newsinalamyloidosisash2016 - semantic scholar · society of hematology (ash) meeting in 2016 are...
TRANSCRIPT
review
memo (2017) 10:66–71DOI 10.1007/s12254-017-0332-6
News in AL Amyloidosis ASH 2016
A rapidly evolving field of investigation
Hermine Agis
Received: 8 March 2017 / Accepted: 18 April 2017 / Published online: 24 May 2017© The Author(s) 2017. This article is an open access publication.
Summary Amyloidosis is a rare but life-threateningprotein misfolding disease. The early diagnosis andenrollment of patients into multicentre trials is ofgreat importance, as is the need for intensive collab-oration between multiple medical departments andexperienced specialists. In the following review, themost interesting abstracts from the annual AmericanSociety of Hematology (ASH) meeting in 2016 arepresented. The topics include the limitations of es-tablished biomarkers in risk assessment and responseevaluation, the introduction of a new biomarker, thecomparison of different treatment sequences and theefficacy of a multiple drug regimen in light-chain (AL)amyloidosis.
Keywords Protein misfolding disease · Antifibrillaryantibody · NEOD001 · 11-1F4 · Anti-SAP antibody
Introduction
Systemic light-chain (AL) amyloidosis is a rare andlife-threatening disease characterised by excessivelight-chain depositions in the tissues and organs. Thetoxic light-chain paraprotein originates from clonalplasma cells or from a small B-cell clone [1]. The mostcommonly involved organs are the heart, kidneys andthe liver along with the gastrointestinal tract andthe peripheral and autonomic nervous systems. Thepattern of organ involvement determines the clini-cal presentation, and the symptoms are often veryunspecific: fatigue, dyspnea, ankle and leg edema,weight loss, diarrhea, obstipation and orthostatic hy-
H. Agis, M.D. (�)Department of Internal Medicine I, Division ofOncology, Medical University Vienna, WähringerGürtel 10–20, 1090 Vienna, [email protected]
potension [2, 3]. However, there are some specific butrare signs and symptoms suggesting the presence ofamyloidosis. These include periorbital ecchymosis,an enlarged tongue, bilateral carpal tunnel syndromesand nail dystrophy [2].
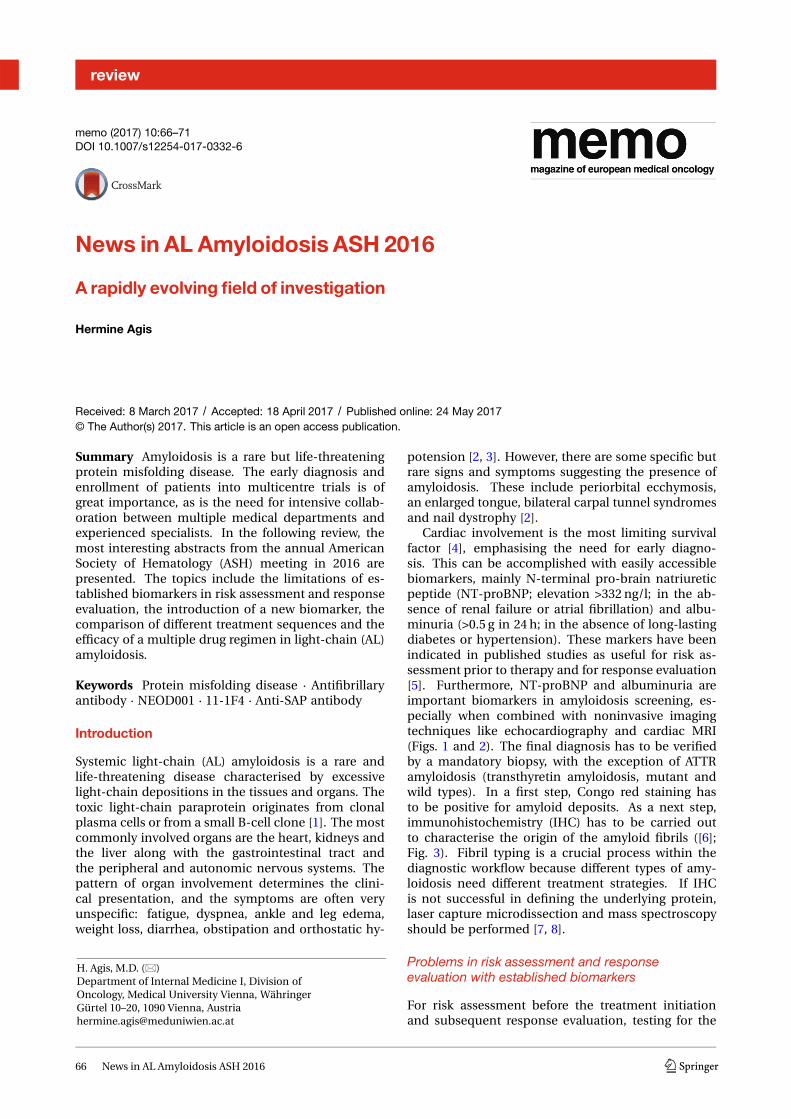
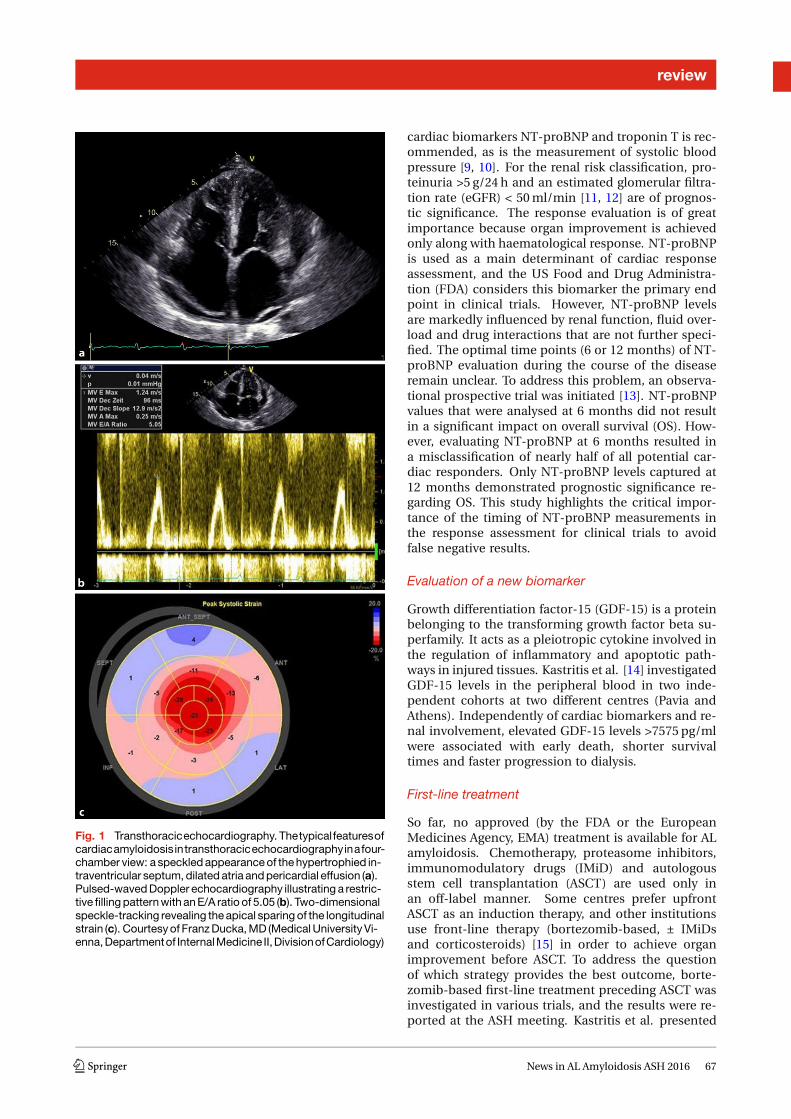
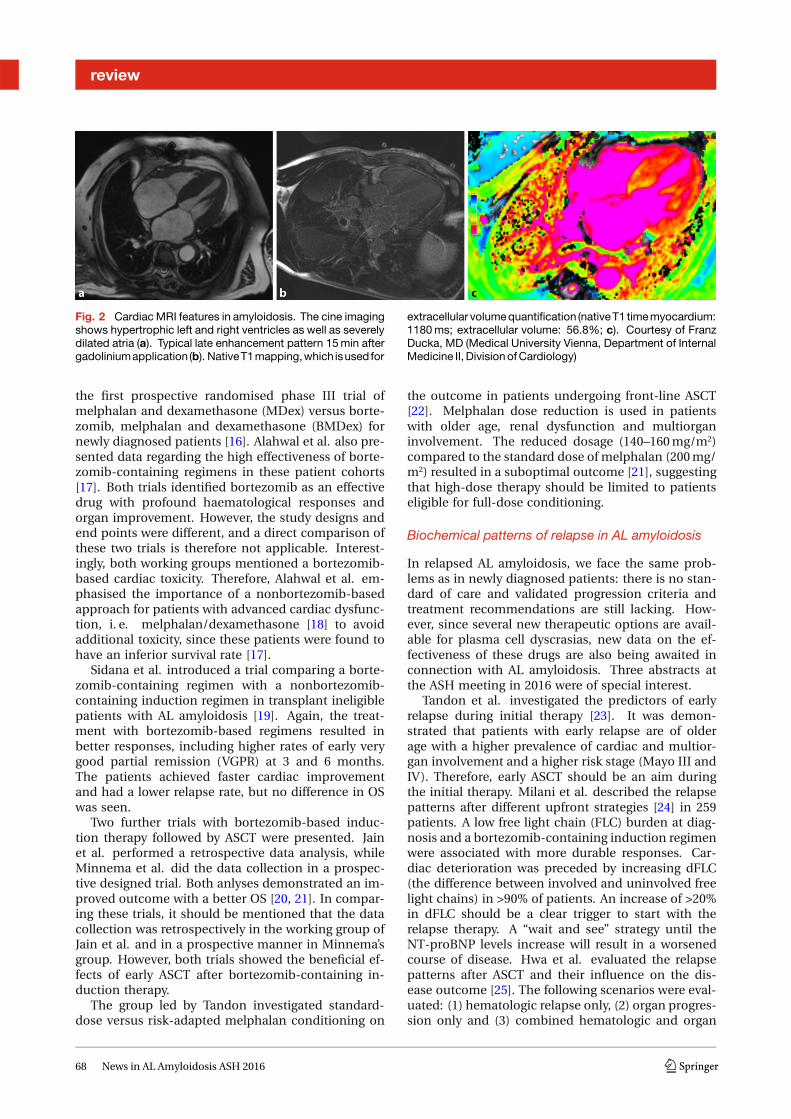
