optimal acs management with antiplatelet...
TRANSCRIPT
Sanjay Kaul, MD
Division of Cardiology
Cedars-Sinai Medical Center
Professor, Geffen School of Medicine at UCLA
Los Angeles, California, USA
Optimal ACS Management
with Antiplatelet Agents
Optimal ACS Management
with Antiplatelet Agents

The 3 Most Important Advances in
Antiplatelet Therapy for ACS
The 3 Most Important Advances in
Antiplatelet Therapy for ACS
• Aspirin
• ADP antagonists
• Platelet GP IIb/IIIa receptor antagonists

2007 ACC/AHA Guideline Recommendations Antithrombotic Therapy for Acute Coronary Syndromes
2007 ACC/AHA Guideline Recommendations Antithrombotic Therapy for Acute Coronary Syndromes
Level C(Consensus opinion,
case studies, or standard of care)
1. GPI + clopidogrel during early PCI in high-risk pts
2. GPI (eptifibatide or tirofiban) during medical Rx
1. Early invasive Rx inunstable high-risk pts
2. Fondaparinux(medical Rx)
3. Bivalirudin (early PCI)
Level B(Single randomized
trial or nonrandomized
studies
1.Fibrinolytic therapy2.GPI (abciximab) during medical Rx
1. Aspirin2. UFH or Enoxaparin3. Clopidogrel4. GPI during early PCI5. Early invasive Rx in stabilized high-risk pts
6. Statins at any LDL level
Level A(Multiple randomized
clinical trials)
IIb(Benefit ? risk)
(May be considered)
IIa(Benefit >>risk)(Reasonably
recommended)
Class III(Risk ? Benefit)
(Not recommended)
Class IIClass I(Benefit >>> risk)
(Highly recommended)
J Am Coll Cardiol 2007; DOI:10.1016/j.jacc.2007.02.028

Antiplatelet AgentsDifferent Mechanisms of Action
Antiplatelet AgentsDifferent Mechanisms of Action
Ticlopidine
Clopidogrel
Prasugrel
Cangrelor
(P2Y receptor)
Platelet Aggregation
GPIIb/IIIa
Receptor
Heparin
LMWH
Hirudin
ADP
EpinephrineCollagen
Thrombin
ArachadonicAcid
TxA2PGI2
CyclooxygenasePGG2
Aspirin
GP 2b/3a
antagonists

Effect of ASA in Non-ST Elevation MI and Unstable Angina
Effect of ASA in Non-ST Elevation MI and Unstable Angina Incidence of Death or Subsequent MI
% of Patients
0
4
8
12
Lewis
P=0.0005
10.110.1 5550%
RRR
0
5
10
15
Cairns
P=0.012
12.912.9 6.26.252%
RRR
0
5
10
15
Theroux
P=0.008
11.911.9 3.33.372%
RRR
0
4
8
12
RISC
P<0.0001
17.117.1 6.56.562%
RRR
N = 155 178 279 276 118 121 397 399
Time 3m 24m 3-9d 3m
Dose 324mg 1300mg 650mg 75mg
Placebo ASA

Limitations of AspirinLimitations of Aspirin
Multiple pathways of platelet activation in vivoThrombin, collagen, high shear stress activate
platelets via non-cyclooxygenase pathways
Catecholamines can overcome antiplatelet effect
Platelet adhesion and thrombus formation notblocked
Prothrombotic effect at higher dosesInhibition of vascular prostacyclin generation
Inhibition of tPA (at doses >300 mg)

New ACC/AHA Guidelines for Management
of Unstable Angina/NSTEMI (2007)
New ACC/AHA Guidelines for Management
of Unstable Angina/NSTEMI (2007)
• Early invasive strategy for high-risk patients (Class I, Level B)
• Add clopidogrel to aspirin and heparin (Class I, Level A)
• Add GP 2b/3a inhibitor (Class I, Level A) to clopidogrel (Class IIa, Level B) prior to angiography
• Add UFH or Enoxaparin (Class I, Level A) or bivalirudin or fondaparinux (Class I, Level B) to antiplatelet therapy with ASA and clopidogrel
• Statin Rx regardless of LDL-C (Class I, Level A)
ACC/AHA Guidelines. August 14, 2007
J Am Coll Cardiol. 2007;50:652-726

3 months ≤≤≤≤ double-blind treatment ≤≤≤≤ 12 months
Aspirin 75-325mg
Clopidogrel(6,259 patients)
Placebo(6,303 patients)
Aspirin 75-325mg
Day 1
6 m. Visit
9 m. Visit
12 m.
or Final Visit
Clopidogrel 300mg loading +75mg qd dose
3 m. Visit
Discharge Visit
1 m. Visit
Patients withAcute Coronary
Syndrome
(UA or MI Without STelevation)
R
Placebo loading dose
R=Randomization
The CURE Trial InvestigatorsThe CURE Trial InvestigatorsThe CURE Trial InvestigatorsThe CURE Trial Investigators. . N Engl J Med.N Engl J Med. 2001;345:4942001;345:494--502.502.
CURE ProtocolCURE Protocol

CURE: ResultsPrimary End-Point
CURE: ResultsPrimary End-Point
581
723
0
200
400
600
800
1000
Number of events RRR = 20%; p=0.00005
CV Death, MI, Stroke
9.28% 11.47%
Clopidogrel + ASA
(n=6259)
Aspirin
(n=6303)
ARR = 2.19
NNT = 46
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.

