nanoparticle-encapsulated doxorubicin enhances cryoablation of cancer stem-like cells
TRANSCRIPT

Nanoparticle-encapsulated doxorubicin enhances cryoablation of cancer stem-like cells Wei Rao1,2, Adriano Bellotti5, Peter J. Littrup6, Jianhua Yu3,4, Xiongbin Lu7 & Xiaoming He1,2,3
Cryoablation is a promising minimally invasive technology for cancer treatment. However, no study was reported concerning the effect of cryoablation on cancer stem-like cells (CSCs) that are capable of reinitiating tumor growth after conventional chemotherapy. Using a biomimetic 3D mammosphere model, we found that cryoablation alone could signifi cantly but incompletely destroy CD44+CD133+ CSCs. Moreover, the combination of cryoablation and conventional chemotherapy using free doxorubicin (fDOX) does not signifi -cantly enhance destruction of the CSCs over the individual treatments. We develop a novel combined treatment of cryoablation and nanoparticle-encapsulated doxorubicin (nDOX) that is capable of achieving nearly complete elimination of the CSCs (from 16.6 to 0.6%). This is attributed in part to the much-enhanced uptake of nDOX (compared to fDOX) by the CSCs. Collectively, this study demonstrates the great potential of a combined therapy of cryoablation and nanodrug for improved cancer treatment by eliminating the root of cancer — the CSCs.
INNOVATIONCryoablation has been explored for treating various cancers and is particularly attractive for fi ghting against breast cancer due to its excellent cosmetic outcome. However, the incomplete destruction of cancer stem-like cells (CSCs) by cryoablation alone may result in post-operational cancer recurrence, a problem that has been plaguing the conventional chemotherapy using free drug for years. Th erefore, the combined treat-ment of cryoablation and nanodrug that is shown using a biomimetic 3D mammosphere model to be particularly eff ective against the CSCs is an innovative strategy for improving the safety and effi cacy of cancer cryoablation. In addition, the use of nanodrug could improve drug delivery to tumor and minimize the drug systemic toxicity in vivo, further enhancing the translational nature of the combined therapy. Th erefore, the nanodrug-based combined treatment of chemo and cryotherapy are likely to emerge as an eff ective clinical strategy for eliminating cancer, particularly malignancies that are refractory to conventional therapies.
INTRODUCTIONCryoablation (also called cryosurgery or cryotherapy) is an energy-based, minimally invasive surgical technique that has been investigated to treat a variety of diseases (e.g., cardiovascular diseases and cancer of various origins including the breast) by freezing the tissue to subzero temperatures using one or more cryoprobes1–3. Th e event of cell death during cryoabla-tion is either directly or indirectly related to ice formation at sub-zero temperatures as has been reviewed elsewhere4–8. For example, signifi cant intracellular ice formation (IIF) is lethal to living cells during cryoablation.
TECHNOLOGY
Ice formed extracellularly can result in an increase in solute concentration in the unfrozen extracellular solution (freeze-concentration), which could compromise living cells as a result of the freeze-concentration induced cell dehydration, protein denaturation, and lipid phase transition within the cells. Although the IIF and freeze-concentration induced cell injury are dependent on the whole thermal history including cooling rate, end temperature, and holding time at the end temperature experienced by cells, the end temperature is generally accepted as the most important parameter in determining cryoinjury during cryoablation5–8. An end temperature below ~ –20 °C is usually required to kill cancer cells while the temperature at the outer peripheral of a frozen tumor iceball created during cryoablation using cryoprobes is much higher than –20 °C1–9.
To improve the effi cacy of cryoablation for cancer treatment at high subzero temperatures (> –20 °C), various strategies have been recently explored to augment cryoinjury to cancer cells. For example, the modifi ca-tion of ice morphology by adding glycine (a nonessential amino acid) or an excess of electrolytes (e.g., sodium and potassium chloride) has been found to enhance cryoinjury to prostate and breast tumor cells10,11. Antifreeze proteins used by arctic fi sh to protect them from freezing have been shown to actually enhance cryoinjury to prostate tumor cells once the cells are frozen, via a mechanism also related to the change of ice morphology12,13. A signifi cant enhancement in cryoablation of prostate tumor has been achieved by inducing pre-treatment infl ammation in the tumor using tumor necrosis factor-alpha (TNF-α) either in its free form or tethered to gold nanoparticles14,15. Enhanced suppression of tumor growth has been observed by combining cryoablation with the local injection of immunopotentiator or mild systemic chemotherapy16. Lastly, anticancer
1Department of Biomedical Engineering , 2Davis Heart and Lung Research Institute, 3Comprehensive Cancer Center, 4Division of Hematology, The Ohio State University, Columbus, OH 43210, USA. 5Department of Biomedical Engineering, North Carolina State University, Raleigh, NC 27606, USA. 6Departments of Interventional Radiology and Oncology, Barbara Ann Karmanos Cancer Institute, Detroit, MI 48201, USA. 7Department of Cancer Biology, The University of Texas MD Anderson Cancer Center, Houston, TX 77030, USA. Correspondence should be addressed to X.H. ([email protected]).
Received 9 March 2013; accepted 22 November 2013; published online 23 January 2014; doi:10.1142/S2339547814500022
28 TECHNOLOGY l VOLUME 2 • NUMBER 1 • MARCH 2014© World Scientific Publishing Co./Imperial College Press
ARTICLE
1450002.indd 281450002.indd 28 3/24/2014 2:31:50 PM3/24/2014 2:31:50 PM
Tec
hnol
ogy
2014
.02:
28-3
5. D
ownl
oade
d fr
om w
ww
.wor
ldsc
ient
ific
.com
by U
NIV
ER
SID
AD
E D
E V
IGO
BIB
LIO
TE
CA
CE
NT
RA
L o
n 04
/22/
14. F
or p
erso
nal u
se o
nly.

29TECHNOLOGY l VOLUME 2 • NUMBER 1 • MARCH 2014© World Scientific Publishing Co./Imperial College Press
ARTICLE
drugs for chemotherapy such as peplomycin, 5-fl uorouracil, bleomycin, and doxorubicin in their free form have been shown to enhance cryoinjury to prostate, liver, and lung tumor cells under mild freezing conditions by inducing apoptosis in the cells17,18. Enhancement of cryoablation using anticancer drugs is of particular interest because both cryoablation and anticancer drugs have been used for treating cancer in the clinic.
However, no study was reported to date concerning the eff ect of cryoablation or the combination of cryoablation and anticancer drug on the cancer stem-like cells (CSCs), rare cell subpopulations among cancer cells that are capable of self-renewal to maintain their “stemness” and diff erentiation to create the heterogeneity in tumor19–21. Th ere is mounting evidence from both basic and clinical studies that the CSCs are responsible for cancer recurrence and metastasis associated with conventional chemotherapy, due at least in part to their high resistance to free anticancer drugs19–22. More recently, it has been shown that the drug resistance of CSCs and multidrug resistant cells can be overcome by delivering anticancer drug using either polymeric or inorganic nanoparticles23–26. Although inorganic nanoparticles (without drug en-capsulation) of high thermal conductivity have been shown to improve the outcome of cryoablation by enhancing the heat transfer in biological samples27,28, the combination of nanoparticle-encapsulated anticancer drug and cryoablation on cancer cells (and particularly, the CSCs) has not yet been explored.
