non-scaly plaques
DESCRIPTION
Group 2 Sy A, Sy J, Sydiongco, Tacata, Tady, Tamondong, Tan E, Tan G, Tan M, Tan S. NON-SCALY PLAQUES. SY, Aaron Keefe S. FIXED DRUG ERUPTION. FIXED DRUG ERUPTION. recur at the same site with each exposure to medications Six or fewer lesions occur, frequently one - PowerPoint PPT PresentationTRANSCRIPT

NON-SCALY PLAQUESGroup 2Sy A, Sy J, Sydiongco, Tacata, Tady, Tamondong, Tan E, Tan G, Tan M, Tan S

FIXED DRUG ERUPTION
SY, Aaron Keefe S.

FIXED DRUG ERUPTION
recur at the same site with each exposure to medications
Six or fewer lesions occur, frequently one
May be present anywhere on the body, but half occur on the oral and genital mucosa

Clinical Features Begins as a red patch Evolves to an iris or target
lesion identical to erythema multiforme that may eventually blister and erode
Lesions of genital and oral mucosa presents as erosions
Most lesions are 1 to several cm in diameter.
New lesions may be added with continiued /repeated ingestion of the medication.

Pathophysiology Exact mechanism is
unknown Recent research suggests a
cell-mediated process that initiates both the active and quiescent lesions.
Lesion contain intraepidermal CD8+ T-cells with the phenotypic markers of effector memory T-cells.
Skin-resident T-cells rapidly produce IFN-γ on exposure to medication.

Histologic Features• An interface dermatitis
occuring with intraepidermal and subepidermal vesicle formation, necrosis of keratinocytes and a mixed superficial and deep infiltrate of neutrophils, eosinophils, and mononuclear cells.
• Stratum corneum is normal in acute stage.
• Papillary dermal fibrosis and deep perivascular pigment incontinence are commonly present from prior episodes.

Etiologic Agents
Medications usually taken intermittently.
NSAIDS, esp. Pyrazole derivatives, Paracetamol, Naproxen, Oxicams, & Mefenamic Acid – predilection for the lips
Sulfonamides, Trimethoprim or the combination – resp. for majority of genital fixed drug eruptions

Possible Etiologic Agents
Include: Barbiturates Tetracyclines Phenolphthalein
(in laxative) Acetaminophen Ceterizine Celecoxib
Dextromethophan Hydroxyzine Lamotrigine Phenylpropanolam
ine Erythromycin Chinese &
Japanese herbs

Patch Testing needed to determine
which drug may be involved
Patch tests with various concentrations of the offending medication can reproduce the lesion on an affected but not unaffected skin.
Most useful in pyrazolone derivative-related reactions.

Nonpigmenting Fixed Drug Eruption
large, tender, often symmetrical eythematous plaques
Resolve completely within weeks.
Pseudoephedrine hydrochloride – most common cause
Baboon Syndrome – buttocks, groin, axilla

Treatment Main goal - identify the causative agent and avoid
it. Lesions of fixed drug eruption resolve
spontaneously with avoidance of the inciting drug.

ERYSIPELASSy, Jamelle D.

ERYSIPELASSt. Anthony’s fire / ignis
sacer
an acute beta-hemolytic group A streptococcal infection of the skin involving the superficial dermal lymphatics
group B – perineal erysipelas

ERYSIPELAS
local redness, heat, swelling, & a highly characteristic raised, indurated border
PMN leukocytosis skin lesions: transient
hyperemia vesicles or bullae
legs and face are the most frequent sites affected

ERYSIPELAS
• septicemia, deep cellulitis, or necrotizing fasciitis
complications:
• operative wounds, fissures, abrasions or scratches, unclean tying of the umbilical cord, venous insufficiency, obesity, lymphedema, and chronic leg ulcers
predisposing causes:
• contact dermatitis from plants, drugs, or dyes, and with angioneurotic edema
may be confused with:

TREATMENT
Pharmacologic
• Vigorous antibiotic therapy for at least 10 days
• systemic penicillin
• erythromycin
Non-pharmacologic
• Ice bags and cold compresses