CURETreatment Effect by Individual Endpoint
CURETreatment Effect by Individual Endpoint
317 340
0
250
500
CV Death
p=ns
5.06
%
5.4%
8
%
RRR
Clopidogrel + ASA
(n=6259)Aspirin
(n=6303)
ARR = 0.34%
NNT = 294
MI
325
421
0
250
500P<0.001
5.19
%
6.68
%
23
%
RRR
ARR = 1.49%
NNT = 67
75
88
0
75
150
Stroke
p=ns
1.4
%
1.2
%
15
%
RRR
ARR = 0.2%
NNT = 500
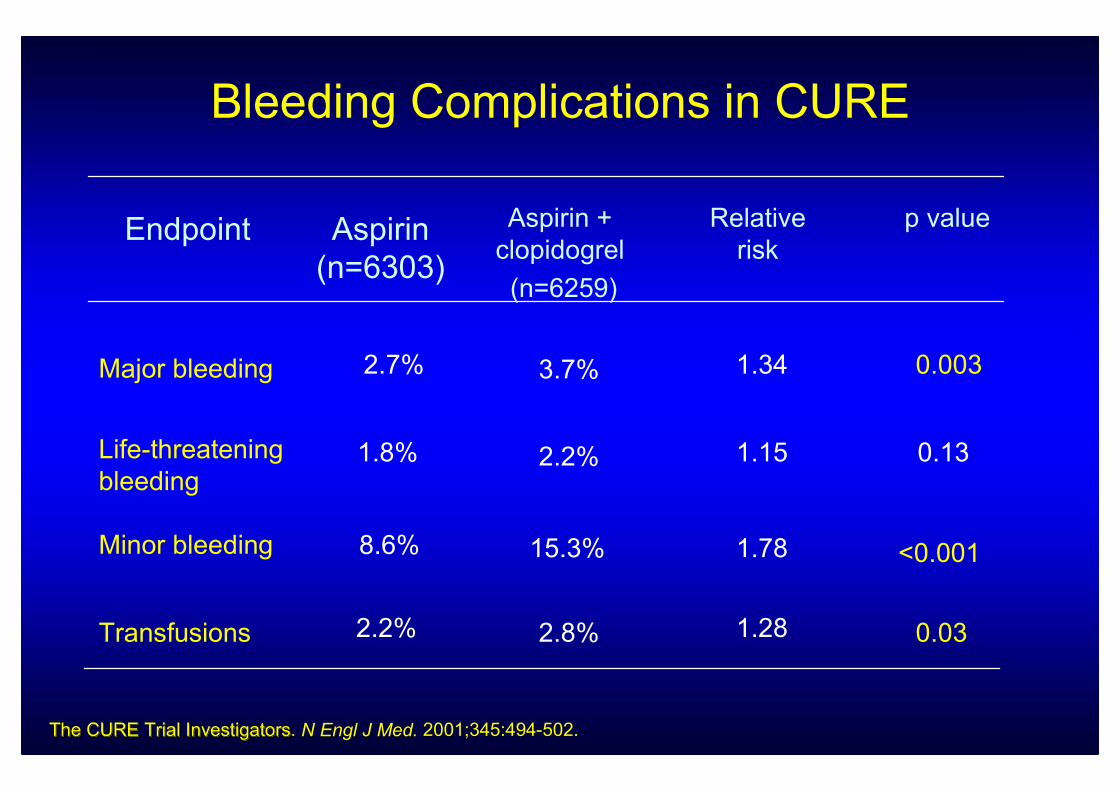
Bleeding Complications in CURE
p valueRelative
riskAspirin
(n=6303)
Endpoint
0.13
8.6%Minor bleeding
2.2%
Major bleeding
Transfusions
Aspirin +
clopidogrel
(n=6259)
2.8%
<0.001
Life-threatening
bleeding
2.2%
1.8%
2.7% 3.7%
15.3%
1.34
1.15
1.78
1.28
0.003
0.03
The CURE Trial InvestigatorsThe CURE Trial InvestigatorsThe CURE Trial InvestigatorsThe CURE Trial Investigators. . N Engl J Med.N Engl J Med. 2001;345:4942001;345:494--502.502.

5.7
11.4
20.7
4.1
9.8
15.9
0
5
10
15
20
25
CURE Trial: Who Are Most Likely to Benefit?Clopidogrel+ASA vs ASA Stratified by TIMI-Risk Score
CURE Trial: Who Are Most Likely to Benefit?Clopidogrel+ASA vs ASA Stratified by TIMI-Risk Score
ASA (n=6303)
Clopidogrel + ASA (n=6259)
No. of pts. 26% 58% 16%
ARD 1.6 1.6 4.8
NNT 63 63 21
Rate of Composite
Endpoints (CVD/MI/stroke)
(%)
Budaj A et al, Circulation.2002;106:1622-1626
Risk Profile Low Intermediate High
P<0.04
P<0.03
P<0.004

Key Issues Regarding Clopidogrel UseKey Issues Regarding Clopidogrel Use
• How long to give it for optimum benefit?
• Is it necessary to pre-treat?
• When to stop prior to CABG?
• Should it be used with GP 2b/3a antagonists?
• What about clopidogrel resistance?

