oligodendroglioma with 1p/19q co-deletion: what is (are ... · oligodendroglioma with 1p/19q...
TRANSCRIPT

Oligodendroglioma with 1p/19q co-deletion: What is (are) the
next question(s)?Marc Sanson
Service de Neurologie Mazarin, Institut du Cerveau et de la Moelle, Hôpital de la Salpêtrière,
Université Pierre et Marie Curie
EANO-EORTC meeting Istanbul 27-
28 march 2015
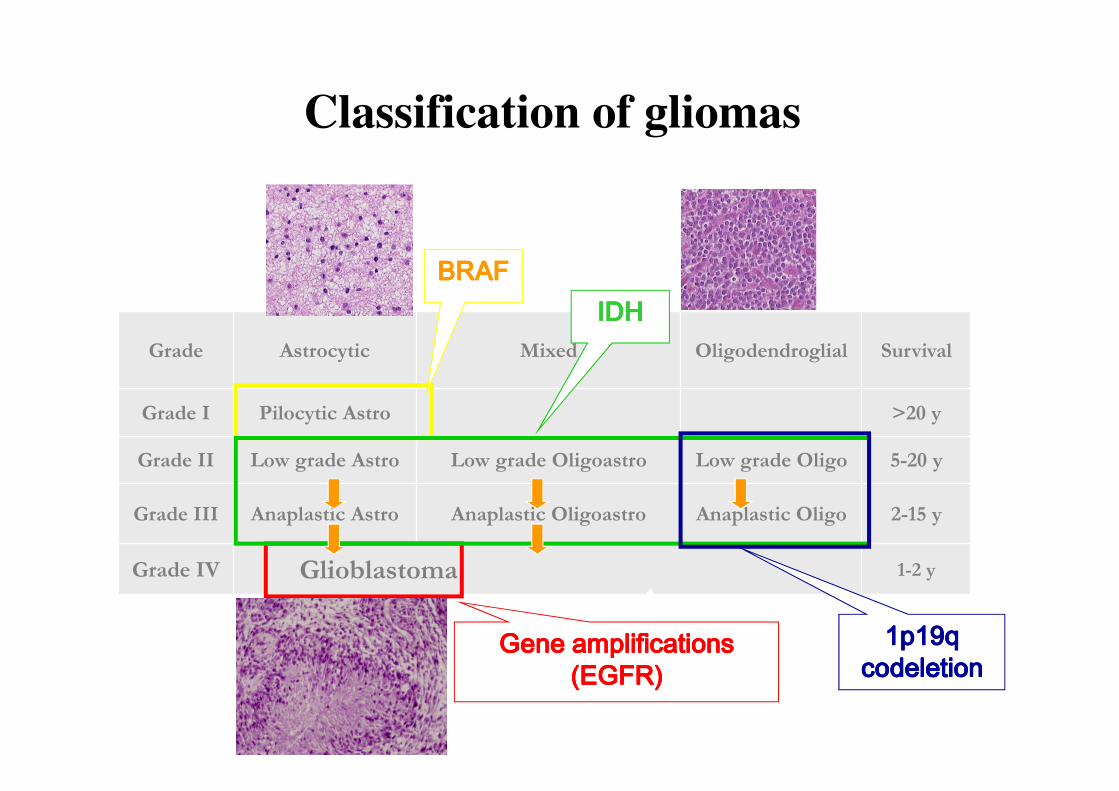
Grade Astrocytic Mixed Oligodendroglial Survival
Grade I Pilocytic Astro >20 y
Grade II Low grade Astro Low grade Oligoastro Low grade Oligo 5-20 y
Grade III Anaplastic Astro Anaplastic Oligoastro Anaplastic Oligo 2-15 y
Grade IV Glioblastoma 1-2 y
BRAFBRAFBRAFBRAFIDHIDHIDHIDH
Gene amplifications Gene amplifications Gene amplifications Gene amplifications (EGFR)(EGFR)(EGFR)(EGFR)
Classification of gliomas
1p19q1p19q1p19q1p19qcodeletioncodeletioncodeletioncodeletion

