national kidney foundation primer on kidney diseases || the kidney in pregnancy
TRANSCRIPT
The Kidney in PregnancyKavitha Vellanki | Susan Hou
50
Pregnancy produces dramatic changes in systemic hemody-namics, leading to an increase in total circulating blood vol-ume and cardiac output and a decrease in systemic vascular resistance (SVR), resulting in a high output state with mildly reduced blood pressure (BP). The kidney experiences a marked increase in glomerular filtration rate (GFR) and renal plasma flow (RPF), which is critical for a favorable outcome in pregnancy. Understanding the adaptive changes that occur during pregnancy is crucial for differentiating and managing normal and compromised pregnancies.
ANATOMIC CHANGES DURING NORMAL PREGNANCY
During pregnancy, the kidney increases by 1 to 1.5 cm in length and by up to 30% in volume, reflecting increases in vascular and interstitial space without accelerated growth, a process akin to compensatory hypertrophy. Significant dilation and decreased peristaltic activity in the collecting system are noted as early as the third month of pregnancy, with more pronounced changes on the right side. Although the etiology is debated, hormonal changes in the initial period and compression of the ureters by the gravid uterus in the late gestational period are among the proposed causative mechanisms. Stasis of at least 200 mL of urine occurs in the collecting system. The increased susceptibility of pregnant women with asymptomatic bacteruria to acute pyelonephritis is attributed to urinary stasis. Magnetic reso-nance imaging can help in distinguishing physiologic hydro-nephrosis from obstruction in pregnancy; ultrasound is less reliable in such a setting. Structural changes generally resolve by 12 weeks postpartum, and persistent hydronephrosis beyond 12 to 16 weeks needs further workup (Box 50.1).
PHYSIOLOGIC CHANGES DURING NORMAL PREGNANCY
SYSTEMIC HEMODYNAMIC CHANGES
Pregnancy leads to vasodilation, and cardiac output increases by 40% to 50% above normal by 24 weeks of gestation. Plasma volume expands by 40% to 50%, whereas red blood cell mass increases by only 18% to 30%, resulting in a drop in hematocrit and leading to physiologic anemia of preg-nancy. Despite the increase in blood volume and cardiac output, systemic BP decreases substantially and this decrease occurs despite an increase in many of the hormones that are generally associated with higher BP (a fourfold increase in
angiotensin, an eightfold increase in plasma renin, and a 10- to 20-fold increase in aldosterone). The pressor effects of these hormones are limited by profound reduction in SVR caused by the production of vasodilatory substances, such as prostacyclin, nitric oxide (NO), and relaxin. The lowest BP is seen between 16 to 20 weeks gestation, with a gradual increase towards term.
RENAL HEMODYNAMIC CHANGES
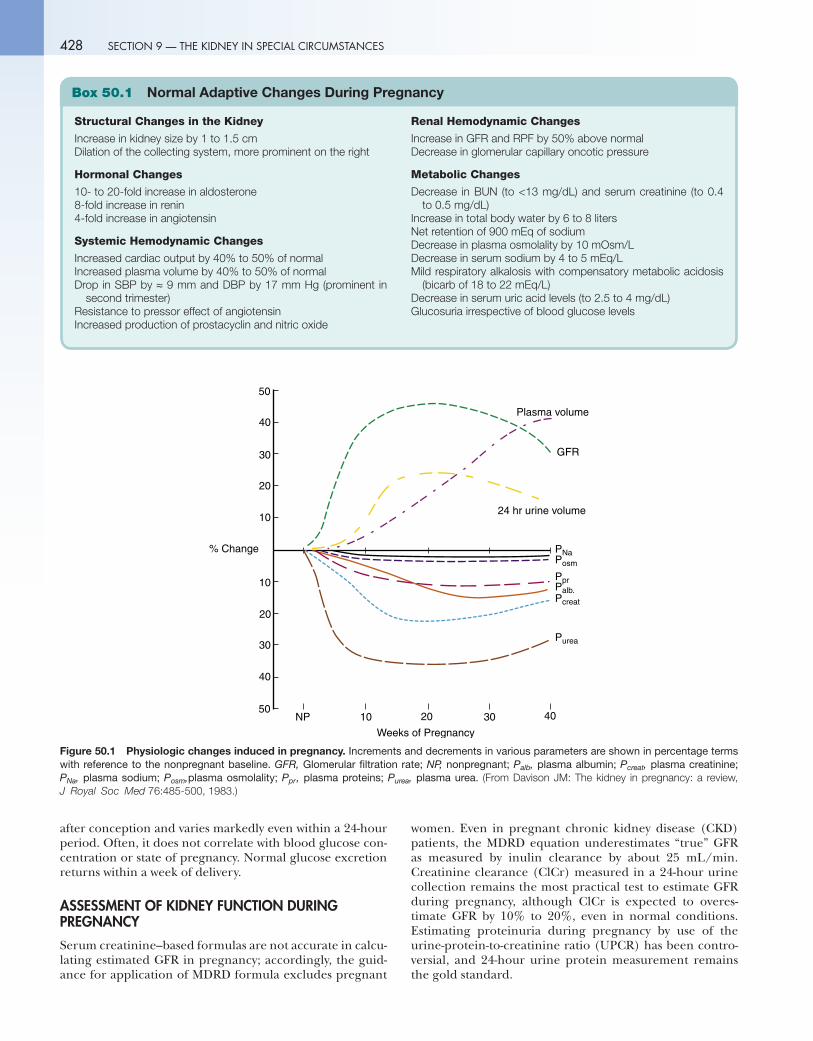
Glomerular filtration rate and RPF increase by approxi-mately 50% with RPF being slightly higher than GFR. Hyperfiltration in pregnancy has been variously attributed to increased RPF, decreased oncotic pressure, and increased glomerular capillary Kf. Increase in GFR is noted as early as 4 weeks gestation, reaches peak level during the first half of pregnancy, and remains constant until term (Fig. 50.1). Despite a major increase in GFR, no long-term effects on glomerular function or structure are noted; this is true even in repetitive pregnancies with normal kidney function because of parallel reductions in both afferent and effer-ent arteriolar resistance with no change in intraglomerular pressure.
In women who previously had unilateral nephrectomy or kidney transplant, increases in GFR and RPF are often noted, because single kidneys can still adapt further as in normal pregnancy, although the changes are smaller and slower than in healthy women with two functioning kidneys.
