nhs bolton clinical commissioning group public … · 3.3 phbs are purely voluntary - no one will...
TRANSCRIPT
1
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: ………11……………… Date of Meeting: …………25th November 2016…………. TITLE OF REPORT:
Personal Health Budgets (PHB) – Policy and Guidance
AUTHOR:
Bernie Horne, CHC Department
PRESENTED BY:
Mary Moore, Chief Nurse
PURPOSE OF PAPER: (Linking to Strategic Objectives)
To seek approval from Board for the PHB Policy And Guidance.
LINKS TO CORPORATE OBJECTIVES (tick relevant boxes):
Delivery of Year 1 Locality Plan. √ Joint collaborative working with Bolton FT and the Council.
√
Supporting people in their home and community.
√
Shared health care records across Bolton. √ Regulatory Requirement √ Standing Item
RECOMMENDATION TO THE BOARD: (Please be clear if decision required, or for noting)
The Board is asked to approve the PHB Policy and Guidance. The Board is asked to note: That there are appendices that support the main policy and guidance document (which are available on request) and include:
• PHB Legislation, Regulations and Guidance.
• PHB Process – Detailed Flowchart. • Delegation of Clinical Tasks to Personal
Assistants. • PHB Financial Process. • Financial Audit Guidance for PHB Direct
Payments. • Equality Analysis.
That the PHB Policy and Guidance should be used in conjunction with the NHS England “Guidance on Direct Payment for Healthcare – Understanding the Regulations (2014)
2
document and the draft Bolton Council’s Draft SEND “Guidance Document for Personalisation and Personal Budgets – Including Direct Payments”. That the Draft Policy and Guidance contains a statement about the CCGs proposed future intentions to offer PHBs to other patients groups not covered under the current PHB Local Offer. Bolton CCGs target (from NHS England for PHBs) is between 303-606 PHBs by 2020. This figure cannot be achieved through the current Local Offer patient groups.
That as PHBs are new and emergent to the NHS, this Policy and Guidance will be subject to regular reviews.
COMMITTEES/GROUPS PREVIOUSLY CONSULTED:
PHB Implementation Group Bolton CCG Exec.
REVIEW OF CONFLICTS OF INTEREST:
VIEW OF THE PATIENTS, CARERS OR THE PUBLIC, AND THE EXTENT OF THEIR INVOLVEMENT:
The Policy has not been through a formal public consultation.
OUTCOME OF EQUALITY IMPACT ASSESSMENT (EIA) AND ANY ASSOCIATED RISKS:
The Equality Analysis is included in the Appendices to the Policy and Guidance

PHB FINAL V11 5/10/16
Page 1 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
Personal Health Budgets (including Direct Payments) – Policy and
Guidance
Policy Number
1
Target Audience
CCG Staff / General Public
Approving Committee
Exec
Date Approved
5/10/16
Last Review Date
Next Review Date
5/04/17
Policy Author
Bernie Horne
Version Number
The CCG is committed to an environment that promotes equality, embraces diversity and respects human rights both within our workforce and in service delivery. This document should be implemented with due regard to this commitment. This document can only be considered valid when viewed via the CCG’s intranet. If this document is printed into hard copy or saved to another location, you must check that the version number on your copy matches that of the one online. Approved documents are valid for use after their approval date and remain in force beyond any expiry of their review date until a new version is available.

PHB FINAL V11 5/10/16
Page 2 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
Version Control Sheet Version
Date
Reviewed By
Comment
7
30/6/16 PHB Implementation Group
Recommend to take to Exec for key decisions
9
20/7/17 Exec Approval for some key decisions – requested to bring back to Exec at a later date
11
05/10/16 Exec Policy and Guidance approved
Analysis of Effect completed:
By: Date:

PHB FINAL V11 5/10/16
Page 3 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
Contents 1 Introduction .......................................................................................................... 4 2 Legislation and Guidance .................................................................................... 4 3 PHB Principles ..................................................................................................... 5 4 What is a PHB?.................................................................................................... 6 5 Who can have a PHB? ......................................................................................... 7 6 Exclusion for PHBs .............................................................................................. 8 7 PHB Management options ................................................................................... 8 8 Direct Payments for Healthcare Guidance ......................................................... 10 9 PHB Pathway ..................................................................................................... 10 10 Termination of a PHB ......................................................................................... 19 11 Governance Frameworks ................................................................................... 20 12 PHB Local Offer – Future Plans for Expansion .................................................. 27 13 Complaints ......................................................................................................... 28 Appendices
• Personal Health Budgets: Legislation, Regulations and Guidance – Extract from NHS England Guidance
• PHB Process – Detailed Flow-chart • NHS Bolton CCG’s Training for Personal Assistants Model • PHB Financial Set-up Process – Direct Payments and Third Party PHBs • Financial Audit Guidance for Personal Health Budgets (including for Direct
Payments and Third Party PHBs) • Equality Analysis - Personal Health Budgets

PHB FINAL V11 5/10/16
Page 4 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
1 Introduction
1.1 This policy and guidance outlines NHS Bolton Clinical Commissioning
Group’s (BCCG’s) principles for the implementation of Personal Health Budgets (PHBs). It balances choice, risk, rights and responsibilities and recognises that risk can be managed to promote a culture of choice and independence that encourages responsible, supported decision making.
1.2 The Policy and Guidance applies to the following groups of patients.
• Those eligible for Adult Continuing Healthcare who are living in their own or family home.
• Those eligible for Children’s Continuing Care and who are living in a community setting.
• Children with Special Educational Needs (SEN) and disabilities (as part of their Education, Health & Care Plans - EHCP)
• Adults and Children with Learning Difficulties (as part of the ‘Transforming Care’ agenda)
An Equality Analysis has been carried out in relation to this Policy and Guidance – see Appendix 6 1.3 The implementation of Personal Health Budgets in Bolton is still at an early
stage and national policy and direction is still evolving. As national direction and policy become clearer it is likely that this Policy and Guidance will need to be amended in line with it. Currently the Policy and Guidance should be read alongside the “Direct Payments for Health Care (Regulations)” and the Bolton Council’s “Guidance Document for Personalisation and Personal Budgets (including direct payments)”. The latter document covers Bolton Council and NHS Bolton CCGs offer of Personal Health Budgets for families of children and young people who will be transferring from having a “statement of educational need” to an “Education, Health and Care Plan” under the “Special Educational Needs (SEN) and disabilities” (SEND) Reforms.
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/398815/SEND_Code_of_Practice_January_2015.pdf 2 Legislation and Guidance
2.1 The initiative for PHBs originated from the government’s Personalisation
programme and much earlier than that from organisations of disabled people pressing for the right for autonomy in their lives and for control over the assistance they needed in order to live independently. Direct Payments and Personal Budgets for social care users have been available since 1996 and 2002 respectively. The following legislation and guidance also describes the evolution of PHBs; NHS Next Stage Review: High quality care or all (Department of Health 2008) outlined plans for PHBs. Health act (2009) Allowed selected primary care trust
PHB FINAL V11 5/10/16
Page 5 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
sites to pilot Direct Payments High quality care for all: The operating framework for the NHS in England 2009/10 this confirms NHS priorities such as better access, reduced inequalities, partnership working in delivering personalised care, supporting service user contributions to improvement and shaping high quality provision. On 1st August 2013, the Direct Payment in Healthcare regulations came into force across England, meaning that the NHS can now lawfully offer Direct Payments for healthcare. Other relevant legislation includes: • Human Rights Act [1998] including Article 8 Right to respect for private
and family life, and Article 14 Prohibition of discrimination • The Data Protection Act (2003) • The Carers (Equal Opportunities) Act (2005) ensures that carers are able
to take up opportunities that people without caring responsibilities often take for granted.
• The Mental Capacity Act (2005). The need to apply the Mental Capacity
Act features strongly in self-directed support where the service user lacks capacity to manage money and/or ability to make decisions about their care.
• Mental Health Act (2007) • Deprivation of Liberty Safeguards (2009) • The Equality Act (2010) Replaced previous anti-discrimination laws with a
single Act. • The Children and Families Act (2014) • The Care Act (2014) See also “Appendix 1 – PHBs – Legislation, Regulations and Guidance”
3 PHB Principles
NHS England has identified key principles for PHBs and personalisation in health;
3.1 Upholding NHS values • The personalised approach must support the principles of the NHS as a
comprehensive service, free at the point of use, as set out in the NHS Constitution, and should remain consistent with existing NHS policy:
• There should be clear accountability for the choices made.

