orthodontic implants
TRANSCRIPT

IMPLANTSIMPLANTSININ
ORTHODONTICSORTHODONTICS
Dr Tony Pious
• IntroductionIntroduction
• Classification of ImplantsClassification of Implants
• Materials used for ImplantsMaterials used for Implants
• OsseointegrationOsseointegration
• Use of Implants in OrthodonticsUse of Implants in Orthodontics

..
• Implants are defined as alloplastic devices which are Implants are defined as alloplastic devices which are surgically inserted into or onto the jaw bone-surgically inserted into or onto the jaw bone-BoucherBoucher
• Linkow- Linkow- Father of oral Implantology.Father of oral Implantology.

CLASSIFICATION OF IMPLANTS.CLASSIFICATION OF IMPLANTS.Based on their locationBased on their location:-:-• SubperiostealSubperiosteal
• TransosseousTransosseous
• EndosseousEndosseous
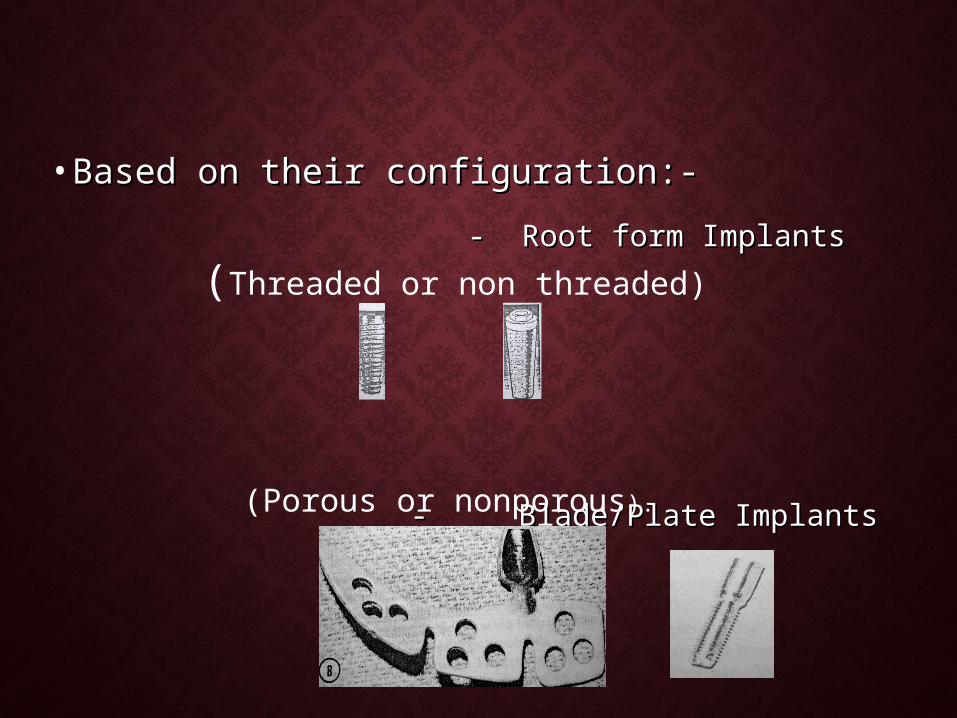
• Based on their configuration:-Based on their configuration:- - Root form Implants- Root form Implants
- Blade/Plate Implants- Blade/Plate Implants
(Threaded or non threaded)
(Porous or nonporous).

• Based on the biologic adaptation at the interfaceBased on the biologic adaptation at the interface:-:-
--Implants which osseointegrate.Implants which osseointegrate. -Implants which do not osseointegrate.-Implants which do not osseointegrate.
• Based on the loading characteristicsBased on the loading characteristics:-:- -Nonlatency implants.-Nonlatency implants. -Latency implants.-Latency implants.
• Based on anchorage requirementBased on anchorage requirement:-:- -Direct anchorage.-Direct anchorage. -Indirect anchorage.-Indirect anchorage.
• According to compositionAccording to composition:-:- -Stainless steel-Stainless steel -Cobalt-Chromium-Molybdenum (Co-Cr-Mo)-Cobalt-Chromium-Molybdenum (Co-Cr-Mo) -Titanium-Titanium -Ceramics.-Ceramics.
• Stainless steel:-Stainless steel:-
-18% Cr & 8% Ni.-18% Cr & 8% Ni. -subjected to crevice & pitting corrosion.-subjected to crevice & pitting corrosion.
• Cobalt-Chromium-Molybdenum AlloyCobalt-Chromium-Molybdenum Alloy :- :-
-used in fabrication of custom designs such -used in fabrication of custom designs such as subperiosteal frames.as subperiosteal frames.
• TitaniumTitanium:-:-most widely used metal for implants.most widely used metal for implants. -Highly reactive & readily oxidises to form oxide. -Highly reactive & readily oxidises to form oxide. -exist in 3 forms-exist in 3 forms -Alpha-Alpha -Beta-Beta -Alpha-Beta phase (most commonly used).-Alpha-Beta phase (most commonly used). Ti-6Al-4VTi-6Al-4V
• Ceramics:-Ceramics:- two types two types Bioactive-HydroxyapatiteBioactive-Hydroxyapatite Bioglass- contain oxides of Ca, Na,Bioglass- contain oxides of Ca, Na, P & Si.P & Si.
• Miscellaneous:-Miscellaneous:- -Vitreous carbon, Vitallium, Tantalum, -Vitreous carbon, Vitallium, Tantalum,
Platinum, Tungsten, Alumina, Polymers & Platinum, Tungsten, Alumina, Polymers & composites.composites.

MATERIALS USED FOR MATERIALS USED FOR IMPLANTSIMPLANTS
• In 16 &17In 16 &17thth century –Ivory dental implants . century –Ivory dental implants .
• 2020thth century-Metal Implant devices. century-Metal Implant devices.
• 1940 &1960’s-CoCrMo subperiosteal & 1940 &1960’s-CoCrMo subperiosteal & titanium blade implants.titanium blade implants.
• 1970’s-Non metal biomaterials1970’s-Non metal biomaterials
• 1982-Branemark Implant.1982-Branemark Implant.
BIOCOMPATIBILITY OF TITANIUM BIOCOMPATIBILITY OF TITANIUM IMPLANTS.IMPLANTS.
• ““Passivity”.Passivity”.
• Modulus of elasticity .Modulus of elasticity .
BIOCOMPATIBILITY OF TITANIUM BIOCOMPATIBILITY OF TITANIUM IMPLANTS:-IMPLANTS:-
• Titanium can be considered as composite Titanium can be considered as composite material.material.
• Chemical process at the Interface:Chemical process at the Interface:Types of bonding by which biomolecules stick to the Implant Types of bonding by which biomolecules stick to the Implant
surface aresurface are -Long range but weak van der waals interaction.-Long range but weak van der waals interaction. -Short range, strong chemical bonding.-Short range, strong chemical bonding. e.g.:-ionic & covalent bonds.e.g.:-ionic & covalent bonds.
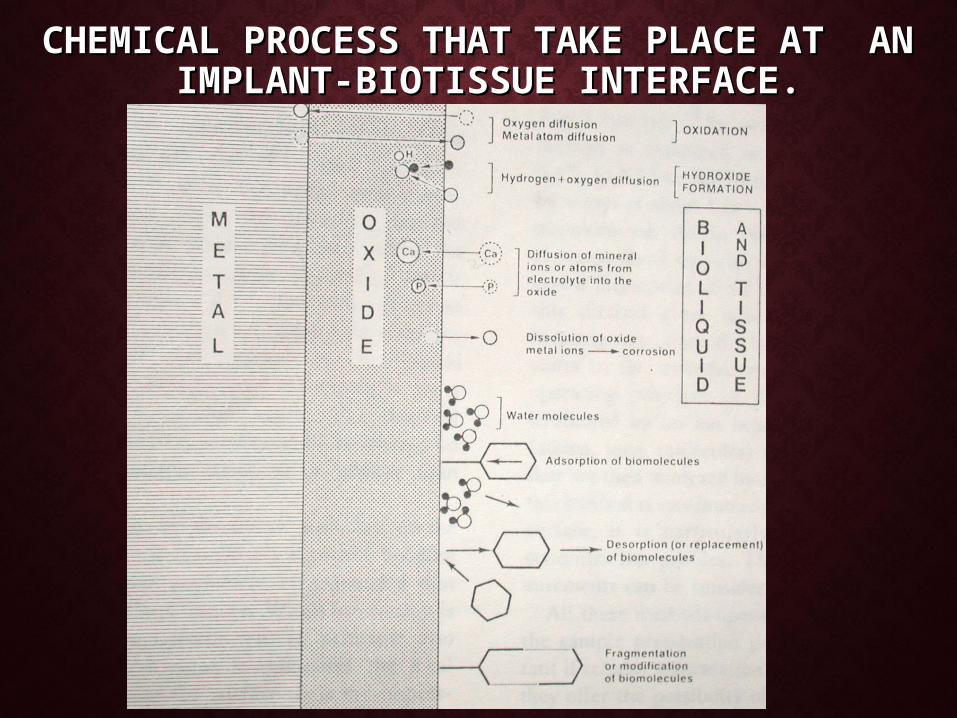
CHEMICAL PROCESS THAT TAKE PLACE CHEMICAL PROCESS THAT TAKE PLACE AT ANAT AN
IMPLANT-BIOTISSUE INTERFACE. IMPLANT-BIOTISSUE INTERFACE.
STUDIES REGARDING THE STABILITY STUDIES REGARDING THE STABILITY OF THE IMPLANT MATERIALS.OF THE IMPLANT MATERIALS.
Gainesforth & Higley (1945):Gainesforth & Higley (1945): -investigated the efficacy of Vitallium screw for orthodontic -investigated the efficacy of Vitallium screw for orthodontic
anchorage.anchorage. -Screws were inserted into the ramus of 6 dogs and -Screws were inserted into the ramus of 6 dogs and
immediately loaded to retract the maxillary cuspids.immediately loaded to retract the maxillary cuspids. --ResultsResults:-All the screws were lost within 16 to 31 days.:-All the screws were lost within 16 to 31 days.

Sherman(1978):-Sherman(1978):- - Inserted Vitreous carbon implants in 6 dogs & allowed to heal for - Inserted Vitreous carbon implants in 6 dogs & allowed to heal for
70 days before applying a force of 175gms.70 days before applying a force of 175gms. Results:-Results:-After 2wks only two implants were stable.After 2wks only two implants were stable.
Smith(1979):-Smith(1979):- - - Investigated bioglass- coated aluminum oxide implants that Investigated bioglass- coated aluminum oxide implants that
were allowed to heal for 12wks before loading them with 425gms were allowed to heal for 12wks before loading them with 425gms of force for 2-9wks.of force for 2-9wks.
Results:-Results:- All the Implants remained stable except for a slight All the Implants remained stable except for a slight movement when the force was doubled.movement when the force was doubled.

Gray(1983):-Gray(1983):- -Tested the bioglass implants & vitallium implants which were placed -Tested the bioglass implants & vitallium implants which were placed
in femur of rabbits. After 28 days healing period, loads of in femur of rabbits. After 28 days healing period, loads of 60,120,&180gms were applied.60,120,&180gms were applied.Results:-Results:-No movement of the implants occurred.No movement of the implants occurred.
Eugene Roberts(1984Eugene Roberts(1984):-):- Inserted pure titanium screws shaped implants into the femurs of Inserted pure titanium screws shaped implants into the femurs of
rabbits & after a healing period of 6-12wks, the paired implants were rabbits & after a healing period of 6-12wks, the paired implants were loaded with 100gms of force for 12 wks.loaded with 100gms of force for 12 wks.
Results:-Results:-Histologically increase in the bone mass in the area of loaded Histologically increase in the bone mass in the area of loaded implant was seen.implant was seen.
Eugene Roberts(1988):Eugene Roberts(1988):-- Examined histologic sections of dog mandibles containing rigid Examined histologic sections of dog mandibles containing rigid
titanium screws to compare the findings of bright field & polarized light titanium screws to compare the findings of bright field & polarized light microscopic illumination to microradiographs of mineralized sections.microscopic illumination to microradiographs of mineralized sections.
Results:-Results:-10% direct bone contact is sufficient to resist the implant 10% direct bone contact is sufficient to resist the implant movement. movement.
Linder-Aronson(1990):-Linder-Aronson(1990):-tested the effectiveness of Branemark tested the effectiveness of Branemark implants in monkeys.implants in monkeys.

OSSEOINTEGRATION.OSSEOINTEGRATION.
• Term & concept of Osseointegration Term & concept of Osseointegration --Branemark.Branemark.
““An intimate structural contact at the An intimate structural contact at the implant surface and adjacent vital bone implant surface and adjacent vital bone devoid of any intervening fibrous devoid of any intervening fibrous tissue.”tissue.”