In this study, we investigated the eff ect of cryoablation alone and its combination with free doxorubicin (fDOX) or nanoparticle-encapsulated doxorubicin (nDOX) on CD44+CD133+ mammary CSCs. CD44 and CD133 are two commonly used cell surface markers for judging CSCs of various malignancies including breast cancer22,29–31. Doxorubicin has been clinically used to treat breast cancer and the nanoparticles used in this study has been shown to target CSCs with great biocompat-ibility in our recent studies23,32,33. Our results show that cryoablation alone is not eff ective in destroying CSCs when the end temperature (or fi nal freezing temperature) is not lower than –8.5 °C and that the combination of cryoablation and doxorubicin (either fDOX or nDOX) at this high subzero temperature is not signifi cantly better than drug treatment alone. Cryoablation alone at –17.4 °C can signifi cantly but not preferentially destroy CSCs, which is not signifi cantly enhanced by combining cryoablation with fDOX (1 μg/ml). In contrast, the combina-tion of cryoablation at –17.4 °C and nDOX (1 μg/ml) can signifi cantly augment the destruction of CSCs (compared to cryoablation or nDOX alone), resulting in eliminating nearly all CSCs (from 16.6 ± 2.8% to 0.6 ± 0.2% for the percentage of the CSC subpopulations). Taken together, this study demonstrates the great potential of a novel combined therapy of cryoablation and nanodrug for improving the safety and effi cacy of treating breast cancer by eliminating the root of cancer resistance associ-ated with conventional chemotherapy — the CSCs.
RESULTS
Destruction of mammosphere cells by cryoablation aloneTh e presence of the rare mammary cancer stem-like cell (CSC) subpopu-lations among mammary cancer cells is evidenced by the formation of mammospheres when mammary cancer cells are cultured singly in stem cell medium in ultralow attachment plate because detached non-stem cancer cells should die (of anoikis) under the non-adherent culture condi-tion23,34,35. Moreover, the mammospheres have been shown to be enriched with CSCs with much higher expression of stem cell genes (e.g., Oct4 and Nanog) and surface marker proteins (e.g., CD44 and CD133) than the parental cancer cells used to obtain the mammospheres23. Th erefore, we fi rst investigated the eff ect of cryoablation on CSCs either singly suspended in culture medium (single cell model, Fig. 1a) or resided in 3D mammospheres (mammosphere model, Fig. 1a) by studying the survival of the mammosphere cells 10 days aft er the cryoablation treatment. Th e 10-day culture time post cryoablation was used to allow enough time for
the CSCs survived the cryoablation treatment to divide, diff erentiate, and grow to form mammospheres23,34,35.
Typical micrographs showing morphologic diff erences between the samples 10 days aft er cryoablation at –2.6, –8.5, or –17.4 °C together with that of samples without cryoablation (37 °C) are given in Fig. 1b. For both the single cell and mammosphere models, it appears that cryoablation at –2.6 or –8.5 °C was not eff ective at all in destroying the mammosphere cells although cryoablation at –17.4 °C greatly reduced both the number and size of mammospheres. This morphological observation was further confi rmed by the quantitative survival of mam-mosphere cells aft er the various treatments as shown in Fig. 1c. Th e cell survival in samples treated with cryoablation at –2.6 or –8.5 °C was not signifi cantly diff erent from that in the control (37 °C) sample. With cryoablation at –17.4 °C, the cell survival was signifi cantly (p = 8.9 × 10–7 and 0.00034 for the mammosphere and single cell model, respectively) reduced to 20–30%. However, no signifi cant diff erence in the cell sur-vival was observed between the single cell and mammosphere model for cryoablation at any of the three diff erent temperatures, which suggests that the microenvironment or niche (i.e., culture medium versus the proteinaceous and cellular microenvironment in 3D mammosphere34) has minimal impact on the sensitivity of CSCs to cryoablation. Since 20–30% of mammosphere cells still survived cryoablation alone at –17.4 °C, we further investigated the eff ect of the combination of cryoablation and anticancer drug (fDOX or nDOX) on the mammosphere cells and the CSCs in particular.
Destruction of mammosphere cells by the combination of cryoablation and anticancer drugWe fi rst examined the combined treatment in inhibiting/destroying the mammosphere cells using the single cell model of CSCs. As shown in Supplementary Fig. 1, either fDOX or nDOX alone was eff ective in inhibiting the formation of mammospheres from the singly suspended CSCs and the combination of the drugs with cryoablation (from 1 to 1.5 h during a 10-day incubation with the drugs) did not signifi cantly aff ect the eff ectiveness at all. Th erefore, this work is focused on examining the effi cacy in destroying mammosphere cells and CSCs by the combined treatment using the mammosphere model hereaft er. Compared to the single cell model, the 3D model of mammospheres enriched with CSCs more closely mimics the 3D tumor microenvironment in human patients.
Typical micrographs showing morphologic diff erences at day 10 between the samples with various treatments and the corresponding quantitative cell survival data are given in Fig. 2a,b, respectively. As controls for the nDOX treatment, the corresponding morphologic and quantitative data for samples treated with nanoparticles (NP) are also shown in the fi gure. Clearly, the combined treatments with cryoablation at –2.6 or –8.5 °C were not signifi cantly diff erent from the corresponding drug (fDOX or nDOX) treatment alone at 37 °C. Th is observation holds true for the combination of NP and cryoablation at –2.6 or –8.5 °C and the cell survival was not signifi cantly diff erent from the no-treatment control (ND) at 37 °C, indicating the nontoxic nature of the nanoparticles used in this study.
As shown in Fig. 2b, aft er cryoablation at –17.4 °C, all the combined treatments were signifi cantly (p = 0.00015, 0.02, and 0.00014 for NP, fDOX, and nDOX, respectively) different from the drug treatment alone at 37 °C. However, the combination of fDOX and cryoablation at –17.4 °C was not signifi cantly diff erent from the cryoablation treatment alone. In contrast, the combined treatment of nDOX and cryoablation at –17.4 °C was signifi cantly (p = 0.0002) diff erent from the cryoablation treatment alone, and more importantly, it was signifi cantly (p = 0.00009) diff erent from the combination of nanoparticles (NP) treatment and cryoablation at –17.4 °C. Interestingly, the combination of nanoparticles and cryoablation at –17.4 °C was also signifi cantly diff erent from either the nanoparticles treatment alone (p = 0.00015) or the cryoablation treatment alone (p = 0.00079).
1450002.indd 291450002.indd 29 3/24/2014 2:31:52 PM3/24/2014 2:31:52 PM
Tec
hnol
ogy
2014
.02:
28-3
5. D
ownl
oade
d fr
om w
ww
.wor
ldsc
ient
ific
.com
by U
NIV
ER
SID
AD
E D
E V
IGO
BIB
LIO
TE
CA
CE
NT
RA
L o
n 04
/22/
14. F
or p
erso
nal u
se o
nly.

ARTICLE
30 TECHNOLOGY l VOLUME 2 • NUMBER 1 • MARCH 2014© World Scientific Publishing Co./Imperial College Press
Destruction of CD44+CD133+ CSCs in mammospheres by the combination of cryoablation and anticancer drugTo identify the cancer stem-like cells among the mammosphere cells, we used CD44 and CD133, two cell surface markers that are overexpressed on CSCs of various malignancies (including breast cancer) and have been commonly used to judge the presence of CSCs22,29–31. Moreover, CD44+CD133+ cell subpopulations have been postulated to be responsible for cancer recurrence after conventional chemotherapy and cancer metastasis22,29–31. Th erefore, we further performed fl ow cytometry studies to understand how the various treatments could aff ect the percentage of the CD44+CD133+ cell subpopulations among the mammosphere cells.