PHB FINAL V11 5/10/16
Page 6 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
• No one will ever be denied essential treatment as a result of having a
PHB. • Having a PHB does not entitle someone to more or more expensive –
services or to preferential access to NHS services. • There should be good and appropriate use of NHS resources.
3.1.1 Quality – safety, effectiveness and experience should be central. The well- being of the individual is paramount. Access to a PHB will be dependent on professionals and the individual agreeing a care / support plan that is safe and will meet agreed health and well-being outcomes. There should be transparent arrangements for continued clinical oversight, proportionate to the needs of the individual and the risks associated with the care package.
3.2 Tackling inequalities and protecting equality - PHBs and the overall movement to personalise services could be a powerful tool to address inequalities in the health service. A PHB must not exacerbate inequalities or endanger equality. Lack of mental capacity should not be a factor. The decision to set up a budget for an individual must be based on their needs, irrespective of race, age, gender, disability, sexual orientation or beliefs.
3.3 PHBs are purely voluntary - No one will ever be forced to take more control than they want, and the CCG does not have to offer an individual a particular way of managing a budget if it does not feel that that is the best way of commissioning services for that individual.
3.4 Making decisions as close to the individual as possible - Appropriate support
should be available to help all those who might benefit from a more personal approach, particularly those least well served by existing services or access and who might benefit from managing a budget.
3.5 Partnership - Personalisation of healthcare embodies co-production. It means individuals working in partnership with their family, carers and professionals to plan develop and procure the services and support that are appropriate for them. It also means CCGs, local authorities and healthcare providers working together to use personal budgets so that health and social care work together as effectively as possible.
4 What is a PHB?
4.1 A PHB is one of the options that NHS Bolton CCG offers to individuals to control and choose the services that they require to support their health needs. Following an assessment, planning and discussion with their clinical team, individuals are able to manage identified risks and to live their lives in ways that best suit them. The agreed PHB amount will be for a 12 months period from the start of the PHB arrangement. The amount of funding will only change should there be a change in the patient’s level of need. In this