Role of ADP Antagonists in AtherothrombosisKey Issues Regarding Clopidogrel Use in Clinical Practice
Role of ADP Antagonists in AtherothrombosisKey Issues Regarding Clopidogrel Use in Clinical Practice
Duration of treatment
• Stable CVD: No long-term benefit in patients with stable CVD or CV risk factors
• UA/NSTEMI: < 1 month (IA), < 12 months (IB) in high-risk pts at low-risk for bleeding
• STEMI: At least 1 month with fibrinolytic Rx; no direct studies with primary PCI
• PCI: At least 1 month (IA) and up to 12m (IB) with BMS; at least 12m (IB) with DES
• Stroke: Not recommended as first-line Rx unless a clear indication is also present

Management of Atherothrombosis with Clopidogrel in
High Risk Patients with Recent TIA or Ischemic Stroke
MATCH Trial (N=7,599)MI, ischemic stroke, vascular death, or rehospitalization
for an acute ischemic event at 18 months
Management of Atherothrombosis with Clopidogrel in
High Risk Patients with Recent TIA or Ischemic Stroke
MATCH Trial (N=7,599)MI, ischemic stroke, vascular death, or rehospitalization
for an acute ischemic event at 18 months
15.716.73
0
5
10
15
20
25
Clop + ASA Clop
Number of People
(%)
2.54
1.3
0
2
4
6
8
Clop + ASA Clop
596 636 96 49
(N=3797) (N=3802)
OR 0.93
95%CI 0.82, 1.05
(N=3759) (N=3781)
Ischemic Events Life Threatening Hemorrhage
OR 2.0
95%CI 1.41, 2.82
Diener HC et al, Lancet 2004;364:331-337.

Antiplatelet Therapy Following StentingAHA/ACC/SCAI/ACS/ADA Science Advisory 2007
Antiplatelet Therapy Following StentingAHA/ACC/SCAI/ACS/ADA Science Advisory 2007

100%31%4yAngiogram
plus clinical
DESMauri, 2007
(N=4545)
NA31%6 mAngiogramDESKuchulakanti, 2006
(N=2974)
100%25%1 mAngiogram
plus clinical
DESOng, 2005
(N=2016)
93%45%9 mAngiogram
or clinical
DESIakovou, 2005
(N=2229)
100%17%9mAngiogram plus
acute MI
BMSHeller, 2001
(N=1855)
70%21%6 mAngiogram or
clinical
BMSCutlip, 2001
(N=6186)
Death
or MI
DeathDurationConfirmation
of stent
thrombosis
Stent
type
Study
Clinical Importance of Stent Thrombosis“Real-World” and RCT Experience
Clinical Importance of Stent Thrombosis“Real-World” and RCT Experience
Cutlip D, et al. Circulation 2001;103:1967; Iakovou I, et al. JAMA 2005;293:2196Kuchulakanti PK et al. Circulation. 2006;113:1108-1113; Ong, et al. JACC 2005:45;2088-2092; Mauri L et al. NEJM 2007;356:1020-9

Longer period of anti-platelet therapy is needed after DES
0
25
50
75
100
0
25
50
75
100
Incomplete coverage Complete coverage
Grade 0 Grade 1 Grade 2 Grade 3
Percent
Percent
Sirolimus-eluting stent
Bare metal stent
Angioscopy at 8 months post SES implantation
Kotani J et al. JACC. 2006,47:2108
Virmani autopsy dataPercentage
Endothelialization
Duration in months
1 2 3 4 5 6 7 8 9 11 15 16 17 20>40
0
10
20
30
40
50
60
70
80
90
100
BMS
DES
Joner M et al. JACC. 2006;48:193.
Incomplete Strut Endothelialization With DES?Incomplete Strut Endothelialization With DES?

Eisenstein E et al. JAMA. 2007;297:159-168

Eisenstein E et al. JAMA. 2007;297:159-168
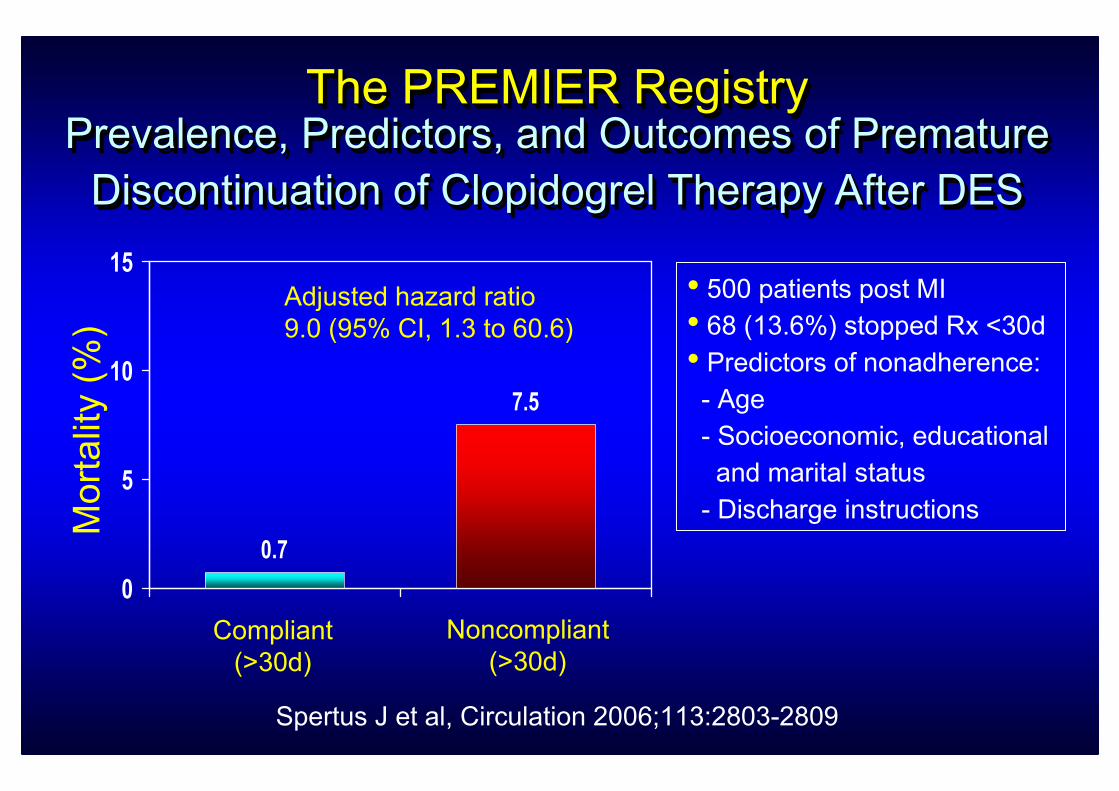
The PREMIER Registry Prevalence, Predictors, and Outcomes of Premature
Discontinuation of Clopidogrel Therapy After DES
The PREMIER Registry The PREMIER Registry Prevalence, Predictors, and Outcomes of PrematurePrevalence, Predictors, and Outcomes of Premature
Discontinuation of Clopidogrel Therapy After DESDiscontinuation of Clopidogrel Therapy After DES
Spertus J et al, Circulation 2006;113:2803-2809
• 500 patients post MI• 68 (13.6%) stopped Rx <30d• Predictors of nonadherence:- Age
- Socioeconomic, educational
and marital status
- Discharge instructionsMortality (%)
Compliant
(>30d)
Noncompliant
(>30d)
0.7
7.5
0
5
10
15
Adjusted hazard ratio
9.0 (95% CI, 1.3 to 60.6)

