mn healthcare news sep 2015
DESCRIPTION
MN Healthcare News | Sept. 2015 | Vol. 13 No. 9 | Perspective | Mental Illness: Reaching out to youth in crisis | Sue Abderholden, MPH | NAMI Minnesota (National Alliance on Mental Illness) | 10 Questions | Diabetes | Scott Benson, MD | Apple Valley Medical Center | Insurance | Diabetes care: Managing the Costs | Matthew Wicklund | Optometry | Sports-Related concussions: Your eye doctor may see the signs | Jessica L. Schara, OD | Wound Care | Your feet and lower extremities: Common risks and complications | Nicole A. Bauerly, DPM, FACFAS, and Michael Hu, MD, FACS | MINNESOTA HEALTH CARE ROUNDTABLE | The new face of health care | Urology | Overactive bladder | Steven Siegel, MD | Chronic Conditions | Living with lupus: Managing an autoimmune disease | Jennifer Monroe, MA, MPH, and Timothy Niewold, MDTRANSCRIPT

September 2015 bull Volume 13 Number 9
Diabetes careBy Matthew Wicklund
Living with lupusBy Jennifer Monroe MA MPH
and Timothy Niewold MD
Sports-related concussions
By Jessica L Schara OD
2 Minnesota HealtH care news September 2015
Learn how to be healthy active and live well with diabetesbull Free health screeningsbull Cooking demonstrationsbull Product exhibits and presentations on diabetes prevention and managementbull Information and activities geared towards kids teens and parents
American Diabetes Association EXPO in Minneapolis
For more information call 1 888 DIABETES EXT 6652 or visit diabetesorgexpominneapolis
Minneapolis Convention Center 1301 Second Avenue S Hall E
Minneapolis MN 55403 Saturday October 10 2015
900 AM - 300 PM Visit EXPO website to print a FREE Metro Transit pass for any buslight rail to the event
SEPTEMBER 2015 Minnesota HealtH care news 3
4 News
7 PeOPLe
8 PeRsPeCTIVe
10 10 QUesTIONs
12 INsURaNCe Diabetes care By Matthew Wicklund
14 OPTOmeTRy sports-related concussions
By Jessica L Schara OD
16 wOUND CaRe your feet and lower
extremities
By Nicole A Bauerly DPM FACFAS and Michael Hu MD FACS
18 CaLeNDaR
28 UROLOgy Overactive bladder By Steven Siegel MD
30 ChRONIC CONDITIONs Living with lupus
By Jennifer Monroe MA MPH and Timothy Niewold MD
September 2015 bull Volume 13 Number 9
Sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Scott Benson MD
Apple Valley Medical Center
Minnesota Heath Care News is published once a month by Minnesota Physician Publishing Inc Our address is 2812 East 26th Street Minneapolis MN 55406 phone 6127288600 fax 6127288601 email mppmppubcom We welcome the submission of manuscripts and letters for possible publication All views and opinions expressed by authors of published articles are solely those of the authors and do not necessarily represent or express the views of Minnesota Physician Publishing Inc or this publication The contents herein are believed accurate but are not intended to replace medical legal tax business or other professional advice and counsel No part of this publication may be reprinted or reproduced without written per-mission of the publisher Annual subscriptions (12 copies) are $3600 Individual copies are $400
Publisher mike starnes | mstarnesmppubcom
editor Lisa mcgowan | lmcgowanmppubcom
AssociAte editor Richard ericson | rericsonmppubcom
Art director Joe Pfahl | joemppubcom
office AdministrAtor amanda marlow | amarlowmppubcom
Account executive stacey Bush | sbushmppubcom
20 mINNesOTa heaLTh CaRe ROUNDTaBLe The new face of health care By MPP Staff
Background and Focus Increasing evidence supports the link between access to mental health care and reducing health care costs Primary care physicians often lack the expertise to diagnose behavioral health correctly and are not always able to easily refer a patient to a mental health care provider Many initiatives nationwide are addressing this issue It is so important that the ACA stipulated the development of the Behavioral Health Home in 2015 Some states including Minnesota are also creating Behavioral Health Home programsObjectives We will review numerous initiatives that support the development of new pathways to behavioral health care We will introduce new ideas and discuss how to incorporate them into our health-care delivery system We will examine the value they can bring and the challenges they will face Our panel of industry experts will outline the steps that must be taken to increase the overall access to mental health care and the broad improvement in population health that this increased access will bring
Panelists include bull Sarah Anderson MSW LICSW CEO Psych Recovery Inc bull Lee Beecher MD President Minnesota Physician-Patient Alliance bull Timothy P Gibbs MD FAPA DFAACAP Chief Medical Officer
Natalis Counseling and Psychology Solutionsbull Martha Lantz MSW LICSW MBA Executive Dir Touchstone Mental Healthbull Judge Kerry W Meyer Hennepin County Criminal Mental Health Court bull Jane Pederson MD Medical Affairs Director Stratis Health bull Jeff Schiff MD MBA Medical Director MN Dept of Human Services bull L Read Sulik MD Chief Integration Officer PrairieCare Sponsors include bull MN Community Healthcare Network bull MN Dept of Human Services bull Natalis Outcomes bull PrairieCare bull Psych Recovery Inc bull Stratis Health
MINNESOTA HEALTH CARE ROUNDTABLE
Please mail call in or fax your registration by 1152015
Please send me tickets at $9500 per ticket Tickets may be ordered by phone at (612) 728-8600 by fax at (612) 728-8601 on our website (mppubcom) or by mail Make checks payable to Minnesota Physician Publishing Mail orders to MPP 2812 East 26th Street Mpls MN 55406 Please note tickets are non-refundable
Name
Company
Address
City State ZIP
TelephoneFAX
Card Exp Date Check enclosed Bill me Credit card (Visa Mastercard American Express or Discover)
Signature
Thursday November 12 2015 bull 100-400 PMDowntown Minneapolis Hilton and Towers
FORTy-FOURTH SESSION
Behavioral Health IntegrationNew pathways to care
4 Minnesota HealtH care news September 2015
N e ws
Drug Companies Delay Reporting Serious Patient Harm to FDADrug manufacturers delay reporting adverse events to the Us Food and Drug administration (FDa) quite often according to a new study from the University of Minnesotarsquos school of Public Health
researchers analyzed 16 million reports submitted through the FDarsquos adverse event reporting system between 2000 and 2014
95 percent of which come from drug manufacturers For each adverse event they calculated the number of days between when doctors alerted the drug companies to when documents were submitted through the reporting system Fed-eral regulation requires that when drug manufacturers receive reports for serious and unexpected adverse events they must report them to the FDa within 15 calendar days
the results show that drug com-panies did not follow this regula-tion for about 10 percent of serious
adverse event cases More than 160000 events were not disclosed to the FDa within the 15-day time frame and more than 40000 of those reports involved patient deaths
ldquoour findings are even more concerning because they are likely an underestimate of the overall underreporting or misreporting of serious or adverse eventsrdquo said Pinar Karaca-Mandic PhD associ-ate professor of health policy at the University of Minnesotarsquos school of Public Health and coauthor of the study ldquoour study analysis is limit-ed to the events that are reported to the FDa and there could be cases in which drug manufacturers fail to report serious or unexpected events at all by downward classifying serious reports as non-seriousrdquo
researchers also found that the delays were longer on average for the cases that involved deaths ldquoa larger fraction of these serious and unexpected events that involved a patient death were delayedmdashabout 12 percent of events with patient death compared to 9 percent of events without patient deathrdquo said Karaca-Mandic
some of the cases were even reported months late ldquowhat was also surprising was that typically these were not delays of just a few daysrdquo said Karaca-Mandic ldquoFor example among events that involved a patient death about 6 percent were reported within 16 to 90 days about 3 percent within 91 to 180 days and about 3 percent were delayed more than 180 daysrdquo
in defense of the findings a spokesperson for the Pharmaceuti-cal research and Manufacturers of america (PhrMa) which rep-resents biopharmaceutical research-ers and biotechnology companies said ldquoit is important to remember that prior to reporting any adverse event including serious unexpected adverse events companies must investigate the reports that they receive from patients and health care professionals companies typ-ically verify the accuracy of patient and physician reports and often contact adverse event reporters to supplement the information that they provide to the FDardquo
the analysis was published online July 27 in the journal JaMa
internal Medicine as part of the report researchers proposed that the FDa create a regulation allowing patients to report side effects directly
ldquoour study suggests that direct submission of reports to the FDa in lieu of submitting to an intermedi-ary such as the drug manufacturer may help reduce reporting delaysrdquo said Paul Ma PhD assistant profes-sor of accounting in carlson school of Management at the University of Minnesota and coauthor of the study ldquowhile it is possible that drug manufacturers spend addi-tional time in verifying reports with more serious patient outcomes the delays are not just by a few days but can be several months or years Future research is needed to help understand the mechanisms behind the drug manufacturerrsquos decision to delay which could help policymak-ers such as the FDa in determining the optimal reporting rulerdquo
Dayton Names Members to New Health Care Program Task Force Gov Mark Dayton has announced his appointments to the 11-member state task force that will evaluate the future of state health care programs including Mnsure and Minnesotacare
the task Force on Health care Financing will look at Mnsurersquos longterm financial viability the possibility of moving to the federal health care exchange and changes to other public health care programs
ldquothe launch of Mnsure created serious problems for many consumers although we have seen significant improvements there are still important unresolved issuesrdquo Dayton wrote ldquolooking ahead we must make some major policy and programmatic decisions that will strengthen Minnesotarsquos position as the nationrsquos health care leader while making the best use of our statersquos financial resourcesrdquo