METABOLIC CHANGES
Increased GFR leads to decreases in blood urea nitrogen (BUN) and serum creatinine levels. A BUN greater than 13 mg/dL or serum creatinine of 0.7 to 0.8 mg/dL is of concern in normal pregnancy and should be further investi-gated. Urinary protein excretion may increase but generally remains below 300 mg/24 hours. Total body water increases by 6 to 8 L, of which 4 to 6 L are extracellular. There is also a gradual cumulative retention of 900 mEq of sodium, the mechanisms of which remain unclear. A reset osmostat leads to a lower plasma osmolality (10 mOsm/L below nor-mal) with a proportionate decrease in serum sodium by 4 to 5 mEq/L. Mild alkalemia from respiratory alkalosis and a compensatory decrease in serum bicarbonate to 18 to 22 mEq/L occur. Uric acid levels drop to 2.5 to 4 mg/dL from the combined effects of increased filtration and decreased tubular reabsorption. Serum levels and renal reabsorption of uric acid are significantly higher in pregnan-cies complicated by preeclampsia and intrauterine growth retardation (IUGR). Excretion of glucose increases soon
427
428 SECTION 9 — THE KIDNEY IN SPECIAL CIRCUMSTANCES
Structural Changes in the Kidney
Increase in kidney size by 1 to 1.5 cmDilation of the collecting system, more prominent on the right
Hormonal Changes
10- to 20-fold increase in aldosterone8-fold increase in renin4-fold increase in angiotensin
Systemic Hemodynamic Changes
Increased cardiac output by 40% to 50% of normalIncreased plasma volume by 40% to 50% of normalDrop in SBP by ≈ 9 mm and DBP by 17 mm Hg (prominent in
second trimester)Resistance to pressor effect of angiotensinIncreased production of prostacyclin and nitric oxide
Renal Hemodynamic Changes
Increase in GFR and RPF by 50% above normalDecrease in glomerular capillary oncotic pressure
Metabolic Changes
Decrease in BUN (to <13 mg/dL) and serum creatinine (to 0.4 to 0.5 mg/dL)
Increase in total body water by 6 to 8 litersNet retention of 900 mEq of sodiumDecrease in plasma osmolality by 10 mOsm/LDecrease in serum sodium by 4 to 5 mEq/LMild respiratory alkalosis with compensatory metabolic acidosis
(bicarb of 18 to 22 mEq/L)Decrease in serum uric acid levels (to 2.5 to 4 mg/dL)Glucosuria irrespective of blood glucose levels
Box 50.1 Normal Adaptive Changes During Pregnancy
40302010NP
50
40
30
20
10
50
40
30
20
10
% Change
Weeks of Pregnancy
Plasma volume
GFR
24 hr urine volume
PNaPosm
Palb.Pcreat
Purea
Ppr
Figure 50.1 Physiologic changes induced in pregnancy. Increments and decrements in various parameters are shown in percentage terms with reference to the nonpregnant baseline. GFR, Glomerular filtration rate; NP, nonpregnant; Palb, plasma albumin; Pcreat, plasma creatinine; PNa, plasma sodium; Posm,plasma osmolality; Ppr, plasma proteins; Purea, plasma urea. (From Davison JM: The kidney in pregnancy: a review, J Royal Soc Med 76:485-500, 1983.)
after conception and varies markedly even within a 24-hour period. Often, it does not correlate with blood glucose con-centration or state of pregnancy. Normal glucose excretion returns within a week of delivery.
ASSESSMENT OF KIDNEY FUNCTION DURING PREGNANCY
Serum creatinine–based formulas are not accurate in calcu-lating estimated GFR in pregnancy; accordingly, the guid-ance for application of MDRD formula excludes pregnant
women. Even in pregnant chronic kidney disease (CKD) patients, the MDRD equation underestimates “true” GFR as measured by inulin clearance by about 25 mL/min. Creatinine clearance (ClCr) measured in a 24-hour urine collection remains the most practical test to estimate GFR during pregnancy, although ClCr is expected to overes-timate GFR by 10% to 20%, even in normal conditions. Estimating proteinuria during pregnancy by use of the urine-protein-to-creatinine ratio (UPCR) has been contro-versial, and 24-hour urine protein measurement remains the gold standard.
429 CHAPTER 50 — THE KIDNEY IN PREGNANCY
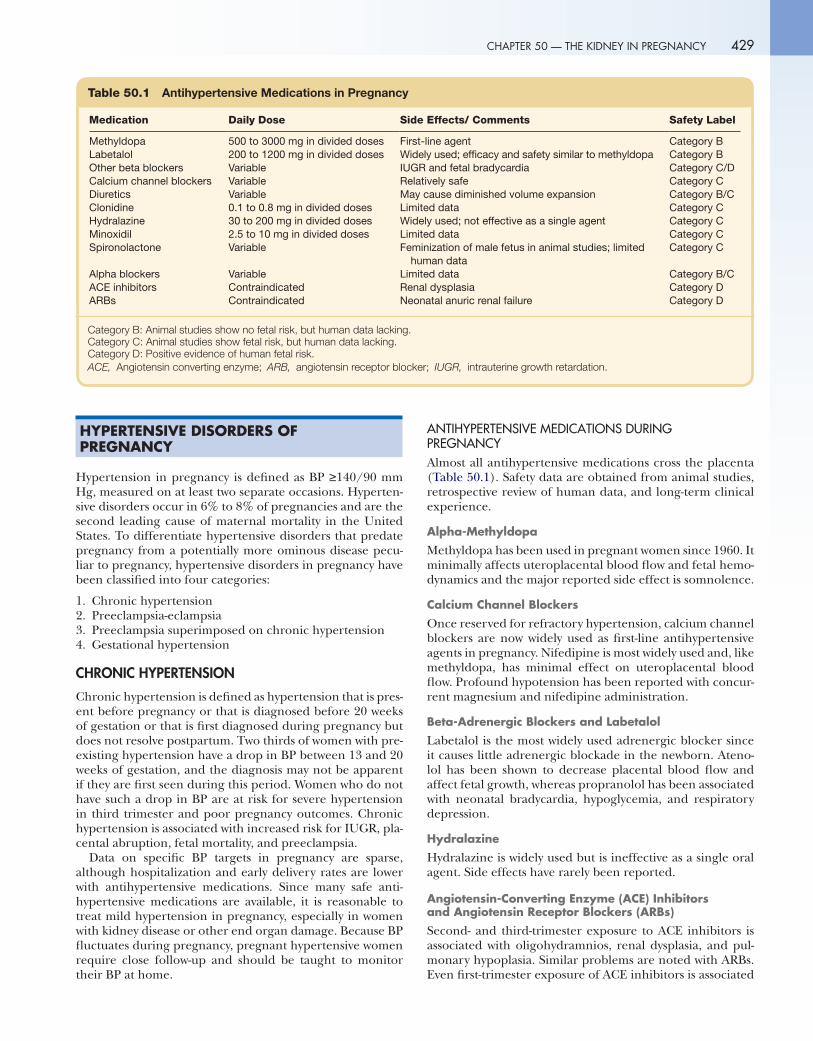
Table 50.1 Antihypertensive Medications in Pregnancy
Medication Daily Dose Side Effects/ Comments Safety Label
Methyldopa 500 to 3000 mg in divided doses First-line agent Category BLabetalol 200 to 1200 mg in divided doses Widely used; efficacy and safety similar to methyldopa Category BOther beta blockers Variable IUGR and fetal bradycardia Category C/DCalcium channel blockers Variable Relatively safe Category CDiuretics Variable May cause diminished volume expansion Category B/CClonidine 0.1 to 0.8 mg in divided doses Limited data Category CHydralazine 30 to 200 mg in divided doses Widely used; not effective as a single agent Category CMinoxidil 2.5 to 10 mg in divided doses Limited data Category CSpironolactone Variable Feminization of male fetus in animal studies; limited
human dataCategory C
Alpha blockers Variable Limited data Category B/CACE inhibitors Contraindicated Renal dysplasia Category DARBs Contraindicated Neonatal anuric renal failure Category D
Category B: Animal studies show no fetal risk, but human data lacking.Category C: Animal studies show fetal risk, but human data lacking.Category D: Positive evidence of human fetal risk.ACE, Angiotensin converting enzyme; ARB, angiotensin receptor blocker; IUGR, intrauterine growth retardation.