PHB FINAL V11 5/10/16
Page 7 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
instance, following a reassessment of need, a new PHB amount will be set for the next 12 months.
4.2 NHS Bolton CCG will;
• Consider any request for a PHB for the patients groups covered by this policy. Requests can come from the patient, their family or any health professionals involved in the patients care.
• Provide information, advice and support in relation to PHBs. 4.3 The CCG supports the following essential requirements for a PHB.
The person with the PHB (or their representative) must:
• Be able to choose the health outcomes they want to achieve. • Know in advance of the planning stage an estimate of how much
money they have for their healthcare and support - an “indicative budget”.
• Be enabled to create their own support plan, with assistance if they want it.
• Be able to choose how their budget is held and managed. • Be able to spend the money in ways and at times that make sense to
them, as agreed in their plan.
The CCG is also committed to promoting patient choice, where available, while supporting patients to manage risk positively, proportionately and realistically.
5 Who can have a PHB? 5.1 From 1 October 2014, Bolton patients eligible for Continuing Healthcare
funding have had a ‘right to have’ a PHB including by way of a direct payment. This includes:
• Patients who are eligible for fully funded NHS continuing healthcare
(adults), including fast track patients; • Families of children eligible for Continuing Care
In the case of children this refers to the element of their care package that would normally be provided by the NHS once they become continuing care eligible and not the element of their care package provided by social care or education.
5.2 Patients and their representatives already in receipt of Continuing Healthcare
funding or Continuing Care may request a personal health budget at any time. Patients and families assessed as eligible for Continuing Healthcare funding or Continuing Care should be routinely informed of their “right to have” their care delivered in this way.
PHB FINAL V11 5/10/16
Page 8 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
5.3 NHS Bolton CCG has since April 1st 2016 extended its offer of PHBs to
include the following patient groups; • Children with Special Educational Needs (SEN) and disabilities (as part of
their Education, Health & Care Plans - EHCP) • Adults and Children with Learning Difficulties (LD - as part of the
‘Transforming Care’ agenda) 6 Exclusion for PHBs
6.1 The CCG may refuse to allow a patient to take their PHB as a Direct Payment
if it considers that there are risks;
• that the person (or their representative) would not be able to manage them;
• that it is inappropriate for that person given their condition or the impact on that person of their particular condition;
• that the benefit to the individual of having a direct payment for healthcare does not represent value for money;
• that providing services in this way will not provide the same or improved outcomes;
• that it would not be possible to set-up the PHB arrangement in the time-scale within which the care needs to be delivered e.g. some fast-track cases;
• that the direct payment will not be used for the agreed purposes. • that it would increase Safeguarding concerns.
6.2 If the CCG decides not to give someone a direct payment it will inform the
person, and any nominee or representative, in writing, and give the reasons.
The person, their nominee or representative may request that the CCG reconsiders its decision not to give a direct payment. They may also provide additional evidence or relevant information to inform that decision. The CCG will reconsider the decision in the light of any new evidence, and then notify and explain the outcome of the deliberation in writing. The CCG only needs to reconsider the decision not to give a direct payment once in any six month period.
Even if someone is not suitable to receive a direct payment, they may still benefit from more personalised care. The CCG will where possible, consider whether other forms of personal health budget, such as a notional budget or a budget held by a third party, might be suitable, or how else the person’s care could be personalised.
7 PHB Management options
7.1 The CCG would like to offer patients the choice in how to manage their PHB.
PHB FINAL V11 5/10/16
Page 9 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
7.2 The most appropriate way to manage a PHB should be discussed and agreed
with the patient, their representative or nominee as part of the Support Planning process. PHBs can now be received and managed in the following ways, or a combination of them; the following is a brief description of how NHS Bolton CCG patients can choose to take and manage their PHB.
• Notional budget – where a patient is informed of the amount of funding
available to them and decides how the budget is used (by input into the support plan) but the CCG continues to commission services, manage contracts and make purchases etc. Notional budgets could be an option for patients who want more choice and control over their healthcare but who do not feel able or willing to manage a budget.
• Third party budget – A different organisation, legally independent of both the patient and the NHS holds the money for the patient and arranges and pays for all of the services on behalf of them in accordance with the support plan. These organisations are also responsible for managing, training and supervising the staff but the patient should have the choice of which staff they use.
• Direct payments: Direct payments for patients with capacity – where the patient receives the funding that is available to them and they purchase the services and support that they want in accordance with the agreed support plan (with or without assistance). The patient can elect to receive and manage the payment themselves into a bank account specifically opened to receive only the direct payment, or decide for it to be received and managed by someone of their choosing (a nominee). If the patient chooses a nominee, that nominee becomes responsible for managing the funds and services and accounting for expenditure. Direct payment support services can provide a range of support to manage a Direct Payment dependent on the level of support that the patient needs or chooses. The CCG will pay for these support services. Direct payments for people who lack capacity – where the patient lacks capacity, an ‘authorised representative’ (agreed by the CCG) receives the funding that is available to the individual as a direct payment. The authorised representative is responsible for managing the funds and services and accounting for expenditure. The ‘authorised representative’ must involve the individual as much as possible and act in their best interests, in accordance with the Mental Capacity Act 2005. Direct payment support services can provide a range of support to representatives to help them manage a Direct Payment. The CCG will pay for these support services.
• Independent User Trusts - Independent user trusts are another option that
can be used to manage a PHB and are most commonly set up where the patient has been assessed as lacking capacity to manage the Direct Payment themselves. An independent user trust consists of trustees who hold money or other assets for the benefit of a third party – the patient.
PHB FINAL V11 5/10/16
Page 10 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
The number of trustees can vary but if a family member wishes to be a trustee there needs to be at least two other trustees.
An independent user trust is a commitment on the part of trustees to manage an agreed sum of NHS money in a way that puts the patient at the heart of decision-making and gives them choice and control in their life.
7.3 In the case of children, direct payments can be received by their parents or
those with parental responsibility for that child. 8 Direct Payments for Healthcare Guidance 8.1 The Regulations around Direct Payment for Healthcare are complex and NHS
England has produced detailed Guidance that will be useful for patients, practitioners, finance teams and commissioners. Where a patient chooses to take their PHB as a Direct Payment staff involved in the setting up of the arrangement will refer closely to the Guidance which is also included in the NHS Bolton CCG PHB Toolkit.
http://www.personalhealthbudgets.england.nhs.uk/_library/Resources/Personalhealthbudgets/2014/Guidance_on_Direct_Payments_for_Healthcare_Understanding_the_Regulations_March_2014.pdf
9 PHB Pathway 9.1 Before a patient can begin the process of setting up a PHB, the CCG requires
the patient to have an up to date health assessment (completed within the last three months). This assessment should have confirmed that the patient is eligible for health funding and for a PHB as per NHS Bolton CCGs PHB Local Offer. It should also identify the current level of the patients health and well-being need. Providing a PHB based on an out-of-date assessment may result in inadequate identification of the current level need and an inaccurate budget being set.
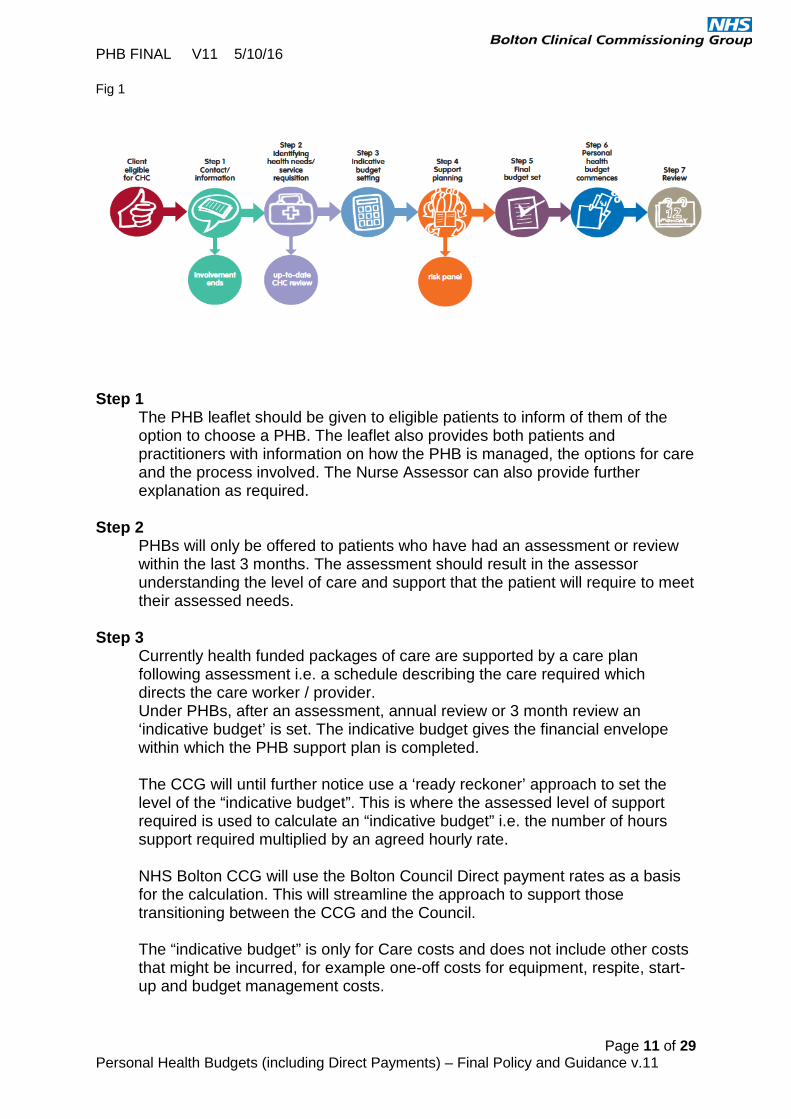
9.2 There are seven key steps to setting up a PHB as outlined in Fig.1 below.
Each step of the process will be described in detail throughout this document.
PHB FINAL V11 5/10/16
Page 11 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
Fig 1
Step 1
The PHB leaflet should be given to eligible patients to inform of them of the option to choose a PHB. The leaflet also provides both patients and practitioners with information on how the PHB is managed, the options for care and the process involved. The Nurse Assessor can also provide further explanation as required.
Step 2 PHBs will only be offered to patients who have had an assessment or review within the last 3 months. The assessment should result in the assessor understanding the level of care and support that the patient will require to meet their assessed needs.
Step 3 Currently health funded packages of care are supported by a care plan following assessment i.e. a schedule describing the care required which directs the care worker / provider. Under PHBs, after an assessment, annual review or 3 month review an ‘indicative budget’ is set. The indicative budget gives the financial envelope within which the PHB support plan is completed.
The CCG will until further notice use a ‘ready reckoner’ approach to set the level of the “indicative budget”. This is where the assessed level of support required is used to calculate an “indicative budget” i.e. the number of hours support required multiplied by an agreed hourly rate.
NHS Bolton CCG will use the Bolton Council Direct payment rates as a basis for the calculation. This will streamline the approach to support those transitioning between the CCG and the Council.
The “indicative budget” is only for Care costs and does not include other costs that might be incurred, for example one-off costs for equipment, respite, start-up and budget management costs.

