nhpco chipps pediatric palliative care newsletter
DESCRIPTION
MDTRANSCRIPT

NHPCO ChiPPS Pediatric Palliative Care NewsletterIssue #4; March, 2006
Welcomeby Charles Corr ([email protected]) and Christy Torkildson ([email protected])
Welcome to the fourth issue of our ChiPPS electronic newsletter! This newsletter is a project of the Education Work Group of ChiPPS, the Children’s Project on Pediatric Palliative/Hospice Services of the National Hospice and Palliative Care Organization.
Children’s Project on Palliative and Hospice Services: An UpdateSusan Huff Stacy [email protected] [email protected]
The Children’s Project on Palliative and Hospice Services (ChiPPS) is the Pediatric Leadership Council of the National Hospice and Palliative Care Organization. In 1998, an interdisciplinary group of pediatric hospice and palliative care professionals met in Dallas Texas. This meeting was the “birth” of ChiPPS. The goals of ChiPPS include supporting education, improving quality, and increasing access to pediatric hospice and palliative care.
The current leadership council is composed of 13 professionals representing Canada and the United States. Members include:
Co–chairpersons: Stacy Orloff and Susan HuffChuck CorrMary Jo GilmerNancy HuttonPeter Lund

Stacy RemkeMaria RuggsBarbara SourkesDavid SteinhornSuzanne Toce
And ex officio members: Marcia Lattanzi-Licht and Stephen Connor.
In addition to sponsoring this newsletter ChiPPS has completed several other projects. If you would like more information regarding ChiPPS please contact either Susan Huff at [email protected] or Stacy Orloff at [email protected].
We would like to share one very timely and exciting project ChiPPS is involved with. NHPCO is a proud partner with ITVS, providing guidance and support, including information regarding end-of-life care to the Lion in the House Project. Lion in the House is an independent film, coming to Independent Lens on PBS channels June 21 and 22, 2006. Lion in the House offers an unprecedented look at the cancer journeys of five young people and their families over a six-year period. Award-winning filmmakers Steven Bognar and Julia Reichert bring audiences face to face with the uncertainty of the entire cancer experience and its rippling effects on family, community, and professional caregivers. Many pediatric hospice and palliative care providers are already developing local activities in their communities to supplement this two-day television event. We encourage all providers to consider offering outreach events leading up to and including the broadcast dates. For more information see www.itvs.org/outreach/lioninthehouse.
Members of this Education Work Group owe a huge debt of gratitude to Stacy Orloff for her many efforts in guiding our efforts during our first year and for inaugurating this newsletter in such fine fashion. In addition to continuing as Co-Chair of the ChiPPS Leadership Advisory Council, we are delighted that Stacy will continue as a member of the Work Group.
We also want to thank you, the readers of this newsletter, for supporting the ChiPPS PPC newsletter and hope that you are finding it useful. We are especially grateful to everyone who has taken the time to offer feedback, support, and suggestions regarding this newsletter. One of our primary goals is that you, the reader, will offer ideas and suggestions regarding themes and content of this newsletter—both current and future. What ideas do you have us to work on? Send an e-mail to Christy ([email protected]) or Chuck ([email protected]). We especially want to publicize conferences and other resources that you are aware of. Please send that information to Sandy Macomber ([email protected]). In that connection, please note that many activities related to pediatric palliative and hospice care will be

included in the forthcoming 7th Clinical Team Conference and Scientific Symposium of the National Hospice and Palliative Care Organization to be held in San Diego, California on April 26-28, 2006 (see the notice of this conference in Sandy’s section on Educational Opportunities and Resources later in this newsletter).
The overall theme of this issue of the newsletter is self care for all who work in pediatric palliative care. That includes caring for oneself and caring for others, caring for individuals and caring for the team.
Here is a brief Table of Contents highlighting each section of this newsletter in the order in which those sections appear. You will notice that each of these sections has a contact name and e-mail address attached to it. We provide these contact names and e-mail addresses in order that you can get in touch with the section’s author(s) to seek ideas or exchange information.
Dale [email protected] Stress Management in Pediatric Palliative and Hospice Care.
As in previous issues of this newsletter, we have selected a theme around which to organize the contents of this issue. In this case, our theme is self care—for oneself and for others, for individuals and for the team. To address this theme, we are delighted that Dale Larson, Ph.D., of Santa Clara University agreed to contribute the keynote piece. Dale is well known to everyone who works in palliative and hospice care, and his book, The Helper’s Journey: Working with People Facing Grief, Loss, and Life-threatening Illness (Champaign, IL: Research Press, 1993) is an excellent resource on this subject, one that is well worth reading by all hospice and palliative care workers. Dale’s article identifies some of the distinctive stressors in pediatric palliative and hospice care, and then suggests strategies for stress management and self-care at both the individual and team levels.
Donna [email protected] Asked Questions: How Do We Support Ourselves?
In this section, Donna poses questions that often arise for care providers whowork in pediatric palliative and hospice care, and offers answers taken from asurvey of team members. Here, the questions and answers address: sources of stress unique to those working in pediatric palliative care; meaningful aspects of this work; how individuals are affected by their work and how they cope with repeated losses; whether or not it is appropriate to share one’s feelings with patients and families; whether awareness of the crises and tragedies that present themselves in this work is or is not a burden; what agencies do to support team members; and what individuals do to take care

of themselves. Be sure to send any questions that you would like addressed in future newsletters to Donna.
Karen Paradise Baranowski [email protected] in Pediatric Palliative and Hospice Care: Causes, Effects, and Coping Strategies
Karen’s contribution to this issue of the newsletter is a detailed review of some of the specific causes of stress when caring for children with life-limiting illnesses, the effects stress has on care providers, and ways to cope with such stress as individuals, teams, and organizations. Four tables in this section identify key elements involved in each of these topics. The closing sentences of this section draw attention to its major lessons: “Clinicians can best cope with the stresses of providing end-of-life care by: (1) learning what causes them stress; (2) learning how to recognize the effects of stress; and (3) developing coping skills and self-care techniques to conquer the stresses they encounter. The responsibility of coping with work stress lies both on the individual and on the organization that provides care to dying children.”
Kate Eastman Alan [email protected] [email protected] Programs and Projects for Staff Support and Care
In this article, Kate and Alan report the results of their survey of PPC team members from across the country about staff support and care. Their goal is to highlight good work that is already being done in this area, as well as to encourage others to draw upon the ideas offered by their respondents. Respondents provide comments about: shared concerns, themes, and approaches to staff support; regular, structured programs; singular and/or sporadic activities; obstacles; and what is most needed. Perhaps the key lessons that emerge from this section appear in its closing lines: “Support doesn’t happen if no one notices that someone is having a difficult time. Being attentive to one another is the first step in offering support.” Kate and Alan include contact information for their respondents so that readers of this newsletter can be in touch with them directly if they wish to do so. Please send to Kate and Alan information about unique programs and projects that you are aware of in any area of PPC and we’ll do our best to include that information in a future newsletter.
Stacy [email protected] as Part of Self Care in Pediatric Palliative and Hospice Care
As a contribution to self care, Stacy shares with us in this section some favorite cartoons that may help to lighten our days when we are involved in the often-difficult and challenging work of pediatric palliative care.

