off-pump versus on-pump coronary bypass in high-risk subgroups
TRANSCRIPT

Off-Pump Versus On-Pump Coronary Bypass inHigh-Risk SubgroupsTaro Yokoyama, MD, PhD, Fritz J. Baumgartner, MD, Ali Gheissari, MD,Eli R. Capouya, MD, George P. Panagiotides, MD, and Richard J. Declusin, MDSt. Vincent Medical Center, Los Angeles, Providence St. Joseph Medical Center, Burbank, and St. John’s Regional Medical Center,Oxnard, California
Background. Cardiopulmonary bypass (CPB) haspathophysiologic sequelae that may be more severe inhigh-risk subsets. We wanted to determine whetheroff-pump coronary bypass (OPCAB) could optimizeoutcomes.
Methods. Our database of 242 OPCAB patients under-going complete revascularization was compared to a baseof 483 CABG patients undergoing CPB. Results werecompared for the overall series and in the followinghigh-risk subsets: 80 years of age or older, ventriculardysfunction (ejection fraction (EF) < 0.25), prior neuro-logic event or renal failure, chronic obstructive pulmo-nary disease (COPD), and reoperation.
Results. In the overall series, OPCAB significantlyreduced the incidence of intraoperative transfusion re-quirements and showed a trend toward reduced morbid-ity in terms of postoperative neurologic and renal com-plications, prolonged ventilator requirement greater than3 days, and bleeding requiring reexploration. Mortalitywas less in the OPCAB group (0.4% versus 2.7%, p 5 notsignificant). Similar results were achieved in the follow-
ing high-risk subgroups (n 5 off-pump/on-pump): 80years of age or older (n 5 28/58), EF less than or equal to25% (n 5 13/26), preoperative neurologic event (n 525/36), preoperative renal failure (n 5 27/46), COPD (n 533/43), and reoperation (n 5 28/76). OPCAB decreased theincidence of prolonged ventilation in COPD patients(0/33 [0%] versus 4/43 [9.3%] p 5 not significant) anddecreased the incidence of renal complications in theelderly (1/28 [3.6%] versus 9/58 [15.5%] p 5 not signifi-cant). Off-pump coronary bypass reduced but did noteliminate neurologic events in the elderly (2/28 [7.1%]versus 8/58 [13.8%] p 5 not significant).
Conclusion: Off-pump coronary bypass significantlyreduced the incidence of transfusion requirement com-pared to the CPB counterparts and had a consistent trendin reducing morbidity and mortality overall and in allhigh-risk subsets. Neurologic events are not eliminatedin OPCAB.
(Ann Thorac Surg 2000;70:1546–50)© 2000 by The Society of Thoracic Surgeons
Diffuse systemic inflammatory responses during andafter cardiac surgery are primarily related to car-
diopulmonary bypass [1–3]. These complex inflammatoryresponses are mediated by complement, cytokine, andkininogen/bradykinin pathways and are intimatelylinked to the coagulation cascade and fibrinolysis.
Minimally invasive direct coronary bypass and off-pump coronary bypass (OPCAB) have eliminated onemajor component of aberrant physiology intrinsic toon-pump coronary bypass procedures. Coronary bypass,without the use of cardiopulmonary bypass (CPB) hasbeen shown to reduce the overall systemic inflammatoryresponse, including cytokine-mediated responses [4–6].Furthermore, cardioplegic arrest adds an additional levelof physiologic derangement directly upon the heart, andtroponin I release and myocardial injury are reduced inoff-pump procedures [4, 7]. The implications for specificorgan systems are that elimination of CPB would lead toa more physiologic mileau that would encourage optimalorgan function during and immediately following coro-
nary revascularization. This conceivably might reduceorgan-specific complications, especially in high-risksubgroups.
The present study attempts to evaluate whether thetheoretical advantages from eliminating CPB from coro-nary revascularization are translated into a decreasedmorbidity and complication rate in these patients. Theseries as a whole, as well as specific high-risk subgroups,are compared between off-pump and on-pump groups.
