ngs, a suitable approach for tp53 screening in cll? - eric · ngs, a suitable approach for tp53...
TRANSCRIPT
NGS, a suitable approach forTP53 screening in CLL?
Ferran Nadeu
2nd ERIC WORKSHOP ON TP53 ANALYSIS IN CHRONIC LYMPHOCYTIC LEUKEMIA7-8 November 2017, Stresa (Italy)
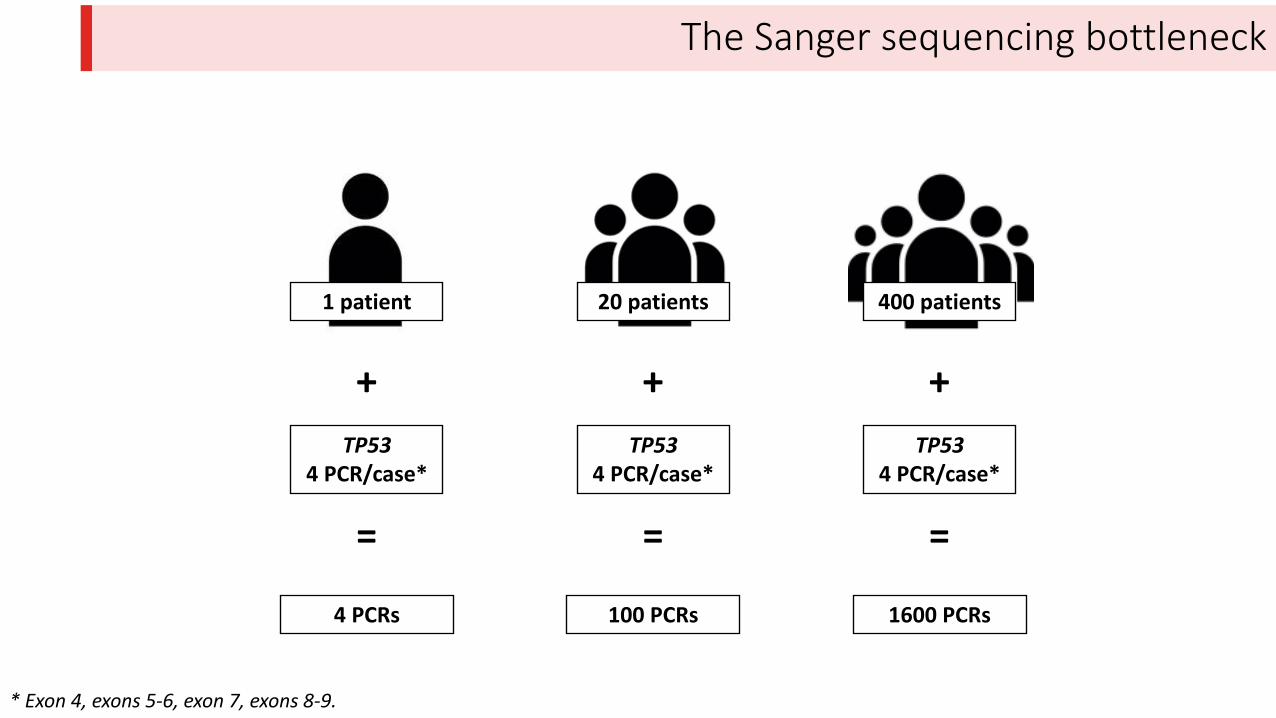
1 patient
TP53
4 PCR/case*
+
* Exon 4, exons 5-6, exon 7, exons 8-9.
=
4 PCRs
20 patients
TP53
4 PCR/case*
+
=
100 PCRs
400 patients
TP53
4 PCR/case*
+
=
1600 PCRs
The Sanger sequencing bottleneck
1 patient
TP53
4 PCR/case*
+
=
4 PCRs
20 patients
TP53
4 PCR/case*
+
=
100 PCRs
400 patients
TP53
4 PCR/case*
+
=
1600 PCRs
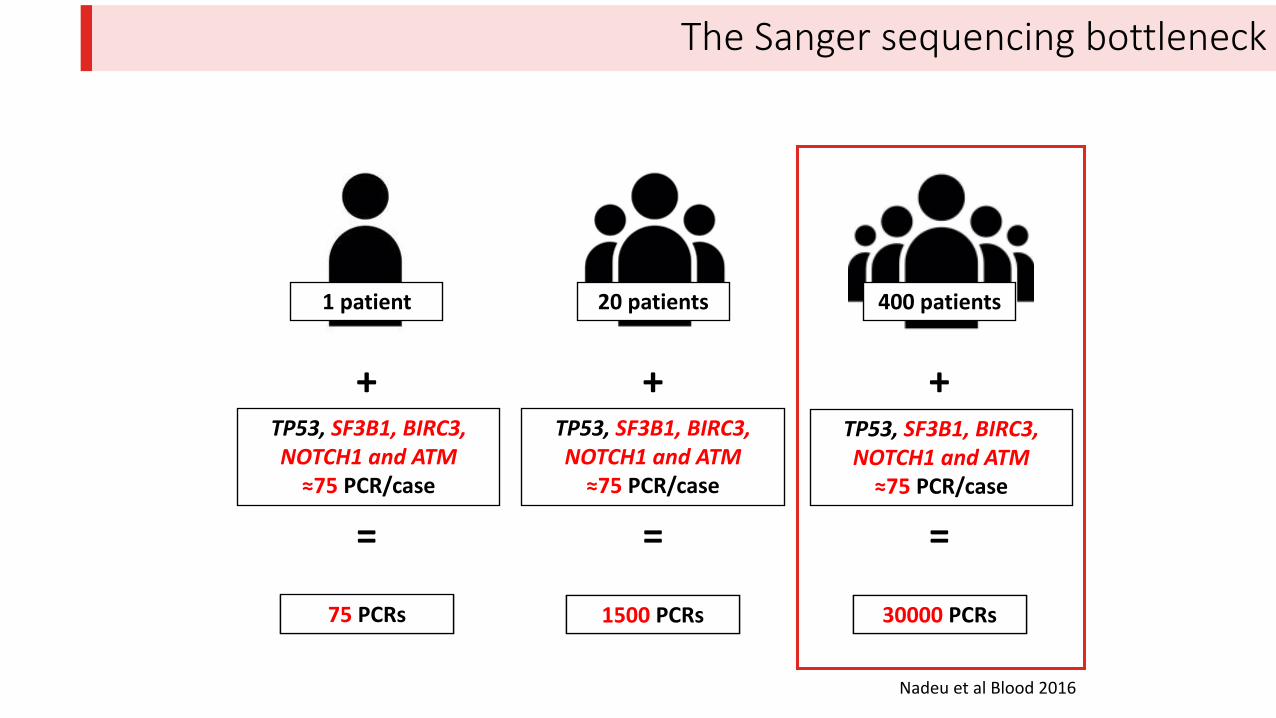
TP53, SF3B1, BIRC3,
NOTCH1 and ATM
≈75 PCR/case
75 PCRs 1500 PCRs