Cardiac involvement is the most limiting survivalfactor [4], emphasising the need for early diagno-sis. This can be accomplished with easily accessiblebiomarkers, mainly N-terminal pro-brain natriureticpeptide (NT-proBNP; elevation >332 ng/l; in the ab-sence of renal failure or atrial fibrillation) and albu-minuria (>0.5 g in 24 h; in the absence of long-lastingdiabetes or hypertension). These markers have beenindicated in published studies as useful for risk as-sessment prior to therapy and for response evaluation[5]. Furthermore, NT-proBNP and albuminuria areimportant biomarkers in amyloidosis screening, es-pecially when combined with noninvasive imagingtechniques like echocardiography and cardiac MRI(Figs. 1 and 2). The final diagnosis has to be verifiedby a mandatory biopsy, with the exception of ATTRamyloidosis (transthyretin amyloidosis, mutant andwild types). In a first step, Congo red staining hasto be positive for amyloid deposits. As a next step,immunohistochemistry (IHC) has to be carried outto characterise the origin of the amyloid fibrils ([6];Fig. 3). Fibril typing is a crucial process within thediagnostic workflow because different types of amy-loidosis need different treatment strategies. If IHCis not successful in defining the underlying protein,laser capture microdissection and mass spectroscopyshould be performed [7, 8].