Patients and Methods
Our database of OPCAB patients undergoing completerevascularization without CPB from 1997 to 1999 wascompared to our database of routine coronary arterybypass grafting (CABG) cases utilizing CPB. Variouspreoperative, intraoperative, and postoperative variableswere studied between the groups as a whole as well aswithin various high-risk subgroups. These high-risk sub-
Accepted for publication April 24, 2000.
Address reprint requests to Dr Baumgartner, 2200 W 3rd St, Suite 300, LosAngeles, CA 90057.
This article has been selected for the open discussionforum on the STS Web site:
http://www.sts.org/section/atsdiscussion/
© 2000 by The Society of Thoracic Surgeons 0003-4975/00/$20.00Published by Elsevier Science Inc PII S0003-4975(00)01922-6

groups included profound ventricular dysfunction (ejec-tion fraction # 0.25 as assessed by left ventriculographyor transesophageal echocardiography or both); 80 yearsof age or older; preoperative neurologic event (stroke ortransient ischemic attack), preoperative renal failure (cre-atinine . 2.0 mg/dl and/or dialysis dependence), chronicobstructive pulmonary disease (COPD) as documentedby altered pulmonary function tests or clinical or radio-graphic emphysematous changes; or reoperative coro-nary surgery.
OPCAB was done by full median sternotomy [8] or byleft posterolateral thoracotomy in instances of reopera-tive coronary revascularization to obtuse marginal ves-sels in patients with patent left internal mammary arterygrafts [9]. The OPCAB generally was not done in patientswith extremely small, heavily calcified, or intramyocar-dial targets, or those with massive cardiomegaly. Severeventricular dysfunction was not a contraindication toOPCAB. Standard CABG was done with full cardiopul-monary bypass, tepid cooling, and antegrade and retro-grade cold blood potassium cardioplegia.
As a general rule, indications for intraoperative bloodtransfusion in patients undergoing CPB include a pre-CPB hematocrit less than 32%, hematocrit less than 19%on CPB, or hematocrit less than 26% immediatelypostCPB. In OPCAB, a hematocrit less than 28% duringthe procedure was an indication for transfusion.
Operative and postoperative variables between thegroups that were investigated included use of intraoper-ative blood transfusions, 30 day operative mortality,neurologic complication (stroke, transient ischemic at-tack, or prolonged mental status changes), renal compli-cation (creatinine elevation above 2.0 mg/dL or need forhemodialysis, when these were not preoperativelypresent), prolonged ventilator dependence beyond 3days, postoperative bleeding requiring reexploration,and postoperative critical care unit (CCU) and hospitalstays. Statistical comparisons were done with the Chi-square and Yates correction.
Results
There were 242 consecutive OPCAB patients; 7 caseswere done utilizing a left posterolateral thoracotomy andthe remainder using a full median sternotomy approach.These were compared to 483 standard CABG patients.
Preoperative risk factors were similar between the twogroups. The preoperative incidence of COPD, preopera-tive stroke or transient ischemic attack, and renal insuf-ficiency for the OPCAB versus on-pump groups was 14%versus 9%, 12% versus 8.3%, and 11% versus 9.5%,respectively. The incidence of ejection fraction less thanor equal to 0.25, age 80 years or older, or reoperations forthe OPCAB versus on-pump groups was 5% versus 5%,12% versus 12%, and 12% versus 16%, respectively.Diabetes mellitus and peripheral vascular disease werepresent in 34% versus 29% and 12% versus 15% of theOPCAB versus on-pump groups, respectively. The meanage was 67 years for the OPCAB and 68 years for theon-pump groups.