HYPERTENSIVE DISORDERS OF PREGNANCY
Hypertension in pregnancy is defined as BP ≥140/90 mm Hg, measured on at least two separate occasions. Hyperten-sive disorders occur in 6% to 8% of pregnancies and are the second leading cause of maternal mortality in the United States. To differentiate hypertensive disorders that predate pregnancy from a potentially more ominous disease pecu-liar to pregnancy, hypertensive disorders in pregnancy have been classified into four categories:
1. Chronic hypertension 2. Preeclampsia-eclampsia 3. Preeclampsia superimposed on chronic hypertension 4. Gestational hypertension
CHRONIC HYPERTENSION
Chronic hypertension is defined as hypertension that is pres-ent before pregnancy or that is diagnosed before 20 weeks of gestation or that is first diagnosed during pregnancy but does not resolve postpartum. Two thirds of women with pre-existing hypertension have a drop in BP between 13 and 20 weeks of gestation, and the diagnosis may not be apparent if they are first seen during this period. Women who do not have such a drop in BP are at risk for severe hypertension in third trimester and poor pregnancy outcomes. Chronic hypertension is associated with increased risk for IUGR, pla-cental abruption, fetal mortality, and preeclampsia.
Data on specific BP targets in pregnancy are sparse, although hospitalization and early delivery rates are lower with antihypertensive medications. Since many safe anti-hypertensive medications are available, it is reasonable to treat mild hypertension in pregnancy, especially in women with kidney disease or other end organ damage. Because BP fluctuates during pregnancy, pregnant hypertensive women require close follow-up and should be taught to monitor their BP at home.
ANTIHYPERTENSIVE MEDICATIONS DURING PREGNANCYAlmost all antihypertensive medications cross the placenta (Table 50.1). Safety data are obtained from animal studies, retrospective review of human data, and long-term clinical experience.
Alpha-Methyldopa
Methyldopa has been used in pregnant women since 1960. It minimally affects uteroplacental blood flow and fetal hemo-dynamics and the major reported side effect is somnolence.
Calcium Channel Blockers
Once reserved for refractory hypertension, calcium channel blockers are now widely used as first-line antihypertensive agents in pregnancy. Nifedipine is most widely used and, like methyldopa, has minimal effect on uteroplacental blood flow. Profound hypotension has been reported with concur-rent magnesium and nifedipine administration.
Beta-Adrenergic Blockers and Labetalol
Labetalol is the most widely used adrenergic blocker since it causes little adrenergic blockade in the newborn. Ateno-lol has been shown to decrease placental blood flow and affect fetal growth, whereas propranolol has been associated with neonatal bradycardia, hypoglycemia, and respiratory depression.
Hydralazine
Hydralazine is widely used but is ineffective as a single oral agent. Side effects have rarely been reported.
Angiotensin-Converting Enzyme (ACE) Inhibitors and Angiotensin Receptor Blockers (ARBs)
Second- and third-trimester exposure to ACE inhibitors is associated with oligohydramnios, renal dysplasia, and pul-monary hypoplasia. Similar problems are noted with ARBs. Even first-trimester exposure of ACE inhibitors is associated

430 SECTION 9 — THE KIDNEY IN SPECIAL CIRCUMSTANCES
00
with increased congenital malformations. ACE inhibitors and ARBs should be avoided both during pregnancy and in women trying to conceive.
Diuretics
Some clinicians are averse to the use of diuretics in preg-nancy because they aggravate the decreased intravascular volume seen with preeclampsia. In a metaanalysis involving more than 7000 normotensive pregnant women receiving diuretics, no increase in adverse fetal effects was noted. In settings where hypertension is related to volume expansion unrelated to pregnancy, diuretics frequently are needed for BP control and can be used with appropriate caution.
ACUTE TREATMENT OF SEVERE HYPERTENSION IN PREGNANCYHydralazine
Intravenous hydralazine in doses of 5 to 10 mg every 20 to 30 minutes is the drug of choice for hypertensive crisis in pregnancy.
Labetalol
Intravenous labetalol is the second most commonly used agent and is given either as a 20-mg loading dose followed by 20 to 30 mg every 30 minutes or as a 1- to 2-mg/min drip. The newborn should be monitored for bradycardia and hypotension.
Nifedipine
Short-acting nifedipine is still being used in a few centers to treat severe hypertension in pregnancy. It can be used when BP cannot be adequately controlled by hydralazine or labetalol.
SECONDARY HYPERTENSIONSecondary hypertension is a less common cause of hyper-tension in pregnancy than essential hypertension and pre-eclampsia. However, undiagnosed pheochromocytoma is associated with a maternal mortality rate as high as 50%. The diagnosis can be made by 24-hour urine measurements of epinephrine, norepinephrine, and their metabolites; values are unaltered in normal pregnancy or preeclampsia. Cocaine use can mimic pheochromocytoma and can be easily detected on toxic screen. Diagnosis of primary hyperaldosteronism is difficult because of alterations in renin and aldosterone secretions during pregnancy. Renovascular hypertension from fibromuscular dysplasia can lead to severe hypertension in pregnancy, and successful control of hypertension with angioplasty has been reported.
PREECLAMPSIA-ECLAMPSIA
Preeclampsia is a multisystem disease unique to human preg-nancy and is the most frequently encountered glomerular complication in pregnancy. It is seen in approximately 5% of pregnancies in the United States, can occur even in molar pregnancies, and usually remits with removal of the placenta. Preeclampsia is characterized by new onset of hypertension (BP of ≥140/90 mm Hg) and proteinuria after 20 weeks of gestation, and is commonly associated with edema and hyper-uricemia. Eclampsia is defined as the occurrence of seizures
in a woman with preeclampsia in which the seizures cannot be attributed to other causes. Notably, preeclampsia is associ-ated with increased lifetime risk for hypertension, ischemic heart disease, stroke, and venous thromboembolism.
RISK FACTORSPreeclampsia is more common in first pregnancies and mul-tigravidas with a new partner, suggesting that prior exposure to paternal antigens may have a protective role. This is fur-ther supported by higher rates of preeclampsia with shorter cohabitation periods prior to pregnancy, barrier method of contraceptive use, and pregnancies induced by artificial insemination with donated sperm. Other risk factors include multiple gestations, molar pregnancies, extremes of maternal age, family history or prior preeclampsia, and underlying maternal medical conditions such as hypertension, diabetes, CKD, obesity, and thrombophilias.