EVOLUTION OF THE CONCEPT EVOLUTION OF THE CONCEPT OF OSSEOINTEGRATIONOF OSSEOINTEGRATION
• Vital microscopic studies of the rabbit fibula-Vital microscopic studies of the rabbit fibula-titanium chambered microscopes.titanium chambered microscopes.
• Series of experimentsSeries of experiments:-:- -Titanium fixtures for immobilization of autologous -Titanium fixtures for immobilization of autologous
bone grafts.bone grafts. - Tooth implants studies for healing & anchorage - Tooth implants studies for healing & anchorage
stability.stability.
• Study done on dogs to find out the load Study done on dogs to find out the load bearing capacity of implants.bearing capacity of implants.
• Optical titanium chambers were implanted Optical titanium chambers were implanted in humans-to assess the tissue reactions of in humans-to assess the tissue reactions of titanium implants.titanium implants.
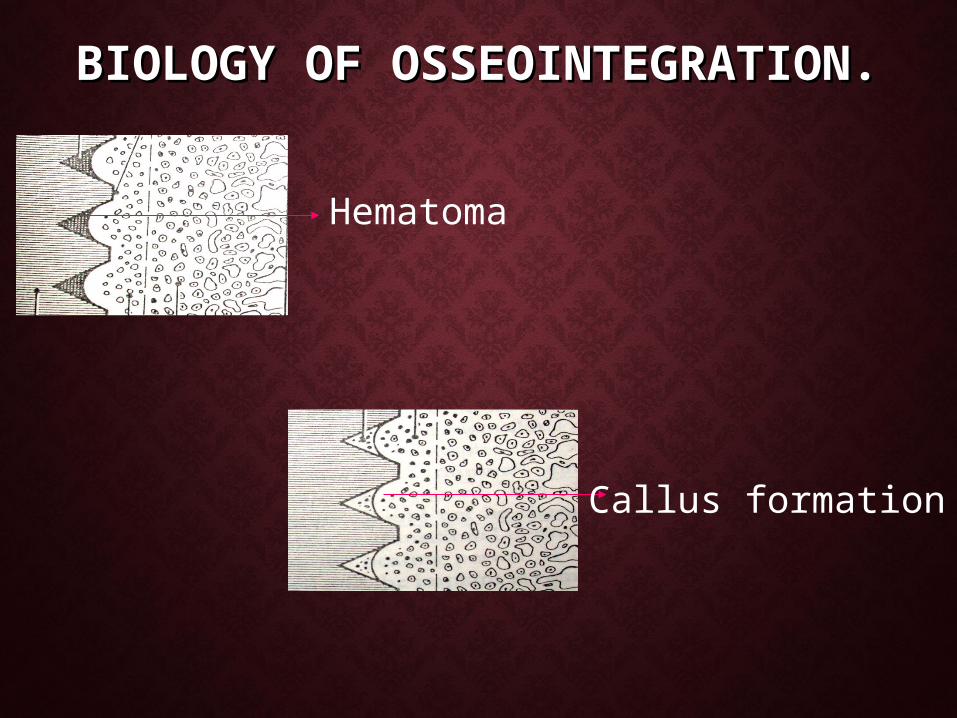
BIOLOGY OF BIOLOGY OF OSSEOINTEGRATION.OSSEOINTEGRATION.
Hematoma
Callus formation

Bone remodeling
Fibrous tissue
PRINCIPLES OF PRINCIPLES OF OSSEOINTEGRATIONOSSEOINTEGRATION
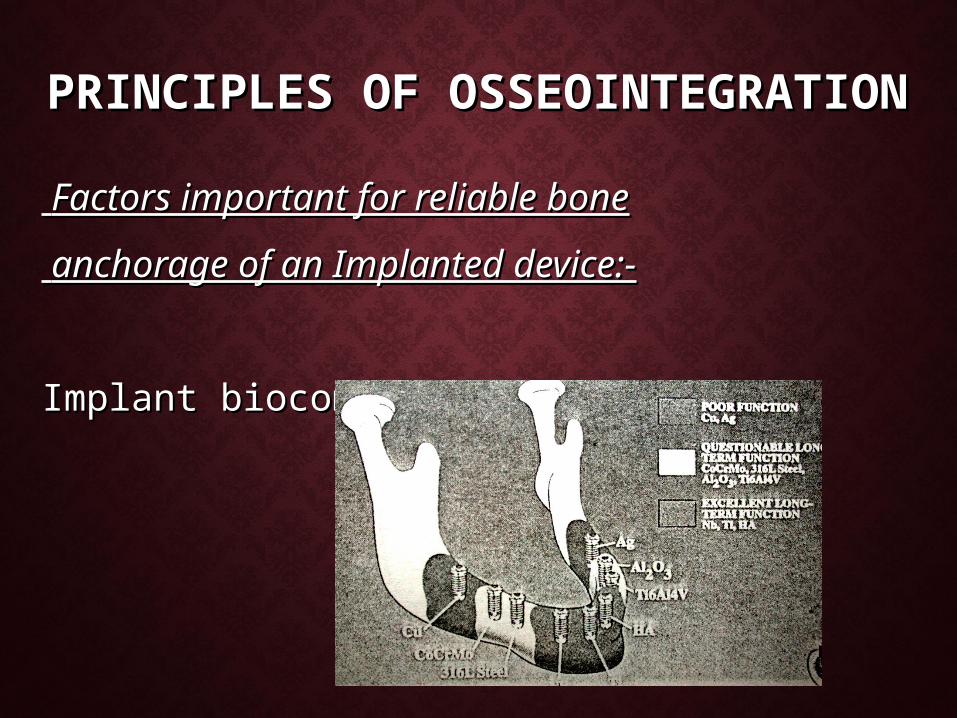
Factors important for reliable boneFactors important for reliable bone
anchorage of an Implanted device:-anchorage of an Implanted device:-
Implant biocompatibility:- Implant biocompatibility:-
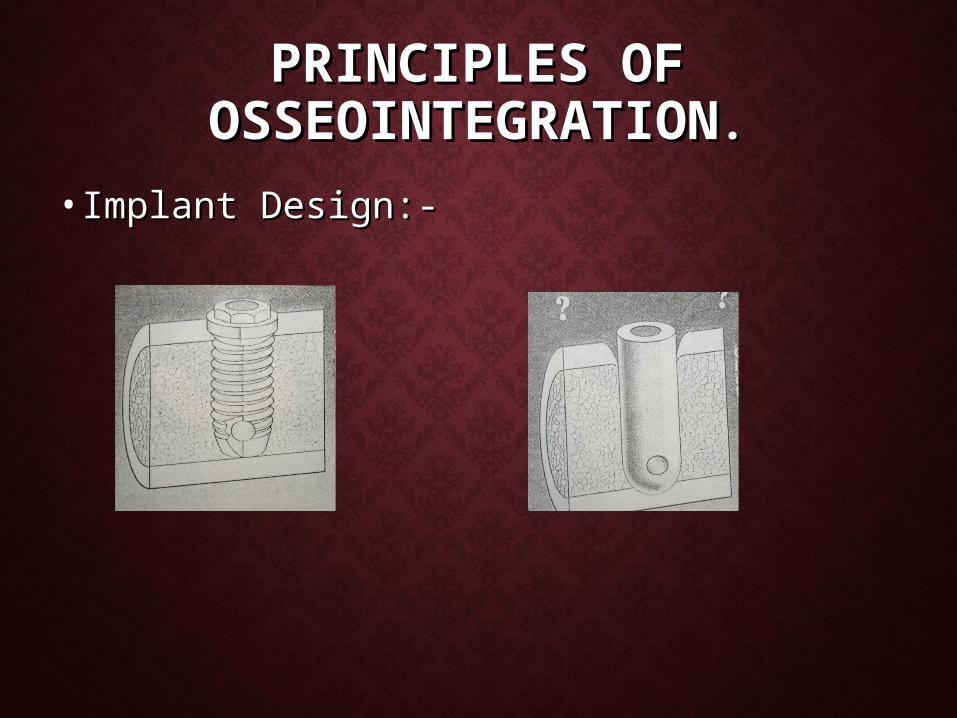
PRINCIPLES OF PRINCIPLES OF OSSEOINTEGRATIONOSSEOINTEGRATION..
• Implant Design:-Implant Design:-

• Implant surface:-Implant surface:-

• State of the host State of the host bed:-bed:-
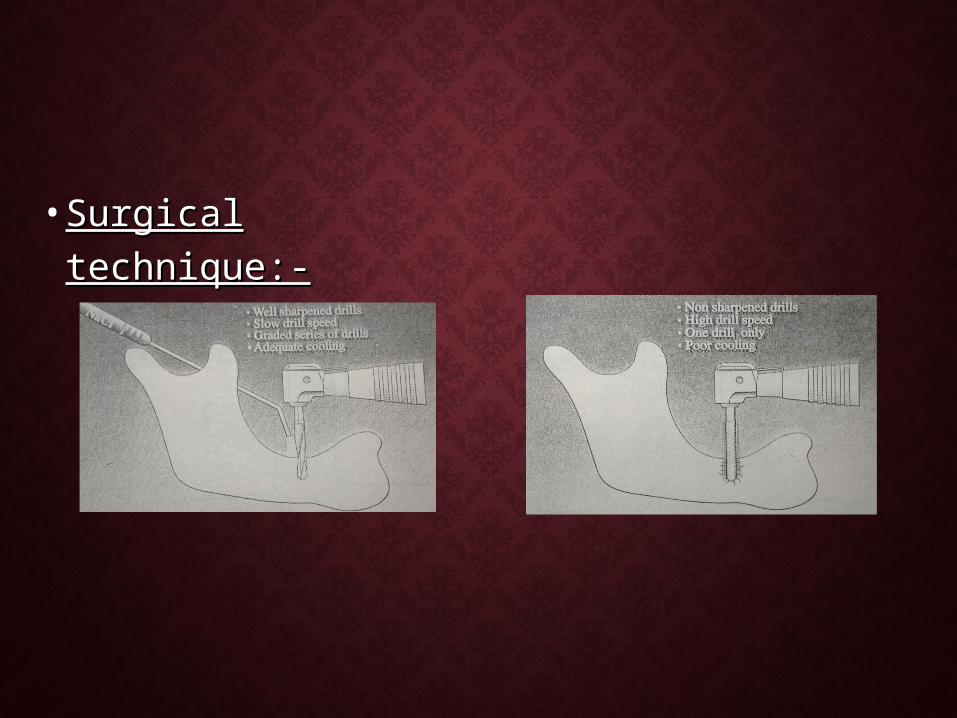
• Surgical technique:-Surgical technique:-

• Loading condition:-Loading condition:-

USE OF IMPLANTS IN USE OF IMPLANTS IN ORTHODONTICSORTHODONTICS
Growth StudiesGrowth Studies
AnchorageAnchorageOrthopaedic
Orthodontic
-Expansion
-Protraction
-Intrusion
-Space closure
-Molar Distalization.

GROWTH STUDIES:-GROWTH STUDIES:-
• Implants are the best means Implants are the best means of reference points for of reference points for studying the longitudinal studying the longitudinal growth studies.growth studies.

• Growth Rotations -Growth Rotations -Bjork & Bjork & skeiller .skeiller .
• Growth of Cleft lip & palate Growth of Cleft lip & palate patients - patients - ShawShaw
..

ANCHORAGE:-ANCHORAGE:-
Orthopeadic correction-Orthopeadic correction-
Two methods for obtaining the Skeletal anchorage:-Two methods for obtaining the Skeletal anchorage:- • Intentionally Ankylosed teeth.Intentionally Ankylosed teeth.
• Endosseous Implants. Endosseous Implants.

• Maxillary Expansion:-Maxillary Expansion:- - - Guyman(1980)Guyman(1980)
-Ankylosed teeth acted as abutments -Ankylosed teeth acted as abutments for palatal expansion in rhesus for palatal expansion in rhesus monkeys.monkeys.
-Transmit the laterally directed forces -Transmit the laterally directed forces across the midpalatal suture.across the midpalatal suture.
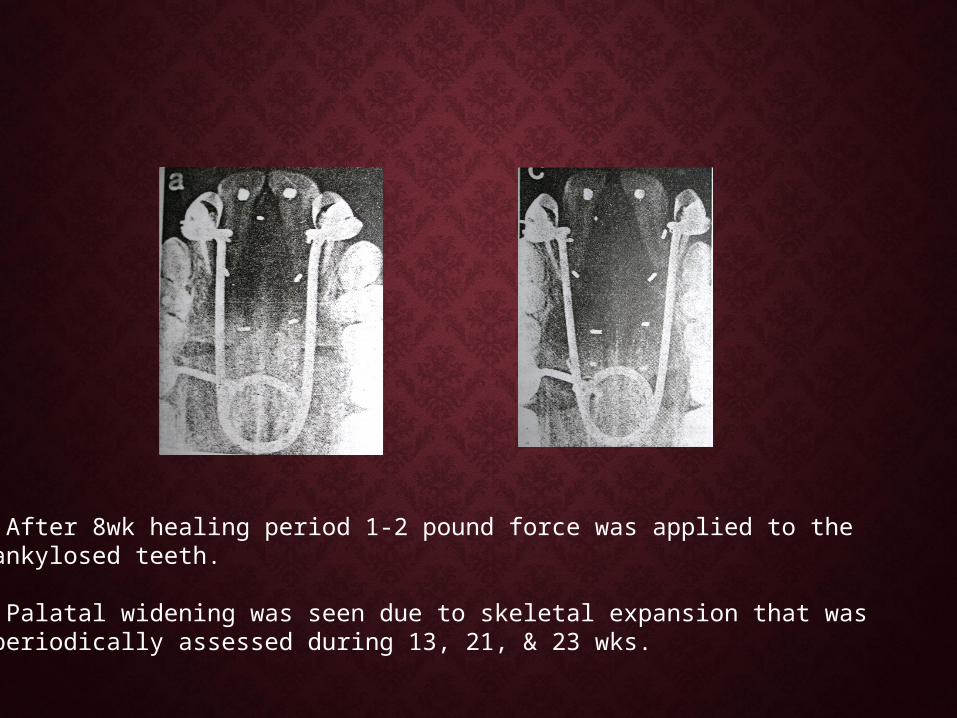
• After 8wk healing period 1-2 pound force was applied to the ankylosed teeth.
• Palatal widening was seen due to skeletal expansion that was periodically assessed during 13, 21, & 23 wks.

FRONTONASAL SUTURE EXPANSION FRONTONASAL SUTURE EXPANSION USING TITANIUM SCREWS.USING TITANIUM SCREWS.-Kiumars Movassaghi et al(1995)
Pure titanium craniofacial plates were contoured into ‘L’ shape with a 90 degree angle at the midpoint.
Plates were placed on either sides of the suture.
A distraction force of 55gms was activated across the sutures.