The overall series 242 OPCAB and 483 on-pump casesis compared in Table 1. The mean number of grafts were3.1 and 4.0 for the off-pump and on-pump groups, re-spectively. OPCAB significantly reduced the number ofpatients requiring intraoperative blood transfusion. Al-though the OPCAB series exhibited a trend of reducedoperative mortality, neurologic and renal complications,prolonged ventilator dependence beyond 3 days, andpostoperative bleeding requiring reexploration, none ofthese variables reached statistical significance. Postoper-ative critical care unit and hospital days were similarbetween the groups, although slightly less in the OPCABgroup.
To determine if the outcome differences between theOPCAB and on-pump groups were more pronounced inhigh-risk subgroups, we separately compared patientswith poor ventricular function, advanced age, preopera-tive neurologic event, COPD, and renal failure betweenthe groups. These data are summarized in Table 2. Novariable, other than the incidence of intraoperative bloodtransfusions, differed with statistical significance be-tween the off-pump versus on-pump groups. Nonethe-less, general trends in reduction in morbidity, mortality,and CCU/postoperative stay between off-pump vs. on-pump groups were apparent in the high-risk subgroups.With the exception of the subset having preoperativeneurologic events, all groups had a statistically signifi-cant decrease in the incidence of intraoperative bloodtransfusion for the OPCAB series. The reoperation sub-group was most pronounced, where only 14% of theOPCAB group required transfusion compared to 58% ofthe on-pump group.
For the COPD subgroup, none of the patients under-going OPCAB had prolonged ventilator requirementsbeyond 3 days, compared with 9.3% of the on-pumpgroup. For the subgroup with preoperative neurologicevents, 12% of OPCAB patients had postoperative neu-rologic complications similar to those on-pump (14%);
Table 1. Comparison of Number of Grafts, Incidence ofIntraoperative Transfusion Requirement, Complications, andCCU/ Postoperative Stay in Off-Pump Versus On-PumpCoronary Artery Bypass Grafting
Off-PumpCoronary
Bypass(n 5 242)
On-Pump(n 5 483)
Mean number of grafts 3.1 4.0Intraoperative transfusion 46 (19%) 218 (45%) p , 0.001Mortality 1 (0.4%) 13 (2.7%) p 5 0.07Neurologic complication 8 (3.3%) 24 (5%)Renal complication 8 (3.3%) 26 (5.4%)Prolonged ventilator need
. 3 days9 (3.7%) 32 (6.6%)
Postoperative bleed 3 (1.2%) 17 (3.5%)Mean CCU postoperative
days1.8 2.3
Mean total postop days 6.2 6.8
CCU 5 critical care unit; postop 5 postoperative.
