opciones terapéuticas en cáncer gástrico...
TRANSCRIPT

Coordinador Científico: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla, Santander
Organizado por: Fundación para el progreso de la oncología en Cantabria, FUPOCAN
Dra Paula Jiménez Fonseca
Opciones terapéuticas en cáncer gástrico metastásico

INDICE
1. Dónde estamos: quimioterapia 1ª línea
2. Dónde estamos: trastuzumab 1ª línea
3. Hacia dónde vamos: fármacos antidiana y perfil molecular
4. Cuales han mostrado eficacia en líneas sucesivas:
antiangiogénicos
5. Qué ocurre en práctica clínica: registro AGAMENON
6. Conclusiones
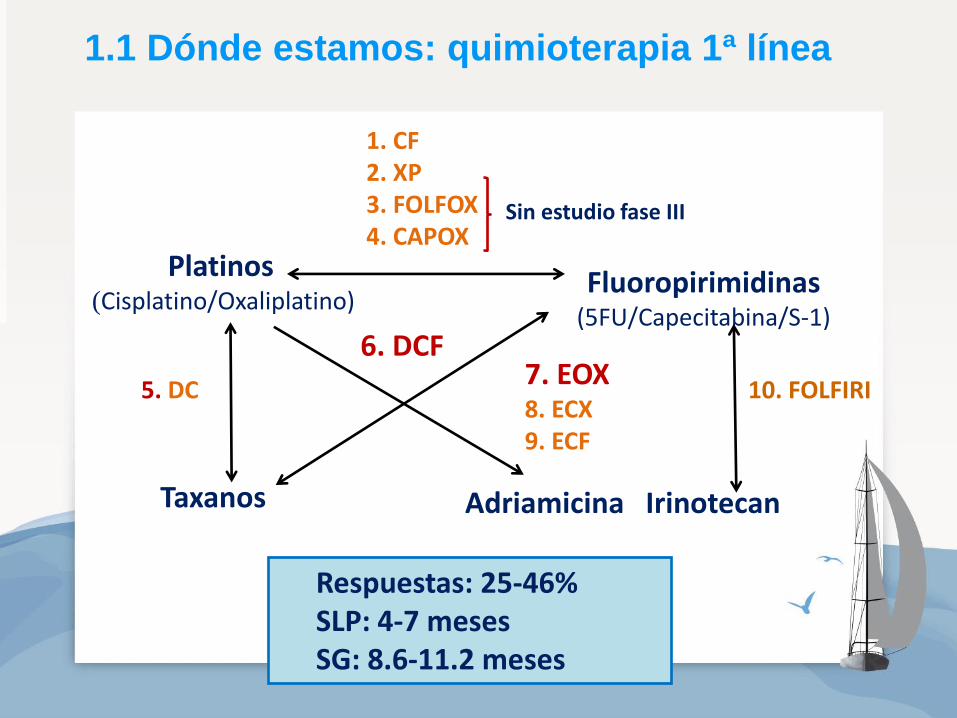
1.1 Dónde estamos: quimioterapia 1ª línea
Platinos (Cisplatino/Oxaliplatino)
Taxanos
Fluoropirimidinas (5FU/Capecitabina/S-1)
Adriamicina Irinotecan
1. CF 2. XP 3. FOLFOX 4. CAPOX
10. FOLFIRI 5. DC
6. DCF 7. EOX 8. ECX 9. ECF
Sin estudio fase III
Respuestas: 25-46% SLP: 4-7 meses SG: 8.6-11.2 meses
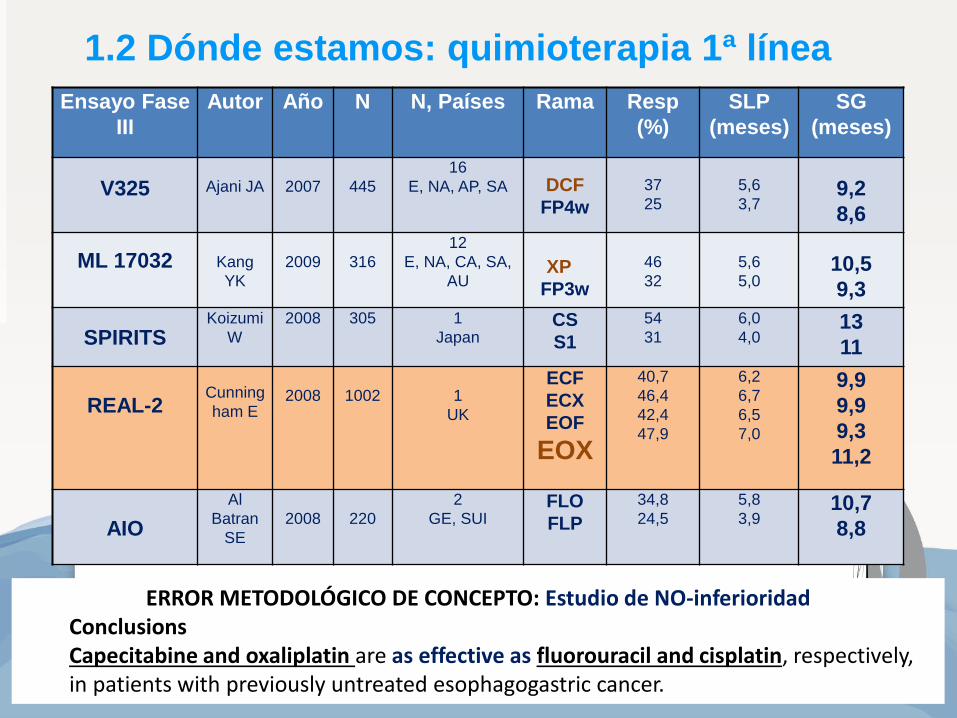
1.2 Dónde estamos: quimioterapia 1ª línea
Ensayo Fase
III
Autor Año N N, Países Rama Resp
(%)
SLP
(meses)
SG
(meses)
V325
Ajani JA
2007
445
16
E, NA, AP, SA
DCF
FP4w
37
25
5,6
3,7
9,2
8,6
ML 17032
Kang
YK
2009
316
12
E, NA, CA, SA,
AU
XP
FP3w
46
32
5,6
5,0
10,5
9,3
SPIRITS Koizumi
W
2008 305 1
Japan CS
S1
54
31
6,0
4,0 13
11
REAL-2
Cunning
ham E
2008
1002
1
UK
ECF
ECX
EOF
EOX
40,7
46,4
42,4
47,9
6,2
6,7
6,5
7,0
9,9
9,9
9,3
11,2
AIO
Al
Batran
SE
2008
220
2
GE, SUI FLO
FLP
34,8
24,5
5,8
3,9 10,7
8,8
ERROR METODOLÓGICO DE CONCEPTO: Estudio de NO-inferioridad Conclusions Capecitabine and oxaliplatin are as effective as fluorouracil and cisplatin, respectively, in patients with previously untreated esophagogastric cancer.