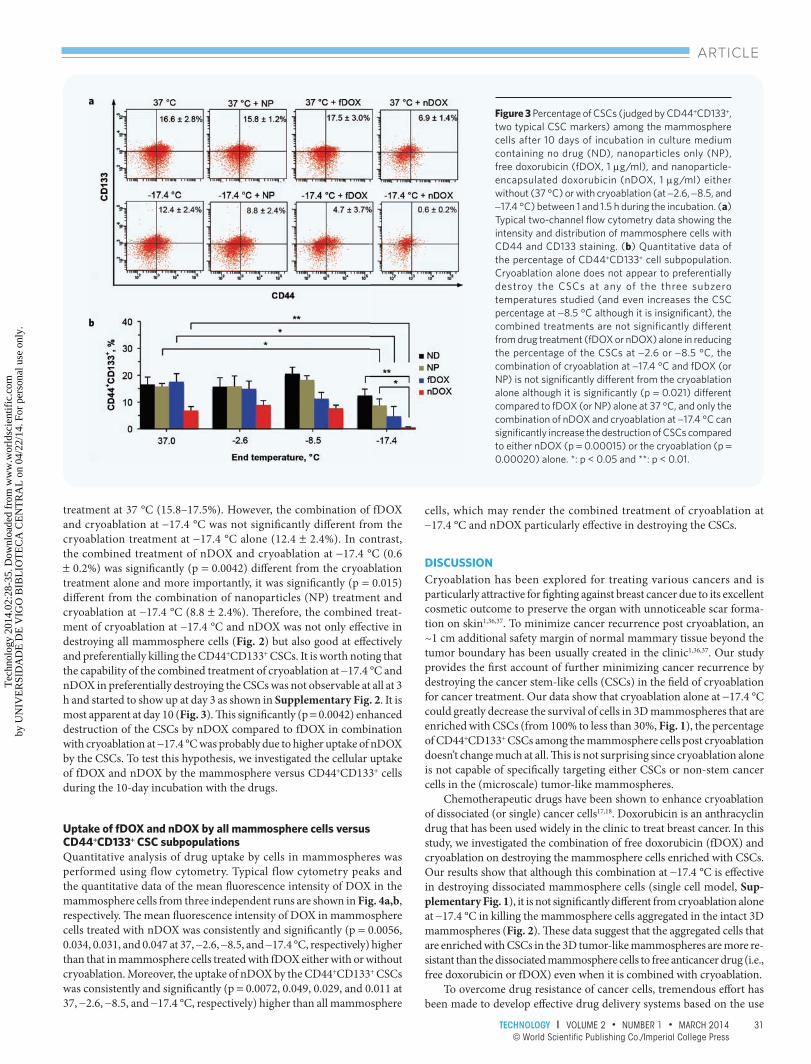
As shown in Fig. 3, cryoablation alone at all three subzero tempera-tures did not signifi cantly alter the percentage of CD44+CD133+ cells although the percentage did appear to increase and decrease slightly at –8.5 and −17.4 °C, respectively. Th e combination of cryoablation at −2.6 and −8.5 °C and anticancer drug (either fDOX or nDOX) was not
Figure 1 Morphologic and quantitative survival of mammosphere cells containing the cancer stem-like cells (CSCs) 10 days after cryoablation at three different subzero temperatures when the CSCs were initially either suspended singly (single cell model) in culture medium or resided in 3D mammospheres (mammosphere model). (a) Typical micrographs showing cell morphology in single cell versus mammosphere model on day 0 before treatment. Note that the same number of mammosphere cells was used in the two models: the cell density appears dilute for the single cell model because the dissociated mammosphere cells suspended homogeneously in culture medium while for the mammosphere model, the aggregated cells sank down on the bottom of dish and appears dense. (b) Typical micrographs showing morphologic survival of the CSCs indicated by the presence of mammospheres under non-adherent culture in stem cell medium. (c) Quantitative survival of the mammosphere cells that contain the CSCs. The data show that cryoablation alone can signifi cantly (p = 8.9 × 10–7 and 0.00034 for mammosphere and single cell model, respectively) decrease the survival of mammosphere cells (from 100% to less than ∼30%) at or below −17.4 °C but is not effective at all in destroying the cells at or above −8.5 °C. In addition, no signifi cant difference was observed between the single cell and mammosphere model. **: p < 0.01.
signifi cantly diff erent from the drug treatment alone (at 37 °C) in terms of their eff ect on the percentage of CD44+CD133+ cells. Th is observation holds true for the combination of NP and cryoablation at −2.6 or −8.5 °C and the percentage was not signifi cantly diff erent from the no-treatment control (ND at 37 °C). Interestingly, unlike its impact on the viability of all mammosphere cells shown in Fig. 2b, the combination of nanoparticles and cryoablation at −17.4 °C was not signifi cantly diff erent from cryoa-blation alone in altering the percentage of CD44+CD133+ cells although it is signifi cantly (p = 0.033) diff erent from the nanoparticles treatment alone (NP at 37 °C). In other words, the combination of cryoablation and nanoparticles without anticancer drug is ineff ective in preferentially destroying the CSCs.
The combined treatment of cryoablation at −17.4 °C with na-noparticles, fDOX, or nDOX could signifi cantly (p = 0.033, 0.029, and 0.0054 for NP, fDOX, and nDOX, respectively) lower the percentage of CD44+CD133+ cells compared to the nanoparticles or drugs alone
Figure 2 Morphologic and quantitative survival of aggregated mammosphere cells (3D mammosphere model enriched with CSCs) after 10 days incubation in culture medium containing no drug (ND), nanoparticles only (NP), free doxorubicin (fDOX, 1 µg/ml), and nanoparticle-encapsulated doxorubicin (nDOX, 1 µg/ml) either without (37 °C) or with cryoablation (at −2.6, −8.5, and −17.4 °C) between 1 and 1.5 h during the incubation. (a) Typical micrographs showing morphologic survival of the mammosphere cells. (b) The corresponding quantitative cell survival. The data show that the combined treatment of cryoablation at −2.6 or −8.5 °C and drug (fDOX or nDOX) is not significantly different from the drug treatment alone (at 37 °C) in destroying the mammosphere cells, and the combined treatment of cryoablation at −17.4 °C and fDOX is not signifi cantly different from the cryoablation treatment alone at −17.4 °C. In contrast, the combined treatment of cryoablation at −17.4 °C and nDOX is signifi cantly more effective than either cryoablation (p = 0.0002) or nDOX (p = 0.00015) alone in destroying the mammosphere cells. In addition, the cytotoxicity of NPs at or above −8.5 °C is negligible. *: p < 0.05 and **: p < 0.01.
1450002.indd 301450002.indd 30 3/24/2014 2:31:52 PM3/24/2014 2:31:52 PM
Tec
hnol
ogy
2014
.02:
28-3
5. D
ownl
oade
d fr
om w
ww
.wor
ldsc
ient
ific
.com
by U
NIV
ER
SID
AD
E D
E V
IGO
BIB
LIO
TE
CA
CE
NT
RA
L o
n 04
/22/
14. F
or p
erso
nal u
se o
nly.
31TECHNOLOGY l VOLUME 2 • NUMBER 1 • MARCH 2014© World Scientific Publishing Co./Imperial College Press
ARTICLE
treatment at 37 °C (15.8–17.5%). However, the combination of fDOX and cryoablation at −17.4 °C was not signifi cantly diff erent from the cryoablation treatment at −17.4 °C alone (12.4 ± 2.4%). In contrast, the combined treatment of nDOX and cryoablation at −17.4 °C (0.6 ± 0.2%) was signifi cantly (p = 0.0042) diff erent from the cryoablation treatment alone and more importantly, it was signifi cantly (p = 0.015) diff erent from the combination of nanoparticles (NP) treatment and cryoablation at −17.4 °C (8.8 ± 2.4%). Th erefore, the combined treat-ment of cryoablation at −17.4 °C and nDOX was not only eff ective in destroying all mammosphere cells (Fig. 2) but also good at eff ectively and preferentially killing the CD44+CD133+ CSCs. It is worth noting that the capability of the combined treatment of cryoablation at −17.4 °C and nDOX in preferentially destroying the CSCs was not observable at all at 3 h and started to show up at day 3 as shown in Supplementary Fig. 2. It is most apparent at day 10 (Fig. 3). Th is signifi cantly (p = 0.0042) enhanced destruction of the CSCs by nDOX compared to fDOX in combination with cryoablation at −17.4 °C was probably due to higher uptake of nDOX by the CSCs. To test this hypothesis, we investigated the cellular uptake of fDOX and nDOX by the mammosphere versus CD44+CD133+ cells during the 10-day incubation with the drugs.
