outbreak of acute pulmonary histoplasmosis in members of a wagon train
TRANSCRIPT

Outbreak of Acute Pulmonary Histoplasmosis in
Members of a Wagon Train
TRACY L. GUSTAFSON, M.D.
LEO KAUFMAN, Ph.D.
ROBERT WEEKS, B.S.
LIBERO AJELLO, Ph.D.
Atlanta, Georgia
ROBERT H. HUTCHESON, Jr., M.D.
Nashville, Tennessee
STANLEY L. WIENER, M.D.
DWIGHT W. LAMBE, Jr., Ph.D.
Johnson City, Tennessee
TOM A. SAYVETZ, M.D.
Atlanta, Georgia
WILLIAM SCHAFFNER, M.D.
Nashville, Tennessee
From the Field Services Division, Epidemiology Program Office, and the Mycology Division, Center for Infectious Diseases, Centers for Disease Control, Atlanta, Georgia; Tennessee Department of Public Health, Nashville, Tennessee; Quillen- Dishner College of Medicine, Johnson City, Ten- nessee; and the Vanderbilt University School of Medicine, Nashville, Tennessee. Reprint requests should be addressed to Dr. Gustafson at the Epi- demiology Program Office, Centers for Disease Control, Atlanta, GA 30333. Manuscript accepted April 7, 1981.
In August 1980, an outbreak of acute pulmonary histoplasmosis occurred among participants in a wagon train as it traveled through eastern Tennessee. Of the 85 people on the train 69 (81 percent) had evidence of infection with Histoplasma capsulatum. Fifty-four people had symptomatic disease. The source of infection was traced to the site of a former winter blackbird roost in Charleston, Ten- nessee, that had been partially cleared five years earlier to make a park. Fourteen of 25 soil samples from this site were cuiture- positive for H. capsuiatum. This is the first reported outbreak to in- volve a large migrant group. The outbreak is unusual in that exposure occurred without excavation, construction or tree-cutting at the site.
Acute pulmonary histopiasmosis is a common disease in states in the
Ohio and Mississippi River valleys. However, because its clinical
manifestations are similar to those of other self-limited pulmonary
infections, the disease is difficult to recognize except in epidemic
situations. In August 1980, a migrant group of teenagers and young
adults traveling by mule-drawn wagon train experienced an epidemic
of acute pulmonary histoplasmosis. Thirty-three wagon train members
were hospitalized in a period of one week with severe influenza-like
symptoms. The infection was acquired at the site of a former winter
blackbird roost where the train had camped for only one day. Although
the soil surface was not disrupted, the group was apparently exposed
to a large dose of inhaled spores aerosolized in the course of routine
camping activities.
The wagon train was a private enterprise for the rehabilitation of
adolescents with behavior and adjustment problems. It provided an
outdoor experience in work and travel for troubled youths who would
otherwise have been referred to criminal justice or mental health in- stitutions. Most of the participants came from Pennsylvania, Arizona
and other states where histopiasmosis is not prevalent. The wagon
train originated in Tucson, Arizona, in March and completed its
cross-country trip to Pennsylvania in November 1980.
The wagon train traveled about 20 miles a day, and members
camped outdoors every night. At the time of the outbreak, the train
included 50 youths and 35 staff counselors. It consisted of seven
covered wagons, two water tanks, one bus, several trucks, and 80
horses and mules. Most of the wagon train members slept in six In- dian-style tepees, but a few slept outside or in motor vehicles. Each