Long-Term Clopidogrel Plus Aspirin Treatment
Results of The CHARISMA Trial (28m)
LongLong--Term Clopidogrel Plus Aspirin Treatment Term Clopidogrel Plus Aspirin Treatment
Results of The CHARISMA Trial (28m)Results of The CHARISMA Trial (28m)
(%)
ASA+Clop
N=7802
ASA
N=7801
6.807.30
0.00
5.00
10.00OR = 0.93 (0.83-1.05)
CV death, MI or stroke
Bhatt DL et al, NEJM 2006
(%)
ASA+Clop
N=7802
ASA
N=7801
2.10
1.30
0.00
1.00
2.00
3.00
Major bleeding (TIMI)
OR = 1.64 (1.27-2.10)
Fatal bleeding
0.3%

Timing of Surgery/Invasive Procedures Post-DES
Special Considerations
Timing of Surgery/Invasive Procedures Post-DES
Special Considerations
• Elective procedures: Postpone• Emergencies/urgencies
- Do not hold aspirin and
clopidogrel unless bleeding
risk is prohibitive
- Cardiology consultation for
“bridging” therapy
- “Code white” for peri-op
CP or ECG changes
(stent thrombosis)
0 1 y ? 2-3 y
• Elective procedures - May be safe
- Do not hold aspirin
unless bleeding risk
outweighs stent thrombosis
risk
• Emergencies/urgencies- Do not hold aspirin unless
prohibitive bleeding risk

“Bridging” Therapy Post-DES(Multidisciplinary Approach)
“Bridging” Therapy Post-DES(Multidisciplinary Approach)
• Formal pre-op evaluation 1 wk prior• Communication between surgeon, anesthesiologist & cardiologist is key
• Hold clopidogrel 5-7d prior• Do not hold aspirin unless prohibitive bleeding risk (increase to 325mg)
• Admit in-patient 3-4 days prior• Initiate IV short-acting GP 2b/3a (eptifibatide or tirofiban) without
loading dose
• Monitor CBC daily for plt count• Stop GP 2b/3a 10-12h prior to procedure (5-6 half-lives)
• Check plt count &/or function 2h prior• Restart clopidogrel (300-600 mg loading dose) >24h post-op
Do’s
• Don’t use abciximab (long half-life)• Heparin, including LMWH, unlikely to be effective
• Antiplatelet agents such as dipyrimadole or aggrenox should
be avoided
• Platelet transfusions not helpful
Dont’s
• Platelet function assay• Random donor plts (apharesis)• Investigational ADP antagonist, IV cangrelor (phase III trials)
Don’t know’s

Key Issues Regarding Clopidogrel UseKey Issues Regarding Clopidogrel Use
• How long to give it for optimum benefit?
• Is it necessary to pre-treat?
• When to stop prior to CABG?
• Should it be used with GP 2b/3a antagonists?
• What about clopidogrel resistance?

Clopidogrel Pre-treatmentFact or Fashion
Clopidogrel Pre-treatmentFact or Fashion
No definite benefit with pretreatment, but a potential risk for
increased bleeding associated with PCI and CABG
TrialPre-Rx
duration Clopidogrel Control Risk ratio
PCI-CURE
(300 mg)59/1313 86/1345 0.70 (0.51 to 0.97)
PCI-CLARITY
(300 mg)
70/933 112/930 0.62 (0.47 to 0.83)
CREDO
(300 mg)
61/900 76/915 0.82 (0.59 to 1.13)
PRAGUE-8*(600 mg)
4/513 4/515 1.00 (0.25 to 4.00)
0 0.5 1 1.5 2
3-120d (10d)
48-192h
3-24h
>6h
Indication
UA/NSTEMI
STEMI
Non-urgent
PCI
Elective
angiography
Endpoint
D, MI, TVR
(30d)
D, MI, CVA
(30d)
D, MI, TVR
(28d)
D, MI, TVR,
CVA (7d)
*Increased bleeding
3.5 vs 1.2% (P=0.02) angio
7.2 vs 0.7% (P=0.006) PCI
Risk ratio