Increase in growth about 6mm was seen across the frontonasal suture.
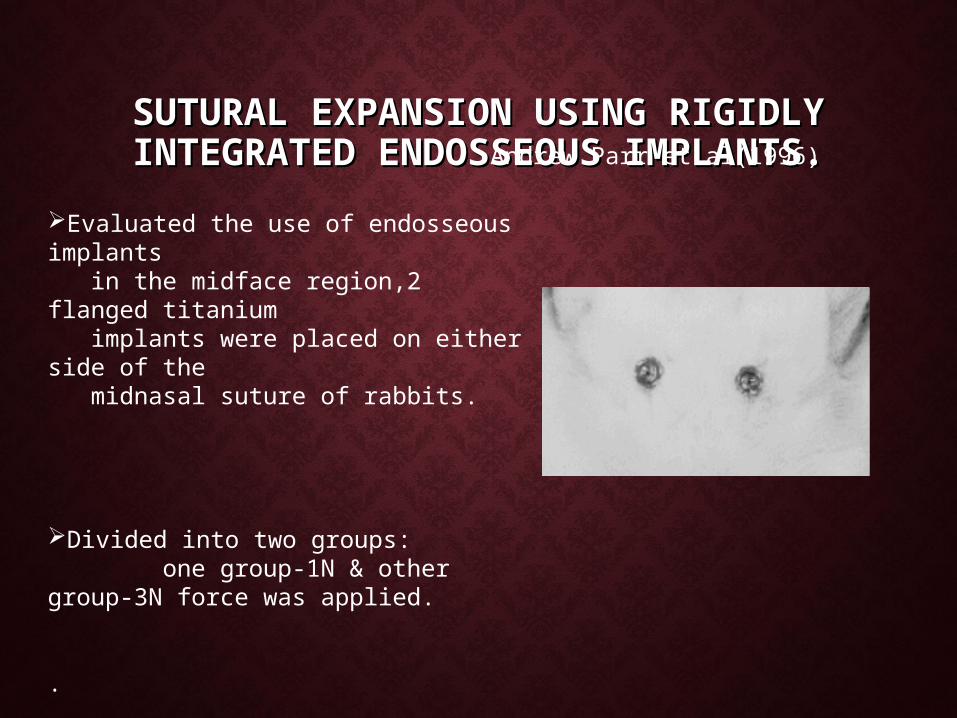
SUTURAL EXPANSION USING RIGIDLY SUTURAL EXPANSION USING RIGIDLY INTEGRATED ENDOSSEOUS INTEGRATED ENDOSSEOUS
IMPLANTS.IMPLANTS.Andrew Parr et al(1996)
Evaluated the use of endosseous implants in the midface region,2 flanged titanium implants were placed on either side of the midnasal suture of rabbits.
Divided into two groups: one group-1N & other group-3N force was applied.
.

Distance between the implants increased significantly in the loaded groups & higher in the 3N group.
An open coil spring has been compressed between the abutments to provide the expansion load.
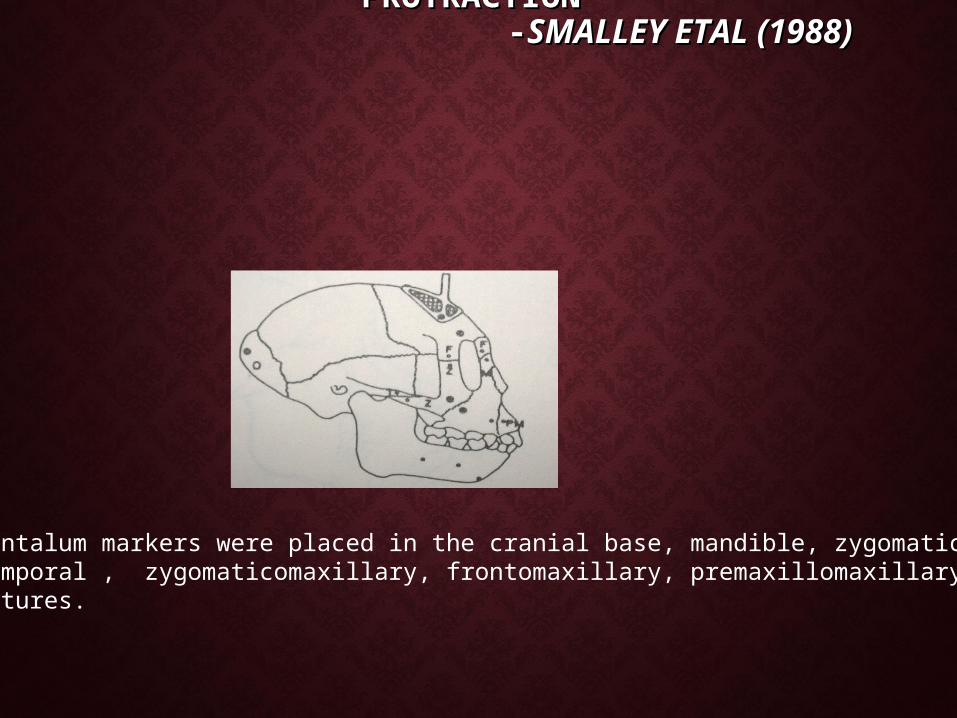
ENDOSSEOUS IMPLANTS FOR MAXILLARY ENDOSSEOUS IMPLANTS FOR MAXILLARY PROTRACTIONPROTRACTION
- -SMALLEY ETAL (1988) SMALLEY ETAL (1988)
Tantalum markers were placed in the cranial base, mandible, zygomaticoTemporal , zygomaticomaxillary, frontomaxillary, premaxillomaxillarySutures.

•A traction force of 600gm is used and protraction was done till 8mm of anterior displacement of maxillary complex occurred.

IMPLANTS FOR INTRUSIONIMPLANTS FOR INTRUSION
Skeletal Anchorage:-Creekmore(1983)
-Vitallium bone screw placed below the anterior nasal spine is used for intrusion of Upper anteriors.
-6mm of upper incisor intrusion was seen after one year.

IMPLANTS FOR SPACE CLOSURE.IMPLANTS FOR SPACE CLOSURE.
• Implanto-Orthodontics-Linkow.(1970).Implanto-Orthodontics-Linkow.(1970).
• Implant was used to replace the missing tooth.Implant was used to replace the missing tooth.
• Upper arch was consolidated using a fixed Upper arch was consolidated using a fixed appliance & in lower arch only premolar and appliance & in lower arch only premolar and molar were banded and connected by o.o4o molar were banded and connected by o.o4o rigid wire.rigid wire.
Elastic

USE OF ENDOSSEOUS IMPLANT FOR USE OF ENDOSSEOUS IMPLANT FOR CLOSURE OF EXTRACTION SITECLOSURE OF EXTRACTION SITE
• Endosseous Implants placed in the retromolar Endosseous Implants placed in the retromolar region are used to close the atrophic region are used to close the atrophic extraction site.extraction site.
-Eugene Roberts (1989)
Pontic


Buccal view after mesial translation of 2nd & 3rd molars.

Diagnostic models,2.5yrsOf post retention.
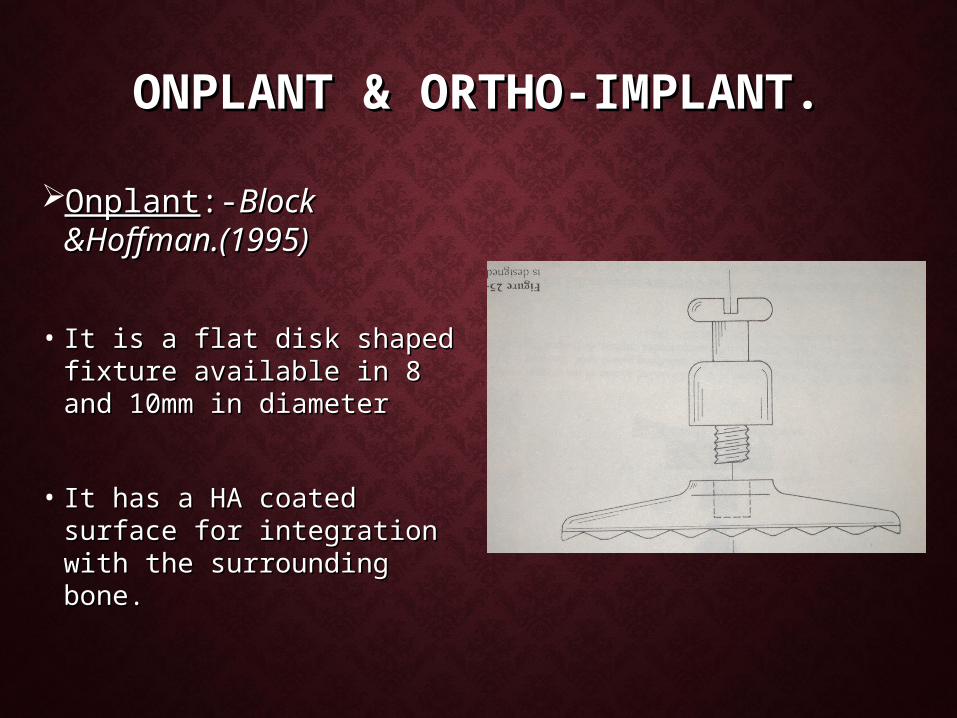
ONPLANT & ORTHO-IMPLANT.ONPLANT & ORTHO-IMPLANT.
OnplantOnplant:-:-Block Block &Hoffman.(1995)&Hoffman.(1995)
• It is a flat disk shaped It is a flat disk shaped fixture available in 8 and fixture available in 8 and 10mm in diameter10mm in diameter
• It has a HA coated surface It has a HA coated surface for integration with the for integration with the surrounding bone.surrounding bone.

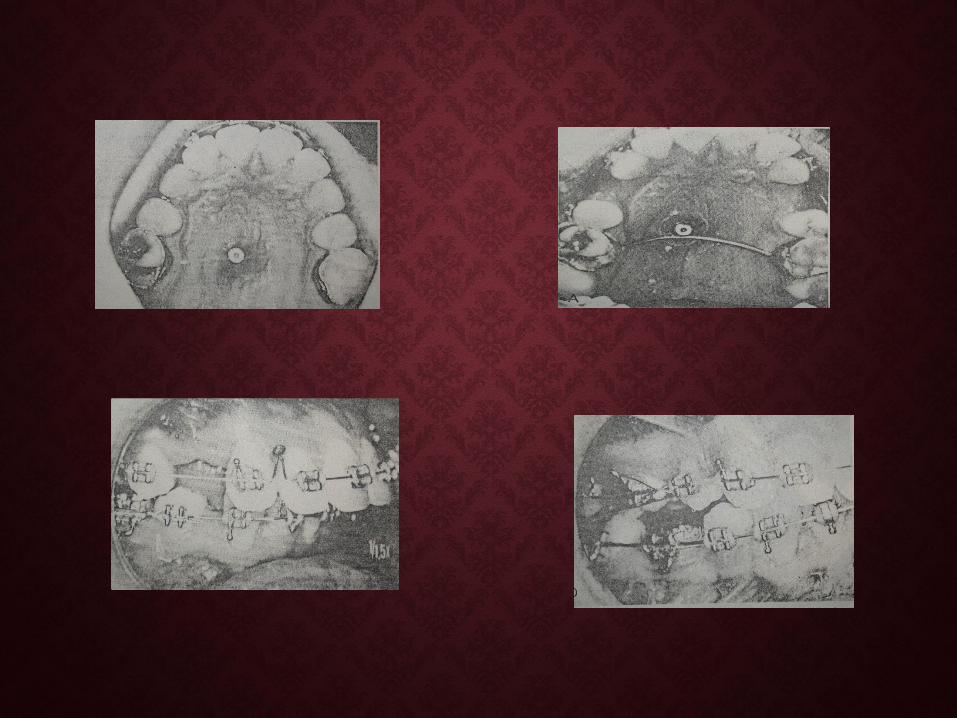
ANIMAL STUDIES: ANIMAL STUDIES:
In the dog, the onplant has been exposed & connected to the contra lateral2nd premolar with a stainless steel spring activated to deliver 110z of force.5months later tooth moved towards the onplant by 8mm from its original position.

An expansion device soldered to a traspalatal bar & secured to the expansion device to control molar distalization.
The 2nd molars were bodily distalized 6mm in 11 months.


ORTHO-IMPLANT ORTHO-IMPLANT - Celenza & Hochman
•Similar to onplant but it is an endosseous Implant.
•Its surface is sandblasted and etched to increase the adhesion to the surrounding bone


USES OF ONPLANT & ORTHO-USES OF ONPLANT & ORTHO-IMPLANTIMPLANT
• Space closure.Space closure.
• Molar distalization.Molar distalization.