tepee group functioned as a unit and was responsible for its own wagon, horses and mules. Youth members spent their time traveling, or at campsites caring for equipment and animals. Staff counselors
November 1981 The American Journal of Medlclne Volume 71 759
WAGON TRAIN HISTOPLASMOSIS-GUSTAFSON ET AL
TABLE I Symptoms in 54 Cases of Acute Pulmonary Histoplasmosis
JULY AUGUST
DATE OF ONSET
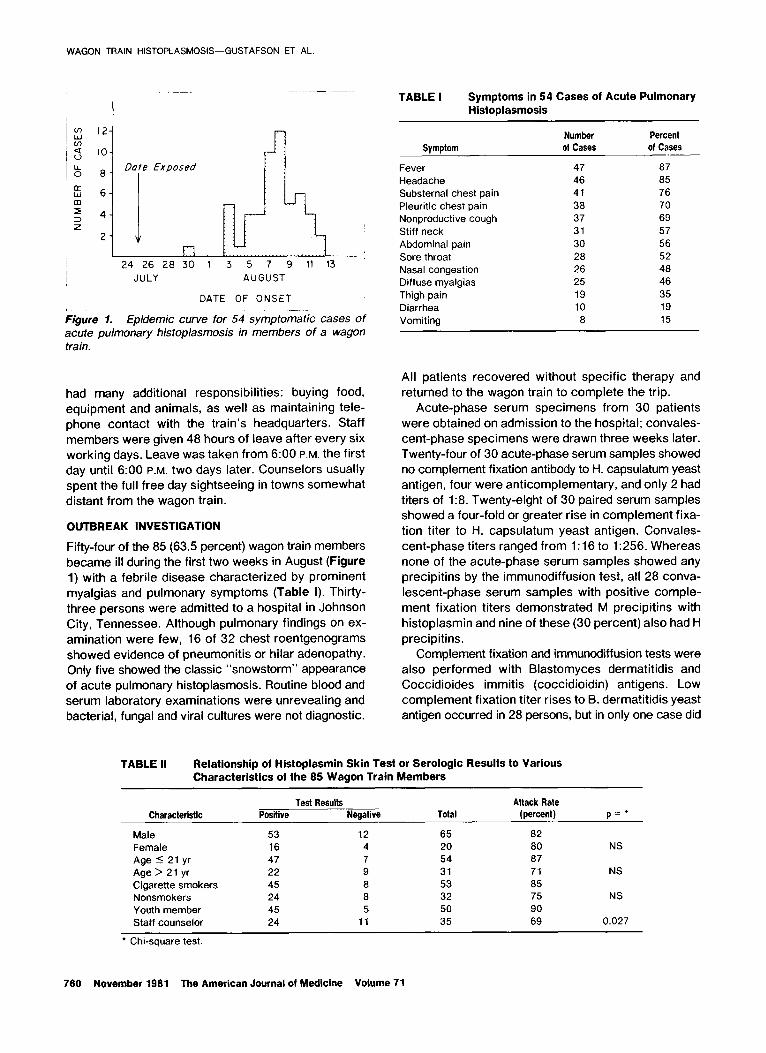
Figure 1. Epidemic curve for 54 symptomatic cases of acute pulmonary histoplasmosis in members of a wagon train.
had many additional responsibilities: buying food,
equipment and animals, as well as maintaining tele-
phone contact with the train’s headquarters. Staff
members were given 48 hours of leave after every six working days. Leave was taken from 6:00 P.M. the first
day until 6:00 P.M. two days later. Counselors usually
spent the full free day sightseeing in towns somewhat
distant from the wagon train.
OUTBREAK INVESTIGATION
Fifty-four of the 85 (63.5 percent) wagon train members became ill during the first two weeks in August (Figure
1) with a febrile disease characterized by prominent
myalgias and pulmonary symptoms (Table I). Thirty-
three persons were admitted to a hospital in Johnson City, Tennessee. Although pulmonary findings on ex-
amination were few, 16 of 32 chest roentgenograms showed evidence of pneumonitis or hilar adenopathy.
Only five showed the classic “snowstorm” appearance
of acute pulmonary histoplasmosis. Routine blood and
serum laboratory examinations were unrevealing and bacterial, fungal and viral cultures were not diagnostic.
Symptom
Fever Headache Substernal chest pain Pleuritic chest pain Nonproductive cough Stiff neck Abdominal pain Sore throat Nasal congestion Diffuse myalgias Thigh pain Diarrhea Vomiting
Number Percent of Cases of Cases
47 87 46 85 41 76 38 70 37 69 31 57 30 56 28 52 26 48 25 46 19 35 10 19 8 15
All patients recovered without specific therapy and
returned to the wagon train to complete the trip.
Acute-phase serum specimens from 30 patients
were obtained on admission to the hospital; convales-
cent-phase specimens were drawn three weeks later.
Twenty-four of 30 acute-phase serum samples showed
no complement fixation antibody to H. capsulatum yeast
antigen, four were anticomplementary, and only 2 had titers of 1:8. Twenty-eight of 30 paired serum samples
showed a four-fold or greater rise in complement fixa-
tion titer to H. capsulatum yeast antigen. Convales-
cent-phase titers ranged from 1:16 to 1:256. Whereas
none of the acute-phase serum samples showed any
precipitins by the immunodiffusion test, all 28 conva-
lescent-phase serum samples with positive comple-
ment fixation titers demonstrated M precipitins with
histoplasmin and nine of these (30 percent) also had H
precipitins. Complement fixation and immunodiffusion tests were
also performed with Blastomyces dermatitidis and Coccidioides immitis (coccidioidin) antigens. Low
complement fixation titer rises to B. dermatitidis yeast
antigen occurred in 28 persons, but in only one case did
TABLE II Relationship of Histoplasmin Skin Test or Serologic Results to Various Characteristics of the 85 Wagon Train Members
Characteristic
Male Female Age I 21 yr Age > 21 yr Cigarette smokers Nonsmokers Youth member Staff counselor
Test Results Attack Rate Positive Negative Total (percent) p=’
53 12 65 a2 16 4 20 60 NS 47 7 54 87 22 9 31 71 NS 45 8 53 85 24 8 32 75 NS 45 5 50 90 24 11 35 69 0.027
l Chi-square test.