the 33-member task force will report to Dayton and the legisla-ture by Jan 15 2016
North Memorial to Open Clinic on Nicollet Mall north Memorial Health care has announced plans for an 8000- square-foot clinic on nicollet Mall in the second-floor space former-ly occupied by the saks off 5th department store this will be the health care systemrsquos 16th location in the metro area
the primary care clinic will offer walk-in appointments advanced imaging mammography podiatry occupational medicine and lab services it will have direct access to Gaviidae common and the iDs center
ldquowith this new location we are bringing the north Memorial care that this community has come to trust and value close to where they live and workrdquo says Kelly Mack-en-Marble president of population health and ambulatory services at north Memorial Health care
United Properties and its joint venture capital partner capital real estate inc purchased the first few floors of the nicollet Mall site in December 2014 north Memorial signed a lease for the second-floor space in May and the clinic will open in november
Report Shows Effect of Air Pollution on Public Healthair pollution in the twin cities metro area contributed to an estimated 2000 deaths 400 hospitalizations and 600 visits to the emergency room in 2008 according to a new report from the Minnesota Department of Health (MDH) and Minnesota Pollution control agency (MPca)
the report called ldquolife and breath How air pollution affects public health in the twin citiesrdquo analyzed air quality data from MPca and public health data from MDH the agencies used mathematical modeling software to estimate the effects of air pollution
on public health for residents of the seven-county metro area in 2008 they found that fine particles or ground-level ozone the two most directly harmful air pollutants made conditions worse for an esti-mated 6 to 13 percent of residents in the area who died and 2 to 5 percent of residents who visited the hospital or emergency room for heart or lung issues
ldquothis report helps us see much more clearly than we could before just who is affected by air pollution how serious the effects are and where we have health disparities that need to be addressedrdquo said ed ehlinger MD Minnesota commissioner of health ldquothis report gives us a baseline by which we can measure the health impacts of future reductions in air pollutionrdquo
researchers analyzed data by ZiP codes and while there were no significant differences in air pollution levels between them the agencies did find that people residing in ZiP codes that had a higher percentage of people of color and residents in poverty had more health effects from the air pollution this is partially due to these areas having higher rates of preexisting heart and lung condi-tions in addition ldquoPlaces that have more elderly people with heart and lung conditions and children with uncontrollable asthma are places where air pollution has a greater impactrdquo according to ehlinger
ldquowe canrsquot control canadian wild fires or who is burning coal around the worldrdquo said John linc stine MPca commissioner ldquowe can look at our own choices every day we can choose the most fuel-efficient transportation we can afford or use mass transit small steps really do add up air pollution is a day-in-day-out cumulative problem we can all make a positive impact with the daily choices we makerdquo
according to ehlinger and stine data from 2014 indicate that air quality has improved since 2008 However it is not yet known whether health outcomes improved as well
September 2015 Minnesota HealtH care news 5
News to page 6
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
HealthPartners to Study Improvements in Prediabetes CareHealthPartners institute for edu-cation and research has launched a five-year study to determine if web-based clinical decision support can help in the identification and treatment of patients with prediabe-tes to help reduce their chances of developing type 2 diabetes
ldquoclinical decision support in electronic medical records has improved care for diabetes and appropriate high-tech imaging and we hope to see if it can improve care for people at risk of developing diabetesrdquo said Jay Desai PhD MPH research fellow at Health-Partners institute for education and research and principal investigator of the study
researchers will study about 17000 patient participants with
prediabetes who receive care at 30 essentia Health clinics in northern Minnesota northwest wisconsin and eastern north Dakota they will implement a clinical decision support system to identify people with prediabetes give personalized care recommendations and evalu-ate the effectiveness of the system
ldquothis study aims to impact our patientsrsquo lives by reducing their cardiovascular risk and improving their quality of liferdquo said Daniel saman DrPH MPH cPH associ-ate research scientist at the essentia institute of rural Health
almost one-third of adults in the Us have prediabetes according to the Us centers for Disease control and Prevention and without intervention care 15 to 30 percent of them will develop type 2 diabetes within five years Patients with diabetes have health care costs that are 23 times higher than people who do not have diabetes according to the american Diabetes association
Hysterectomy Linked to Risks for Women Under Age 50researchers at Mayo clinic have shown that hysterectomy may be a marker of early cardiovascular risk and disease most notably for women less than 35 years of age
through the rochester epide-miology Project the researchers analyzed 3816 available records of women who had a hysterectomy with ovarian conservation in olmsted county between 1965 and 2002 they then determined a randomly selected control group of another 3816 women of the same age who had not undergone a hysterectomy and compared cardio-vascular risk factors and diseases for the women they discovered that the women who had a hyster-ectomy had slightly higher odds of having hyperlipidemia obesity and metabolic syndrome
ldquocardiovascular disease is the leading cause of death among women and women see primarily gynecologists between 18 years and 64 yearsmdasha time when early screening for cardiovascular disease would be importantrdquo said shannon laughlin-tommaso MD obstetri-ciangynecologist at Mayo clinic and lead author of the study ldquowe wanted to do this study to find a gynecologic screening method for cardiovascular diseaserdquo
in addition stroke was signifi-cantly more common among wom-en who had a hysterectomy before the age of 35 compared to women of the same age who did not have a hysterectomy women ages 35 to 40 that had a hysterectomy were more likely to have hypertension and women who had a hysterectomy at the age of 50 or older didnrsquot demon-strate any notable increases in risk factors and contrastingly were less likely to have had a stroke or congestive heart failure compared with women of the same age that did not have a hysterectomy
6 Minnesota HealtH care news September 2015
News from page 5
Zhi Halbach DO has joined Hutchinson Health as a family physician Halbach earned her doctor-ate in osteopathic medicine from the Des Moines University College of Osteopathic Medicine She is originally from Chaska and has moved back to Minnesota after completing her residency at St Lukersquos University Hospital in Pennsylvania Hal-bechrsquos special interests include womenrsquos health
preventive care and office procedures In addition Tiffany Trenda DO has joined Hutchinson Health as a pediatri-cian Trenda earned her doctorate in osteopathic medicine from Lake Erie College of Osteopathic Medicine in Pennsylvania and is moving back to her home state of Minnesota after completing her pediatric residency through Palmetto HealthUni-versity of South Carolina Trenda has spent time as a volunteer pediatrician in medically underserved communities in Nicaragua and El Salvador
Kevin Lindgren MD and Jaclyn Bailey MD have joined St Croix Orthopaedics as orthopedic surgeons Lindgren earned his medical degree from the Medical College of Wisconsin and completed an orthopaedic surgery residency at the University of Nebraska Medical CenterCreighton University where he received the Frank P Stone MD award for Outstanding Resident Lindgren completed his fellowship training at the University of Utah where
he specialized in hip and knee reconstruction and hip preservation surgery Bailey earned her doctor of medicine degree at the Univer-sity of Minnesota Medical School and completed an orthopaedic surgery residency at Grand Rapids Medical Education PartnersMichigan State University She completed her fellowship training in hand and upper extremity surgery at the University of California in San Francisco Lindgren will begin seeing patients at the Maplewood and Woodbury clinics in early September and at the new St Paul clinic when it opens later this fall Bailey will begin seeing patients at the Maplewood and Wyoming clinics at the end of September as well as at the new St Paul clinic
Samith Kochuparambil MD has joined Minne sota Oncology with the practice of medical oncology and hematology at the Minneapolis clinic Ko chu pa rambil earned his medical degree from the Madras Medical College Chennai India He completed a residency in internal medicine at the Medical College of Georgia where he received a STAR resident award and completed his fellowship in medical oncology and hematology at Mayo Clinic Kochuparambil specializes in treating pros-tate cancer kidney cancer bladder cancer multiple myeloma and general oncology
Peo Ple
September 2015 MINNESOTA HEALTH CARE NEWS 7
Kevin Lindgren MD
Samith Kochuparambil
MD
Zhi Halbach DO
Tiffany Trenda DO
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Young people experiencing their first psychotic episode wait an average of 72 weeks to seek treatment Other studies report that people
wait an average of 10 years before treatment
Half of all people living with a serious mental illness began experiencing symptoms before the age of 14 Three-quarters will develop a mental illness by age 24 So it is a ldquoyoung personrsquosrdquo illness during a prime time in their lives
For any health care condition early identifica-tion and treatment are critical The more we wait to treat a mental illness the more likely it is to become severe and for the individual to develop a substance use disorder as well So why is this happening
