oct 25 caphc concurrent symposium - sleep disorders - dr. penny corkum and dr. shelly weiss
TRANSCRIPT

2016 CAPHC Annual Conference
October 23-25, 2016
Halifax, NS
Sleep Disorders in Canadian Children:
What Can We Do to Ensure Better Nights and Better
Days for Children and their Families?
Penny Corkum, PhD, Registered Psychologist
Professor, Department of Psychology & Neuroscience; Psychiatry
Dalhousie University
IWK Scientific Staff; CEH ADHD Clinic
Shelly Weiss, MD FRCPC, Pediatric Neurologist
Professor, Faculty of Medicine,
Hospital for Sick Children, University of Toronto
1

Outline
Introductions & Objectives
Xavier’s story
Importance of sleep
Access to services in Canada
Barriers to care
Guidelines for pediatric sleep
Service delivery models
Introduction to Better Nights, Better Days
Discussion/Questions
2

Main Goal for Workshop
Determine how we can all work together (as
administrators, policy makers, researchers,
clinicians, and families) to improve paediatric
sleep assessment and treatment in Canada so that
there is access to services for all in need, no matter
where they live
3

Importance of Sleep

Causes of Sleep
Disorders/Problems
Prevalence
25% of typically developing children
≥ 80% of children with physical and
mental health disorders
Causes
Sleep disorders
Lifestyle factors
5

Classification
DSM-5 (2013) / ICSD-3 (2013)
10 different sleep disorders/sleep disorder groupings
1) Insomnia Disorder
2) Hypersomnolence Disorder
3) Narcolepsy
4) Breathing-related sleep disorders
5) Circadian rhythm sleep-wake disorders
6) Non–rapid eye movement (NREM) sleep arousal disorders
7) Nightmare disorder
8) Rapid eye movement (REM) sleep behavior disorder
9) Restless legs syndrome
10) Substance/medication-induced sleep disorder
6

Insomnia
Most common sleep disorder in TD children and children with mental health and physical health disorders
Criteria
Reports of difficulties falling asleep, staying asleep, and/or early waking
Daytime consequences of sleep problem
Adequate opportunity for sleeping
Frequent (≥3x/wk) and chronic (≥3 mos)
Not explained by another sleep-wake disorder, medical condition or mental health disorder
7

Lifestyle Factors
People of all ages are sleeping less now than ever before
Sleeping about 1 hour less now than at the beginning of
the century
Reasons…
Electronics
Sleep not seen as a priority
Extra-curricular activities
Social activity
School start times
Results in a Social Jet Lag & Sleep Debt
8

Factors Affecting Sleep in Children
Sleep
Genetics
Sleep Environ-
ment
Family/ Parents
Health
Develop-ment
Social –Emotional
Social –Cultural
Sleep Practices
Slide courtesy of Jodi Mindell
9

Chronicity of Sleep Disorders
Transient and persistent sleep problems
Genetics may play the largest role in stability of
sleep problems
Stability depends in part on the type of sleep
problem and the treatment provided
Even when a sleep problem does not persist it
predict later behavioral/mental health problems
10

Cognition/
Learning
Mental
Health
Physical
Health
Quality
of Life
Consequences of Sleep Disorders 11

Consequences of Sleep Disorders
Community
School
Family
Child
12

Importance
Sleep problems could put individuals at risk for mental
health or physical health disorders
Sleep problems could mimic mental health disorders and as
such need to be considered as a differential diagnosis
Sleep problems could exacerbate mental health
problems/increase symptoms severity and chronicity
Treatment of sleep problems may reduce impairment and
may even act as an enhancement therapy (e.g. make other
therapies more effective)
The treatment of mental health problems with medication
may increase sleep problems
13