CELLULITISSydiongco, Paula

Diffuse suppurative inflammation of connective tissue with severe inflammation of dermal and subcutaneous layers of the skin
Malaise, chills, fever, and toxicity may occur
Lymphangitis, regional lymphadenopathy, or both may be present
In severe cases, patients may develop hypotension and area infiltrated and pits on pressure

No racial and sex predilection
No age predilection; individuals older than 45 years
• Facial cellulitis is more common in children younger than 3 years.
• Perianal cellulitis is predominantly a disease of children.
Site of infection may occur anywhere on the body, but the leg is the most common site of the infection, followed by the arm, and then the head and neck areas. • following surgery or trauma
wounds, cellulitis can develop in the abdomen or chest areas.
• morbid obesity, it can also develop in the abdominal area

Incubation• 24 hours or can take days to
develop.Duration• less than a week to
disappear with antibiotic therapy.
• months to resolve completely in more serious cases and can result in severe debility or even death if untreated.
• Not properly treated, it may appear to improve but can resurface months or even years later.

break in the skin such as a fissure, cut, laceration, insect bite, or puncture wound
Risk factors: tinea pedis; elderly and those with immunodeficiency; diabetic people; Immunosuppressive drugs; Chickenpox and shingles; chronic venous insufficiency and varicose veins; pregnancy and obesity
Organisms on the skin and its appendages gain entrance to the dermis and multiply to cause cellulitis
The vast majority of cases are caused by Streptococcus pyogenes or Staphylococcus aureus

Cellulitis• S pyogenes
• Immunocompetent adults• Perianal cellulitis (children)
• perianal erythema and pruritus, purulent secretions, painful defecation, and bleeding in the stools
• S aureus• Children
• Pasteurella multocida• dog or cat bite or scratch
• Pseudomonas aeruginosa• after a puncture wound
• Non–group A streptococci (ie, groups B, C, and G)• lymphatic obstruction or venectomy for coronary artery
bypass graft• Aeromonas hydrophilia, Vibrio vulnificus
• after exposure to freshwater or seawater

Haemophilus influenzae cellulitis• Haemophilus influenzae type B• Children < 6 y.o.• Rare in countries where vaccination is available• Bacteremia may lead to meningitis, orbital cellulitis,
osteomyelitis, or pyarthrosis• Culture, needle aspirate• Cefotaxime and ceftriaxone; Rifampin
Pneumococcal facial cellulitis• S pneumoniae• Young children• Extremity involvement: DM, subs. abuse• Head, neck & upper torso involvement: SLE, nephrotic
syndrome, hematologic dso.• Fever, leukocytosis, and septicemia• Penicillin, vancomycin

Helicobacter cellulitis• Helicobacter cinaedi
• Fever, bacteremia, cellulitis and arthritis• HIV- infected patients; malignancy,
diabetes; and acoholism• distinctive red-brown or copper color w/
minimal warmth• Ciprofloxacin
Tuberculous cellulitis• Mycobacterium
• TB px taking chronic corticosteroids• Past history of pulm. TB• Four drug treatment

Diagnosis
Cellulitis is most often a clinical diagnosis
Blood cultures usually are positive only if the patient develops generalized sepsis
Resemble Cellulitis: • deep vein thrombosis: compression leg ultrasound• Lyme disease has been misdiagnosed as staph- or strep-
induced cellulitis (bullseye rash does not always appear): to rule out Lyme disease is with a blood test, which is recommended during warm months in areas where the disease is endemic.[2]

Complications
Gangrene Metastatic abscess
Grave sepsis
Children and
compromised adults

Treatment & PreventionRest affected limb & cleaning the wound site and treatment with oral antibiotics
Early lesions:
• Intralesional inj of triamcinolone acetonide 1:10
Mild cellulitis:
• Flucloxacillin monotherapy (to cover staphylococcal infection)
Moderate cases or where streptococcal infection is suspected:
• combined with oral phenoxymethylpenicillin or intravenous benzylpenicillin, or ampicillin/amoxicillin ; cefazolin or vancomycin

Severe cases:• require admission and intravenous (IV) therapy.
Wound:• cleaned and dressed appropriately done daily or when they become wet or dirtyMedical advice should be
sought:• wound deep or dirty and retained foreign bodies

URTICARIATACATA, PatriciaTADY, Clarissa Marie

URTICARIA (HIVES)
characterized by wheals surrounded by a red halo or flare
severe itching, stinging or pricking
annular or polycyclic pattern clearing of central region and coalescence of lesions

URTICARIA (HIVES)
Subcutaneous swellings (angioedema) may accompany the wheals target the
gastrointestinal and respiratory tracts resulting in abdominal pain, coryza, asthma and respiratory problems.