1.3 Dónde estamos: quimioterapia 1ª línea
Ensayo
Fase III
Autor Año N N
Países
Rama Resp
(%)
mSLP
(m)
mSG
(m)
V325
Ajani JA
2007
445
16
E, NA, AP, SA
DCF
FP4w
37
25
5,6
3,7
9,2
8,6
ML 17032
Kang YK
2009
316
12
E, NA, CA, SA,
AU
XP
FP3w
46
32
5,6
5,0
10,5
9,3
SPIRITS Koizumi
W
2008 305 1
Japan CS
S1
54
31
6,0
4,0 13
11
REAL-2
Cunningh
am E
2008
1002
1
UK
ECF
ECX
EOF
EOX
40,7
46,4
42,4
47,9
6,2
6,7
6,5
7,0
9,9
9,9
9,3
11,2
Conclusions
To our knowledge, V325 is the first phase III trial to report clinical benefit in AGGEC
patients.
Clinical benefit was assessed beyond protocol-specific chemotherapy.
The addition of D to CF not only significantly improved clinical benefit but also
improved quality of life, time to progression, and overall survival compared with CF.


Platino + Fluoropirimidina
+ Anthraciclinas
Platino + Fluoropirimidina
1.5 ¿Aporta añadir un 3º fármaco?
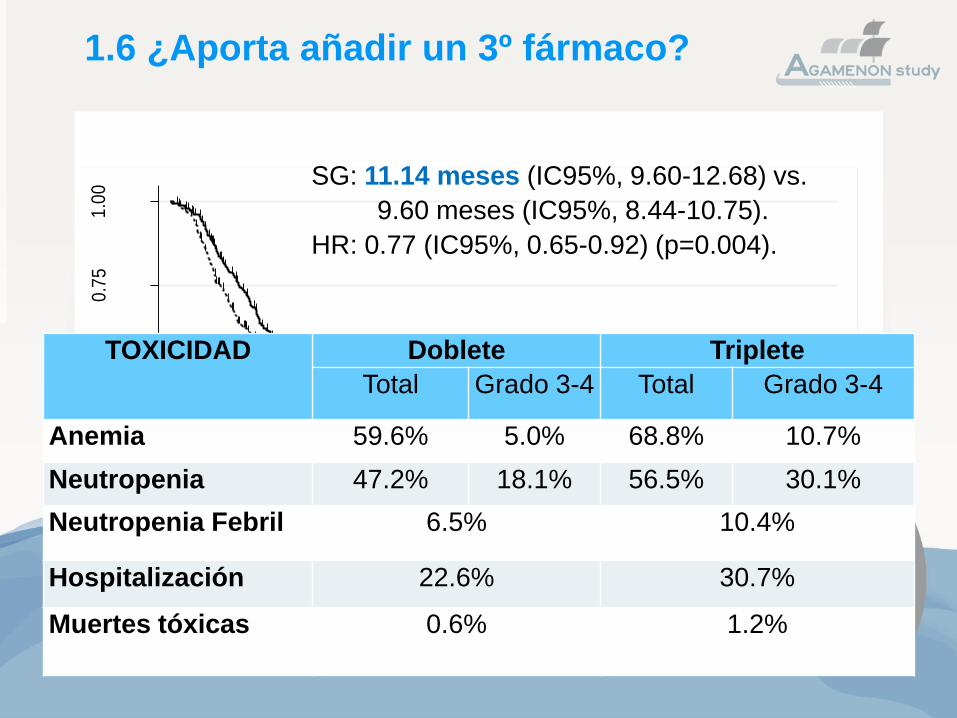
1.6 ¿Aporta añadir un 3º fármaco? 0
.00
0.2
50
.50
0.7
51
.00
Pro
ba
bili
ty o
f su
rviv
al
0 12 24 36 48 60Months of follow up
Doublet Triplet
SG: 11.14 meses (IC95%, 9.60-12.68) vs.
9.60 meses (IC95%, 8.44-10.75).
HR: 0.77 (IC95%, 0.65-0.92) (p=0.004).
TOXICIDAD
Doblete Triplete
Total Grado 3-4 Total Grado 3-4
Anemia 59.6% 5.0% 68.8% 10.7%
Neutropenia 47.2% 18.1% 56.5% 30.1%
Neutropenia Febril 6.5% 10.4%
Hospitalización 22.6% 30.7%
Muertes tóxicas 0.6% 1.2%

JNCI J Natl Cancer Inst, 2016, Vol. 108, No. 10
CONCLUSIONS: Based on efficacy and toxicity, F-doublets FOx, FI, and FT are
preferred as 1-line treatment for AEGC compared with C-doublets, A-triplets, and
TCF. FOxT is the most promising triplet.
REFLEXIÓN SOBRE 1ª LÍNEA
En la actualidad HAY CONSENSO en afirmar que no existe consenso sobre la primera línea de quimioterapia en cánceres no susceptible de recibir trastuzumab.
El papel de las antraciclinas no ha podido confirmarse.
Los tripletes añaden TOXICIDAD y dudoso beneficio.
2ª línea: PACLITAXEL + RAMUCIRUMAB
1ª línea: PLATINO + FLUOROPIRIMIDINA No taxano por usarse en 2ª línea
¿? oxaliplatino pq su neuropatía podría condicionar el uso paclitaxel
FOLFIRI en no candidatos a cisplatino

INDICE
1. Dónde estamos: quimioterapia 1ª línea
2. Dónde estamos: trastuzumab 1ª línea
3. Hacia dónde vamos: fármacos antidiana y perfil molecular
4. Cuales han mostrado eficacia en líneas sucesivas:
antiangiogénicos
5. Qué ocurre en práctica clínica: registro AGAMENON
6. Conclusiones

2.1. Trastuzumab en 1ª línea

2.2. Dónde estamos: trastuzumab 1ª línea
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84
0
20
40
60
80
100
Months of follow up
Surv
ival pro
bability (
%)
Classification of centers by quartiles
Q1
Q2
Q3
Q4
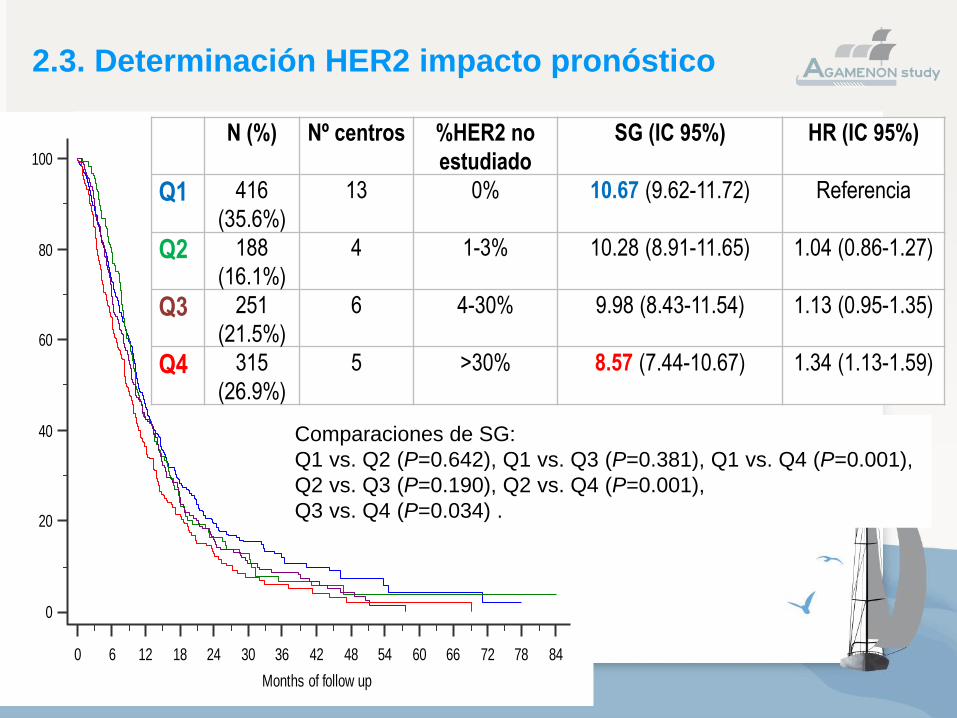
N (%) Nº centros %HER2 no
estudiado
SG (IC 95%) HR (IC 95%)
Q1 416
(35.6%)
13 0% 10.67 (9.62-11.72) Referencia
Q2 188
(16.1%)
4 1-3% 10.28 (8.91-11.65) 1.04 (0.86-1.27)
Q3 251
(21.5%)
6 4-30% 9.98 (8.43-11.54) 1.13 (0.95-1.35)
Q4 315
(26.9%)
5 >30% 8.57 (7.44-10.67) 1.34 (1.13-1.59)
Comparaciones de SG:
Q1 vs. Q2 (P=0.642), Q1 vs. Q3 (P=0.381), Q1 vs. Q4 (P=0.001),
Q2 vs. Q3 (P=0.190), Q2 vs. Q4 (P=0.001),
Q3 vs. Q4 (P=0.034) .
2.3. Determinación HER2 impacto pronóstico

