normal pressure hydrocephalus - web.brrh.comweb.brrh.com/msl/practical neuroscience for the...
TRANSCRIPT
Normal Pressure Hydrocephalus
Jonathan Oren Harris MD
Frank D Vrionis MD
Disclosures
• Bocacare employee
Objectives
• Understand
– What NPH is
– How does NPH present
– How is NPH diagnosed
– Treatment of NPH
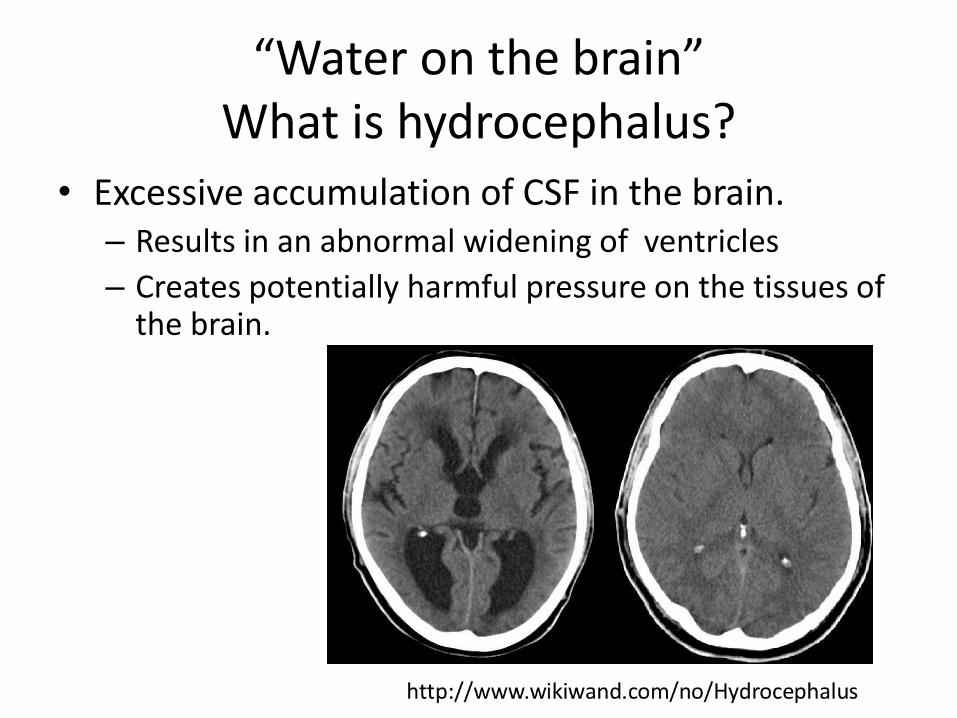
“Water on the brain” What is hydrocephalus?
• Excessive accumulation of CSF in the brain. – Results in an abnormal widening of ventricles
– Creates potentially harmful pressure on the tissues of the brain.
“Water on the brain” What is hydrocephalus?
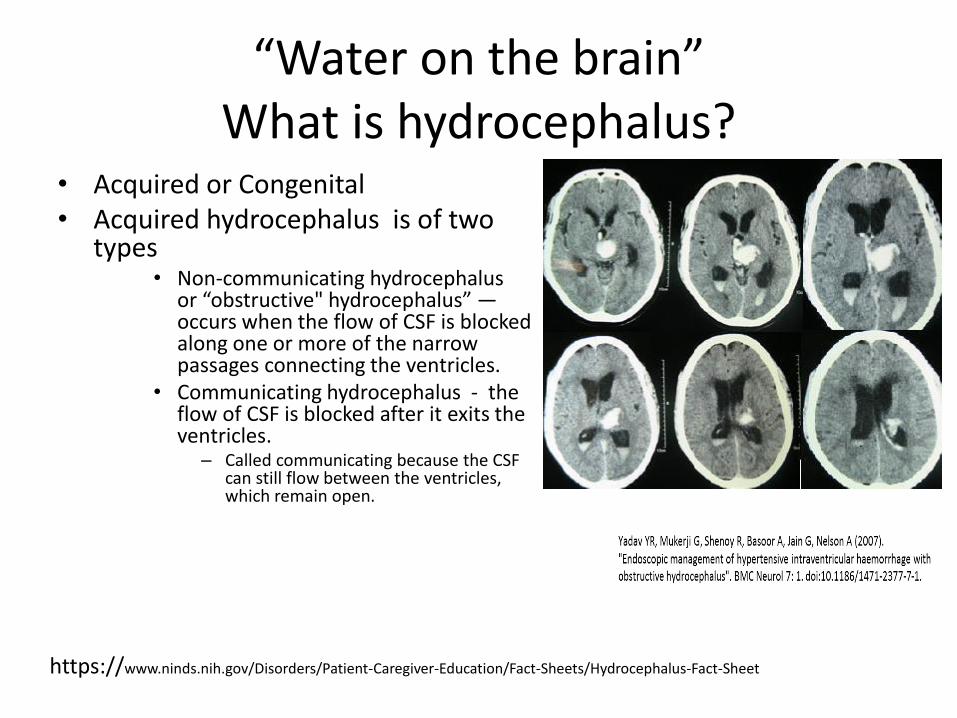
• Acquired or Congenital • Acquired hydrocephalus is of two
types • Non-communicating hydrocephalus
or “obstructive" hydrocephalus” — occurs when the flow of CSF is blocked along one or more of the narrow passages connecting the ventricles.