Problems in risk assessment and responseevaluation with established biomarkers
For risk assessment before the treatment initiationand subsequent response evaluation, testing for the
66 News in AL Amyloidosis ASH 2016 K
review
Fig. 1 Transthoracicechocardiography. Thetypicalfeaturesofcardiacamyloidosisintransthoracicechocardiographyinafour-chamber view: a speckled appearance of the hypertrophied in-traventricular septum, dilated atria and pericardial effusion (a).Pulsed-waved Doppler echocardiography illustrating a restric-tive filling pattern with an E/A ratio of 5.05 (b). Two-dimensionalspeckle-tracking revealing the apical sparing of the longitudinalstrain (c). Courtesy of Franz Ducka, MD (Medical University Vi-enna, Departmentof InternalMedicine II,DivisionofCardiology)
cardiac biomarkers NT-proBNP and troponin T is rec-ommended, as is the measurement of systolic bloodpressure [9, 10]. For the renal risk classification, pro-teinuria >5 g/24 h and an estimated glomerular filtra-tion rate (eGFR) < 50ml/min [11, 12] are of prognos-tic significance. The response evaluation is of greatimportance because organ improvement is achievedonly along with haematological response. NT-proBNPis used as a main determinant of cardiac responseassessment, and the US Food and Drug Administra-tion (FDA) considers this biomarker the primary endpoint in clinical trials. However, NT-proBNP levelsare markedly influenced by renal function, fluid over-load and drug interactions that are not further speci-fied. The optimal time points (6 or 12 months) of NT-proBNP evaluation during the course of the diseaseremain unclear. To address this problem, an observa-tional prospective trial was initiated [13]. NT-proBNPvalues that were analysed at 6 months did not resultin a significant impact on overall survival (OS). How-ever, evaluating NT-proBNP at 6 months resulted ina misclassification of nearly half of all potential car-diac responders. Only NT-proBNP levels captured at12 months demonstrated prognostic significance re-garding OS. This study highlights the critical impor-tance of the timing of NT-proBNP measurements inthe response assessment for clinical trials to avoidfalse negative results.
Evaluation of a new biomarker
Growth differentiation factor-15 (GDF-15) is a proteinbelonging to the transforming growth factor beta su-perfamily. It acts as a pleiotropic cytokine involved inthe regulation of inflammatory and apoptotic path-ways in injured tissues. Kastritis et al. [14] investigatedGDF-15 levels in the peripheral blood in two inde-pendent cohorts at two different centres (Pavia andAthens). Independently of cardiac biomarkers and re-nal involvement, elevated GDF-15 levels >7575 pg/mlwere associated with early death, shorter survivaltimes and faster progression to dialysis.
First-line treatment
So far, no approved (by the FDA or the EuropeanMedicines Agency, EMA) treatment is available for ALamyloidosis. Chemotherapy, proteasome inhibitors,immunomodulatory drugs (IMiD) and autologousstem cell transplantation (ASCT) are used only inan off-label manner. Some centres prefer upfrontASCT as an induction therapy, and other institutionsuse front-line therapy (bortezomib-based, ± IMiDsand corticosteroids) [15] in order to achieve organimprovement before ASCT. To address the questionof which strategy provides the best outcome, borte-zomib-based first-line treatment preceding ASCT wasinvestigated in various trials, and the results were re-ported at the ASH meeting. Kastritis et al. presented
K News in AL Amyloidosis ASH 2016 67
review
Fig. 2 Cardiac MRI features in amyloidosis. The cine imagingshows hypertrophic left and right ventricles as well as severelydilated atria (a). Typical late enhancement pattern 15 min aftergadoliniumapplication (b). NativeT1mapping,which isusedfor
extracellular volume quantification (native T1 time myocardium:1180 ms; extracellular volume: 56.8%; c). Courtesy of FranzDucka, MD (Medical University Vienna, Department of InternalMedicine II, Division of Cardiology)
the first prospective randomised phase III trial ofmelphalan and dexamethasone (MDex) versus borte-zomib, melphalan and dexamethasone (BMDex) fornewly diagnosed patients [16]. Alahwal et al. also pre-sented data regarding the high effectiveness of borte-zomib-containing regimens in these patient cohorts[17]. Both trials identified bortezomib as an effectivedrug with profound haematological responses andorgan improvement. However, the study designs andend points were different, and a direct comparison ofthese two trials is therefore not applicable. Interest-ingly, both working groups mentioned a bortezomib-based cardiac toxicity. Therefore, Alahwal et al. em-phasised the importance of a nonbortezomib-basedapproach for patients with advanced cardiac dysfunc-tion, i. e. melphalan/dexamethasone [18] to avoidadditional toxicity, since these patients were found tohave an inferior survival rate [17].
Sidana et al. introduced a trial comparing a borte-zomib-containing regimen with a nonbortezomib-containing induction regimen in transplant ineligiblepatients with AL amyloidosis [19]. Again, the treat-ment with bortezomib-based regimens resulted inbetter responses, including higher rates of early verygood partial remission (VGPR) at 3 and 6 months.The patients achieved faster cardiac improvementand had a lower relapse rate, but no difference in OSwas seen.