INDICE
1. Dónde estamos: quimioterapia 1ª línea
2. Dónde estamos: trastuzumab 1ª línea
3. Hacia dónde vamos: fármacos antidiana y perfil molecular
4. Cuales han mostrado eficacia en líneas sucesivas: antiangiogénicos
5. Qué ocurre en práctica clínica: registro AGAMENON
6. Conclusiones
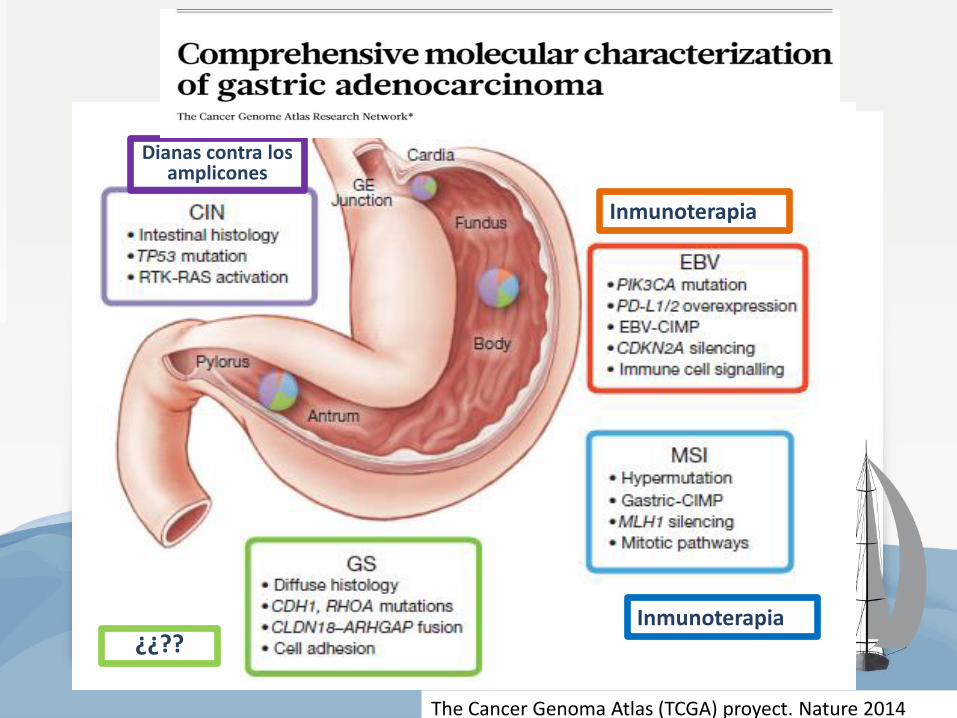
The Cancer Genoma Atlas (TCGA) proyect. Nature 2014
Inmunoterapia
Inmunoterapia
Dianas contra los amplicones
¿¿??