• Communicating hydrocephalus - the flow of CSF is blocked after it exits the ventricles.
– Called communicating because the CSF can still flow between the ventricles, which remain open.
https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Hydrocephalus-Fact-Sheet
Communicating hydrocephalus
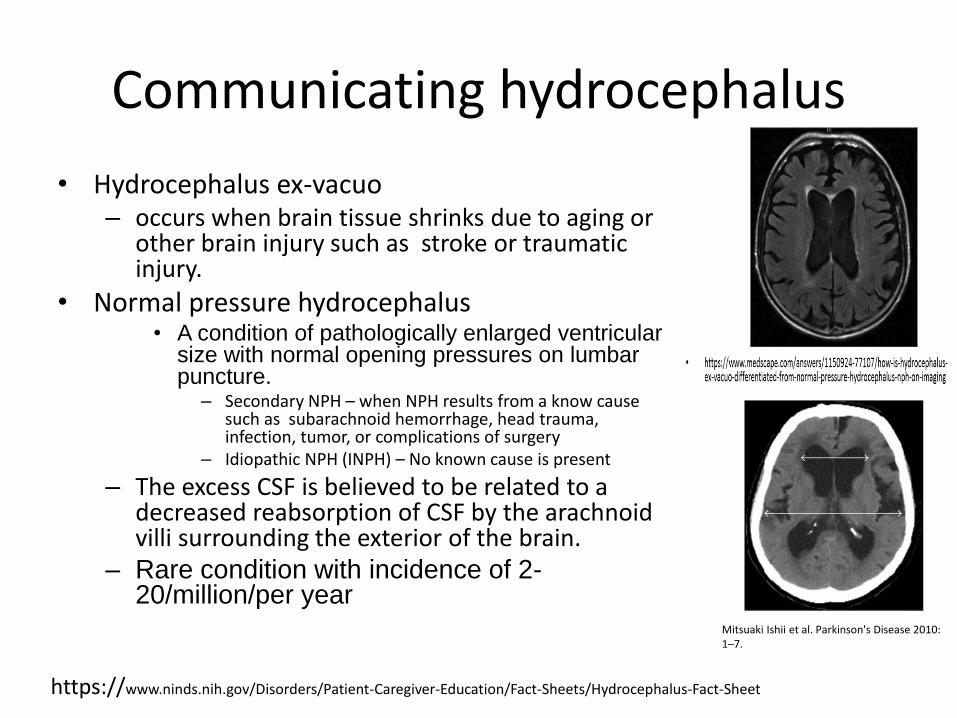
• Hydrocephalus ex-vacuo – occurs when brain tissue shrinks due to aging or
other brain injury such as stroke or traumatic injury.
• Normal pressure hydrocephalus • A condition of pathologically enlarged ventricular
size with normal opening pressures on lumbar puncture.
– Secondary NPH – when NPH results from a know cause such as subarachnoid hemorrhage, head trauma, infection, tumor, or complications of surgery
– Idiopathic NPH (INPH) – No known cause is present
– The excess CSF is believed to be related to a decreased reabsorption of CSF by the arachnoid villi surrounding the exterior of the brain.
– Rare condition with incidence of 2-20/million/per year
https://www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Hydrocephalus-Fact-Sheet
Mitsuaki Ishii et al. Parkinson's Disease 2010: 1–7.