1547Ann Thorac Surg BAUMGARTNER ET AL2000;70:1546–50 OPCAB IN HIGH-RISK SUBGROUPS
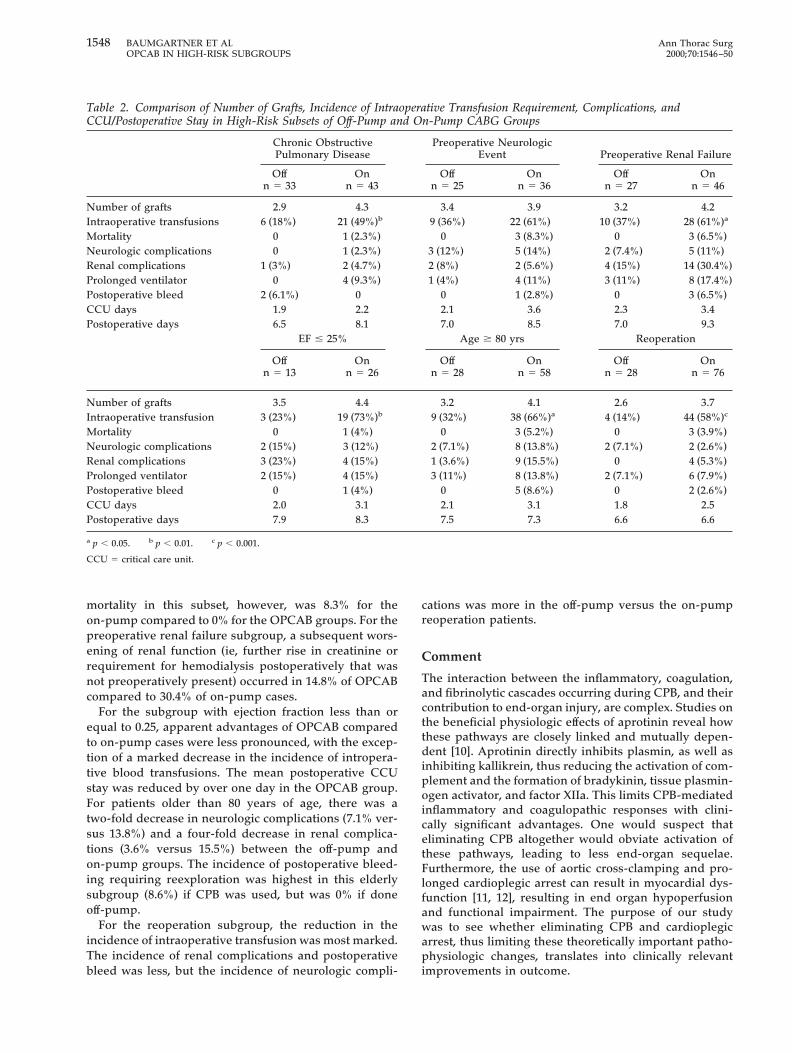
mortality in this subset, however, was 8.3% for theon-pump compared to 0% for the OPCAB groups. For thepreoperative renal failure subgroup, a subsequent wors-ening of renal function (ie, further rise in creatinine orrequirement for hemodialysis postoperatively that wasnot preoperatively present) occurred in 14.8% of OPCABcompared to 30.4% of on-pump cases.
For the subgroup with ejection fraction less than orequal to 0.25, apparent advantages of OPCAB comparedto on-pump cases were less pronounced, with the excep-tion of a marked decrease in the incidence of intropera-tive blood transfusions. The mean postoperative CCUstay was reduced by over one day in the OPCAB group.For patients older than 80 years of age, there was atwo-fold decrease in neurologic complications (7.1% ver-sus 13.8%) and a four-fold decrease in renal complica-tions (3.6% versus 15.5%) between the off-pump andon-pump groups. The incidence of postoperative bleed-ing requiring reexploration was highest in this elderlysubgroup (8.6%) if CPB was used, but was 0% if doneoff-pump.
For the reoperation subgroup, the reduction in theincidence of intraoperative transfusion was most marked.The incidence of renal complications and postoperativebleed was less, but the incidence of neurologic compli-
cations was more in the off-pump versus the on-pumpreoperation patients.
Comment
The interaction between the inflammatory, coagulation,and fibrinolytic cascades occurring during CPB, and theircontribution to end-organ injury, are complex. Studies onthe beneficial physiologic effects of aprotinin reveal howthese pathways are closely linked and mutually depen-dent [10]. Aprotinin directly inhibits plasmin, as well asinhibiting kallikrein, thus reducing the activation of com-plement and the formation of bradykinin, tissue plasmin-ogen activator, and factor XIIa. This limits CPB-mediatedinflammatory and coagulopathic responses with clini-cally significant advantages. One would suspect thateliminating CPB altogether would obviate activation ofthese pathways, leading to less end-organ sequelae.Furthermore, the use of aortic cross-clamping and pro-longed cardioplegic arrest can result in myocardial dys-function [11, 12], resulting in end organ hypoperfusionand functional impairment. The purpose of our studywas to see whether eliminating CPB and cardioplegicarrest, thus limiting these theoretically important patho-physiologic changes, translates into clinically relevantimprovements in outcome.