Building awarenessOne reason is that many people including youth are not aware of the symptoms of mental illness Teachers donrsquot receive much initial educa-tion about mental illnesses Limited access to treatment transportation insurance coverage and parent work schedules cause many to go without treatment
Minnesota schools do not require mental health education although there are mental health compo-nents in the National Health Education Standards However there are recommended free and low-cost programs available to schools including NAMI Minnesotarsquos free Ending the Silence program
Ending the Silence fits into 50-minute high school or middle school class periods and covers how common mental illnesses are signs and symptoms and the personal story of a young adult doing well in recovery Students receive resources to get help for themselves or a friend and information on how to fight the stigma of mental illnesses NAMI Minne-sota also developed a website for youth
In 2003 Minnesota became the first state to require continuing education for teachers on the key warning signs of early-onset mental illnesses in chil-dren and adolescents In 2013 trauma and autism were added These trainings help teachers under-stand the difference between willful behavior and symptomsmdashnot to have teachers diagnose students but to know when to talk to parents about a referral
In 2007 the Legislature funded school-linked mental health grants Grants are provided to mental health providers who then co-locate in the schools eliminating the barriers to treatment Funds pay for activities not funded by insurance such as collabo-ration with school support staff and teachers and for treatment of children who are uninsured and
underinsured Data from the first four years show that nearly half of the children had never received treatment and half of those had a serious mental illness While funding was doubled in 2013 only roughly 50 percent of schools have such a program
Reducing stigmaAnother issue is that parents and other adults work-ing with youth are not aware of the symptoms and frankly have stigmatizing attitudes Some believe that mental illnesses cannot occur in children and others believe that itrsquos just a ldquophaserdquo
We use slang words such as ldquocrazyrdquo and ldquonutsrdquo for people with mental illnesses but we donrsquot have slang words for other illnesses We never think to use the words ldquocourageousrdquo or ldquodeterminedrdquo to de-
scribe someone with schizo-phrenia or depression These are no ldquohot-dishrdquo or get-well card illnesses By harboring negative views we make it more difficult for people to seek treatment
Several strategies help to address this Mental Health First Aid an eight-hour class geared toward
youth or older adults increases mental health litera-cy It teaches people about the symptoms of mental illnesses and how to help when a person is in crisis or is suicidal The nation-wide class educates people about the signs and symptoms of mental illnesses
Another strategy is the Make It Ok campaign a one-hour presentation on how we talk and think about how mental illnesses impact peoplersquos lives Online videos of people with mental illnesses and their families present the impact of mental illnesses as well as personal stories of recovery The goal is to ldquomake it okrdquo to talk about mental illnesses
First Episode programs strive to identify psy-chosis early provide intensive treatment and help young people return to school or work so that they do not become disabled by their illness Early signs can include changing sleep patterns beginning to feel paranoid or having odd thought patterns hav-ing a hard time paying attention avoiding bathing and grooming and cognitive decline Efforts are underway to identify young people at closer to four weeks instead of 72 weeks But parents need to be watchful and not pass it off as a phase Funding was provided by the Legislature in 2015 For details visit the NAMI Minnesota website wwwnamihelpsorg
Progress and hopeWe are making progress that will lead to earlier identification and treatment but our work is not yet done Itrsquos important for everyone to learn about signs symptoms and what actions to take
Mental IllnessReaching out to youth in crisis
Pe RsPec t ive
Half of all people living with a serious mental illness began
experiencing symptoms before the age of 14
8 Minnesota HealtH care news September 2015
sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Ms Abderholden is the executive director of NAMI Minnesota (National Alliance on Mental Illness) a nonprofit organization that works to improve the lives of children and adults with mental illnesses and their families through its programs of education support and advocacy NAMI Minnesota offers more than 500 free classes and presentations and over 60 support groups each year
Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
September 2015 Minnesota HealtH care news 9
10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
2 Minnesota HealtH care news September 2015
Learn how to be healthy active and live well with diabetesbull Free health screeningsbull Cooking demonstrationsbull Product exhibits and presentations on diabetes prevention and managementbull Information and activities geared towards kids teens and parents
American Diabetes Association EXPO in Minneapolis
For more information call 1 888 DIABETES EXT 6652 or visit diabetesorgexpominneapolis
Minneapolis Convention Center 1301 Second Avenue S Hall E
Minneapolis MN 55403 Saturday October 10 2015
900 AM - 300 PM Visit EXPO website to print a FREE Metro Transit pass for any buslight rail to the event
SEPTEMBER 2015 Minnesota HealtH care news 3
4 News
7 PeOPLe
8 PeRsPeCTIVe
10 10 QUesTIONs
12 INsURaNCe Diabetes care By Matthew Wicklund
14 OPTOmeTRy sports-related concussions
By Jessica L Schara OD
16 wOUND CaRe your feet and lower
extremities
By Nicole A Bauerly DPM FACFAS and Michael Hu MD FACS
18 CaLeNDaR
28 UROLOgy Overactive bladder By Steven Siegel MD
30 ChRONIC CONDITIONs Living with lupus
By Jennifer Monroe MA MPH and Timothy Niewold MD
September 2015 bull Volume 13 Number 9
Sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Scott Benson MD
Apple Valley Medical Center
Minnesota Heath Care News is published once a month by Minnesota Physician Publishing Inc Our address is 2812 East 26th Street Minneapolis MN 55406 phone 6127288600 fax 6127288601 email mppmppubcom We welcome the submission of manuscripts and letters for possible publication All views and opinions expressed by authors of published articles are solely those of the authors and do not necessarily represent or express the views of Minnesota Physician Publishing Inc or this publication The contents herein are believed accurate but are not intended to replace medical legal tax business or other professional advice and counsel No part of this publication may be reprinted or reproduced without written per-mission of the publisher Annual subscriptions (12 copies) are $3600 Individual copies are $400
Publisher mike starnes | mstarnesmppubcom
editor Lisa mcgowan | lmcgowanmppubcom
AssociAte editor Richard ericson | rericsonmppubcom
Art director Joe Pfahl | joemppubcom
office AdministrAtor amanda marlow | amarlowmppubcom
Account executive stacey Bush | sbushmppubcom
20 mINNesOTa heaLTh CaRe ROUNDTaBLe The new face of health care By MPP Staff
Background and Focus Increasing evidence supports the link between access to mental health care and reducing health care costs Primary care physicians often lack the expertise to diagnose behavioral health correctly and are not always able to easily refer a patient to a mental health care provider Many initiatives nationwide are addressing this issue It is so important that the ACA stipulated the development of the Behavioral Health Home in 2015 Some states including Minnesota are also creating Behavioral Health Home programsObjectives We will review numerous initiatives that support the development of new pathways to behavioral health care We will introduce new ideas and discuss how to incorporate them into our health-care delivery system We will examine the value they can bring and the challenges they will face Our panel of industry experts will outline the steps that must be taken to increase the overall access to mental health care and the broad improvement in population health that this increased access will bring
Panelists include bull Sarah Anderson MSW LICSW CEO Psych Recovery Inc bull Lee Beecher MD President Minnesota Physician-Patient Alliance bull Timothy P Gibbs MD FAPA DFAACAP Chief Medical Officer
Natalis Counseling and Psychology Solutionsbull Martha Lantz MSW LICSW MBA Executive Dir Touchstone Mental Healthbull Judge Kerry W Meyer Hennepin County Criminal Mental Health Court bull Jane Pederson MD Medical Affairs Director Stratis Health bull Jeff Schiff MD MBA Medical Director MN Dept of Human Services bull L Read Sulik MD Chief Integration Officer PrairieCare Sponsors include bull MN Community Healthcare Network bull MN Dept of Human Services bull Natalis Outcomes bull PrairieCare bull Psych Recovery Inc bull Stratis Health
MINNESOTA HEALTH CARE ROUNDTABLE
Please mail call in or fax your registration by 1152015
Please send me tickets at $9500 per ticket Tickets may be ordered by phone at (612) 728-8600 by fax at (612) 728-8601 on our website (mppubcom) or by mail Make checks payable to Minnesota Physician Publishing Mail orders to MPP 2812 East 26th Street Mpls MN 55406 Please note tickets are non-refundable
Name
Company
Address
City State ZIP
TelephoneFAX
Card Exp Date Check enclosed Bill me Credit card (Visa Mastercard American Express or Discover)
Signature
Thursday November 12 2015 bull 100-400 PMDowntown Minneapolis Hilton and Towers
FORTy-FOURTH SESSION
Behavioral Health IntegrationNew pathways to care
4 Minnesota HealtH care news September 2015
N e ws
Drug Companies Delay Reporting Serious Patient Harm to FDADrug manufacturers delay reporting adverse events to the Us Food and Drug administration (FDa) quite often according to a new study from the University of Minnesotarsquos school of Public Health
researchers analyzed 16 million reports submitted through the FDarsquos adverse event reporting system between 2000 and 2014
95 percent of which come from drug manufacturers For each adverse event they calculated the number of days between when doctors alerted the drug companies to when documents were submitted through the reporting system Fed-eral regulation requires that when drug manufacturers receive reports for serious and unexpected adverse events they must report them to the FDa within 15 calendar days
the results show that drug com-panies did not follow this regula-tion for about 10 percent of serious