Sandy [email protected] Opportunities and Resources
This section describes upcoming conferences, some books and articles, a website, and a new tool called “Come to Your Senses.” Sandy’s goal in compiling this section is to make readers aware of educational opportunities and resources that might be of value in their work. As we all know, it can be difficult to obtain information about such opportunities and resources, so we invite you to submit to Sandy any information of this type that you would like to share with other readers. Please help us help each other—a fine example of self care and staff support.
If you are not on our mailing list and received this newsletter from a friend or some other source, please send an email message to [email protected] requesting to be added to our mailing list.
We hope you have enjoyed reading this newsletter as much as we enjoyed putting it together! Thank you for taking time to read this issue of our newsletter and for any feedback that you can offer us. Providing pediatric palliative and hospice care to children, adolescents, and their family members has made great strides in recent years, even though it is certainly not always easy and still faces many challenges and obstacles. Perhaps we can minimize or at least reduce some of those challenges and obstacles through caring for ourselves and others in constructive ways. We wish you all the best in your good work. Look for the next issue of this newsletter in late summer.
Stress Management in Pediatric Palliative and Hospice Care
Dale G. Larson, Ph.D., Santa Clara [email protected]
We are shaped and fashioned by what we love. Goethe
Most veteran end-of-life professionals pay special tribute to their committed and courageous colleagues working in the emerging specialty area of pediatric palliative and hospice care. They recognize that caring for seriously-ill children and their families, work that is both greatly needed and richly rewarding, is also terrifically challenging. The challenges include not just the everyday stressors of modern end-of-life care, like time pressure, late referrals, physical demands, team and organizational issues, and complex ethical dilemmas, but also repeated exposure to one of life’s greatest tragedies, the death of a child. This brief essay will highlight some of the distinctive stressors in pediatric palliative

and hospice care and then suggest strategies for stress management and self-care at the individual and team levels.
Emotional Demands, Personal Losses, and Vulnerability
Care of parents and family members
Pediatric palliative care providers are lifelines for parents. Staff have intense personal involvement with parents and family members. When a child dies, these relationships continue, and staff serve as important resources for the bereaved. Family members typically expect these continuing involvements by pediatric staff and like them to attend bereavement services for their child and to remain available for contact after the loss (Macdonald et al., 2005). Although staff usually welcome the opportunities for continuing contact and find them personally rewarding, these occasions represent an additional emotional demand.
A related emotional demand is that of repeatedly empathizing with parents and family members. This empathic relating is key to effective care, but it brings risks. Emotionally connecting with traumatized parents can sometimes lead to a kind of vicarious traumatization, which adds a dimension to the stress equation that is different from the exhaustion, demoralization, and diminished caring that characterize burnout (Larson, 2000). In a helping relationship, these reactions can lead either to avoidance, distancing, and detachment or to tendencies to become overinvolved. Whether traumatizing or not, helping in this context is not going to be free of all distress. Helping a parent to talk about death with his or her child (Hilden & Tobin, 2003) is going to move you, maybe shake you. Being an expert companion and caring presence for a parent as he or she cries out in anguish is going to affect you profoundly. However, there is more than distress here—beauty, courage, healing, and growth are also often present in these powerful encounters. The adaptive challenges that you face in these helping encounters can make you more resilient and alive, but vulnerability and a kind of personal grief work are inescapable companions to this growth.
Care of the dying child
Caring for seriously-ill and dying children is extremely demanding, professionally and personally. Enhancing quality of life, responding to feelings and needs, and being a haven of safety and security in a time of chronic crisis—all require tremendous clinical skill and emotional involvement. As the illness progresses, particularly in a terminal hospitalization, each step toward greater intimacy, each discovery of a new quality in the child, of a way the relationship enriches both provider and child, becomes more poignant with the awareness of the impending death, and each must ultimately be assimilated as losses the provider must endure. Emotional involvement can be even greater if the palliative care team members are the same pediatric staff who cared for the child for many months or years, living through treatments, remissions, and recurrences with the child and

the family. This history, and the attachments that come with it, can lead to strong staff grief reactions to pediatric deaths.
Strategies for Stress Management and Self-Care
Here are just a few recommendations for stress management and self-care at the individual and team level. Since stress results when demands exceed resources, each of the following recommendations is designed either to reduce demands or to strengthen resources and coping strategies.
Take charge
Perhaps the most important principle of stress management is to take charge. Change your environment or change yourself, and do not fall into the trap of believing there is nothing you can do about the stress in your work. Ask “What can I do to change this stressful situation?” Allow some creative options to emerge, and then actively pursue one or more of these alternative behaviors. You can take charge by discussing a situation with a team member, concentrating on something good that could come out of it, or by looking for some small way you can control some of the stressful aspects of your work.
Practice the art of the possible
Unrealistic self-expectations can be a major source of stress. The best antidote is to practice the art of the possible and work consistently toward the goals that matter to you. In other words, develop realistic self-expectations without losing hold of the vision that inspires and guides you.
Stay out of the Helper’s Pit
Emotional arousal and states of personal distress can lead you to fall into what I have termed the “helper’s pit” (Larson, 1993a). Staying emotionally balanced and out of the helper’s pit requires a special empathic stance toward the distress we encounter. Carl Rogers once made a distinction in his definition of empathy that is useful here. He described empathy as sensing the client’s private world as if it were your own but without ever losing the as if quality. We want to be close enough to have contact, but not so close that we lose our balance and identify our whole selves with what we encounter. To steady yourself and maintain this balanced emotional involvement, it is important to draw on the various coping resources (personal strengths, social support, clinical and stress management skills) that support you in your helping efforts.
Practice self-care
Giving to others must be balanced with giving to yourself. Discuss cases with colleagues, travel, attend workshops, take all your vacation time (!), develop your