ACUTE VS. CHRONIC URTICARIA
•days to weeks •Produce evanescent wheals that
rarely last >12h•Resolution within 6 weeks of onset
ACUTE
•Daily episodes of urticaria and/or angioedema lasting >6w
•Physical urticaria commonCHRONIC
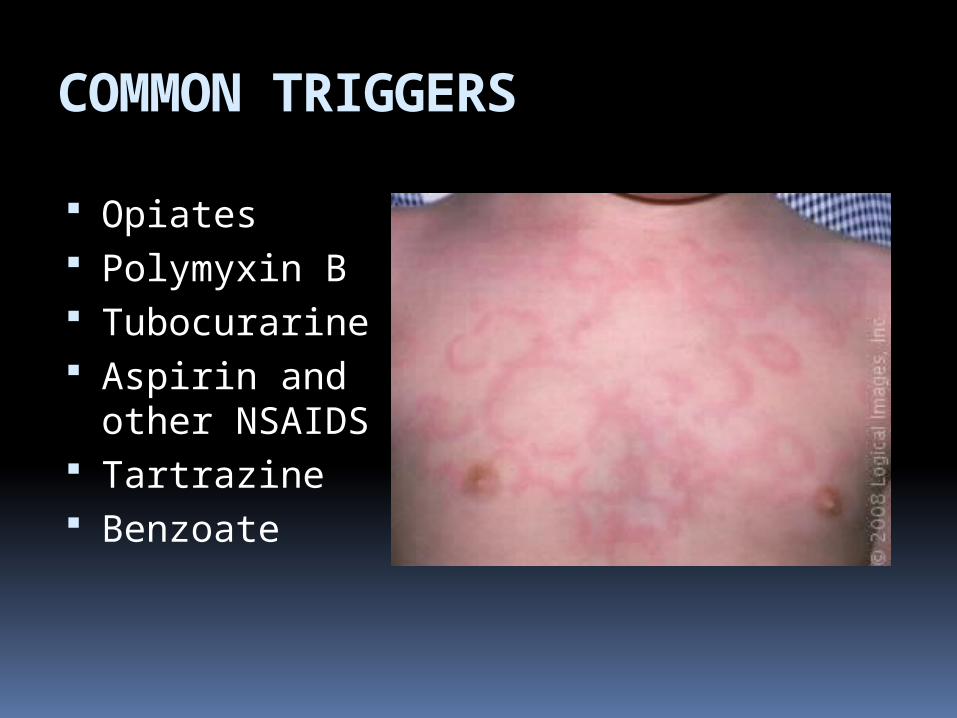
COMMON TRIGGERS
Opiates Polymyxin B Tubocurarine Aspirin and other
NSAIDS Tartrazine Benzoate

ETIOLOGIC FACTORS
•Most frequent cause of acute urticaria
•MOST COMMON: Penicillin and related antibiotics
•Allergic rhinitis or asthma, nasal polyps and food induced anaphylaxis
A.DRUGS
•frequent cause of acute urticaria whereas in chronic urticaria food is a less frequent factor
•MOST COMMON: Chocolate, shellfish, nuts, peanuts, eggs and milk
•Serum radiallergosorbent tests(RASTs) can be used to detect specific IgE and elimination of diets can be of benefit.
B. FOOD

ETIOLOGIC FACTORS•Natural food additives: yeasts,
salicylates, citric acid, egg and fish albumin
•Synthetic additives: azo dyes, sulfites, penicillin, benzoic acid derivatives
•With the exception of sulfite and penicillin, most food additives can be avoided by eating only meat produce and dairy products
•Packaged food are largely prohibited.
C. Food
Additives