How could poor sleep in
children affect your
service?
14

Access to Services
in Canada
Facts about the gaps in
Canadian resources for sleep
Despite high prevalence of sleep
disorders/problems, chronicity, and significant
impact, they are often unrecognized and under
treated by clinicians
Main Reasons
Limited awareness and knowledge of the importance
of sleep
Limited skills in this area for health care providers
Limited access to services and resources/tools
16
Access to services to diagnose
Obstructive Sleep Apnea in
Canadian children
What is the gold standard for diagnosis?
Where are the sleep clinics?
Where are the pediatric sleep practitioners?
17

PSG is gold standard to
diagnose OSA
18

Canadian Sleep Society Clinic Map
www.css-scs.ca
19

Western Canada 20

Eastern Canada21

22

Pediatric sleep resources for
OSA in Canada
Survey study of pediatric sleep practitioners and sleep
laboratories
Results
No sleep practitioners (for OSA) or PSG available in
Yukon, NWT, Nunavut, Saskatchewan, Nova Scotia, New
Brunswick, PEI, NFLD/Labrador
Wait time for PSG varied from < 1 months to 1.5-2 years
Lack of resources and services for pediatric sleep
disordered breathing has great geographical disparity
23

24

Service Providers
CSS listing for sleep clinics, insomnia treatment providers, dentists (searchable by province)
https://css-scs.ca/resources/types-of-providers
Diagnosis
Physicians
Psychologists
Treatment
Physicians
Psychologists and other allied health professionals
Dentists
Sleep Consultants
http://goodnightsleepsite.com/toronto/
Others (e.g., naturopath, chiropractor)
Main concern – Lack of regulation of field and some service providers!
25

Barriers to Care

Limited awareness and
knowledge of the importance of
sleep
27

28

29

30

Methods
124 Canadian health care providers were surveyed
about barriers and facilitators
Included: physicians, nurse, psychologist, social
workers
31

32

33

New RCPSC initiative in sleep
education
Currently no route to certification for subspecialist physicians who practice sleep medicine in Canada
As of July 2016, there will be a AFC (Area of Focused Competence/Diploma) in sleep medicine
1 year – include ongoing maintenance of certification
Eligible for physicians who are specialists in : ENT, respirology, psychiatry, neurology, developmental pediatrics
34

Guidelines for
Pediatric Sleep
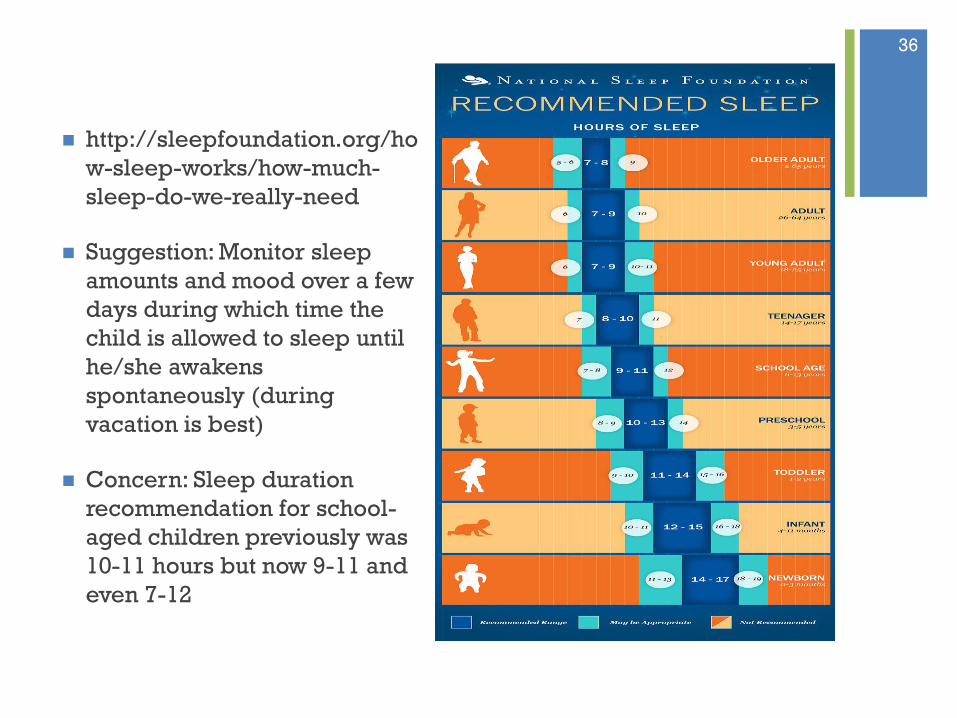
http://sleepfoundation.org/ho
w-sleep-works/how-much-
sleep-do-we-really-need
Suggestion: Monitor sleep
amounts and mood over a few
days during which time the
child is allowed to sleep until
he/she awakens
spontaneously (during
vacation is best)
Concern: Sleep duration
recommendation for school-
aged children previously was
10-11 hours but now 9-11 and
even 7-12
36