760 November 1961 The American Journal of Medicine Volume 71
WAGON TRAIN HISTOPLASMOSIS-GUSTAFSON ET AL.
TABLE III Positive Histoplasmin Skin Test or Serologic Results Correlated with Dates of Leave for 35 Staff Counselors
Date
On Leave This Dale Not on Leave This Date Positive Percent Positive Percent Results Total Positive Results Total Positive p=*
July 19 July 21 July 23 July 25 July 27 July 29 July 31 August 2
75 20 31 65 NS 75 20 31 65 NS 83 18 29 62 NS
0 23 29 79 0.0006 100 19 31 61 NS
71 18 28 64 NS 100 21 33 64 NS
40 21 30 70 NS
* Fisher’s exact test (one-tailed).
the titer to B. dermatitidis antigen exceed that to H.
capsulatum yeast antigen. Only one person showed a
complement fixation titer rise to coccidioidin. Immu-
nodiffusion tests for B. dermatitidis and C. immitis
precipitins all gave negative results. Serologic tests
were also performed that excluded influenza, parain-
fluenza, adenovirus, respiratory syncytial virus, psit-
tacosis, mycoplasma and Legionnaire’s disease.
Six weeks after the outbreak, histoplasmin skin tests
were applied to the 85 original wagon train members.
Twenty-one new wagon train members, who had joined
the train after it left Tennessee, also were tested.
Sixty-seven of the 85 original wagon train members (79
percent) showed induration of more than 5 mm. In two
cases, the skin tests gave negative results, but the
persons had serologic evidence of acute histoplas-
mosis. Only two of 21 (10 percent) new wagon train
members had positive skin test results.
A “case” was defined as a positive skin test result
or a four-fold or greater rise in complement fixation titer
to H. capsulatum yeast antigen in any wagon train
member. This case definition was met in 69 of the 85
wagon train members (81 percent). A “symptomatic
case” was defined as any case in which documented
fever and one other symptom, or three of the symptoms
in Table I without fever, occurred. Fifty-four of the 69
cases (78 percent) were “symptomatic.”
As shown in Table II, sex, age and smoking status
were not associated with increased susceptibility to histoplasmosis. There was, however, a significant dif-
ference in attack rates among youth members (90 percent) and staff counselors (69 percent) (p = 0.027
by Chi-square test). Unlike youth members, staff
counselors did not spend all their time with the wagon
train. From two to seven counselors were on leave at
any given time, and every other day a few counselors would miss one campsite entirely. Table III lists the dates of possible exposure to H. capsulatum for the 20
days before the peak of the epidemic and the number
of staff counselors on leave on each of these days. Only campsites comptetely missed by some counselors are
shown. It is clear from this analysis that wagon train
members were exposed on July 25, 14 days before the
peak of the clinical epidemic. None of the six staff counselors on leave on July 25 had a positive histo-
plasmin skin test or serologic result, whereas 23 of the
29 staff counselors (79 percent) present at the July 25 campsite had a positive test result. In addition, one youth
member who had run away and was absent on July 25 had a negative skin test result.
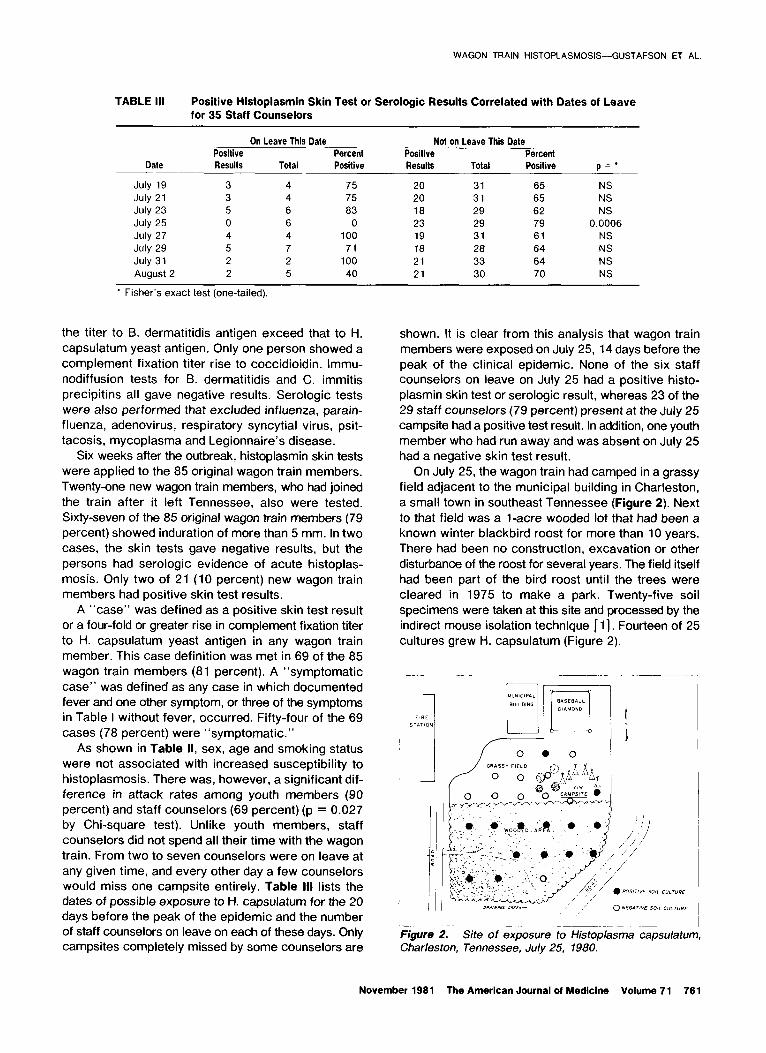
On July 25, the wagon train had camped in a grassy
field adjacent to the municipal building in Charleston,
a small town in southeast Tennessee (Figure 2). Next
to that field was a l-acre wooded lot that had been a
known winter blackbird roost for more than 10 years.