PALATAL BONE SUPPORT FOR PLACEMENT PALATAL BONE SUPPORT FOR PLACEMENT OF AN ORTHODONTIC IMPLANT IS OF AN ORTHODONTIC IMPLANT IS SUFFICIENT ENOUGH WITHOUT CAUSING SUFFICIENT ENOUGH WITHOUT CAUSING
ANY DAMAGE TO THE NASAL FLOOR.ANY DAMAGE TO THE NASAL FLOOR.-Heinrich et al (1999)

IMPACTED TITANIUM POST IMPACTED TITANIUM POST FOR ANCHORAGEFOR ANCHORAGE
-Frederic Bousquet etal(1996)
•35-yr old female before treatment, showing anterior crowding.
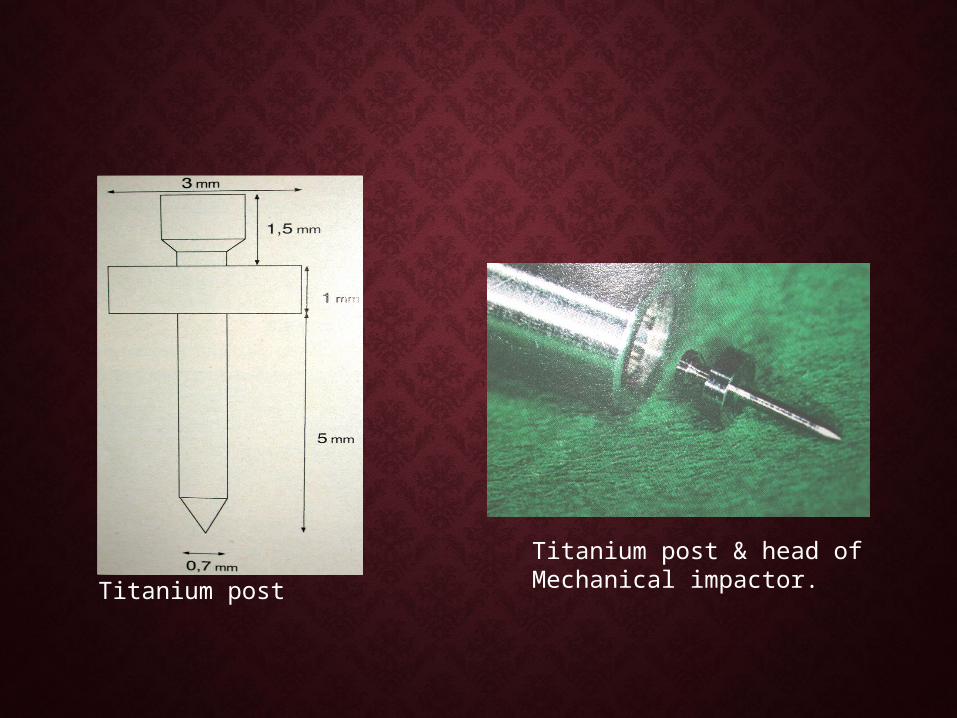
Titanium post
Titanium post & head of Mechanical impactor.

Post impacted in interdental septum between 1st molar & extraction site.
Rigid .040 wire connecting 1st molar tube to post.

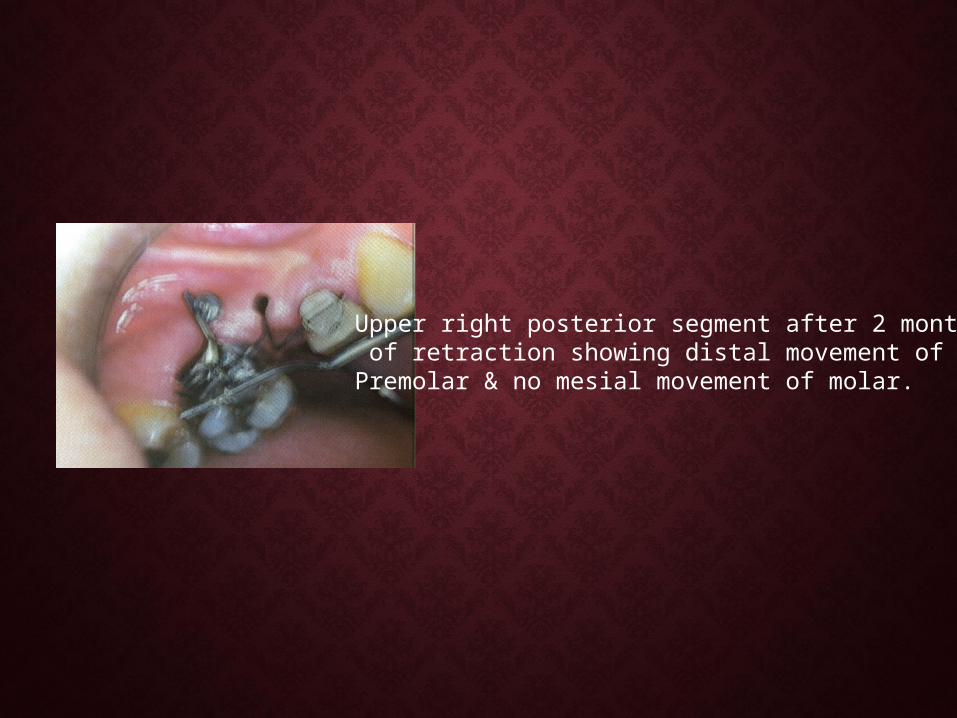
Upper right posterior segment after 2 months of retraction showing distal movement of Premolar & no mesial movement of molar.

Cast models after 18 months of treatment.

MINI-IMPLANT FOR MINI-IMPLANT FOR ORTHODONTIC ANCHORAGE:-ORTHODONTIC ANCHORAGE:-
• Mini-Implant is 1.2mm in diameter and Mini-Implant is 1.2mm in diameter and 6mm in length.6mm in length.
-Ryuzo Kanomi(1997)

After raising of mucoperiosteal flapand denuding of bone, 2mm of round bur is used.
Pilot drill used to enter bone same Distance as the length of mini-implant.
Mini-Implant inserted with accompanying screw driver.
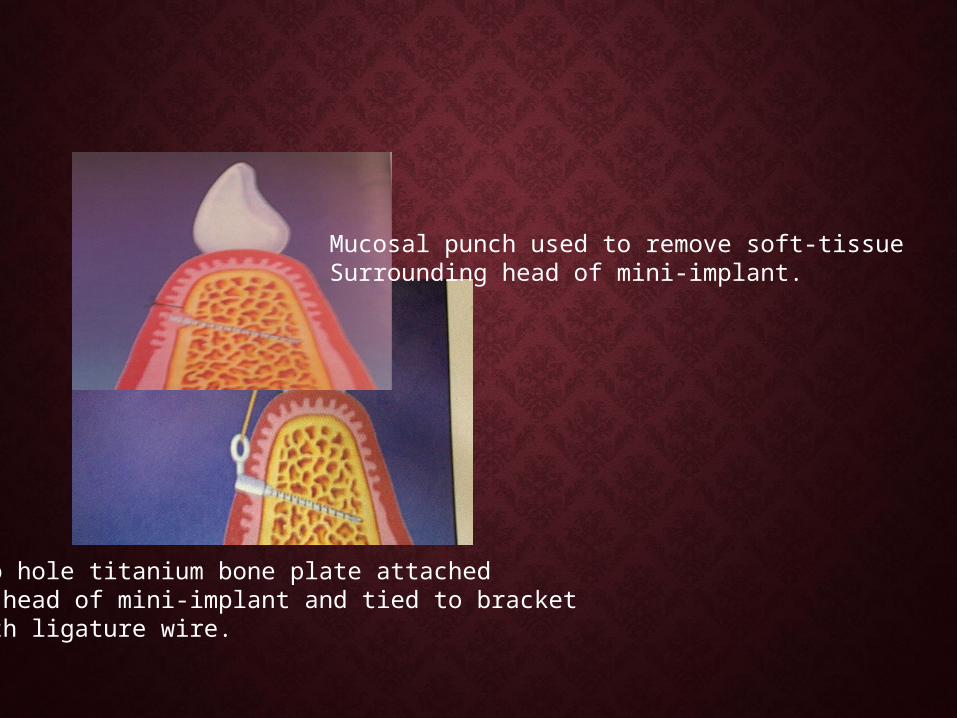
Mucosal punch used to remove soft-tissueSurrounding head of mini-implant.
Two hole titanium bone plate attached to head of mini-implant and tied to bracket with ligature wire.

Patient at start of incisor intrusion.
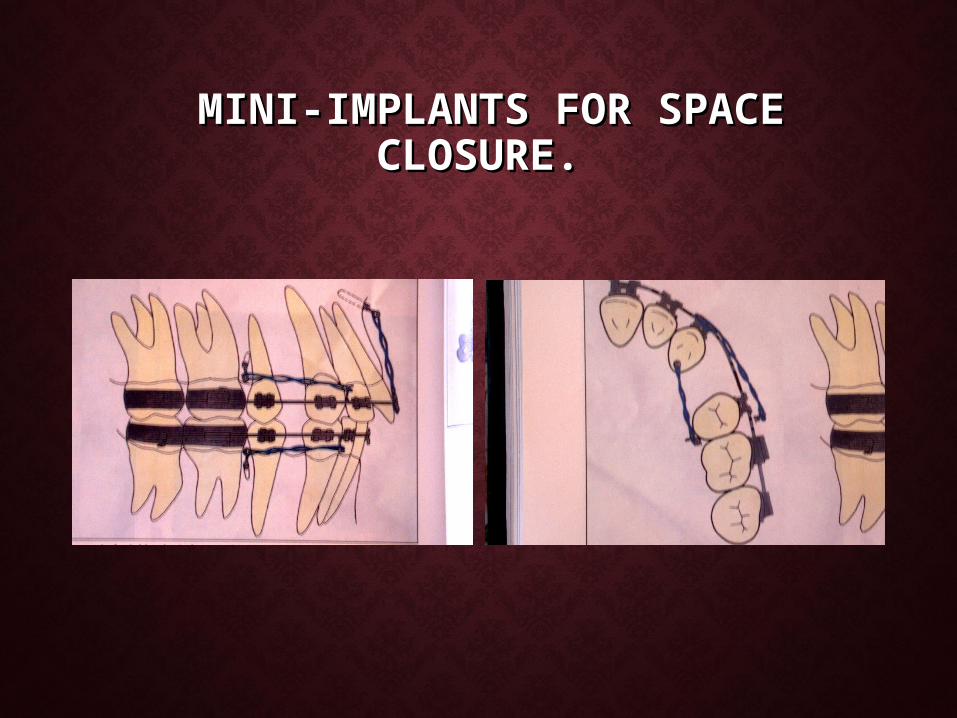
MINI-IMPLANTS FOR SPACE MINI-IMPLANTS FOR SPACE CLOSURE.CLOSURE.
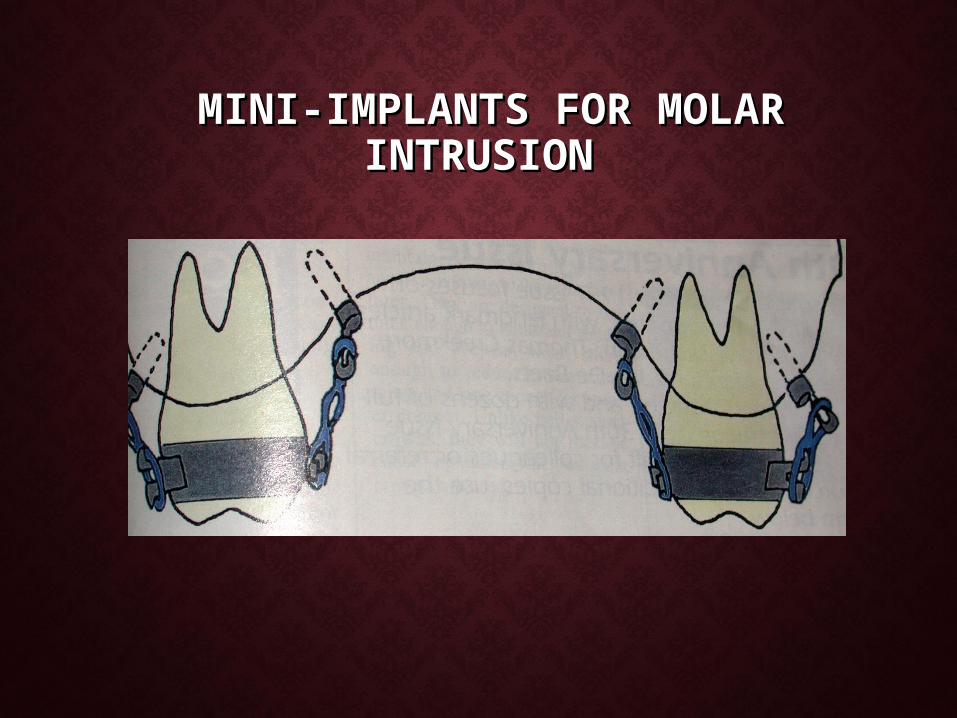
MINI-IMPLANTS FOR MOLAR MINI-IMPLANTS FOR MOLAR INTRUSIONINTRUSION

SKELETAL ANCHORAGE SYSTEM FOR SKELETAL ANCHORAGE SYSTEM FOR OPEN BITE CORRECTIONOPEN BITE CORRECTION -Umemori , Sugawara etal (1999)
• Control of vertical dimension is very important in correction of anterior open bite
•‘L’ shaped titanium miniplates are used as aSource of anchorage for intruding the molars.

