures placed through me
namics.
DISCUSSION
In 1999 the perineal male sling procedure was firstpresented as treatment for incontinence in post-prostatectomy cases.6 Bone anchors do not requireblind suture passage suprapubically to achieve ure-thral compression and they eliminate the need foran abdominal incision.4 Intermediate term resultsfor the male sling show improved incontinence ingreater than 80% of post-prostatectomy patients.5
Furthermore, 70% of patients report satisfactionwith the procedure.7 To our knowledge we report thefirst application of the male sling in pediatric pa-tients with neurogenic sphincteric incontinence.
The optimal procedure to increase outflow resis-tance should provide urinary continence and upperurinary tract preservation The fact that no singletechnique has achieved consensus shows the limita-tions of current management. We currently offer en-doscopic bladder neck bulking as well as the InVanceperineal sling to these patients and allow them toself select the most appropriate option. Our experi-ence with bladder neck bulking is that while it can beeffective in many patients, most require repeat injec-tions.8,9 We avoid open bladder neck reconstructionbecause of its potential for difficult catheterization andvariable continence outcomes, and its nonreversiblenature. This may be a critical barrier to functionaloutcomes should the potential of bladder reinnerva-tion surgery be realized, as described by Xiao.10
We do not use an AUS because 63% to 74% ofpatients perform CIC after AUS placement.1 Thissuggests that in patients on CIC a complex empty-ing mechanism is not being used and the additionalhardware may be a source of complication. Further-more, erosion was described in 16% of patients withthe AMS 800™11 and the overall sphincter revisionrate in contemporary series is 19% to 33%.1,12 Un-like the AUS, in which circumferential urethralcompression may predispose to urethral atrophy
sling in position, compressing bulbar urethra
and erosion, the male sling compresses only the

PERINEAL SLING FOR NEUROGENIC INCONTINENCE 1795
ventral bulbar urethra and leaves the dorsal/lateralblood supply intact.3 The bulbospongiosus muscle issimilarly left intact to provide a cushion betweenurethra and sling that may further minimize therisk of erosion.3
All of our patients were already on an establishedcatheterization regimen. Accordingly our techniquediffers from that described in men after prostatec-tomy, in that we place a greater degree of compres-sion on the urethra to achieve continence. We placethe titanium screws at the junction of the pubis andthe ischial rami to further enhance compression.While previously reported techniques describe tight-ening the sling using perfusion sphincterometry to aretrograde leak point pressure of 60 cm H2O,3 wecalibrate the sling to the maximal urethral compres-sion that permits passage of the standard patientcatheter (range 12Fr to 14Fr). Future investigationof intraoperative urethral pressure profiles mightyield more precise tension guidelines.
We noted 3 complications in our initial experiencewith the male perineal sling, which were likely re-lated to our initial inexperience and patient selec-tion. These 3 complications yielded an overall reop-erative rate of 50%. Two of the 6 patients (33%)experienced infection. Each is wheelchair bound andhas a history of decubitus. Now wheelchair boundpatients meet with a wheelchair seating specialist tooptimize cushioning and support. More recently themanufacturer replaced the previously used meshwith an antibiotic impregnated product that maydecrease the infection rate. We changed our protocolto include oral ciprofloxacin starting 1 day beforesurgery and extending for 1 week postoperatively.Also, we perform intensive perineal scrubbing in theoperating room before making the surgical incision.
The other complication developed in the secondpatient to undergo sling placement in our experi-ence. It resulted from detachment of a bone an-chored screw. He underwent subsequent revisionand experienced an otherwise uncomplicated course.This complication was seen in other series.13 Possi-ble reasons for poor fixation are inadequate softtissue dissection over the periosteum and placementinto the arcuate ligament rather than the ischialrami. We modified our technique to include intraop-erative fluoroscopy to confirm screw fixation, whichshould decrease this complication in the future.
While we report a novel application of thepolypropylene perineal sling for neurogenic sphinc-teric incontinence, several concerns remain to beaddressed. The effects of fixed urethral obstructionon long-term urinary tract function must be care-fully monitored. While the safety of sling proceduresin boys without augmentation was reported,14 long-term close observation must be the rule. All patients
must be counseled on the strong likelihood of retro-grade ejaculation after sling placement, which cre-ates urethral obstruction, as well as the reproduc-tive options available to obviate this issue. Bonepain was described in adults who undergo this pro-cedure, which is believed to be the result of traumato the superficial perineal nerve, a branch of thepudendal nerve.15 We have not seen this in ourpatient population. While the incidence of osteomy-elitis and osteitis pubis are low in the adult popula-tions,3 the implications of this fixed restriction onpelvic bone growth remains to be determined.
The scope of the outcomes described is limited topostpubertal boys. Our initial approach in prepubertalboys is to initially start with bladder neck bulking.Because of patient dissatisfaction with the need forrebulking, we started to use this device in prepubertalboys but the potential impact on pelvic growth andurethral compression with time remains unknown.These patients require close monitoring and potentialsling removal if these issues become problematic.
Our study has several limitations, including thesmall number of patients followed, and its retrospec-tive nature and relatively brief followup. Anotherlimitation is that while we determined leak pointpressure preoperatively, the functional continenceoutcome rather than urodynamic leak point pres-sure was used to confirm success postoperatively.Future studies would benefit from a prospective,randomized structure in a larger number of patientsfollowed for many years. Several years of followupare required to determine the risk of urethral ero-sion with this compressive sling.
