oh my aching knee jeffrey rosenberg md department of family medicine montefiore hospital bronx ny
TRANSCRIPT

Oh My Aching Knee
Jeffrey Rosenberg MDJeffrey Rosenberg MD
Department of Family MedicineDepartment of Family Medicine
Montefiore HospitalMontefiore Hospital
Bronx NYBronx NY

Objectives
Learn to evaluate an adolescent’s knee Learn to evaluate an adolescent’s knee Learn to evaluate an acutely injured kneeLearn to evaluate an acutely injured knee Learn to evaluate an older patient’s kneeLearn to evaluate an older patient’s knee Learn How to examine the KneeLearn How to examine the Knee

Anterior Knee

Posterior Knee

Adolescent Knee Pain
15 year old male, plays multiple sports with 15 year old male, plays multiple sports with insidious onset of anterior knee pain. insidious onset of anterior knee pain. Worse after sitting in class, up and down Worse after sitting in class, up and down stairs. No instabilitystairs. No instability
On exam, no effusion, non tender at tibial On exam, no effusion, non tender at tibial tubercle, but peripatellar tissues are tender. tubercle, but peripatellar tissues are tender. Increased Q angle, increased patellar laxityIncreased Q angle, increased patellar laxity

Adolescents Non Traumatic
Osgood-Schlaters Disease-Pain at Tibial Osgood-Schlaters Disease-Pain at Tibial TubercleTubercle
Patellar Tendonitis-Usually Proximal Patellar Tendonitis-Usually Proximal Patellar-Athletes that JumpPatellar-Athletes that Jump
Ilio-Tibial Band:RunnersIlio-Tibial Band:Runners All the Rest: Patellar Femoral SyndromeAll the Rest: Patellar Femoral Syndrome

Patellar Femoral Syndrome
Mal-alignment-Q Mal-alignment-Q Repetitive ForcesRepetitive Forces Muscle TightnessMuscle Tightness Exam: Patellar GlideExam: Patellar Glide
Patellar CompressionPatellar Compression
Patellar Tilt Patellar Tilt ROM/FlexibilityROM/Flexibility

Q Angle
Should be <20 male, Should be <20 male, <25 Female<25 Female
Flat feet, wide pelvis Flat feet, wide pelvis widen angle widen angle
Treatment: VMO Treatment: VMO strengthening, strengthening, stretching, McConnell stretching, McConnell TapingTaping

Case #2 Acute Traumatic Knee
23 yo female soccer player comes in two 23 yo female soccer player comes in two hours after being slid into from the side. hours after being slid into from the side. No pop felt, but not able to bear weight No pop felt, but not able to bear weight immediately afterwards, feels unstable immediately afterwards, feels unstable
On exam, tense effusion, limited ROM, On exam, tense effusion, limited ROM, lachmans’ positive with loss of endpoint lachmans’ positive with loss of endpoint and increased movement on Anterior and increased movement on Anterior DrawerDrawer

Acute Knee Injuries
Patellar Dislocation: Patellar Dislocation: Traumatic vs Non Traumatic; RecurrentTraumatic vs Non Traumatic; Recurrent All need Bracing for 2 to 4 weeks, PTAll need Bracing for 2 to 4 weeks, PT
Collateral Ligaments: If Laxity with Stress, may Collateral Ligaments: If Laxity with Stress, may be complete tear. Functional Brace, PTbe complete tear. Functional Brace, PT
ContusionContusion ACLACL Meniscus TearMeniscus Tear
ACL Injury Non Traumatic vs TraumaticNon Traumatic vs Traumatic
Women have more non traumatic ACL Women have more non traumatic ACL tearstears
High Impact, Planted Foot, Valgus Force or High Impact, Planted Foot, Valgus Force or Medial Rotation of TibiaMedial Rotation of Tibia
Field Sports, SkiingField Sports, Skiing Pop (60-70%)Pop (60-70%) Swells < 2 hours, feels well in a few daysSwells < 2 hours, feels well in a few days Recurrent Instability with twisting/stairsRecurrent Instability with twisting/stairs

Anterior Cruciate Testing
ACL should feel taught, like rope stretched to its maximum. Loss of this endpoint is consistent with tear