There had been no construction, excavation or other
disturbance of the roost for several years. The field itself
had been part of the bird roost until the trees were
cleared in 1975 to make a park. Twenty-five soil
specimens were taken at this site and processed by the
indirect mouse isolation technique [ 11. Fourteen of 25
cultures grew H. capsulatum (Figure 2).
-.
Figure 2. Site of exposure to Histoplasma capsdatum, Charleston, Tennessee, July 25, 1980.
November 1981 The American Journal of Medicine Volume 71 761
WAGON TRAIN HISTOPLASMOSIS-GUSTAFSON ET AL.
TABLE IV Relationship Between Tepee Group and Histoplasmin Skin Test or Serologic Results in 49 Youths Present on July 25’
Tepee Group Positive Results Attack Rate
Negative Total (percent) p=t
5 4 4 8
1,2,3,4,6 41 0 41 Totals 45 4 49
l The one youth (ruhaway) not present on July 25 is excluded from this table. 7 Fisher’s exact test (on&ailed).
50 100 .0003
The wagon train traveled through Tennessee during
the record-setting heat wave of 1980, and virtually no
rain had fallen for more than a month. On July 25, the
high temperature in this town was 89’F, the humidity
was 52 percent and the wind was from the south at 8
to 10 knots. There were several brief, light thunder-
showers on the afternoon of the 25th.
The wagon train began arriving at the campsite
around 10:00 A.M. The wagon train’s horses and mules
were tethered at the junction of the field and wooded
area, and undoubtedly raised some dust. There were,
however, no group activities or games that would have
raised large amounts of dust. Setting up camp involved
placing some stakes in the ground and digging a small firepit. Several members also entered the wooded area
to seek shade, gather firewood or urinate.
Only one group activity could be confirmed; tepee Group 5 spent the afternoon of July 25 in a nearby town.
Youth members in tepee Group 5 had a significantly
lower attack rate than did youth members in all other
tepee groups (Table IV). Ail youth members (except the
one runaway) and ail staff counselors (except the six
on leave) slept in this field on the night of July 25. It
appears, therefore, that the afternoon of July 25 was
the period of highest risk for acquiring histoplas-
mosis.
COMMENTS
The first reported outbreak of acute pulmonary histo-
plasmosis occurred in 1938, but the fact that it was
caused by the same fungus responsible for the fatal disseminated form of the disease was not recognized
until more than 10 years later [2,3]. Since then, nu-
merous outbreaks have been reported and reviewed
[3-51. These investigations have firmly established the
clinical manifestations of acute pulmonary histopias-
mosis and the association of the fungus with chicken
houses, blackbird roosts and pigeon- or bat-occupied buildings and caves.
Analyses of these outbreaks suggest that H. capsu- iatum, although worldwide in distribution, produces the large concentrations of spores necessary to cause
epidemic illness only in certain moist and heavily fer- tilized “microfoci” [6,7]. Several authors also contend
that most endemic histoplasmosis is attributable not to
small numbers of fungi distributed throughout the soil,
but to airborne spread of spores from a relatively few
concentrated foci [ 8- 111.