ETIOLOGIC FACTORS
•Streptococcal infections •Chronic viral infection (Hep B & C)•Helminths (ascaris,
ankylostoma,filaria)D. Infection
s•Severe emotional stress no matter
what the primary cause•Initiating stimulus in CHOLINERGIC
URTICARIAE. Emotional Stress
•Associated with carcinomas and Hodgkin’s diseaseF.
Neoplasms

ETIOLOGIC FACTORS
•Grass pollens, house dust mites, feathers, formaldehyde, etc.G.
Inhalants
•Induced by ingestion of alcoholH.
Alcohol
•Rarely causes urticaria
I. Mentho
l

PATHOGENESIS
Capillary permeability
Release of histamine from the MAST CELLS (PRIMARY EFFECTOR in urticarial reactions)
Serotonin, leukotrienes, prostaglandins, proteases and kinins – other substances that may cause vasodilation and capillary permeability

DIAGNOSIS• Clinical grounds• Fixed lesions >24h: Urticarial vasculitis,
granuloma annulare, sarcoidosis, cutaneous T – cell lymphoma
• Skin biopsy: if wheals last >24hCLINICAL EVALUATION• Detailed history and physical examination• Radiologic sinus evaluation • Blood count to detect eosinophilia • Review of medications in chronic urticaria • Skin biopsy

ANAPHYLAXIS
An acute and often life
threatening immunologic
reaction
Scalp pruritus, diffuse
erythema, urticaria and angioedema
Most common causes of serious anaphylactic reactions:• Penicillins,
radiographic contrast agents
• Hymenoptera stings, shellfish and other food allergens

Treatment Acute Urticaria
Antihistamines Non-sedating Histamines pose a lower risk
of psychomotor problem in adults. Avoid the trigger if the cause can be
identified Systemic corticosteroids For severe reactions, respiratory and
cardiovascular support is essential. Intubation and tracheotomy may be
required.

Chronic Urticaria Mainstay treatment: Antihistamines
Should be taken on a daily basis and not prescribed to be taken as needed
Second generation antihistamine produce less sedation in most patients
Second line treatment Phototherapy Calcium channel antagonist Antimalarial medications Methotrexate
Corticosteroids produce long term side effects Local treatment
Tepid or cold tub baths Topical camphor and menthol

OTHER URTICARIAL VARIANTS

Angioedema
▫Acute, evanescent, circumscribed edema
▫Area of predeliction: Eyelids, lips, lobes of ears, external
genitalia, or mucous membranes of the mouth, tongue, or larynx
▫ Swelling occurs in the lower layers of the skin or in the subcutaneous tissues
▫ Frequently begins during night and is found on awakening
▫ Two subtypes: Deep form Angioedema associated w/ C1 esterase inhibitor
deficiency


Hereditary Angioedema (HAE)▫ Quincke edema▫ 2nd – 4th decade, Autosomal dominant inheritance▫ Swelling: Asymmetrical without urticaria or itching In subcutaneous tissues and abdominal organs mimicking surgical emergencies, and the upper airway (larynx) – life-threatening▫ Little response to antihistamines, epinephrine, or steroids▫ High mortality rate – death often caused by laryngeal edema▫ 3 phenotypic forms: Type I Type II Type III ▫ Trigger factors: minor trauma, surgery, sudden changes in temperature, or sudden emotional stress


Acquired C1 Esterase Inhibitor Deficiency
Usually occurs after 4th decade of life No family history Not associated w/ pruritis or urticaria Two subtypes: A. Acquired angioedema-I
▫ Rare disorder associated with lymphoproliferative diseases
▫ Treatment: Replacement of C1-EI with concentrates or FFP; antifibrinolytic agents; synthetic Danazol
B. Acquired angioedema-II▫ Extremely rare disease▫ Treatment: Immunosuppresive therapy; Synthetic
corticosteroids (temporarily effective); Plasmapheresis
Episodic Angioedema with Eosinophilia
Uncommon disorder w/ no underlying disease
Isolated facial edema May occur with fever, weight gain,
eosinoophilia and elevated eosinophil major basic protein
Treatment: administration of systemic steroidal medications, antihistamines, and IVG

Schnitzler Syndrome
▫Rare disorder▫Combination of chronic, non-pruritic
urticaria, fever of unknown origin, disabling bone pain, hyperostosis, increased erythrocyte sedimentation rate, and monoclonal IgM gammopathy
▫Age of onset: 29-77 years old; affects both sex
▫Effective therapy has not been determined
▫Bone pain and urticarial lesion respond to systemic corticosteroids