spiritual life, and do other things to find balance between giving to others and giving to yourself. When demands and resources are in balance, helping is a natural expression of the healthy human heart, and our caring connections with others in turn sustain our own health.
Exercise deserves special emphasis. Because stress is unavoidable, we need to make some of our stress-management interventions at a more downstream point in the stress cycle. Once the stress hormones have been released into your body, the best thing you can do is to get them out of your system, and exercise is probably the best way to do this.
Develop a strong support system
Self-doubt and other uncomfortable feelings are unavoidable in end-of-life care. When these difficult experiences are not shared with empathetic others and normalized, they corrode from within as what I call “helper secrets” (Larson, 1993b). A staff support group or regular peer mutual support meetings with a trusted colleague can be an excellent resource for coping with these internal stressors.
Acknowledge losses
Perhaps the most important guidelines for coping with the grief that is part of your work are to acknowledge its presence, accept it as part of the work you do, construct a personal philosophy of life that can make sense of the losses you encounter, and find supportive others, particularly colleagues, with whom to safely share your experiences. Because helper grief is not often discussed and is even to some degree stigmatized in the professional helping world, normalization of these grief reactions and acceptance from self and peers are essential. Organizational and team support are also needed to create opportunities for acknowledging losses in these ways. This support can take the form of providing bereavement sessions for staff following pediatric deaths or offering the flexibility needed for staff to attend funerals and have additional contacts with families.
Strategies for Team Stress Management and Self-Care
The interdisciplinary team is at the heart of pediatric palliative and hospice care because it takes a team to address the emotional, physical, social, and spiritual dimensions of care for children and their families. Physicians, nurses, social workers, chaplains, child life specialists, dietitians, music and other therapists, and other professionals all combine their expertise to meet the needs of patients and family members. Although stress-free teams do not exist, high team self-efficacy and collective self-esteem are powerful deterrents to stress and promote continued success and well-being. Team members are enabled to fulfill their personal missions as helpers while they pursue the team's shared goals.

What can you do to make your team healthier and more productive? Some of the keys to creating a productive and healthy team are as follows.
Encourage shared leadership
Just as no single person can achieve the basic task or mission of the team, no single person can make the decisions and lead the team in every situation. Instead, team members must assume shared leadership responsibilities, and these include both task functions, like problem solving and building work agendas, and process functions like making sure everyone’s contributions are considered.
Recognize good work
Praise, awards, and recognition dispensed within the team are among the best buffers against stress. All team members need occasional affirmation of the good things they do and of their importance to the team effort.
Build caring relationships
Share your best helping self with other team members. Openness, trust, respect, and authenticity should not be reserved for patients and family members, but should also be offered to colleagues. Empathy among team members and an atmosphere of goodwill lead to fewer stressful interactions and sustained personal growth of team members.
Empower one another
The interdisciplinary team is like a team of climbers working together interdependently to get to the top of the mountain. In the end, you are able to achieve something you could not do alone. It is important to overcome interdisciplinary myopia and to work to understand what other team members bring to the caregiving table. You can also teach team members from other disciplines skills and share knowledge with them, examples of what I call a kind of transdisciplinary team functioning that reduces interdisciplinary myopia and feelings of "This is my turf."
Study the team's process
To be effective, the team needs to study itself. Take time to discuss how the team can work together more effectively to work through any problems that may exist. Be proactive and take time for the team to renew itself through regular team-building experiences like retreats, brainstorming sessions, happy hours, and social occasions.
Conclusion

The emerging specialty of pediatric palliative and hospice care, perhaps because of the profound rewards and daunting challenges it offers, particularly attracts highly motivated, committed, and empathic professionals. This is a great gift to the children and families you care for, but also a point of vulnerability for you. Research shows, in fact, that the most idealistic, altruistic, and committed helpers are among the first to burn out—as is a bright flame by virtue of its intensity. The trick is to find a way to allow this bright flame of caring to inspire great acts of caring—to take that extra empathy and to put it to work—without burning out. This is the challenge of caring. If you can establish a balance between the demands you face and the resources you have to meet them, between giving to others and giving to yourself, you can achieve both personal growth and professional success as you continue your important work to improve the quality of life for children with life-limiting conditions and their families.
References
Hilden, J., & Tobin, D. R. (2003). Shelter from the storm. Cambridge, MA: Perseus.
Larson, D. G. (1993a). The helper's journey: Working with people facing grief, loss, and life-threatening illness. Champaign, IL: Research Press.
Larson, D. G. (1993b). Self-concealment: Implications for stress and empathy in oncology care. Journal of Psychosocial Oncology, 11, 1-16.
Larson, D. G. (2000). Anticipatory mourning: Challenges for professional and volunteer caregivers. In T. A. Rando (Ed.), Clinical dimensions of anticipatory mourning: Theory and practice in working with the dying, their loved ones, and their caregivers (pp. 379-395). Champaign, IL: Research Press.
Macdonald, M. E., Liben, S., Carnevale, F. A., Rennick, J. E., Wolf, S. L., Meloche, D., et al. (2005). Parental perspectives on hospital staff members' acts of kindness and commemoration after a child's death. Pediatrics 116(4), 884-890.
Frequently Asked Questions: How Do We Support Ourselves?
Donna [email protected]
Caring for children in with life-threatening and terminal illnesses and their families is emotional and intense to say the least. How does this work affect the staff? How do they cope? Many hospice/palliative care staff working with children report a high sense of satisfaction with this work. They value the relationships they form with patients and families, as well as the ability to make a difference
during very difficult circumstances. Support from those who have shared the same experience is also extremely helpful. Team members were surveyed to get a look inside the emotional experience of the caregiver.
What are some sources of stress unique to those working in pediatric palliative care?
The most obvious source of stress is the tragic circumstance of death of a child.
Maintaining healthy boundaries. Lines can get blurred during emotionally intense situations.
The higher level of needs and intense psychosocial issues related to complicated grief.
The involvement of multiple providers (pediatric sub specialists, school personnel, advocacy groups, etc).
Complex family dynamics due to a larger number of family members (siblings, grandparents, aunts, uncles, etc.) involved in the patient’s care.
What do you find most meaningful about your work with pediatric palliative care?
Listening to families discuss coping/love/commitment. The opportunity to alleviate emotional distress in persons facing such
extremely disheartening circumstances. Being able to make a difference in another family. The chance to meet and encourage some incredible families who live
through unbelievable tragedies and struggles. Knowing you are helping sick children and their families through a difficult
time. The willingness of most of the families to open up to our team. Assisting families in making memories. The relationships with children and families are extraordinarily meaningful.
I grow and learn more about how to live from each experience.
How do you cope with repeated losses?
Prayer and personal reflection. By focusing on the services provided that would have otherwise made a
sad situation more difficult. The belief that we have made a difference. Emotional support from friends/co-workers/team members. Remembering the treasured memories they (the patients and families)
have left. Spirituality.
How does your work affect you physically, emotionally, and spiritually?