3.2. Dianas y fármacos
GRANITE x
SHINE x
RILOMET x
Panitumumab Cetuximab
REAL-3 x EXPAND x
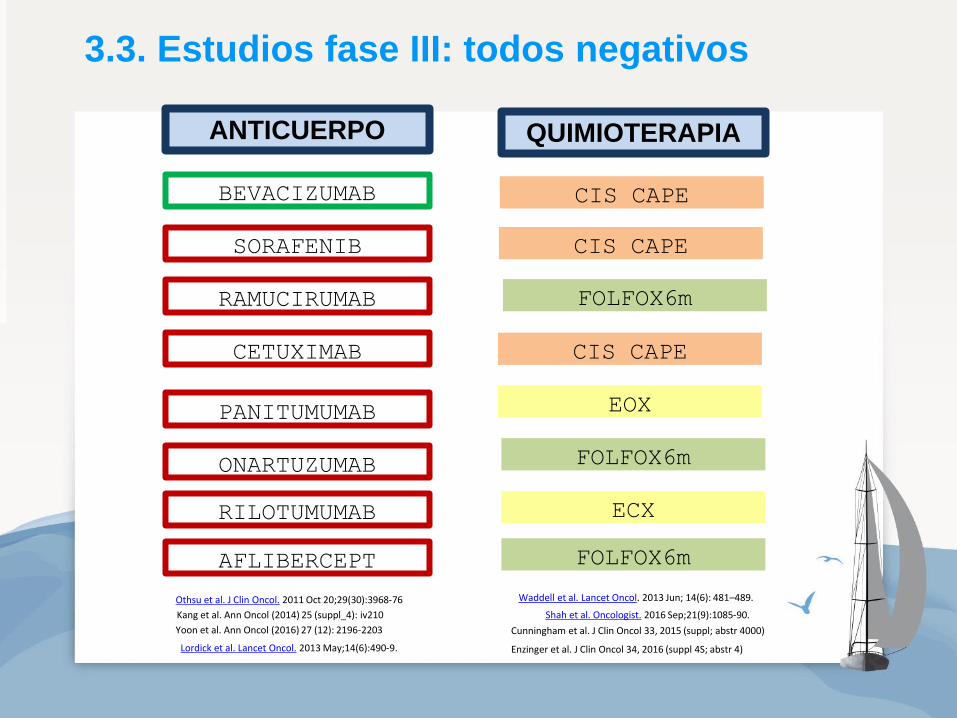
BEVACIZUMAB
SORAFENIB
RAMUCIRUMAB
CETUXIMAB
PANITUMUMAB
ONARTUZUMAB
RILOTUMUMAB
AFLIBERCEPT
QUIMIOTERAPIA
CIS CAPE
CIS CAPE
FOLFOX6m
CIS CAPE
EOX
FOLFOX6m
ECX
FOLFOX6m
Othsu et al. J Clin Oncol. 2011 Oct 20;29(30):3968-76
Lordick et al. Lancet Oncol. 2013 May;14(6):490-9.
Kang et al. Ann Oncol (2014) 25 (suppl_4): iv210
Yoon et al. Ann Oncol (2016) 27 (12): 2196-2203
Waddell et al. Lancet Oncol. 2013 Jun; 14(6): 481–489.
Shah et al. Oncologist. 2016 Sep;21(9):1085-90.
Cunningham et al. J Clin Oncol 33, 2015 (suppl; abstr 4000)
Enzinger et al. J Clin Oncol 34, 2016 (suppl 4S; abstr 4)
ANTICUERPO
3.3. Estudios fase III: todos negativos
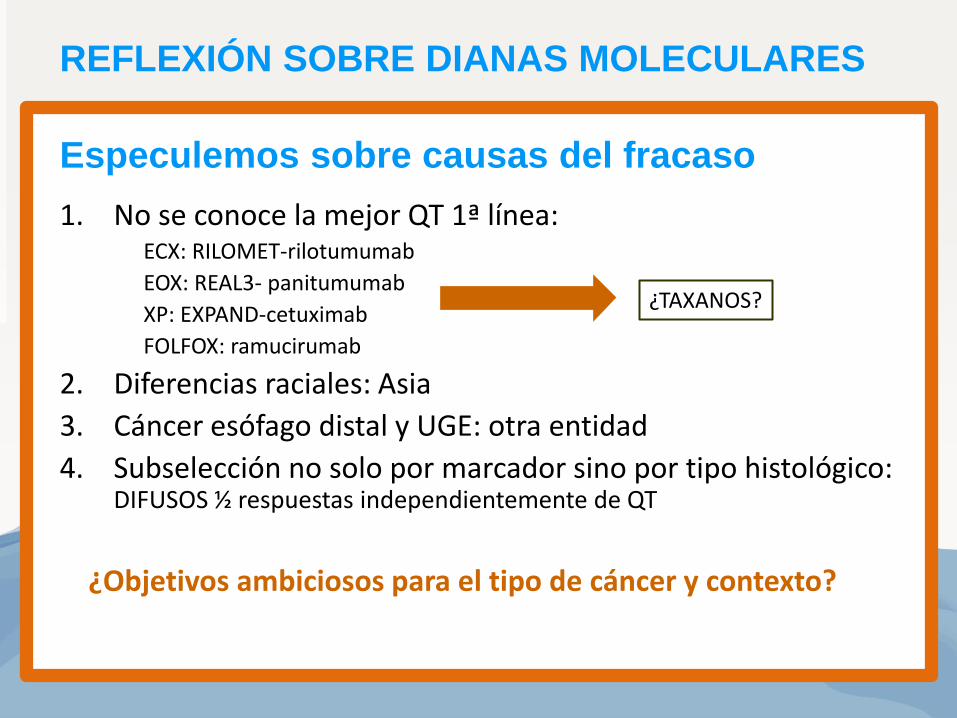
Especulemos sobre causas del fracaso
1. No se conoce la mejor QT 1ª línea: ECX: RILOMET-rilotumumab
EOX: REAL3- panitumumab
XP: EXPAND-cetuximab
FOLFOX: ramucirumab
2. Diferencias raciales: Asia
3. Cáncer esófago distal y UGE: otra entidad
4. Subselección no solo por marcador sino por tipo histológico: DIFUSOS ½ respuestas independientemente de QT
¿Objetivos ambiciosos para el tipo de cáncer y contexto?
¿TAXANOS?
REFLEXIÓN SOBRE DIANAS MOLECULARES
INDICE
1. Dónde estamos: quimioterapia 1ª línea
2. Dónde estamos: trastuzumab 1ª línea
3. Hacia dónde vamos: fármacos antidiana y perfil molecular
4. Cuales han mostrado eficacia en líneas sucesivas:
antiangiogénicos
5. Qué ocurre en práctica clínica: registro AGAMENON
6. Conclusiones
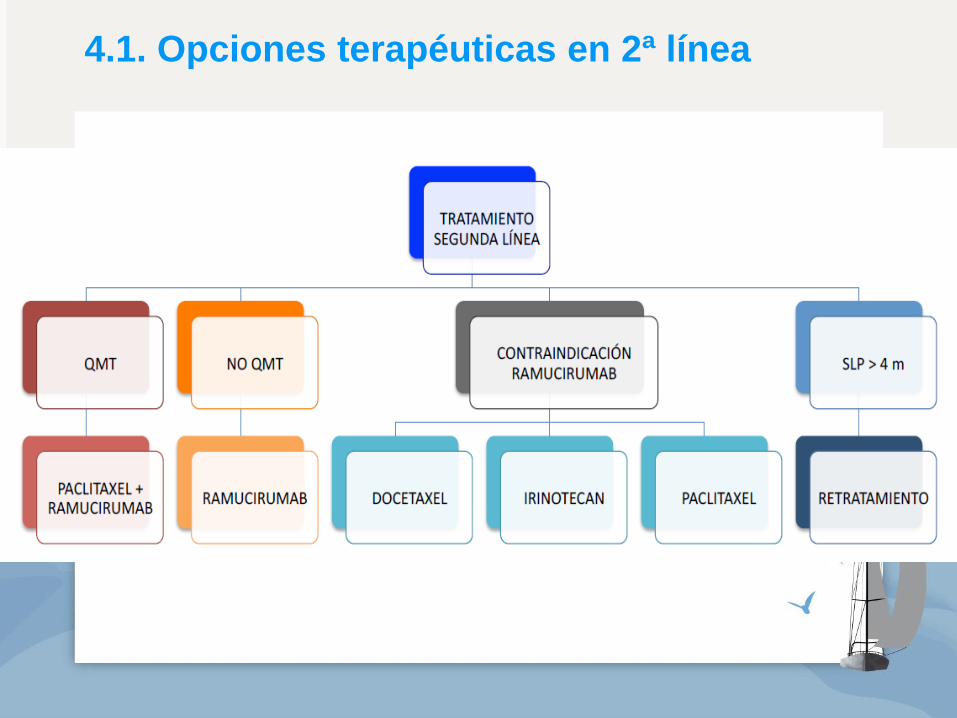
4.1. Opciones terapéuticas en 2ª línea
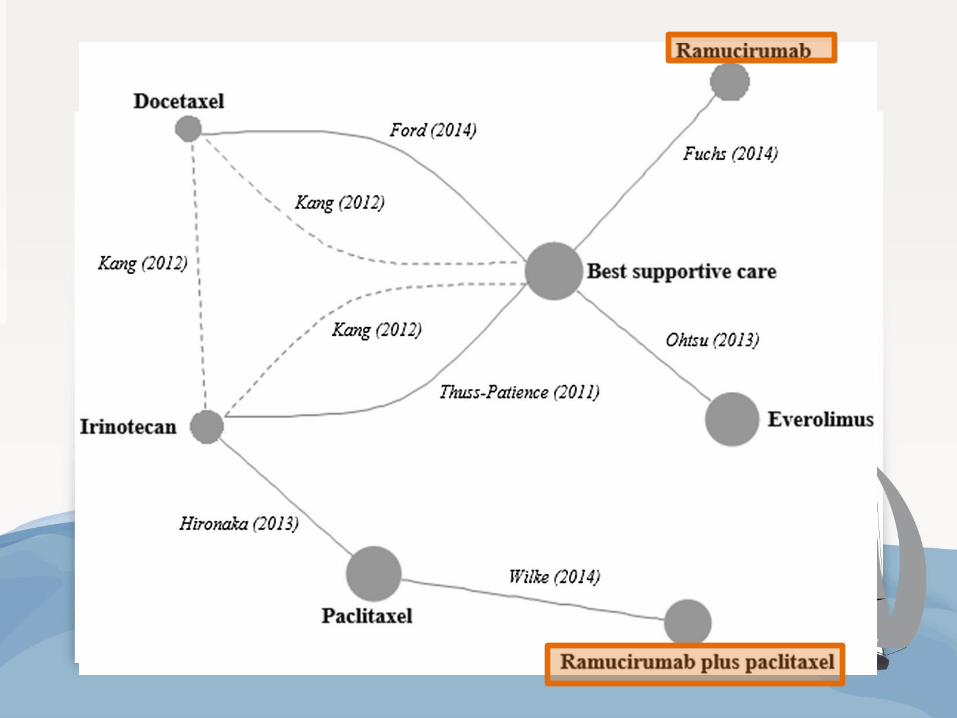