Physical Urticarias Occur most frequently in ages 17-40 years
old Most common form
dermatographism > cholinergic > cold urticaria
Chronic idiopathic urticaria: Dermatographism, delayed pressure, cholinergic,
and cold urticaria Other forms:
Adrenergic Urticaria Vibratory Angioedema
Heat Urticaria Aquagenic Urticaria Solar Urticaria Pressure Urticaria
( Delayed Pressure)

Dermatographism▫Sharply localized edema or wheal
with a surrounding erythematous flare occurring within seconds to minutes after the skin has been stroked
▫Affects 2-5% of the population▫Arise spontaneously after drug-induced
urticaria and persist for months▫H2 antihistamine may be of benefit

Cholinergic Urticaria▫ Produced by the action of AcH on the mast cell▫ Characterized by minute, highly pruritic,
punctuate wheals or papules 1-3 mm in diameter and surrounded by areas of erythema
▫ Area of predilection: trunk and face ▫ Persists for 30-90 min and followed by a refractory
period with no lesions of up to 24 hours▫ Palms and soles are spared▫ Trigger factors: exercise, emotional stress,
increased environmental temperature, or intradermal injection of nicotine picrate or methacholine
▫ Treatment: adequate dosage of antihistamines; Danazol in refractory cases

Cold Urticaria Exposure to cold may develop edema and wheals
on the exposed areas; usually on the face and hands
Urticaria does not develop during chilling but on rewarming
Types: Primary – no underlying systemic disease - Tx: Doxepin, Cyproheptadine;
Acrivastine and Cetirizine Secondary - Associated with underlying
systemic disease such as
cryoglobulinemia Familial Cold Urticaria- produces a
Burning sensation with cyanotic centers
and surrounding white halos
lasting for 24 – 48 hrs - Leukocytosis - Tx: Stanozolol
therapy

ERYTHEMA MULTIFORMETamondong, RoxanneTan, Ernie Joe

Erythema Multiforme
Erythema multiforme minor Herpes simplex-associated erythema
multiforme (HAEM) Strongly associated with preceding
herpetic infection

Clinical features
Self-limited Recurrent disease Young adults 1-4 weeks Sharply marginated, erythematous
macules
Raised, edematous papules
24-48 hrs

Classic target or iris lesion
A ring of erythema that forms around the periphery, and centrally the lesions are flatter, more purpuric, and dusky
3 zones: Central dusky purpura Elevated, edematous pale ring Surrounding macular erythema
Typical target lesions best seen in palms and soles

Lesions appear symmetrically and acrally
Initial involvement most frequently of the dorsal hands
Dorsal feet, extensor limbs, elbows, knees, palms and soles
10% of cases, more widespread lesions occur on the trunk
Mucosal involvement in 25% of cases and is limited to the oral mucosa

Atypical HAEM
Outbreaks of unilateral or segmental papules and plaques that may be few in number or solitary
Lesions may be up to 20cm in diameter
Plaques- erythematous and evolve to have a dusky center, which desquamates
Subcutaneous nodules may be present

Histology: features of EM and HSV can be seen
Acyclovir – prevents the lesions Prednisone – increase the frequency
of attacks

Etiologic factors Preceding orolabial HSV infection Appear 1-3 weeks (average of 10 days)
after the herpes outbreak Not all episodes of EM may follow every
episode of herpes

Pathogenesis
due to an allergic reaction(medication) or infection(HSV or Mycoplasma)
involves damage to the blood vessels of the skin followed by damage to skin tissues.
Activated T lymphocytes are present in lesions of Erythema Multiforme. Epidermis – Cytotoxic or Suppressor cellsDermis – Helper T-cells
EM minor is linked to HLA type HLA-DQ3

Histopathology
Histologic Features are NOT predictive of etiology due to similar feature from
EM to TEN(Toxic epidermal necrolysis) Extent of epidermal involvement depends
on the duration of the lesion and where in the lesion the biopsy is taken
Biopsy- “basket-weave stratum corneum” - suggest acute process where in
there was not enough time to produce abnormal keratin