I love this work. I feel we do make a difference. Playing with my own grandchildren seems to balance sorrow. It can be physically tiring, emotionally draining, and spiritually uplifting. It makes you appreciate each day more. Overall, it has given me a change in life view. There is a definite
awareness that life is a journey and it is important to make the most of each day.
Work is “draining” on occasion. It can drain you physically, emotionally, and spiritually if you don’t take care of yourself.
It does drain me physically. Emotionally, my heart feels raw at times. However, I am spiritually inspired and encouraged by my experiences at
Hospice. This work can be overwhelming and exhausting. It is also incredibly
rewarding to “share the journey” with such special children and families. It helps you keep your priorities straight—“don’t sweat the small stuff” Some days, I’m so exhausted I feel that when the day is over there will be
nothing left of me. But, most days, the rewards I receive are priceless.
Do you think it is appropriate to share your feelings with your patients and families? To share a part of yourself?
Yes/No. It is a way to relay empathy. Yes, but only if it will clearly be of encouragement or help to patients and
families. It is not appropriate if it may be a worry or a burden to the patient or
family. I think it is inevitable—you get very close to them and they value your
opinions. But, it should be limited to your thoughts/feelings related to patient status and plan of care.
Sharing of your feelings and relating empathy is a way to connect with patients and families.
With our work in palliative care, we realize each day is a gift, is this awareness a burden? Would it be easier to be oblivious to all the crises and tragedies?
No, it is not a burden. I appreciate that I have a better understanding of such awareness.
Yes, it can be a burden, but it is freeing. I think about death daily; it weighs heavily on me on some days. Other days it frees me to think about how I really want to live my life.
It is not a burden. If you were oblivious to all the crises/tragedies, you would be “cold”/unfeeling.
This awareness helps me to remember how fortunate I am, and to treat these kids as the special kids they are.

It is definitely not a burden, but a gift. Having the attitude that each day is a gift helps me deal with the loss of my patients because I consider the moment in time they are in my life as a gift as well.
No it is not a burden. It provides a greater insight and world view. Would it be easier? Yes, but a shallow existence may be easier but much less fulfilling.
Never is the knowledge of the blessings of a brand new day a burden. We need to realize that others do have crises and tragedies in order to keep ourselves in line and appreciate our own blessings.
What does your agency do to support you?
Encouraging professional development through conferences and educational materials.
Processing/debriefing with team and supervisor after a patient’s death. Encouragement from supervisor to engage in self-care including taking
time off. Consultation about difficult cases Staff retreat
What other things do you do to take care of yourself?
Maintaining healthy boundaries. Exercising. Spending time with family/friends. Engaging in personal hobbies (scrapbooking, reading, gardening, painting,
etc.) Maintaining a healthy lifestyle (getting enough rest, avoiding caffeine,
drugs, alcohol, and eating properly). Spirituality/religion.
Stress in Pediatric Palliative and Hospice Care: Causes, Effects, and Coping Strategies
Karen Paradise Baranowski

Caring for dying children and their families can be challenging and stressful. It is difficult to acknowledge that a child is dying and will not live a normal lifespan. Clinicians share many of the same stresses that the child’s family members experience. The strain, disruption, pressure, and depletion associated with such stress require significant personal and professional efforts to adapt and achieve balance (Davies & Eng, 1993)
We all experience stress in our lives, especially when working with dying children and their families. This section will focus on some of the specific causes of stress when caring for children with life-limiting illnesses, the effects stress has, and ways to cope with the stress as individuals, teams, and organizations.
Causes of Stress
Stress is any demand that exceeds a person’s ability to cope with or control it. Stress is experienced from both our personal and professional lives. In pediatric palliative care both the work environment and the nature of caring for dying children cause stress. Barnes (2001) found that team conflict and communication problems among staff were more stressful than actually caring for the dying. When stress is associated with caring for the child, it may be caused by an inability to relieve distressing symptoms or a lack of time to grieve after the death of a child (Barnes, 2001). Table 1 summarizes some of the common causes of work stress.

Table 1: Causes of Work StressPersonal Variables Personality characteristics (perfectionism) Over involvement with patients Identification with patients Self-esteem Sense of mastery Purpose in life Unrealistic expectations Feelings of inadequacy History of psychiatric illness Emotional demands Increased awareness of own losses,
vulnerabilities, and fear of own death Cumulative losses
Interpersonal Variables Physicians’ failure to understand hospice Conflicts with colleagues Poor communication among staff Lack of supportive, collaborative workplace
relationships Low team morale Disagreement about goals of care Patients’ family dynamics Patient psychological issues Poor relationship with patient/family Patient and family stressors (degree to which
patient/family accept illness and impending death, rate of patient’s deterioration)
Difficulty controlling patient’s pain/symptoms Difficulty predicting when death will occur Not being present when the patient dies Caring for a famous, extremely angry, or depressed
patient Secondary traumatic stress (knowledge of another’s
suffering or trauma and trying to alleviate it) Long-term relationships
Health Care System Variables Paperwork Increased workload Understaffing Too many patients dying at one time Decreased resources Organization stresses (scheduling conflicts,
funding issues) Lack of communication and/or support from
administration Role conflict View death as failure
Professional Variables Lack of experience and preparation Moral and ethical dilemmas Adverse effects of treatments Treatment errors Professional liability
Along with the frequent causes of stress in working with dying patients there are also some distinctive causes of stress when working with dying children. One stress unique to pediatric palliative care is the long-term relationship that often develops. Pediatric clinicians are often involved from the time of diagnosis through phases of hope and despair, relapse, deterioration, death, and possibly beyond (Davies & Eng, 1993). It is very difficult to watch a child’s condition deteriorate over time, especially when a close relationship has developed. Professional boundaries and relationships are often challenged when working with dying children. If the relationship becomes personal the clinician may feel more like a friend, will likely experience greater grief, and may have a hard time knowing when the relationship should end. A professional relationship is one that is time-limited, goal-oriented, and patient centered with professional knowledge and skills employed in the patient’s behalf (Davies & Eng, 1993). In some cases, involvement with families may go on for years after the death of a child. The effect may be that clinicians become uncertain of their role and when to withdraw from relationships, resulting in stress in the caregiver (Barnes, 2001).
Another area of stress common in pediatric palliative care is the clinicians’ inexperience and lack of preparedness in caring for dying children and their

families. Until recently it has been challenging to prepare clinicians because of the lack of research and education available on pediatric end-of-life care.
Many pediatric patients still die in the hospital setting where the focus is on diagnosing, curing, and prolonging life. Life-saving efforts are usually common when the patient is a child. When working with the dying these skills are irrelevant and can lead to potential for conflict in goals, values, interests, and frames of references (Davies & Eng, 1993).
Prognostication of life expectancy in children is difficult. There are very few prognostication tools or guidelines available in pediatrics. Many parents are told their child will die within a few days and the child ends up living several years. The challenges of prognostication increase stress among clinicians especially when a death is expected and does not occur or when the death is sudden and unexpected.
Along with the stress experienced because of the nature of the work in caring for dying children, personal characteristics also influence the way in which clinicians are able to cope. Some of the characteristics include clinicians’ attitudes toward death and terminal care, duration of nursing experience, ability to set personal limits, avoidance of over-involvement, letting needs be known, engaging in staff socials, keeping communication lines open, and attendance at funerals. If the causes of stress are not managed effectively, physical and emotional manifestations of the stress may appear.
Effects of Stress
If clinicians fail to recognize and manage the causes of stress, it may lead to compassion fatigue, burnout, and even compromise the care provided. Burnout and compassion fatigue are familiar in healthcare, as the stresses of the environment have overwhelmed healthcare workers’ abilities to cope.
In stressful times, those who provide pediatric palliative care may feel they are losing their own sense of self to the clients they serve. Compassion fatigue is an emotional accumulation of dealing with the needs of others on a regular basis. Compassion fatigue occurs when the clinician feels a state of tension and preoccupation with the client by re-experiencing their traumatic event, avoiding reminders of the event, and continual persistent discussion about the event. In pediatric palliative care this “event” is often the death or dying experience of a child.
The SIOP (2000) defines burnout as mental and physical exhaustion, indifference, sense of failure as a professional, and sense of failure as a person. Those whose work revolves around the problems and challenges facing others are especially vulnerable to burnout; health care professionals head the list of those who are susceptible (SIOP, 2000).