Uptake of fDOX and nDOX by all mammosphere cells versus CD44+CD133+ CSC subpopulationsQuantitative analysis of drug uptake by cells in mammospheres was performed using flow cytometry. Typical flow cytometry peaks and the quantitative data of the mean fl uorescence intensity of DOX in the mammosphere cells from three independent runs are shown in Fig. 4a,b, respectively. Th e mean fl uorescence intensity of DOX in mammosphere cells treated with nDOX was consistently and signifi cantly (p = 0.0056, 0.034, 0.031, and 0.047 at 37, −2.6, −8.5, and −17.4 °C, respectively) higher than that in mammosphere cells treated with fDOX either with or without cryoablation. Moreover, the uptake of nDOX by the CD44+CD133+ CSCs was consistently and signifi cantly (p = 0.0072, 0.049, 0.029, and 0.011 at 37, −2.6, −8.5, and −17.4 °C, respectively) higher than all mammosphere
cells, which may render the combined treatment of cryoablation at −17.4 °C and nDOX particularly eff ective in destroying the CSCs.
DISCUSSIONCryoablation has been explored for treating various cancers and is particularly attractive for fi ghting against breast cancer due to its excellent cosmetic outcome to preserve the organ with unnoticeable scar forma-tion on skin1,36,37. To minimize cancer recurrence post cryoablation, an ~1 cm additional safety margin of normal mammary tissue beyond the tumor boundary has been usually created in the clinic1,36,37. Our study provides the fi rst account of further minimizing cancer recurrence by destroying the cancer stem-like cells (CSCs) in the fi eld of cryoablation for cancer treatment. Our data show that cryoablation alone at −17.4 °C could greatly decrease the survival of cells in 3D mammospheres that are enriched with CSCs (from 100% to less than 30%, Fig. 1), the percentage of CD44+CD133+ CSCs among the mammosphere cells post cryoablation doesn’t change much at all. Th is is not surprising since cryoablation alone is not capable of specifi cally targeting either CSCs or non-stem cancer cells in the (microscale) tumor-like mammospheres.
Chemotherapeutic drugs have been shown to enhance cryoablation of dissociated (or single) cancer cells17,18. Doxorubicin is an anthracyclin drug that has been used widely in the clinic to treat breast cancer. In this study, we investigated the combination of free doxorubicin (fDOX) and cryoablation on destroying the mammosphere cells enriched with CSCs. Our results show that although this combination at −17.4 °C is eff ective in destroying dissociated mammosphere cells (single cell model, Sup-plementary Fig. 1), it is not signifi cantly diff erent from cryoablation alone at −17.4 °C in killing the mammosphere cells aggregated in the intact 3D mammospheres (Fig. 2). Th ese data suggest that the aggregated cells that are enriched with CSCs in the 3D tumor-like mammospheres are more re-sistant than the dissociated mammosphere cells to free anticancer drug (i.e., free doxorubicin or fDOX) even when it is combined with cryoablation.
To overcome drug resistance of cancer cells, tremendous eff ort has been made to develop eff ective drug delivery systems based on the use
Figure 3 Percentage of CSCs (judged by CD44+CD133+, two typical CSC markers) among the mammosphere cells after 10 days of incubation in culture medium containing no drug (ND), nanoparticles only (NP), free doxorubicin (fDOX, 1 µg/ml), and nanoparticle-encapsulated doxorubicin (nDOX, 1 µg/ml) either without (37 °C) or with cryoablation (at −2.6, −8.5, and −17.4 °C) between 1 and 1.5 h during the incubation. (a) Typical two-channel fl ow cytometry data showing the intensity and distribution of mammosphere cells with CD44 and CD133 staining. (b) Quantitative data of the percentage of CD44+CD133+ cell subpopulation. Cryoablation alone does not appear to preferentially destroy the CSCs at any of the three subzero temperatures studied (and even increases the CSC percentage at −8.5 °C although it is insignifi cant), the combined treatments are not significantly different from drug treatment (fDOX or nDOX) alone in reducing the percentage of the CSCs at −2.6 or −8.5 °C, the combination of cryoablation at −17.4 °C and fDOX (or NP) is not signifi cantly different from the cryoablation alone although it is signifi cantly (p = 0.021) different compared to fDOX (or NP) alone at 37 °C, and only the combination of nDOX and cryoablation at −17.4 °C can signifi cantly increase the destruction of CSCs compared to either nDOX (p = 0.00015) or the cryoablation (p = 0.00020) alone. *: p < 0.05 and **: p < 0.01.
1450002.indd 311450002.indd 31 3/24/2014 2:31:55 PM3/24/2014 2:31:55 PM
Tec
hnol
ogy
2014
.02:
28-3
5. D
ownl
oade
d fr
om w
ww
.wor
ldsc
ient
ific
.com
by U
NIV
ER
SID
AD
E D
E V
IGO
BIB
LIO
TE
CA
CE
NT
RA
L o
n 04
/22/
14. F
or p
erso
nal u
se o
nly.

32 TECHNOLOGY l VOLUME 2 • NUMBER 1 • MARCH 2014© World Scientific Publishing Co./Imperial College Press
ARTICLE
of nanoparticles made of various organic and inorganic materials with promising outcome. For example, it has been shown that doxorubicin either tethered on gold or entrapped in porous silica or polymeric na-noparticles can facilitate its intracellular delivery to multidrug resistant cancer cells under 2D monolayer culture24–26. We have shown that the drug (fDOX) resistance of CSCs (at 37 °C) can be eff ectively reduced by using Pluronic F127-chitosan nanoparticle-encapsulated doxorubicin (nDOX)23. Th e combination of nDOX and cryoablation (< 37 °C) was further investigated in this study with the combination of nanoparticles (containing no drug) and cryoablation being studied in parallel as control.
Interestingly, the combination of cryoablation at −17.4 °C and nanoparticles (with no drug) is signifi cantly more eff ective than either nanoparticles alone at 37 °C (p = 0.00015) or the cryoablation alone (p = 0.00079) in destroying all mammosphere cells and the combination is also signifi cantly more eff ective than nanoparticles alone at 37 °C (p = 0.033) in destroying the CD44+CD133+ CSC subpopulation. Th e capability of augmenting cancer cryoablation has also been reported for inorganic nanoparticles, which was attributed to the enhancement of heat transfer to achieve better freezing cells and tissue27,28. Since our nanoparticles are polymeric with low thermal conductivity, their capability of enhancing heat transfer is not anticipated. One possible explanation for the observation in this study is that freezing at −17.4 °C alone could induce temporary (or reversible) hyperpermeability of the cell plasma membrane5–8, which might become irreversible in the presence of nanoparticles because they might get stuck in the hyperpermeable membrane during the deep freezing and cell death ensues. Another possibility is that the nanoparticles could aff ect the ice nucleation and/or morphology during the deep cryoablation to induce better destruc-tion of the mammosphere cells, as with other adjuvants reported in the literature10–13. Even more interestingly, the combination of nanoparticles and cryoablation at −17.4 °C is not signifi cantly better compared to the cryoablation alone in destroying the CD44+CD133+ CSC subpopulations. Th e exact mechanism on how the polymeric nanoparticles could enhance cryoablation of the mammosphere cells but not the CD44+CD133+ CSC subpopulation is unclear and certainly warrants further investigation.