PHB FINAL V11 5/10/16
Page 12 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
It is important to note that the budget at this time is not ‘finalised’ – it is an approximation of what might be a reasonable amount for the patient to purchase the care they need and may change on completion of the support plan. If a patient cannot purchase the care and support they need using the indicative budget then there may be a requirement to increase the final budget to meet the care needs. Similarly if the patient can manage to meet their needs more cost effectively there may be a reduction in the final budget.
“Indicative budgets” will be agreed through the existing Funded Care Panels or Care Boards, which meet frequently. Continuing Healthcare packages via the FCT Panel chaired by Funded Care Team Modern Matron. Meets weekly Children’s Continuing Care / SEND (health component) packages via the Children’s Continuing Care Panel chaired by the Senior Commissioning Manager – Women & Children. Meets monthly and as required. Transforming Care packages for people with learning disabilities / mental health via the Transforming Care Board chaired by the Integrated Commissioning Manager (Disabilities). Meets Monthly
Once the “indicative budget” has been approved a letter is sent to the patient / representative / nominee to inform them of the amount and about the next steps for developing a Support Plan. Where the patient is using a broker to complete their Support Plan the broker will be notified of the “indicative budget”.
Step 4 – Support Planning and Brokerage Start-up costs
NHS Bolton CCG will pay for any costs incurred in setting up the PHB. These may include for any of the following.
Assistance with • Support Planning • Information and Advice about services • Recruitment • Training for staff
The CCG will also pay for the assistance needed to manage PHBs including for • Fully managed bank accounting • Payroll • Insurance

PHB FINAL V11 5/10/16
Page 13 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
The CCG will consider requests to fund one-off purchases (e.g. for specialist equipment) or for respite services on a case by case basis. Where specialist equipment is concerned funding will only be agreed following recommendation from a relevant health professional e.g. physiotherapist, occupational therapist. The decision to fund would also take into consideration the cost effectiveness of each purchase.
Support Planning
One of the main aims of Support Planning is to facilitate a shift in decision making that enables a changed relationship between the NHS and the patient.
A support plan should demonstrate how health needs will be met in order to achieve the agreed outcomes, and should be clear about how resources will be used to achieve this. It should capture what is most important to the patient, as well as what is important for their health and wellbeing.
Planning with a PHB is not just about planning how to spend the money but ensuring that as part of the planning process we consider all the resources that the patient may have, i.e. their ‘real wealth’. This is in part to ensure that we do not encourage an over reliance on statutory funding to fulfill all life outcomes, where those outcomes could be met from within a person’s own family, networks and support systems including use of universal and community services.
Crucially the plan must be an integrated co-developed plan between the individual, the practitioner and support planner if they are using one. It must contain information about clinical diagnosis and options for treatment or care but be balanced with contextual information from an individual about lifestyle and the impact of their health condition on that lifestyle.
Support brokerage
A support broker is a person who helps patients to decide how their “indicative” budget could be used to get the care and support they require. It is their role to provide information on a range of local care and support resources available.
Support Brokers can be independent or part of a provider organisation. They are often linked to organisations that provide support with the financial management of Direct Payments or Third party PHBs.
NHS Bolton CCG Is developing the use of the local Support Brokerage market. Service providers will be brought under a Quality Assurance Framework.
What can / can’t a Personal Health Budget be used for?
The Department of Health advises that PHBs should not be used to purchase primary medical services provided by GPs, or:
PHB FINAL V11 5/10/16
Page 14 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
• vaccination or immunization • screening • the national child measurement programme and • NHS Health Checks
PHBs cannot be used for urgent or emergency treatment services such as un-planned in-patient admissions to hospital or accident and emergency.
PHBs cannot be used for surgical procedures.
PHBs cannot be used to pay for any NHS charges, such as prescription or for dental charges.
PHBs cannot be used:
• to purchase alcohol or tobacco • for gambling • to repay a debt (with the exception of debts relating to services
specified in the Support Plan) Requests to fund building adaptations with PHBs will only be considered once an application for Disabled Facilities Grant has first been explored.
A PHB direct payment can only be used to pay an individual living in the same household, a close family member or a friend if the CCG is satisfied that to secure a service from that person is necessary in order to satisfactorily meet the person receiving care’s need for that service; or to promote the welfare of a child for whom direct payments are being made. The CCG will make these judgements on a case by case basis any may insist that the family member or friend is registered with and paid via a third party organisation.
In addition PHBs cannot be used to purchase anything illegal or unlawful.
The Department of Health requires that PHBs should be compatible with the core principle of the NHS that care is based on clinical need, not ability to pay.
The PHB can only be spent on what has been agreed in the Support Plan. Any use of the PHB must have been agreed in advance by the CCG.
It is important to ensure that the spending of the PHB is directly linked to the achievement of personal health outcomes that are, in turn, directly linked to the patients identified health needs. The Support Plan should show this ‘golden thread’ and clearly indicate how the resources are being used to this end.
PHBs will be likely to push the boundaries of what the CCG has traditionally spent health money on and therefore it is important that where funding is being used in different ways this is always clearly linked back to a person’s outcomes and assessed needs. This means that something that would be
PHB FINAL V11 5/10/16
Page 15 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
agreed as appropriate spending for one patient because the link is clear, may not be agreed for another patient.
Where a Support Plan indicates that the PHB may be used to fund things that may be seen as non-traditional or suggest a high level of risk, the panel will make the decision on whether or not to agree the Plan and may request more frequent reviews and financial auditing be undertaken to ensure that the budget is meeting the person’s outcomes as set out in their Plan.
In addition to this the CCG has identified the need to co-opt as required experienced individuals to support a Panels decision making this will include advice and guidance for the consideration of support plans that the panel consider contain a significant amount of clinical, financial or organisational risk.
Step 5 – Setting the Final Budget Agreeing the Support Plan
All PHB Support Plans will need to be clinically agreed. This is the, responsibility of the practitioner and the relevant decision-making Panel or Care Board, to check that the plan meets the criteria in the “Support Plan checklist”.
Bolton CCG has set the following criteria, which must be met before a support plan can be agreed.
• The plan contains a summary of the person’s health and well-being
needs • The plan identifies what is important “to” the person – “these are the
things that make life worth living” • The plan identifies what is important “for” the person – “these are the
things that must happen to keep the person safe and well” • The plan shows what the person wants to change • The plan shows how the person will be supported in all aspects of their
life – not just paid support (Including other NHS services, paid/natural support, assistive technology, equipment, community resources etc.)
• The plan shows how the PHB will be managed i.e. self-managed, managed by a representative / nominee, by a Direct Payment support service or Third Party PHB support service
• The plan shows how the person will stay in control of their life, and maximise their independence.
• The plan identifies any risks and how they will be managed (Including Personal Assistant training )
• The plan sets out what the person is going to do to make their plan happen (action plan) to keep themselves healthy, safe and well
• The plan meets the person’s assessed needs and is clinically safe • The plan sets out how the person will spend their Personal Health
Budget within the budget provided.