Optimal Timing of Clopidogrel Pre-Treatment
(300mg): CREDO Post hoc Analysis
Results at 28 days
Optimal Timing of Clopidogrel Pre-Treatment
(300mg): CREDO Post hoc Analysis
Results at 28 days
Steinhubl, S. R. et al. J Am Coll Cardiol 2006;47:939-943
Pretreatment with 300mg loading for at least 15h and ideally 24h

Kandzari D. et al. J Am Coll Cardiol, 2004; 44:2133-2136
2-3h
N=367
>12h
N=746
4.4%
3.5%
D, MI or uTVR
2-3h
N=367
12h
N=746
4.1%3.4%
MI
2-3h
N=36712h
N=746
1.6%1.2%
Major bleeding
16 26 15 256 9
OR = 0.82 (0.44-1.54) OR = 0.74 (0.26-2.06)OR = 0.80 (0.43-1.47)
No time-dependence with 600mg loading dose + GP2b/3a
Optimal Timing of Clopidogrel Pre-Treatment
(600mg): ISAR-REACT Post hoc Analysis
Results at 30 days
Optimal Timing of Clopidogrel Pre-Treatment
(600mg): ISAR-REACT Post hoc Analysis
Results at 30 days

Role of ADP Antagonists in AtherothrombosisKey Issues Regarding Clopidogrel Use in Clinical Practice
Role of ADP Antagonists in AtherothrombosisKey Issues Regarding Clopidogrel Use in Clinical Practice
Pre-treatment ?
• Favorable data in retrospective analysis (EPISTENT, ESPRIT, TARGET)
• Pretreatment hypothesis not validated in the only prospective assessment (CREDO)
• Guideline recommendations:
- ESC: 600 mg loading 2-6h pre-PCI (IC)
- ACC/AHA: 300 mg loading dose 6h pre-PCI without (IA) or with (IIa, B) GP IIb/IIIa in ACS
- ACCP: 300 mg loading dose 6h pre-PCI without (IA)
• Prudent to rule out surgical CAD before pretreatment to avoid bleeding risk
• A properly designed clinical trial is warranted to provide unequivocal support

Key Issues Regarding Clopidogrel UseKey Issues Regarding Clopidogrel Use
• How long to give it for optimum benefit?
• Is it necessary to pre-treat?
• When to stop prior to CABG?
• Should it be used with GP 2b/3a antagonists?
• What about clopidogrel resistance?

0
5
10
Number of events
(%)
4.4% 9.6%
>5 days
(n=456)
<5 days
(n=436)
ARI = 5.2%
NNH = 18
P=0.003
The CURE Trial InvestigatorsThe CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
Key Issues Regarding Clopidogrel Use in ACSWhen Should Clopidogrel be Stopped Prior to CABG?
Key Issues Regarding Clopidogrel Use in ACSWhen Should Clopidogrel be Stopped Prior to CABG?
Major Bleeding
N=20
N=42
At least 5 days and preferably 7 days (I, B)

Key Issues Regarding Clopidogrel UseKey Issues Regarding Clopidogrel Use
• How long to give it for optimum benefit?
• Is it necessary to pre-treat?
• When to stop prior to CABG?
• Should it be used with GP 2b/3a antagonists?
• What about clopidogrel resistance?

ISAR-REACT 2 Trial: Study DesignISAR-REACT 2 Trial: Study Design
• Primary Endpoint: Composite of death, MI, and urgent target vessel
revascularization (TVR) due to myocardial ischemia within 30 days
• Secondary Endpoint: In-hospital major and minor bleeding
2022 patients with an episode of angina within the preceding 48 hours and an elevated
troponin T level or new ST-segment depression of ≥≥≥≥0.1 mV or transient (<20 minutes)
ST-segment elevation of ≥≥≥≥0.1 mV or new or presumed new bundle-branch block;
significant angiographic lesions in a native coronary vessel or venous bypass graft
amenable to and requiring a PCI Placebo Controlled. Randomized. Blinded.
24% female, mean age 66 years, mean follow-up 30 days
Abciximab
(usual bolus or infusion dose)
n=1012
Placebo
n=1010
Pre-treatment with high dose (600mg) clopidogrel at least 2 hours pre-procedure
Kastrati, A. et al. JAMA 2006;295:1531-1538

ISAR-REACT 2Results at 30 days
ISAR-REACT 2Results at 30 days
Kastrati, A. et al. JAMA 2006;295:1531-1538
Placebo
N=1,010
Abciximab
N=1,012
11.9%
8.9%
D, MI or uTVR
Placebo
N=1,010
Abciximab
N=1,012
11.5%
8.6%
Death or MI
Placebo
N=1,010Abciximab
N=1,012
1.4% 1.4%
Major bleeeding
0.75 (0.58-0.97)
120 90
0.75 (0.57-0.97) 1.00 (0.50-2.08)
116 8714 14

ISAR-REACT 2Results Stratified by Baseline Troponin
ISAR-REACT 2Results Stratified by Baseline Troponin
Kastrati, A. et al. JAMA 2006;295:1531-1538
Placebo
N=536
Abciximab
N=513
18.3%
13.1%
30 day
D, MI or uTVR
Placebo
N=474
Abciximab
N=499
4.6% 4.6%
Troponin <0.03µg/L
0.71 (0.54-0.95)
98 67
0.99 (0.56-1.76)
22 23
Troponin >0.03µg/L