More importantly, unlike fDOX, the combination of nDOX and cryoablation at −17.4 °C is significantly more effective than either nDOX alone at 37 °C (p = 0.00015) or cryoablation alone at −17.4 °C (p = 0.0002) in destroying all mammosphere cells and the CD44+CD133+ CSC subpopulation, which is attributed at least in part to the enhanced de-livery of nDOX into the mammosphere (and particularly CD44+CD133+) cells, compared to fDOX. Th e low uptake of fDOX might be attributed at least in part to the multifaceted drug resistance of the CSCs enriched in the mammospheres (e.g., quiescence and capability of pumping out free anticancer drug)38–41. Th e high uptake of nDOX was probably a result of its special properties. Firstly, the nDOX is 21.4 ± 0.8 nm in diameter at 37 °C, which is in the range of nanoparticle size reported to be optimal for cellular uptake via endocytosis and systemic delivery33,42,43. Secondly, the nDOX is positively charged23. Th erefore, it has high electrostatic affi nity to the negatively charged cell plasma membrane, which should facilitate its uptake by mammalian cells32. Th irdly, the chitosan decorated on the nDOX surface has been shown to have high affi nity to CD44+ cells23, which may explain the much higher mean fl uorescence intensity of DOX in CD44+CD133+ cells compared to that in all mammosphere cells as shown in Fig. 4.
Th e fi ndings discussed above are schematically illustrated in Fig. 5. Th e combined treatment of nDOX and cryoablation could minimize cancer recurrence by eliminating the CSCs that are capable of creating the heterogeneity in tumor to reinitiate and further maintain tumor growth post conventional treatments19–21. It is worth noting that although the 3D mammosphere model used in this study is indeed biomimetic to in vivo tumor at the microscale and has been reported to be a highly appropriate model for studying the sensitivity of the tumorigenic stem cells in tumor to therapeutic agents and treatment modalities44, it does not completely
recapitulate the exact microenvironment in vivo. Nonetheless, cancer cells in in vivo tumor have been shown to be more susceptible to cryoabla-tion because of several in vivo injury mechanisms secondary to direct cell injury including damage due to vascular stasis and potential cryo-immunological responses7,8,45,46. Moreover, nanoparticle-encapsulated drug has been extensively reported to enhance the in vivo bioavailability of anticancer drug in tumor and minimize the drug systemic toxicity9. Th erefore, even greater effi cacy on cancer (stem) cell destruction may occur in vivo than in vitro for the combined therapy of cryoablation and nDOX, pending further substantiation with in vivo studies to monitor tumor relapse. Taken together, this study demonstrates the great potential of a novel combined therapy of cryoablation and nanodrug for improving the safety and effi cacy of breast cancer treatment by eliminating the root of cancer resistance associated with conventional chemotherapy — the CSCs.
METHODS
MaterialsDoxorubicin hydrochloride with purity > 98% was purchased from Sigma (St. Louis, MO, USA). Pluronic F127 (MW: 12.6 kD) was obtained from BASF Corp (Wyandotte, MI, USA). Chitosan oligosaccharides of pharmaceutical grade (MW: 1.2 kD, 95.5% deacetylation) were purchased from Zhejiang Golden-Shell Biochemical Co. Ltd (Zhejiang, China). Th e WST-1 cell proliferation reagent was purchased from Roche Diagnostics (Mannheim, Germany). Fetal bovine serum (FBS), penicillin, and streptomycin were purchased from Hyclone (Logan, Utah, USA). Th e EMEM and DMEM/F-12K cell culture media were purchased from ATCC
Figure 4 Uptake of free doxorubicin (fDOX, 1 µg/ml) versus nanoparticle-encapsulated doxorubicin (nDOX, 1 µg/ml) in all mammosphere cells and the CSC subpopulation (CD44+CD133+) either without cryoablation (i.e., kept at 37 °C) or with freezing to −2.6, −8.5, or −17.4 °C from 1 to 1.5 h during 10-day incubation with the anticancer drugs. (a) Typical fl ow cytometry peaks. (b) The mean fl uorescence intensity of DOX in the mammosphere and CD44+CD133+ cells from three independent runs. Uptake of nDOX by the mammosphere cells is signifi cantly (p = 0.0056, 0.034, 0.031, and 0.047 at 37, −2.6, −8.5, and −17.4 °C, respectively) higher than that of fDOX under all the conditions. Moreover, uptake of nDOX by the CSC subpopulations (CD44+CD133+) is signifi cantly (p = 0.0072, 0.049, 0.029, and 0.011 at 37, −2.6, −8.5, and −17.4 °C, respectively) higher than that by all mammosphere cells. *: p < 0.05 and **: p < 0.01.
1450002.indd 321450002.indd 32 3/24/2014 2:31:56 PM3/24/2014 2:31:56 PM
Tec
hnol
ogy
2014
.02:
28-3
5. D
ownl
oade
d fr
om w
ww
.wor
ldsc
ient
ific
.com
by U
NIV
ER
SID
AD
E D
E V
IGO
BIB
LIO
TE
CA
CE
NT
RA
L o
n 04
/22/
14. F
or p
erso
nal u
se o
nly.

33TECHNOLOGY l VOLUME 2 • NUMBER 1 • MARCH 2014© World Scientific Publishing Co./Imperial College Press
ARTICLE
(Manassas, VA, USA). All other chemicals were purchased from Sigma (St. Louis, MO, USA) unless specifi cally mentioned otherwise.
Cell and mammosphere culture MCF-7 human breast cancer cells (ATCC, Manassas, VA, USA) were cultured in EMEM supplemented with 10% fetal bovine serum (FBS), 10 μg/ml insulin, 100 U/ml penicillin, and 100 μg/ml streptomycin in T-fl asks at 37 °C in humidifi ed air with 5% CO2. Medium was changed every other day. Cells between passage 5 and 20 at 70% confl uence were detached for passaging and/or further experimental use.
To obtain mammospheres enriched with mammary cancer stem-like cells (CSCs), detached single MCF-7 cells were cultured in 6-well ultralow attachment plates (Corning, Lowell, MA) at a density of 20,000 cells/ml in 1 ml CSC medium consisting of serum-free DMEM/F12-K supplemented with 5 μg/ml insulin, 20 ng/ml epidermal growth factor (EGF), 20 ng/ml basic fi broblast growth factor (bFGF), 1× B27 (Invitrogen, Carlsbad, CA, USA), and 0.4% (w/v) bovine serum albumin (BSA). Aft er 10 days, the mammospheres were collected for further experimental use. For single cell model, mammospheres were treated using collagenase to dissociate the aggregated mammosphere cells into single cells and re-suspended in CSC medium for further treatment studies while the same number of mammospheres was used directly for the 3D mammosphere model.
Synthesis of Pluronic F127-chitosan nanoparticlesTh e Pluronic F127-chitosan nanoparticles with a core-shell structure were synthesized using a previously reported method23,33. In short, a total of 500 μl of 4-nitrophenyl chloroformate (4-NPC) activated Pluronic F127 (300 mg/ml) in dichloromethane was added dropwise into 5 ml chitosan solution (15 mg/ml) in deionized (DI) water at pH 10 under sonication using a Branson 450 digital sonifi er (Danbury, CT, USA) at 16% of maximum amplitude for 3 min. Dichloromethane was then removed by rotary evaporation. Th e resultant solution was hydrolyzed by adjusting the solution pH to 12 using sodium hydroxide and stirred for 30 min to remove any residual 4-NPC in the nanoparticles that did
not react with chitosan. Aft erward, the solution was dialyzed against DI water with a Spectra/Por dialysis tube (MWCO, 50 kDa) overnight and further dialyzed against DI water for 3 h using a 1000 kDa Spectra/Por dialysis tube. Finally, the sample was freeze-dried for 48 h to obtain dry nanoparticles.