adverse event cases More than 160000 events were not disclosed to the FDa within the 15-day time frame and more than 40000 of those reports involved patient deaths
ldquoour findings are even more concerning because they are likely an underestimate of the overall underreporting or misreporting of serious or adverse eventsrdquo said Pinar Karaca-Mandic PhD associ-ate professor of health policy at the University of Minnesotarsquos school of Public Health and coauthor of the study ldquoour study analysis is limit-ed to the events that are reported to the FDa and there could be cases in which drug manufacturers fail to report serious or unexpected events at all by downward classifying serious reports as non-seriousrdquo
researchers also found that the delays were longer on average for the cases that involved deaths ldquoa larger fraction of these serious and unexpected events that involved a patient death were delayedmdashabout 12 percent of events with patient death compared to 9 percent of events without patient deathrdquo said Karaca-Mandic
some of the cases were even reported months late ldquowhat was also surprising was that typically these were not delays of just a few daysrdquo said Karaca-Mandic ldquoFor example among events that involved a patient death about 6 percent were reported within 16 to 90 days about 3 percent within 91 to 180 days and about 3 percent were delayed more than 180 daysrdquo
in defense of the findings a spokesperson for the Pharmaceuti-cal research and Manufacturers of america (PhrMa) which rep-resents biopharmaceutical research-ers and biotechnology companies said ldquoit is important to remember that prior to reporting any adverse event including serious unexpected adverse events companies must investigate the reports that they receive from patients and health care professionals companies typ-ically verify the accuracy of patient and physician reports and often contact adverse event reporters to supplement the information that they provide to the FDardquo
the analysis was published online July 27 in the journal JaMa
internal Medicine as part of the report researchers proposed that the FDa create a regulation allowing patients to report side effects directly
ldquoour study suggests that direct submission of reports to the FDa in lieu of submitting to an intermedi-ary such as the drug manufacturer may help reduce reporting delaysrdquo said Paul Ma PhD assistant profes-sor of accounting in carlson school of Management at the University of Minnesota and coauthor of the study ldquowhile it is possible that drug manufacturers spend addi-tional time in verifying reports with more serious patient outcomes the delays are not just by a few days but can be several months or years Future research is needed to help understand the mechanisms behind the drug manufacturerrsquos decision to delay which could help policymak-ers such as the FDa in determining the optimal reporting rulerdquo
Dayton Names Members to New Health Care Program Task Force Gov Mark Dayton has announced his appointments to the 11-member state task force that will evaluate the future of state health care programs including Mnsure and Minnesotacare
the task Force on Health care Financing will look at Mnsurersquos longterm financial viability the possibility of moving to the federal health care exchange and changes to other public health care programs
ldquothe launch of Mnsure created serious problems for many consumers although we have seen significant improvements there are still important unresolved issuesrdquo Dayton wrote ldquolooking ahead we must make some major policy and programmatic decisions that will strengthen Minnesotarsquos position as the nationrsquos health care leader while making the best use of our statersquos financial resourcesrdquo
the 33-member task force will report to Dayton and the legisla-ture by Jan 15 2016
North Memorial to Open Clinic on Nicollet Mall north Memorial Health care has announced plans for an 8000- square-foot clinic on nicollet Mall in the second-floor space former-ly occupied by the saks off 5th department store this will be the health care systemrsquos 16th location in the metro area
the primary care clinic will offer walk-in appointments advanced imaging mammography podiatry occupational medicine and lab services it will have direct access to Gaviidae common and the iDs center
ldquowith this new location we are bringing the north Memorial care that this community has come to trust and value close to where they live and workrdquo says Kelly Mack-en-Marble president of population health and ambulatory services at north Memorial Health care
United Properties and its joint venture capital partner capital real estate inc purchased the first few floors of the nicollet Mall site in December 2014 north Memorial signed a lease for the second-floor space in May and the clinic will open in november
Report Shows Effect of Air Pollution on Public Healthair pollution in the twin cities metro area contributed to an estimated 2000 deaths 400 hospitalizations and 600 visits to the emergency room in 2008 according to a new report from the Minnesota Department of Health (MDH) and Minnesota Pollution control agency (MPca)
the report called ldquolife and breath How air pollution affects public health in the twin citiesrdquo analyzed air quality data from MPca and public health data from MDH the agencies used mathematical modeling software to estimate the effects of air pollution
on public health for residents of the seven-county metro area in 2008 they found that fine particles or ground-level ozone the two most directly harmful air pollutants made conditions worse for an esti-mated 6 to 13 percent of residents in the area who died and 2 to 5 percent of residents who visited the hospital or emergency room for heart or lung issues
ldquothis report helps us see much more clearly than we could before just who is affected by air pollution how serious the effects are and where we have health disparities that need to be addressedrdquo said ed ehlinger MD Minnesota commissioner of health ldquothis report gives us a baseline by which we can measure the health impacts of future reductions in air pollutionrdquo
researchers analyzed data by ZiP codes and while there were no significant differences in air pollution levels between them the agencies did find that people residing in ZiP codes that had a higher percentage of people of color and residents in poverty had more health effects from the air pollution this is partially due to these areas having higher rates of preexisting heart and lung condi-tions in addition ldquoPlaces that have more elderly people with heart and lung conditions and children with uncontrollable asthma are places where air pollution has a greater impactrdquo according to ehlinger
ldquowe canrsquot control canadian wild fires or who is burning coal around the worldrdquo said John linc stine MPca commissioner ldquowe can look at our own choices every day we can choose the most fuel-efficient transportation we can afford or use mass transit small steps really do add up air pollution is a day-in-day-out cumulative problem we can all make a positive impact with the daily choices we makerdquo
according to ehlinger and stine data from 2014 indicate that air quality has improved since 2008 However it is not yet known whether health outcomes improved as well
September 2015 Minnesota HealtH care news 5
News to page 6
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
HealthPartners to Study Improvements in Prediabetes CareHealthPartners institute for edu-cation and research has launched a five-year study to determine if web-based clinical decision support can help in the identification and treatment of patients with prediabe-tes to help reduce their chances of developing type 2 diabetes
ldquoclinical decision support in electronic medical records has improved care for diabetes and appropriate high-tech imaging and we hope to see if it can improve care for people at risk of developing diabetesrdquo said Jay Desai PhD MPH research fellow at Health-Partners institute for education and research and principal investigator of the study
researchers will study about 17000 patient participants with
prediabetes who receive care at 30 essentia Health clinics in northern Minnesota northwest wisconsin and eastern north Dakota they will implement a clinical decision support system to identify people with prediabetes give personalized care recommendations and evalu-ate the effectiveness of the system
ldquothis study aims to impact our patientsrsquo lives by reducing their cardiovascular risk and improving their quality of liferdquo said Daniel saman DrPH MPH cPH associ-ate research scientist at the essentia institute of rural Health
almost one-third of adults in the Us have prediabetes according to the Us centers for Disease control and Prevention and without intervention care 15 to 30 percent of them will develop type 2 diabetes within five years Patients with diabetes have health care costs that are 23 times higher than people who do not have diabetes according to the american Diabetes association
Hysterectomy Linked to Risks for Women Under Age 50researchers at Mayo clinic have shown that hysterectomy may be a marker of early cardiovascular risk and disease most notably for women less than 35 years of age
through the rochester epide-miology Project the researchers analyzed 3816 available records of women who had a hysterectomy with ovarian conservation in olmsted county between 1965 and 2002 they then determined a randomly selected control group of another 3816 women of the same age who had not undergone a hysterectomy and compared cardio-vascular risk factors and diseases for the women they discovered that the women who had a hyster-ectomy had slightly higher odds of having hyperlipidemia obesity and metabolic syndrome
ldquocardiovascular disease is the leading cause of death among women and women see primarily gynecologists between 18 years and 64 yearsmdasha time when early screening for cardiovascular disease would be importantrdquo said shannon laughlin-tommaso MD obstetri-ciangynecologist at Mayo clinic and lead author of the study ldquowe wanted to do this study to find a gynecologic screening method for cardiovascular diseaserdquo
in addition stroke was signifi-cantly more common among wom-en who had a hysterectomy before the age of 35 compared to women of the same age who did not have a hysterectomy women ages 35 to 40 that had a hysterectomy were more likely to have hypertension and women who had a hysterectomy at the age of 50 or older didnrsquot demon-strate any notable increases in risk factors and contrastingly were less likely to have had a stroke or congestive heart failure compared with women of the same age that did not have a hysterectomy