Impact of Triple Antiplatelet Rx in Non-urgent PCI(ASA, Clopidogrel, Abciximab)
Death, MI or Urgent TVR at 30 days
Impact of Triple Antiplatelet Rx in Non-urgent PCI(ASA, Clopidogrel, Abciximab)
Death, MI or Urgent TVR at 30 days
Abciximab Control Risk ratio
(95% CI)Trial
ISAR REACT 45/1079 43/1080 1.05 (0.7 to 1.58)
ISAR REACT-2* 22/474 23/499 1.01 (0.57 to 1.78)
ISAR SWEET 20/351 15/350 1.33 (0.69 to 2.55)
ISAR SMART-2 13/251 8/251 1.63 (0.69 to 3.85)
Combined 100/2155 89/2180 1.14 (0.86 to 1.50)0 1 2 3 4
* Troponin negative pts Abciximab
betterAbciximab
worse
Adjunctive therapy with GP 2b/3a not effective and safe in stable pts

Key Issues Regarding Clopidogrel UseKey Issues Regarding Clopidogrel Use
• How long to give it for optimum benefit?
• Is it necessary to pre-treat?
• When to stop prior to CABG?
• Should it be used with GP 2b/3a antagonists?
• What about clopidogrel resistance?

Adapted from Angiolillo DJ et al. Am J Cardiol. 2006;97:38-43.
Individual Response Variability to Dual Antiplatelet Rx in the Steady State PhaseIndividual Response Variability to Dual Antiplatelet Rx in the Steady State Phase
% Platelet Aggregation (LTA-ADP 20µmol/L)
97.5
92.5
87.5
82.5
77.5
72.5
67.5
62.5
57.5
52.5
47.5
42.5
37.5
32.5
27.5
22.5
17.5
12.5
7.5
2.5
20
15
10
5
0
Numberof Patients Bleeding risk Ischemic risk
~ 5-30% incidence of ‘hyporesponsiveness’ to clopidogrel

Cellular FactorsCellular Factors• Accelerated platelet turnoverAccelerated platelet turnover
•• Reduced CYP3A metabolic activityReduced CYP3A metabolic activity
•• Increased ADP exposure Increased ADP exposure
•• UpUp--regulation of the P2Yregulation of the P2Y1212 pathwaypathway
•• UpUp--regulation of the P2Yregulation of the P2Y11 pathway pathway
•• UpUp--regulation of P2Yregulation of P2Y––independent independent
pathwayspathways
(collagen, epinephrine, TXA(collagen, epinephrine, TXA22, thrombin), thrombin)
Clinical FactorsClinical Factors• Failure to prescribe/poor complianceFailure to prescribe/poor compliance
•• UnderUnder--dosing dosing
•• Poor absorptionPoor absorption
•• DrugDrug--drug interactions involving CYP3A4drug interactions involving CYP3A4
•• Acute coronary syndromeAcute coronary syndrome
•• Diabetes mellitus/insulin resistanceDiabetes mellitus/insulin resistance
•• Elevated body mass indexElevated body mass index
Genetic FactorsGenetic Factors• Polymorphisms of CYPPolymorphisms of CYP
•• Polymorphisms of Polymorphisms of GPIaGPIa
•• Polymorphisms of P2YPolymorphisms of P2Y1212
•• Polymorphisms of Polymorphisms of GPIIIaGPIIIa
Clopidogrel Response Variability
Angiolillo DJ et al. J Am Coll Cardiol. 2007; 49: 1505-1516 .

Clinical RelevanceFunctional ParameterN
Post-PCI ischemic events
(30 days)↑↑↑↑ platelet aggregation292Cuisset et al.
JACC 2006
Post-PCI ischemic events
(30 days)
Post-PCI ischemic events
(3 months)
Post-PCI ischemic events
(12 months)
↑↑↑↑ platelet aggregation (3rd & 4th quartiles)
↓↓↓↓ platelet inhibition
↑↑↑↑ platelet aggregation
802
379
100
Hocholzer et al.
JACC 2006
Geisler et al.
Eur Heart J 2006
Bliden et al.
JACC 2007
Post PCI-myonecrosis↑↑↑↑ clopidogrel/aspirin-resistant patients120Lev et al.
JACC 2006
Post-PCI ischemic events
(30 days)↑↑↑↑ platelet aggregation106Cuisset et al.
J Thromb Haemost 2006
Myonecrosis and inflammation marker release
↑↑↑↑ periprocedrual platelet aggregation 120Gurbel et al.
Circulation 2005
Post-PCI ischemic events
(6 months) ↑↑↑↑ periprocedrual platelet aggregation 192Gurbel et al.
JACC 2005
Post-primary PCI ischemic events (6 months)
↑↑↑↑ platelet aggregation (4th quartile)60Matezky et al.
Circulation 2004
Angiolillo DJ et al. Am J Cardiol Drugs. 2007.
Post-Stent Ischemic Events and Periprocedural Infarction
Clinical Relevance of Clopidogrel Non-responsiveness
Clinical Relevance of Clopidogrel Non-responsiveness