CONCLUSIONS
Our preliminary study suggests that the polypro-pylene male perineal sling may be a minimally in-vasive, outpatient option for neurogenic inconti-nence secondary to sphincteric incompetence. Weperformed this procedure safely in adolescent boysand achieved 100% continence in 5 of the 6 whocurrently have a sling in place. We noted a relativelyhigh 33% infection rate (2 of 6 cases), which webelieve will decrease with appropriate patient selec-tion, and modification to the sling material and tech-nique. Further studies must be performed in alarger series of patients to determine whether oursuccess is confirmed. Additional issues currently be-ing investigated are the appropriate intraoperativeleak point pressure required to achieve satisfactoryresults and the applicability of this approach in pre-pubertal patients.
ACKNOWLEDGMENTS
Dr. Alexis Te suggested this technique for neuro-
genic sphincteric incontinence.
PERINEAL SLING FOR NEUROGENIC INCONTINENCE1796
REFERENCES
1. Kryger JV, González R and Barthold JS: Surgicalmanagement of urinary incontinence in childrenwith neurogenic sphincteric incompetence. J Urol2000; 163: 256.
2. Lapides J, Diokno AC, Silber SJ et al: Clean,intermittent self-catheterization in the treatmentof urinary tract disease. J Urol 1972; 107: 458.
3. Comiter CV: The male sling for stress urinaryincontinence: a prospective study. J Urol 2002;167: 597.
4. Comiter CV: The male perineal sling: intermedi-ate-term results. Neurourol Urodyn 2005; 24: 648.
5. Fassi-Fehri H, Badet L, Cherass A et al: Efficacy ofthe InVance male sling in men with stress urinaryincontinence. Eur Urol 2007; 51: 498.
6. Madjar S, Jacoby K, Giberti C et al: Bone anchoredsling for the treatment of post-prostatectomy incon-
EDITORIAL COMMENT
who have never been operated on unde
7. Rajpurkar AD, Onur R and Singla A: Patient sat-isfaction and clinical efficacy of the new perinealbone-anchored male sling. Eur Urol 2005; 47:237.
8. Dean GE and Doumanian LR: The extended use ofDeflux (dextranomer/hyaluronic acid) in pediatricurology. Curr Urol Rep 2006; 7: 143.
9. Dean GE, Kirsch AJ, Packer MG et al: Antegradeand retrograde endoscopic dextranomer/hyal-uronic acid bladder neck bulking for pediatricincontinence. J Urol 2007; 178: 652.
10. Xiao CG: Reinnervation for neurogenic bladder:historic review and introduction of a somatic-autonomic reflex pathway procedure for patientswith spinal cord injury or spina bifida. Eur Urol2006; 49: 22.
11. Herndon CDA, Rink RC, Shaw MBK et al: The
rgo this proce-
ters in children and young adults. J Urol 2003;169: 650.
12. Levesque PE, Bauer SB, Atala A et al: Ten-yearexperience with the artificial urinary sphincter inchildren. J Urol 1996; 156: 625.
13. Mahdy A, Elmissiry M and Ghoniem G: Recurrentstress urinary incontinence after dislodged screwsin patient with bone-anchored suburethral sling.Urology 2008; 72: 1185.e11.
14. Snodgrass WT, Elmore J and Adams R: Bladderneck sling and appendicovesicostomy withoutaugmentation for neurogenic incontinence in chil-dren. J Urol 2007; 177: 1510.
15. Sénéchal C, Limani K, Djeffal C et al: Perineo-scrotal pain after InVance suburethral sling:cadaver anatomical study. Prog Urol 2008; 18:
tinence. J Urol 2001; 165: 72. Indiana experience with artificial urinary sphinc- 456.
These authors present an interesting and appar-ently simple alternative for a difficult problem. Theyplaced a perineal polypropylene sling in 6 postpu-bertal patients with refractory neurogenic urinaryincontinence. Median followup is 33 months. Thismethodology was successfully reported in inconti-nent adults with nonneurogenic incontinence andthe authors applied the same principles to pediatricneurogenic incontinence. Local infection seems to bea problem to be overcome. Although half of the pa-tients required sling removal shortly after place-ment, it was successfully replaced in 2 of 3 and mostwere satisfied with the outcome. Surprisingly nopatient had urethral erosion likely related to incor-porating the bulbospongiosus muscle under thesling, providing additional cushioning for the ure-thra. Also, none had deterioration in bladder com-pliance but followup is rather limited.
Questions remain to be answered. 1) Should males
dure initially or should it be reserved only for those inwhom initial bladder neck repair failed and who can-not catheterize without difficulty? 2) Should surgicalmanagement for refractory incontinence be deferredto the postpubertal period when this approachseems appropriate, according to the author results?3) Although the authors report no scrotal problems,is it possible that urinary retention with bacteria inthe posterior urethra after intermittent catheteriza-tion may cause recurrent epididymitis episodes?
This is a preliminary experience with a simpletechnique, which if confirmed in larger series and atother institutions, should be added to the armamen-tarium for surgical treatment for refractory urinaryincontinence.
J. L. Pippi Salle
Division of UrologyHospital for Sick Children
Toronto, Ontario
Canada