Burnout is seen as a multi-step process progressing slowly over time. Initially, the individual may feel emotionally empty and physically exhausted. The individual may feel overwhelmed and manifest symptoms of depression, poor concentration, insomnia, and changes in appetite. The next step is a stage of indifference. The individual becomes cynical, uncaring, unmotivated, and unable to communicate effectively. The third step is a sense of failure as a professional, followed by a sense of failure as a person. The last stage is often termed as ‘dead inside’ where the individual lacks affect and does his/her work without involvement, commitment, or enthusiasm (Barnes, 2001; SIOP 2000).
Accumulated stress occurs from both our personal lives and our work. Clinicians must learn how to recognize sources of stress and should try to recognize in themselves and their colleagues the symptoms of stress, compassion fatigue, and burnout as soon as they arise. Table 2 summarizes many of the common effects stress has on individuals.
Table 2: Effects and Symptoms of StressPhysical Symptoms Changes in appetite Gastrointestinal
disturbances Somatic complaints Headaches Exhaustion Clammy hands Increased motor activity Changes in sleep Illness Fatigue Substance abuse
Psychological symptoms Frustration Feeling depleted and irritable Anger Depression Guilt Nervousness Low self-esteem and self-
doubt Hopelessness Helplessness Loss of interest, meaning, and
purpose Increased isolation Memory disturbances Impaired judgment and
reasoning Short attention span Contempt Suicidal ideation
Effects on Work Questions ability to provide
good care Avoiding patients and
families Disinterest in and concern
for patients Believe patient’s complaints
to be manipulative Derogatory or inappropriate
jokes Lack of clarity about
professional role Burnout Feel imposed upon Sense of professional
loneliness Social distancing
Relationships Conflicts at home and
work Severing long-term
relationships
Stress may also affect interdisciplinary teams as a whole. Teams that are under stress may experience increased staff turnover, increased missed workdays, decreased productivity, and patient dissatisfaction with care.
Coping Strategies and Self-Care
Once clinicians recognize their reactions to stress they must utilize good self-care and learn various coping strategies to prevent or overcome the effects of stress. Sherman defines self-care as “the self-initiated behavior that people choose to incorporate to promote good health and general well-being” (2004, p.52). Clinicians must take care of themselves and identify coping mechanisms

that are effective. Along with the individual’s responsibility to take care of himself or herself there is also responsibility among employers to provide staff support.
One of the first coping skills individuals must develop is the ability to come to terms with their own thoughts and feelings about children dying. Staff must develop comfort in working with dying children and be able to move toward, rather than away, from them as they are dying. Also crucial to pediatric palliative care is the establishment of professional boundaries with both the child and family. This is crucial to be able to maintain therapeutic relationships. Clinicians should be reminded that they are part of a team, and are not responsible to meet all of the patient’s and family’s needs by themselves (Children’s Project on Palliative/Hospice Services, [ChiPPS], 2004).
Clinicians must be able to balance their professional and private lives. Dedicating efforts to family and interests outside of work will help maintain a healthy balance. Barnes (2001) warns that staff should be aware of tendencies towards overwork and must learn to set their own personal limits, avoiding over-involvement, maintaining open communication with colleagues, and informing peers of particular needs as they arise. Refer to table 3 for a summary of self-care and coping strategies.
Table 3: Self-Care & Coping StrategiesPhysical Health Eating well Exercise and recreation Restful and relaxing
activities (massage therapy, napping, warm baths)
Biofeedback Acupuncture
Mental Health Setting priorities Saying no Letting go of conflict Keeping an open mind to
new ideas In-services and continuing
education Interests such as music or
hobbies
Work Coping Strategies Professional boundaries Know why you chose a career
caring for terminally ill children Don’t view death as a failure. Reflect on rewards of work and
moments where you made the greatest difference
Speak with administrators for appropriate resources, staffing, and workloads
Taking time off Working part-time Reduce stressors Join professional organizations Explore professional and personal
goals Journal—express feelings about
caring for patients Patient memory books Support from colleagues Seek professional counseling Define your role Avoid distancing from
patients/families
Emotional Health Meditation Reflection Listening to quiet music Letting go of resentment Interacting with optimistic
people Enjoying fantasy and play Keeping a daily journal Speaking with colleagues or
friends Sense of humor Self-confidence—
competence and control Social support
Intuitional Health Religious/spiritual practices Consider personal beliefs Meditation Mind-body-spirit
connections Relaxation Ethics committees Create a sacred place where
you can retreat to collect yourself
Create a small “shrine” Promote inner harmony Self awareness