EANO Marseille 6-9 october
anaplastic oligodendroglioma with 1p19q
codeletion: response to chemotherapy
2 cycles2 cycles2 cycles2 cycleschemotherapychemotherapychemotherapychemotherapy
Chr 1p lossChr 1p lossChr 1p lossChr 1p lossChr 19q lossChr 19q lossChr 19q lossChr 19q loss
Jenkins, 2006Jenkins, 2006Jenkins, 2006Jenkins, 2006

0 1000 2000 3000 4000 5000 6000 7000 8000 9000 10 000
0
10
20
30
40
50
60
70
80
90
(days)
MT
D (
mm
)
A No 1p19q deletion = 5.9 mm/yearNo 1p19q deletion = 5.9 mm/yearNo 1p19q deletion = 5.9 mm/yearNo 1p19q deletion = 5.9 mm/year
1p19q deletion = 3.4 mm/year1p19q deletion = 3.4 mm/year1p19q deletion = 3.4 mm/year1p19q deletion = 3.4 mm/year
Ricard et al, 2007
Natural history:1p19q codeleted LGG grow
slower

All the 1p19q codeleted gliomas are IDH mutatedAll the 1p19q codeleted gliomas are IDH mutatedAll the 1p19q codeleted gliomas are IDH mutatedAll the 1p19q codeleted gliomas are IDH mutatedisocitrate
α-ketoglutarate
NADP
NADPH
IDH1
nal
+
D-2-H glutarate↑↑
NADP+
NADPH
IDH1
mut
Reshape cell epigenome
• DNA hypermethylation (CIMP)
• Histone methylation
++++
----
O
Dang et al, Nature 2010; van den Bent et al, Clin Cancer Res 2011; Turcan et al, Nature 2012; Lu et al, Nature 2012
Gène MGMT
Promoter
Unmethylated
Promoter
methylated
Gène MGMT

1p19q codeletion and IDH mutation
Only IDH mutation
None of these alterations
All gliomas with 1p19q codeletion are IDH mutated
Months
Grade III
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 50 100 150 200 250
Grade II
Months
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 50 100 150 200
Survival %
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
0 50 100 150 200
Grade IV
Months
Labussière 2010, 2014
Prognostic classification based on IDH and 1p19q status

IDH Mutated Non mutated
Telomere maintenance
hTERTpromotermutation
ATRX mutationALT (alternative
lenghteningtelomeres)
hTERT promoter mutation
Other frequent
alterations
1p19q codeletion
TP53 mut Gene amplif (EGFR), loss 10q..
Predominant histology
Oligo Astro GBM
MedianSurvival
>14 y 4-7 y 1.5 y
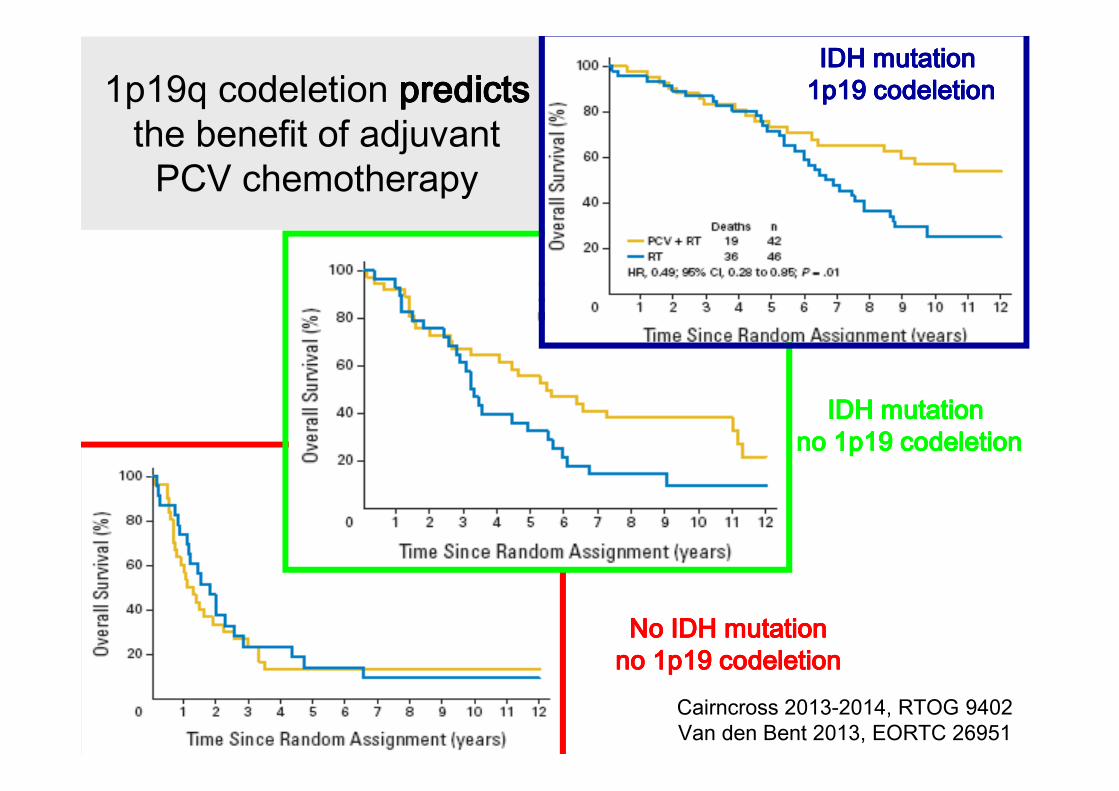
1p19q codeletion predictspredictspredictspredictsthe benefit of adjuvant
PCV chemotherapy
Cairncross 2013-2014, RTOG 9402Van den Bent 2013, EORTC 26951
IDH mutation IDH mutation IDH mutation IDH mutation no 1p19 codeletionno 1p19 codeletionno 1p19 codeletionno 1p19 codeletion
No IDH mutationNo IDH mutationNo IDH mutationNo IDH mutationno 1p19 codeletionno 1p19 codeletionno 1p19 codeletionno 1p19 codeletion
IDH mutation IDH mutation IDH mutation IDH mutation 1p19 codeletion1p19 codeletion1p19 codeletion1p19 codeletion