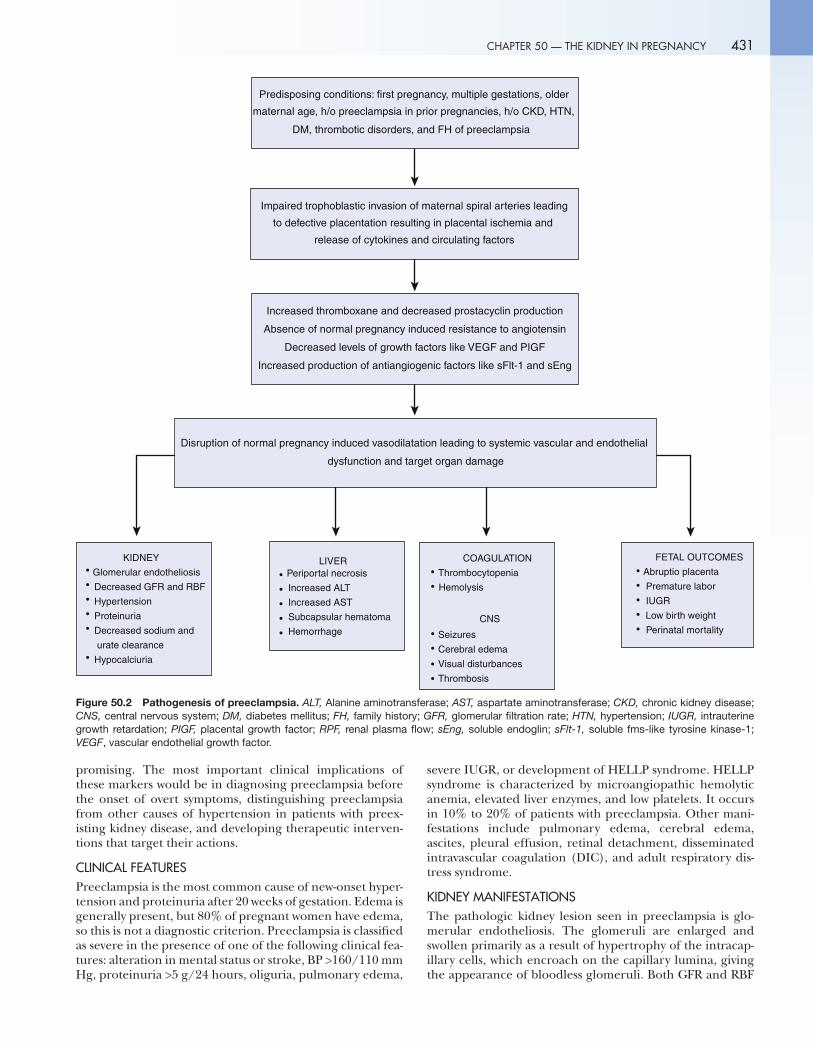
PATHOGENESISPlacental abnormalities are universally noted in preeclamp-sia (Fig. 50.2). During pregnancy, trophoblasts migrate into uterine spiral arteries, transforming the thick muscular arteries into high-capacity vessels that permit greater blood flow to the uteroplacental unit. In preeclampsia, this pro-cess is incomplete and spiral arteries remain high-resistance vessels, leading to inadequate placental oxygen delivery, causing placental ischemia and release of factors that induce maternal vascular endothelial dysfunction. Whether placental ischemia alone is sufficient to cause preeclampsia is debatable because IUGR, also characterized by placental insufficiency, frequently occurs without preeclampsia.
Pregnancy is accompanied by increased production of vasodilator substances such as prostacyclin and NO. Despite the increased production of vasoconstrictors such as throm-boxane and angiotensin, thromboxane increases less than prostacyclin, and there is resistance to the pressor effects of angiotensin. This balance is disrupted in preeclampsia. The ratio of thromboxane and prostacyclin is reversed, NO pro-duction is decreased, and sensitivity to the pressor effects of angiotensin returns before the onset of clinical symptoms.
Over the years, there has been intense effort to identify circulating factors that can explain the pathogenesis and ultimately lead to treatment of preeclampsia. Accumulating evidence points toward the role of placental antiangiogenic factors such as soluble fms-like tyrosine kinase-1 (sFlt1) and soluble endoglin (sEng) in pathogenesis of preeclampsia. sFlt1 is a soluble vascular endothelial growth factor (VEGF) receptor that binds to proangiogenic factors such as VEGF and placental growth factor (PIGF), neutralizing their effects. sEng is a soluble tumor growth factor (TGF) beta co-receptor that inhibits angiogenesis and induces vascular permeability and hypertension. Both sFlt1 and sEng have been shown to increase before onset of preeclampsia, with levels increasing precipitously just before the onset of clini-cal symptoms and generally normalizing several days after delivery, coinciding with improvement in proteinuria and hypertension. It is believed that preeclampsia occurs as a result of a decrease in growth factors such as VEGF and PIGF, along with overproduction of antiangiogenic factors such as sFlt1 and sEng. Although no screening test is yet proven accurate enough to predict preeclampsia, the use of a combination of the previously mentioned factors appears
p90
431 CHAPTER 50 — THE KIDNEY IN PREGNANCY
Predisposing conditions: first pregnancy, multiple gestations, older
maternal age, h/o preeclampsia in prior pregnancies, h/o CKD, HTN,
DM, thrombotic disorders, and FH of preeclampsia
Impaired trophoblastic invasion of maternal spiral arteries leading
to defective placentation resulting in placental ischemia and
release of cytokines and circulating factors
Increased thromboxane and decreased prostacyclin production
Absence of normal pregnancy induced resistance to angiotensin
Decreased levels of growth factors like VEGF and PIGF
Increased production of antiangiogenic factors like sFlt-1 and sEng
Disruption of normal pregnancy induced vasodilatation leading to systemic vascular and endothelial
dysfunction and target organ damage
KIDNEY
Glomerular endotheliosis
Decreased GFR and RBF
Hypertension
Proteinuria
Decreased sodium and
urate clearance
Hypocalciuria
LIVERPeriportal necrosis
Increased ALT
Increased AST
Subcapsular hematoma
Hemorrhage
COAGULATION
Thrombocytopenia
Hemolysis
CNS
Seizures
Cerebral edema
Visual disturbances
Thrombosis
FETAL OUTCOMES
Abruptio placenta
Premature labor
IUGR
Low birth weight
Perinatal mortality
Figure 50.2 Pathogenesis of preeclampsia. ALT, Alanine aminotransferase; AST, aspartate aminotransferase; CKD, chronic kidney disease; CNS, central nervous system; DM, diabetes mellitus; FH, family history; GFR, glomerular filtration rate; HTN, hypertension; IUGR, intrauterine growth retardation; PIGF, placental growth factor; RPF, renal plasma flow; sEng, soluble endoglin; sFlt-1, soluble fms-like tyrosine kinase-1; VEGF, vascular endothelial growth factor.
promising. The most important clinical implications of these markers would be in diagnosing preeclampsia before the onset of overt symptoms, distinguishing preeclampsia from other causes of hypertension in patients with preex-isting kidney disease, and developing therapeutic interven-tions that target their actions.
CLINICAL FEATURESPreeclampsia is the most common cause of new-onset hyper-tension and proteinuria after 20 weeks of gestation. Edema is generally present, but 80% of pregnant women have edema, so this is not a diagnostic criterion. Preeclampsia is classified as severe in the presence of one of the following clinical fea-tures: alteration in mental status or stroke, BP >160/110 mm Hg, proteinuria >5 g/24 hours, oliguria, pulmonary edema,
severe IUGR, or development of HELLP syndrome. HELLP syndrome is characterized by microangiopathic hemolytic anemia, elevated liver enzymes, and low platelets. It occurs in 10% to 20% of patients with preeclampsia. Other mani-festations include pulmonary edema, cerebral edema, ascites, pleural effusion, retinal detachment, disseminated intravascular coagulation (DIC), and adult respiratory dis-tress syndrome.
KIDNEY MANIFESTATIONSThe pathologic kidney lesion seen in preeclampsia is glo-merular endotheliosis. The glomeruli are enlarged and swollen primarily as a result of hypertrophy of the intracap-illary cells, which encroach on the capillary lumina, giving the appearance of bloodless glomeruli. Both GFR and RBF

432 SECTION 9 — THE KIDNEY IN SPECIAL CIRCUMSTANCES
are decreased, the former more than the latter, leading to a 25% reduction in filtration fraction. Because GFR increases in pregnancy, serum creatinine levels in preeclampsia may still appear relatively normal. Proteinuria is generally non-selective and can appear late in pregnancy. The etiology of proteinuria is uncertain because podocytes are typically intact. There is impaired excretion of sodium and uric acid, the latter producing hyperuricemia, an important marker of preeclampsia. In contrast to normal pregnancy, preeclampsia is often associated with hypocalciuria.
FETAL OUTCOMESMost babies of mothers with preeclampsia are at risk for preterm delivery, expedited to minimize maternal com-plications. Chronic placental hypoperfusion may lead to oligohydramnios and IUGR. Abruptio placentae has been reported with severe preeclampsia.