6 Minnesota HealtH care news September 2015
News from page 5
Zhi Halbach DO has joined Hutchinson Health as a family physician Halbach earned her doctor-ate in osteopathic medicine from the Des Moines University College of Osteopathic Medicine She is originally from Chaska and has moved back to Minnesota after completing her residency at St Lukersquos University Hospital in Pennsylvania Hal-bechrsquos special interests include womenrsquos health
preventive care and office procedures In addition Tiffany Trenda DO has joined Hutchinson Health as a pediatri-cian Trenda earned her doctorate in osteopathic medicine from Lake Erie College of Osteopathic Medicine in Pennsylvania and is moving back to her home state of Minnesota after completing her pediatric residency through Palmetto HealthUni-versity of South Carolina Trenda has spent time as a volunteer pediatrician in medically underserved communities in Nicaragua and El Salvador
Kevin Lindgren MD and Jaclyn Bailey MD have joined St Croix Orthopaedics as orthopedic surgeons Lindgren earned his medical degree from the Medical College of Wisconsin and completed an orthopaedic surgery residency at the University of Nebraska Medical CenterCreighton University where he received the Frank P Stone MD award for Outstanding Resident Lindgren completed his fellowship training at the University of Utah where
he specialized in hip and knee reconstruction and hip preservation surgery Bailey earned her doctor of medicine degree at the Univer-sity of Minnesota Medical School and completed an orthopaedic surgery residency at Grand Rapids Medical Education PartnersMichigan State University She completed her fellowship training in hand and upper extremity surgery at the University of California in San Francisco Lindgren will begin seeing patients at the Maplewood and Woodbury clinics in early September and at the new St Paul clinic when it opens later this fall Bailey will begin seeing patients at the Maplewood and Wyoming clinics at the end of September as well as at the new St Paul clinic
Samith Kochuparambil MD has joined Minne sota Oncology with the practice of medical oncology and hematology at the Minneapolis clinic Ko chu pa rambil earned his medical degree from the Madras Medical College Chennai India He completed a residency in internal medicine at the Medical College of Georgia where he received a STAR resident award and completed his fellowship in medical oncology and hematology at Mayo Clinic Kochuparambil specializes in treating pros-tate cancer kidney cancer bladder cancer multiple myeloma and general oncology
Peo Ple
September 2015 MINNESOTA HEALTH CARE NEWS 7
Kevin Lindgren MD
Samith Kochuparambil
MD
Zhi Halbach DO
Tiffany Trenda DO
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Young people experiencing their first psychotic episode wait an average of 72 weeks to seek treatment Other studies report that people
wait an average of 10 years before treatment
Half of all people living with a serious mental illness began experiencing symptoms before the age of 14 Three-quarters will develop a mental illness by age 24 So it is a ldquoyoung personrsquosrdquo illness during a prime time in their lives
For any health care condition early identifica-tion and treatment are critical The more we wait to treat a mental illness the more likely it is to become severe and for the individual to develop a substance use disorder as well So why is this happening
Building awarenessOne reason is that many people including youth are not aware of the symptoms of mental illness Teachers donrsquot receive much initial educa-tion about mental illnesses Limited access to treatment transportation insurance coverage and parent work schedules cause many to go without treatment
Minnesota schools do not require mental health education although there are mental health compo-nents in the National Health Education Standards However there are recommended free and low-cost programs available to schools including NAMI Minnesotarsquos free Ending the Silence program
Ending the Silence fits into 50-minute high school or middle school class periods and covers how common mental illnesses are signs and symptoms and the personal story of a young adult doing well in recovery Students receive resources to get help for themselves or a friend and information on how to fight the stigma of mental illnesses NAMI Minne-sota also developed a website for youth
In 2003 Minnesota became the first state to require continuing education for teachers on the key warning signs of early-onset mental illnesses in chil-dren and adolescents In 2013 trauma and autism were added These trainings help teachers under-stand the difference between willful behavior and symptomsmdashnot to have teachers diagnose students but to know when to talk to parents about a referral
In 2007 the Legislature funded school-linked mental health grants Grants are provided to mental health providers who then co-locate in the schools eliminating the barriers to treatment Funds pay for activities not funded by insurance such as collabo-ration with school support staff and teachers and for treatment of children who are uninsured and
underinsured Data from the first four years show that nearly half of the children had never received treatment and half of those had a serious mental illness While funding was doubled in 2013 only roughly 50 percent of schools have such a program
Reducing stigmaAnother issue is that parents and other adults work-ing with youth are not aware of the symptoms and frankly have stigmatizing attitudes Some believe that mental illnesses cannot occur in children and others believe that itrsquos just a ldquophaserdquo
We use slang words such as ldquocrazyrdquo and ldquonutsrdquo for people with mental illnesses but we donrsquot have slang words for other illnesses We never think to use the words ldquocourageousrdquo or ldquodeterminedrdquo to de-
scribe someone with schizo-phrenia or depression These are no ldquohot-dishrdquo or get-well card illnesses By harboring negative views we make it more difficult for people to seek treatment
Several strategies help to address this Mental Health First Aid an eight-hour class geared toward
youth or older adults increases mental health litera-cy It teaches people about the symptoms of mental illnesses and how to help when a person is in crisis or is suicidal The nation-wide class educates people about the signs and symptoms of mental illnesses
Another strategy is the Make It Ok campaign a one-hour presentation on how we talk and think about how mental illnesses impact peoplersquos lives Online videos of people with mental illnesses and their families present the impact of mental illnesses as well as personal stories of recovery The goal is to ldquomake it okrdquo to talk about mental illnesses
First Episode programs strive to identify psy-chosis early provide intensive treatment and help young people return to school or work so that they do not become disabled by their illness Early signs can include changing sleep patterns beginning to feel paranoid or having odd thought patterns hav-ing a hard time paying attention avoiding bathing and grooming and cognitive decline Efforts are underway to identify young people at closer to four weeks instead of 72 weeks But parents need to be watchful and not pass it off as a phase Funding was provided by the Legislature in 2015 For details visit the NAMI Minnesota website wwwnamihelpsorg
Progress and hopeWe are making progress that will lead to earlier identification and treatment but our work is not yet done Itrsquos important for everyone to learn about signs symptoms and what actions to take
Mental IllnessReaching out to youth in crisis
Pe RsPec t ive
Half of all people living with a serious mental illness began
experiencing symptoms before the age of 14
8 Minnesota HealtH care news September 2015
sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Ms Abderholden is the executive director of NAMI Minnesota (National Alliance on Mental Illness) a nonprofit organization that works to improve the lives of children and adults with mental illnesses and their families through its programs of education support and advocacy NAMI Minnesota offers more than 500 free classes and presentations and over 60 support groups each year
Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
September 2015 Minnesota HealtH care news 9
10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

SEPTEMBER 2015 Minnesota HealtH care news 3
4 News
7 PeOPLe
8 PeRsPeCTIVe
10 10 QUesTIONs
12 INsURaNCe Diabetes care By Matthew Wicklund
14 OPTOmeTRy sports-related concussions
By Jessica L Schara OD
16 wOUND CaRe your feet and lower
extremities
By Nicole A Bauerly DPM FACFAS and Michael Hu MD FACS
18 CaLeNDaR
28 UROLOgy Overactive bladder By Steven Siegel MD
30 ChRONIC CONDITIONs Living with lupus
By Jennifer Monroe MA MPH and Timothy Niewold MD
September 2015 bull Volume 13 Number 9
Sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Scott Benson MD
Apple Valley Medical Center
Minnesota Heath Care News is published once a month by Minnesota Physician Publishing Inc Our address is 2812 East 26th Street Minneapolis MN 55406 phone 6127288600 fax 6127288601 email mppmppubcom We welcome the submission of manuscripts and letters for possible publication All views and opinions expressed by authors of published articles are solely those of the authors and do not necessarily represent or express the views of Minnesota Physician Publishing Inc or this publication The contents herein are believed accurate but are not intended to replace medical legal tax business or other professional advice and counsel No part of this publication may be reprinted or reproduced without written per-mission of the publisher Annual subscriptions (12 copies) are $3600 Individual copies are $400
Publisher mike starnes | mstarnesmppubcom
editor Lisa mcgowan | lmcgowanmppubcom
AssociAte editor Richard ericson | rericsonmppubcom
Art director Joe Pfahl | joemppubcom
office AdministrAtor amanda marlow | amarlowmppubcom
Account executive stacey Bush | sbushmppubcom
20 mINNesOTa heaLTh CaRe ROUNDTaBLe The new face of health care By MPP Staff