Despite detailed clinical descriptions and excellent
reviews, the clinical diagnosis of acute pulmonary histoplasmosis remains difficult [ 12- 151. In epidemics,
prolonged febrile illness or unusual roentgenographic
infiltrates may be the first clues that a viral agent is not
responsible. in sporadic cases, the diagnosis is rarely made at all. Improved serologic tests to confirm the
diagnosis are now available. A four-fold rise in com-
plement fixation titer to H. capsuiatum yeast antigen
provides strong evidence of acute infection. This test
can now be supplemented by the less sensitive but more specific immunodiffusion tests. The new ap-
pearance of M precipitins in convalescent serum is
considered diagnostic of acute disease. H precipitins
are the least sensitive of ail the tests (20 to 30 percent),
but are nearly 100 percent specific for recent active
infection [ 16,171.
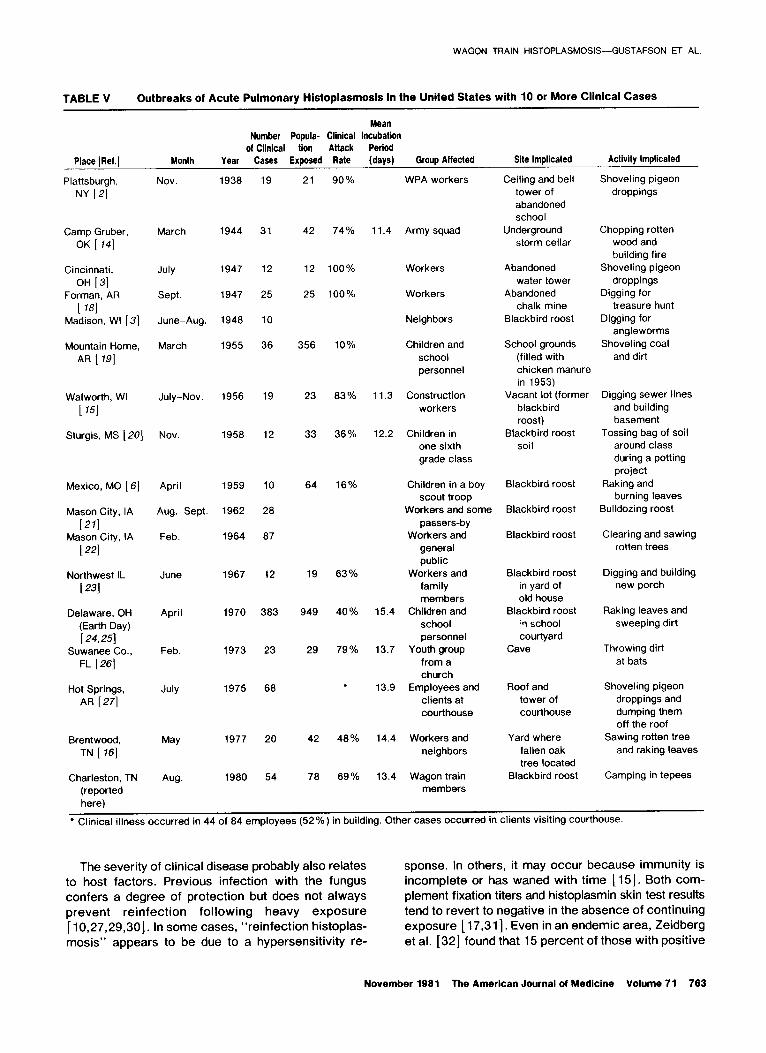
Large epidemics of acute pulmonary histopiasmosis are not rare. Sixteen of the reported outbreaks in the
United States involved 10 or more symptomatic cases
(Table V). All the states represented are considered within the endemic region [28]. Reported outbreaks
have tended to cluster in low or “fringe” endemic areas
where the “susceptible” population may be larger, but this may be a bias resulting from reports of the un-
usual.
There is no seasonal trend for outbreaks, except that indoor sites predominate in cold weather, and outdoor
locations are more common in spring and summer. Warm or dry weather is apparently not required for
aerosolization of spores. In two situations, sites were
purposely disturbed in winter after the soil was wetted
down to minimize dust. Nevertheless, both disturbances
resulted in infections [ 13,221.
Clinical attack rates have varied in these outbreaks from 10 percent to 100 percent. Because more than 99 percent of all H. capsulatum infections are asymp- tomatic, it is generally held that particularly heavy in-
halation exposure is required to produce symptomatic acute pulmonary disease [ 151. in most outbreaks, a
clear relation between the degree of dust exposure and
severity of disease can be demonstrated.
762 November 1961 The American Journal of Medicine Volume 71
WAGON TRAIN HISTOPLASMOSIS--GUSTAFSON ET AL.