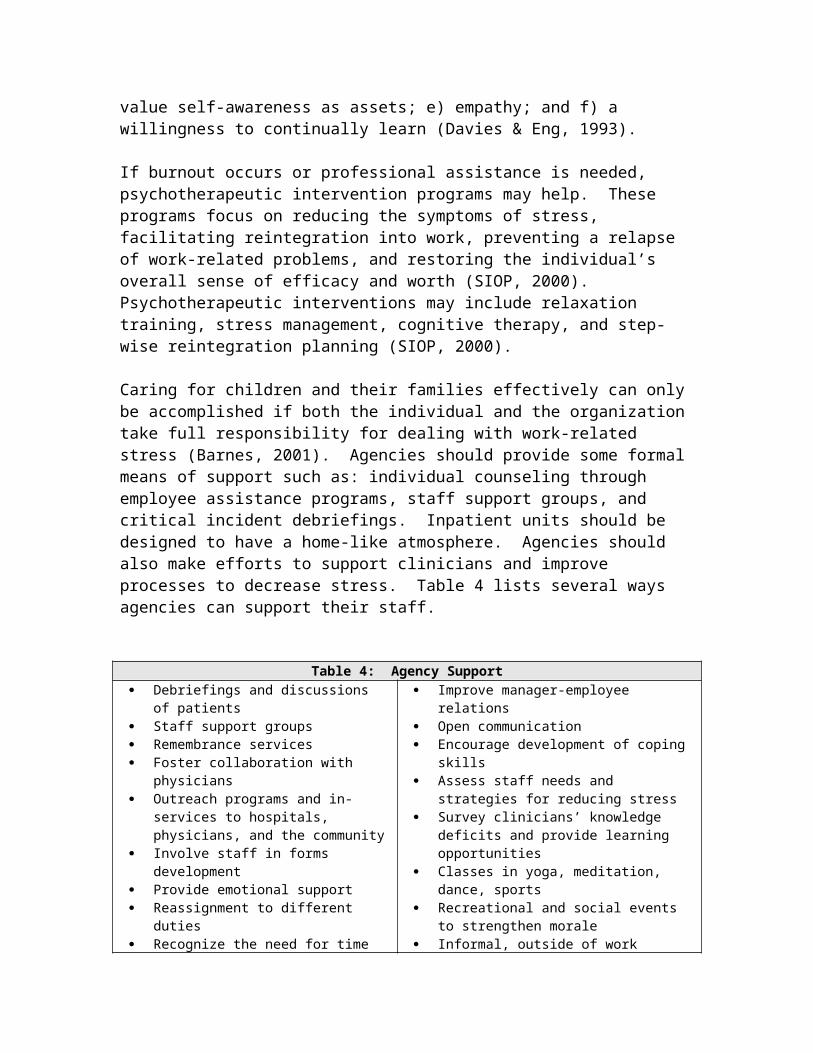
Individuals who have developed a wide range of coping skills through diverse life experiences will be better able to cope with the stresses of pediatric palliative care. There are also several personality characteristics that appear to affect clinicians’ ability to cope with these stresses. Some of these personal qualities include: a) high tolerance for ambiguity, flexibility, and an appreciation for individual differences; b) good external support networks and a realistic awareness of personal limits; c) a sense of humor; d) an open communication style and a tendency to value self-awareness as assets; e) empathy; and f) a willingness to continually learn (Davies & Eng, 1993).
If burnout occurs or professional assistance is needed, psychotherapeutic intervention programs may help. These programs focus on reducing the symptoms of stress, facilitating reintegration into work, preventing a relapse of work-related problems, and restoring the individual’s overall sense of efficacy and worth (SIOP, 2000). Psychotherapeutic interventions may include relaxation training, stress management, cognitive therapy, and step-wise reintegration planning (SIOP, 2000).
Caring for children and their families effectively can only be accomplished if both the individual and the organization take full responsibility for dealing with work-related stress (Barnes, 2001). Agencies should provide some formal means of support such as: individual counseling through employee assistance programs, staff support groups, and critical incident debriefings. Inpatient units should be designed to have a home-like atmosphere. Agencies should also make efforts to support clinicians and improve processes to decrease stress. Table 4 lists several ways agencies can support their staff.
Table 4: Agency Support
Debriefings and discussions of patients Staff support groups Remembrance services Foster collaboration with physicians Outreach programs and in-services to
hospitals, physicians, and the community Involve staff in forms development Provide emotional support Reassignment to different duties Recognize the need for time off EAP
Improve manager-employee relations Open communication Encourage development of coping skills Assess staff needs and strategies for reducing
stress Survey clinicians’ knowledge deficits and
provide learning opportunities Classes in yoga, meditation, dance, sports Recreational and social events to strengthen
morale Informal, outside of work activities Good orientation for new staff 1 on 1 supervision and monthly meetings
Clinicians must be prepared both emotionally and intellectually to care for dying children and their families. The more prepared clinicians are, the less fear and stress they will experience. Extensive orientation and on-going education for staff must be provided by organizations that care for children with life-limiting illnesses.

The best coping strategies for teams are to have high morale and good teamwork. High morale is achieved with individual job satisfaction, job involvement, and peer support. Teamwork is improved when there is a sense of belonging to an effective team. In a study on a pediatric ward caring for children with life-limiting conditions, Barnes (2001) found that staff with lower levels of stress valued talking with colleagues. Strong teams have good communication skills, creative thinking, provide social support for each other, and engage in skilled team building efforts. Teams that have trust in each other’s abilities, strengths, and skills have more realistic limits of involvement of individual team members and flexibility in roles (Sumner, 2001). Having good teamwork and high morale enables staff to support each other and deal with work stress.
Conclusion
Individuals who work in pediatric palliative and hospice care face many unique stresses and challenges in their work. It requires a commitment from themselves and their agencies to foster a continual sense of renewal in their capacity to care for these children (Sumner, 2001). Clinicians can best cope with the stresses of providing end-of-life care by: (1) learning what causes them stress; (2) learning how to recognize the effects of stress; and (3) developing coping skills and self-care techniques to conquer the stresses they encounter. The responsibility of coping with work stress lies both on the individual and on the organization that provides care to dying children.
References
Barnes, K. (2001, May). Staff stress in the children's hospice: Causes, effects and coping strategies. International Journal of Palliative Nursing, 7(5), 248-255.
Children’s Project on Palliative/Hospice Services (ChiPPS). (2004). Caring for kids: How to develop a home-based support program. Alexandria, VA: National Hospice and Palliative Care Organization
Davies, B., & Eng, B. (1993, January-February). Factors influencing nursing care of children who are terminally ill: A selective review. Pediatric Nursing, 19(1), 9-14.
Sherman, D. (2004, May). Nurses’ stress & burnout. American Journal of Nursing, 104(5), 48-56.
SIOP (International Society of Pediatric Oncology) Working Committee on Psychosocial Issues in Pediatric Oncology. (2000). Guidelines for the Recognition, Prevention, and Remediation of Burnout in Health Care Professionals Participating in the Care of Children With Cancer. Retrieved January 31, 2006, from The International Confederation of Childhood Cancer

Parent Organisations Website: http://www.icccpo.org/articles/psychosocial/guidelines_burnout.html
Sumner, L.H. (2001). Staff support in pediatric hospice care. In A. Armstrong-Dailey & S. Zarbock (Eds.), Hospice care for children (pp. 190-212). New York: NY: Oxford.
Unique Programs and Projects for Staff Support and Care
Compiled by:Kate Eastman Alan [email protected] [email protected]
Five areas of interest on staff support and care came to the surface as a result of the responses we received from across the country. Where we deem it important for our readers to be in touch with those who have given the ideas, we have put the person’s name following the program/idea. Where there is no name, we summarize the content of what we received to indicate that many people are also offering similar ways of offering staff support and care. We hope that the summaries will confirm the good work that is being done as well as encourage others to take up the challenges implicit in the ideas offered. The names of those who responded and ways to be in touch with them follow this article.
1. What are the shared concerns, themes, and approaches? Staff is offered counseling for individual as well as group settings by chaplains who also make rounds, respond to referrals, and focus on staff as wall as patients and families. The Employee Support Program is a resource for staff providing personal, private counseling. There is an interdisciplinary committee that plans events to improve employee morale. Mediation is offered in the chapel on a weekly basis and bereavement rituals are shared at staff meetings.
Debriefings regularly occur with a designated leader, such as a Critical Incident Stress Management Team or a regularly scheduled debriefing with an outside consultant. During weekly psychosocial rounds losses are announced, along with a summary of how the family and staff members are coping. Educational sessions are provided to deal with various modes of stress management.
There are programs that are monthly, quarterly, or annually to remember the children who have died. These are Memorial Services that staff plan and in which they participate. Such services include appropriate readings, music, stories, and photos in a supportive setting for the staff and the families of the deceased child.
There are educational opportunities for staff in self care and off campus retreats. There are hand massages weekly or free massages given regularly. Someone

