neoplastic transformation of oral lichen
TRANSCRIPT

Neoplastic transformation of oral lichen planus :case report and review of the literatureBY : DR APARNA SRIVASTAVA.

chronic, immunological mucocutaneous disease with a widerange of clinical manifestations.
pre-malignant condition
a recall system has been recommended one to four times annuallyto facilitate the early diagnosis of malignant transformation.
Case report
60-year-old female
sharp and widespread pain in the oral cavity which had been present for approximately one
year and which worsened when in contact with food.

The most significant anamnestic findings were
cholecystectomy, 20 years previously, for gallstones;
chronic gastritis with hiatus hernia, under treatmentwithomeprazole and levosulpiride
hypothyroidism oral treatment with levothyroxine
asymptomatic hepatitis C virus (HCV) positive
non drinker, non smoker
mean corpuscular haemoglobin MCH)33.3 pg; erythrocyte sedimentation rate
(ESR) 27 mm/h
fibrinogen 403 mg/dl,
SGPT 52 IU/l,
Electrocardiogram (ECG) and chest X-ray were both negative

HISTOLOGICAL REPORTS
Fig. 1 Fig.2Fig. 1

Fig. 3 Fig. 4

Discussion

It is defined as a common chronic immunological
mucocutaneousdisorder that varies in appearnce from
keratotic to erythematous and ulcerative Wilson
1896
Lichen planus is relatively common
disorder of the stratified
squamous epithelia skullyand El-kom1985
Eisen D 2005 defined oral
lichen planus as a relatively
common chronic inflammatory
disorder affecting the
statifiedsquamous epithelia
A common disorder in which auto-
cytotoxic T lymphocytes trigger
apoptosis of epithelial cells
leading to chronic inflammation. Oral LP (OLP) can be a source of severe
morbidity and has a small potential to be malignant. Crispian
Scully 2007

Common mucocutaneous disease with varying clinical presentation
Also known as Lichen Rubber Planus
First described clinically :- 1869 – Wilson
Erasmus Wilson (1869)-Mixed non Scrapable Red and white lesion in themouth-Can occur individually or with skin lesions.
*Lichen in Greek – tree moss *Planus in Latin – flat.
Epidemiology
• 1% of general population is affected
• 0.14-0.8% worldwide
• 2/3rd of cases occur in middle age
• No racial predilection reported although some authors claims a predilection in blacks
• Increased in the month of Jun-July & Dec-Jan

• Male: Female - 1:1• 20% females with oral lesions have genital involvement
• 2/3rd of the cases are symptomatic• 40%- of patients have both Oral & Cutaneous lesions
• 35%- of patients have Cutaneous lesions only• 25%- of the cases presents with mucosal lesions only

Buccal mucosa often bilaterally
Tongue
Lip
Gingiva
Patate
Floor of mouth
Co
mm
on
si
tes

"5 P's“
Pruritic
planar
Purple
Polygonal
papules

Louis frederic wickham described the
presence of fine white or grey lines or dots
seen on the top of the pruritic rash on the skin
in lichen planus . These striae are popularly
referred to as “WICKHAMS STRIAE or
HONITON LACE” Text book of oral
medicine and radiology –ongole first edition

ETIOLOGY
Etiology is unknown.
Immune System has a primary role
in the development
of this disease.
Genetic background
Dental materials-metallic &
non metallic restoration
Drugs & chemicals
Infectious agents
AutoimmunityChronic liver
disease Immunodefici
encies


subepithelial band–formed infiltrate dominated by T lymphocytes,macrophages and the degeneration of basal cells known as liquefaction degeneration .
expression of the cell-mediated immune system being involved in the pathogenesis of OLP
T-lymphocyte cytotoxicity directed against antigens
expressed by the basal cell layer.

Pathogenesis of lichen planus; TCR-T cell receptor, MHC-Major histocompatibility receptor, TNF-Tumor necrosis factor, MMP-Matrix metalloproteinases

photomicrography
FIRST DESCRIBE
D BY DUBRENIL
L 1906 later
revised by Shklar in
1972

RETICULAR FORM
• white lines or striae.
• The striae may form a network but can also
show annular (circular) patterns.
• The striae often display a peripheral
erythematous zone, which reflects the
subepithelial inflammation.
• all regions of the oral mucosa, most
frequently this form is observed bilaterally in
the buccal mucosa and rarely on the mucosal
side of the lips.
• sometimes at the vermilion border.