Preparation of nanoparticle-encapsulated doxorubicin (nDOX)Th e preparation of nDOX is the same as that reported elsewhere23. In short, 0.2 mg of free doxorubicin hydrochloride (fDOX, 579.98 D) and 10 mg of Pluronic F127-chitosan nanoparticles (synthesized using a method reported elsewhere23,33 and detailed in Supporting Information) were dis-solved in 500 μl deionized (DI) water at 4 °C when the nanoparticles were swollen with high wall-permeability. Aft er 1 h, the sample was lyophilized at −50 °C for 24 h and further dried at 25 °C for 3 h to remove water from both inside and outside the nanoparticles. Th e dried sample was then put in a humidifi ed oven at 37 °C to shrink the nanoparticles and encapsulate the surrounded fDOX. Th en, the shrunken sample of both encapsulated and non-encapsulated doxorubicin was dissolved in 1 ml warm (37 °C) DI water in a 20 kDa Spectra/Por dialysis tube and dialyzed against warm DI water for 16 h to obtain clean nanoparticle-encapsulated doxorubicin (nDOX). Th e sample was then either used immediately or dried at 37 °C for future use. Th e nDOX was determined to be 21.4 ± 0.8 nm in diameter with a surface zeta potential of 21.3 ± 0.67 mV at 37 °C in aqueous solution23.
Drug (fDOX or nDOX) and cryoablation treatmentFor the combined treatment, the same number of mammosphere cells either dissociated into single cells (single cell model) or remained intact as aggregated cells in 3D mammospheres (mammosphere model) obtained using the aforementioned method for mammosphere culture, were incubated in 1 ml CSC culture medium containing 1 μg/ml of fDOX or nDOX at 37 °C for 1 h. Th e samples in the culture plates were then cooled by placing the plates on the cooling surface (precooled at −5 °C) in the chamber of a SP Scientifi c Virtis (Warminster, PA, USA) benchtop freeze-dryer for 12 min. Th e samples were then seeded with ice by locally cooling them through the outside plastic wall of culture plates using a metal wrench precooled in liquid nitrogen to mimic ice seeding by the metal cryoprobe used during cryoablation in vivo5–8,47. Th e cells were further frozen by setting the temperature of the cooling surface in the freeze-dryer at −5, −10, or −20 °C. Th e freezing time for the cooling surface temperature set at −5 °C was 15 min while it was 18 min for the cooling surface temperature set at −10 and −20 °C. Th e diff erent freezing times were used because it took ~3 min for the cooling surface temperature to change from −5 to −10 or −20 °C according to the built-in display of the cooling surface temperature in the freeze-dryer. Aft erward, the cells were allowed to passively thaw at room temperature for 10 min and then incubated at 37 °C for up to 10 days. It is worth noting that the protocol for freezing and thawing was chosen based on that used clini-cally for cryoablation of breast cancer36,37. Th e temperature during the aforementioned cryoablation procedure was recorded (Supplementary Fig. 3) and the actual end temperature was determined to be −2.6 ± 0.2, −8.5 ± 0.1, and −17.4 ± 0.1 °C for the cooling surface temperature set at −5, –10, and −20 °C, respectively. As controls, cells with no drug (ND) treatment or those incubated with empty nanoparticles (NP, 0.51 mg/ml, the same concentration of nanoparticles used for nDOX treatments) either with or without cryoablation treatment were studied in parallel.
Quantifi cation of cell viabilityThe morphological survival of cells/mammospheres in the various samples was monitored and imaged using a Zeiss Axio Observer.Z1 inverted microscope (Oberkochen, Germany). The total number of cells in each sample was quantifi ed using the WST-1 assay according to the manufacturer’s instructions by measuring the absorbance at 450 nm using a Perkin Elmer VICTORTM X4 multilabel plate reader (Waltham,
Figure 5 A schematic illustration of the resistance of cancer stem-like cells (CSCs) after cryoablation alone and its combinations with free doxorubicin (fDOX) or nanoparticle-encapsulated doxorubicin (nDOX). Cryoablation may destroy most tumor cells while the remnant CSCs will reinitiate tumor growth and tumor relapse ensues. Cryoablation combined with fDOX is not effective enough to destroy all CSCs either to prevent tumor relapse. In contrast, cryoablation combined with nDOX could effectively kill all CSCs, resulting in the eventual elimination of cancer because the non-stem cancer cells could not create the heterogeneity (e.g., cancer cells, fi broblasts, and endothelial cells) in tumor to maintain its growth.
1450002.indd 331450002.indd 33 3/24/2014 2:31:57 PM3/24/2014 2:31:57 PM
Tec
hnol
ogy
2014
.02:
28-3
5. D
ownl
oade
d fr
om w
ww
.wor
ldsc
ient
ific
.com
by U
NIV
ER
SID
AD
E D
E V
IGO
BIB
LIO
TE
CA
CE
NT
RA
L o
n 04
/22/
14. F
or p
erso
nal u
se o
nly.
34 TECHNOLOGY l VOLUME 2 • NUMBER 1 • MARCH 2014© World Scientific Publishing Co./Imperial College Press
ARTICLE
MA, USA). Quantitative cell viability was calculated as the ratio of the total cell count determined for each sample to that of the control cells with no drug treatment and kept at 37 °C.
Quantifi cation of CD44+CD133+ CSC subpopulation and drug uptake by fl ow cytometryTo quantify the percentage of CSCs in a sample, mammospheres in the sample were collected by gravity sedimentation, washed with 37 °C 1× PBS, detached using trypsin/EDTA, and further dissociated by gentle pipetting. Th e dissociated mammosphere cells were washed with 1× PBS and stained with CD44-FITC (Invitrogen, Carlsbad, CA) and CD133-APC (Miltenyi Biotec Ltd., Surrey, UK) antibodies according to the manufacturer’s instructions. Lastly, the stained samples were analyzed using a BD LSR-II Flow Cytometer together with BD FACSDiva soft ware (Franklin Lakes, NJ, USA).
To quantify cellular uptake of fDOX or nDOX, mammosphere cells with various treatment were collected aft er 10 days of incubation with the drugs, washed with 37 °C 1× PBS, detached using trypsin/EDTA, and analyzed using the BD LSR-II Flow Cytometer and BD FACSDiva/FlowJo soft ware.
Statistical analysisAll data are reported as mean ± standard error of mean from three independent runs (n = 3). Student’s two-tailed t-test assuming equal variance was performed using Microsoft ® Excel to determine the p value for assessing statistical signifi cance.
ACKNOWLEDGEMENTSTh is work was partially supported by an American Cancer Society (ACS) Research Scholar Grant (#120936-RSG-11-109-01-CDD) and the SUC-CESS program of the College of Medicine at Th e Ohio State University. We would like to thank Kaileen Zhang for her help with experiments and proofreading the manuscript.
AUTHOR CONTRIBUTIONSX.H. conceived the project; W.R., A.B., and X.H. designed experiments; W.R. and A.B. performed experiments; W.R., A.B., J.Y., X.L., and X.H. analyzed data; W.R., A.B. and X.H. wrote the manuscript; and W.R., A.B., P.J.L., J.Y., X.L., and X.H. discussed the results and reviewed the manuscript.
COMPETING INTERESTS STATEMENTTh e authors declare that they have no competing interests.