needs to recognize the need for support and care in self and others. Getting help doesn’t happen if no one notices that someone is having a difficult time.
2. What are specifically unique, regular, and structured programs?
“Come to Your Senses” is a weekly staff rejuvenation program that focuses on the five senses and adds a sixth one: Nonsense. It offers a “pause” in the workplace to renew the staffs’ energies and is a resource notebook with 6 CD’s for the night as well as the day shifts. It can be led by anyone. This resource is listed in the Educational Opportunities section of this newsletter. Allison and Heather
The SEED program of the hospital is a way to recognize and support our coworkers. It is highly visible and used throughout the hospital. There are rewards that come from the recognition by coworkers. Allison
“Good Grief” is a monthly program focusing on an issue of grief affecting the staff. It is a free lunch for one hour sponsored by the Bereavement Council of the hospital. Allison
There are scheduled and organized devotionals, blessings, and worship services for staff and have prayer at nursing stations. Karen
There is a Remembrance Week sponsored by the Hospital Wide Bereavement Committee and is dedicated to “caring for ourselves while remembering those who have touched our hearts.” Kristen
“The Art of Being a Healing Presence” is a workshop of the fundamentals of human interaction. It affirms the power of human interaction and how another person’s experience impacts us. It encourages staff to become more aware of their internal responses, strengths, and limitations. Kristen
“Personal Death Awareness Training” encourages participants to explore their own loss histories and perceptions of death. Kristen
“Self-care” tools through the hospital’s benefits program, such as: back-up child care, focused health support and education, a wellness library, financial counseling, a contract with Errand Solutions, discounted tickets for entertainment/food, onsite bachelors/masters level classes, and Spanish language classes. Kristen
The Butterfly Program is pediatric palliative care that lets the family know someone is there for them as their child enters into the end of life. It offers 24-hour availability with medical director, nursing, social work, and a chaplain both in the hospital and at home. Trish

ACT or “Attending Caring Team” initiatives are based on Jean Watson’s theory of “Human Caring,” and have incorporated Lundin’s FISH philosophy. Bridget
“Soul Food” was started in the Cynthiana office of Hospice of the Bluegrass, created by the team of chaplains. The purpose of this 5-10 minute activity is to encourage staff members and provide an outlet for some of the stresses felt by working with a specialized, pediatric population. Some examples of “Soul Food” provided are: poems, stories, karaoke performances, pictures, newspaper articles, comics, guided relaxation exercises, and announcements. The items are usually humorous, although many are serious, encouraging, and reflective. “Soul Food” is shared on a weekly basis among the staff members, at the beginning of a staff meeting. It is widely participated in by all disciplines, and received well by all staff. Donna
3. What are singular and/or sporadic activities? There are organizations that have a Sunshine Committee, a group that supports staff through flowers, cards, etc., when there is a birthday or a crisis or a personal concern that is affecting the staff person.
A chaplain is encouraged to walk with the staff to take the deceased patient to the morgue and occasionally a chaplain has performed a ritual of cleansing or renewing or simply has prayed with the staff before another patient is admitted into the room where a death has occurred.
It is imperative to have available someone who can cover for a coworker when another coworker needs some time to reflect, renew, or rejuvenate after the death of a patient. It would be helpful to make a more concerted effort to give some well-earned time off and/or a retreat may give time for staff to spend time together and focus on a topic of interest.
4. What are the obstacles? We need more staff, more time, more financial support, more space to meet, and management support to provide support. Even recognizing our own needs, it still is difficult to make it priority to give and receive structured support. There is also resistance to being seen as “needing” support. Yet the lack of funds prevents us from bringing in speakers and changing ingrained behavior that says, “I’ll be just fine.”
Time outs, mental health days, in-services, and retreats can offset the expectations of being an “Iron Maiden.” It would also be great to get the doctors on board in this approach of staff support and care!!
5. And what is most needed? It is helpful to hear from others as the above information indicates. Get in touch with each other to pursue ideas and questions, share programs and resources. Along with the programs and

sporadic activities we learned that “generous listening—allowing us to vent without being judged and to be recognized for our own needs” is significant, as well as having support systems that are available. An open and safe atmosphere for sharing frustrations and grief leads to support when the context is non-threatening.
Volunteers have also been good at offering staff support just by caring and kindnesses. The gift of just being present is still a hallmark of support. It is crucial for someone to effectively be the champion for the money, time, and space for staff support. Along with this comes the specific needs of having inpatient coverage during staff support (although if there is just a 30 minute “check in” twice during each shift one staff will cover their coworker who attends one session and then that staff will cover their coworker for the second session.) And integrating cultural differences into this support may be an issue for a future newsletter.
Support doesn’t happen if no one notices that someone is having a difficult time. Being attentive to one another is the first step in offering support.
************************************************************************
These are the people from whom we excerpted portions of their responses to the survey as they wrote it.
Allison Sickel. The Children's Hospital, Denver. [email protected]
Bridget Darden. The Children's Hospital, Denver. [email protected]
Donna Armstrong. Daniel’s Care, Hospice of the Bluegrass, Lexington, KY. [email protected]
Heather Soistmann. The Children's Hospital, Denver. [email protected]
Karen Black. Our Children's House at Baylor, Dallas, TX. [email protected]
Kristen James. Children's Memorial Hospital, Chicago. [email protected]
Trish Montano. The Children's Hospital, Denver. [email protected]
These are persons who responded to our survey; their responses were interwoven in the text of this newsletter on staff support and care.

Cynthia Trapenese. [email protected]
Bev Hatter. Mary Bridge Children's Hospital and Health Center, Tacoma, WA. [email protected]
Brent Peery. Memorial Hermann Children's Hospital, Dallas, TX. [email protected]
Diane Thrush. Methodist Children's Hospital, San Antonio, TX. [email protected]
Doreen Duley. [email protected]
Evelyn Keever. [email protected]
Humor as Part of Self Care in Pediatric Palliative and Hospice Care
Stacy [email protected]
It seems appropriate to include a section on humor when discussing self care. I often ask myself “when was the last time I laughed out loud at work?” and all too frequently the answer is too long ago and not long enough. I try to keep up with the newspaper comics and my favorite cartoonists through their many books. I have a cartoon file I keep handy and I do try to use some cartoons with power point presentations and memos I might send. Sometimes I just pull the file out and read them to myself (it’s almost as good as reading my chocolate cookbook recipes when I need a chocolate “fix” but not quite!).
So, in honor of self care I am sharing a few of my favorite cartoons with you. I must say it was very hard to choose which ones to include. I’m thinking it might be nice to include some of our favorite cartoons in subsequent newsletters. What do you think? E-mail me and feel free to share your cartoons. Looking forward to hearing from you. Hope these bring a smile to your face and some laughter from your belly.