Two further trials with bortezomib-based induc-tion therapy followed by ASCT were presented. Jainet al. performed a retrospective data analysis, whileMinnema et al. did the data collection in a prospec-tive designed trial. Both anlyses demonstrated an im-proved outcome with a better OS [20, 21]. In compar-ing these trials, it should be mentioned that the datacollection was retrospectively in the working group ofJain et al. and in a prospective manner in Minnema’sgroup. However, both trials showed the beneficial ef-fects of early ASCT after bortezomib-containing in-duction therapy.
The group led by Tandon investigated standard-dose versus risk-adapted melphalan conditioning on
the outcome in patients undergoing front-line ASCT[22]. Melphalan dose reduction is used in patientswith older age, renal dysfunction and multiorganinvolvement. The reduced dosage (140–160mg/m2)compared to the standard dose of melphalan (200mg/m2) resulted in a suboptimal outcome [21], suggestingthat high-dose therapy should be limited to patientseligible for full-dose conditioning.
Biochemical patterns of relapse in AL amyloidosis
In relapsed AL amyloidosis, we face the same prob-lems as in newly diagnosed patients: there is no stan-dard of care and validated progression criteria andtreatment recommendations are still lacking. How-ever, since several new therapeutic options are avail-able for plasma cell dyscrasias, new data on the ef-fectiveness of these drugs are also being awaited inconnection with AL amyloidosis. Three abstracts atthe ASH meeting in 2016 were of special interest.
Tandon et al. investigated the predictors of earlyrelapse during initial therapy [23]. It was demon-strated that patients with early relapse are of olderage with a higher prevalence of cardiac and multior-gan involvement and a higher risk stage (Mayo III andIV). Therefore, early ASCT should be an aim duringthe initial therapy. Milani et al. described the relapsepatterns after different upfront strategies [24] in 259patients. A low free light chain (FLC) burden at diag-nosis and a bortezomib-containing induction regimenwere associated with more durable responses. Car-diac deterioration was preceded by increasing dFLC(the difference between involved and uninvolved freelight chains) in >90% of patients. An increase of >20%in dFLC should be a clear trigger to start with therelapse therapy. A “wait and see” strategy until theNT-proBNP levels increase will result in a worsenedcourse of disease. Hwa et al. evaluated the relapsepatterns after ASCT and their influence on the dis-ease outcome [25]. The following scenarios were eval-uated: (1) hematologic relapse only, (2) organ progres-sion only and (3) combined hematologic and organ
68 News in AL Amyloidosis ASH 2016 K

review
Fig. 3 Colonic AL amy-loidosis. aHistology anda hematoxylin and eosin(H&E) stain; original mag-nification (x10). Focaleosinophilic homogeni-sation of the submucosa.b Immunohistological amy-loidtypingwithakappalight-chain antibody revealing thespecific positive stainingof the deposits. cCongored staining of the depositswithdcharacteristic apple-green birefringence underpolarised light. Courtesy ofIngrid Simonitsch-Klupp,MD (Medical University Vi-enna, Institute of Pathology)
relapse. As expected, the OS rates 4 years after ASCTwere 87.8% for hematologic relapse, 63.9% for organrelapse and 56.7% (p = 0.0016) for combined organand hematologic progression.
New therapeutic options in relapsed patients
Lagos et al. presented data from a phase II trial withbendamustine combined with dexamethasone. Theregimen was well tolerated with significant success inhematologic response rates in previously treated ALamyloidosis [26]. Cohen et al. investigated the effectsof carfilzomib [27] in the relapse setting. Carfilzomibwas feasible and effective, including in bortezomibpretreated patients, with a maximal tolerated dose(MTD) of 20mg/m2 at the first infusion followed bya dosage of 36mg/m2 as a 30min infusion. However,cardiac, pulmonary and renal toxicities were docu-mented. The close monitoring of blood pressure withthe avoidance of hypertensive episodes during andafter the drug infusion is recommended. NT-proBNPlevels may rise without a direct correlation with pro-gressive cardiac dysfunction. The same effect is ob-served during IMiD therapy. The mechanism of thisphenomenon is not fully understood. Increasing NT-proBNP levels in these special settings has to inter-preted with great caution. Kaufmann et al. presenteddata on the use of daratumumab in heavily pretreatedpatients with cardiac involvement [28]. In this retro-spective single centre study, antibody treatment withdaratumumab was very well tolerated, resulting inrapid and significant hematologic responses. Aftera median time of 4 months of therapy, cardiac dys-
function improved markedly. Other mAbs with differ-ent modes of action were also investigated, as listedbelow.