Histopathology
Vacuolar interface dermatitis is present with vacuoles and foci of individual cells necrosis out of proportion to the no. of lymphocytes
Dermal infiltrate is largely mononuclear and tends to be primarily around the upper dermal vessels and along the dermo-epidermal junction.
Eosinophils may be present but rarely prominent and not predictive of etiology

Histopathology of EM must be differentiated from the following:
Fixed Drug Eruption
Graft vs Host disease
Pityriasis lichenoides
Lupus erythematosu
s-deeper infiltrate-w/ eosinophil and neutrophils- papillary dermal fibrosis- melanophages around post-capillary venules
-More compact stratum corneum -Epithelial disorder resembling Bowens Disease
-w/ lymphocyte in every vacuole- w/ erythrocyte extravasasion - neutrophil margination within dermal vessels
-Compact hyperkertosis- a deeper periadnexal infiltrate- dermal mucin and basement membrane thickening

Differential Diagnosis when Bullae are prominent:
Pemphigus Bullous pemphigoid
Paraneoplastic pemphigus
- Prominent mucous membrane involvment
- Lesions are small - erythema prominent at periphery of the bulla
-May produce atypical target lesions- mucosal involvement - vacuolar interface dermatitis - appear very similar to EM major

Treatment
Most cases are self limited and symptomatic treatment may be all that required-Anti-histamine, Moist compress, Topical anesthetics and Acetaminophen
Prevention:Sunscreen lotion and sunscreen-containing lip balm – prevent UVB induced outbeaks of HSV
Therapy:Oral Anti-viral (acyclovir, valacyclovir or famciclovir)Dapsone – antibacterial that inhibits synthesis of dihydrofolic acid - alternative drug when anti-virals are not effectiveSystemic Steroids – control inflammationIntravenous Immunoglobulin – to stop disease process

EXFOLIATIVE DERMATITIS
Genevieve Lynn C. Tan

Exfoliative Dermatitis
Dermatitis exfoliativa Pityriasis rubra (Hebra) Erythroderma (Wilson – Brocq)

Exfoliative Dermatitis
Extensive erythema and scaling
Entire body surface is dull scarlet
Small, laminated scales
No vesicles and pustules
Extensive telogen effluvium
Etiology
Result of generalization of preexisting chronic dermatosis (61%)
Medications allopurinol, sulfas, gold, phenytoin, phenobarbital,
isoniazid, carbamazepine, cisplatin, dapsone, mefloquine, tobramycine, minocycline, nifedipine and iodine
Inadequate intake of branched chain amino acids in infants with MSUD
Idiopathic

Etiology
Sezary syndrome Generalized
exfoliative dermatitis with intense puritus
Leonine facies Alopecia Palmoplantar
hyperkeratosis Onychodystrophy

Criteria for diagnosis of Sezary syndrome: Absolute Sezary cell count of at least
1000/mm3 CD4/CD8 ratio >10 Increase Lymphocyte count with evidence
of T cell clone Chromosomally abnormal T cell clone