Background and Focus Increasing evidence supports the link between access to mental health care and reducing health care costs Primary care physicians often lack the expertise to diagnose behavioral health correctly and are not always able to easily refer a patient to a mental health care provider Many initiatives nationwide are addressing this issue It is so important that the ACA stipulated the development of the Behavioral Health Home in 2015 Some states including Minnesota are also creating Behavioral Health Home programsObjectives We will review numerous initiatives that support the development of new pathways to behavioral health care We will introduce new ideas and discuss how to incorporate them into our health-care delivery system We will examine the value they can bring and the challenges they will face Our panel of industry experts will outline the steps that must be taken to increase the overall access to mental health care and the broad improvement in population health that this increased access will bring
Panelists include bull Sarah Anderson MSW LICSW CEO Psych Recovery Inc bull Lee Beecher MD President Minnesota Physician-Patient Alliance bull Timothy P Gibbs MD FAPA DFAACAP Chief Medical Officer
Natalis Counseling and Psychology Solutionsbull Martha Lantz MSW LICSW MBA Executive Dir Touchstone Mental Healthbull Judge Kerry W Meyer Hennepin County Criminal Mental Health Court bull Jane Pederson MD Medical Affairs Director Stratis Health bull Jeff Schiff MD MBA Medical Director MN Dept of Human Services bull L Read Sulik MD Chief Integration Officer PrairieCare Sponsors include bull MN Community Healthcare Network bull MN Dept of Human Services bull Natalis Outcomes bull PrairieCare bull Psych Recovery Inc bull Stratis Health
MINNESOTA HEALTH CARE ROUNDTABLE
Please mail call in or fax your registration by 1152015
Please send me tickets at $9500 per ticket Tickets may be ordered by phone at (612) 728-8600 by fax at (612) 728-8601 on our website (mppubcom) or by mail Make checks payable to Minnesota Physician Publishing Mail orders to MPP 2812 East 26th Street Mpls MN 55406 Please note tickets are non-refundable
Name
Company
Address
City State ZIP
TelephoneFAX
Card Exp Date Check enclosed Bill me Credit card (Visa Mastercard American Express or Discover)
Signature
Thursday November 12 2015 bull 100-400 PMDowntown Minneapolis Hilton and Towers
FORTy-FOURTH SESSION
Behavioral Health IntegrationNew pathways to care
4 Minnesota HealtH care news September 2015
N e ws
Drug Companies Delay Reporting Serious Patient Harm to FDADrug manufacturers delay reporting adverse events to the Us Food and Drug administration (FDa) quite often according to a new study from the University of Minnesotarsquos school of Public Health
researchers analyzed 16 million reports submitted through the FDarsquos adverse event reporting system between 2000 and 2014
95 percent of which come from drug manufacturers For each adverse event they calculated the number of days between when doctors alerted the drug companies to when documents were submitted through the reporting system Fed-eral regulation requires that when drug manufacturers receive reports for serious and unexpected adverse events they must report them to the FDa within 15 calendar days
the results show that drug com-panies did not follow this regula-tion for about 10 percent of serious
adverse event cases More than 160000 events were not disclosed to the FDa within the 15-day time frame and more than 40000 of those reports involved patient deaths
ldquoour findings are even more concerning because they are likely an underestimate of the overall underreporting or misreporting of serious or adverse eventsrdquo said Pinar Karaca-Mandic PhD associ-ate professor of health policy at the University of Minnesotarsquos school of Public Health and coauthor of the study ldquoour study analysis is limit-ed to the events that are reported to the FDa and there could be cases in which drug manufacturers fail to report serious or unexpected events at all by downward classifying serious reports as non-seriousrdquo
researchers also found that the delays were longer on average for the cases that involved deaths ldquoa larger fraction of these serious and unexpected events that involved a patient death were delayedmdashabout 12 percent of events with patient death compared to 9 percent of events without patient deathrdquo said Karaca-Mandic
some of the cases were even reported months late ldquowhat was also surprising was that typically these were not delays of just a few daysrdquo said Karaca-Mandic ldquoFor example among events that involved a patient death about 6 percent were reported within 16 to 90 days about 3 percent within 91 to 180 days and about 3 percent were delayed more than 180 daysrdquo
in defense of the findings a spokesperson for the Pharmaceuti-cal research and Manufacturers of america (PhrMa) which rep-resents biopharmaceutical research-ers and biotechnology companies said ldquoit is important to remember that prior to reporting any adverse event including serious unexpected adverse events companies must investigate the reports that they receive from patients and health care professionals companies typ-ically verify the accuracy of patient and physician reports and often contact adverse event reporters to supplement the information that they provide to the FDardquo
the analysis was published online July 27 in the journal JaMa
internal Medicine as part of the report researchers proposed that the FDa create a regulation allowing patients to report side effects directly
ldquoour study suggests that direct submission of reports to the FDa in lieu of submitting to an intermedi-ary such as the drug manufacturer may help reduce reporting delaysrdquo said Paul Ma PhD assistant profes-sor of accounting in carlson school of Management at the University of Minnesota and coauthor of the study ldquowhile it is possible that drug manufacturers spend addi-tional time in verifying reports with more serious patient outcomes the delays are not just by a few days but can be several months or years Future research is needed to help understand the mechanisms behind the drug manufacturerrsquos decision to delay which could help policymak-ers such as the FDa in determining the optimal reporting rulerdquo
Dayton Names Members to New Health Care Program Task Force Gov Mark Dayton has announced his appointments to the 11-member state task force that will evaluate the future of state health care programs including Mnsure and Minnesotacare
the task Force on Health care Financing will look at Mnsurersquos longterm financial viability the possibility of moving to the federal health care exchange and changes to other public health care programs
ldquothe launch of Mnsure created serious problems for many consumers although we have seen significant improvements there are still important unresolved issuesrdquo Dayton wrote ldquolooking ahead we must make some major policy and programmatic decisions that will strengthen Minnesotarsquos position as the nationrsquos health care leader while making the best use of our statersquos financial resourcesrdquo
the 33-member task force will report to Dayton and the legisla-ture by Jan 15 2016
North Memorial to Open Clinic on Nicollet Mall north Memorial Health care has announced plans for an 8000- square-foot clinic on nicollet Mall in the second-floor space former-ly occupied by the saks off 5th department store this will be the health care systemrsquos 16th location in the metro area
the primary care clinic will offer walk-in appointments advanced imaging mammography podiatry occupational medicine and lab services it will have direct access to Gaviidae common and the iDs center
ldquowith this new location we are bringing the north Memorial care that this community has come to trust and value close to where they live and workrdquo says Kelly Mack-en-Marble president of population health and ambulatory services at north Memorial Health care
United Properties and its joint venture capital partner capital real estate inc purchased the first few floors of the nicollet Mall site in December 2014 north Memorial signed a lease for the second-floor space in May and the clinic will open in november
Report Shows Effect of Air Pollution on Public Healthair pollution in the twin cities metro area contributed to an estimated 2000 deaths 400 hospitalizations and 600 visits to the emergency room in 2008 according to a new report from the Minnesota Department of Health (MDH) and Minnesota Pollution control agency (MPca)
the report called ldquolife and breath How air pollution affects public health in the twin citiesrdquo analyzed air quality data from MPca and public health data from MDH the agencies used mathematical modeling software to estimate the effects of air pollution
on public health for residents of the seven-county metro area in 2008 they found that fine particles or ground-level ozone the two most directly harmful air pollutants made conditions worse for an esti-mated 6 to 13 percent of residents in the area who died and 2 to 5 percent of residents who visited the hospital or emergency room for heart or lung issues
ldquothis report helps us see much more clearly than we could before just who is affected by air pollution how serious the effects are and where we have health disparities that need to be addressedrdquo said ed ehlinger MD Minnesota commissioner of health ldquothis report gives us a baseline by which we can measure the health impacts of future reductions in air pollutionrdquo
researchers analyzed data by ZiP codes and while there were no significant differences in air pollution levels between them the agencies did find that people residing in ZiP codes that had a higher percentage of people of color and residents in poverty had more health effects from the air pollution this is partially due to these areas having higher rates of preexisting heart and lung condi-tions in addition ldquoPlaces that have more elderly people with heart and lung conditions and children with uncontrollable asthma are places where air pollution has a greater impactrdquo according to ehlinger
ldquowe canrsquot control canadian wild fires or who is burning coal around the worldrdquo said John linc stine MPca commissioner ldquowe can look at our own choices every day we can choose the most fuel-efficient transportation we can afford or use mass transit small steps really do add up air pollution is a day-in-day-out cumulative problem we can all make a positive impact with the daily choices we makerdquo
according to ehlinger and stine data from 2014 indicate that air quality has improved since 2008 However it is not yet known whether health outcomes improved as well
September 2015 Minnesota HealtH care news 5
News to page 6