DIAGNOSISDiagnosis of preeclampsia, largely based on the characteris-tic clinical findings described earlier, is difficult in patients with underlying kidney disease and hypertension because these patients commonly have edema, hypertension, and proteinuria at baseline.
TREATMENTDefinitive management of preeclampsia is delivery of the placenta and fetus. When the fetus is mature enough to be delivered, the decision is easy. When the fetus is immature, careful monitoring of both the fetus and mother, treatment of hypertension, and prevention of maternal seizures with magnesium are critical. Continuous magnesium infusion must be cautiously used in kidney disease, with frequent monitoring of serum magnesium levels.
Data on low-dose aspirin for the prevention of preeclamp-sia are conflicting, although a recent metaanalysis suggested a 17% reduction of risk for preeclampsia with antiplatelet agents, largely consisting of low-dose aspirin; risk reductions were most notable in the high-risk group. Accordingly, the UK National Institute of Health and Clinical Excellence 2010 guidelines recommend 75 mg of aspirin daily for women at moderate to high risk for preeclampsia from 12 weeks of gestation until delivery. Data on the role of calcium in preventing preeclampsia are not convincing.
PREECLAMPSIA SUPERIMPOSED ON CHRONIC HYPERTENSION
Women with chronic hypertension who develop new-onset proteinuria after 20 weeks of gestation are diagnosed with superimposed preeclampsia. If such patients have protein-uria at baseline, diagnosis is difficult because proteinuria increases during pregnancy. These patients are considered preeclamptic if severe hypertension develops (≥160/110 mm Hg) in the latter half of pregnancy. Fetal outcomes are worse in hypertensive women with superimposed preeclamp-sia than in normotensive women developing preeclampsia.
GESTATIONAL HYPERTENSION
De novo BP elevation after mid-pregnancy and without proteinuria is classified as gestational hypertension. This
nonspecific diagnosis is generally used only during preg-nancy until a more specific diagnosis can be assigned. If preeclampsia has not developed and BP returns to normal by 12 weeks postpartum, it is called transient hypertension of pregnancy. If hypertension persists beyond 12 weeks postpartum, it is classified as chronic hypertension.
ACUTE KIDNEY INJURY IN PREGNANCY
Acute kidney injury (AKI) is a rare but serious complication. Although any form of AKI that affects adults in the general population can also affect pregnant women, a few causes are particularly common in pregnant women (Box 50.2). Prerenal azotemia is the most common cause of rise in serum creatinine in pregnancy, often occurring in the setting of hyperemesis gravidarum, uterine hemorrhage, or pyelonephritis.
URINARY TRACT OBSTRUCTION
Acute kidney injury from obstruction in pregnancy is seen more often in the setting of solitary kidney and polyhydram-nios. Bilateral ureteral obstruction is a rare complication that generally resolves rapidly with delivery. AKI from func-tional hydronephrosis of pregnancy is rare but has been reported, and normalization of kidney function in lateral recumbent position may help in establishing the diagnosis. In rare cases, delivery of the fetus or percutaneous drain with nephrostomy may be required.
RENAL CORTICAL NECROSIS
Bilateral cortical necrosis is a pathologic diagnosis and can occur with pregnancy-related complications such as abruptio placentae, placenta previa, and prolonged intrauterine death. Severe renal ischemia and primary DIC have been proposed as the inciting agents leading to endothelial damage and thrombosis. Pregnant women with severe renal ischemia are more likely to develop cortical necrosis than the general pop-ulation, and affected women generally have sudden onset of oliguria/anuria with flank pain, hematuria, and hypotension. Computed tomography or ultrasound can help establish the diagnosis by demonstrating hypoechoic or hypodense areas in the renal cortex. Many patients require dialysis with partial renal recovery seen in only to 20% to 40% of the cases.
Volume depletionHyperemesis gravidarumPostpartum bleedingPlacental abruption
SepsisSeptic abortionAcute pyelonephritis
Severe preeclampsiaBilateral cortical necrosisThrombotic microangiopathies (TTP-HUS)Acute fatty liver of pregnancyUrinary tract obstruction from gravid uterus
Box 50.2 Causes of Acute Kidney Injury in Pregnancy
THROMBOTIC MICROANGIOPATHIES
Thrombotic thrombocytopenic purpura (TTP), hemolytic ure-mic syndrome (HUS), and severe preeclampsia with HELLP syndrome are important causes of AKI in late pregnancy.
TTP-HUS is characterized by unexplained thrombocyto-penia and microangiopathic hemolytic anemia with kidney failure frequently present. Traditionally, TTP is considered when neurologic abnormalities are dominant, and HUS when there is profound kidney failure, especially in the postpartum period. TTP has been associated with deficiency of von Willebrand factor cleaving protease (ADAMTS 13) in nonpregnant states, but this association is not established in pregnancy. Mutations in genes encoding complement regu-lation have been associated with pregnancy-related HUS. Regardless, both TTP and HUS in pregnancy are treated with plasma exchange, and the dramatic decline in mater-nal mortality has been credited to its widespread use. Recur-rence of TTP-HUS has been described both in subsequent pregnancies and in response to other inciting factors such as infections and drugs such as cyclosporine.
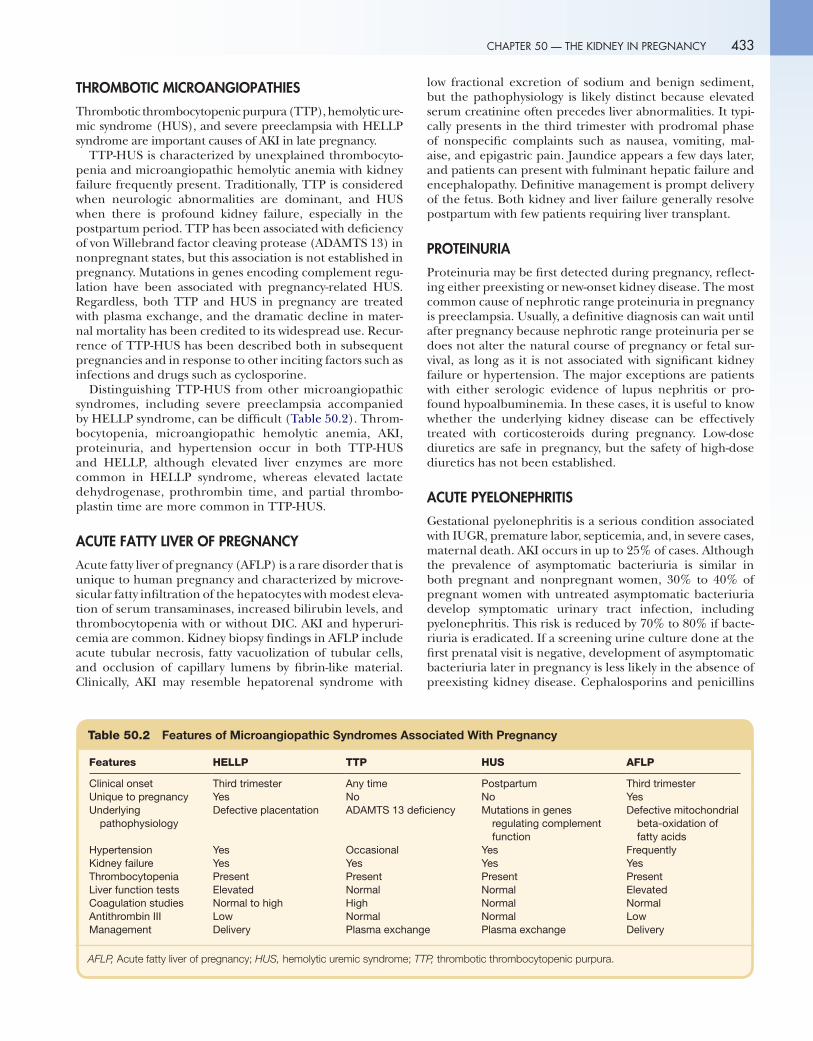
Distinguishing TTP-HUS from other microangiopathic syndromes, including severe preeclampsia accompanied by HELLP syndrome, can be difficult (Table 50.2). Throm-bocytopenia, microangiopathic hemolytic anemia, AKI, proteinuria, and hypertension occur in both TTP-HUS and HELLP, although elevated liver enzymes are more common in HELLP syndrome, whereas elevated lactate dehydrogenase, prothrombin time, and partial thrombo-plastin time are more common in TTP-HUS.