TP53, SF3B1, BIRC3,
NOTCH1 and ATM
≈75 PCR/case
30000 PCRs
TP53, SF3B1, BIRC3,
NOTCH1 and ATM
≈75 PCR/case
The Sanger sequencing bottleneck
Nadeu et al Blood 2016
Outline
1. NGS overcomes this Sanger sequencing bottleneck (focus on the Access-Array system)
2. NGS for TP53 analysis:
a) Access-Array system
b) Comparison of NGS libraries
3. Pros and cons of the use of NGS:
a) Sensitivity
b) Bioinformatic analysis
c) Accuracy
d) Possibility to study several genes simultaneously (i.e. panel of genes)
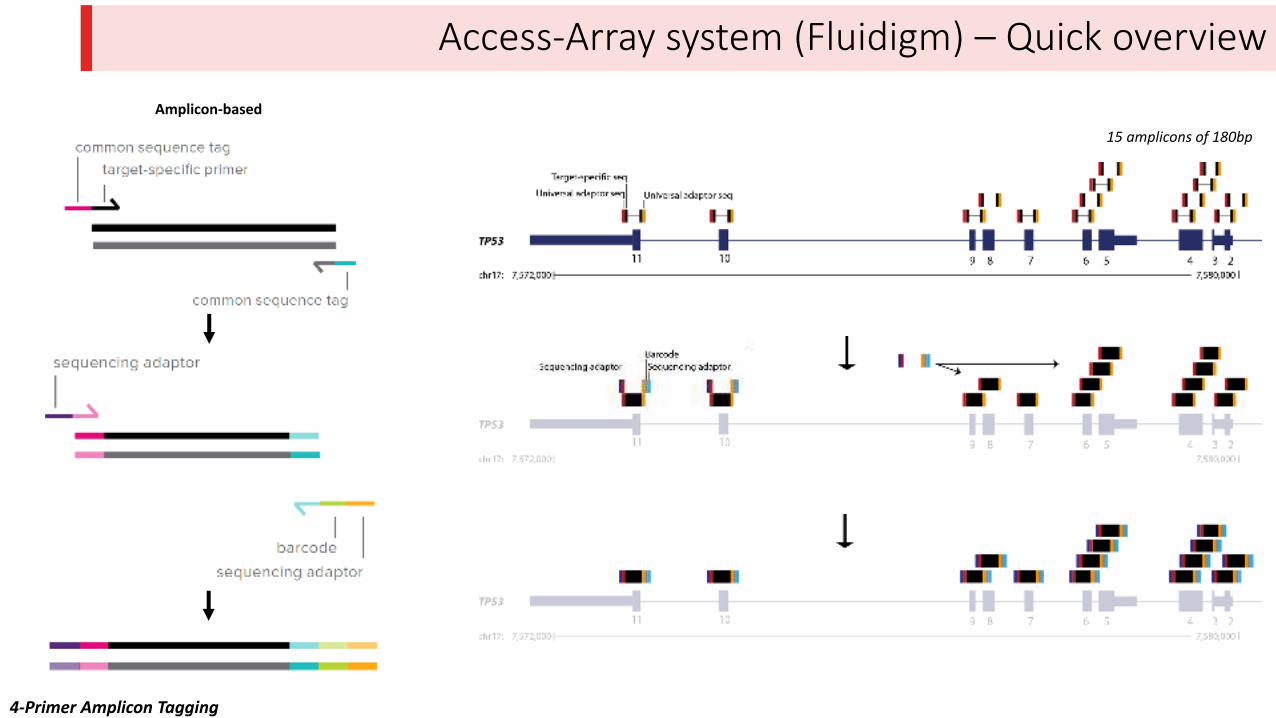
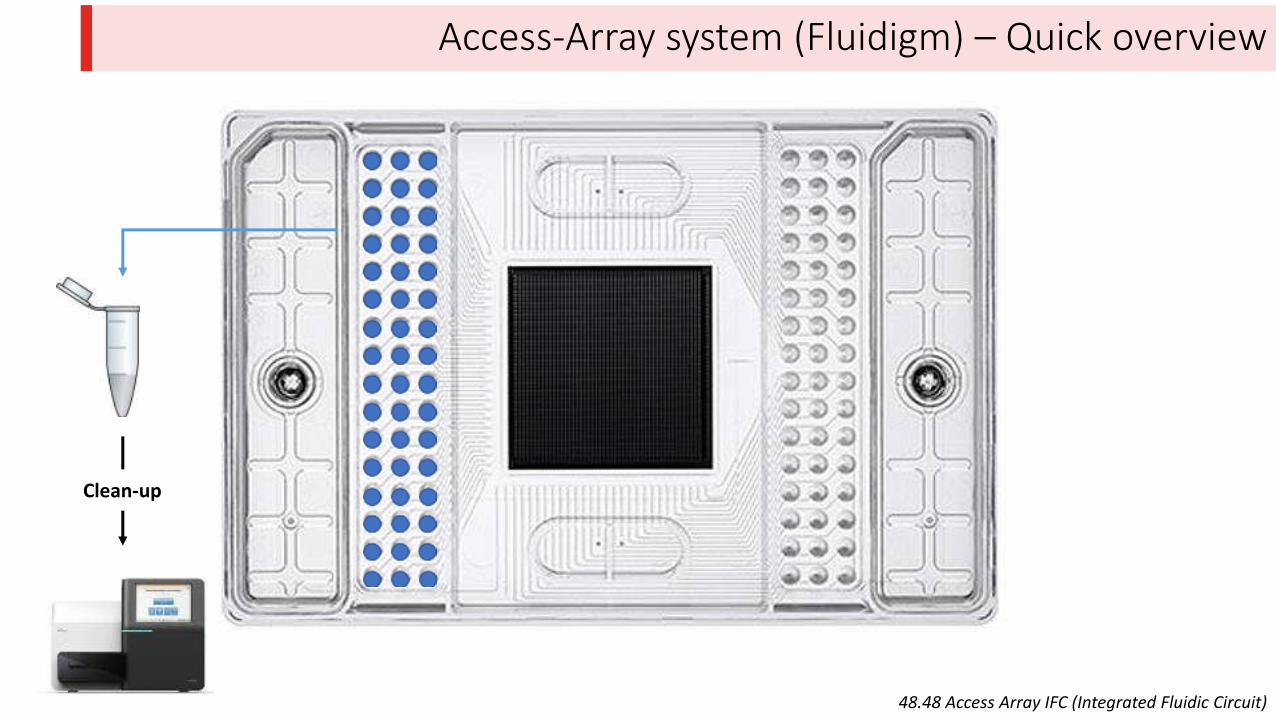
Access-Array system (Fluidigm) – Quick overview
Amplicon-based
15 amplicons of 180bp
4-Primer Amplicon Tagging
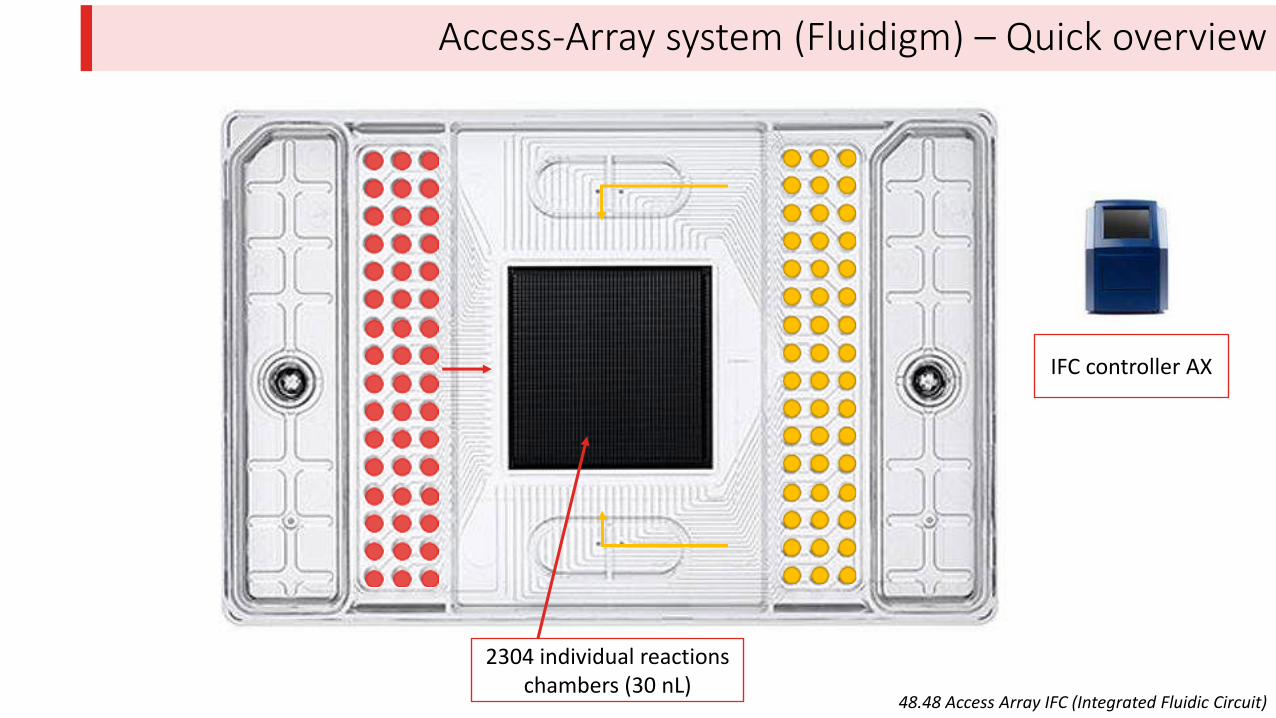