28th Annual Conference of the Association for Death Education and Counseling (ADEC)Grief and Loss: Wisdom and Insight, March 29 – April 2 , 2006Tampa Marriott Waterside Hotel & Marina, Tampa, Florida, USA
The ADEC Annual Conference presents a unique opportunity for interaction between individuals concerned with psychosocial, clinical, and educational aspects of death and loss. The Conference also provides a forum for the exchange of information in death education, care of the dying, and bereavement counseling and support.
Choose the ADEC Annual Conference in order to:
Learn about cutting-edge research and clinical work in the thanatology field. Create a curriculum tailored to your individual needs and disciplinary program. Participate in informal and formal networking opportunities.
Make the most of continuing education credits, the bookstore, and the exhibition.
Contact ADEC at www.adec.orgRegister online now using our Secure Online Registration form or download a Registration Form (29kb PDF).
2006 End-of-Life Conference, April 18-19, 2006 in St. Cloud, MNThe annual conference is quickly approaching! Find the conference brochure, physicians' brochure, and exhibitor and sponsor information (pdf format) on the End-of-Life Conference Web page. Online registration is also available. Contact: Frances Conklin, tel. 651-659-0423; [email protected]
16th Annual Provincial Conference on Palliative and End-of-Life CareSponsored by: Humber/Ontario Palliative Care AssociationApril 23-25, 2006, Marriott Eaton Centre Hotel, Toronto, OntarioContact information: 416-674-2472; e-mail: [email protected]; event web site: www.palliativecare.humber.caFor further information about this program, please contact: Teresa Sottile, Conference Manager, Phone: 416-675-6622, Ext. 4559; Fax: 416-675-0135; Email: [email protected]
National Hospice and Palliative Care Organization 7th Clinical Team Conference and Scientific SymposiumApril 26-28, 2006, Town and Country Resort, San Diego, California

www.nhpco.org/ctc2006
The 7th Clinical Team Conference (CTC) is specifically designed for the hospice/palliative interdisciplinary team, the heart of quality end-of-life care. This unique educational opportunity offers an intensive educational curriculum created to equip, educate, and excite.
Journey of the Heart Conference A Women's Retreat designed for moms who have experienced the loss of a child. A weekend filled with love, hope, peace, comfort and encouragement. The image of spring is one of refreshment and renewal and that's what you'll find at the "Journey of the Heart" Women's Conference located in beautiful Palm Springs, California. May 19-21, 2006, The Doral Desert Princess, Vista Chino at Landau, Palm Springs, CA; http://www.doralpalmsprings.com/gallery.htm... Scholarships Available.
7th International Symposium on Pediatric PainJune 25-29, 2006, Vancouver, BC, Canada
The 7th International Symposium on Pediatric Pain is hosted by the Canadian Pain in Child Health Society for the Special Interest Group on Pain in Childhood of the International Association for the Study of Pain.For more information contact Patrick McGrath through the following web site: www.ispp2006.com
Books/ Articles
The Helper's Journey: Working with People Facing Grief, Loss, and Life-Threatening Illness by Dr. Dale G. LarsonChampaign, Illinois: Research Press, 1993. Paperback, 6 × 9, 292 pages. ISBN 0-87822-344-4
This groundbreaking work, written for both professionals and volunteers, combines an inspiring view of helpers and helping with a focus on meeting the personal, interpersonal, and team challenges of caring for people facing grief, loss, and life-threatening illness. It teaches specific skills and strategies for stress management, effective helping communication, interdisciplinary teamwork, and increased personal and professional growth. Sensitively exploring the inner world of helping, this award-winning book includes numerous case examples and

verbatim disclosures that powerfully convey the joys and sorrows of the helper's journey. I'm Here To Help: A Guide for Caregivers, Hospice Workers, and Volunteersby M. Catherine Ray Revised and expanded edition; New York: Bantam Doubleday Dell Pub (Trade Paperback, 112 pages. Publication date: April 1, 1997. ISBN: 0553377973
Vachon, M. (1987). Team stress in palliative/hospice care. The Hospice Journal, 3, 75-103.Vachon, M. (1997). Recent research into staff stress in palliative care. European Journal of Palliative Care, 4, 99-103.
These two articles by one of the best known researchers who has studied stress in adult hospice and palliative care for many years may offer useful insights for those working in the pediatric field.
Websites:
Managing Stress For Hospice ProfessionalsHospice workers can help each other by volunteering to take cases that may be unduly stressful for co-workers with family crises. Doing Something Nice For Yourself. We are often too generous.www.americanhospice.org/articles/hospicestress.htm
New Tools:
“Come to Your Senses”
This is a program for rejuvenation and renewal for hospital staff. The intent is to provide engaging, imaginative, creative, and participatory ways for staff to have a regular, sustained time to restore themselves during their shift. These six sessions were designed by Alan Johnson, MDiv, Staff Chaplain, and Kelly West, RN, BSN, staff of The Children's Hospital, Denver, Colorado.
The six CDs in this program and the printed material in notebook form offer the structure of six 15-25 minute sessions. Each CD contains a narrative and explanation of the exercises; each notebook provides an outline of each session, a list of materials that are needed, and instructions for the group facilitator. The set is self-contained, meaning that anyone could be the convener of the sessions. Each session focuses on one of the five senses, with the addition of the sixth one, nonsense.

We developed "Come to Your Senses" as we sought a way to bring staff back to themselves and to their center in the midst of their work, and to help them make sense of things. Concentrating on our senses of taste, hearing, touch, smell, and sight brings us to the here and the now and focuses on tangible ways that we can get back in touch with our selves in the cacophony of our daily work. We added nonsense since we can also play, work, and live in situations that do not make sense and yet we can still hang in there and be renewed rather than being drained. It may be one way to make some sense out of nonsense.
All of our senses, even nonsense, can be avenues for rejuvenation!
Come to Your Senses: A program for rejuvenation and renewalOrder formI would like to order ____ Notebook(s) of the program "Come to Your Senses"Suggested donation: $55 for one Notebook, which includes 6 CDs and guidelines.$4.75 Postage (in the US)Total $____ EnclosedPlease make checks payable to:The Children’s Hospital Foundation1245 E. Colfax Ave., Suite 400Denver, CO 80218Name: ____________________________________Organization: ______________________________Address: __________________________________City: ______________________________________State: ______________ Zip Code: ____________Country: __________________________________Phone: ____________________________________E-mail: ____________________________________
For more informationAlan Johnson, Staff Chaplain, MDivThe Children’s Hospital303-864-5350; [email protected] West, BSN, RNThe Children’s Hospital303-861-6511; [email protected]