Clinical signs of NPH
• Classic triad – Gait instability, urinary incontinence and dementia
• All three components need not be present for the diagnosis of INPH to be made.
• Is most commonly a gait disturbance followed in frequency by cognitive impairment and less frequently urinary incontinence – Cognitive disturbances do not occur in all patients, and the severity of
cognitive and motor symptoms does not necessarily correlate at baseline or progress in parallel.
– Incontinence in INPH is difficult to distinguish from urinary symptoms associated with other common disorders
• Should be considered in the differential diagnosis of any unexplained disturbance of gait, cognition, or continence that begins insidiously in an adult.
Neurosurgery 57 (NUMBER 3) | SEPTEMBER 2005 SUPPLEMENT
Clinical signs of NPH
• Gait features – Described as “apractic,” “bradykinetic,” “glue-footed,” “magnetic,”
“parkinsonian,” “short-stepped,” and “shuffling.” – Difficulty in ascending or descending stairs and curbs and in walking at the
expected pace. – Difficulty rising from a chair, – As the disease progresses, turning in place requires multiple steps (en bloc).
• Cognitive symptoms – Subcortical dementing process, including slowing of thought, inattentiveness,
and apathy, as well as encoding and recall problems
• Urinary symptoms – Incontinence – Urgency – Frequency – Nocturia
Neurosurgery 57 (NUMBER 3) | SEPTEMBER 2005 SUPPLEMENT
Gait Video
Diagnosis
• The diagnosis is based on clinical history, examination, and brain imaging
• Imaging – The hallmark finding on CT or MRI is ventriculomegaly
in the absence of, or out of proportion to, sulcal enlargement, with no evidence of obstruction at the level of the third or fourth ventricles.
• Additional tests may improve diagnostic confidence, promote differential diagnosis, or assist in prognosticating about response to shunt placement.
Neurosurgery 57 (NUMBER 3) | SEPTEMBER 2005 SUPPLEMENT
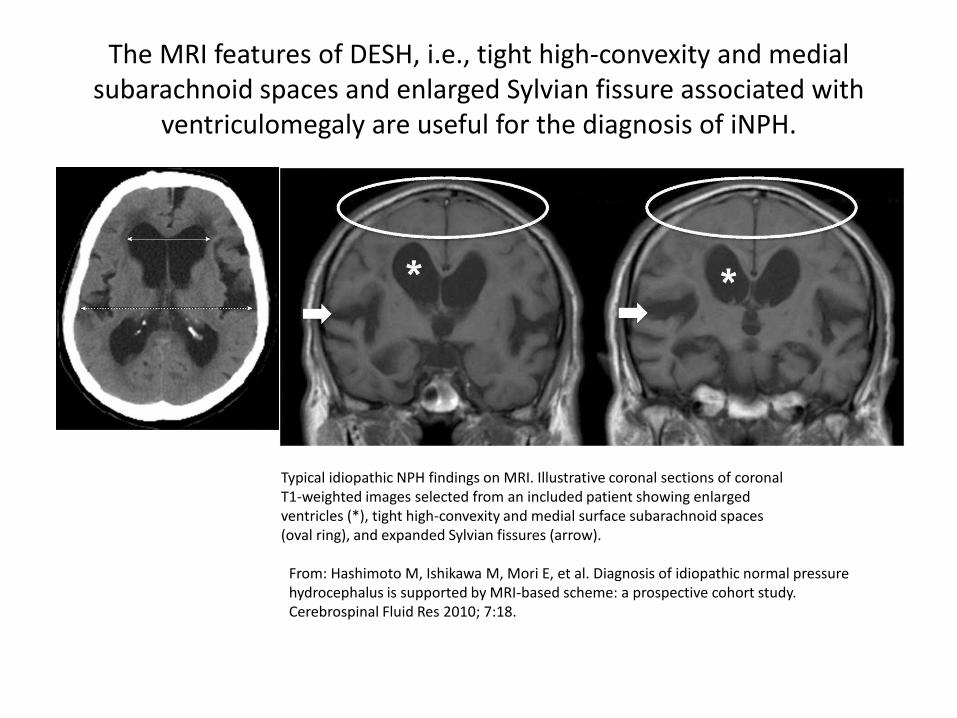
The MRI features of DESH, i.e., tight high-convexity and medial subarachnoid spaces and enlarged Sylvian fissure associated with
ventriculomegaly are useful for the diagnosis of iNPH.