Access-Array system (Fluidigm) – Quick overview
48.48 Access Array IFC (Integrated Fluidic Circuit)
IFC controller AX
2304 individual reactions
chambers (30 nL)
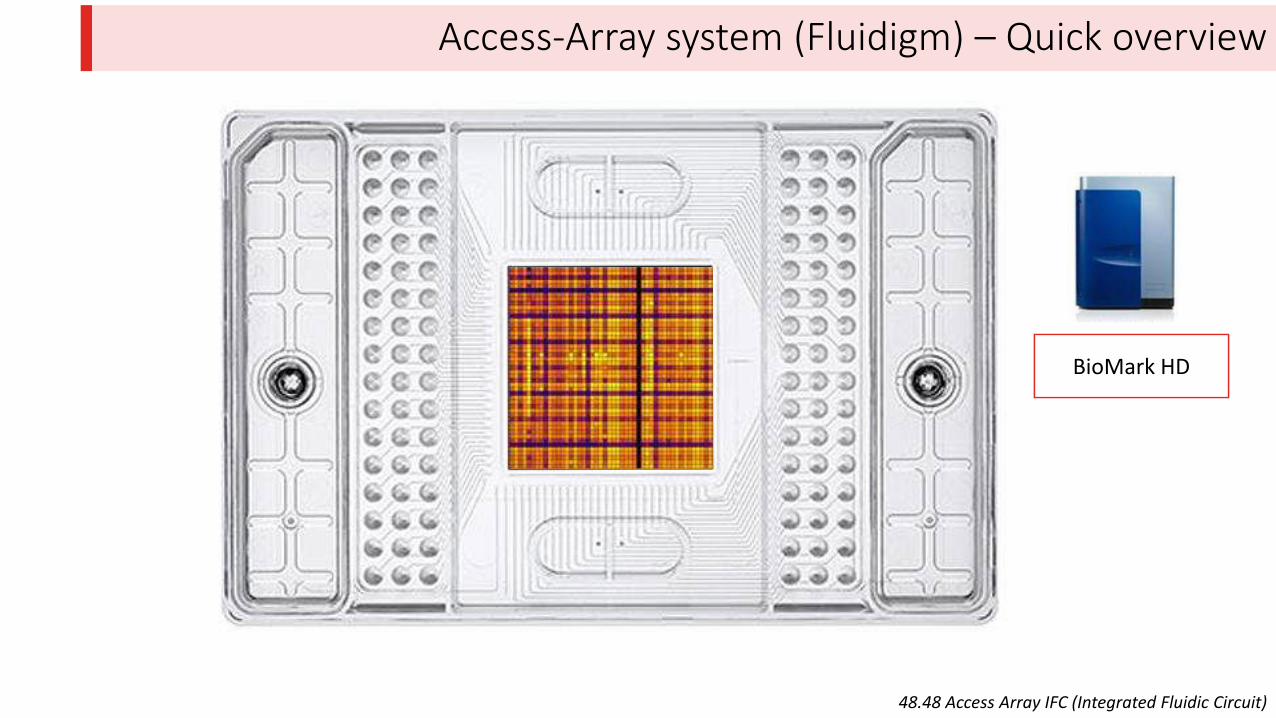
Access-Array system (Fluidigm) – Quick overview
48.48 Access Array IFC (Integrated Fluidic Circuit)
IFC controller AX BioMark HD
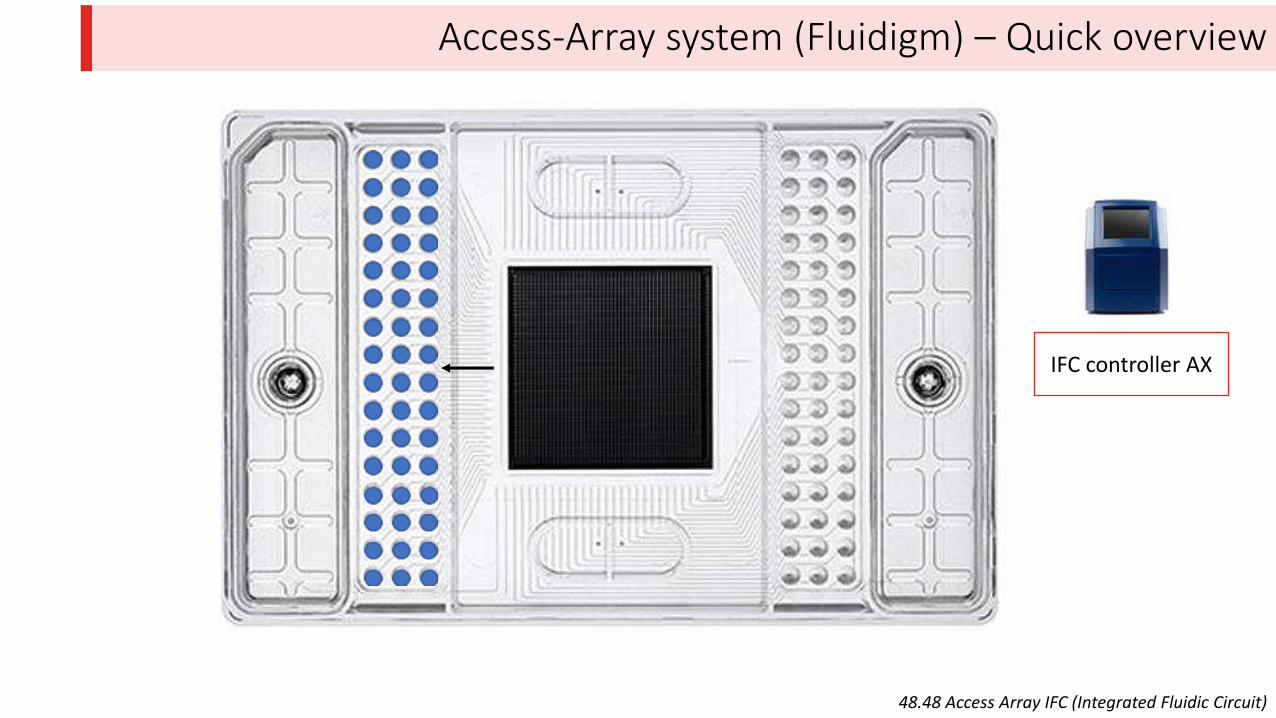
Access-Array system (Fluidigm) – Quick overview
48.48 Access Array IFC (Integrated Fluidic Circuit)
IFC controller AX
Access-Array system (Fluidigm) – Quick overview
48.48 Access Array IFC (Integrated Fluidic Circuit)
Clean-up
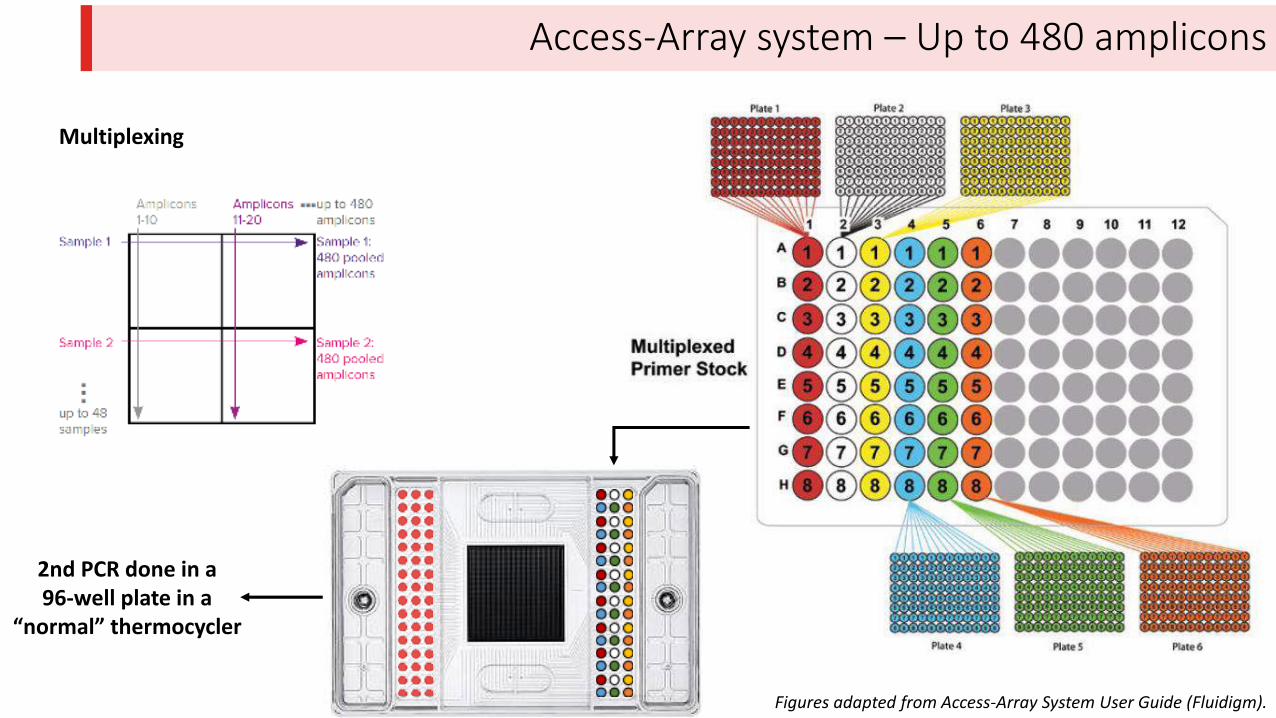
Access-Array system – Up to 480 amplicons
Multiplexing
Figures adapted from Access-Array System User Guide (Fluidigm).