• Procedure for miniplate Procedure for miniplate insertion:-insertion:-


Pretreatment facial photographs
Pretreatment intraoral photographs

Post treatment intraoral photographs
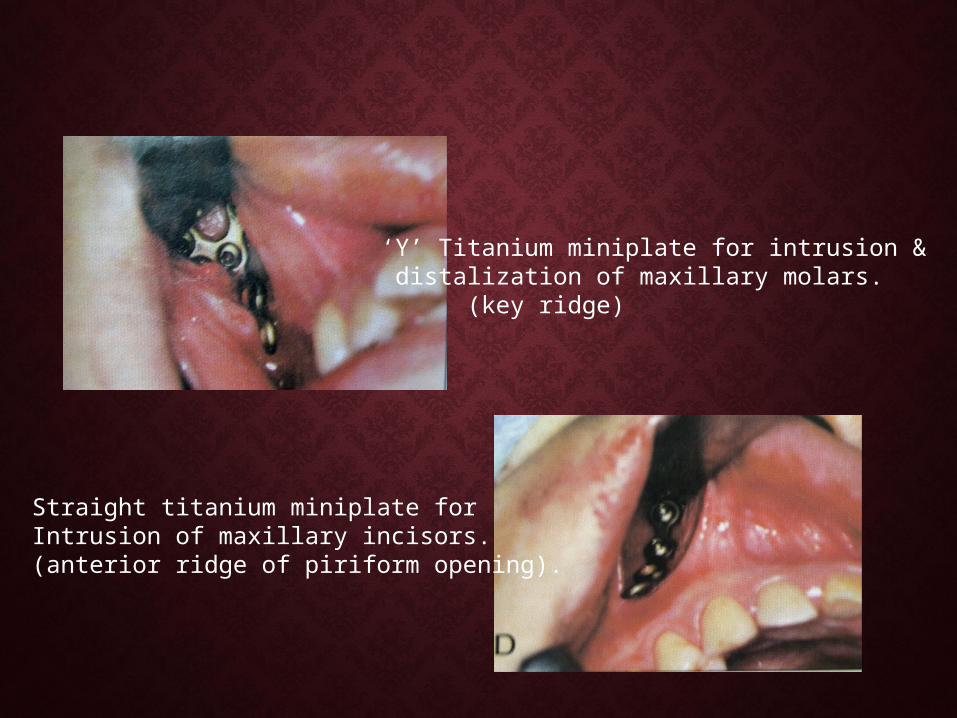
‘Y’ Titanium miniplate for intrusion & distalization of maxillary molars. (key ridge)
Straight titanium miniplate for Intrusion of maxillary incisors.(anterior ridge of piriform opening).

INTRUSION OF MAXILLARY ANTERIOR INTRUSION OF MAXILLARY ANTERIOR TEETH USING SASTEETH USING SAS
Before treatment Intrusion of maxillary anteriors
After treatment

MICROIMPLANT (ABSOANCHOR)MICROIMPLANT (ABSOANCHOR)Kyung, Park et al
Recent among the implants – Microimplant.
To overcome disadvantages of conventional Osseointegrated implants like -size, procedure of insertion, cost, & bulkiness.
Diameter is 1.2mm but available in different sizes.


Usually 4-5mm length of implant with 1.2-1.3mm diameter will provide adequate retention, but in maxilla a microimplant of 6-8mm is used.
Microimplant insertion:-

Periapical radiograph to see the root approximation.
• NiTi coil spring applied to maxillary buccal & lingual and mandibular buccal microimplants.
MICRO IMPLANTMICRO IMPLANT
• Dimension of micro implant are 1.2mm in diameter Dimension of micro implant are 1.2mm in diameter & 6mm in length.& 6mm in length.
-Park et al
28yr old female with CL-I bialveolar protrusion before treatment.

PLACED IN THE BUCCAL ALVEOLAR BONE BETWEEN PLACED IN THE BUCCAL ALVEOLAR BONE BETWEEN 22NDND PREMOLAR &1 PREMOLAR &1STST MOLAR IN THE UPPER ARCH & MOLAR IN THE UPPER ARCH & BETWEEN 1BETWEEN 1STST MOLAR & 2 MOLAR & 2NDND MOLAR IN THE LOWER MOLAR IN THE LOWER
ARCH. ARCH.
Placement of maxillary microscrew. Mandibular microscrew.

Initial maxillary canine retraction force applied withtieback between micro-implant & canine.
After 2 months of treatment, maxillaryanterior retraction force applied with nickel titanium coil spring.

Mandibular micro-implants between 1st & 2nd molars. Force applied with elastic thread between microscrews & mandibular archwire.

Mechanism of bodily retraction of anterior segment, with force applied against microimplant passing near center of resistance of six anterior teeth.
Mandibular microimplant uprights & intrudes the molars.

Patient after 18 months of treatment.
Superimposition of pre & post- treatment cephalometric tracings.
MICRO-IMPLANT FOR ANCHORAGEMICRO-IMPLANT FOR ANCHORAGEIN LINGUAL ORTHODONTICSIN LINGUAL ORTHODONTICS
19yr old female with skeletal CL-II malocclusion before treatment.

Palatal microscrew should be implanted into the alveolar boneat 30-40 degree between 1st & 2nd molar to avoid root damage.

Lingual Sliding mechanics using nickel titanium coil springsto microimplants.

Patient after 16 months of treatment.
Superimpositions of cephalometric tracings before & after treatment.

28yr old female CL-II patient with lip protrusion & gummy smile before treatment.

Insertion site measured from guide bar on bite-wing x-ray
Stab incision for flap reflectionDrilling through cortical bone only.
Microimplant insertion.

Maxillary .017x.o25 ss closing loop archwire & .016x.016ss overlay intrusion archwire used to retract anterior teeth upward & backward.

Schematic of retraction wire.

Improvement in profile & gummy smile after treatment.

USE OF OSSEOINTEGRATED USE OF OSSEOINTEGRATED IMPLANTS IN IMPLANTS IN
UNILATERAL CLEFT LIP & PALATE UNILATERAL CLEFT LIP & PALATE PTS.PTS.
• Unilateral cleft pts who needed maxillary Unilateral cleft pts who needed maxillary lateral bony defect in the alveolar region lateral bony defect in the alveolar region restricts orthodontic accomplishment.restricts orthodontic accomplishment.
• Late secondary bone grafting to the cleft region Late secondary bone grafting to the cleft region followed by the insertion of the followed by the insertion of the Osseointegrated implants provides good Osseointegrated implants provides good retention to the maxillary arch.retention to the maxillary arch.
Hiroaki et al (1999)
BIBLIOGRAPHY.BIBLIOGRAPHY.
• Implants in dentistry-Hobkirk.Implants in dentistry-Hobkirk.• Block & Kent- Oral Implantology.Block & Kent- Oral Implantology.• Science of dental materials- Skinner.Science of dental materials- Skinner.• Orthodontic principles & practice-Graber & Orthodontic principles & practice-Graber &
Vanarsdall.Vanarsdall.

• Bone responses to orthodontic forces on vitreous carbon Bone responses to orthodontic forces on vitreous carbon dental implants –Alan Sherman AJO:JULY 78.dental implants –Alan Sherman AJO:JULY 78.
• Bone dynamics associated with the controlled loading of Bone dynamics associated with the controlled loading of bioglass coated aluminum oxide endosteal implants-John bioglass coated aluminum oxide endosteal implants-John Smith AJO:DEC 79.Smith AJO:DEC 79.
• Ankylosed teeth as abutments for palatal expansion in Ankylosed teeth as abutments for palatal expansion in rhesus monkeys. Guyman et al AJO :sep 83.rhesus monkeys. Guyman et al AJO :sep 83.
• Osseous adaptation to continuous loading of rigid Osseous adaptation to continuous loading of rigid endosseous implants. AJO :AUG 84.endosseous implants. AJO :AUG 84.
• Osseointegrated titanium implants for maxillofacial Osseointegrated titanium implants for maxillofacial protraction-Smalley et al AJO:OCT 88.protraction-Smalley et al AJO:OCT 88.

• Implant-Orthodontics-Linkow JCO MAY 70.Implant-Orthodontics-Linkow JCO MAY 70.
• Possibility of skeletal anchorage- Creekmore JCO APR 83.Possibility of skeletal anchorage- Creekmore JCO APR 83.
• Absolute anchorage device-Hoffman & block AJO MAR 95.Absolute anchorage device-Hoffman & block AJO MAR 95.
• Rigid implant anchorage to close a mandibular first molar extraction site Rigid implant anchorage to close a mandibular first molar extraction site –Roberts et al JCO:DEC 94.–Roberts et al JCO:DEC 94.
• Osseointegration and its experimental background.-J.Prosth. dent sep 83.Osseointegration and its experimental background.-J.Prosth. dent sep 83.
• Biocompatibility of titanium implants –kasemo. J.Prosth.dent jun 83.Biocompatibility of titanium implants –kasemo. J.Prosth.dent jun 83.
• Endosseous implants as anchorage to protract molars and close an Endosseous implants as anchorage to protract molars and close an atrophic extraction site.-Roberts, Marshall AO sep 89.atrophic extraction site.-Roberts, Marshall AO sep 89.

• Frontonasal suture expansion in rabbits using titanium screws.-Frontonasal suture expansion in rabbits using titanium screws.-Movassaghi et al J. of oral max. surg 95.Movassaghi et al J. of oral max. surg 95.
• Sutural expansion in using endosseous implants –Rabbit study-Parr AO Sutural expansion in using endosseous implants –Rabbit study-Parr AO may 96.may 96.
• Use of impacted titanium post for orthodontic anchorage –Bousquet et al Use of impacted titanium post for orthodontic anchorage –Bousquet et al JCO AUG 96.JCO AUG 96.
• Mini-Implant-Ryuzo kanomi. JCO 97.Mini-Implant-Ryuzo kanomi. JCO 97.
• Skeletal Anchorage System-Sugawara JCO DEC 99.Skeletal Anchorage System-Sugawara JCO DEC 99.

• Micro-Implant anchorage for treatment Micro-Implant anchorage for treatment of skeletal class-I Bialveolar protrusion-of skeletal class-I Bialveolar protrusion-Hyo-Sang Park.2001 JUL JCO.Hyo-Sang Park.2001 JUL JCO.

MAGNETSMAGNETS
IN IN
ORTHODONTICSORTHODONTICS

• IntroductionIntroduction
• Types of magnetic materials Types of magnetic materials
• Properties of magnetsProperties of magnets
• Application of magnets in orthodontics.Application of magnets in orthodontics.

• In 1953, magnets were first used for denture In 1953, magnets were first used for denture retention by retention by BEHRAN & EGAN.BEHRAN & EGAN.
• Use of magnets in orthodontic- Use of magnets in orthodontic- BLECHMAN &BLECHMAN & SMILEY.SMILEY.
PROPERTIES OF MAGNETSPROPERTIES OF MAGNETS
• Flux DensityFlux Density

• In dentistry, ferromagnetic materials with static field In dentistry, ferromagnetic materials with static field are used.are used.
• Magnetocrystalline Anisotropy.Magnetocrystalline Anisotropy.
• Coercivity.Coercivity.

• Coulombs lawCoulombs law:-:-This law states that This law states that force between two magnetic poles is force between two magnetic poles is directly proportional to magnitude & directly proportional to magnitude & inversely proportional to square of the inversely proportional to square of the distance between them.distance between them.
• Curie pointCurie point:-:-Pierre Curie(1859-1906)Pierre Curie(1859-1906)

• High force to volume ratio.High force to volume ratio.
• Maximal force at shorter distances.Maximal force at shorter distances.
• No interruption of magnetic force lines by No interruption of magnetic force lines by intermediate media.intermediate media.
• No energy loss. No energy loss.

TYPES OF MAGNETIC TYPES OF MAGNETIC MATERIALSMATERIALS
• Platinum-cobalt (Platinum-cobalt (Pt-coPt-co))• Aluminium-Nickel-Cobalt(Aluminium-Nickel-Cobalt(Al-Ni-CoAl-Ni-Co))• FerriteFerrite• Chromium-cobalt-IronChromium-cobalt-Iron• Samarium Cobalt(Samarium Cobalt(SmCoSmCo))• Neodymium-Iron-Boron(NdNeodymium-Iron-Boron(Nd22FeFe1414BB))

• AdvantagesAdvantages:-:- -Continuous force is exerted.-Continuous force is exerted. - Eliminates the patient co-operation.- Eliminates the patient co-operation. -No friction.-No friction.
• DisadvantagesDisadvantages:-:- -Tarnish & corrosion products are cytotoxic.-Tarnish & corrosion products are cytotoxic. -Cost factor.-Cost factor.
• Biological effect of magnetic forces:-Biological effect of magnetic forces:-
AAronsonronson:-thinning of epithelium under :-thinning of epithelium under attracting & repelling magnets.attracting & repelling magnets.
McDonald McDonald - - proliferative activity of proliferative activity of fibroblasts in presence of static magnetic fieldfibroblasts in presence of static magnetic field
Lars Bondemark & KurolLars Bondemark & Kurol studied changes in studied changes in human dental pulp and gingival tissue. human dental pulp and gingival tissue.