Ramucirumab en 2ª línea: 2 estudios fase III positivos
Fuchs, Lancet 2014; Wilke, Lancet Oncol 2014

4.3. Opciones terapéuticas en 2ª línea
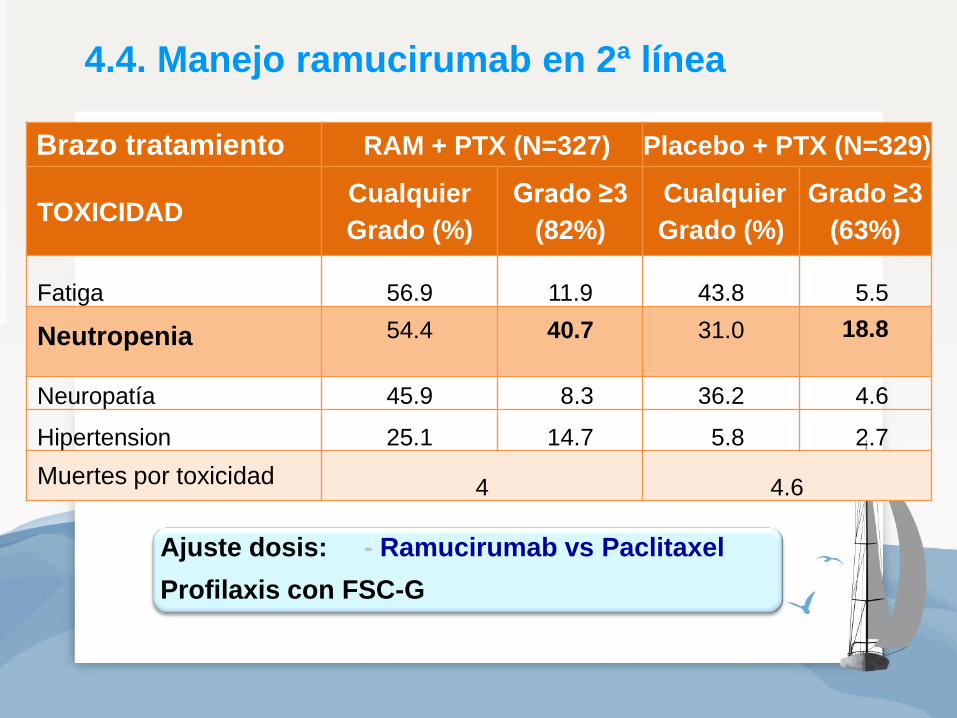
Brazo tratamiento RAM + PTX (N=327) Placebo + PTX (N=329)
TOXICIDAD Cualquier
Grado (%)
Grado ≥3
(82%)
Cualquier
Grado (%)
Grado ≥3
(63%)
Fatiga 56.9 11.9 43.8 5.5
Neutropenia
54.4
40.7
31.0
18.8
Neuropatía 45.9 8.3 36.2 4.6
Hipertension 25.1 14.7 5.8 2.7
Muertes por toxicidad 4 4.6
Ajuste dosis: - Ramucirumab vs Paclitaxel
Profilaxis con FSC-G
4.4. Manejo ramucirumab en 2ª línea
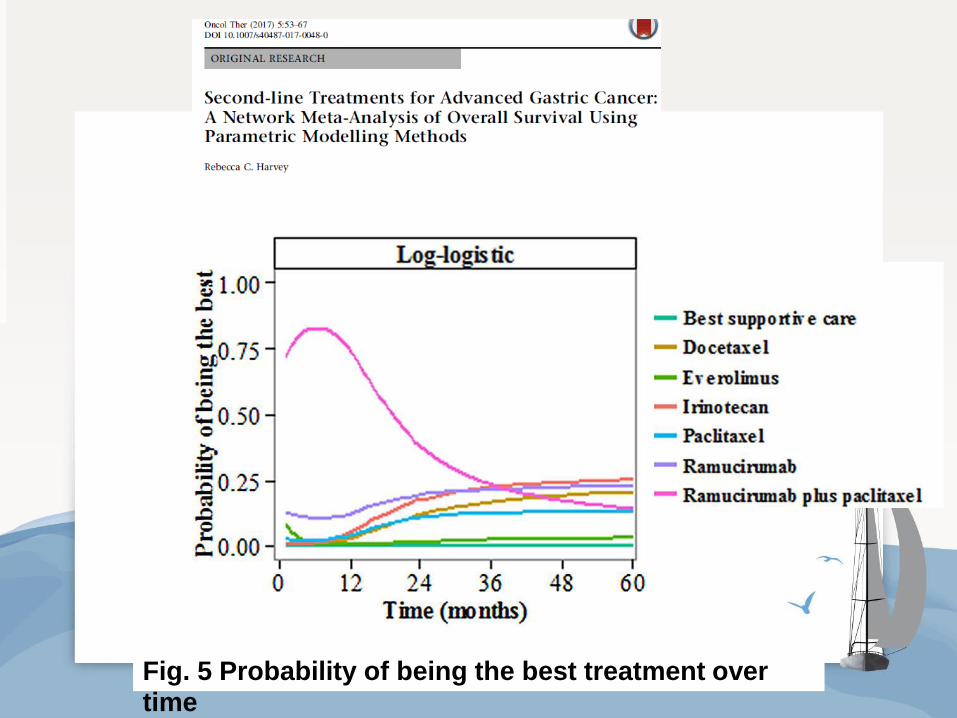
Fig. 5 Probability of being the best treatment over time