ACUTE FATTY LIVER OF PREGNANCY
Acute fatty liver of pregnancy (AFLP) is a rare disorder that is unique to human pregnancy and characterized by microve-sicular fatty infiltration of the hepatocytes with modest eleva-tion of serum transaminases, increased bilirubin levels, and thrombocytopenia with or without DIC. AKI and hyperuri-cemia are common. Kidney biopsy findings in AFLP include acute tubular necrosis, fatty vacuolization of tubular cells, and occlusion of capillary lumens by fibrin-like material. Clinically, AKI may resemble hepatorenal syndrome with
433 CHAPTER 50 — THE KIDNEY IN PREGNANCY
low fractional excretion of sodium and benign sediment, but the pathophysiology is likely distinct because elevated serum creatinine often precedes liver abnormalities. It typi-cally presents in the third trimester with prodromal phase of nonspecific complaints such as nausea, vomiting, mal-aise, and epigastric pain. Jaundice appears a few days later, and patients can present with fulminant hepatic failure and encephalopathy. Definitive management is prompt delivery of the fetus. Both kidney and liver failure generally resolve postpartum with few patients requiring liver transplant.
PROTEINURIA
Proteinuria may be first detected during pregnancy, reflect-ing either preexisting or new-onset kidney disease. The most common cause of nephrotic range proteinuria in pregnancy is preeclampsia. Usually, a definitive diagnosis can wait until after pregnancy because nephrotic range proteinuria per se does not alter the natural course of pregnancy or fetal sur-vival, as long as it is not associated with significant kidney failure or hypertension. The major exceptions are patients with either serologic evidence of lupus nephritis or pro-found hypoalbuminemia. In these cases, it is useful to know whether the underlying kidney disease can be effectively treated with corticosteroids during pregnancy. Low-dose diuretics are safe in pregnancy, but the safety of high-dose diuretics has not been established.
ACUTE PYELONEPHRITIS
Gestational pyelonephritis is a serious condition associated with IUGR, premature labor, septicemia, and, in severe cases, maternal death. AKI occurs in up to 25% of cases. Although the prevalence of asymptomatic bacteriuria is similar in both pregnant and nonpregnant women, 30% to 40% of pregnant women with untreated asymptomatic bacteriuria develop symptomatic urinary tract infection, including pyelonephritis. This risk is reduced by 70% to 80% if bacte-riuria is eradicated. If a screening urine culture done at the first prenatal visit is negative, development of asymptomatic bacteriuria later in pregnancy is less likely in the absence of preexisting kidney disease. Cephalosporins and penicillins
Table 50.2 Features of Microangiopathic Syndromes Associated With Pregnancy
Features HELLP TTP HUS AFLP
Clinical onset Third trimester Any time Postpartum Third trimesterUnique to pregnancy Yes No No YesUnderlying
pathophysiologyDefective placentation ADAMTS 13 deficiency Mutations in genes
regulating complement function
Defective mitochondrial beta-oxidation of fatty acids
Hypertension Yes Occasional Yes FrequentlyKidney failure Yes Yes Yes YesThrombocytopenia Present Present Present PresentLiver function tests Elevated Normal Normal ElevatedCoagulation studies Normal to high High Normal NormalAntithrombin III Low Normal Normal LowManagement Delivery Plasma exchange Plasma exchange Delivery
AFLP, Acute fatty liver of pregnancy; HUS, hemolytic ure mic syndrome; TTP, thrombotic thrombocytopenic purpura.

p02
434 SECTION 9 — THE KIDNEY IN SPECIAL CIRCUMSTANCES
are generally safe and effective. Treatment should be intra-venous until the patient is afebrile and then continued for 14 days. Relapses of pyelonephritis can occur; accordingly, suppressive therapy with nitrofurantoin or a cephalosporin is recommended in women with normal and abnormal kid-ney function, respectively.
PREGNANCY IN CHRONIC KIDNEY DISEASE
Pregnancy in women with CKD may be complicated by hypertension/preeclampsia, worsening proteinuria, and premature delivery. The most serious concern for women with CKD who conceive is the potential for rapid loss of kid-ney function. The loss occurs irrespective of the cause of the underlying disease, with the risk increasing dramatically once a critical degree of baseline insufficiency is present. Failure to compensate increased GFR in the setting of the increased intraglomerular pressure is the most likely cause of such a rapid decline and cannot be predictably reversed once it occurs, even by terminating the pregnancy. Women who start dialysis for rapidly progressive kidney disease dur-ing pregnancy usually require continued dialysis postpartum. Despite the maternal risk for progressive kidney failure, the likelihood of the pregnancy resulting in a surviving infant is good. The most common adverse fetal outcomes noted are prematurity (40%-70%) and IUGR (20%-60%).
In many women, the initial diagnosis of CKD may occur during pregnancy; however, kidney biopsy typically is deferred until after pregnancy because of fear of increased risk for bleeding. When indicated, a kidney biopsy can be safely done with percutaneous ultrasound guidance in the usual prone position early in pregnancy or in lateral decubi-tus position later in pregnancy.
POLYCYSTIC KIDNEY DISEASE
Advanced kidney disease in women with polycystic kid-ney disease (PKD) generally develops after childbearing age. However, pregnant women with PKD experience an increased incidence of asymptomatic bacteruria, more severe urinary tract infections, and an increase in the size and number of hepatic cysts due to estrogen stimulation. Women with intracranial aneurysms may be at increased risk for subarachnoid hemorrhage during labor.
GITELMAN AND BARTTER SYNDROMES
Increased requirement of potassium and magnesium supple-mentation in pregnant patients with underlying Gitelman syndrome and Bartter syndrome has been reported. Fetal survival is generally good, but these patients need frequent monitoring of their electrolytes.
LUPUS NEPHRITIS
Lupus nephritis is among the most variable and dangerous kidney diseases affecting pregnant women. Pregnancy-related immunologic and hormonal changes are associated with flares in approximately half of lupus nephritis patients, particularly in those with diffuse proliferative lesions. An
45
increase in proteinuria or a decline in GFR, as well as the entire spectrum of life-threatening nonkidney manifesta-tions such as cerebritis, pericarditis, and mesenteric vasculitis, can occur. Preeclampsia is a frequent complication (higher incidence in lupus nephritis compared with lupus patients with no kidney involvement) and often difficult to distinguish from a lupus nephritis flare. Fetal outcomes are generally good, with approximately 75% of pregnancies resulting in surviving infants when therapeutic abortions are excluded. Autoantibodies can cross the placenta, causing transient manifestations of lupus in the newborn. One of the classic manifestations in the neonate is congenital heart block asso-ciated with maternal anti-SSA antibody. Plasmapheresis has been attempted to clear anti-SSA antibodies without consis-tent success.