Typical idiopathic NPH findings on MRI. Illustrative coronal sections of coronal T1-weighted images selected from an included patient showing enlarged ventricles (*), tight high-convexity and medial surface subarachnoid spaces (oval ring), and expanded Sylvian fissures (arrow).
From: Hashimoto M, Ishikawa M, Mori E, et al. Diagnosis of idiopathic normal pressure hydrocephalus is supported by MRI-based scheme: a prospective cohort study. Cerebrospinal Fluid Res 2010; 7:18.
THE VALUE OF SUPPLEMENTAL PROGNOSTIC TESTS
• Radionuclide cisternography does not improve the diagnostic accuracy of identifying shunt responsive INPH
• Symtomatic improvement after lumbar puncture and drainge of 40- to 50-ml of CSF improves the certainty for a favorable response to shunt placement than can be obtained by clinical examination. – However, the tap test cannot be used as an exclusionary test because
of its low sensitivity (26–61%).
• Determination of the CSF outflow resistance via an infusion test carries a higher sensitivity (57–100%) compared with the tap test and a similar positive predictive value of 75 to 92%.
• Prolonged external lumbar drainage in excess of 300 ml is associated with high sensitivity (50–100%) and high positive predictive value (80–100%).
Neurosurgery VOLUME 57 | NUMBER 3 | SEPTEMBER 2005 SUPPLEMENT | S2-17
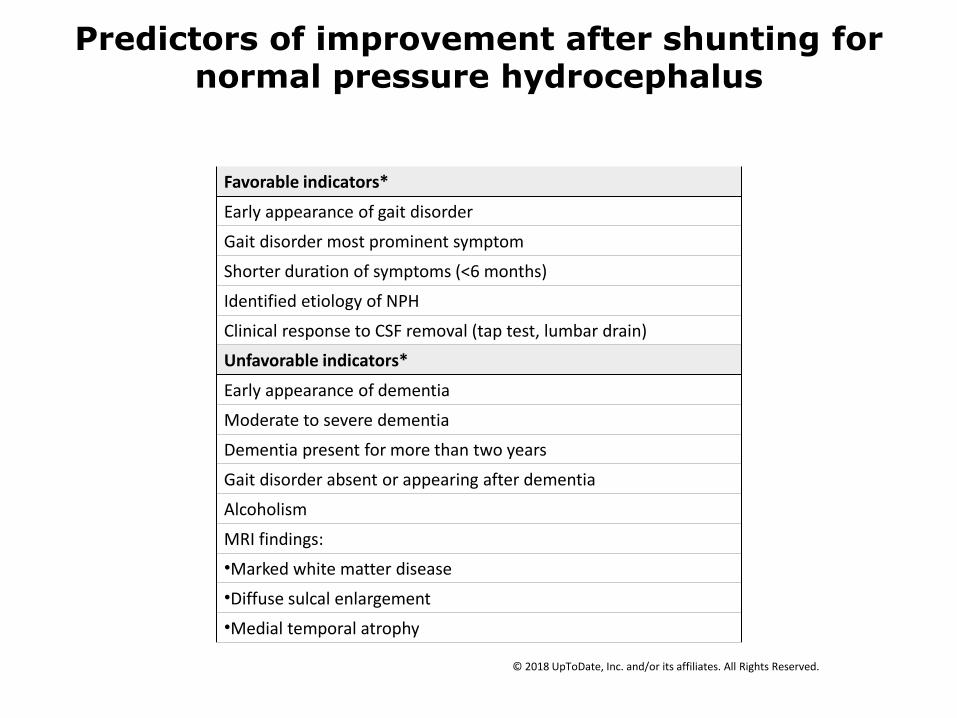
Predictors of improvement after shunting for normal pressure hydrocephalus
Favorable indicators*
Early appearance of gait disorder
Gait disorder most prominent symptom
Shorter duration of symptoms (<6 months)
Identified etiology of NPH
Clinical response to CSF removal (tap test, lumbar drain)
Unfavorable indicators*
Early appearance of dementia
Moderate to severe dementia
Dementia present for more than two years
Gait disorder absent or appearing after dementia
Alcoholism
MRI findings:
•Marked white matter disease
•Diffuse sulcal enlargement
•Medial temporal atrophy
© 2018 UpToDate, Inc. and/or its affiliates. All Rights Reserved.