PAPULAR FORMpresent in the initial phase of the disease.
It is clinically characterized by small white dots, which in most occasions intermingle with the reticular form.
Sometimes the papular elements merge with striae as part of the natural course.
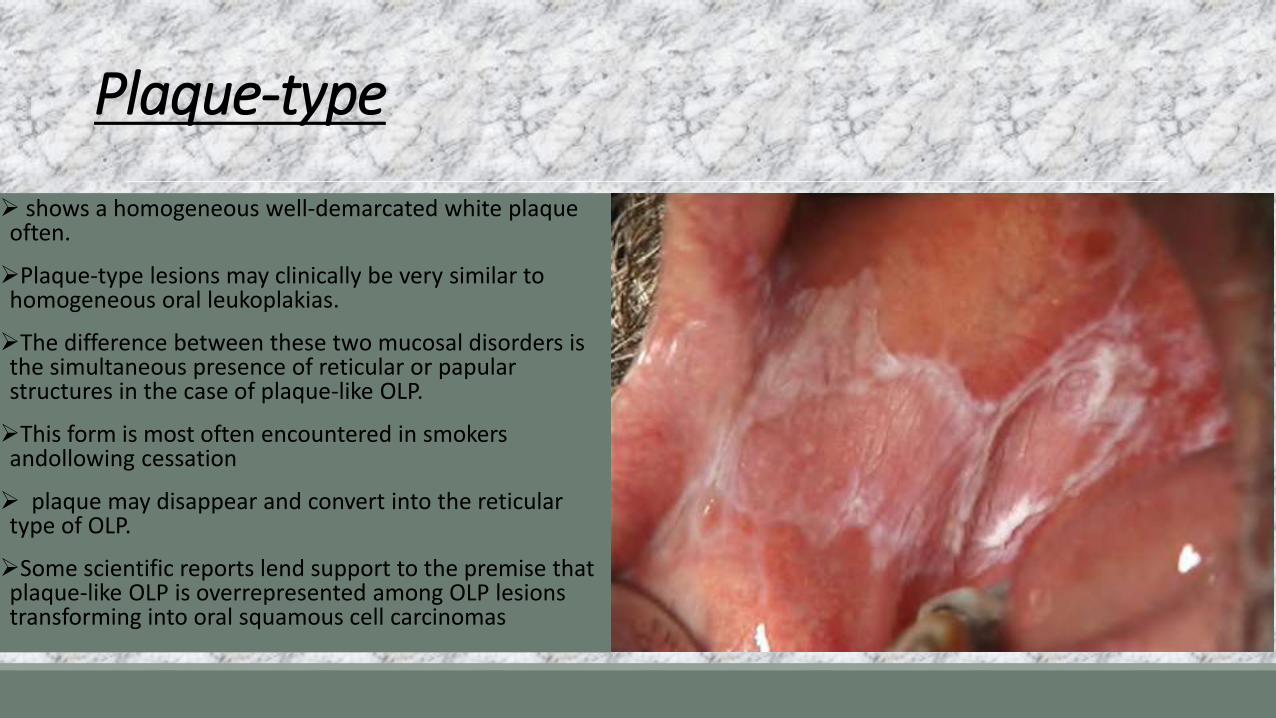
Plaque-type
shows a homogeneous well-demarcated white plaque often.
Plaque-type lesions may clinically be very similar to homogeneous oral leukoplakias.
The difference between these two mucosal disorders is the simultaneous presence of reticular or papularstructures in the case of plaque-like OLP.
This form is most often encountered in smokers andollowing cessation
plaque may disappear and convert into the reticular type of OLP.
Some scientific reports lend support to the premise that plaque-like OLP is overrepresented among OLP lesions transforming into oral squamous cell carcinomas

Erythematous lichen planus

Erosive type

Bullous typeVesciculobullous presentation combined with reticular or erosive pattern
Rare form characterized by large vesicles or bullae (4mm to 2cm)
Lesions usually develop within an erythematus base, rupture immediately leaving painful ulcers
Usually have peripheral radiating striae and seen on posterior part of buccal mucosa

type Incidence percent
Reticular 94
Atrophic 44
Plaque like 36
Papular 11
Atrophic 9
Erosive 1
Modified World Health Organization diagnostic criteria of OLPPresence of bilateral, more or less symmetrical lesions
Presence of a lacelike network of slightly raised gray- white lines(reticular pattern)
Erosive, atrophic, bullous and plaque-type lesions are accepted only as a subtype in the presence of reticular lesion else where in the oral mucosa
In all other lesions that resemble OLP but do not complete the aforemented criteria, the term “clinically compatible with” should be used.

IncidenceMalignant potentialThe most important complication of OLP is the development of oral squamous cell carcinoma.
Frequency of malignant transformation varies greatly, between 0.4% to over 5%, over periods of observation from 0.5 to over 20 years (van der Meijet al, 1999).
Significantly increased risk of oral cancer appears to be independent of the clinical type of OLP and therapy administered (Gandolfo et al, 2004)
Considerable controversy regarding themalignant transformation of OLP. Despite the fact thatmore than 25 follow-up studies have focused on this topic, as recently reviewed by Barnard et al (Barnardet al, 1993)

scrupulous attention is necessary
concomitant skin invasion
of lichen,
HCV infection
HBV infection
autoimmune diseases.

Malignant transformation observed
3 months after lichen planus with lichenoid dysplasia
3 months after lichenoid dysplasia and ulcerated infiltrating cancer G1-G2
suggests the need for histopathological observations at more frequent intervals (at least every 3months) from the time of the first diagnosis

Incidence :
Erosive type Ulcerative type Atrophic type Plaque type

Investigations
• Incisional biopsy• Immunoflourescent studies-Fluorescent
dyes like FITC
• Immunoglobulin assay
• PAS staining

Treatment planning

Differential diagnosis
1. Lychenoid reaction
2. Graft verses host response
3. Leukoplakia
4. Frinctional keratosis



REASON FOR CHOOSING THIS ARTICLE

1. Kilpi A, Rich AM, Reade PC, Konttinen YT. Studies of the inflammatory process and malignant potential of oral mucosal lichen planus. Aust Dent J 1996;41:87-90.
2. Ognjenovic M, Karelovic D, Cindro VV, Tadin I. Oral lichen planus and HLA A. Coll Antropol1998;22:89-92
3.\Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology. 2nd ed. Saunders: Elsevier; 2005. p. 89.
4. BURKET’S ORAL MEDICINE 11TH EDITION BY GREENBERG,GLICK,SHIP CBS PUBLISHERS AND DISTRIBUTERS
5. DIAGNOSTIC OF ORAL MEDICINE, B K Venkatraman 1st Edition,Willams and Wilkins publishers

6. Roy K, Bagg J. Hepatitis C virus and oral disease: a critical Review. Oral Dis 1999;5:270-7.
7. Rajendran R, Sivapathasundaram B. Shafer’s Textbook of Oral Pathology.6th ed.Elsevier.Dehli; 2009: p.48-54 Radiology.