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
HealthPartners to Study Improvements in Prediabetes CareHealthPartners institute for edu-cation and research has launched a five-year study to determine if web-based clinical decision support can help in the identification and treatment of patients with prediabe-tes to help reduce their chances of developing type 2 diabetes
ldquoclinical decision support in electronic medical records has improved care for diabetes and appropriate high-tech imaging and we hope to see if it can improve care for people at risk of developing diabetesrdquo said Jay Desai PhD MPH research fellow at Health-Partners institute for education and research and principal investigator of the study
researchers will study about 17000 patient participants with
prediabetes who receive care at 30 essentia Health clinics in northern Minnesota northwest wisconsin and eastern north Dakota they will implement a clinical decision support system to identify people with prediabetes give personalized care recommendations and evalu-ate the effectiveness of the system
ldquothis study aims to impact our patientsrsquo lives by reducing their cardiovascular risk and improving their quality of liferdquo said Daniel saman DrPH MPH cPH associ-ate research scientist at the essentia institute of rural Health
almost one-third of adults in the Us have prediabetes according to the Us centers for Disease control and Prevention and without intervention care 15 to 30 percent of them will develop type 2 diabetes within five years Patients with diabetes have health care costs that are 23 times higher than people who do not have diabetes according to the american Diabetes association
Hysterectomy Linked to Risks for Women Under Age 50researchers at Mayo clinic have shown that hysterectomy may be a marker of early cardiovascular risk and disease most notably for women less than 35 years of age
through the rochester epide-miology Project the researchers analyzed 3816 available records of women who had a hysterectomy with ovarian conservation in olmsted county between 1965 and 2002 they then determined a randomly selected control group of another 3816 women of the same age who had not undergone a hysterectomy and compared cardio-vascular risk factors and diseases for the women they discovered that the women who had a hyster-ectomy had slightly higher odds of having hyperlipidemia obesity and metabolic syndrome
ldquocardiovascular disease is the leading cause of death among women and women see primarily gynecologists between 18 years and 64 yearsmdasha time when early screening for cardiovascular disease would be importantrdquo said shannon laughlin-tommaso MD obstetri-ciangynecologist at Mayo clinic and lead author of the study ldquowe wanted to do this study to find a gynecologic screening method for cardiovascular diseaserdquo
in addition stroke was signifi-cantly more common among wom-en who had a hysterectomy before the age of 35 compared to women of the same age who did not have a hysterectomy women ages 35 to 40 that had a hysterectomy were more likely to have hypertension and women who had a hysterectomy at the age of 50 or older didnrsquot demon-strate any notable increases in risk factors and contrastingly were less likely to have had a stroke or congestive heart failure compared with women of the same age that did not have a hysterectomy
6 Minnesota HealtH care news September 2015
News from page 5
Zhi Halbach DO has joined Hutchinson Health as a family physician Halbach earned her doctor-ate in osteopathic medicine from the Des Moines University College of Osteopathic Medicine She is originally from Chaska and has moved back to Minnesota after completing her residency at St Lukersquos University Hospital in Pennsylvania Hal-bechrsquos special interests include womenrsquos health
preventive care and office procedures In addition Tiffany Trenda DO has joined Hutchinson Health as a pediatri-cian Trenda earned her doctorate in osteopathic medicine from Lake Erie College of Osteopathic Medicine in Pennsylvania and is moving back to her home state of Minnesota after completing her pediatric residency through Palmetto HealthUni-versity of South Carolina Trenda has spent time as a volunteer pediatrician in medically underserved communities in Nicaragua and El Salvador
Kevin Lindgren MD and Jaclyn Bailey MD have joined St Croix Orthopaedics as orthopedic surgeons Lindgren earned his medical degree from the Medical College of Wisconsin and completed an orthopaedic surgery residency at the University of Nebraska Medical CenterCreighton University where he received the Frank P Stone MD award for Outstanding Resident Lindgren completed his fellowship training at the University of Utah where
he specialized in hip and knee reconstruction and hip preservation surgery Bailey earned her doctor of medicine degree at the Univer-sity of Minnesota Medical School and completed an orthopaedic surgery residency at Grand Rapids Medical Education PartnersMichigan State University She completed her fellowship training in hand and upper extremity surgery at the University of California in San Francisco Lindgren will begin seeing patients at the Maplewood and Woodbury clinics in early September and at the new St Paul clinic when it opens later this fall Bailey will begin seeing patients at the Maplewood and Wyoming clinics at the end of September as well as at the new St Paul clinic
Samith Kochuparambil MD has joined Minne sota Oncology with the practice of medical oncology and hematology at the Minneapolis clinic Ko chu pa rambil earned his medical degree from the Madras Medical College Chennai India He completed a residency in internal medicine at the Medical College of Georgia where he received a STAR resident award and completed his fellowship in medical oncology and hematology at Mayo Clinic Kochuparambil specializes in treating pros-tate cancer kidney cancer bladder cancer multiple myeloma and general oncology
Peo Ple
September 2015 MINNESOTA HEALTH CARE NEWS 7
Kevin Lindgren MD
Samith Kochuparambil
MD
Zhi Halbach DO
Tiffany Trenda DO
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Young people experiencing their first psychotic episode wait an average of 72 weeks to seek treatment Other studies report that people
wait an average of 10 years before treatment
Half of all people living with a serious mental illness began experiencing symptoms before the age of 14 Three-quarters will develop a mental illness by age 24 So it is a ldquoyoung personrsquosrdquo illness during a prime time in their lives
For any health care condition early identifica-tion and treatment are critical The more we wait to treat a mental illness the more likely it is to become severe and for the individual to develop a substance use disorder as well So why is this happening
Building awarenessOne reason is that many people including youth are not aware of the symptoms of mental illness Teachers donrsquot receive much initial educa-tion about mental illnesses Limited access to treatment transportation insurance coverage and parent work schedules cause many to go without treatment
Minnesota schools do not require mental health education although there are mental health compo-nents in the National Health Education Standards However there are recommended free and low-cost programs available to schools including NAMI Minnesotarsquos free Ending the Silence program
Ending the Silence fits into 50-minute high school or middle school class periods and covers how common mental illnesses are signs and symptoms and the personal story of a young adult doing well in recovery Students receive resources to get help for themselves or a friend and information on how to fight the stigma of mental illnesses NAMI Minne-sota also developed a website for youth
In 2003 Minnesota became the first state to require continuing education for teachers on the key warning signs of early-onset mental illnesses in chil-dren and adolescents In 2013 trauma and autism were added These trainings help teachers under-stand the difference between willful behavior and symptomsmdashnot to have teachers diagnose students but to know when to talk to parents about a referral
In 2007 the Legislature funded school-linked mental health grants Grants are provided to mental health providers who then co-locate in the schools eliminating the barriers to treatment Funds pay for activities not funded by insurance such as collabo-ration with school support staff and teachers and for treatment of children who are uninsured and
underinsured Data from the first four years show that nearly half of the children had never received treatment and half of those had a serious mental illness While funding was doubled in 2013 only roughly 50 percent of schools have such a program
Reducing stigmaAnother issue is that parents and other adults work-ing with youth are not aware of the symptoms and frankly have stigmatizing attitudes Some believe that mental illnesses cannot occur in children and others believe that itrsquos just a ldquophaserdquo
We use slang words such as ldquocrazyrdquo and ldquonutsrdquo for people with mental illnesses but we donrsquot have slang words for other illnesses We never think to use the words ldquocourageousrdquo or ldquodeterminedrdquo to de-
scribe someone with schizo-phrenia or depression These are no ldquohot-dishrdquo or get-well card illnesses By harboring negative views we make it more difficult for people to seek treatment
Several strategies help to address this Mental Health First Aid an eight-hour class geared toward
youth or older adults increases mental health litera-cy It teaches people about the symptoms of mental illnesses and how to help when a person is in crisis or is suicidal The nation-wide class educates people about the signs and symptoms of mental illnesses
Another strategy is the Make It Ok campaign a one-hour presentation on how we talk and think about how mental illnesses impact peoplersquos lives Online videos of people with mental illnesses and their families present the impact of mental illnesses as well as personal stories of recovery The goal is to ldquomake it okrdquo to talk about mental illnesses
First Episode programs strive to identify psy-chosis early provide intensive treatment and help young people return to school or work so that they do not become disabled by their illness Early signs can include changing sleep patterns beginning to feel paranoid or having odd thought patterns hav-ing a hard time paying attention avoiding bathing and grooming and cognitive decline Efforts are underway to identify young people at closer to four weeks instead of 72 weeks But parents need to be watchful and not pass it off as a phase Funding was provided by the Legislature in 2015 For details visit the NAMI Minnesota website wwwnamihelpsorg