Table 2. Comparison of Number of Grafts, Incidence of Intraoperative Transfusion Requirement, Complications, andCCU/Postoperative Stay in High-Risk Subsets of Off-Pump and On-Pump CABG Groups
Chronic ObstructivePulmonary Disease
Preoperative NeurologicEvent Preoperative Renal Failure
Offn 5 33
Onn 5 43
Offn 5 25
Onn 5 36
Offn 5 27
Onn 5 46
Number of grafts 2.9 4.3 3.4 3.9 3.2 4.2Intraoperative transfusions 6 (18%) 21 (49%)b 9 (36%) 22 (61%) 10 (37%) 28 (61%)a
Mortality 0 1 (2.3%) 0 3 (8.3%) 0 3 (6.5%)Neurologic complications 0 1 (2.3%) 3 (12%) 5 (14%) 2 (7.4%) 5 (11%)Renal complications 1 (3%) 2 (4.7%) 2 (8%) 2 (5.6%) 4 (15%) 14 (30.4%)Prolonged ventilator 0 4 (9.3%) 1 (4%) 4 (11%) 3 (11%) 8 (17.4%)Postoperative bleed 2 (6.1%) 0 0 1 (2.8%) 0 3 (6.5%)CCU days 1.9 2.2 2.1 3.6 2.3 3.4Postoperative days 6.5 8.1 7.0 8.5 7.0 9.3
EF # 25% Age $ 80 yrs Reoperation
Offn 5 13
Onn 5 26
Offn 5 28
Onn 5 58
Offn 5 28
Onn 5 76
Number of grafts 3.5 4.4 3.2 4.1 2.6 3.7Intraoperative transfusion 3 (23%) 19 (73%)b 9 (32%) 38 (66%)a 4 (14%) 44 (58%)c
Mortality 0 1 (4%) 0 3 (5.2%) 0 3 (3.9%)Neurologic complications 2 (15%) 3 (12%) 2 (7.1%) 8 (13.8%) 2 (7.1%) 2 (2.6%)Renal complications 3 (23%) 4 (15%) 1 (3.6%) 9 (15.5%) 0 4 (5.3%)Prolonged ventilator 2 (15%) 4 (15%) 3 (11%) 8 (13.8%) 2 (7.1%) 6 (7.9%)Postoperative bleed 0 1 (4%) 0 5 (8.6%) 0 2 (2.6%)CCU days 2.0 3.1 2.1 3.1 1.8 2.5Postoperative days 7.9 8.3 7.5 7.3 6.6 6.6
a p , 0.05. b p , 0.01. c p , 0.001.
CCU 5 critical care unit.
1548 BAUMGARTNER ET AL Ann Thorac SurgOPCAB IN HIGH-RISK SUBGROUPS 2000;70:1546–50

Of the variables studied in the overall series, OPCABsignificantly affected only the incidence of intraoperativetransfusion, although an improved OPCAB mortality rateapproached statistical significance. Neurologic, renal, co-agulopathic, and prolonged ventilator complicationswere all reduced in the OPCAB group, and although theresults were not statistically significant, the trends wereconsistent.
It is reasonable to suspect that patients at highest riskfor undergoing CPB and cardioplegic arrest, includingthose with advanced age, ventricular dysfunction, stroke,COPD, renal failure, or prior CABG, would be preciselythose patients in whom OPCAB would likely have themost beneficial impact. Looking at these various high-risk subgroups, the only variable that was found to yielda statistically significant difference between on-pumpand off-pump groups was intraoperative transfusion re-quirement. This reduced incidence of transfusion re-quirement in OPCAB is likely related to inflammatoryand coagulopathic sequelae intrinsic to CPB, as well asthe hemodilution effect of the pump priming fluid.
No patient with COPD who underwent OPCAB re-quired prolonged mechanical ventilation, compared to9.3% of standard CABG patients, likely related to fluidshifts and damaging inflammatory effects inflicted byCPB on an already compromised lung. Interestingly, allother high risk subgroups who underwent OPCAB hadsome patients requiring prolonged ventilator support(although still generally less than the on-pump groups).The reason COPD patients undergoing OPCAB had theleast incidence of prolonged ventilatory requirementscompared to other high-risk subgroups is unclear, butmay be related to a greater preoperative awareness andinitiation of pulmonary treatment protocols.