PHB FINAL V11 5/10/16
Page 16 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
• The plan identifies contingency arrangements that ensures that the person will be safe and well should the usual support arrangement not be available e.g. a plan around being unwell - their Personal Assistant(s) not being available
It is crucial that these criteria are used by both those writing and those agreeing support plans. Agreeing the Funding
As per all packages of care under the current PHB Local Offer PHBs that are within the Level One funding range can be agreed by the appropriate Panel or Care Board as follows;
• Continuing Healthcare CCG Adult Funded Care Panel / FCT Modern Matron • Children’s Continuing Care via the Children’s Continuing Care Panel • SEND (health component) via the Children’s Continuing Care Panel • Transforming Care via the Transforming Care Board.
PHBs that cost within Level Two funding will also require the approval of the CCG Lead Nurse All packages that exceed the Level Two funding range will need to have the signed authorisation of the CCG Chief Officer or Chief of Finance following approval by the CCG Lead Nurse and the relevant panel. For details of funding levels see Appendix 4 “PHB Financial Process” of the PHB Policy and Guidance. Once the funding for the Support Plan has been agreed it may take some time to get the support in place. This may involve
• Recruiting staff • Training staff • Sourcing provider agencies • Buying equipment etc.
Patients can have assistance with this from their chosen brokerage provider. If a patient already has a package of care in place, this will continue to be commissioned until the CCG is notified that the PHB package is ready to commence by the patient / their representative or nominee or by their broker. Where a patient has been receiving a Bolton Council funded direct payment care package but has become eligible for a Bolton CCG Funded PHB, the Council will continue to fund the package until the PHB is in place. The Council will be informed of the eligibility date by the nurse assessor at the point of eligibility for health funding being agreed.
PHB FINAL V11 5/10/16
Page 17 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
The nurse assessor will notify the CCG Finance Team when the PHB Direct Payments should begin – this information is included in the CCGs Payment Schedule form for PHB Direct Payments. CCG Finance will then notify the Council of the PHB start date so that the Council can stop making payments and invoice the CCG for any costs they have incurred. The Council will invoice the CCG to cover the period from the date when the CCG became the responsible commissioners to the date that the Bolton CCG PHB starts. Risk and Panel The Adults and Children’s Continuing Care Panels and care Boards will make decisions on whether to approve part or whole of the PHB. Where there is increased risk or complexity the panels may co-opt experienced individuals to support the panels in their decision making function. The co-opted individuals who provide support to the panels can include for instance, the patient, family members, social services and executive members of the CCG including the Chief Nurse. The applicant has the right to appeal the decision and process through Bolton CCGs Appeals Panel. If the person, their representative or nominee is still not happy with the decision of the Appeals Panel then the Complaints Procedure will be followed. (See Section 13) Step 6 - PHB Commences
For Direct Payments
Before a Direct Payment can be made to a patient or their representative / nominee they must open a separate bank account. If a patient has received a Direct Payment from social care in the past then it will be possible to use the same account for their PHB as long as that bank account has been set up specifically for Direct Payments. Direct Payments cannot be paid into a patient’s current account.
Payments are made by the CCG into a patient’s bank account on a monthly basis. The CCG will also pay the equivalent of four weekly payments on top of the first monthly payment for the element of the package that is provided through a Direct Payment. This ensures that there is a level of “contingency” funding which the patient could use if for example their planned care arrangements break-down or a personal assistant is not available due to sickness.
Where the patient has chosen to have a “managed direct payment” the payments will be made by the CCG to the direct payment support service provider who should hold separate bank account for all patients.

PHB FINAL V11 5/10/16
Page 18 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
All patients taking their PHB as a Direct Payment must sign Bolton CCG’s “direct payment agreement”.
All “direct payment agreements” also need to be signed by either the CCG Chief Officer or Chief of Finance.
All direct payments can be audited at any time by the CCG
For Third Party PHBs
For this option payments will be made by the CCG to the chosen third party as per any other provider.
For Notional PHBs
With this option payments will be made by the CCG to the chosen support / care agency providers on the patient’s behalf.
Step 7 Review
The CCG will review PHB packages after three months and again after one year. The CCG may decide to undertake more frequent reviews should it be deemed necessary to manage any perceived risk.
If the assessment process has indicated a need for the care and support arrangements to be reviewed more regularly this must be established at the time the PHB commences.
Reviews will be robust and consider the potential for people to suffer from neglect or abuse. Although there is little evidence to suggest to date that people using PHBs are more at risk than people receiving direct services, it is important that the review process prioritises and risk assesses keeping the patient safe and protected from abuse.
The review will consider whether outcomes have been met. This should be a primary focus of the review and provides a platform for understanding how plans may need to change and adapt to be effective.
If it is clear that the budget is not meeting the patient’s health needs at a review an application for an increase in the budget needs to be made. The process for making a budget change or a change to the Direct Payment amount is the same as that used for setting up a new PHB and requires the same authorisation process. Any request for a revision to the budget should be evidenced by a corresponding change in the Support Plan. Patients may enlist the help of their support broker to make the necessary change to the support plan or amend it themselves. Agreement for the changes to the support plan will be through the same process as when agreeing the initial plan.
PHB FINAL V11 5/10/16
Page 19 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
If, at any time, the patient decides that their PHB arrangement is not working for them, they will have the option to have their care and support provided in the traditional way or through a “notional” PHB. See Appendix 2 – PHB Process – Detailed Flow-chart
10 Termination of a PHB
10.1 The CCG will terminate the PHB arrangement following notice to the patient
or their representative if: • The patient has deceased • The patient has transferred into a long term nursing home placement • One or more of the terms and conditions of the PHB Agreement are not being
met • The patient or their representative are using the money illegally or not in
accordance with the Support Plan as agreed with the CCG • The patient or their representatives use of the money is not in the patients
best interests • The patient’s health or safety is at risk • The patient or their representative are unable to provide the CCG with
adequate records on the money spent on services or support • The patient or their representative have told us that they no longer wish to
continue the arrangement • The patient or their representative is no longer capable of managing the
Personal Health Budget even with support available. 10.2 On termination of the PHB Agreement, all money held in the PHB bank
account must be paid immediately to the CCG and the account should be closed.
For “Notional” and “Third Party” Personal Health Budgets, the policy is to
recover any payment made to providers from the date of death/transfer/other reason for stopping the PHB as per any other commissioned package of care.
For Direct Payment Personal Health Budgets the policy is to use unspent
funds at the date the PHB ends to settle any debts owed to agencies or Personal Assistants up to and including the date of death/transfer/other reason for stopping the PHB.
Any unspent funds after debts have been settled will be claimed by the CCG.
If there are insufficient funds in a patients direct payment account to settle any
outstanding debts the policy is to treat this as an ‘exceptional circumstance’ which can be dealt with at the discretion of the CCG.