TABLE V Outbreaks of Acute Pulmonary Histoplasmosis in the United States with 10 or More Clinical Cases
Mean Number Popula- Clinical incubation
of Clinical tion Anack Period Place (Ref.] Month Year Cases Exposed Rate (days) Group Affected Site Implicated Activity Implicated
Ceiling and bell tower of abandoned school
Underground storm cellar
Shoveling pigeon droppings
Plattsburgh,
NY [21 Nov 1938 19 21 90% WPA workers
1944 31 42
July 1947
Sept. 1947
June-Aug. 1948
March 1955
12 12
25 25
Chopping rotten wood and building fire
Shoveling pigeon droppings
Digging for treasure hunt
Digging for angleworms
Shoveling coal and dirt
Camp Gruber, OK [ 141
Cincinnati,
OH [31 Forman, AR
[ 181 Madison, WI [3]
Mountain Home, AR [ 191
74%
100%
100%
10
36 356 10%
11.4 Army squad
Abandoned water tower
Abandoned chalk mine
Blackbird roost
Workers
Neighbors
Children and school personnel
11.3 Construction workers
School grounds (filled with chicken manure in 1953)
Vacant lot (former blackbird roost)
Blackbird roost soil
Walworth, WI
t 751 July-Nov 1956 19 23 83%
Sturgis, MS [ 201 Nov. 1958 12 33 36%
Digging sewer lines and building basement
‘Tossing bag of soil around class during a potting project
Raking and burning leaves
Bulldozing roost
Clearing and sawing rotten trees
Digging and building new porch
Raking leaves and sweeping dirt
Throwing dirt at bats
Shoveling pigeon droppings and dumping them off the roof
Sawing rotten tree and raking leaves
Camping in tepees
12.2 Children in one sixth grade class
Children in a boy scout troop
Workers and some passers-by
Workers and general public
Workers and family members
15.4 Children and school personnel
13.7 Youth group from a church
13.9 Employees and clients at courthouse
Mexico, MO [S]
Mason City, IA
(271 Mason City, IA
[221
Northwest IL
[ 231
Delaware, OH (Earth Day)
[24,25] Suwanee Co.,
FL [ 261
Hot Springs, AR [27]
April 1959 10
Aug.-Sept. 1962 28
Feb. 1964 87
1967 12
April 1970
1973
1975
383
Feb. 23
68
64 16% Blackbird roost
Blackbird roost
Blackbird roost
19
949
29
63%
40%
79%
Blackbird roost in yard of old house
Blackbird roost :‘1 school courtyard
Cave
Roof and tower of courthouse
Yard where fallen oak tree located
Blackbird roost
42 48% 14.4 Workers and neighbors
78 69% 13.4 Wagon train members
Brentwood. TN [ 161
Charleston, TN (reported here)
1977
Aug. 1980
20
54
* Clinical illness occurred in 44 of 84 employees (52%) in building. Other cases occurred in clients visiting courthouse.
The severity of clinical disease probably also relates sponse. In others, it may occur because immunity is to host factors. Previous infection with the fungus incomplete or has waned with time [ 151. Both com- confers a degree of protection but does not always plement fixation titers and histoplasmin skin test results prevent reinfection following heavy exposure tend to revert to negative in the absence of continuing [ 10,27,29,30]. In some cases, “reinfection histoplas- exposure [ 17,311. Even in an endemic area, Zeidberg mosis” appears to be due to a hypersensitivity re- et al. [32] found that 15 percent of those with positive
November 1961 The American Journal of Medicine Volume 71 763

WAGON TRAIN HISTOPLASMOSIS-GUSTAFSON ET AL.
skin test results had negative results when retested two
years later [32]. A second host factor thought to influence the clinical
attack rate is age. In the wagon train members, whose
ages ranged from 13 to 58 years, age was not related
to acquisition or severity of disease. Younger children
are said to have a high rate of asymptomatic and mild
infections. In the four major outbreaks involving chil-
dren, the proportions of infected children with asymp-
tomatic disease were significant: 75 percent in Moun-
tain Home [ 191, 50 percent in Sturgis [20], 73 percent in Mexico [6] and 48 percent in the Earth Day outbreak
[24]. However, their exposure was less direct than that
in most outbreaks involving adults.
The incubation period of acute pulmonary histo- plasmosis is best estimated from large outbreaks in-
which exposure was limitedto one or two days. There
is excellent agreement among eight such outbreaks
listed in Table V in which the incubation period ranges
from five to 25 days with a mean of 14 days, as in this
outbreak. Reinfection histoplasmosis may have a
shorter incubation period (three to seven days), but this
is not as well established [ 15,291.