Although antiphospholipid antibody syndrome (APS) was initially considered wholly a part of the SLE syndrome, it has become increasingly evident that it can occur as a pri-mary disease. APS is associated with a high risk for repeated abortions before 20 weeks gestation and unexpected intra-uterine deaths in the second and third trimesters. Maternal complications include venous and/or arterial thrombosis, thrombocytopenia, pregnancy-induced hypertension, and preeclampsia. Management of APS consists of low-dose aspirin and heparin use.
New-onset lupus is an indication for biopsy during preg-nancy since proliferative lupus nephritis requires prompt treatment, and first-line treatments are teratogenic (Table 50.3). Cyclosporine, azathioprine, and prednisone are con-sidered safer in pregnancy than other agents, with cyclo-sporine probably being the most effective. For women with preexisting lupus nephritis, pregnancy is safest if the disease is in remission for 6 months on less than 10 mg daily pred-nisone, serum creatinine is less than 1.5 mg/dL, and BP is well controlled.
PREGNANCY IN DIALYSIS PATIENTS
Conception is rare in dialysis patients and is associated with poor fetal outcomes. Emerging data suggest that intensive dialysis results in better outcomes and may be a viable option for women whose reproductive years might otherwise be lost to CKD.
Menstrual irregularities generally begin as GFR falls below 15 mL/min, with amenorrhea typical at GFR below 5 mL/min. Early menopause is common, and, even in those patients who menstruate, cycles are often anovulatory. Numerous endocrine abnormalities have been suggested to play a role, including absent luteinizing hormone surge, shortened luteal phase, decreased progesterone and estra-diol levels, and higher prolactin levels. Furthermore, lack of libido from medications, anemia, depression, and fatigue is common. Fertility rates are uncertain, ranging from 0.3% to 1% per year, with recent data suggesting improved con-ception rates. Conception rates appear significantly lower in women treated with peritoneal dialysis. Possibly, hypertonic solutions in the intraperitoneal space or compression of the fallopian tubes may interfere with transport of the ovum to the fallopian tube.
Pregnancy outcomes have significantly improved since the report of the first successful pregnancy in a dialysis patient
435 CHAPTER 50 — THE KIDNEY IN PREGNANCY
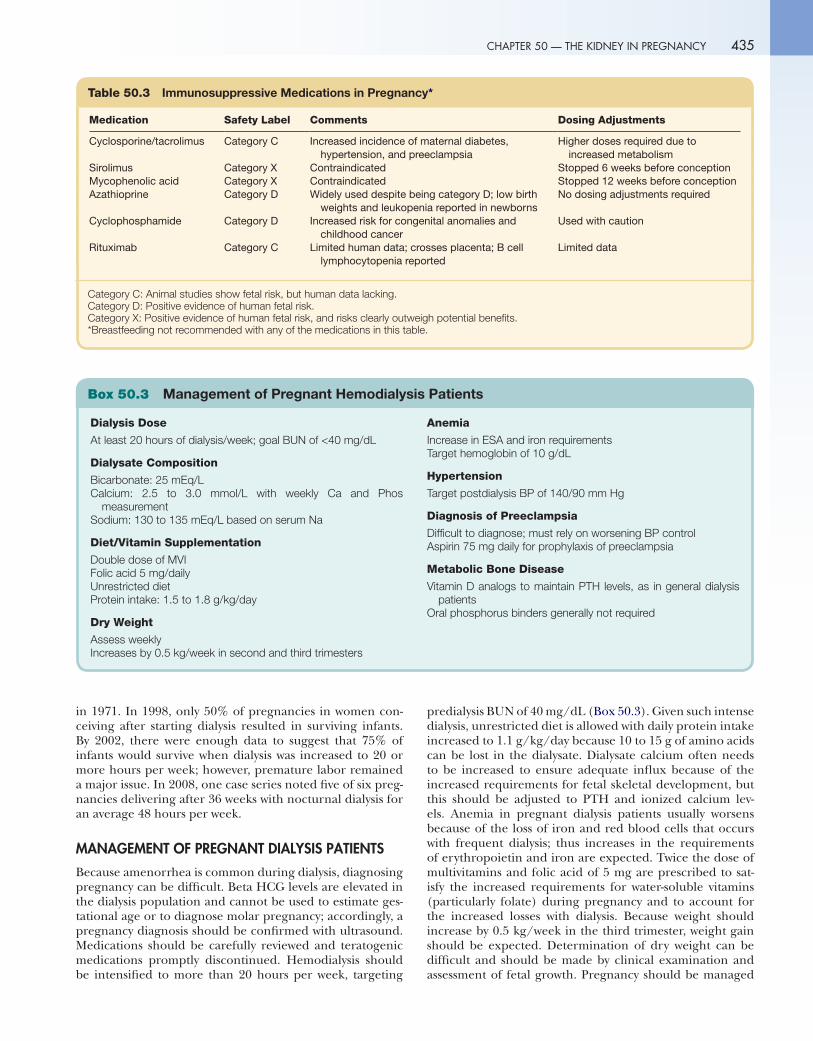
Table 50.3 Immunosuppressive Medications in Pregnancy*
Medication Safety Label Comments Dosing Adjustments
Cyclosporine/tacrolimus Category C Increased incidence of maternal diabetes, hypertension, and preeclampsia
Higher doses required due to increased metabolism
Sirolimus Category X Contraindicated Stopped 6 weeks before conceptionMycophenolic acid Category X Contraindicated Stopped 12 weeks before conceptionAzathioprine Category D Widely used despite being category D; low birth
weights and leukopenia reported in newbornsNo dosing adjustments required
Cyclophosphamide Category D Increased risk for congenital anomalies and childhood cancer
Used with caution
Rituximab Category C Limited human data; crosses placenta; B cell lymphocytopenia reported
Limited data
Category C: Animal studies show fetal risk, but human data lacking.Category D: Positive evidence of human fetal risk.Category X: Positive evidence of human fetal risk, and risks clearly outweigh potential benefits.*Breastfeeding not recommended with any of the medications in this table.
Dialysis Dose
At least 20 hours of dialysis/week; goal BUN of <40 mg/dL
Dialysate Composition
Bicarbonate: 25 mEq/LCalcium: 2.5 to 3.0 mmol/L with weekly Ca and Phos
measurementSodium: 130 to 135 mEq/L based on serum Na
Diet/Vitamin Supplementation
Double dose of MVIFolic acid 5 mg/dailyUnrestricted dietProtein intake: 1.5 to 1.8 g/kg/day
Dry Weight
Assess weeklyIncreases by 0.5 kg/week in second and third trimesters
Anemia
Increase in ESA and iron requirementsTarget hemoglobin of 10 g/dL
Hypertension
Target postdialysis BP of 140/90 mm Hg
Diagnosis of Preeclampsia
Difficult to diagnose; must rely on worsening BP controlAspirin 75 mg daily for prophylaxis of preeclampsia
Metabolic Bone Disease
Vitamin D analogs to maintain PTH levels, as in general dialysis patients
Oral phosphorus binders generally not required
Box 50.3 Management of Pregnant Hemodialysis Patients
in 1971. In 1998, only 50% of pregnancies in women con-ceiving after starting dialysis resulted in surviving infants. By 2002, there were enough data to suggest that 75% of infants would survive when dialysis was increased to 20 or more hours per week; however, premature labor remained a major issue. In 2008, one case series noted five of six preg-nancies delivering after 36 weeks with nocturnal dialysis for an average 48 hours per week.