Participation 2016 Report Card37

38

Recommended hours of sleep
Age 5-13 years: 9-11 hours
Age 14-17 years: 8-10 hours
39

• Healthy sleep is the goal for all infants, children and adolescents
• Guidelines to evaluation and treatment of sleep disorders
• Position statement endorsed by College of Family Physicians, Canadian Psychiatry Association and Canadian Sleep Society
• Endorsement by Canadian Pediatric Society (pending)
Published Jn Can Acad Child and Adol Psychiatry, Vol 23 (3), 2014
40

41

What do you see as the
main barriers to sleep
services in your
communities?
42

Service Delivery Models

Current Service Delivery
Large differences between provinces and regions
(urban/rural)
Focus on obstructive sleep apnea
Use of medications that do not have efficacy data to
support their use in children
Limited access to behavioural treatments
44

Measurement of Sleep
PSG ActigraphySleep Diary
Questionnaires
Interviews
Objective Subjective
45

Best Practices – Assessment
• PSG/MLST
• Actigraphy/ Videography
• Interviews/ Sleep Diaries
• Screening/ Questionnaires
46
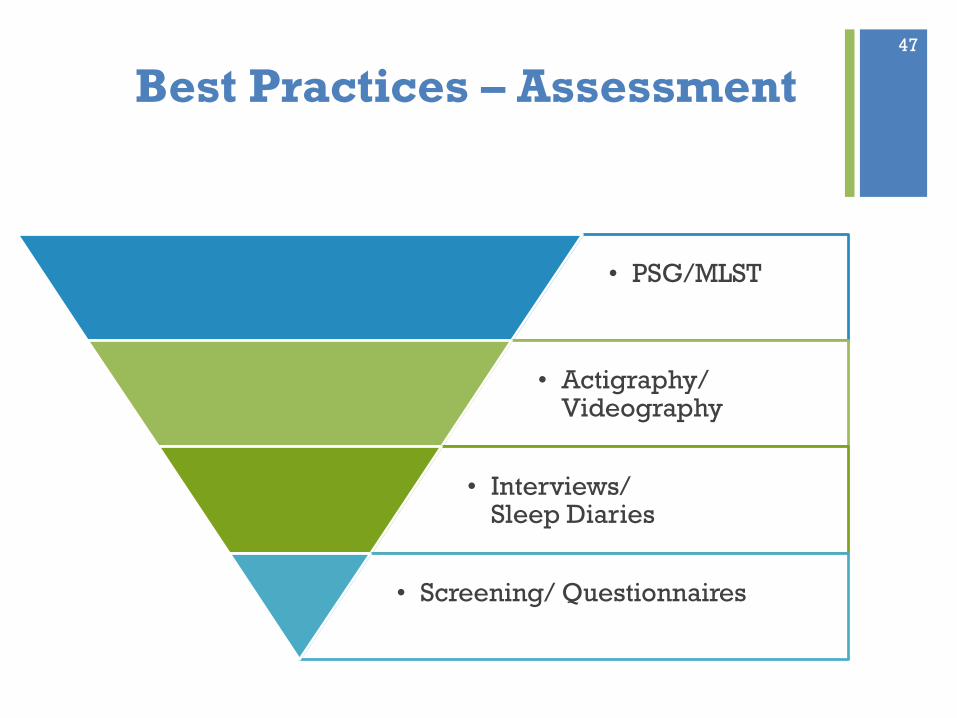
Best Practices – Assessment
• PSG/MLST
• Actigraphy/ Videography
• Interviews/ Sleep Diaries
• Screening/ Questionnaires
47