The sources of these outbreaks include all the
common habitats of H. capsulatum. One outbreak was
attributed to chicken manure, two to soil in bat-infested
caves, three to the sawing of rotten wood, three to pi-
geon droppings in old buildings and seven to the soil of
blackbird roosts. These sources are also representative
of smaller reported outbreaks, except that chicken
houses figure more prominently in small family out-
breaks [4,5]. In every outbreak, digging, raking or
otherwise aerosolizing contaminated dust or manure
was the activity leading to exposure. In most cases, only people within 10 to 20 feet of dust-raising activities
acquired the disease. Indeed, in only five outbreaks did
persons other than those actually performing the work
become ill. In three of these five outbreaks, large
populations were exposed when spores were aero-
solized within a few feet of air-conditioning intake vents
[ 19,24,27]. In the other two outbreaks, disruption of the
sites continued for several weeksand the exact nature
of exposure at these locations could not be determined
[21,22]. Sporadic cases and small family outbreaks of acute
pulmonary histoplasmosis have been attributed to seemingly mild dust exposures [ 10,331. This is the first large outbreak, however, in which no obvious disruption
of infected soil or rotten wood occurred. There was no
major dust-raising activity in the wooded area or the field
on which the wagon train members camped. Since
most of the wagon train members never entered the
wooded area, exposure probably resulted from the small
amount of dust raised in the field by the animals and by
the setting up of camp.
No previous report of an outbreak has implicated a
roost site that had been cleared of trees for years. It is
known, however, that soil can remain positive for at
least 10 years after a roost is cleared [ 71. The recently
demonstrated ability to decontaminate H. capsul-
atum-infected soil with formalin has led some to call for
regulations regarding the disturbance of blackbird roosts
[34-361. A major hindrance to efforts to control epi-
demic histoplasmosis, and perhaps to have an impact on endemic diseases as well, is the difficulty and ex-
pense involved in culturing soil samples for H. capsul-
atum. We are also unable to predict which microfoci will
support exuberant growth and heavy spore production
by the fungus. Most blackbird roosts in endemic areas
that have been occupied by birds for more than three
years are believed to support heavy growth of H. cap- sulatum. Of more than 100 of these older roosts sam-
pled in the Mississippi and Ohio River valleys, 79 per-
cent have yielded positive soil cultures (Weeks R, un-
published data). The potential public health hazard of blackbird roosts
is large, and the continuing blackbird and starling pop-
ulation explosion has provided impetus to efforts to
control the spread of H. capsulatum microfoci. Blackbird
roosts, commonly inhabited by both blackbirds and
starlings, are frequently disrupted to eliminate the nui-
sance created by large concentrations of birds. The
experience of the wagon train members suggests that caution should be exercised not only in clearing or
disrupting a roost, but also in considering possible future
uses of contaminated sites.
ADDENDUM
Since submission of the manuscript for publication, a
large outbreak of histoplasmosis due to an unidentified
source has been reported in Indianapolis [37].
ACKNOWLEDGMENT
We thank Ms. Mildred Cooper, Immunization Repre-
sentative, Tennessee Department of Public Health; Mr.
Tpm DeMelfi, Pennsylvania Department of Public Health; and Ms. Diane Riley and other members of the
wagon train for their cooperation.
REFERENCES
1. Tosh FE, Weeks RJ, Pfeiffer FR, Hendricks SL, Greer DL, Chin 62: 1-16. TDY: The use of formalin to kill Histoplasma capsulatum 3. Grayston JT, Furcolow ML: The occurrence of histoplasmosis at an epidemic site. Am J Epidemiol 1967; 85: 259-265. in epidemics-epidemiolo@cal studies. Am J Public Health
2. White FC, Hill HE: Disseminated pulmonary calcification: a 1953; 43: 665-676. report of 114 cases with observations of an antecedent 4. Lehan PH, Furcolow ML: Epidemic histoplasmosis. J Chronic pulmonary disease in 15 individuals. Am Rev Tuberc 1950; Dis 1957; 5: 489-503.
764 November 1961 The American Journal of Medicine Volume 71
WAGON TRAIN HISTOPLASMOSIS-GUSTAFSON ET AL.
5.
6.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
Sarosi GA, Parker JD, Tosh FE: Histoplasmosis outbreaks: their patterns. In, Balows A, ed: Histoplasmosis, proceed- ings of the Second National Conference. Springfield, Illinois: Charles C Thomas, 1971; 123-128.
Furcolow ML, Tosh FE, Larsh HW, Lynch HJ, Shaw G: The emerging pattern of urban histoplasmosis: studies on an epidemic in Mexico, Missouri. N Engl J Med 1961; 264: 1226-1230.
DiSalvo AF, Johnson WM: Histoplasmosis in South Carolina: support for the microfocus concept. Am J Epidemiol 1979; 109: 480-492.
Rooks R: Air-borne Histoplasma capsulatum spores. Science 1954; 119: 385-386.
Dodge HJ, Ajello L, Engelke OK: The association of a bird- roosting site with infection of school children by Histo- plasma capsulatum. Am J Public Health 1965; 55: 1203-1211.
Sutliff WD, Ajello L: Histoplasma capsulatum in the environ- ment of sporadic histoplasmosis cases. Mycopath et Mycol Appl 1970; 40: 45-51.
Furcolow ML: Epidemiology of histoplasmosis. In, Sweany HC, ed: Histoplasmosis. Springfield, Illinois: Charles C Thomas, 1960; 113-148.