Adverse cerebral outcomes after coronary bypass sur-gery increase dramatically in elderly populations, andwere believed to be largely due to CPB and aorticmanipulation [13]. Cognitive changes after CABG, how-ever, appear to be a much more multifactorial problemassociated with medical as well as surgical variables [14].These variables include the nonspecific effects that anes-thesia and any prolonged surgery with or without CPBhave on the cognitive status of elderly patients in general.In our series, 5% of all patients undergoing standardCABG sustained a neurologic complication, but of thepatients 80 years of age or older, 13.8% sustained aneurologic complication, approximating the findings ofRoach and colleagues [13]. In our OPCAB patients, therewas an overall 3.3% incidence of neurologic complica-tions, but of the OPCAB patients 80 years of age or older,there was a 7.1% incidence. Elimination of CPB seemedto reduce the incidence of neurologic complications,particularly in the elderly population, but certainly didnot eliminate neurologic complications. Furthermore, inpatients who had preoperative strokes or transient isch-emic attacks, OPCAB and standard CPB did not substan-tially differ in our series in the relatively high incidence ofpostoperative neurologic complications (12% to 14%).
In the preoperative renal insufficiency subgroup,OPCAB decreased the incidence of further renal deteri-
oration. A recent prospective randomized study showedthat glomerular filtration (creatinine clearance) and renaltubular function were significantly improved in off-pumpcompared to on-pump CABG [14]. The authors con-cluded that OPCAB offered superior renal protectioncompared to standard CABG.
OPCAB has been shown to reduce myocardial injuryand troponin I release compared to standard CABG withcardioplegic arrest [4, 7]. This could presumably translateinto improved clinical results, particularly for the mostseverely compromised ventricles. In our subgroup ofpatients with profoundly impaired ventricles with ejec-tion fraction less than or equal to 0.25, early postoperativeventricular function was not routinely evaluated by echo-cardiography or ventriculography. Besides the reductionin transfusion requirements, no obvious differences be-tween the off-pump and on-pump groups were readilyapparent. There was a higher incidence of renal compli-cations in the OPCAB group, but this was likely relatedmore to intrinsic patient factors than to merits of stan-dard CPB.
A point worth mentioning is that all our patients,despite their profound ventricular dysfunction, were inNew York Heart Association functional classes I and II atthe time of surgery. This likely contributed to the simi-larly low morbidities and mortalities for both on-pumpand off-pump groups. More pronounced differences be-tween the groups would have probably been found if thepatients had undergone emergency surgery while inheart failure.
Patients of advanced age of 80 years or older are in ahigh-risk subgroup that would be expected to benefitsubstantially from eliminating CPB. As mentioned above,neurologic complications were reduced in the OPCABgroup. Furthermore, renal complications, postoperativebleeding, and mortality were also all reduced in theOPCAB group. The individual organ systems of patientswith advanced age seem to be particularly at risk for thepathophysiologic sequelae of CPB.
Reoperations exhibited a marked difference in theincidence of intraoperative blood transfusions forOPCAB. This is a reasonable prediction considering thedissection necessary to clear adhesions and CPB-mediated activation of inflammatory and coagulopathiccascades on raw surfaces.
In all these high-risk subgroups, there were no opera-tive mortalities for OPCAB, with mortalities for CPBgroups ranging from 2.3% to 8.3%. With few exceptions,OPCAB reduced the incidence for every complicationstudied when compared to on-pump groups, as well asreducing postoperative CCU and hospital stays. Whilenot statistically significant, the trends were nonethelessconsistent.
We conclude that eliminating CPB in coronary revas-cularization reduces the incidence of intraoperativeblood transfusion requirements. Our study further sup-ports the provocative possibility that obviating the needfor CPB and cardioplegic arrest may improve clinicaloutcomes, particularly in some high-risk groups such asthe elderly and those with specific organ dysfunction.