Best Practices –Treatment
• Medication
• Specific behavioural sleep interventions
• Implement healthy sleep practices
• Psycho-education
48

Best Practices –Treatment
• Medication
• Specific behavioural sleep interventions
• Implement healthy sleep practices
• Psycho-education
49

Suggested Model: Stepped Care
Individualized intervention provided by sleep medicine
specialist
Individualized intervention by highly trained health professional
(non-sleep specialist)
Manualized in-person individual or group intervention provided by trained health
professional (non-sleep specialist)
Self (parent) administered interventions with human support (non-specialist)
Self (parent) administered interventions (no direct human support) BNBD-TD / BNBD-NDD
Public education/ prevention/ screening
*adapted from Espie, C.A. (2009). “Stepped Care”: A health technology solution for delivering cognitive behavioral therapy as a first line insomnia treatment. Sleep, 32(12), 1549-1558.
50

Introduction to
Better Nights,
Better Days

52
http://betternightsbetterdays.ca/
http://ndd.betternightsbetterdays.ca/

Session 1: Sleep Information
Session 2: Healthy Sleep Practices
Session 3: Settling to Sleep
Session 4: Going Back to Sleep
Session 5: Looking Ahead
Z
ZZZ
BNBD Intervention Program
53

Program Tools and Supports
Daily online Sleep Diary
allows participants to track their
results and see patterns in their
child’s sleep and behaviour Sleep Diary
Weekly
Activities
and Reviews
Track Your
Progress
Participants receive feedback on their
progress
Activities help participants
make positive changes to their
child’s sleep
• Learn how to create sleep
routines, a healthy sleep
environment, and practice
techniques to reduce stress
54

BNBD-TD
Randomized Control Trial
Goal: 500 participants
55

Who Can
Participate
http://betternightsbetterdays.ca/
56

Steps to Study ParticipationWebsite Self-Screen
Screening
Eligibility Assessment
Baseline
Randomization
Better
Nights,
Better Days
Intervention
Usual Care
4 Month Follow-Up
8 Month Follow-Up
Study End 57

Recruitment and Enrollment Update
• As of Oct 21, 2016, we have had:– 852 parents express interest in the study– 503 consent to screening– 293 consent to participate in the study– 204 deemed eligible– 196 start baseline
• Recruiting 400 English-speaking parents/guardians from 4 Canadian regions (Atlantic, Central, Prairies, West Coast/Northern) – 100 parents per region– Atlantic Canada region has met quota and is not closed
• Recruiting 100 French speaking parents across Canada (Winter 2017)
58

Discussion/
Questions

How to improve awareness and knowledge of the
importance of sleep?
How to train health care providers in sleep assessment
and treatment?
How to increase equitable accesses to services and
resources?
How to work together to to improve paediatric sleep
assessment and treatment in Canada so that there is
access to services for all in need, no matter where they
live?
What would you need to make a stepped care model
for pediatric sleep work in your service?60

Thank you
Web Resources
Canadian Sleep Society http://www.css.to/
National Sleep Foundation http://www.sleepfoundation
.org
Star Sleeper http://www.professorgarfiel
d.org/pgf_StarSleeper.html
Insomnia Rounds http://www.insomniarounds
.ca
61
http://myweb.dal.ca/pvcorkum/