2nd PCR done in a
96-well plate in a
or al ther ocycler
Outline
1. NGS overcomes this Sanger sequencing bottleneck (Access-Array system)
2. NGS for TP53 analysis:
a) Access-Array system
b) Comparison of NGS libraries
3. Pros and cons of the use of NGS:
a) Sensitivity
b) Bioinformatic analysis
c) Accuracy
d) Possibility to study several genes simultaneously
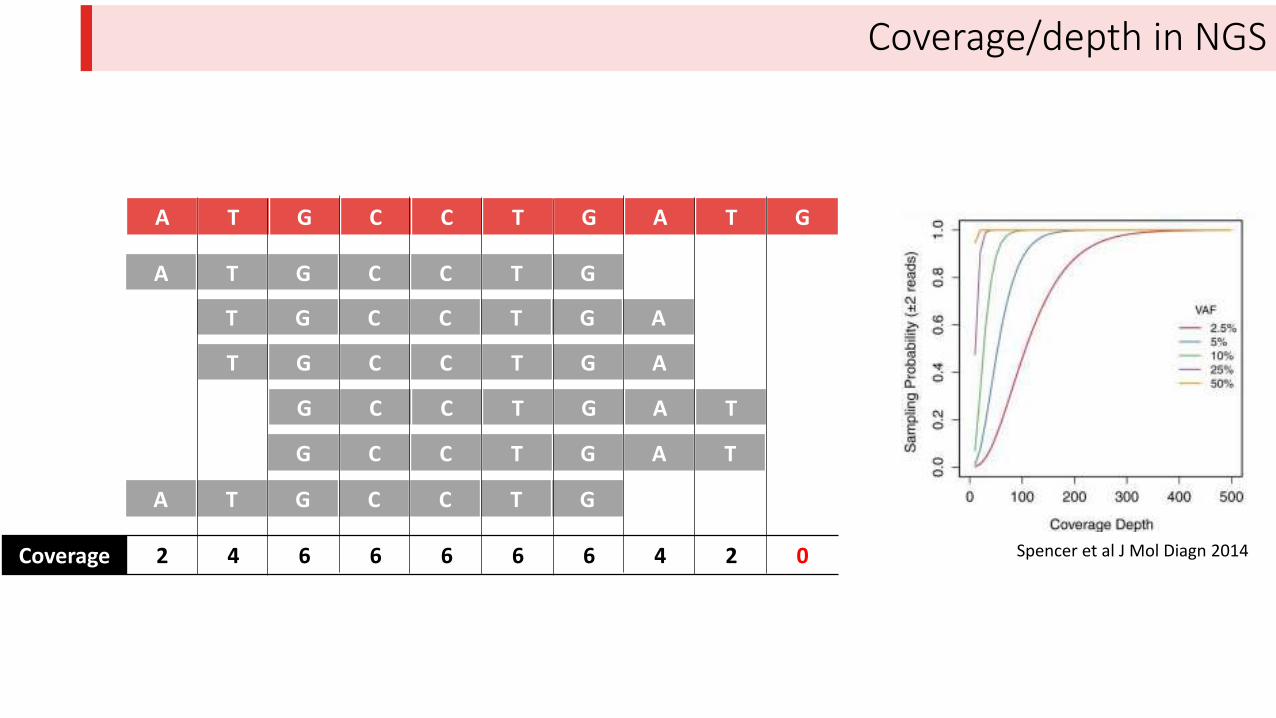
Coverage/depth in NGS
A T G C C T G A T G
Spencer et al J Mol Diagn 20142 4 6 6 6 6 6 4 2 0Coverage
T G C C T G A
A T G C C T G
G C C T G A T
T G C C T G A
G C C T G A T
A T G C C T G
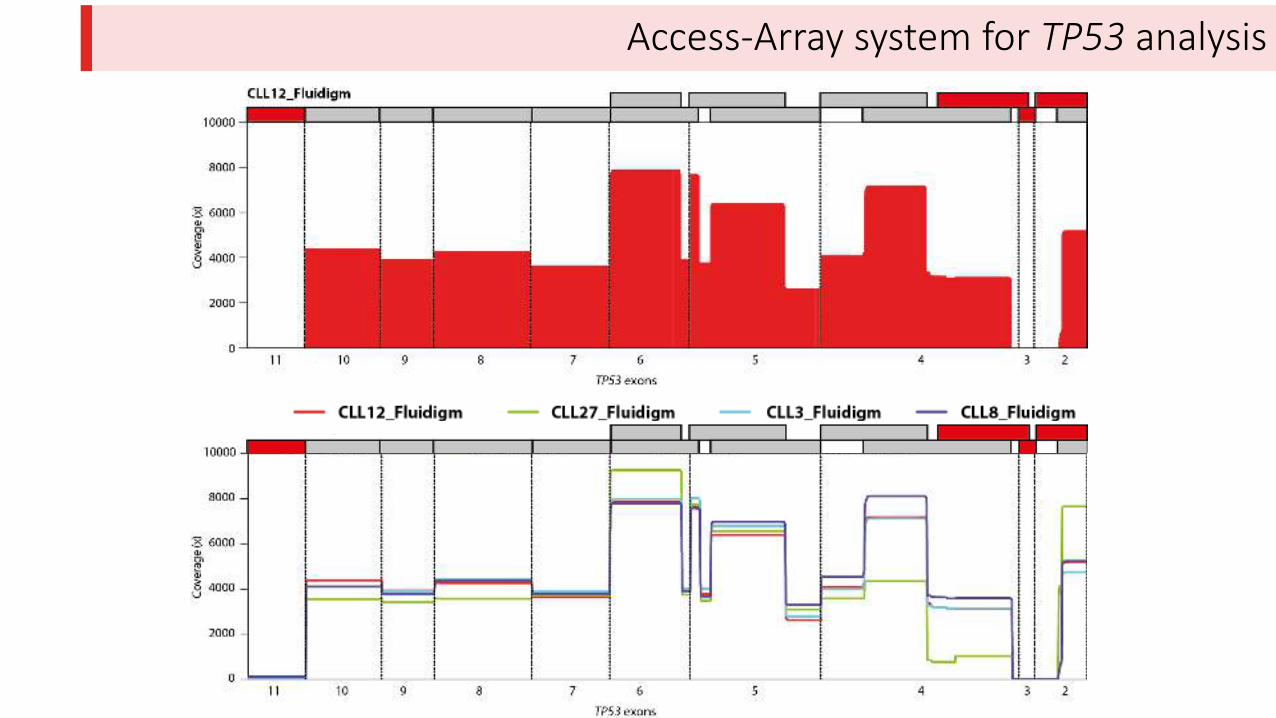
Access-Array system for TP53 analysis
Access-Array system (Fluidigm) – Coverage
Nadeu et al Blood 2016
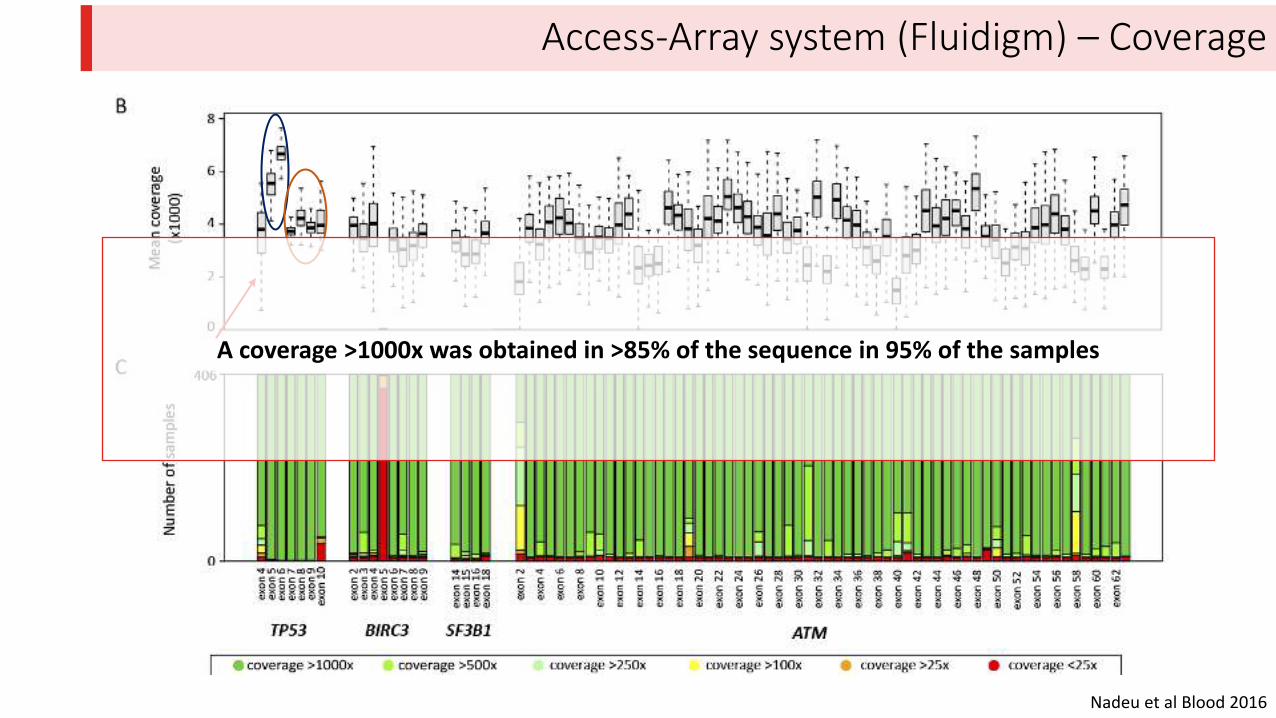
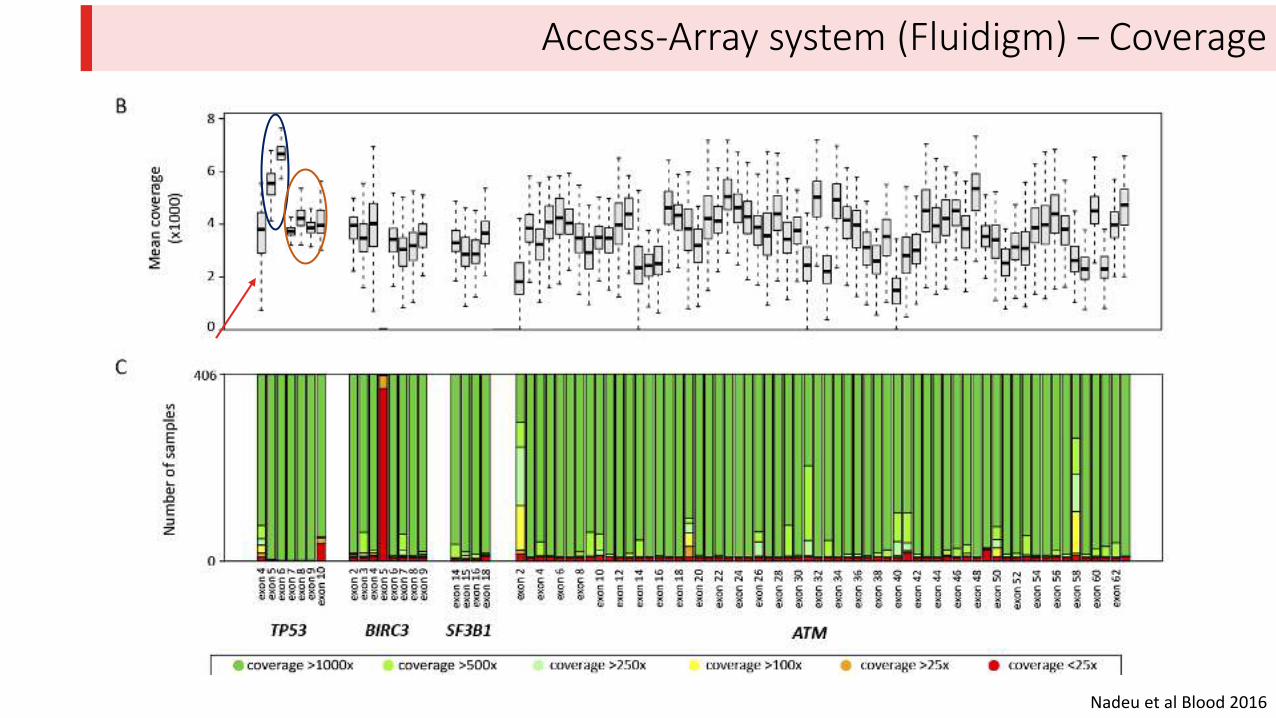
Access-Array system (Fluidigm) – Coverage
Nadeu et al Blood 2016