ACL ACL
TestiTestingng
SensitivitySensitivity SpecificitySpecificity Positive Positive LRLR
Negative Negative LRLR
CompoCompositesite
82%82% 94%94% 2525 0.040.04
AnteriAnterior or DraweDrawerr
62% 62%
(9-93%)(9-93%)
67% 67% (23-100%)(23-100%)
3.83.8 0.300.30
LachLachmansmans
84%84%(60-100%)(60-100%)
100% 100% (POOR (POOR QUALITY)QUALITY)
4242 0.100.10
PivotPivot 38% 38%
(27-95%)(27-95%)Solomon, et al: JAMA 286:13

Meniscus Tear
Twisting Injury with knee in flexionTwisting Injury with knee in flexion Can be degenerative tears-non traumaticCan be degenerative tears-non traumatic Pain with Stairs/SquattingPain with Stairs/Squatting Instability/giving way/true lockingInstability/giving way/true locking

Meniscus Test
Start with knee in flexion. Place Start with knee in flexion. Place thumb and index finger along thumb and index finger along joint line.joint line.
Flex the leg fully, internally rotate Flex the leg fully, internally rotate foot, abduct the lower leg and foot, abduct the lower leg and extend joint. Feel for click along extend joint. Feel for click along medial joint line, or pain medial joint line, or pain
Repeat for lateral meniscus: Repeat for lateral meniscus: externally rotate foot and adduct externally rotate foot and adduct the leg the leg
Appley’s grind test-also not Appley’s grind test-also not specificspecific
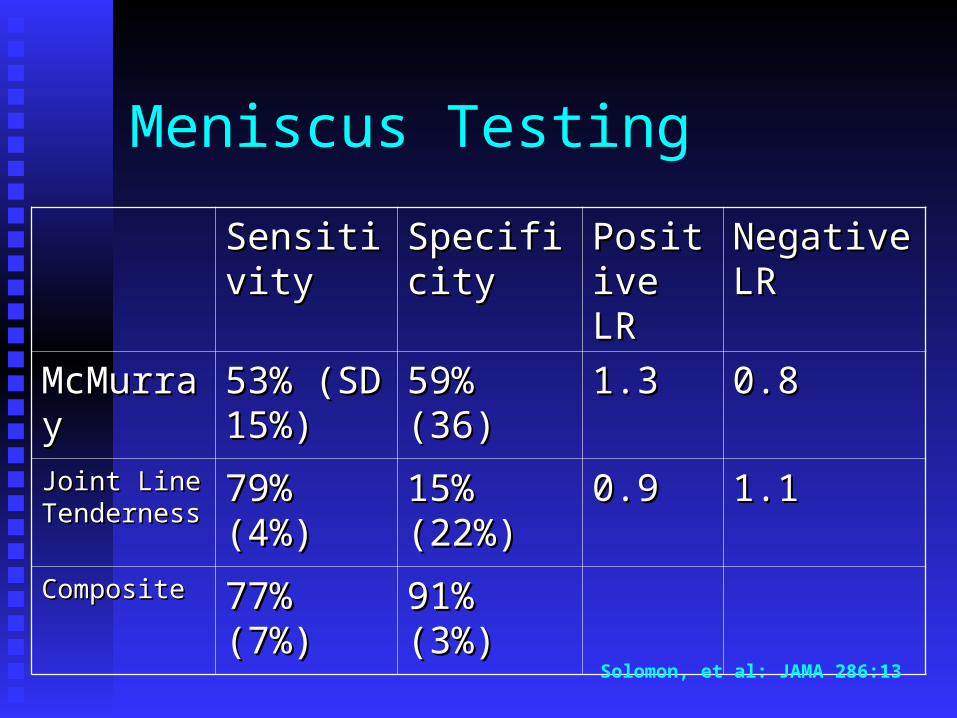
Meniscus Testing
SensitivitySensitivity SpecificitySpecificity Positive Positive LRLR
Negative Negative LRLR
McMurrayMcMurray 53% (SD 53% (SD 15%)15%)
59% (36)59% (36) 1.31.3 0.80.8
Joint Line Joint Line TendernessTenderness
79% (4%)79% (4%) 15% 15% (22%)(22%)
0.90.9 1.11.1
CompositeComposite 77% (7%)77% (7%) 91% (3%)91% (3%)
Solomon, et al: JAMA 286:13