4.5. 3ª línea y sucesivas líneas: APATINIB

4.6. 3ª línea y sucesivas líneas: APATINIB
Apatinib: diana
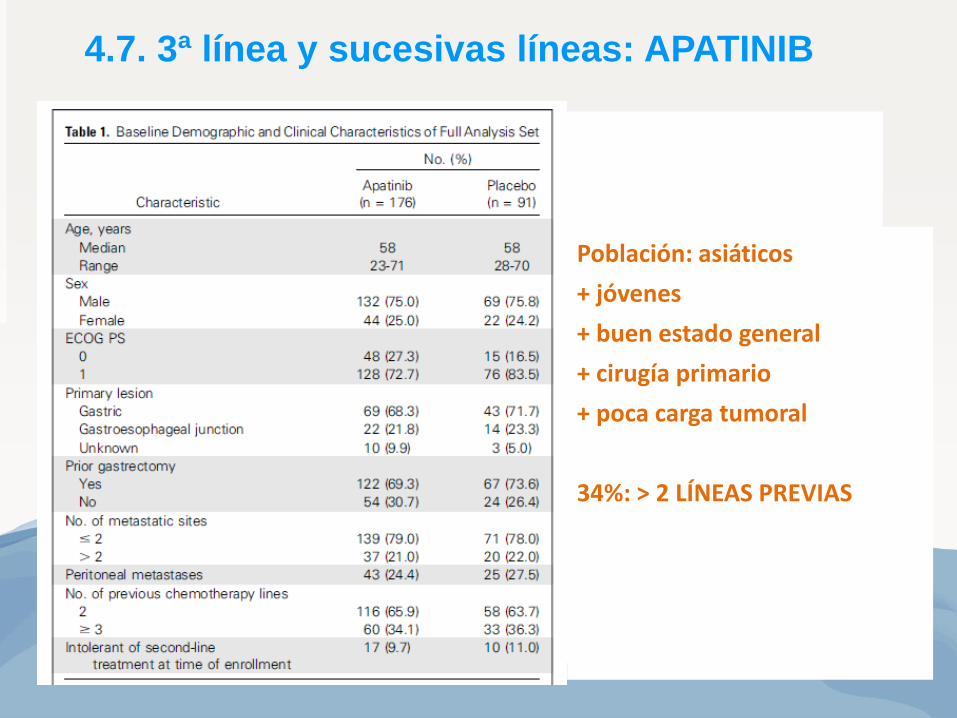
Población: asiáticos
+ jóvenes
+ buen estado general
+ cirugía primario
+ poca carga tumoral
34%: > 2 LÍNEAS PREVIAS
4.7. 3ª línea y sucesivas líneas: APATINIB

Supervivencia
Apatinib: 6.5 (4.8-7.6)
Placebo: 4.7 (3.6-5.4)
HR 0.70 (0.53-0.93)
Supervivencia libre progresión
Apatinib: 2.6 (2.0-2.9)
Placebo: 1.8 (1.4-1.9)
HR 0.44 (0.33-0.59)
4.7. 3ª línea y sucesivas líneas: APATINIB
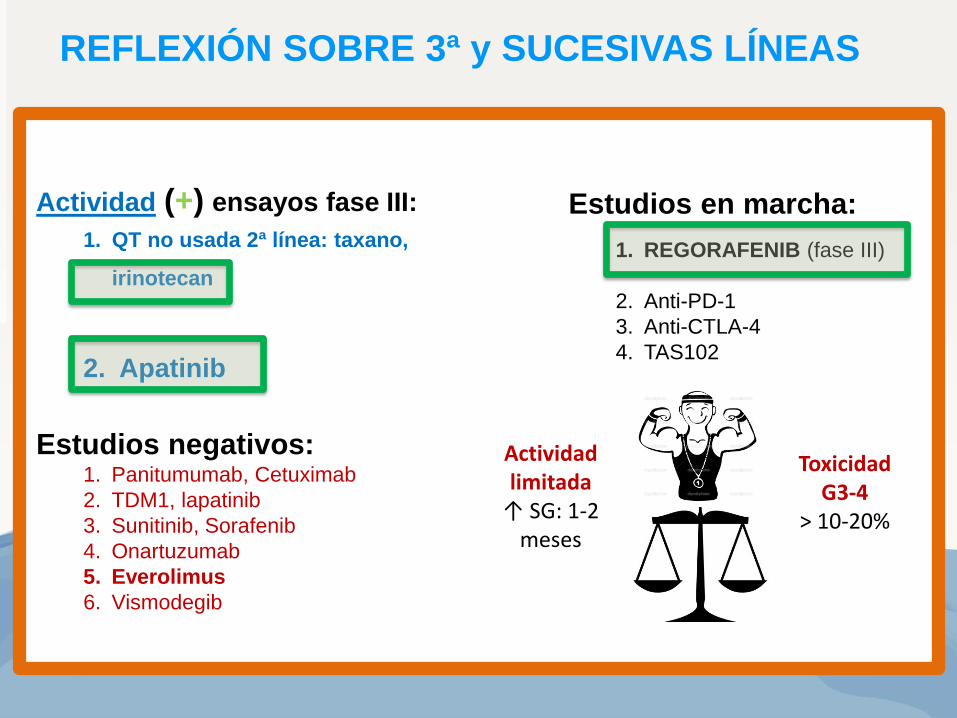
Actividad (+) ensayos fase III:
1. QT no usada 2ª línea: taxano,
irinotecan
2. Apatinib
Estudios negativos: 1. Panitumumab, Cetuximab
2. TDM1, lapatinib
3. Sunitinib, Sorafenib
4. Onartuzumab
5. Everolimus
6. Vismodegib
Estudios en marcha:
1. REGORAFENIB (fase III)
2. Anti-PD-1
3. Anti-CTLA-4
4. TAS102
Actividad limitada
↑ SG: 1-2 meses
Toxicidad G3-4
> 10-20%
REFLEXIÓN SOBRE 3ª y SUCESIVAS LÍNEAS
INDICE
1. Dónde estamos: quimioterapia 1ª línea
2. Dónde estamos: trastuzumab 1ª línea
3. Hacia dónde vamos: fármacos antidiana y perfil molecular
4. Cuales han mostrado eficacia en líneas sucesivas:
antiangiogénicos
5. Qué ocurre en práctica clínica: registro AGAMENON
5. Nomograma 6. Lauren 7. Ancianos 8. Cirugía de metástasis 9. Score trombosis 10. 6 meses vs hasta progresión

0 25 50 75 100 125 150 175
La Paz
Central Asturias
Tenerife
Gregorio Marañon
Morales Meseguer
Ciudad Real
El Mar
Galdakao
Doce Octubre
Las Palmas
Ramón y Cajal
Navarra
Valdecilla
Elche
Son Espases
Virgen Rocío
Tecknon Barcelona
Reina Sofía
Clinic Barcelona
Miguel Servet
CUNs Reclutamiento: 01.06.2017
Pacientes
5.1. Registro nacional: 2318 pacientes en 3 años
www.agamenonstudy.com