A coverage >1000x was obtained in >85% of the sequence in 95% of the samples
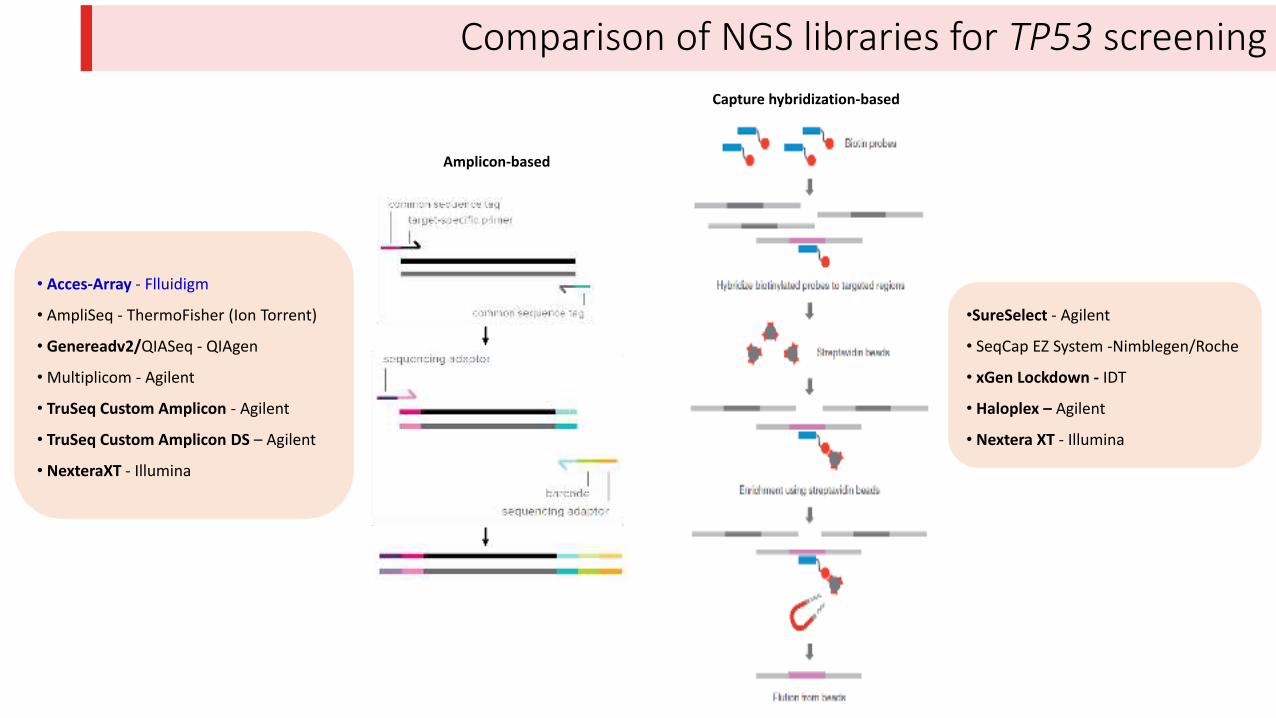
Capture hybridization-based
Amplicon-based
• Acces-Array - Flluidigm
• AmpliSeq - ThermoFisher (Ion Torrent)
• Genereadv2/QIASeq - QIAgen
•Multiplicom - Agilent
• TruSeq Custom Amplicon - Agilent
• TruSeq Custom Amplicon DS – Agilent
• NexteraXT - Illumina
•SureSelect - Agilent
• SeqCap EZ System -Nimblegen/Roche
• xGen Lockdown - IDT
• Haloplex – Agilent
• Nextera XT - Illumina
Comparison of NGS libraries for TP53 screening
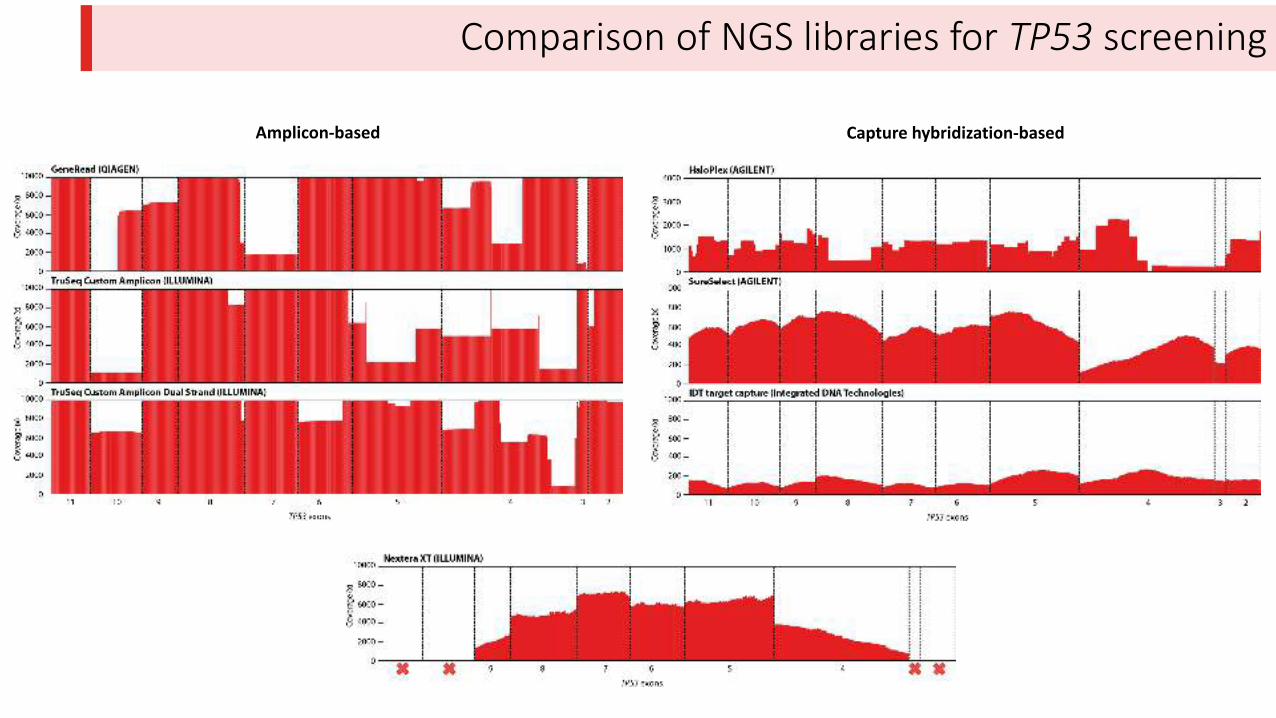
Comparison of NGS libraries for TP53 screening
Amplicon-based Capture hybridization-based
Outline
1. NGS overcomes this Sanger sequencing bottleneck (Access-Array system)
2. NGS for TP53 analysis:
a) Access-Array system
b) Comparison of NGS libraries
3. Pros and cons of the use of NGS:
a) Sensitivity
b) Bioinformatic analysis