● The first additional study involved antifibrillarymAbs directed against epitopes expressed only bymisfolded amyloid fibrils. Gertz et al. [29] investi-gated NEOD001 in the PRONTO trial (a phase I/IIdose-escalation trial). NEOD001 is a humanisedmAb binding to a cryptic epitope unique to mis-folded light-chain fibrils. This epitope is exposedduring misfolding and aggregation and is not tar-getable in regular conformation. This mAb notonly disrupts amyloid fibrils, but also stimulatesmacrophages to phagocyte amyloid deposits. Pa-tients eligible for this study had completed at leastone round of previous therapy, with at least a partialhematologic response or better, and suffer fromper-sistent organ dysfunction. NEOD001 was adminis-tered intravenously every 28 days to the 27 patientsenrolled. No drug-related serious adverse events(AEs) were documented; the patients reported onlyfatigue, upper respiratory tract infection, nauseaand diarrhea at a maximum of grade I or II (whichwas not clearly related to the study drug). No dis-continuations were reported. Eight of 14 patientswith cardiac involvement met the criteria for car-diac response (measured as the percentage of de-crease in the pro-BNP levels), and 9 of 15 patientswith renal involvement met the criteria for renalresponse (measured as the percentage of decreasein proteinuria in g/24 h). Because of these promis-ing results, an expansion cohort was initiated, and
K News in AL Amyloidosis ASH 2016 69

review
the follow-up results were presented at the ASHmeeting in 2016 [30]. Forty-two additional patientswere enrolled, including 16 patients with renal in-volvement, 15 patients with cardiac involvementand 11 patients with peripheral nerve amyloido-sis. Again, no dose-limiting toxicities or discon-tinuations were reported. Of the cardiac-affectedpatients, 53% met the criteria for organ responsealongwith 63%of renal-affected patients (expressedas the percentage of decrease in NT-proBNP or pro-teinuria in g/24 h); none of the patients experienceddisease progression. The median times to the initialresponsewere 2months (cardiac) and 4months (re-nal). After 9 months of treatment, 82% of patientswith peripheral neuropathy achieved a responsebased on the Neuropathy Impairment Score in theLower Limbs (NIS-LL score).Edwards et al. [31] presented the results of a chimericamyloid fibril reactive mAb 11-1F4 mediating amy-loid destabilisation and the initiation of cell-me-diated phagocytosis. The first data collected ina phase Ia trial were presented at the ASH meet-ing in 2015. At the ASH meeting in 2016, the follow-up results from a phase Ia/b trial were introduced[31]. The mAb 11-1F4 was administered without se-vere adverse events (only fatigue, upper respiratorytract infection, nausea and diarrhea), and no dose-limiting toxicities up to an MTD of 500mg/m2 weredocumented. The clinical efficacy resulted in anearly and sustained organ response.
● The second additional study involved an anti-SAPmAb directed against the ubiquitously present SAP(Serum Amyloid P) component. The anti-SAP mAbworks only in conjunction with the small moleculedrug CPHPC, which was constructed for the bind-ing and elimination of circulating SAP moleculesfrom the blood stream. In a second step, the anti-SAP mAb was administered intravenously. This an-tibody binds to the residual SAP molecules locatedin the tissue amyloid deposits, triggering rapid amy-loid clearance through complement activation andmacrophage stimulation. The first results with thisnew drug combination were presented at the ASHmeeting in 2014. In 2015, Richards et al. publishedthis open-labelled, single-dose escalation, phase Itrial titled “Therapeutic Clearance of Amyloid byAntibodies to Serum Amyloid P Component” in theNew England Journal of Medicine [32]. This phase Itrial involved 15 patients with amyloidosis (twowith AA amyloidosis, eight with AL amyloidosis,four with AFib amyloidosis and one with AApoA1amyloidosis). The affected organs were the kidney,liver, spleen and lymph nodes. Patients with cardiacinvolvement were strictly excluded. No serious sideeffects were reported with the anti-SAP antibodyand CPHPC. A response assessment was conductedafter 6 weeks with a SAP scan using the 123I-SAPscintigram and a FIBRO scan. After 6 weeks, de-creased liver stiffness was detected by FIBRO scan
and by 123I-SAP scan. In one patient improvementin the liver function tests were measured. The samereduction was seen in the spleen and in the affectedlymph nodes also documented by the SAP scan [32].