1549Ann Thorac Surg BAUMGARTNER ET AL2000;70:1546–50 OPCAB IN HIGH-RISK SUBGROUPS

Anatomic factors, however, including cardiomegaly andsmall, intramyocardial, or heavily calcified vessels re-quiring endarterectomy may preclude OPCAB in someinstances. Refinements in routine on-pump CABG havereduced morbidity and mortality rates to the point thatsubtle differences in clinical outcomes would only beexpected to manifest statistical significance in a largeseries. Nonetheless, the physiologic rationale for avoid-ing or limiting CPB and cardioplegic arrest remainssound, particularly for at-risk patient populations.
References
1. Cremer J, Martin M, Redl H, et al. Systemic inflammatoryresponse syndrome after cardiac operations. Ann ThoracSurg 1996;61:1714–20.
2. Wan S, LeClerc JL, Vincent JL. Inflammatory response tocardiopulmonary bypass: mechanisms involved and possi-ble therapeutic strategies. Chest 1997;697–2.
3. Myles PS, Olenikou I, Bujor MA, Davis BB. ACE-inhibitors,calcium antagonists and low systemic vascular resistancefollowing cardiopulmonary bypass. A case-control study.Med J Aust 1993;158:675–7.
4. Wan S, Izzat MB, Lee TW, Wan IYP, Tang NLS, Yim APC.Avoiding cardiopulmonary bypass in multivessel CABGreduces cytokine response and myocardial injury. Ann Tho-rac Surg 1999;68:52–7.
5. Struber M, Cremer JT, Gohrbandt B, et al. Human cytokineresponses to coronary artery bypass grafting with and with-out cardiopulmonary bypass. Ann Thorac Surg 1999;68:1330–5.
6. Gu YJ, Mariani MA, van Oeveren W, Grandjean JG, Boon-stra PW. Reduction of the inflammatory response in patientsundergoing minimally invasive coronary artery bypassgrafting. Ann Thorac Surg 1998;65:420–4.
7. Biridi I, Caputo M, Hutter JA, Bryan AJ, Angelini GD.Troponin I release during minimally invasive coronary sur-gery. J Thorac Cardiovasc Surg 1997;114:509–10.
8. Baumgartner FJ, Gheissari A, Capouya ER, Panagiotides GP,Katouzian A, Yokoyama T. Technical aspects of total revas-cularization in off-pump coronary bypass via sternotomyapproach. Ann Thorac Surg 1999;67:1653–8.
9. Baumgartner FJ, Gheissari A, Panagiotides GP, Capouya ER,Declusin RJ, Yokoyama T. Off-pump obtuse marginal graft-ing with local stabilization: thoracotomy approach in reop-erations. Ann Thorac Surg 1999;68:946–8.
10. Mohammad MHK, Gikakis N, Miyamoto S, et al. Aprotinininhibits thrombin formation and monocyte tissue factor insimulated cardiopulmonary bypass. Ann Thorac Surg 1999;68:473–8.
11. Buckberg GD. Update on current techniques of myocardialprotection. Ann Thorac Surg 1995;60:805–14.
12. Ascione R, Lloyd CT, Gomes WJ, Caputo M, Bryan AJ,Angelini GD. Coronary revascularization with or withoutcardiopulmonary bypass: evaluation of myocardial functionin a prospective randomised study. Eur J Cardiothorac Surg1999;15:685–90.
13. Roach GW, Kanchuger M, Mangano CM, et al. Adversecerebral outcomes after coronary artery bypass surgery.N Engl J Med 1996;335:1857–63.
14. Ascione R, Lloyd CT, Underwood MJ, Gomes WJ, AngeliniGD. On-pump versus off-pump coronary revascularization:evaluation of renal function. Ann Thorac Surg 1999;68:493–8.
1550 BAUMGARTNER ET AL Ann Thorac SurgOPCAB IN HIGH-RISK SUBGROUPS 2000;70:1546–50