Case #3 Older Patient
65 year old female with acute knee pain x 65 year old female with acute knee pain x two weeks. Increases with walking, stairs. two weeks. Increases with walking, stairs. Throbbing pain at nighttime (like a tooth Throbbing pain at nighttime (like a tooth ache). Tylenol helpful. On examination ache). Tylenol helpful. On examination mod sized effusion, mildly warm, decreased mod sized effusion, mildly warm, decreased ROM. What could be the diagnosisROM. What could be the diagnosis

American College of Rheumatology-Osteoarthritis Age > 50Age > 50 Morning Stiffness < 30 minsMorning Stiffness < 30 mins CrepitusCrepitus Bony EnlargementBony Enlargement Bony TendernessBony Tenderness Lack of WarmthLack of Warmth 34 % prevalence in adult population34 % prevalence in adult population

Osteoarthritis
Glucosamine Chondroitin: 2000 mg/day x Glucosamine Chondroitin: 2000 mg/day x 12 weeks, then lower to 1000 mg/day12 weeks, then lower to 1000 mg/day
Acetominophen >> NSAIDSAcetominophen >> NSAIDS Maintain strength, flexibility-swimming, Maintain strength, flexibility-swimming,
biking, tai chi, etcbiking, tai chi, etc Steroid Injections: Short term gainSteroid Injections: Short term gain Viscosupplementation: ControversialViscosupplementation: Controversial

Osteoarthritis
Patient now trips and falls. Presents two Patient now trips and falls. Presents two days later with increased knee pain, days later with increased knee pain, decreased ROM, Pain with all Weight decreased ROM, Pain with all Weight Bearing. On exam, her knee is swollen and Bearing. On exam, her knee is swollen and very tender? What happened?very tender? What happened?

Knee Effusion
Trauma to previously arthritic kneeTrauma to previously arthritic knee Arthropathy-Gout/PseudogoutArthropathy-Gout/Pseudogout ContusionContusion FractureFracture Does she need an x-ray? Does she need an x-ray? Arthrocentesis/Injection-Will make all of Arthrocentesis/Injection-Will make all of
the above (except fracture) betterthe above (except fracture) better

Ottawa Knee Rules-Validated Multiple Times >1000 pts to ED in Canada; 68 had Fracture>1000 pts to ED in Canada; 68 had Fracture Xrays needed if fall/blow to knee and:Xrays needed if fall/blow to knee and:
Age > 55, Isolated Tenderness head of Age > 55, Isolated Tenderness head of fibula or patella, inability to weight bear fibula or patella, inability to weight bear for 4 steps,inability to flex > 90 for 4 steps,inability to flex > 90
100% sens, 49-55 % specific. 100% sens, 49-55 % specific. Does not miss fracture, decrease xray by Does not miss fracture, decrease xray by
25%25%

Osteoarthritis
She did well for several years, then presents She did well for several years, then presents with acute worsening of pain, non with acute worsening of pain, non traumatic. She is unable to weight bear in traumatic. She is unable to weight bear in the office. On exam mod effusion, the office. On exam mod effusion, exquisitely tender on Medial Femoral exquisitely tender on Medial Femoral Condyle, not the joint spaceCondyle, not the joint space
What could be going on?What could be going on?

Avascular Necrosis
Usually > 50, often in setting of OAUsually > 50, often in setting of OA Steroids, Alcoholism, SmokerSteroids, Alcoholism, Smoker X-ray often normal initiallyX-ray often normal initially MRI will show changes before X-rayMRI will show changes before X-ray Non Weight Bearing-can take months to Non Weight Bearing-can take months to
improveimprove If no better -> Hemi or Total ArthroplastyIf no better -> Hemi or Total Arthroplasty


Teaching File Case: Osteonecrosis/Osteochondrosis
Diagnosis: Spontaneous Osteonecrosis of the Medial Femoral Condyle
Findings: Osteochondral abnormality of the
medial femoral condyle.
Pathology: Finding not evident with loss of overlying cartilage on initial radiograph (05/08/01). Osteochondral defect more evident on follow upradiograph (08/08/01) (arrowhead).
Slide 2 of 3
Clinical History: Acute onset of painin knee.

Teaching File Case: Osteonecrosis/Osteochondrosis
Diagnosis: Spontaneous Osteonecrosis of the Medial Femoral Condyle
Findings: Osteochondral abnormality of the medial femoral condyle clearly.
Pathology: Evident on follow upradiograph (08/08/01) (arrowhead).
Slide 3 of 3
Clinical History: Acute knee pain 3 months prior to this radiograph.