• Molecular oligodendrogliomas
• Tertp-mut, IDH-mut, proneural
expression profile (Alpha-internexine
expression)
• OS=14 years « LGG like »
• Standard: RT-PCV (>RT alone)
• Concern: long term toxicity
IDHmut
with 1p19q
codeletion

1p19q codeleted (oligodendro)gliomas:
next questions
• Can we consider to delay the radiotherapy
in grade III 1p19q codeleted glioma?
• Should we separate grade II and III?
• Which chemotherapy TMZ? PCV?
• New molecular markers
• New therapies
EANO-EORTC meeting Istanbul 27-
28 march 2015EANO-EORTC meeting Istanbul 27-
28 march 2015
EANO-EORTC meeting Istanbul 27-28
march 2015

Can we consider to delay the radiotherapy
in grade III 1p19q?
• Risk of radiation-induced cognitive dysfunction:
– Among 32 long-term progression-free survivors treated within the EORTC
26951 trial: 74% cognitively impaired (30% severely) (Habets 2014).
• In LLG, deferring RT until tumor progression did not impair OS as
compared to early RT (Van den Bent 2005)
• Chemotherapy alone not inferior to RT alone (Wick 2009)
• No difference of chemotherapy alone (10.5 years) vs RT plus
chemotherapy (8.4 years) (Lassman 2011)
• Survey of treatment recommendation, 42% of neuro-oncologists
deferred radiotherapy (Abrey 2007)
EANO-EORTC meeting Istanbul 27-
28 march 2015EANO-EORTC meeting Istanbul 27-
28 march 2015
EANO-EORTC meeting Istanbul 27-28
march 2015

POLCA TrialMulticentric study comparing chemotherapy with PCV alone vs radiotherapy
followed by PCV as post operative treatment of anaplastic oligodendroglial
tumors with 1p/19q codeletion
Lassman et al, Neuro-Oncology 2011 13:649–659; Cairncross et al, J clin Oncol 2012;31:337-43; Ducray, PHRC 2013
RT
280 patients
PCV 6 adjuvant cycles
R
PCV 6 cycles
RT
74% cognitive impairment (30% severe)
POLCA trial (1p-19q codeleted)
Primary objective: survival
without cognitive deterioration
Secondary objectives:
PFS, OS, QoL,…