REFERENCES 1. Gage, A.A. & Baust, J.G. Cryosurgery for tumors. J. Am. Coll. Surg. 205, 342–356
(2007). 2. Callstrom, M.R. et al. Percutaneous image-guided cryoablation of painful metastases
involving bone: Multicenter trial. Cancer 119, 1033–1041 (2013). 3. Geha, A.S. & Abdelhady, K. Current status of the surgical treatment of atrial fi brillation.
World J. Surg. 32, 346–349 (2008). 4. Bischof, J.C. & He, X. Thermal stability of proteins. Ann. N. Y. Acad. Sci. 1066, 12–33
(2005). 5. Gage, A.A. & Baust, J. Mechanisms of tissue injury in cryosurgery. Cryobiology 37,
171–186 (1998). 6. He, X. & Bischof, J.C. Quantifi cation of temperature and injury response in thermal
therapy and cryosurgery. Crit. Rev. Biomed. Eng. 31, 355–422 (2003). 7. Hoffmann, N.E. & Bischof, J.C. The cryobiology of cryosurgical injury. Urology 60,
40–49 (2002). 8. He, X. Thermostability of biological systems: Fundamentals, challenges, and quanti-
fi cation. Open Biomed. Eng. J. 5, 47–73 (2011). 9. Gilstrap, K., Hu, X., Lu, X. & He, X. Nanotechnology for energy-based cancer therapies.
Am. J. Cancer Res. 1, 508–520 (2011).10. Han, B. & Bischof, J.C. Direct cell injury associated with eutectic crystallization during
freezing. Cryobiology 48, 8–21 (2004).
11. Wang, C.L.,Teo, K.Y. & Han, B. An amino acidic adjuvant to augment cryoinjury of MCF-7 breast cancer cells. Cryobiology 57, 52–59 (2008).
12. Koushafar, H. & Rubinsky, B. Effect of antifreeze proteins on frozen primary prostatic adenocarcinoma cells. Urology 49, 421–425 (1997).
13. Pham, L., Dahiya, R. & Rubinsky, B. An in vivo study of antifreeze protein adjuvant cryosurgery. Cryobiology 38, 169–175 (1999).
14. Chao, B.H., He, X. & Bischof, J.C. Pre-treatment infl ammation induced by TNF-alpha augments cryosurgical injury on human prostate cancer. Cryobiology 49, 10–27 (2004).
15. Shenoi, M.M. et al. Nanoparticle delivered vascular disrupting agents (VDAs): Use of TNF-alpha conjugated gold nanoparticles for multimodal cancer therapy. Mol. Pharm. 10, 1683–1694 (2013).
16. Forest, V. et al. Benefit of a combined treatment of cryotherapy and che-motherapy on tumour growth and late cryo-induced angiogenesis in a non-small-cell lung cancer model. Lung Cancer 54, 79–86 (2006).
17. Clarke, D.M., Baust, J.M., Van Buskirk, R.G. & Baust, J.G. Chemo-cryo combination therapy: An adjunctive model for the treatment of prostate cancer. Cryobiology 42, 274–285 (2001).
18. Mir, L.M. & Rubinsky, B. Treatment of cancer with cryochemotherapy. Br. J. Cancer 86, 1658–1660 (2002).
19. Jordan, C.T., Guzman, M.L. & Noble, M. Cancer stem cells. N. Engl. J. Med. 355, 1253–1261 (2006).
20. Frank, N.Y., Schatton, T. & Frank, M.H. The therapeutic promise of the cancer stem cell concept. J. Clin. Invest. 120, 41–50 (2010).
21. Visvader, J.E. & Lindeman, G.J. Cancer stem cells in solid tumours: Accumulating evidence and unresolved questions. Nat. Rev. Cancer 8, 755–768 (2008).
22. Al-Hajj, M. et al. Prospective identifi cation of tumorigenic breast cancer cells. Proc. Natl. Acad. Sci. USA 100, 3983–3988 (2003).
23. Rao, W. et al. Augmented destruction of cancer stem-like cells in 3D mammospheres by encapsulating doxorubicin in nanoparticles surface-decorated with chitosan. Biomaterials, in preparation (2013).
24. Wang, F. et al. Doxorubicin-tethered responsive gold nanoparticles facilitate intracel-lular drug delivery for overcoming multidrug resistance in cancer cells. ACS Nano 5, 3679–3692 (2011).
25. Gao, Y. et al. Controlled intracellular release of doxorubicin in multidrug-resistant cancer cells by tuning the shell-pore sizes of mesoporous silica nanoparticles. ACS Nano 5, 9788–9798 (2011).
26. Kabanov, A.V., Batrakova, E.V. & Alakhov, V.Y. Pluronic block copolymers for overcoming drug resistance in cancer. Adv. Drug Deliv. Rev. 54, 759–779 (2002).
27. Di, D.R., He, Z.Z., Sun, Z.Q. & Liu, J. A new nano-cryosurgical modality for tumor treatment using biodegradable MgO nanoparticles. Nanomedicine 8, 1233–1241 (2012).
28. Yan, J.F. & Liu, J. Nanocryosurgery and its mechanisms for enhancing freezing effi ciency of tumor tissues. Nanomedicine 4, 79–87 (2008).
29. Shipitsin, M. et al. Molecular defi nition of breast tumor heterogeneity. Cancer Cell 11, 259–273 (2007).
30. Lorico, A. & Rappa, G. Phenotypic heterogeneity of breast cancer stem cells. J. Oncol. 2011, 135039 (2011).
31. Wright, M.H. et al. B rca1 breast tumors contain distinct CD44+/CD24− and CD133+ cells with cancer stem cell characteristics. Breast Cancer Res. 10, R10 (2008).
32. Zhang, W. et al. Synthesis and characterization of thermally responsive Pluronic F127-chitosan nanocapsules for controlled release and intracellular delivery of small molecules. ACS Nano 4, 6747–6759 (2010).
33. Rao, W. et al. Thermally responsive nanoparticle-encapsulated curcumin and its combination with mild hyperthermia for enhanced cancer cell destruction. Acta Biomater., DOI: 10.1016/j.actbio.2013.10.020 (2013).
34. Dontu, G. et al. In vitro propagation and transcriptional profi ling of human mammary stem/progenitor cells. Genes Dev. 17, 1253–1270 (2003).
35. Shaw, F.L. et al. A detailed mammosphere assay protocol for the quantifi cation of breast stem cell activity. J. Mammary Gland Biol. Neoplasia 17, 111–117 (2012).
36. Littrup, P.J. et al. Cryotherapy for breast cancer: A feasibility study without excision. J. Vasc. Interv. Radiol. 20, 1329–1241 (2009).
37. Sabel, M.S. et al. Cryoablation of early-stage breast cancer: Work-in-progress report of a multi-institutional trial. Ann. Surg. Oncol. 11, 542–549 (2004).
38. Naumov, G.N. et al. A model of human tumor dormancy: An angiogenic switch from the nonangiogenic phenotype. J. Natl. Cancer Inst. 98, 316–325 (2006).
39. Chuthapisith, S., Eremin, J., El-Sheemey, M. & Eremin, O. Breast cancer che-moresistance: Emerging importance of cancer stem cells. Surg. Oncol. 19, 27–32 (2010).
40. Korkaya, H., Liu, S. & Wicha, M.S. Breast cancer stem cells, cytokine networks, and the tumor microenvironment. J. Clin. Invest. 121, 3804–3809 (2011).
41. Chin, A.R. & Wang, S.E. Cytokines driving breast cancer stemness. Mol. Cell. Endocrinol., in press (2013).
42. Gao, H.J., Shi, W.D. & Freund, L.B. Mechanics of receptor-mediated endocytosis. Proc. Natl. Acad. Sci. USA 102, 9469–9474 (2005).