c) Accuracy
d) Possibility to study several genes simultaneously
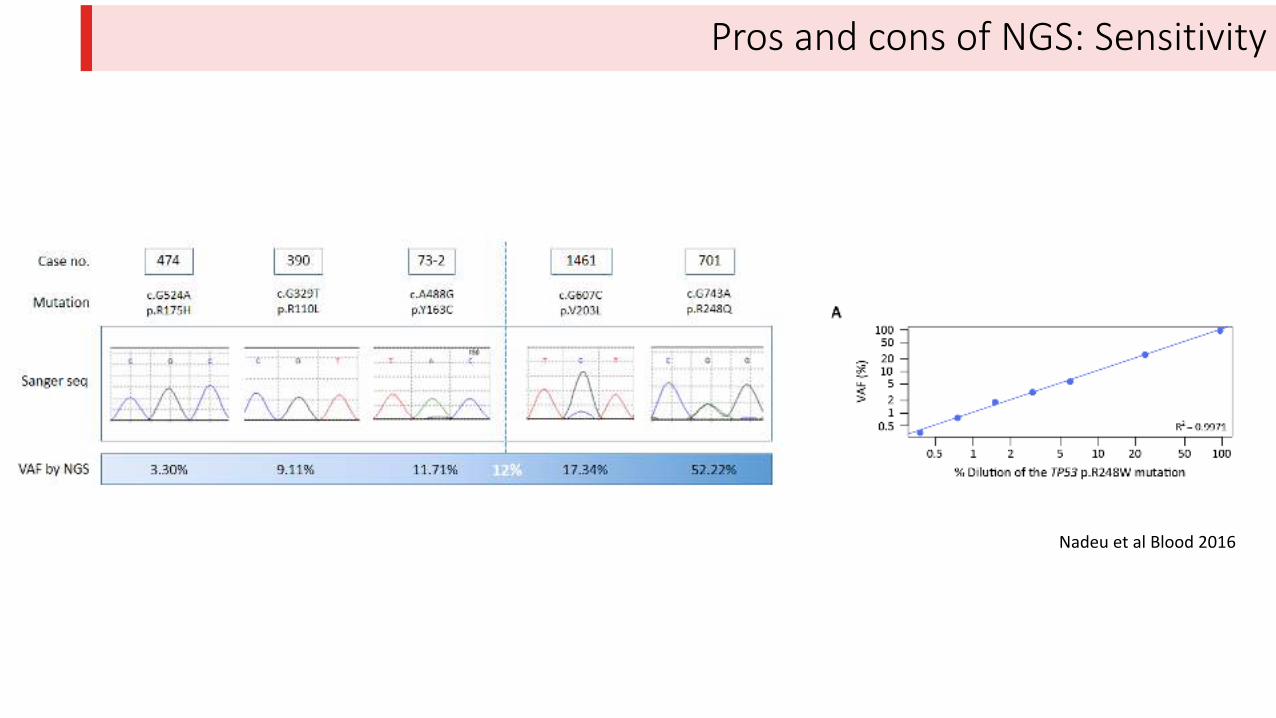
Pros and cons of NGS: Sensitivity
Nadeu et al Blood 2016
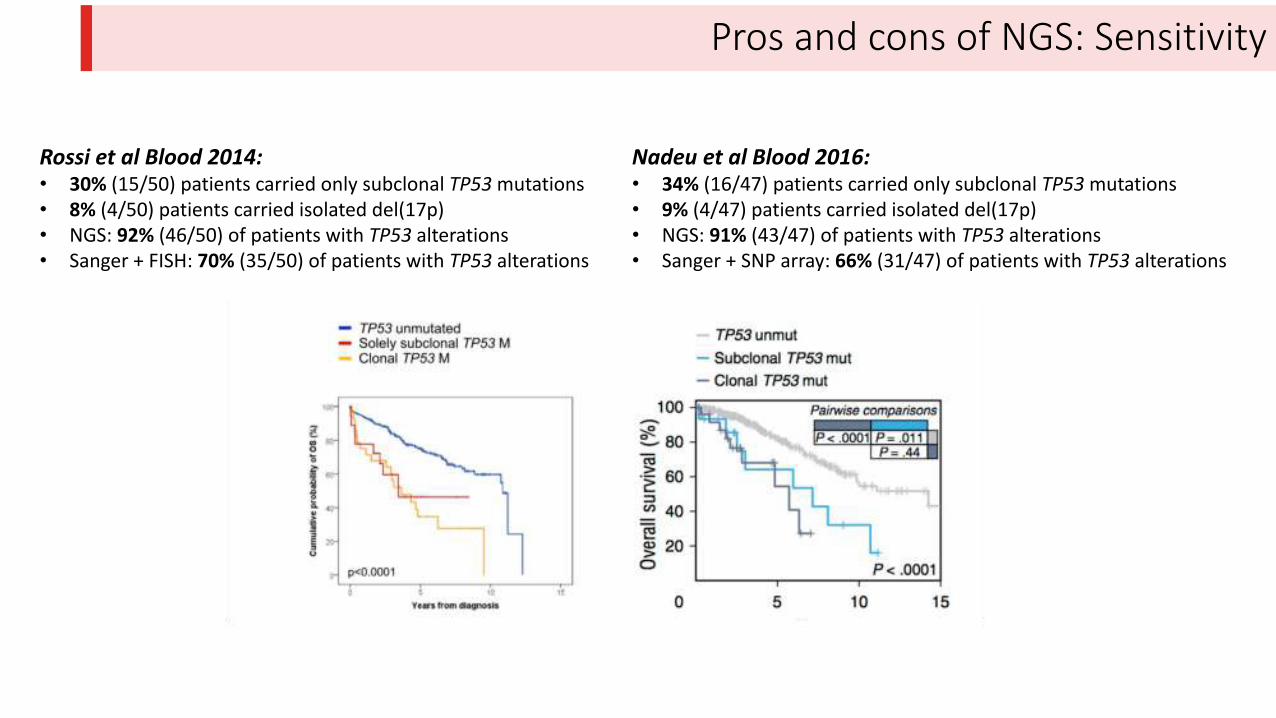
Pros and cons of NGS: Sensitivity
Rossi et al Blood 2014:
• 30% (15/50) patients carried only subclonal TP53 mutations
• 8% (4/50) patients carried isolated del(17p)
• NGS: 92% (46/50) of patients with TP53 alterations
• Sanger + FISH: 70% (35/50) of patients with TP53 alterations
Nadeu et al Blood 2016:
• 34% (16/47) patients carried only subclonal TP53 mutations
• 9% (4/47) patients carried isolated del(17p)
• NGS: 91% (43/47) of patients with TP53 alterations
• Sanger + SNP array: 66% (31/47) of patients with TP53 alterations
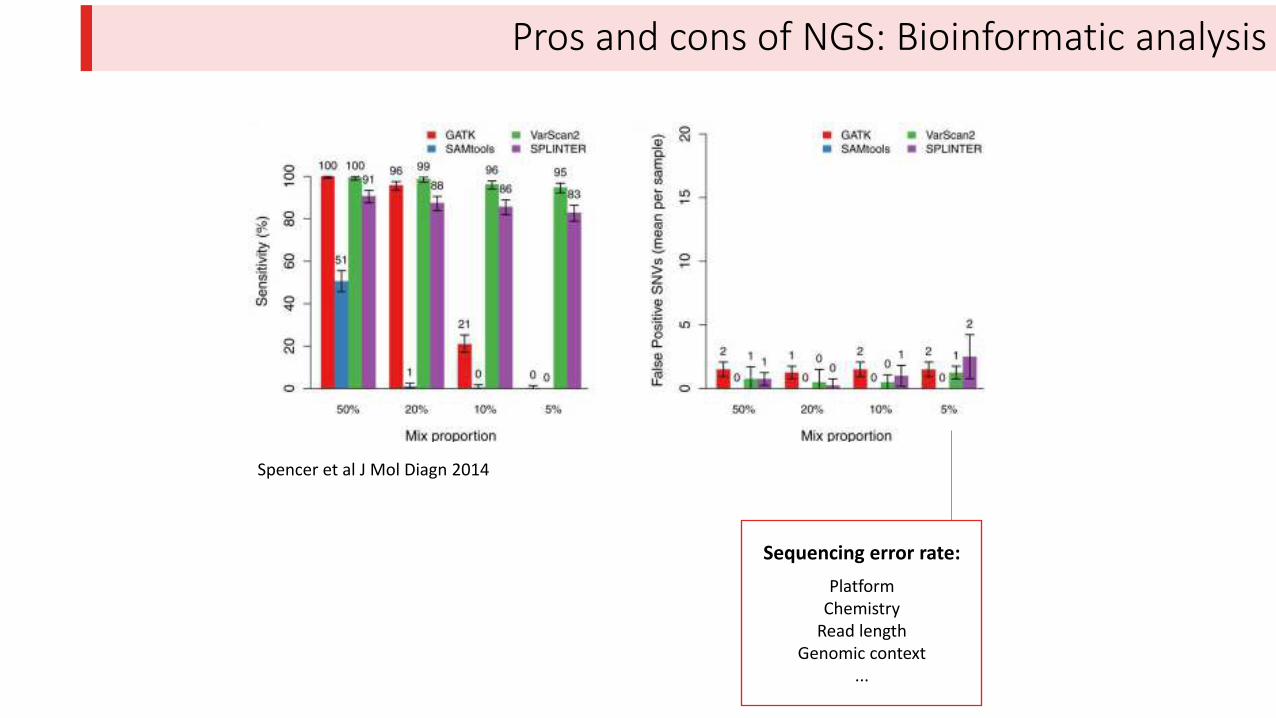
Pros and cons of NGS: Bioinformatic analysis
Sequencing error rate:
Platform
Chemistry
Read length
Genomic context
...