C-Index, SCORES:
0.547 (95% CI, 0.53-0.57) RMH-I
0.570 (95% CI, 0.54-0.60) KCC-S
0.583 (95% CI, 0.55-0.61) SMC-I
0.673 (95% CI, 0.64-0.71)
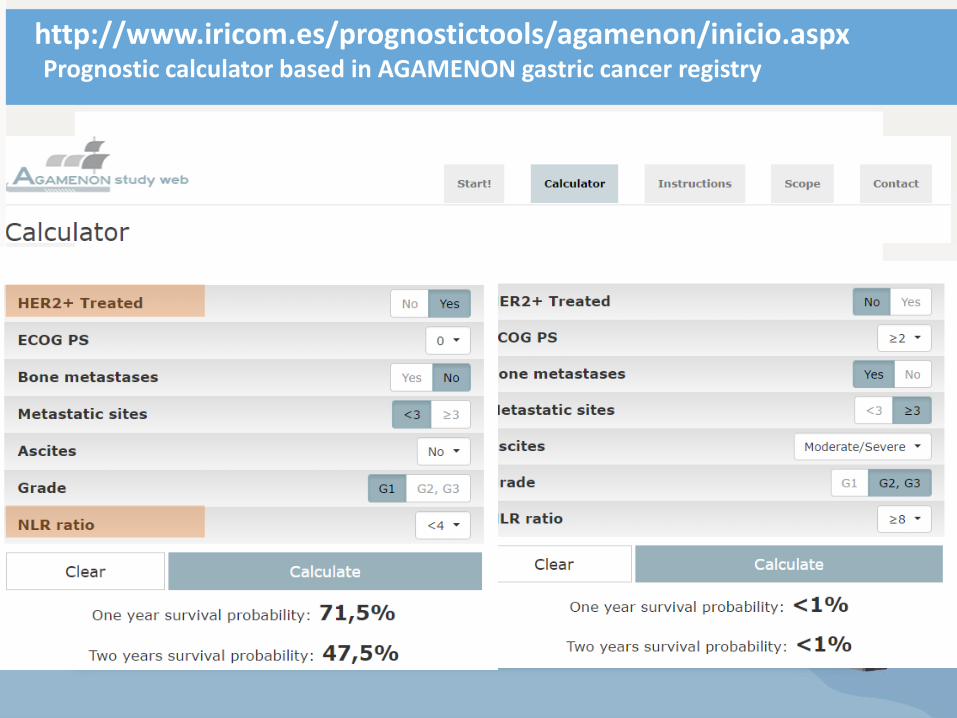
http://www.iricom.es/prognostictools/agamenon/inicio.aspx Prognostic calculator based in AGAMENON gastric cancer registry
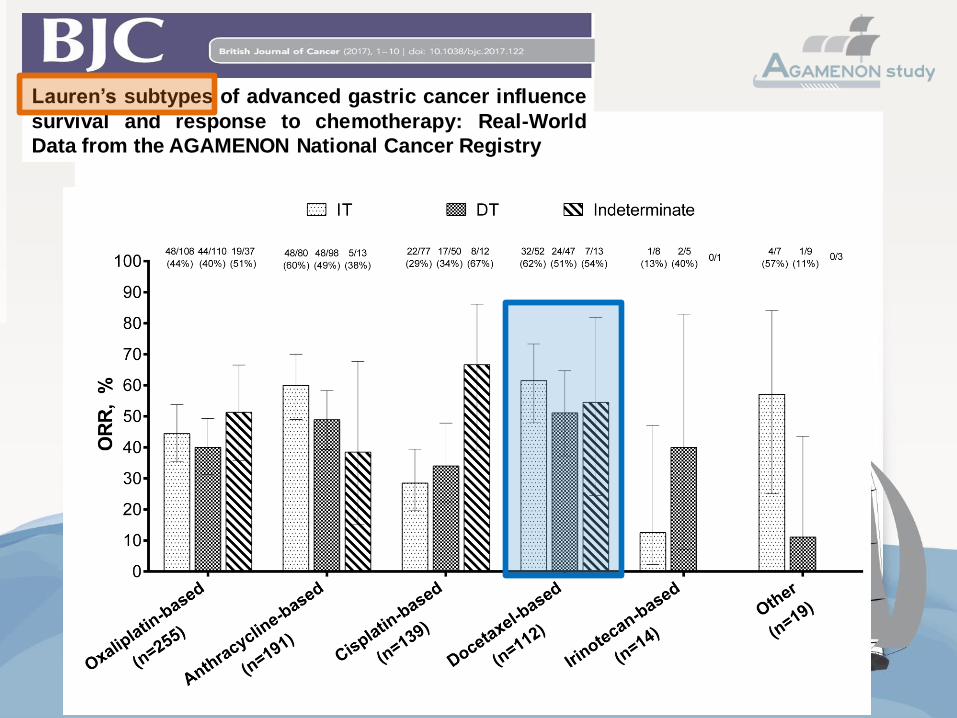
Lauren’s subtypes of advanced gastric cancer influence
survival and response to chemotherapy: Real-World
Data from the AGAMENON National Cancer Registry

Lancet Oncol. 2016;17(12):1697-708. Histopathological regression after neoadjuvant docetaxel, oxaliplatin, fluorouracil,
and leucovorin versus epirubicin, cisplatin, and fluorouracil or capecitabine in
patients with resectable gastric or gastro-oesophageal junction adenocarcinoma
(FLOT4-AIO): results from the phase 2 part of a multicentre, open-label, randomised
phase 2/3 trial. Al-Batran.
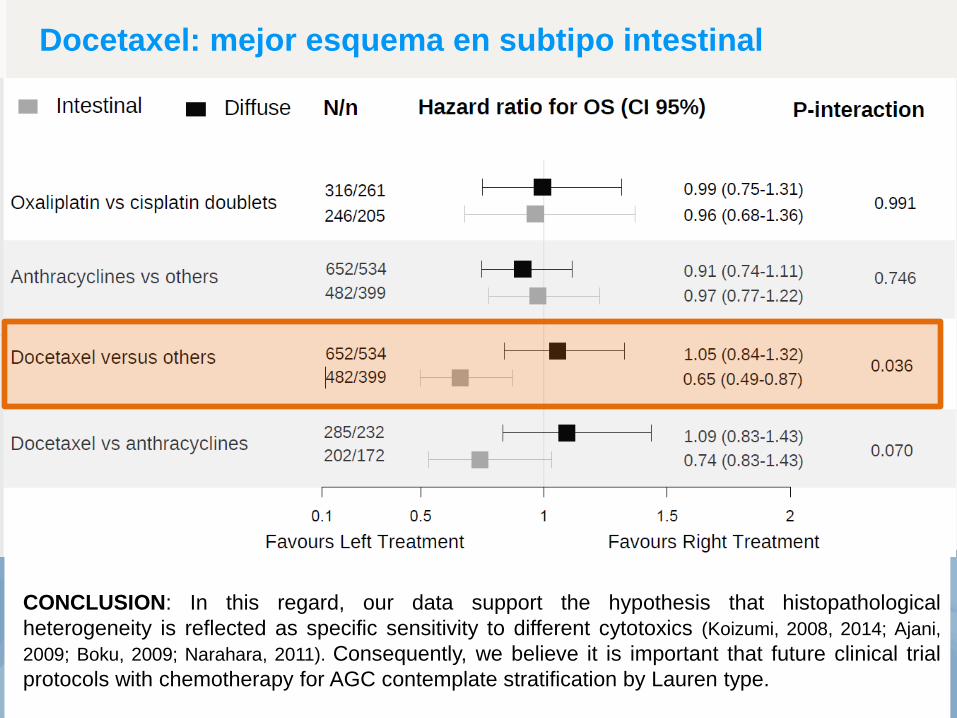
Docetaxel: mejor esquema en subtipo intestinal
CONCLUSION: In this regard, our data support the hypothesis that histopathological
heterogeneity is reflected as specific sensitivity to different cytotoxics (Koizumi, 2008, 2014; Ajani,
2009; Boku, 2009; Narahara, 2011). Consequently, we believe it is important that future clinical trial
protocols with chemotherapy for AGC contemplate stratification by Lauren type.