CLINICAL APPLICATIONS OF CLINICAL APPLICATIONS OF MAGNETS.MAGNETS.
Orthopaedic - Expansion
-Growth modulation
Orthodontic -Tooth Intrusion
-Space closure
-Molar Distalization.
-Retainer.
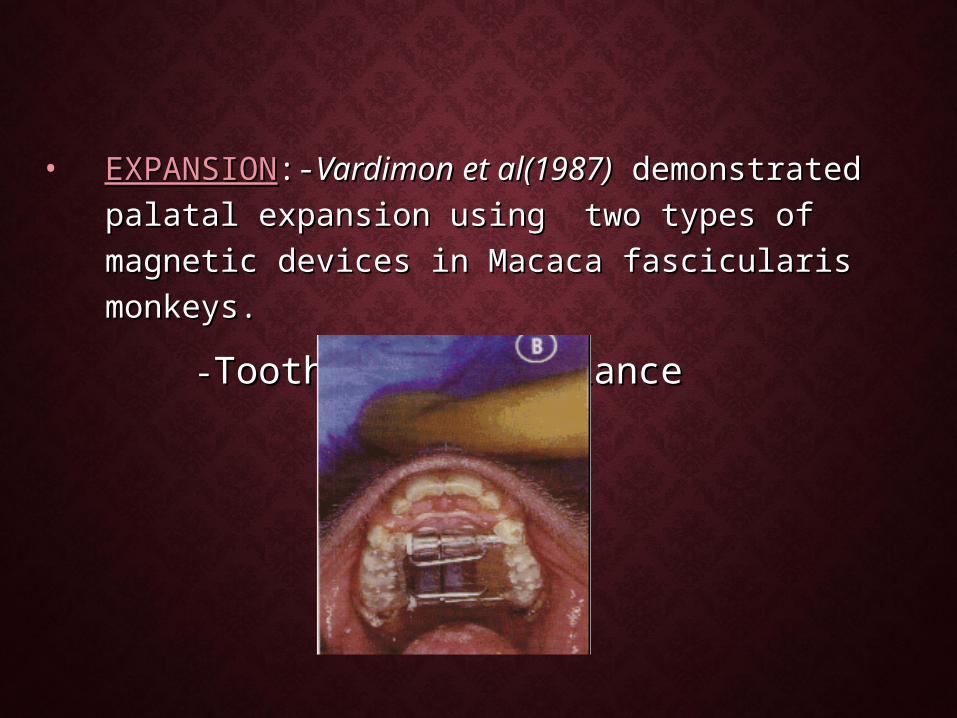
• EXPANSIONEXPANSION:-:-Vardimon et al(1987)Vardimon et al(1987) demonstrated demonstrated palatal expansion using two types of magnetic palatal expansion using two types of magnetic devices in Macaca fascicularis monkeys.devices in Macaca fascicularis monkeys.
--Tooth borne applianceTooth borne appliance

• Tissue borne appliance (attached Tissue borne appliance (attached directly to palate by endosseous directly to palate by endosseous pins).pins).
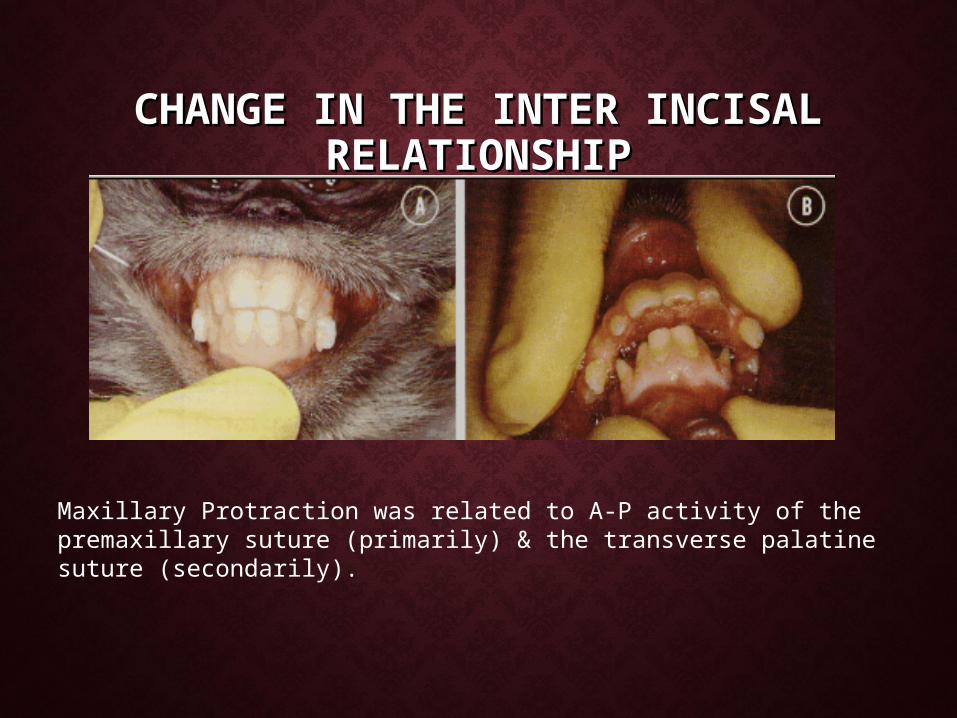
CHANGE IN THE INTER INCISAL CHANGE IN THE INTER INCISAL RELATIONSHIPRELATIONSHIP
Maxillary Protraction was related to A-P activity of the premaxillary suture (primarily) & the transverse palatine suture (secondarily).
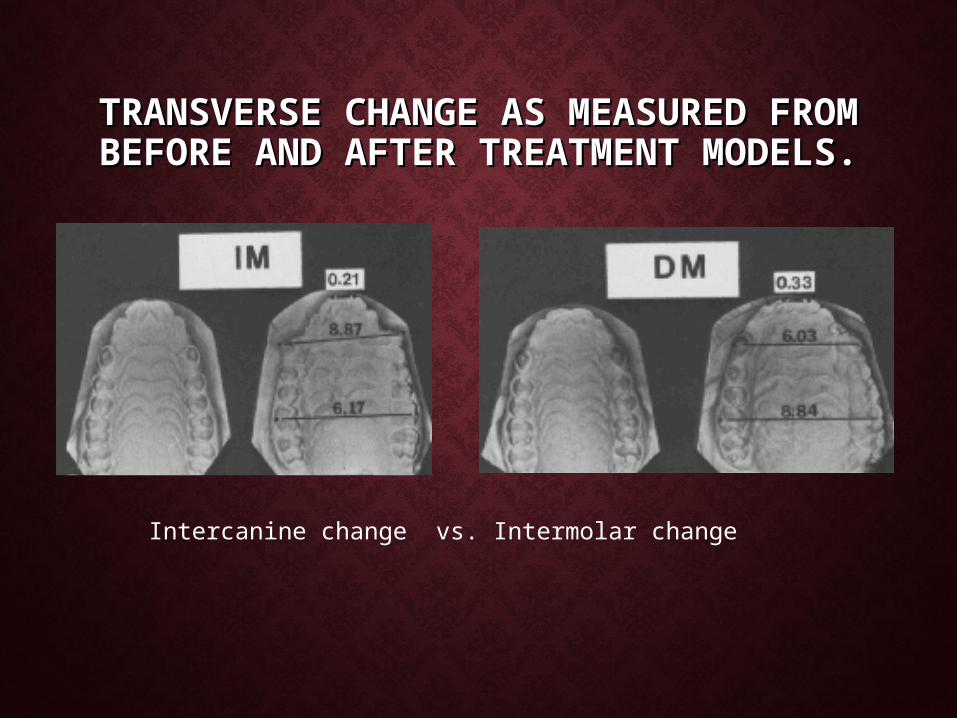
TRANSVERSE CHANGE AS MEASURED TRANSVERSE CHANGE AS MEASURED FROM BEFORE AND AFTER FROM BEFORE AND AFTER
TREATMENT MODELS.TREATMENT MODELS.
Intercanine change vs. Intermolar change

• Functional Orthopaedic Magnetic Functional Orthopaedic Magnetic AppliancesAppliances:-:-Vardimon(1989)Vardimon(1989)
--for correction of CL-IIfor correction of CL-II


4 types of functional magnetic system:-


• Magnetic Twin BlockMagnetic Twin Block:-:-Clark(1996)Clark(1996)
--Samarium cobalt Samarium cobalt magnets were magnets were embedded in the embedded in the inclined surface of the inclined surface of the twin block in attractive twin block in attractive mode.mode.
• Magnetic Activator Device(MAD):-Magnetic Activator Device(MAD):- --DarendilierDarendilier (1993) developed this magnetically (1993) developed this magnetically
active functional appliance.active functional appliance.
-MAD I-mandibular deviations-MAD I-mandibular deviations -MAD II-CLII malocclusion-MAD II-CLII malocclusion -MADIII-CLIII malocclusion-MADIII-CLIII malocclusion -MADIV-skeletal open bite correction.-MADIV-skeletal open bite correction.
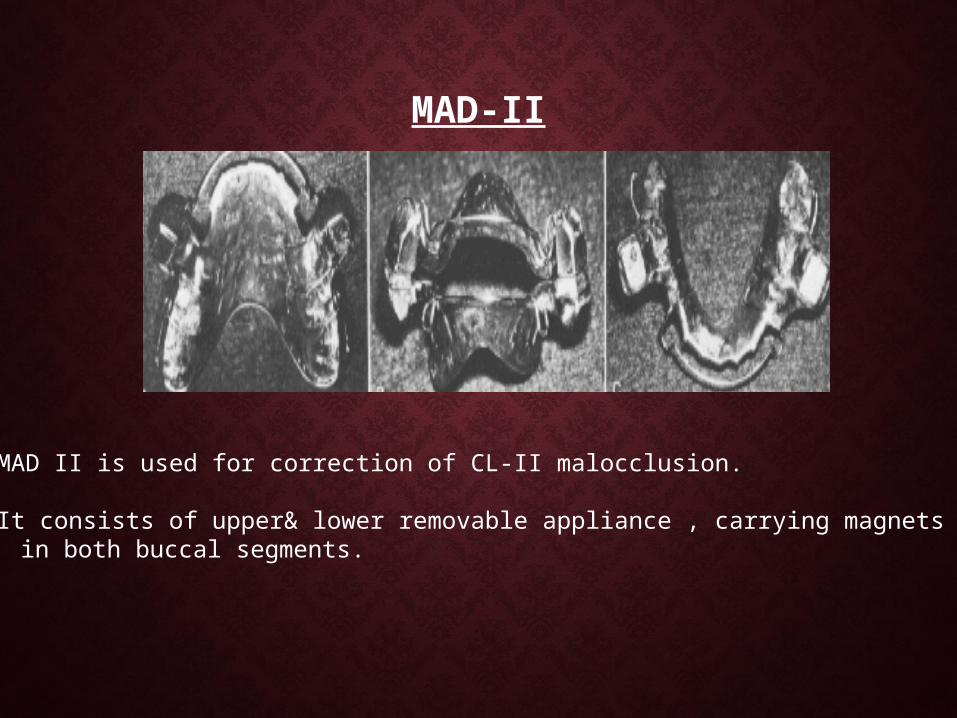
MAD-II
MAD II is used for correction of CL-II malocclusion.
It consists of upper& lower removable appliance , carrying magnets in both buccal segments.

A 30 degree inclination of the occlusal surface of the magnet to the basal surface produces an oblique force vector to correct a CL-II malocclusion.
Mechanical retention of the appliance against the magnetic forces is by clasps on the posterior teeth & in the anterior area by adding small amount of composite on the labial surface so that the labial bow rests on it.
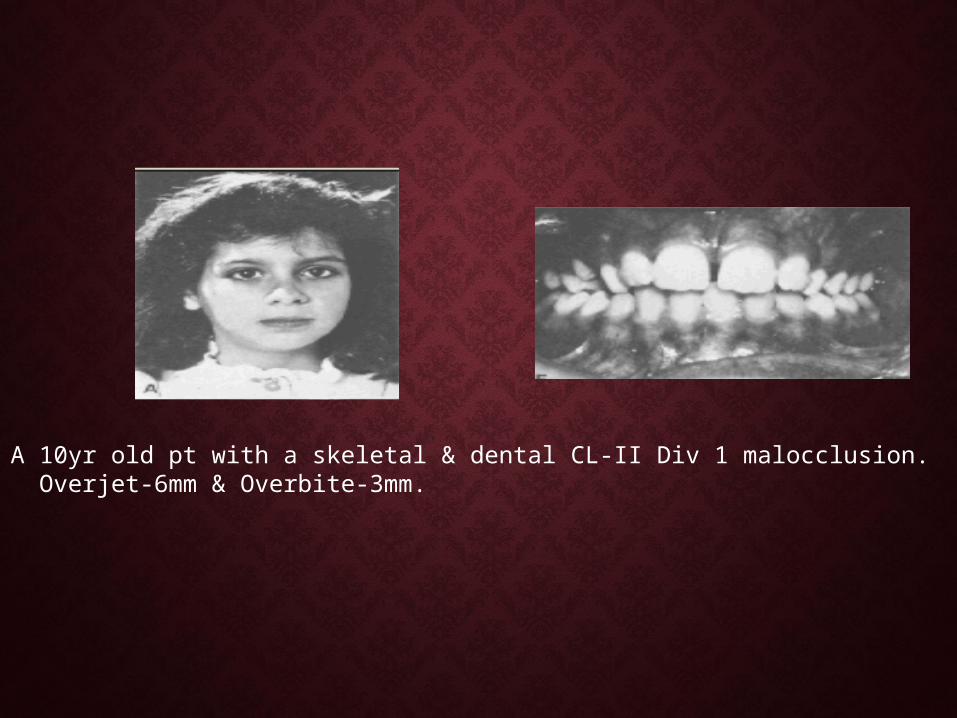
• A 10yr old pt with a skeletal & dental CL-II Div 1 malocclusion. Overjet-6mm & Overbite-3mm.