PHB FINAL V11 5/10/16
Page 20 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
Bolton CCG will maintain the right to lay claim to funds owed following ceasing of the PHB using the standard financial procedures for claims against an estate.
In line with the PHB Agreement, in the event of death, the patients Estate
needs to ensure that all surplus monies held in the Direct Payment Account will revert back to the CCG. In these circumstances, the account will be closed and the closing balance forwarded to Bolton CCG.
The CCG recognises that if the person, their representative or nominee was
an employer, their employees will have employment rights, which may include a paid period of notice or redundancy payment.
• The Estate must also provide Finance department with the account’s final statement and any additional information requested.
11 Governance Frameworks
Governance is the foundation stone for minimising and managing risk to both the organisation and the patient. Governance in the NHS is informed by national policy, regulation, professional standards and ethics.
Equally, it is informed by people and their families and is responsive to their experience and priorities.
Governance
11.1 A PHB Implementation Group has been established to progress the delivery
of PHBs. The Implementation Group is supported by Work-streams which are developing the detailed changes to services, systems and the tools required. Once work is completed the Implementation Group will continue to monitor the impact of the changes and report to the CCG Exec. As required.
CCG Exec
PHB Implementation
Group
PHB Policy
Quality Assurance Framewor
k
PHB Finance
Processes
PHB Process /
Toolkit
PHB Expansion Delivery
Plan
PHB FINAL V11 5/10/16
Page 21 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
11.2 Organisational risk 11.2.1 Authorisation of PHBs is the responsibility of NHS Bolton CCG. 11.2.2 NHS Bolton CCG has an obligation to ensure that:
• health and well-being needs are being met • safeguarding duties are fully met • best interests are met • it is fulfilling its duty of care and statutory obligations • it is fulfilling its responsibility to ensure that public funds are used to enable
patients to live independent and full lives – ensuring value for money • PHB expenditure is managed within the overall CCG budgetary allocation
ensuring NHS Bolton CCG fulfils its statutory duty to remain within its allocated funding resourcing limits.
• that public funds are used appropriately 11.2.3 NHS Bolton CCG is committed to shifting the balance of risk towards a
positive approach of supported decision-making for individuals, the organisation, and its partners.
11.2.4 NHS Bolton CCG will work with partner organisations to promote a wider
understanding of this approach to risk. It will also seek to secure from partners involved in delivering PHBs, a complementary approach to risk which is as light touch as is reasonable.
11.2.5 NHS Bolton CCG will work with the Local Authority where necessary should
any safeguarding concerns arise in relation to physical, sexual or financial abuse of an individual receiving a PHB. These will be investigated accordingly.
11.2.6 To sign off a PHB request, NHS Bolton CCG will approve:
• the proposed budget • level of clinical input • the outcomes identified in the Support plan • a plan for contingencies • supporting risk assessments • effective reporting mechanisms to demonstrate improved outcomes, benefit
and value for money 11.2.7 NHS Bolton CCG will have an appeals process to consider appeals in the
following situations:
• a request for a PHB which was not approved • the type of PHB offered is not acceptable to the individual • the final funding allocation is challenged by the individual, or • The decision making process is challenged by the individual.
11.3 Clinical risk
PHB FINAL V11 5/10/16
Page 22 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
This Policy and Guidance should be read in conjunction with the following NHS Bolton CCG Policy and Guidance
• NHS Bolton CCG Safeguarding Policy • NHS Bolton CCG Safeguarding Children and Adults at Risk Safeguarding
Supervision Framework 11.3.1 NHS Bolton CCG is committed to promoting individual choice, while
recognising the need to manage risk positively, proportionately and realistically. Good practice must support individual choice.
11.3.2 Enabling individuals to exercise choice and control over their lives, and
therefore their own management of risk, is central to achieving better outcomes for individuals. A degree of risk can be accommodated within the aim of enhancing the quality of people’s lives.
11.3.3 An individual who has the mental capacity to make a decision, and chooses
voluntarily to live with a level of risk, is entitled to do so. NHS Bolton CCG requires that any PHB Support Plan clearly evidences the rationale in relation to the management and reduction of risk where appropriate or necessary. This will be considered as part of the PHB approval process by NHS Bolton CCG. Empowering people to take control of their own health may generate a perception of increased risk and adverse consequences. However, in reality there is likely to be a reduced risk because individuals have been consulted about their choices, are actively involved in decision-making and take ownership of, and some pride in, the responsibility for achieving their outcomes.
11.3.4 Where the individual lacks capacity and has no legal representative, family or
friends, an independent mental capacity advocate will be contacted to assist in making best interest decisions on behalf of the individual.
11.3.5 The Mental Capacity Act 2005 and Personal Health Budgets guidance DH
2010 sets out that a nominated person or representative is expected to act in the best interests of the individual and to consider what they would have wanted if they had capacity. Nominated persons and representatives will be responsible for contractual arrangements secured by a direct payment, including employment contracts (where staff are to be directly employed), and management of the budget including repayment where this may be required.
11.3.6 The attitude of health care professionals should be to support and encourage
individuals’ choice as much as possible, and to keep the individual informed, in a positive way, of any issues associated with those choices and how to take reasonable steps to manage them.
11.3.7 NHS Bolton CCG will ensure that such risk is fully understood by the individual and managed in the context of ensuring that the individual’s needs and their best interests are safeguarded.