43. Chauhan, V.P. et al. Normalization of tumour blood vessels improves the delivery of nanomedicines in a size-dependent manner. Nat. Nanotechnol. 7, 383–388 (2012).
1450002.indd 341450002.indd 34 3/24/2014 2:31:58 PM3/24/2014 2:31:58 PM
Tec
hnol
ogy
2014
.02:
28-3
5. D
ownl
oade
d fr
om w
ww
.wor
ldsc
ient
ific
.com
by U
NIV
ER
SID
AD
E D
E V
IGO
BIB
LIO
TE
CA
CE
NT
RA
L o
n 04
/22/
14. F
or p
erso
nal u
se o
nly.
35TECHNOLOGY l VOLUME 2 • NUMBER 1 • MARCH 2014© World Scientific Publishing Co./Imperial College Press
ARTICLE
44. Grimshaw, M.J. et al. Mammosphere culture of metastatic breast cancer cells enriches for tumorigenic breast cancer cells. Breast Cancer Res. 10, R52 (2008).
45. Sabel, M.S. Cryo-immunology: A review of the literature and proposed mecha-nisms for stimulatory versus suppressive immune responses. Cryobiology 58, 1–11 (2009).
46. Dong, J., Liu, P. & Xu, L.X. Immunologic response induced by synergistic effect of alternating cooling and heating of breast cancer. Int. J. Hyperthermia 25, 25–33 (2009).
47. He, X. & Bischof, J.C. Analysis of thermal stress in cryosurgery of kidneys. J. Biomech. Eng. 127, 656–661 (2005).
SUPPLEMENTARY INFORMATION
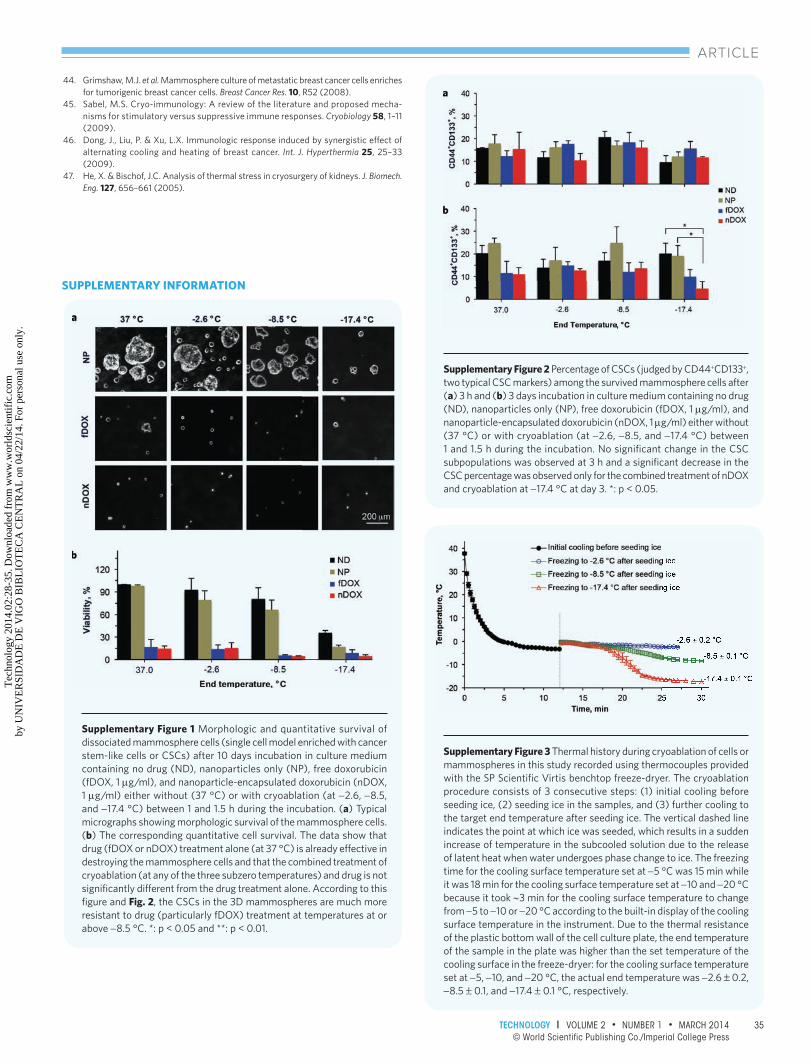
Supplementary Figure 1 Morphologic and quantitative survival of dissociated mammosphere cells (single cell model enriched with cancer stem-like cells or CSCs) after 10 days incubation in culture medium containing no drug (ND), nanoparticles only (NP), free doxorubicin (fDOX, 1 µg/ml), and nanoparticle-encapsulated doxorubicin (nDOX, 1 µg/ml) either without (37 °C) or with cryoablation (at −2.6, −8.5, and −17.4 °C) between 1 and 1.5 h during the incubation. (a) Typical micrographs showing morphologic survival of the mammosphere cells. (b) The corresponding quantitative cell survival. The data show that drug (fDOX or nDOX) treatment alone (at 37 °C) is already effective in destroying the mammosphere cells and that the combined treatment of cryoablation (at any of the three subzero temperatures) and drug is not signifi cantly different from the drug treatment alone. According to this fi gure and Fig. 2, the CSCs in the 3D mammospheres are much more resistant to drug (particularly fDOX) treatment at temperatures at or above −8.5 °C. *: p < 0.05 and **: p < 0.01.
Supplementary Figure 2 Percentage of CSCs (judged by CD44+CD133+, two typical CSC markers) among the survived mammosphere cells after (a) 3 h and (b) 3 days incubation in culture medium containing no drug (ND), nanoparticles only (NP), free doxorubicin (fDOX, 1 µg/ml), and nanoparticle-encapsulated doxorubicin (nDOX, 1 µg/ml) either without (37 °C) or with cryoablation (at −2.6, −8.5, and −17.4 °C) between 1 and 1.5 h during the incubation. No signifi cant change in the CSC subpopulations was observed at 3 h and a signifi cant decrease in the CSC percentage was observed only for the combined treatment of nDOX and cryoablation at −17.4 °C at day 3. *: p < 0.05.
Supplementary Figure 3 Thermal history during cryoablation of cells or mammospheres in this study recorded using thermocouples provided with the SP Scientifi c Virtis benchtop freeze-dryer. The cryoablation procedure consists of 3 consecutive steps: (1) initial cooling before seeding ice, (2) seeding ice in the samples, and (3) further cooling to the target end temperature after seeding ice. The vertical dashed line indicates the point at which ice was seeded, which results in a sudden increase of temperature in the subcooled solution due to the release of latent heat when water undergoes phase change to ice. The freezing time for the cooling surface temperature set at −5 °C was 15 min while it was 18 min for the cooling surface temperature set at −10 and −20 °C because it took ∼3 min for the cooling surface temperature to change from −5 to −10 or −20 °C according to the built-in display of the cooling surface temperature in the instrument. Due to the thermal resistance of the plastic bottom wall of the cell culture plate, the end temperature of the sample in the plate was higher than the set temperature of the cooling surface in the freeze-dryer: for the cooling surface temperature set at −5, −10, and −20 °C, the actual end temperature was −2.6 ± 0.2, −8.5 ± 0.1, and −17.4 ± 0.1 °C, respectively.
1450002.indd 351450002.indd 35 3/24/2014 2:31:58 PM3/24/2014 2:31:58 PM
Tec
hnol
ogy
2014
.02:
28-3
5. D
ownl
oade
d fr
om w
ww
.wor
ldsc
ient
ific
.com
by U
NIV
ER
SID
AD
E D
E V
IGO
BIB
LIO
TE
CA
CE
NT
RA
L o
n 04
/22/
14. F
or p
erso
nal u
se o
nly.