After 4 months of night time wear
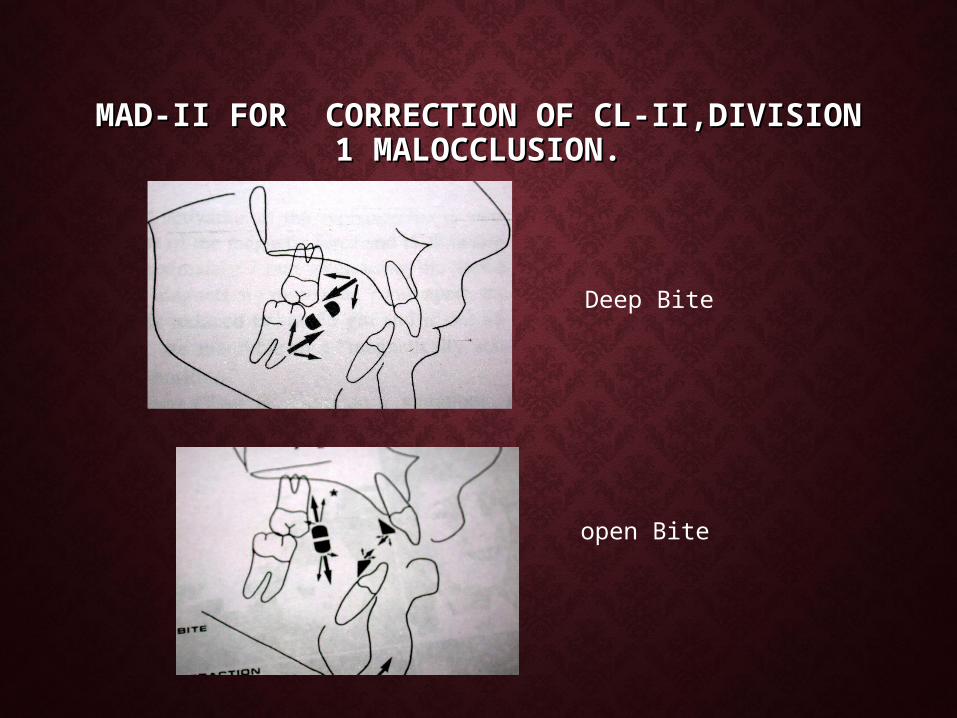
MAD-II FOR CORRECTION OF CL-II,DIVISION MAD-II FOR CORRECTION OF CL-II,DIVISION 1 MALOCCLUSION.1 MALOCCLUSION.
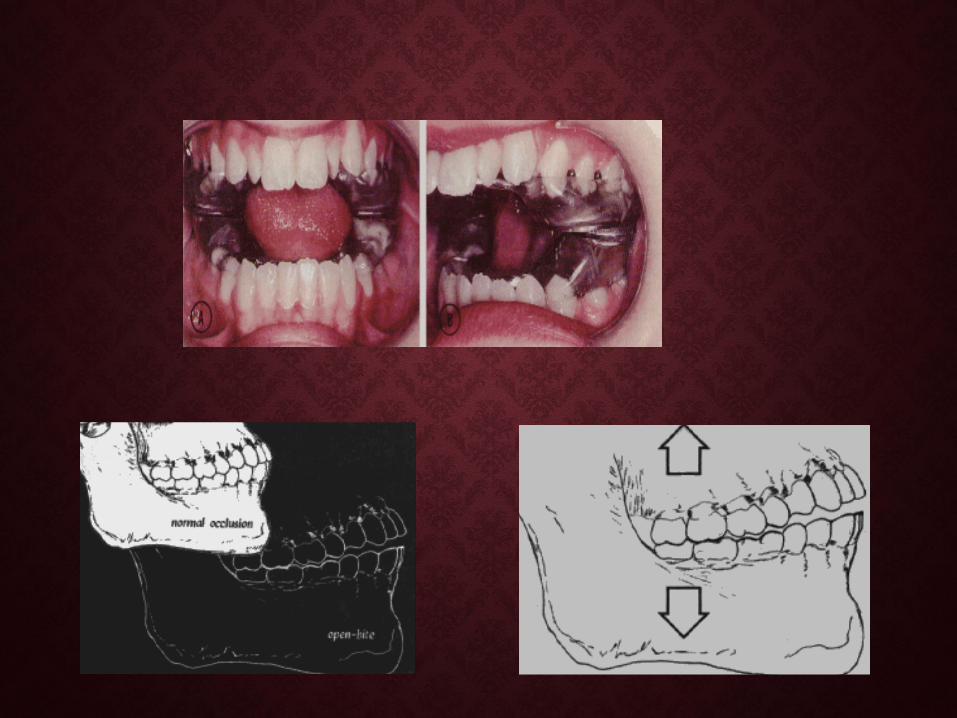
Deep Bite
open Bite
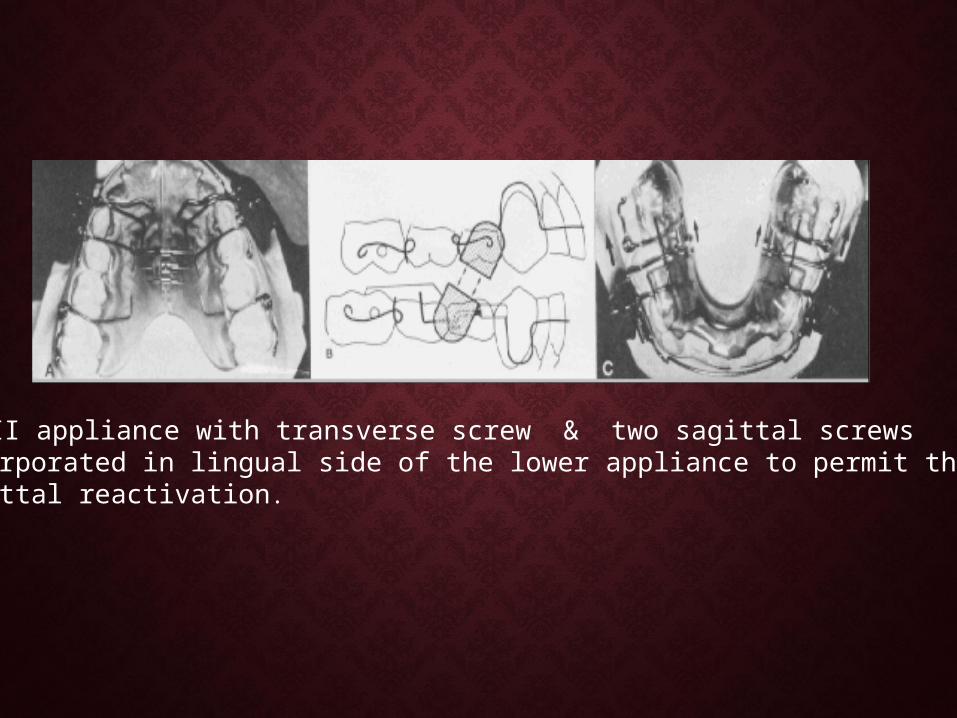
MAD II appliance with transverse screw & two sagittal screws incorporated in lingual side of the lower appliance to permit the sagittal reactivation.

EARLY CL-III TREATMENT WITH EARLY CL-III TREATMENT WITH MAGNETIC APPLIANCE.MAGNETIC APPLIANCE.
Patient before treatment.

• MAD IIIMAD IIICombined MED & MAD III appliance
Bonded upper plate ,with twomidpalatal Samarium cobalt magnets.
Removable lower plate with buccalmagnets.


Patient after 14 months of treatment.

• MAD - IVMAD - IVMagnetic activator device IV uses anterior attracting & posterior repelling magnets.

•MAD IV consists of removable upper & lower plates each of which contains three cylindrical neodymium magnets coated with stainless steel.

MAD IV(a)
MAD IV( b)
MAD IV( c)

• Tooth IntrusionTooth Intrusion:-:- Active Vertical Corrector-Active Vertical Corrector-DellingerDellinger(1986)(1986) -Samarium cobalt magnets in the repelling -Samarium cobalt magnets in the repelling
mode are used.mode are used.

Pre-Treatment Post-Treatment
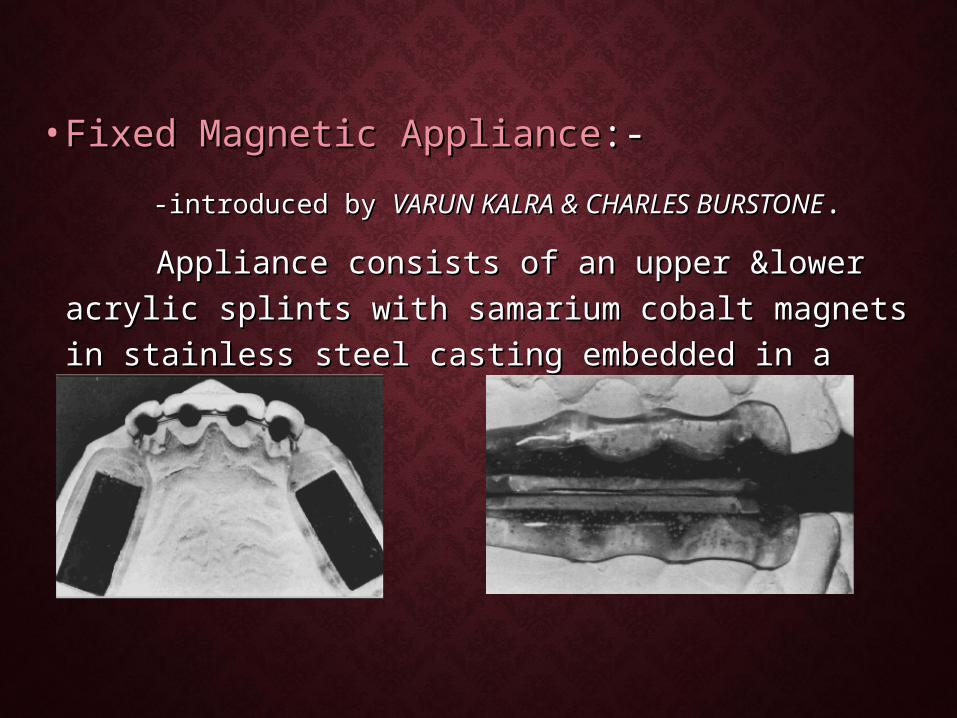
• Fixed Magnetic ApplianceFixed Magnetic Appliance:-:- -introduced by -introduced by VARUN KALRA & CHARLES BURSTONEVARUN KALRA & CHARLES BURSTONE.. Appliance consists of an upper &lower acrylic Appliance consists of an upper &lower acrylic
splints with samarium cobalt magnets in stainless splints with samarium cobalt magnets in stainless steel casting embedded in a repelling mode.steel casting embedded in a repelling mode.
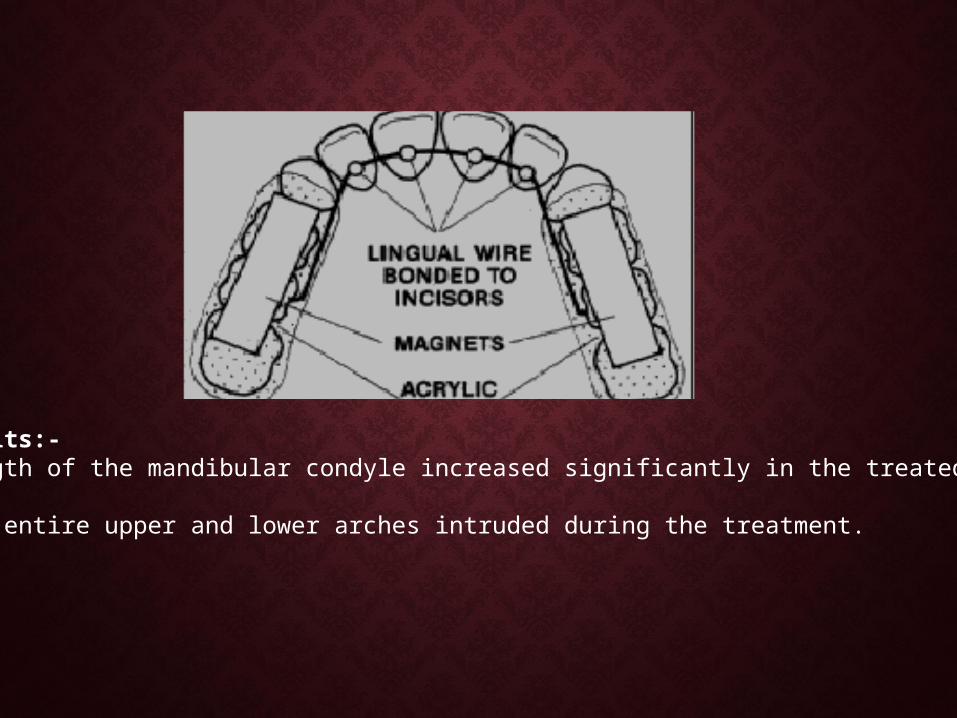
Results:--Length of the mandibular condyle increased significantly in the treated group.
-the entire upper and lower arches intruded during the treatment.
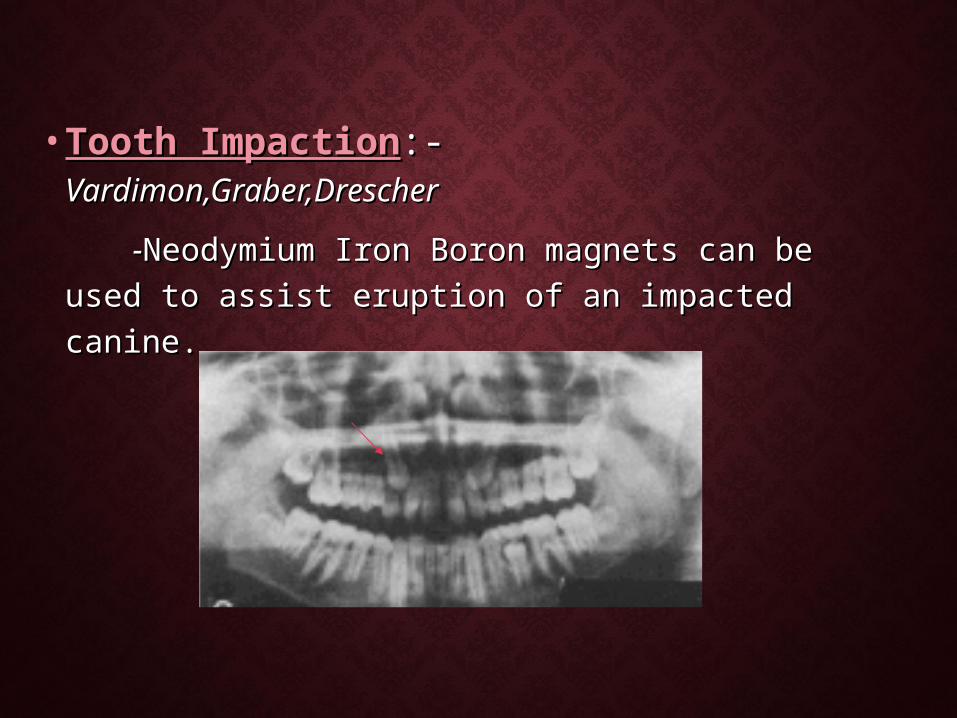
• Tooth ImpactionTooth Impaction:- :- Vardimon,Graber,Drescher Vardimon,Graber,Drescher
--Neodymium Iron Boron magnets can be Neodymium Iron Boron magnets can be used to assist eruption of an impacted canine.used to assist eruption of an impacted canine.