Take-homemessages AL amyloidosis is a life-threat-ening systemic disease requiring early diagnosis withaccessible biomarker measurements. For the final di-agnosis, a multidisciplinary approach by specialisedand experienced teams is strongly recommended. En-rolling patients in prospective, randomised interna-tional trials should still be the goal because no ther-apeutic standard option has been approved so far.However, an increasing number of trials with promis-ing monoclonal antibodies and small molecules arebeing conducted in specialised amyloidosis centres.
Conflict of interest H. Agis declares that she has no compet-ing interests.
Open Access This article is distributed under the terms ofthe Creative Commons Attribution 4.0 International License(http://creativecommons.org/licenses/by/4.0/), which per-mits unrestricted use, distribution, and reproduction in anymedium, provided you give appropriate credit to the origi-nal author(s) and the source, provide a link to the CreativeCommons license, and indicate if changes were made.
References
1. Kyle RA, Gertz MA. Primary systemic amyloidosis: clinicaland laboratory features in 474 cases. Semin Hematol.1995;32(1):45–59.
2. Mahmood S, Palladini G, Sanchorwala V, et al. Updateon treatment of light chain amyloidosis. Haematologica.2014;99(2):209–21.
3. MerliniG,BelottiV.Molecularmechanismsofamyloidosis.NEngl JMed. 2003;349(6):583–96.
4. MerliniG,PalladiniG.Lightchainamyloidosis: theheartoftheproblem.Haematologica. 2013;98:1492–5.
5. MerliniG,WechalekarAD,PalladiniG. Systemic light chainamyloidosis an update for treating physicians. Blood.2013;121(26):5124–30.
6. PickenMM. Amyloidosis where are we now and where areweheading? ArchPatholLabMed. 2010;134(4):545–51.
7. Vrana JA, Gamez JD, Madden BJ, et al. Classification ofamyloidosis by laser microdissection andmass spectrom-etry-basedproteomicanalysis in clinical biopsy specimen.Blood. 2009;114(24):4957–9.
8. Brambilla F, Lavatalli F, Di SilvestreD, et al. Reliable typingof systemic amyloidosis through proteomic analysis ofsubcutaneousadiposetissue. Blood. 2012;119(8):1844–7.
9. Dispenzieri A, Gertz MA, Kyle RA, et al. Serum cardiactroponins and N-terminal pro-brain natriuretic peptide:a staging system for primary systemic amyloidosis. J ClinOncol. 2004;22(18):3751–7.
10. Kumar S,Dispenzieri A, LacyMQ, et al. Revisedprognosticstaging system for light chain amyloidosis incorporatingcardiac biomarkers and serum free light chain measure-ments. JClinOncol. 2012;30(9):989–95.
11. Merlini G, Lousada I, Ando Y, et al. Rationale, applicationand clinical qualification for NT-proBNP as a surrogate
70 News in AL Amyloidosis ASH 2016 K

review
end point in pivotal clinical trials in patients with ALamyloidosis. Leukemia. 2016;30:1979–86.
12. Palladini G, Hegenbart U, Milani P, et al. A stagingsystem for renal outcome and early markers of renalresponse to chemotherapy in AL amyloidosis. Blood.2014;124(15):2325–32.
13. Wechalekar A, Foard D, Whelan C, et al. Challenges ofUsing NT-ProBNP for response assessment in aystemicAL amyloidosis – Analysis of a prospective study. Blood.2016;128:abstr4511.
14. Kastritis E, Merlini G, Papassotiriou I, et al. Growth Dif-ferentiation Factor-15 (GDF-15) Is a new biomarker withindependent prognostic significance for survival and renaloutcomes in different cohorts of patients with light chain(AL)Amyloidosis. Blood. 2016;128:abstr648.