Etiology
Hodgkin’s Disease Generalized exfoliative dermatitis Fever Lymphadenopathy Hepatosplenomegaly ESR
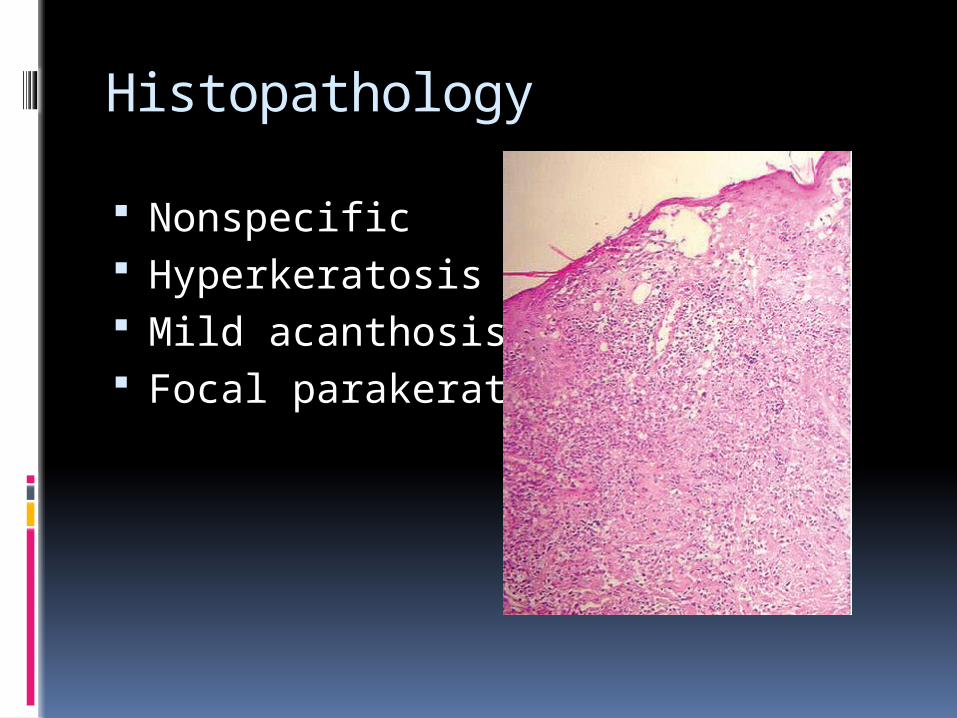
Histopathology
Nonspecific Hyperkeratosis Mild acanthosis Focal parakeratosis

Treatment
Drug-induced – stop drug Application of mild corticosteroid
after soaking and occlusion under sauna suit
Acitretin, cyclosporin, methotrexate for psoriatic erythroderma
Isotretinoin, acetretin, methotrexate for PRP
Azathioprine and methotrexate for idiopathic erythroderma unresponsive to therapy

HANSEN’S DISEASE
Tan, Marie DoloresTan, Samantha

Hansen’s Disease Also known as LEPROSY
Chronic, systemic, infectious disease caused by Mycobacterium leprae
Granulomatous or neutrophelic lesions in different parts of the body like: Skin Mucous Membrane Nerves Anterior Segment of the Eye Bones Viscera

Hansen’s Disease
Mycobacterium leprae
Weakly acid fast Grows 32-35°C Cultivated in mouse pads and
armadillos Favors intracellular location Only bacterium to invade
peripheral nerves Phenolic Glycolipid (PGL-1) – unique
to leprosy bacillus

Epidemiology
10-15 million worldwide
Asia (Indian Subcontinent), Sub-Saharan Africa, South and Central America, Pacific Islands, and the Philippines
Most cases in tropical and developing world
More common in people who are of low economic status, w/ inadequate housing, unsuitable sanitation, poor nutrition, and lack of education

Epidemiology
Men > Female Occurs in all ages Peak presentations in children aged
10-20 years old and in adults 30-60 years old
Mode of transmission: controversial (respiratory route: infectious droplets from nasal secretions)
Genetic susceptibility

PATHOGENESIS
Patient’s immune reaction to the leprosy bacillus: critical element in determining the outcome of infection.
TUBERCULOID LEPROMATOUS
Granulomas Well-formed, contain helper T-cells
Poorly-formed, predominant suppressor T-cells
Cytokine profile IFN-γ, IL-2 IL-4, -5, and -10 prominent
Cell-mediated immunity
Good Downregulated

DIAGNOSIS Identification of M. leprae in the affected tissue
Skin biopsies Skin or nerve lesions Stain: visualize the bacillus with Fite-Faraco stain
Slit smears Lesions and cooler areas of the skin Stain: acid-fast stain Multibacillary: organisms found on the skin smears Paucibacillary: negative skin smears (and 5 or fewer
lesions) Serologic tests
Detects antibodies against M. leprae-unique antigens (PGL-1)
PCR detects small numbers of organisms in infected tissue

Diagnostic procedures
Histamine Test
Metacholine Sweat Test
Skin Sensory Test
Lepromin Test (Mitsuda Reaction)

Hansen’s Disease
Presents with a broad spectrum of clinical diseases
Exposure
No clinical disease
(Spontaneous cure)
Develops clinical disease
Paucibacillary
Multibacillary