PHB FINAL V11 5/10/16
Page 23 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
11.3.8 A tiered approach to risk, when considering a request for a PHB, will be taken by NHS Bolton CCG. In practice, this means that the majority of people requesting a PHB should be successful. Those individuals considered not suitable for a direct payment will be offered a budget held by a third party organisation, and is there is no reason why at minimum, a notional budget (which must be supported by an outcomes focussed support plan), should not be offered to all who request a PHB, as there is no increased risk involved .
11.3.9 Risk is also a consideration when the individual (or carers acting on their
behalf) is deciding how they want to spend their money to meet their outcomes. Some choices made by individuals will be easy for the care coordinator to support - for example employing a personal assistant to visit at the times that suit the individual’s or family’s lifestyle, rather than a carer who attends at a time convenient to the service provider, or in the case of an adult PHB, going swimming rather than attend physiotherapy.
11.3.10 Other choices may be considered to be less orthodox, causing concern in
professionals trained to adhere to evidence based practice. 11.3.11Ways of mitigating the risk should be explored with the individual or their
carers acting on their behalf. Depending on the situation and the risk, it may be possible to agree a trial period with the individual that includes frequent monitoring.
11.3.12 NHS Bolton CCG recognises that this is a very different way of working, and
it may be a challenge for a professional. The requirement to work alongside an individual to deliver their choices may appear to conflict as to whether a proposed activity or service will meet the need and deliver the outcomes.
11.3.13 To support the decision making function of the Funded Care Panels and Care Boards, individuals may be co-opt to provide expertise and support to discuss complex, unusual or potentially higher risk PHB requests.
A Panel chair can seek advice and support on whether or not to approve some aspect or the entire PHB request. Where the Panel with the advice and guidance of the co-opted members feels that the risks presented by the PHB are unmanageable, they will notify the patient / representative / nominee of the decision.
11.4 Clinical Governance
11.4.1 NHS Bolton CCG endeavour to commission quality services for all patients
irrespective of how they are funded or delivered. 11.4.2 The CCG has “Safeguarding” policies and procedures in place. CCG staff are
required to complete training in accordance with the “Safeguarding” policies and procedures.
11.4.3 The implementation of PHBs gives rise to new and important issues associated with Clinical Governance, risk management, training, competencies and accountability; particularly if the patient in receipt of a PHB chooses to employ Personal Assistants [PA] to meet their individual needs.

PHB FINAL V11 5/10/16
Page 24 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
11.4.4 This is a relatively new concept for the CCG, health service providers and health care professionals to embrace.
11.4.5 The key Clinical Governance issues associated with a PHB include:
• How and when to delegate health care responsibilities • How training is provided and quality assured • Who pays for the training? • Who is accountable for the health care task? • Who is liable if harm occurs to the patient? • Risk management associated with delegation of health care tasks
11.4.6 These issues will be of equal concern to the budget holder, the Personal
Assistant, CCG and practitioners. PA’s are a growing work force with increasing responsibilities for the delivery of skilled health care provision. This is considered to ultimately enhance the budget holders’ quality of life by providing continuity and flexibility of care, as well as enhancing the skills and career prospects of the PA.
11.4.7 When deciding whether or not to employ someone, patients must follow best practice guidance in relation to safeguarding, vetting and barring including satisfying themselves of a person’s identity, their qualifications and professional registration if appropriate and taking up references.
11.4.8 Bolton CCG will work with local Direct payment brokerage providers to ensure patients can access appropriate training for any PA’s that they choose to employ. Similarly Third Party PHB providers will be expected to adhere to the standards for staff training in the Quality Assurance Framework for PHB Support Service providers.
11.4.9 The Quality Assurance Framework provides guidelines for accountability and
the risk management of patients, health care professionals and PA’s. This supports Clinical Governance.
11.4.10 Before a PHB is agreed the CCG needs to be assured that any PA providing support to a patient has received appropriate training and is considered competent to carry out any delegated healthcare task. This will be evidenced in the Support Plan. It should also be made clear in the plan how the competencies of PAs will be monitored and any further need for training delivered.
11.4.11 The CCG acknowledges its responsibility to ensure access to local training and support for PA’s. This will ensure that the necessary support, development and training needs of the PA are put in place in a timely way, ensuring the health care needs of the budget holder are met safely.
See Appendix 3 – NHS Bolton CCG’s Training for Personal Assistants Model 11.5 Financial Risk 11.5.1NHS Bolton CCG requires that the implementation of PHBs to demonstrate
value for money and be affordable. National pilots have shown that a PHB need not be more expensive than traditionally commissioned services. PHB’s are often less costly, as well as giving greater individual satisfaction. The
PHB FINAL V11 5/10/16
Page 25 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
budget should always be sufficient to meet the outcomes identified in the support plan and allow for planned contingencies.
11.5.2 All new PHBs will be reviewed after 3 months and then at regular intervals to
ensure that budget levels are correct. Revisions to budgets will be agreed with individuals as required based on financial monitoring and will help inform the budget setting for future PHB’s.
11.5.3 An estimate per PHB, where it is being taken as a direct payment, will be
factored in to the budget to allow for additional elements of spend which may arise (i.e. planned contingencies).
11.5.4 The following costs will normally be paid as part of the PHB:
• the direct cost of providing the service, including budget management costs • liability insurance where budget holders are employing their own PA’s • start-up costs such as initial staff training, support planning • staff training • equipment costs (where equipment specifically forms part of the PHB and is
not provided via Bolton CCG equipment services. • funding to cover the contingency plan
11.5.5 Bolton CCG has agreed financial management processes and documentation
to ensure robust management of individual PHB payments. These include PHB agreements whereby:
• The individual and case manager has to sign a Direct Payment Agreement
confirming their acknowledgement of the PHB purpose and funding arrangements and restrictions.
• The individual has to provide evidence to Bolton CCG of expenditure through bank statements, receipts etc.
• Overpayments will be reclaimed if representing more than two month’s payment (unless otherwise agreed in contingency plan).
• Records are retained by the individual and made available for inspection by Bolton CCG.
11.5.6 It is the responsibility of the budget holder to inform Bolton CCG as soon as
they become aware of factors which may affect costs. Individuals must be made aware that Bolton CCG will not automatically fund increased costs which have not been pre-approved through the usual care review process.
11.5.7 Other benefits that the PHB applicants are entitles to should also be taken
into account during the Support Planning process to ensure that the PHB doesn’t duplicate other sources of funding (e.g. winter fuel allowance, Motability allowance).
11.6 Financial Governance
The three most common ways that PHBs are taken or managed are;