Cain JC, Devins EJ, Downing JE: An unusual pulmonary dis- ease. Arch Intern Med 1947; 79: 626-641.
Wilcox KR, Waisbren BA. Martin JM: The Walworth, Wis- consin, epidemic of histoplasmosis. Ann Intern Med 1958; 49: 388-418.
Rogers DE: The spectrum of histoplasmosis in man. Med Times 1966; 94: 664-682.
Goodwin RA, Des Prez RM: State of the art: histoplasmosis. Am Rev Respir Dis 1978; 117: 929-956.
Ward JI, Weeks M, Allen D, et al.: Acute histoplasmosis: clinical, epidemiologic and serologic findings of an outbreak associated with exposure to a fallen tree. Am J Med 1979; 66: 587-595.
Buechner HA, Seabury JH, Campbell CC, Georg LK, Kaufman L, Kaplan W: The current status of serologic, immunologic and skin tests in the diagnosis of pulmonary mycoses. Chest 1973; 63: 259-270.
Washburn AM, Touhy JH, Davis EL: Cave sickness: a new disease entity? Am J Public Health 1948; 38: 1521- 1526.
Chin TDY, Ney P, Saltzman B, et al: An epidemic of histo- plasmosis among school children in Arkansas. South Med J 1956; 49:785-792.
Hagstrom RM: Epidemiologic studies by county health de- partments. Miss Doctor 1959; 37: 141-145.
D’Alessio DJ, Heeren RH, Hendricks SL, Ogilve P, Furcolow ML: A starling roost as the source of urban epidemic his- toplasmosis in an area of low incidence. Am Rev Respir
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
Dis 1965; 92: 725-731. Tosh FE, Doto IL, D’Alessio DJ, Medeiros AA, Henricks SL,
Chin TDY: The second of two epidemics of histoplasmosis resulting from work on the same starling roost. Am Rev Respir Dis 1966; 94:406-413.
Younglove RM. Terry RM, Rose NJ, Martin RJ, Schnurren- berger PR: An outbreak of histoplasmosis associated with starlings. III Med J 1968; 134: 259-263.
Brodsky AL, Gregg MB, Loewenstein MS, Kaufman L, Mallison GF: Outbreak of histoplasmosis associated with the 1970 Earth Day activities. Am J Med 1973; 54: 333-342.
Fass RJ, Saslaw SS: Earth Day histoplasmosis: a new type of urban pollution. Arch Intern Med 1971; 128: 588-590.
Lottenberg R, Waldman RH, Ajello L, Hoff GL, Bigler WW, Zellner SR: Pulmonary histoplasmosis associated with exploration of a bat cave. Am J Epidemiol 1979; 110: 156-161.
Dean AG, Bates JH, Sorrels C, et al.: An outbreak of histo- plasmosis at an Arkansas courthouse, with five cases of probable reinfection. Am J Epidemiol 1978; 108: 36-46.
Ajello L: Distribution of Histoplasma capsulatum in the United States. In, Balows A, ed: Histoplasmosis: proceedings of the Second National Conference. Springfield, Illinois: Charles C Thomas, 1971; 103-122.
Tosh FE: Reinfection histoplasmosis. In, Balows A, ed: His- toplasmosis: proceedings of the Second National Confer- ence. Springfield, Illinois: Charles C Thomas, 1971; 260-268.
Powell KE, Hammerman KJ, Dahl BA, Tosh FE: Acute rein- fection pulmonary histoplasmosis: a report of six cases. Am Rev Respir Dis 1973; 107: 374-378.
Furcolow ML: Tests of immunity in histoplasmosis. N Engl J Med 1963; 268: 357-361.
Zeidberg LD, Dillon A, Gass R: Some factors in the eprdem- iology of histoplasmin sensitivity in Williamson County, Tennessee. Am J Public Health 1951; 41: 80-88.
Byrd RB. Leavey R, Trunk G: The Chanute histoplasmosis epidemic: new variations on urban histoplasmosis. Chest 1975; 68: 791-795.
Campbell CC: Histoplasmosis outbreaks: recommendation for mandatory treatment of known microfoci of H. capsul- atum in soils. Chest 1980; 77: 6-7.
Chick EW, Flanigan C, Compton SE. et al.: Blackbird roosts and histoplasmosis: an increasing medical problem? Chest 1980; 77: 684-605.
Anderson HR: Bird roosts and histoplasmosis. J Tenn Med Assoc 1980; 73: 732-733.
Wheat LJ, Slama TG, Eitzen HE, Kohler RB, French MLV, Bi- esecker JL: A large urban outbreak of histoplasmosis: clinical features. Ann Intern Med 1981; 94: 331-337.
November 1981 The American Journal of Medicine Volume 71 765