1p19q codeleted (oligodendro)gliomas:
current questions
• Can we consider to delay the radiotherapy in
grade III 1p19q codeleted glioma?
• Should we separate grade II and III?
• Which chemotherapy TMZ? PCV?
• New molecular markers
• New therapies
EANO-EORTC meeting Istanbul 27-
28 march 2015EANO-EORTC meeting Istanbul 27-
28 march 2015
EANO-EORTC meeting Istanbul 27-28
march 2015

Overall survival grade II and III gliomas
0 100 2000
50
100
Codel IICodel III
IDHmut non-codel II
IDHmut non-codel III
IDHwt II
IDHwt III
p=0.13
*** p<0.001
*** p<0.001
OS (month)
Perc
en
t su
rviv
al
n=89n=96
n=208
n=166
n=81
n=169
Relevance of grade according to molecular subtype
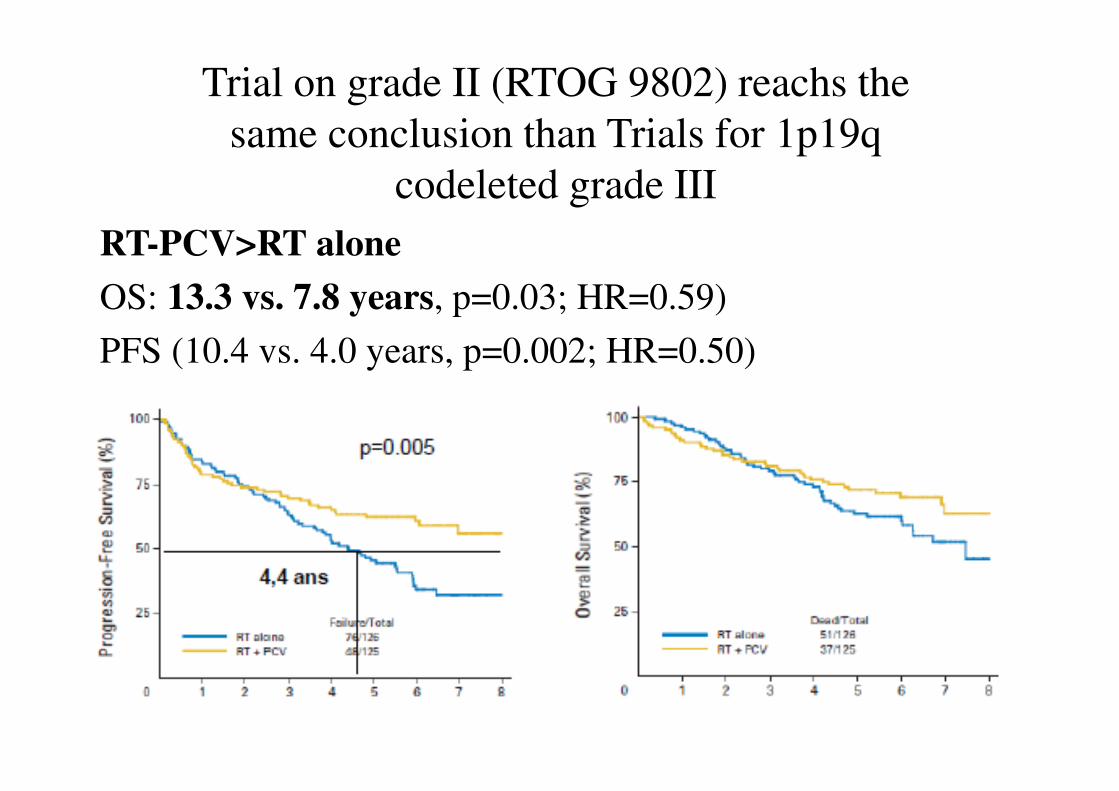
Trial on grade II (RTOG 9802) reachs the
same conclusion than Trials for 1p19q
codeleted grade III
RT-PCV>RT alone
OS: 13.3 vs. 7.8 years, p=0.03; HR=0.59)
PFS (10.4 vs. 4.0 years, p=0.002; HR=0.50)

Codel Trial
Inclusion of grade II (54 Gy) and
III (59 gy)
235 pts RT→PCV
235 pts RT-TMZ→TMZ
50 pts TMZ→ → → RT-PCV
EANO-EORTC meeting Istanbul 27-
28 march 2015