PHB FINAL V11 5/10/16
Page 26 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
• Notional PHB – where the services continue to be directly commissioned
• Third Party PHB – where a patient chooses an independent provider to manage their budget and provide their care.
• Direct Payment – where a patient (or a chosen representative, including Direct Payment support providers and Independent Trust) manages the budget.
11.6.1 The NHS Bolton CCG Finance Team has procedures and guidance in place to ensure that all of the options for PHBs can be chosen by patients and payments made efficiently. See Appendices 4 and 5 “PHB Financial Set-up Process – Direct Payments and Third Party PHBs” “Financial Audit Guidance for Personal Health Budgets (including for Direct Payments and Third Party PHBs” Monitoring and reviewing Direct Payments 11.6.1 The CCG Finance Team provides an auditing and monitoring service to ensure that patients who are fully-funded by the CCG are being supported to use their PHB appropriately. 11.6.2 PHB Direct Payments are public money and NHS Bolton CCG has a responsibility to ensure they are used to meet the health needs and the broader health and wellbeing outcomes of those to whom they are given. The CCG also has a responsibility to effectively manage the risks associated with people using PHB Direct Payments including minimising the risk of fraud and the risk of money being used in ways that are either illegal or otherwise prohibited or do not work towards meeting people’s health outcomes. 11.7.3 Whilst managing these risks the CCG recognises that it is important that the uses of Direct Payments are not overly prescribed and that as far as possible people are supported in the choices they make. The CCG has made it clear in this Policy what patients can and cannot spend their money on and we expect our practitioners to emphasise this in their day to day work with patients. The “NHS Bolton CCG Direct Payment Agreement” that the patient or their representative needs to sign will help practitioners to explain this. 11.7.4 NHS Bolton CCG intends to take a proportionate approach to monitoring PHB Direct Payments, an approach which takes account of the specific risks relating to each particular individual and situation. The Chartered Institute of Personal Finance and Accountancy (CIPFA) guidance 7 issued in 2007 supported this approach, but beyond the need to reflect good practice there is also a financial incentive to ensure monitoring processes do not take up disproportionate amounts of time and resources. 11.7.5 Clinical staff should carry out an outcome-focused review after three months, and then at least annually, which looks at how the PHB has been used to

PHB FINAL V11 5/10/16
Page 27 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
meet the person’s identified health needs and achieve the agreed outcomes. Financial reviews should take place at the same time, rather than as a separate process. Joining up the two processes can save time and give a more rounded picture of whether resources are being used effectively. 11.7.6 Bolton CCG requires patients with Direct Payment funding to provide financial records to evidence what the funding has been spent on. The CCG Finance Team will set the frequency rate for these records to be submitted depending on the level of perceived financial risk that the individual package presents. 11.7.7 Where it is found that people appear to have wilfully made inappropriate use of the money the Finance Team will liaise with the named Nurse Assessor to work with the person to understand why this has happened and to consider
whether further action needs to be taken to recoup monies. The Nurse Assessor in turn should alert the CCG Finance Team regarding any concerns. 11.7.8 Bolton CCG has in place a clear process for setting out how and under what circumstances money would be reclaimed from people making sure they don’t penalise those who have made a genuine mistake. In addition, where people still need services, a decision will be made as to whether those needs should be met through notional or third party arrangements rather than via a Direct Payment. If not a commissioned package of care will be offered. 11.7.9 If someone is holding a significant amount of unused money from his or her Direct Payment and where this is not allocated for a particular purpose, this may be an indicator that a reassessment is appropriate. However, it is important that people are allowed to hold a certain amount of money for contingencies where this has been indicated and agreed in their Support Plan. Bolton CCG currently allows up to 4 week of contingency funding for Direct Payments. This will be reviewed from time to time. 12 PHB Local Offer – Future Plans for Expansion
NHS England is expecting that there will be a significant increase in the number of Personal Health Budgets by 2020. This could equate to around 1 - 2 in 1,000 people (0.1 - 0.2% of the population). For NHS Bolton CCG this means between 303 and 606 PHBs. This cannot be achieved by offering PHBs to only the patient groups included in Bolton CCGs PHB Local Offer for 2016-17 In order to increase the opportunity for wider groups of patients to have the benefits that PHBs can bring NHS Bolton CCG will, from 2017-2020, explore the possibility of PHBs for;

PHB FINAL V11 5/10/16
Page 28 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
• People with long-term conditions for whom current services are not fully meeting their health and wellbeing needs resulting in increased dependence on acute services; an
• People who need high cost, longer term rehabilitation e.g. people with acquired brain injury, spinal injury or specific packages of care to enable mental health recovery usually provided in specialist facilities.
• End of Life Care including exploring the possibility of a “hospice at home” model funded via PHBs.
The CCG will also explore how integrated care budgets could work for people with complex needs who don’t meet the criteria for Continuing Health Care including for people with learning disabilities and complex mental health. NHS Bolton is committed to piloting a new personal health budget scheme that will offer more choice of where wheelchairs can be bought as well as a detailed care plan that will help users make informed decision about their wheelchair. The care plans will also go beyond purchasing the chair to also include guidance on future maintenance, repair and replacement needs.
NHS Bolton CCG is also a pioneer site for piloting PHBs for maternity care. Pregnant women living in Bolton could be offered a personal budget and will be able to use it to make choices for each of three stages of the pathway – antenatal, intrapartum and postnatal care.
This means a woman would have a wider choice of who provides the maternity care she would prefer, such as a birthing pool, specialisation in teenage, older, or first time mothers, or a provider with a good reputation for breastfeeding support.
NHS England and other partners will work with the pioneer sites to develop and test new approaches which can then be rolled out nationally.
13 Complaints 13.1 Bolton Clinical Commissioning Group (CCG) is committed to commissioning high quality care for its patients. The CCG welcomes and actively encourages all service users and carers to comment on their experience. Compliments/positive feedback about local health services will be recorded and when things go wrong or are perceived to have fallen below the required standards, Bolton CCG will provide an accessible and impartial Patient Advice and Liaison Service (PALS) and complaints service. 13.2 Bolton CCG is committed to equality of opportunity and no person expressing concerns/raising a complaint will be treated differently to any other on the grounds of race, disability, age, religion or belief, gender or sexual orientation. 13.3 Bolton CCG recognises that comments and complaints are a valuable source of information from service users about the quality of the care it commissions and are seen as vital information to help support the continuous improvement of services and

PHB FINAL V11 5/10/16
Page 29 of 29 Personal Health Budgets (including Direct Payments) – Final Policy and Guidance v.11
make best effective use of NHS resources. All concerns and suggestions for improvement will be positively received and responded to in an open and transparent way. Complex PALS enquiries and complaints will be investigated to identify learning points with the aim of reducing the risk of another patient/family having a similar, unsatisfactory experience. 13.4 Bolton CCG also recognises the complaints process needs to take account of the individual needs of the patient and/or complainant. Complainants will be given the opportunity to discuss the handling of their complaint, agree a timescale and confirm their desired outcome. The full version of the NHS Bolton CCG Compliments, PALS and Complaints Policy can be found via the link below http://www.boltonccg.nhs.uk/media/1318/compliments-pals-and-complaints-policy.pdf