Inhibition of ADP-induced
Aggregation @ 6 days (%)
Ist Qrt
(n=15)
• 60 patients with STEMI undergoing primary PCI <6h• Aspirin, heparin, eptifibatide during PCI• Clopidogrel 300 mg load post-PCI, 75 mg daily x3 months
Matetzky S et al, Circulation. 2004;109:3171-3175
Clopidogrel ResistanceClopidogrel Resistance
40
0.7
0
0
0 10 20 30 40 50
-9
-22
-28
-45
-50 -40 -30 -20 -10 0
Recurrent CVS Events
@ 6 months (%)
2nd Qrt
(n=15)
3rd Qrt
(n=15)
4th Qrt
(n=15)
P<0.01 P<0.007
Total # of events = 8
(7/15)
(1/15)

Role of ADP Antagonists in AtherothrombosisKey Issues Regarding Clopidogrel Use in Clinical Practice
Role of ADP Antagonists in AtherothrombosisKey Issues Regarding Clopidogrel Use in Clinical Practice
Clopidogrel resistance
• Unclear entity with unclear definition (variable “responsiveness” or true “resistance”)
• Unclear diagnosis (? optimum test)
• Unclear mechanism
• Unclear clinical relevance (? prediction of clinical outcomes; ? titration of drug Rx)
• Not recommended by ISTH, ACCP, ESC
• A thorough assessment of the phenomenon is indicated

≈≈≈≈ 95%
(few minutes)
≈≈≈≈ 95%
(2-4 hours)
≈≈≈≈ 70%
(<1 hour)
Mean
Platelet
Inhibition
(Time
Required)
CHAMPION
PLATO
TRITON
Trials
(Phase III)DoseActionRouteTypeDrug
4 µg/kg/minCompetitive
bindingParenteral
ATP analogue –
Direct inhibition
Cangrelor
(ARC-669931MX)
90 mg bidCompetitive
bindingOral
Cyclopetyl-
triazolopy-
rimidine –
Direct inhibitionAZD6140
60 mg
loading
dose, 10 mg
maintenance
dose
Irreversible
bindingOral
Thienopyridine
(3rd gen) –
requires hepatic
conversion to
active
metabolite
Prasugrel
(CS-747)
Novel P2Y12 ADP Receptor AntagonistNovel P2Y12 ADP Receptor Antagonist
More potent and less variability!!More potent and less variability!!Angiolillo DJ et al. J Am Coll Cardiol. 2007; 49: 1505-1516 .

New ACC/AHA Guidelines for Management
of Unstable Angina/NSTEMI
New ACC/AHA Guidelines for Management
of Unstable Angina/NSTEMI
• Early invasive strategy for high-risk patients (Class I, Level B)
• Add clopidogrel to aspirin and heparin (Class I, Level A)
• Add GP 2b/3a inhibitor (Class I, Level A) to clopidogrel (Class IIa, Level B) prior to angiography
• Add UFH or Enoxaparin (Class I, Level A) or bivalirudin or fondaparinux (Class I, Level B) to antiplatelet therapy with ASA and clopidogrel
• Statin Rx regardless of LDL-C (Class I, Level A)
ACC/AHA Guidelines. August 14, 2007
J Am Coll Cardiol. 2007;50:652-726

Boersma et al, Lancet 2002;359:189-1198.
GUSTO IV
PRISM
PRISM-Plus
PURSUIT
PARAGON A
PARAGON B
POOLED
Trial (IIb/IIIa) Placebo 2b/3a
7800
3232
1570
9461
1513
5169
28,745
N
8.0
7.0
11.9
15.7
11.7
11.4
12.5
8.7
5.7
8.7
14.2
10.3
10.5
11.3
Better Worse0.1 1 10
Death / MI at 30 days
Risk Ratio & 95% CI (%) (%)
0.91 (0.86, 0.99)
P=0.015
P=0.339
Breslow-Day
Homogeneity
ARR = 1.2%
RRR = 9%
Clinical Importance vs Statistical SignificanceImpact of GP IIb/IIIa Inhibitor on Death or MI
Clinical Importance vs Statistical SignificanceImpact of GP IIb/IIIa Inhibitor on Death or MI

GP 2b/3a Inhibitors in ACS (N=31,402)30-Day Death/MI and Bleeding Complications
GP 2b/3a Inhibitors in ACS (N=31,402)30-Day Death/MI and Bleeding Complications
11.810.8
0
5
10
15
20
25
Placebo GPI
Number of People
(%)
(N=13105) (N=18297)
OR 0.91
95%CI 0.84, 0.98
P=0.015
1550 1980
Death/MI
1.4
2.4
0
1
2
3
4
Placebo GPI
(N=13105) (N=18297)
OR 1.62
95%CI 1.36, 1.97
P<0.0001
180 445
Major Bleeding
Boersma et al, Lancet 2002;359:189-1198.

GP 2b/3a Inhibitors in ACS (N=32,402)30-Day Death/MI According to PCI Within 5d (14%)
GP 2b/3a Inhibitors in ACS (N=32,402)30-Day Death/MI According to PCI Within 5d (14%)
11.4 10.7
0
5
10
15
20
25
Placebo GPI
1266 1695
(N=11148) (N=15876)
OR 0.95
95%CI 0.87, 1.02
NNT=143
- PCI
Number of People
(%)
14.5
11.8
0
5
10
15
20
25
Placebo GPI
284 285
(N=1957) (N=2421)
+ PCIOR 0.77
95%CI 0.64, 0.92
NNT=37
Boersma et al, Lancet 2002;359:189-1198.