Efficacy and safety of chemotherapy in elderly versus non-elderly patients with advanced gastric cancer: a real-world data, non-inferiority analysis Laura Visa, P Jimenez-Fonseca2, J Gallego3, R Hernández4, A Custodio5, M. Garrido6, A Viudez7, E Buxo8, I. Echavarria9, JM Cano10, I Macias11, M Mangas12,
E Martínez de Castro13, T García14, F Á Manceñido15, A Fernández Montes16, A Azkarate17, F Longo18, A Díaz19, C López20, A Hurtado21, P Cerdá22, R Serrano23, A
Gil-Negrete24, A Martín Carnicero25, P Pimentel26, A Ramchandani27, A Carmona-Bayonas28. On behalf of the AGAMENON Study Group.
CONCLUSION: In short, this study provides evidence (grade C) that the use of
chemotherapy regimens in the elderly is non-inferior in terms of OS with respect to
schedules used in younger patients, with comparable grade 3-4 toxicity, although this may be
due in part to small modifications or adaptations made ad hoc by medical oncologists when
administering treatments.
R e s p o n s e a s s e s s m e n t b y R E C I S T , %
0 5 1 0 1 5 2 0 2 5 3 0 3 5 4 0 4 5 5 0 5 5 6 0
C o m p le te re s p o n s e
P artia l re s p o n s e
P ro g res s iv e d is eas e
S tab le d is eas e
7 0< 7 0
R e s p o n s e a s s e s s m e n t b y R E C I S T , %
0 5 1 0 1 5 2 0 2 5 3 0 3 5 4 0 4 5 5 0 5 5 6 0
C o m p le te re s p o n s e
P artia l re s p o n s e
P ro g res s iv e d is eas e
S tab le d is eas e
7 0< 7 0
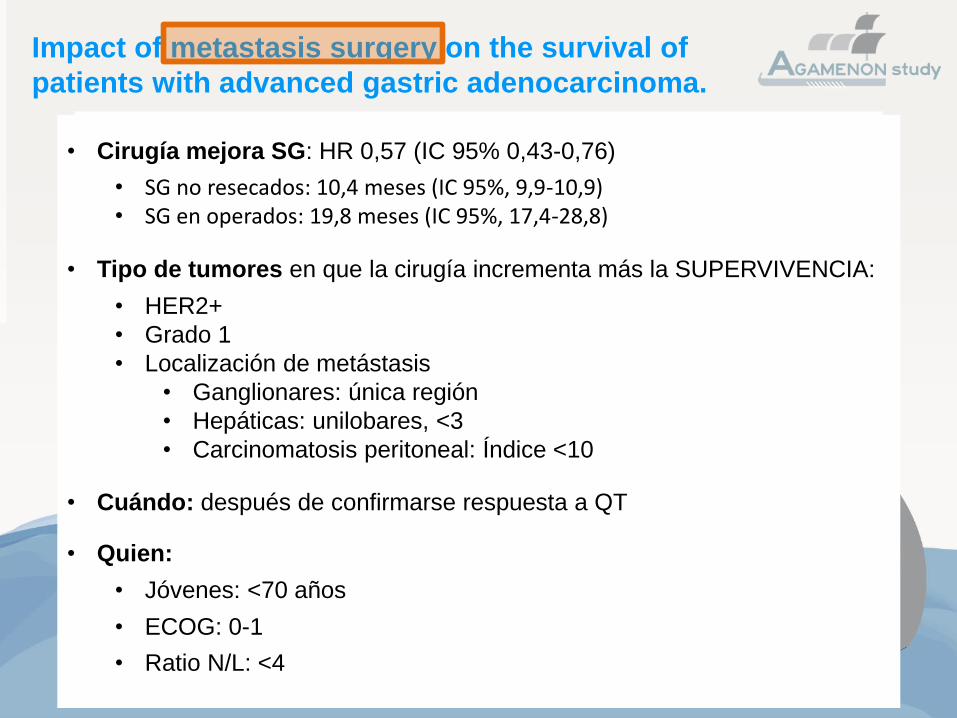
Impact of metastasis surgery on the survival of
patients with advanced gastric adenocarcinoma.
• Cirugía mejora SG: HR 0,57 (IC 95% 0,43-0,76)
• SG no resecados: 10,4 meses (IC 95%, 9,9-10,9) • SG en operados: 19,8 meses (IC 95%, 17,4-28,8)
• Tipo de tumores en que la cirugía incrementa más la SUPERVIVENCIA:
• HER2+
• Grado 1
• Localización de metástasis
• Ganglionares: única región
• Hepáticas: unilobares, <3
• Carcinomatosis peritoneal: Índice <10
• Cuándo: después de confirmarse respuesta a QT
• Quien:
• Jóvenes: <70 años
• ECOG: 0-1
• Ratio N/L: <4
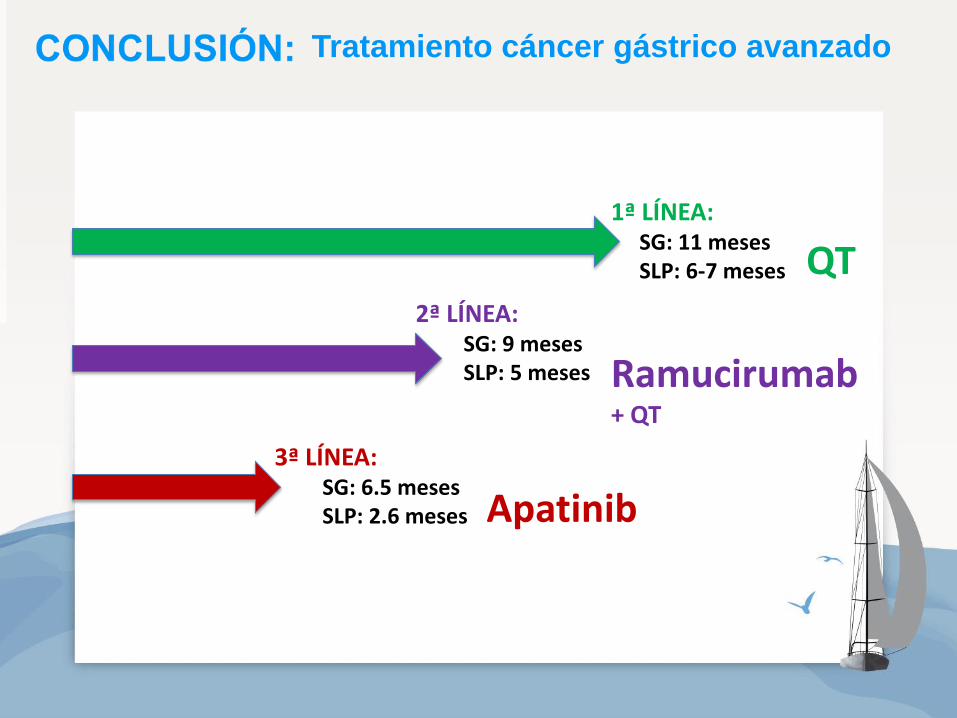
1ª LÍNEA: SG: 11 meses SLP: 6-7 meses
2ª LÍNEA: SG: 9 meses SLP: 5 meses
3ª LÍNEA: SG: 6.5 meses SLP: 2.6 meses
QT
Ramucirumab
+ QT
Apatinib
Tratamiento cáncer gástrico avanzado

CONCLUSIÓN:
1ª línea
• Platino + Fluoropirimidina
• Si erbB2+: + Trastuzumab
• Si nec respuesta en intestinal: +docetaxel
• No platino: FOLFIRI
2ª línea
• Paclitaxel + Ramucirumab
• ECOG2: ramucirumab
• Si PE> 4 meses desde stop 1ª línea: reiniciar
3ª línea
• Apatinib • Inmunoterapia
• Regorafenib
Score pronóstico AGAMENON:
http://www.iricom.es/prognostictools/agamenon/inicio.aspx
Tratamiento cáncer gástrico avanzado