Vertical &Horizontal magnetic brackets were designed with the magnetic axis magnetized parallel and perpendicular to the base of the edge wise bracket.
•Vertical type –Impacted canines & incisors.•Horizontal type –Impacted premolars &molars.

Surgical procedure:-Surgical procedure:-
Palatal approach was used to expose the maxillary canine.
Vertical magnetic bracket bonded on the palatal crown surface of the impacted canine.

• A spacer of 2.5mm is positioned between the magnetic bracket & loose intraoral magnet.
•Fixation of the intraoral magnet to the Hawley type retainer with self curing acrylic followed by removal of spacer , to apply an attraction force of 0.3N.
•Treatment progression of the magnetic attractionafter 3 months.
• Fixed appliance treatment stage.

AN ATTRACTIVE SOLUTION TO AN ATTRACTIVE SOLUTION TO UNERUPTED TOOTH.UNERUPTED TOOTH.-Sandler(1991)
•Upper left canine erupting through the mucosa.
•Larger magnet repositioned to allow further movement.
•Sufficient eruption to allow attachment to beplaced.

Detailing with fixed Appliance. Post -treatment
ManciniMancini(1996)-force levels are sufficient enough to induce the (1996)-force levels are sufficient enough to induce the cellular & biochemical changes required to produce orthodontic cellular & biochemical changes required to produce orthodontic tooth movement.tooth movement.
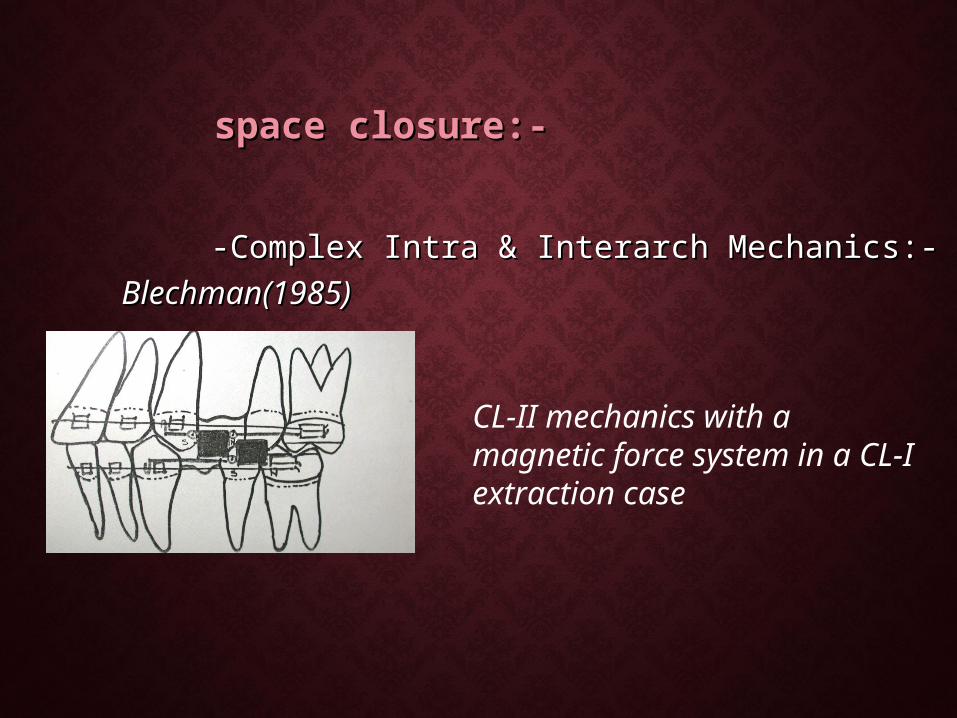
space closure:-space closure:-
-Complex Intra & Interarch Mechanics:--Complex Intra & Interarch Mechanics:-Blechman(1985)Blechman(1985)
CL-II mechanics with a magnetic force system in a CL-I extraction case
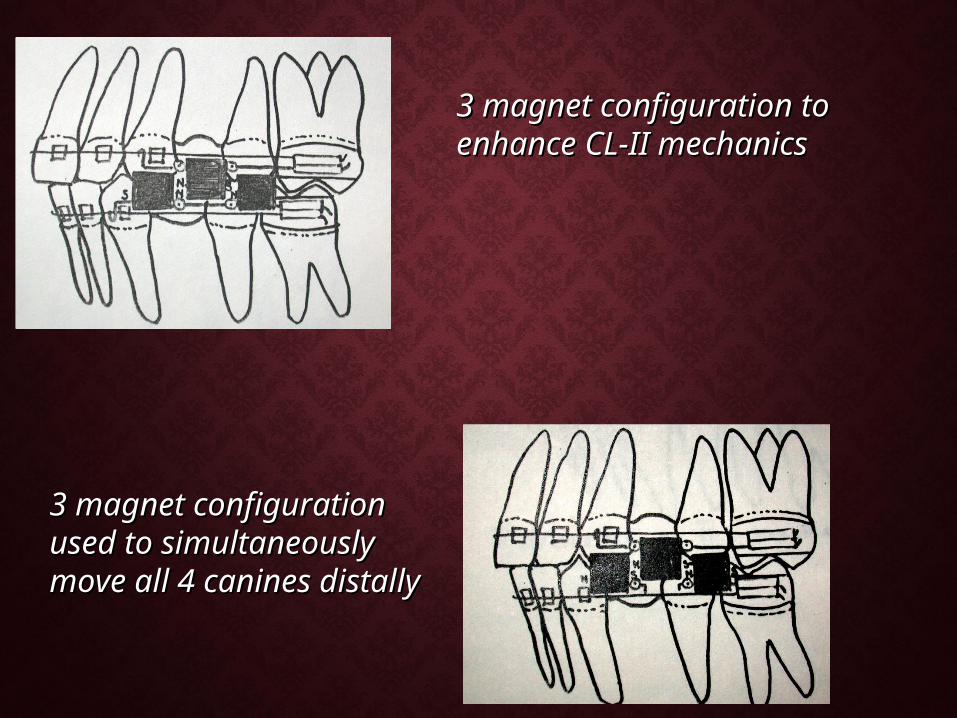
3 magnet configuration to enhance 3 magnet configuration to enhance CL-II mechanics CL-II mechanics
3 magnet configuration 3 magnet configuration used to simultaneously used to simultaneously move all 4 canines distallymove all 4 canines distally

Intramaxillary magnetic force to move Canine distally.

Pre-treatment. Upper canine retraction
Lower canine retraction Post-treatment

• Molar DistalizationMolar Distalization:-:-
--GianellyGianelly et al(1989):-repelling magnets in et al(1989):-repelling magnets in conjunction with a modified Nance appliance was conjunction with a modified Nance appliance was used.used.
Lateral view of magnets in position.

-A 11yr/F with a CL-II DIV I malocclusion in the late mixed dentition period.-Nance appliance was seated on the second deciduous molar.Results:-Molar movement in distal direction-3.2mm Deciduous molar movement in mesial direction-0.6mm

MOLAR DISTALIZATION WITH MOLAR DISTALIZATION WITH REPELLING MAGNETSREPELLING MAGNETS-Takami etal(1991)
The Molar distalization system uses two opposing magnets for each maxillary quadrant.
.• Nance appliance is placed to reinforce the anchorage.
• Constant magnetic force of 80z is applied.
• Magnets are reactivated for every 2wks

CASE FROM THE PRESENT STUDY BEFORE & CASE FROM THE PRESENT STUDY BEFORE & AFTER RAPID MOLAR DISTALIZATION.AFTER RAPID MOLAR DISTALIZATION.

REPELLING MAGNETS VS. SUPERELASTIC REPELLING MAGNETS VS. SUPERELASTIC NI-TI COILS.NI-TI COILS.
• In simultaneous distal movement of maxillary In simultaneous distal movement of maxillary first & second molarsfirst & second molars
-Mean distal movement for supercoils is -Mean distal movement for supercoils is 3.2mm.3.2mm.
-for magnets is 2.2mm.-for magnets is 2.2mm.
Bondemark & Kurol (1992).

• Magnetic Edgewise BracketsMagnetic Edgewise Brackets:-:-KawataKawata(1987)(1987) -Samarium cobalt magnet with an edgewise -Samarium cobalt magnet with an edgewise
bracket (obracket (o.018slot.018slot) .) .

Clinical application of magnetic brackets in crowded dental arch.
Cast models before & after treatment.
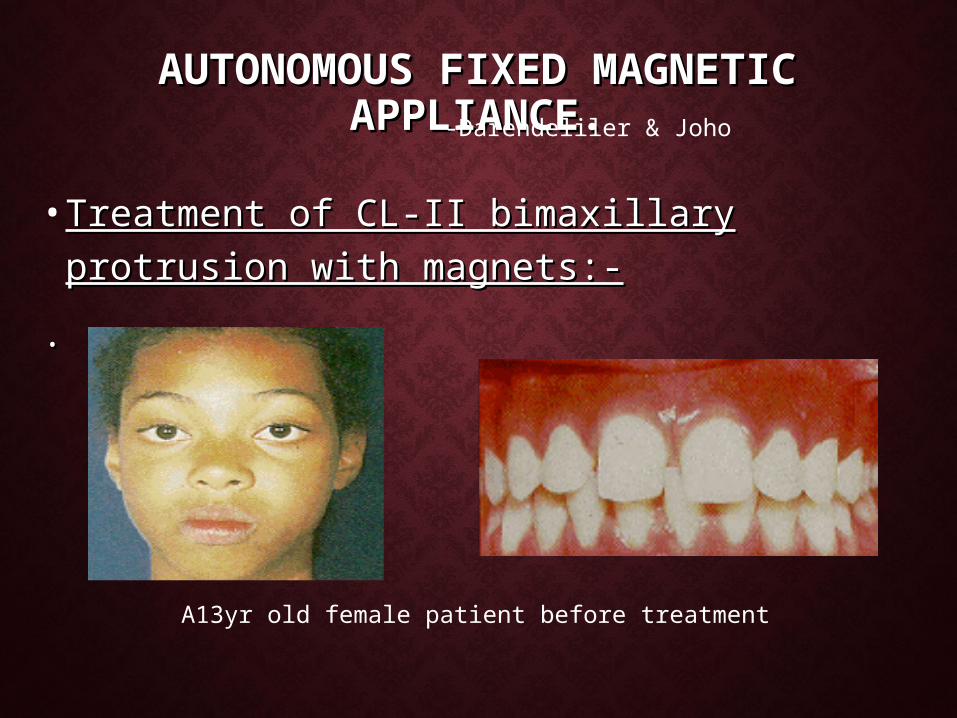
AUTONOMOUS FIXED MAGNETIC AUTONOMOUS FIXED MAGNETIC APPLIANCE.APPLIANCE.
• Treatment of CL-II bimaxillary protrusion Treatment of CL-II bimaxillary protrusion with magnets:-with magnets:-
..
-Darendeliler & Joho
A13yr old female patient before treatment

•Ideal arch form using Bonwill-Hawleys method.
•Calculation of mesial & distal magnet cuts needed to create proper arch form.
•Upper & lower magnetic arches before coating.

Lower magnets temporarily affixed to cast for Indirect bonding.

Magnetic arches in place.

Additional magnet bonded to close median diastema
Patient after 6 months of treatment with AFA

• Propellant Unilateral Magnetic AppliancePropellant Unilateral Magnetic Appliance (PUMA) (PUMA)
- Chate(1995)Chate(1995)
Magnets are use to stimulate costo-chondral bone Magnets are use to stimulate costo-chondral bone graft in Hemi facial microsomia.graft in Hemi facial microsomia.

• RetainersRetainers:-:-Springate Springate & Sandler(1991)& Sandler(1991)
-micro magnets -micro magnets made of neodymium made of neodymium iron boron magnets as iron boron magnets as a fixed retainer in a a fixed retainer in a patient with persistent patient with persistent diastema.diastema.
• BibliographyBibliography:-:- -Dentofacial Orthopedics with functional appliances-T.M Graber, -Dentofacial Orthopedics with functional appliances-T.M Graber,
Rakosi,Petrovic.Rakosi,Petrovic. -Magnetic force systems in orthodontics-Blechman AJO 78.-Magnetic force systems in orthodontics-Blechman AJO 78. -Rare earth magnets and Impaction-Vardimon AJO 91.-Rare earth magnets and Impaction-Vardimon AJO 91. -Use of magnets to move the molars distally-Gainelly AJO 89.-Use of magnets to move the molars distally-Gainelly AJO 89. -Magnetic vs Mechanical expansion with different thresholds and -Magnetic vs Mechanical expansion with different thresholds and
points of force application. Vardimon.AJO 87.points of force application. Vardimon.AJO 87. -Effects of fixed magnetic appliance on the dentofacial complex. -Effects of fixed magnetic appliance on the dentofacial complex.
Kalra.AJO 89.Kalra.AJO 89. -A new orthodontic force system of magnetic brackets. Kawata AJO -A new orthodontic force system of magnetic brackets. Kawata AJO
87.87. -An open bite correction with MAD IV. JCO 95. Darendeliler.-An open bite correction with MAD IV. JCO 95. Darendeliler.