Spencer et al J Mol Diagn 2014
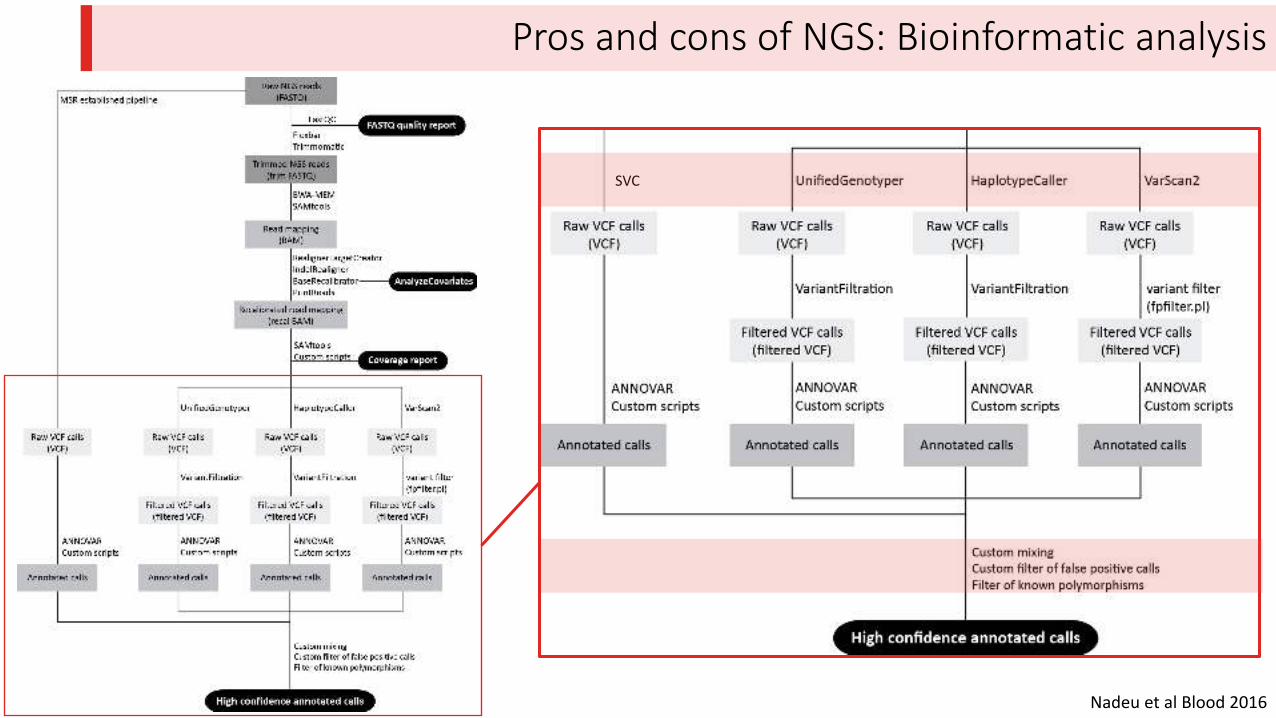
Pros and cons of NGS: Bioinformatic analysis
SVC
Nadeu et al Blood 2016
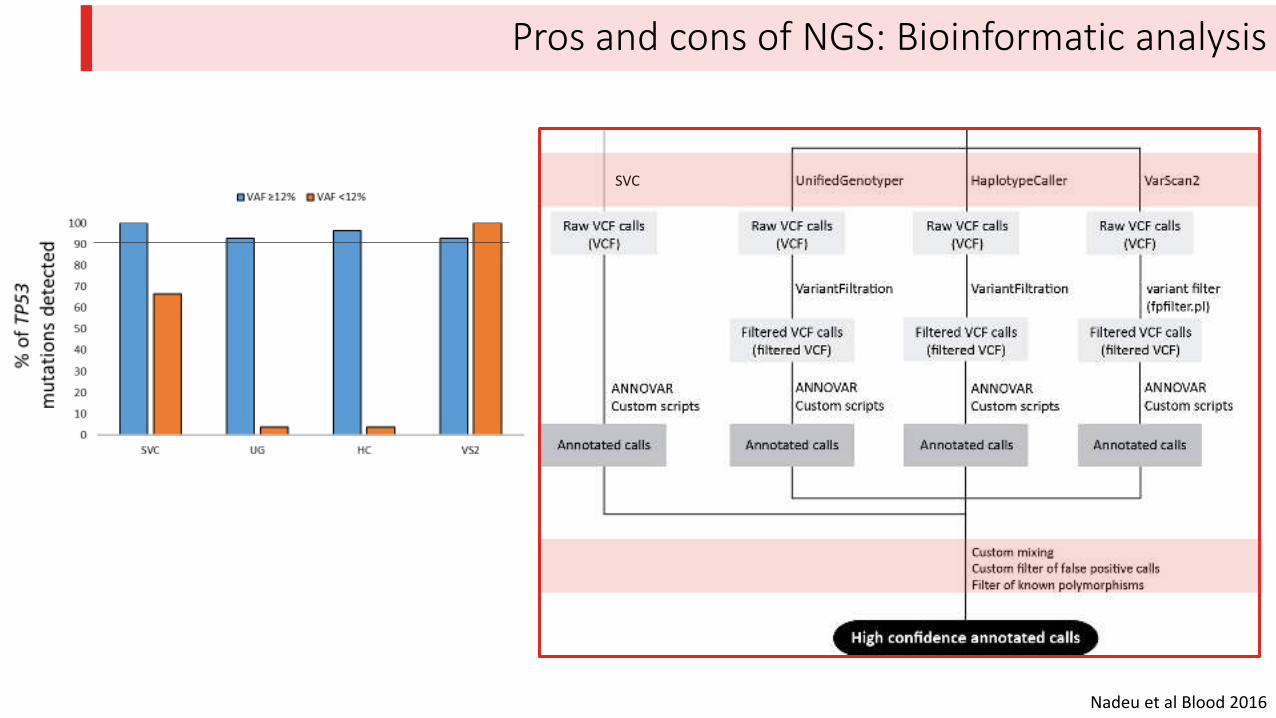
Pros and cons of NGS: Bioinformatic analysis
SVC
Nadeu et al Blood 2016
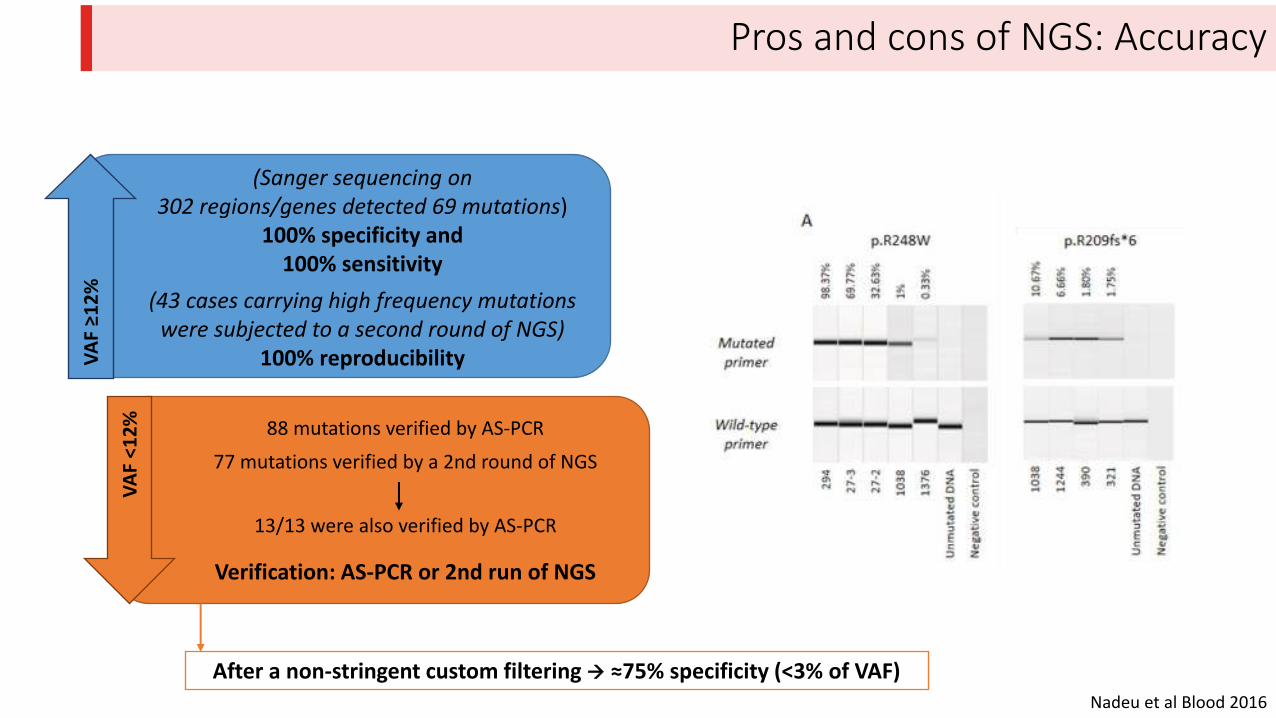
Pros and cons of NGS: Accuracy
Nadeu et al Blood 2016
VAF ≥
%
VA
F <
12
%
(Sanger sequencing on
302 regions/genes detected 69 mutations)
100% specificity and
100% sensitivity
(43 cases carrying high frequency mutations
were subjected to a second round of NGS)
100% reproducibility
88 mutations verified by AS-PCR
77 mutations verified by a 2nd round of NGS
13/13 were also verified by AS-PCR
Verification: AS-PCR or 2nd run of NGS
After a non-stringent custom filtering ≈75% specificity < % of VAF
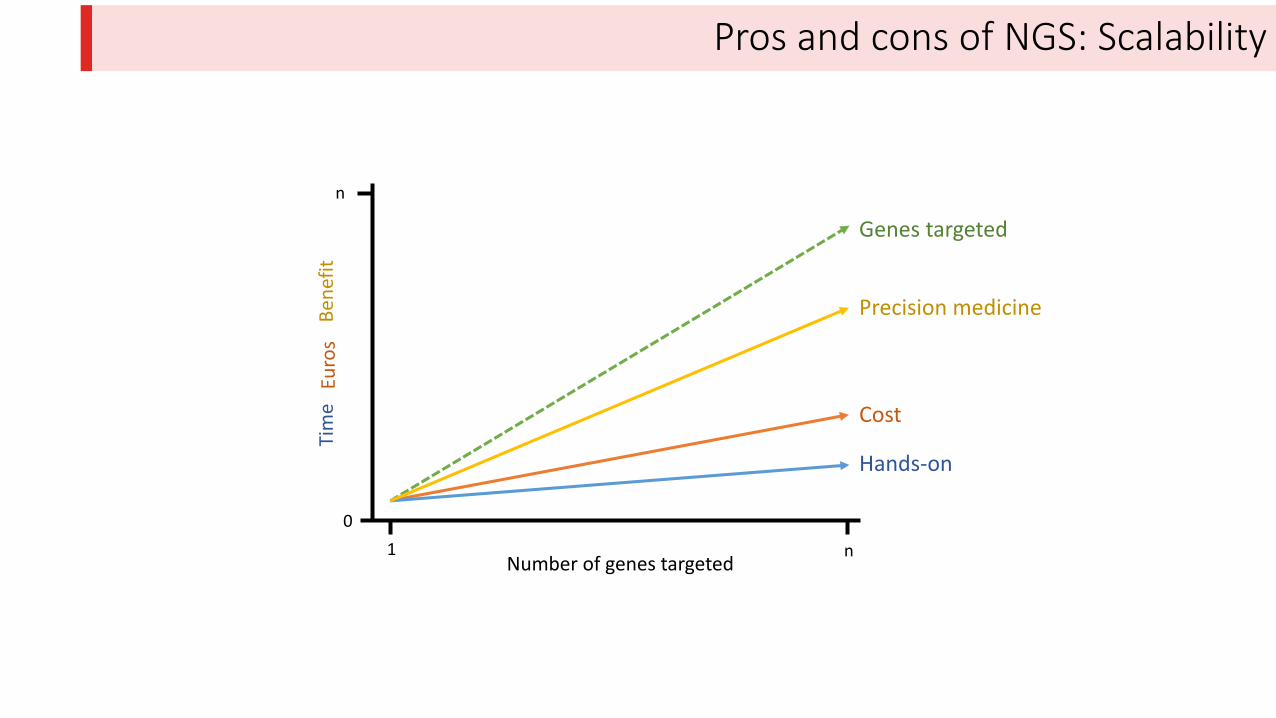
Pros and cons of NGS: Scalability
Genes targeted
Cost
Hands-on
Precision medicine
1 nNumber of genes targeted
n
0
Tim
eE
uro
sB
en
efi
t
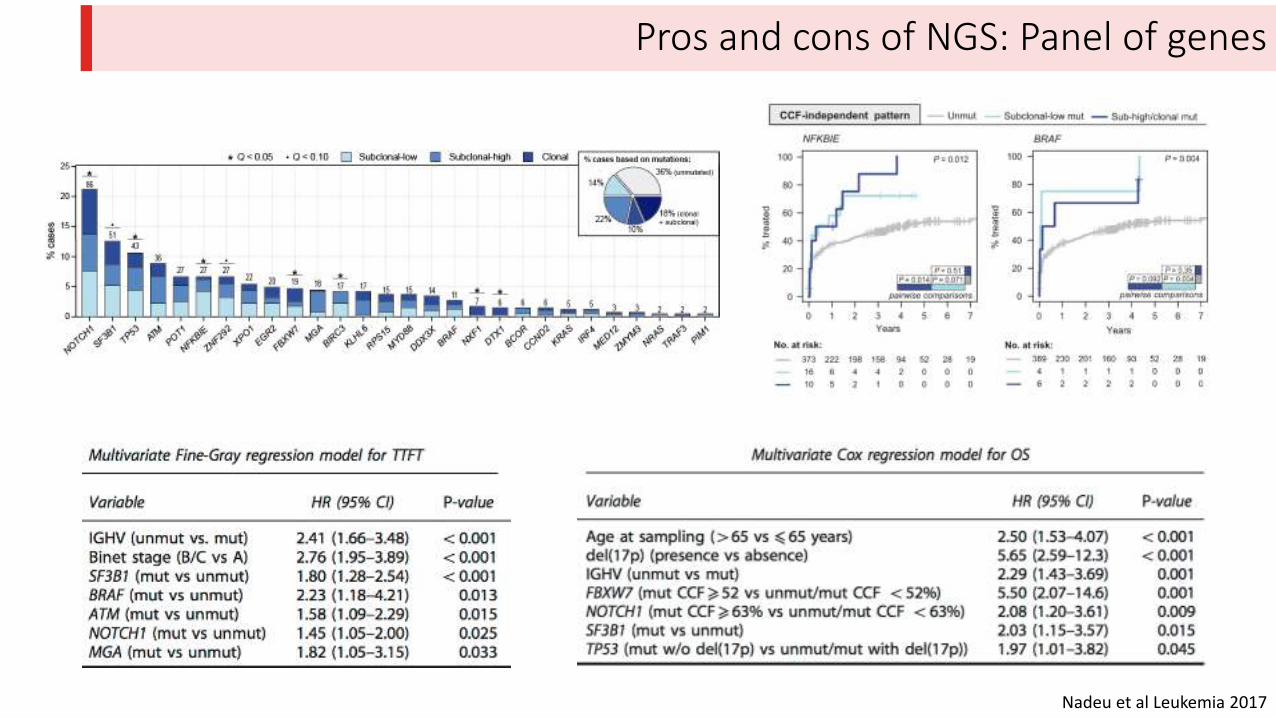
Pros and cons of NGS: Panel of genes
Nadeu et al Leukemia 2017
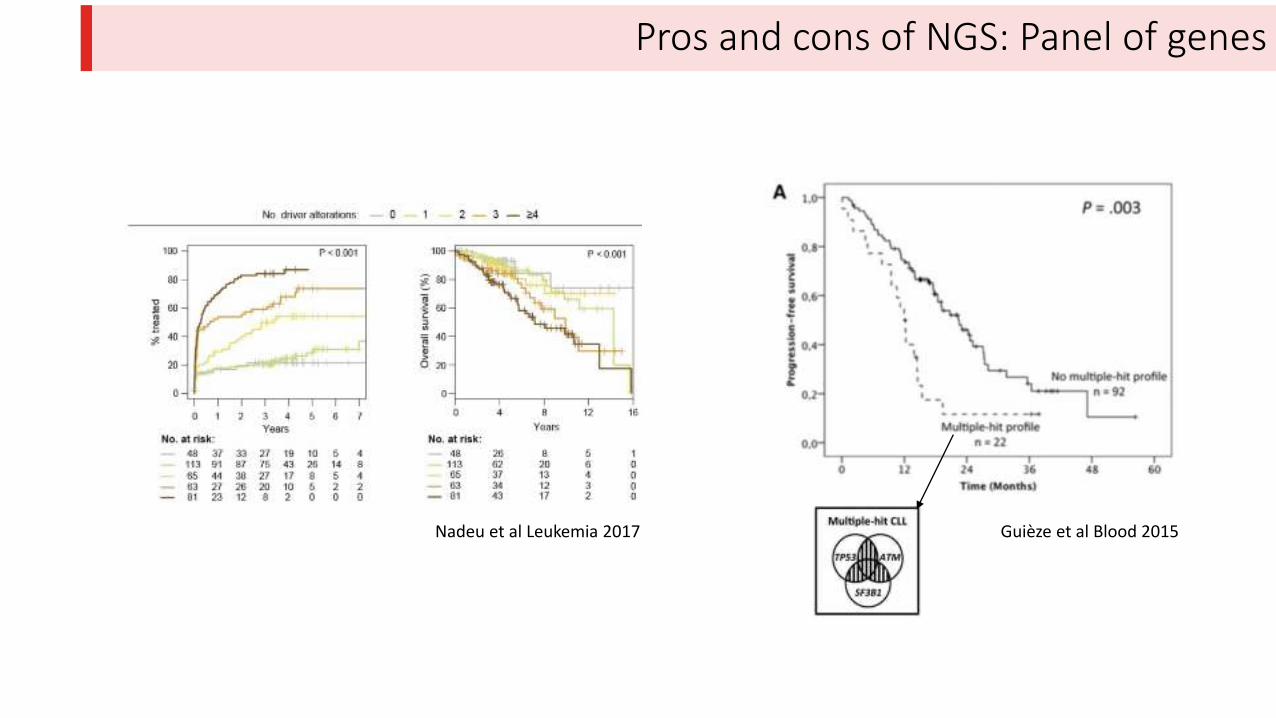
Pros and cons of NGS: Panel of genes
Nadeu et al Leukemia 2017 Guièze et al Blood 2015
NGS libraries and TP53
• Easy design
• Short hands-on time
• Compatible with multiple sequencing platforms (Illumina, Ion Torrent, etc.)
• Percentage of amplification success ≥95%, and good accuracy (>90% mapping to target)
• Uniform coverage
• Highly sensitive and reproducible approach to detect mutations in TP53 and other genes in clinical samples
Take home messages
NGS in the clinics
• Many different library approaches work well.
• We may face a CLL (or lymphoma) panel rather than analyzing an individual gene
• Which genes? How we validate it in larger cohorts?
• Should we sequence the normal DNA? It could be useful for the study of ATM mutations and for the variant calling.
Bioinformatic approach (still not well defined)
• A gold-standard bioinformatic pipeline for deep-targeted NGS is not yet stablished.
• Limited accuracy in the detection of clinically relevant very low VAF mutations. Verification may be needed.
• Feasible identification of CNA [del(17p), del(11q)] from the same NGS data is still pending.
…should all this be uniform for the different centers?
Elías Campo
Cristina Capdevila
Sara Guijarro
Julio Delgado
Guillem Clot
Thank you for your attention!
Acknowledgment
Anna Enjuanes
Magda Pinyol
Helena Suárez-Cisneros
Montse Sanchez
Laura Pla