15. Dispenzieri A, Buadl F, Kumar SK, et al. Treatment ofimmunoglobulin light chain amyloidosis. MayoClin Proc.2015;90(8):1054–81.
16. Kastritis E, Leleu X, Arnulf B, et al. A randomized phaseIII trial of Melphalan and Dexamethasone (MDex) ver-sus Bortezomib,Melphalan andDexamethasone (BMDex)for untreated patients with AL Amyloidosis. Blood.2016;128:abstr646.
17. Alahwal H, Song KW, Duggan P, et al. Bortezomib-con-taining regimens for the treatment of newly diagnosed ALAmyloidosis. Blood. 2016;128:abstr2131.
18. Palladini G, Milani P, Foli A, et al. Oral melphalan anddexamethasone grants extended survival with minimaltoxicity in AL amyloidosis: long-term results of a risk-adaptedapproach.Haematologica. 2014;99(4):743–50.
19. Sidana S, Tandon N, Dispenzieri A, et al. Bortezomibversus non-Bortezomib based treatment for transplantineligible patients with light chain Amyloidosis. Blood.2016;128:abstr3317.
20. Jain T, Kung ST, Shah V, et al. Treatment with Bortezomib-based therapy followed by Autologous stem cell trans-plantation improves outcomes in light chain Amyloidosis.Blood. 2016;128:abstr4629.
21. MinnemaM,NasserinejadK,Hazenberg B, et al. Results of25 patients from amulticenter, multinational, prospectivephaseIIstudyofBortezomibbasedinductiontreatmentfol-lowed by Autologous stem cell transplantation in patientswithnewlydiagnosedAlAmyloidosis. Blood. 2016;128:ab-str4628.
22. Tandon N, Sidana S, Dispenzieri A, et al. Standard doseversus risk adapted Melphalan conditioning on outcomesin systemic AL Amyloidosis patients undergoing frontlineautologous stem cell transplant based on revised mayostage. Blood. 2016;128:abstr4627.
23. Tandon N, Sidana S, Gertz MA, et al. Predictors ofEarly Relapse (ER) following initial therapy for sys-temic immunoglobulin light chain Amyloidosis. Blood.2016;128:abstr2082.
24. Milani P, Basset M, Russo F, et al. Patterns of relapse afterupfront therapy in AL Amyloidosis. Blood. 2016;128:abstr2140.
25. HwaYL,WarsameR,GertzMA,etal. Practicepatternsof re-initiation of therapy at time of relapse or progressionpost-autologous stem cell transplant among patients with ALAmyloidosis. Blood. 2016;128:abstr3444.
26. Lagos GG, Lentzsch S, Comenzo RL, et al. Final results ofaphase2 studyofBendamustine incombinationwithDex-amethasone in patients with previously treated systemiclight-chainAmyloidosis. Blood. 2016;128:abstr4523.
27. Cohen AD, Landau H, Scott EC, et al. Safety and efficacyof Carfilzomib in previously treated systemic light-chainAmyloidosis. Blood. 2016;128:abstr645.
28. Kaufmann G, Witteles R, Wheeler M, et al. Hematologicresponses andcardiacorgan improvement inpatientswithheavilypretreatedcardiacimmunoglobulinlightchain(AL)Amyloidosis receivingDaratumumab. Blood. 2016;128:ab-str4525.
29. GertzMA, LandauH,CommenzoRL, et al. First-in-humanphase I/II study of NEOD001 in patients with light chainAmyloidosisandpersistentorgandysfunction. JClinOncol.2016;34(10):1097–103.
30. Gertz MA, Comenzo RL, Landau H, et al. NEOD001demonstrates organ biomarker responses in patients withlight chain Amyloidosis and persistent organ dysfunction:results from the expansion cohort of a phase 1/2 study.Blood. 2016;128:abstr644.
31. Edwards CV, Gould J, Langer AL, et al. Analysis of thephase 1a/b study of chimeric fibril-reactive monoclonalantibody 11-1F4 in patients with AL Amyloidosis. Blood.2016;128:abstr643.
32. Richards DB, Cookson LM, Berges AC, et al. Therapeuticclearance of Amyloid by antibodies to serum Amyloid Pcomponent. NEngl JMed. 2015;373(12):1106–14.
7For latest news from interna-tional oncology congresses see: http://www.springermedizin.at/memo-inoncology
K News in AL Amyloidosis ASH 2016 71