GP 2b/3a Inhibitors in ACS (N=32,402)30-Day Death/MI According to Troponin Status (35%)
GP 2b/3a Inhibitors in ACS (N=32,402)30-Day Death/MI According to Troponin Status (35%)
6.2 7
0
5
10
15
20
Placebo GPI
153 255
(N=2452) (N=3653)
OR 1.17
95%CI 0.94, 1.44
Troponin -
Boersma et al, Lancet 2002;359:189-1198.
Number of People
(%)
1210.3
0
5
10
15
20
Placebo GPI
222 321
(N=1851) (N=3113)
Troponin +
OR 0.85
95%CI 0.70, 1.03

GUSTO IV-ACS: 48-hour OutcomesGUSTO IV-ACS: 48-hour Outcomes
1.8
0.3
2.6
0.7
3.1
0.9
0
1
2
3
4
Death/MI Death
Placebo
Abciximab 24 hours
Abciximab 48 hours
P = 0.006
% Patients
Lancet 2001

Key Points Regarding GP IIb/IIIa Inhibitors in ACSKey Points Regarding GP IIb/IIIa Inhibitors in ACS
• Should be considered in high-risk patients oriented to an
early invasive strategy (I, A); abciximab for upstream Rx if
no appreciable delay in angiography (I, B)
• Small molecules (tirofiban & eptifibatide) approved
for medical stabilization therapy (IIa, B)
• Combination Rx with ASA, heparin and clopidogrel may have
a favorable risk-benefit in high-risk pts - � TnI (IIa, B)
• Abciximab is contraindicated for medical therapy (Class III)

Optimal ACS Management with Antiplatelet Agents
Conclusion
Optimal ACS Management with Antiplatelet Agents
Conclusion
• Aspirin and clopidogrel are the most used, effective, safe and
cost-effective therapies
• GP IIb/IIIa inhibitors offer significant benefits with potential of
cost-effectiveness in high-risk patients
• Newer therapies look promising (prasugrel, cangrelor, AZD6140)
• Strategies for risk stratification and optimization of cost-benefit-
risk profile are worthwhile goals

“The aim of science is not only to
open the door to endless wisdom
but also to put a limit to endless error”
Galileo


Given our limited understanding of the exact mechanism and
incidence of stent thrombosis, our inability to accurately identify
at-risk patients and the lack of effective and safe therapies
to mitigate this risk, the most prudent strategy to limit this rare
but potentially life-threatening complication at the current time
is a selective, thoughtful and evidence-based application of
drug-eluting stents in clinical practice

0%
use
100%
use
~60% “off-label”(TAXUS ARRIVE 1, BASKET-LATE)
(� stent thrombosis = 2-3%)
Balancing Risk and BenefitDES Utilization: 2006
Balancing Risk and BenefitDES Utilization: 2006

Evidence-based
threshold
0%
use
100%
use
Balancing Risk and BenefitDES Utilization: 2007
Balancing Risk and BenefitDES Utilization: 2007
2007

Role of Clopidogrel in CHDRole of Clopidogrel in CHD
Stable CVDMI
Stroke
PAD
CHARISMA CURE
ACSUA/NSTEMI
CREDO
PCI-CURE
PCI-CLARITY
PCIStable CAD
UA/NSTEMI
STEMI
CLARITY
COMMIT
STEMI
Trial
Indication
Duration 28 months 9 months 1-12 months 8-28 days

Role of Clopidogrel in CHDRole of Clopidogrel in CHD
0 0.5 1 1.5
CV Death, MI or Stroke
CURE (9m)
CHARISMA (28m)
CLARITY (30d)
COMMIT (28d)
2
CREDO (12m)
Odds ratio
Major Bleeding
0 0.5 1 1.5 2
Odds ratio
Eshaghian, Kaul et al. Ann Int Med 2007

Role of Clopidogrel in CHD
Benefit-Risk Profile
Role of Clopidogrel in CHD
Benefit-Risk Profile
0
5
10
15
20
25
30
35
6 7 8 9 10 11 12
Control Event Rate (%)
0
5
10
15
20
25
30
35
Treatment benefit
Bleeding hazard
Bleeding hazard
(number per 1000)T
reatment benefit
(number per 1000)
CHARISMACOMMIT
CLARITY
CURE
CREDO
Eshaghian, Kaul et al. Ann Int Med 2007

Therapeutic Options in ACS (2007 Update)Therapeutic Options in ACS (2007 Update)
PCI eligible
Yes
PTCA/Stent
No
CABG or
Medical Rx
UFH or
LMWH or
Fondaparinux
(FRICESSENCE
TIMI-11B
FRAXIS
OASIS-5)
Convenient, reliable, safe,
as good as UFH
GP IIb/IIIa + heparin
(SYNERGY, A-to-Z)
Bivalirudin(ACUITY)
↓ Safety= efficacy
LMWH (dalteparin)
(FRISC-II)
Safe, effective,
‘Bridge’-Rx
+ GP IIb/IIIa +
(GUSTO IV-ACS
ACUTE-2)
Safe
? efficacy
USAP/NSTEMIASA + Clopidogrel (CURE)
UFH or
LMWH (enoxaparin)
(SYNERGY, A-to-Z)
GP IIb/IIIa
(Abciximab if no delay)
↓ Safety= efficacy
Aggressive strategy
Cor angio within 24-48h
Yes (FRISC II, TIMI 18-TACTICS, ICTUS)
Medical
stabilization Rx
No
High-risk
(don’t switch to UFH)
Cath Lab
+ _
Medical Rx
Stress test
(LVEF >40%)
>12-24h minimum