Early indeterminate leprosy
Insidous onset Slight prodromal symptoms “Numbness” – first clinical manifestation First lesion is a solitary, ill-defined
hypopigmented macule (sometimes erythematous) Succeeding lesions common: Cheeks, upper arms,
thigh, and buttocks Peripheral Nerves not enlarged No plaques No nodules No or very few bacilli on biopsy

SPECTRUM OF HOST-PARASITE RESISTANCE in leprosy
High resistance Unstable resistance No resistance
Tuberculoid (TT)
BorderlineTuberculoid (BT)
Borderline (BB)
Borderline Lepromatous (BL)
Lepromatous (LL)
Lesions 1-3 Few Few or manyasymmetrical
Many Numerous and asymmetrical
Smear for bacilli
0 1+ 2+ 3+ 4+
Lepromin test
3+ 2+ + + 0
Histology Epithelioid cells decreasing → Increasing histiocytes, foam cells, granuloma, xanthoma-like
Nerve destruction, sarcoid-like granuloma

Tuberculoid leprosy Solitary, large, few (<3), asymmetrically
distributed lesions Sharply defined and elevated border that
slopes down to flattened atrophic centers– “Saucer Right Side Up” appearance
Palpable indurations Dry hairless hypo/hyperpigmented lesions Lesions are anesthetic/hyposthenic and
anhidrotic Enlarged peripheral nerves (great auricular
nerve and ulnar nerve) Muscular weakness and atrophy Common sites of lesion: Face, Limbs or Trunk
www.aifo.it/.../online/courses/lepdd

Borderline tuberculoid leprosy
Lesions are similar to tuberculoid lesions, but smaller and more numerous (>10-20)
Satellite lesions around large macules or plaques
Less hair loss Nerves slightly enlarged Common sites of lesion:
face and limbs
www.aifo.it/.../online/courses/lepdd

Borderline leprosy Small, numerous (but
countable), cutaneous lesions Generalized, but
asymmetrical lesions Erythematous, irregularly
shaped, ill defined borders Erythematous plaques with
islands of normal skin – “Swiss Cheese Appearance”
Nerves are slightly enlarged, thicker, and tender
Anesthesia is only moderatewww.aifo.it/.../online/courses/lepdd

Borderline Lepromatous Leprosy
Numerous (too many to count), symmetrical lesions: macules, papules, plaques, and nodules
Ill-defined outer border and sharply marginated inner border - “Inverted saucer shaped” or “Punched Out”
Reverse configuration of tuberculoid type
Nerve lesions appear later, enlarged, tender, or both
Anesthesia is often absent
www.aifo.it/.../online/courses/lepdd

Lepromatous Leprosy Numerous, symmetrical
macules, papules, plaques, and nodules
Lepromas (nodules) on the earlobes, nose, lips, eyebrows
Little or no loss of sensation over the lesions
No nerve thickening No changes in sweating “Leonine Fascies” Madarosis – lateral thinning of
eyebrows Nasal ulceration
www.aifo.it/.../online/courses/lepdd

TreatmentWHO Western Pacific recommendation

Reactional states
Characteristic and clinically important aspect of Hansen’s disease
Experienced by 50% of patients after institution of multidrug therapy
Triggers: intercurrent infections, vaccination, pregnancy, vitamin A, iodides, bromide
Severe, abrupt 2 Forms
TYPE 1 TYPE 2Caused/Mediated By:
Cell-mediated Immune complexes
Occur In: Borderline Leprosy(BT, BB, BL)
Lepromatous patients(BL, LL)
Management of reactions Even though reactions may appear after drug
treatment is instituted, it is not advisable to discontinue or reduce anti-leprosy medication.
MILD REACTIONS No neurologic complications or severe systemic
symptoms Supportive treatment, bed rest, aspirin or NSAIDs
TYPE 1 REACTIONS Prednisone Clofazimine
TYPE 2 REACTIONS (ENL) Thalidomide: drug of choice; potent teratogen Systemic corticosteroids

prevention
BCG vaccination alone provides about 34% prevention against infection
BCG + heat-killed M. leprae increases protection to 64%
Treat active multibacillary patients and examine exposed persons on an annual basis to detect early evidence of infection
Chemoprophylaxis in hyperendemic regions Once yearly multidrug therapy with single dose
rifampin+minocycline+clofazamine