1p19q codeleted (oligodendro)gliomas:
current questions
• Can we consider to delay the radiotherapy in
grade III 1p19q codeleted glioma?
• Should we separate grade II and III?
• Which chemotherapy TMZ? PCV?
• New molecular markers
• New therapies
EANO-EORTC meeting Istanbul 27-
28 march 2015EANO-EORTC meeting Istanbul 27-
28 march 2015
EANO-EORTC meeting Istanbul 27-28
march 2015

- Longer TTP compared to TMZ (Lassman 2011)
- Sustained effect of PCV chemotherapy
Peyre 2010
Why PCV (and not TMZ) ?Why PCV (and not TMZ) ?Why PCV (and not TMZ) ?Why PCV (and not TMZ) ?
EANO-EORTC meeting Istanbul 27-
28 march 2015

Peyre 2010
Case 1 Case 2Start PCVStart PCVStart PCVStart PCV Start PCVStart PCVStart PCVStart PCV
End PCVEnd PCVEnd PCVEnd PCV End PCVEnd PCVEnd PCVEnd PCVBest RespBest RespBest RespBest Resp Best RespBest RespBest RespBest Resp
EANO-EORTC meeting Istanbul 27-
28 march 2015

1p19q codeleted (oligodendro)gliomas:
current questions
• Can we consider to delay the radiotherapy in
grade III 1p19q codeleted glioma?
• Should we separate grade II and III?
• Which chemotherapy TMZ? PCV?
• New molecular markers: Tertp, IDHmut,
CIC, FUBP1, Notch pathway
• New therapies
EANO-EORTC meeting Istanbul 27-
28 march 2015EANO-EORTC meeting Istanbul 27-
28 march 2015
EANO-EORTC meeting Istanbul 27-28
march 2015

Gleize 2015
CIC mutations
• CIC(capicua homologue) on
19q13.2 is a transcriptional
repressor
• 50-60% of 1p19q codeleted
gliomas (60/109)
• Specific to 1p19q codeleted
gliomas
• Inactivated by mutation

• CIC inactivating mutation
are associated with poorer
outcome
• CIC mutated LGG grow
faster
• CIC inactivation results in
resistance to TMZ
Gleize 2015
Clinical impact of CIC mutations

1p19q codeleted (oligodendro)gliomas:
current questions
• Can we consider to delay the radiotherapy in
grade III 1p19q codeleted glioma?
• Should we separate grade II and III?
• Which chemotherapy TMZ? PCV?
• New molecular markers
• New therapies
EANO-EORTC meeting Istanbul 27-
28 march 2015EANO-EORTC meeting Istanbul 27-
28 march 2015
EANO-EORTC meeting Istanbul 27-28
march 2015

Future therapies: IDH mutated gliomas
isocitrate
α-ketoglutarate
NADP
NADPH
IDH1
nal
+
D-2-H glutarate↑↑
NADP+
NADPH
IDH1
mut
Reshape cell epigenome
• DNA hypermethylation (CIMP)
• Histone methylation
++++
----
• Demethylating agents (5-Aza)
• Specific inhibitor of IDHmut enzyme
O

AG120
In acute myeloid leukemia (AML):
• 14 relapsed and/or refractory AML
• 7 Responses (4 CR)
• Reduced plasmatic D-2HG
• Re-differenciation
EANO-EORTC meeting Istanbul 27-
28 march 2015
Pollyea et al 26th EORTC-NCI-AACR Symposium on Molecular Targets and Cancer Therapeutics Barcelona, 2014
Still on evaluation in gliomas (phase 1)

Conclusion
• Molecular signature (ie1p19q codeletion) more
important than grade
• Predictive marker
• Two goals for the treatment
– To maintain (increase) long survival (oncological
endpoint)
– To preserve cognitive function and QOL (neurological
endpoint)
• Futures perspectives
– To « reprogramme » and to differentiate IDH-mut tumor
– New targets specific to 1p19q codeleted gliomas

Department of Neurology
Experimental Neuro-oncology
Université Pierre et Marie Curie
• Jean-Yves Delattre
• Khe Hoang-Xuan
• Ahmed Idbaih
• Agusti Alentorn
• Vincent Gleize
• Marianne Labussière
• Amithys Rahimian
• Karima Mokhtari (neuropath)
• Laurent Capelle (neurosurgery)
• Matthieu Peyre (neurosurgery)
• François Ducray (HopitalNeurologique, Lyon)