MANAGEMENT OF PREGNANT DIALYSIS PATIENTS
Because amenorrhea is common during dialysis, diagnosing pregnancy can be difficult. Beta HCG levels are elevated in the dialysis population and cannot be used to estimate ges-tational age or to diagnose molar pregnancy; accordingly, a pregnancy diagnosis should be confirmed with ultrasound. Medications should be carefully reviewed and teratogenic medications promptly discontinued. Hemodialysis should be intensified to more than 20 hours per week, targeting
predialysis BUN of 40 mg/dL (Box 50.3). Given such intense dialysis, unrestricted diet is allowed with daily protein intake increased to 1.1 g/kg/day because 10 to 15 g of amino acids can be lost in the dialysate. Dialysate calcium often needs to be increased to ensure adequate influx because of the increased requirements for fetal skeletal development, but this should be adjusted to PTH and ionized calcium lev-els. Anemia in pregnant dialysis patients usually worsens because of the loss of iron and red blood cells that occurs with frequent dialysis; thus increases in the requirements of erythropoietin and iron are expected. Twice the dose of multivitamins and folic acid of 5 mg are prescribed to sat-isfy the increased requirements for water-soluble vitamins (particularly folate) during pregnancy and to account for the increased losses with dialysis. Because weight should increase by 0.5 kg/week in the third trimester, weight gain should be expected. Determination of dry weight can be difficult and should be made by clinical examination and assessment of fetal growth. Pregnancy should be managed

p
436 SECTION 9 — THE KIDNEY IN SPECIAL CIRCUMSTANCES
by a multi-disciplinary team that includes high-risk obstetri-cians and nephrologists.
PREGNANCY IN KIDNEY TRANSPLANT
Sexual dysfunction and infertility often reverse posttransplan-tation. Optimal contraception should be initiated during the peritransplant period. Since intrauterine devices need an intact immune system to function efficiently and high failure rates are associated with barrier methods, oral contraceptive pills may be the best choice, presuming that BP is adequately controlled. Alternatively, two barrier methods can be used in combination.
The optimal timing of pregnancy depends on the indi-vidual circumstances of the transplant recipient. Because women with CKD experience premature menopause, both chronologic age and risk for early menopause should be considered when planning for pregnancy posttransplant. The consensus opinion of the American Transplant Society is that pregnancy can be planned when the patient reaches 1 year posttransplantation, as long as the following criteria are met: adequate kidney function, stable immunosuppres-sive medication dosing in place, no rejection episodes in the past year, no recent infections that could jeopardize fetal survival, and no teratogenic medications being taken.
The major concerns are the effect of pregnancy on maternal allograft function and potential side effects of medications on fetal growth. Preeclampsia, premature deliv-ery, low birth weight, and neonatal deaths are common in transplant recipients. Case-control studies have shown no increase in graft loss and do not indicate that pregnancy per se increases rejection risk; however, detection of rejection can be difficult because of pregnancy-related changes in renal physiology. When it doubt, kidney biopsy can be safely performed. Management of hypertension is important since many of these patients have chronic hypertension. Treatment recommendations are generally more aggressive than in the general pregnant population; targeting normo-tension is the goal.
All immunosuppressive medications cross the maternal-fetal circulation, and no choice exists other than to expose the fetus to the least offensive medications. Much remains to be learned about the pharmacokinetics and pharmaco-dynamics of immunosuppressive medications during preg-nancy, and as expected, most of the available information is from retrospective review and clinical experience (see Box 50.3). Maintenance immunosuppression in pregnant trans-plant patients generally includes cyclosporine or tacrolimus, azathioprine, and prednisone. Mycophenolate should be avoided in transplant patients planning to become pregnant,
0310
with azathioprine frequently used in its place. Antibodies used to treat rejection, such as thymoglobulin and alemtu-zumab, cross the placenta. There is insufficient experience with these agents in pregnancy. Their use would seem prefer-able to losing the kidney, but this should be reserved for cases in which high-dose steroids are ineffective and a reasonable chance exists that the kidney can be salvaged.
BIBLIOGRAPHYAbalos E, Duley L, Steyn DW, et al: Antihypertensive drug therapy for
mild to moderate hypertension during pregnancy, Cochrane Database Syst Rev 2007.
Barua M, Hladunewich M, Keunen J, et al: Successful pregnancies on nocturnal home hemodialysis, Clin J Am Soc Nephrol 3:392-396, 2008.
Baumann MU, Nick A, Bersinger, et al: Serum markers for predicting preeclampsia, Mol Aspects Med 28:227-244, 2007.
Bobrie G, Liote F, Houillier P, et al: Pregnancy in lupus nephritis and related disorders, Am J Kidney Dis. 9:339, 1987.
Cornelis T, Odutayo A, Keunen J, et al: The kidney in normal pregnancy and preeclampsia, Semin Nephrol 31:4-14, 2011.
Davison JM: Changes in renal function in early pregnancy in women with one kidney. Yale J Biol Med 51:347-349, 1978.
Davison JM: The kidney in pregnancy: a review, J Royal Soc Med 76:485-500, 1983.
Duley L, Henderson-Smart DJ, Meher S, et al: Anti-platelet agents for preventing preeclampsia and its complications, Cochrane Database Syst Rev 2004.
Fakhouri F, Roumenina L, Provot F, et al: Pregnancy-associated hemolytic syndrome revisited in the era of complement gene mutations, J Am Soc Nephrol 21:859-867, 2010.
Hladunewich M, Hercz AE, Keunen J, et al: Pregnancy in end stage renal disease, Semin Dialysis 24:634-639, 2011.
Hou SH, Grossman SD, Madias NE: Pregnancy in women with renal disease and moderate renal insufficiency, Am J Med 78:185-194, 1985.
Imbasciati E, Gregorini G, Cabiddu G, et al: Pregnancy in CKD stages 3 to 5: fetal and maternal outcomes, Am J Kidney Dis 49:753-762, 2007.
Lindheimer MD, Davison JM, Katz AI: The kidney and hypertension in pregnancy: twenty existing years, Semin Nephrol 21:173-189, 2001.
Maynard SE, Karumanchi SA: Angiogenic factors and preeclampsia, Semin Nephrol 31:33-46, 2011.
McKay DB, Josephson MA: Pregnancy after kidney transplantation, Clin J Am Soc Nephrol 3:S117-S125, 2008.
National Collaborating Centre for Women’s and Children Health: Hypertension in pregnancy: the management of hypertensive disorders during pregnancy London, 2010, Royal College of Obstetricians and Gynae-cologists. Availablehttp://guidance.nice.org.uk/CG107/guidance.
Okundaye IB, Abrinko P, Hou S: A registry for pregnancy in dialysis patients, Am J Kidney Dis 31:766-773, 1998.
Report of the national high blood pressure education program working group on high blood pressure in pregnancy, Am J Obstet Gynecol 183: S1-S22, 2000; July.
Sibai BM, Grossman RA, Grossman SG: Effects of diuretics on plasma vol-ume in pregnancies with long term hypertension, Am J Obstet Gynecol 150:831-835, 1984.
Singh Ajay K: Lupus nephritis and the anti-phospholipid antibody syndrome in pregnancy, Kidney Int 58:2240-2254, 2000.
Smith MC, Moran P, Ward MK, et al: Assessment of glomerular filtration rate during pregnancy using the MDRD formula, BJOG 115:109-112, 2008.