Progress and hopeWe are making progress that will lead to earlier identification and treatment but our work is not yet done Itrsquos important for everyone to learn about signs symptoms and what actions to take
Mental IllnessReaching out to youth in crisis
Pe RsPec t ive
Half of all people living with a serious mental illness began
experiencing symptoms before the age of 14
8 Minnesota HealtH care news September 2015
sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Ms Abderholden is the executive director of NAMI Minnesota (National Alliance on Mental Illness) a nonprofit organization that works to improve the lives of children and adults with mental illnesses and their families through its programs of education support and advocacy NAMI Minnesota offers more than 500 free classes and presentations and over 60 support groups each year
Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
September 2015 Minnesota HealtH care news 9
10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

4 Minnesota HealtH care news September 2015
N e ws
Drug Companies Delay Reporting Serious Patient Harm to FDADrug manufacturers delay reporting adverse events to the Us Food and Drug administration (FDa) quite often according to a new study from the University of Minnesotarsquos school of Public Health
researchers analyzed 16 million reports submitted through the FDarsquos adverse event reporting system between 2000 and 2014
95 percent of which come from drug manufacturers For each adverse event they calculated the number of days between when doctors alerted the drug companies to when documents were submitted through the reporting system Fed-eral regulation requires that when drug manufacturers receive reports for serious and unexpected adverse events they must report them to the FDa within 15 calendar days
the results show that drug com-panies did not follow this regula-tion for about 10 percent of serious
adverse event cases More than 160000 events were not disclosed to the FDa within the 15-day time frame and more than 40000 of those reports involved patient deaths
ldquoour findings are even more concerning because they are likely an underestimate of the overall underreporting or misreporting of serious or adverse eventsrdquo said Pinar Karaca-Mandic PhD associ-ate professor of health policy at the University of Minnesotarsquos school of Public Health and coauthor of the study ldquoour study analysis is limit-ed to the events that are reported to the FDa and there could be cases in which drug manufacturers fail to report serious or unexpected events at all by downward classifying serious reports as non-seriousrdquo
researchers also found that the delays were longer on average for the cases that involved deaths ldquoa larger fraction of these serious and unexpected events that involved a patient death were delayedmdashabout 12 percent of events with patient death compared to 9 percent of events without patient deathrdquo said Karaca-Mandic
some of the cases were even reported months late ldquowhat was also surprising was that typically these were not delays of just a few daysrdquo said Karaca-Mandic ldquoFor example among events that involved a patient death about 6 percent were reported within 16 to 90 days about 3 percent within 91 to 180 days and about 3 percent were delayed more than 180 daysrdquo
in defense of the findings a spokesperson for the Pharmaceuti-cal research and Manufacturers of america (PhrMa) which rep-resents biopharmaceutical research-ers and biotechnology companies said ldquoit is important to remember that prior to reporting any adverse event including serious unexpected adverse events companies must investigate the reports that they receive from patients and health care professionals companies typ-ically verify the accuracy of patient and physician reports and often contact adverse event reporters to supplement the information that they provide to the FDardquo
the analysis was published online July 27 in the journal JaMa
internal Medicine as part of the report researchers proposed that the FDa create a regulation allowing patients to report side effects directly
ldquoour study suggests that direct submission of reports to the FDa in lieu of submitting to an intermedi-ary such as the drug manufacturer may help reduce reporting delaysrdquo said Paul Ma PhD assistant profes-sor of accounting in carlson school of Management at the University of Minnesota and coauthor of the study ldquowhile it is possible that drug manufacturers spend addi-tional time in verifying reports with more serious patient outcomes the delays are not just by a few days but can be several months or years Future research is needed to help understand the mechanisms behind the drug manufacturerrsquos decision to delay which could help policymak-ers such as the FDa in determining the optimal reporting rulerdquo
Dayton Names Members to New Health Care Program Task Force Gov Mark Dayton has announced his appointments to the 11-member state task force that will evaluate the future of state health care programs including Mnsure and Minnesotacare
the task Force on Health care Financing will look at Mnsurersquos longterm financial viability the possibility of moving to the federal health care exchange and changes to other public health care programs
ldquothe launch of Mnsure created serious problems for many consumers although we have seen significant improvements there are still important unresolved issuesrdquo Dayton wrote ldquolooking ahead we must make some major policy and programmatic decisions that will strengthen Minnesotarsquos position as the nationrsquos health care leader while making the best use of our statersquos financial resourcesrdquo
the 33-member task force will report to Dayton and the legisla-ture by Jan 15 2016
North Memorial to Open Clinic on Nicollet Mall north Memorial Health care has announced plans for an 8000- square-foot clinic on nicollet Mall in the second-floor space former-ly occupied by the saks off 5th department store this will be the health care systemrsquos 16th location in the metro area
the primary care clinic will offer walk-in appointments advanced imaging mammography podiatry occupational medicine and lab services it will have direct access to Gaviidae common and the iDs center
ldquowith this new location we are bringing the north Memorial care that this community has come to trust and value close to where they live and workrdquo says Kelly Mack-en-Marble president of population health and ambulatory services at north Memorial Health care
United Properties and its joint venture capital partner capital real estate inc purchased the first few floors of the nicollet Mall site in December 2014 north Memorial signed a lease for the second-floor space in May and the clinic will open in november
Report Shows Effect of Air Pollution on Public Healthair pollution in the twin cities metro area contributed to an estimated 2000 deaths 400 hospitalizations and 600 visits to the emergency room in 2008 according to a new report from the Minnesota Department of Health (MDH) and Minnesota Pollution control agency (MPca)
the report called ldquolife and breath How air pollution affects public health in the twin citiesrdquo analyzed air quality data from MPca and public health data from MDH the agencies used mathematical modeling software to estimate the effects of air pollution
on public health for residents of the seven-county metro area in 2008 they found that fine particles or ground-level ozone the two most directly harmful air pollutants made conditions worse for an esti-mated 6 to 13 percent of residents in the area who died and 2 to 5 percent of residents who visited the hospital or emergency room for heart or lung issues
ldquothis report helps us see much more clearly than we could before just who is affected by air pollution how serious the effects are and where we have health disparities that need to be addressedrdquo said ed ehlinger MD Minnesota commissioner of health ldquothis report gives us a baseline by which we can measure the health impacts of future reductions in air pollutionrdquo
researchers analyzed data by ZiP codes and while there were no significant differences in air pollution levels between them the agencies did find that people residing in ZiP codes that had a higher percentage of people of color and residents in poverty had more health effects from the air pollution this is partially due to these areas having higher rates of preexisting heart and lung condi-tions in addition ldquoPlaces that have more elderly people with heart and lung conditions and children with uncontrollable asthma are places where air pollution has a greater impactrdquo according to ehlinger
ldquowe canrsquot control canadian wild fires or who is burning coal around the worldrdquo said John linc stine MPca commissioner ldquowe can look at our own choices every day we can choose the most fuel-efficient transportation we can afford or use mass transit small steps really do add up air pollution is a day-in-day-out cumulative problem we can all make a positive impact with the daily choices we makerdquo
according to ehlinger and stine data from 2014 indicate that air quality has improved since 2008 However it is not yet known whether health outcomes improved as well
September 2015 Minnesota HealtH care news 5
News to page 6
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
HealthPartners to Study Improvements in Prediabetes CareHealthPartners institute for edu-cation and research has launched a five-year study to determine if web-based clinical decision support can help in the identification and treatment of patients with prediabe-tes to help reduce their chances of developing type 2 diabetes
ldquoclinical decision support in electronic medical records has improved care for diabetes and appropriate high-tech imaging and we hope to see if it can improve care for people at risk of developing diabetesrdquo said Jay Desai PhD MPH research fellow at Health-Partners institute for education and research and principal investigator of the study
researchers will study about 17000 patient participants with
prediabetes who receive care at 30 essentia Health clinics in northern Minnesota northwest wisconsin and eastern north Dakota they will implement a clinical decision support system to identify people with prediabetes give personalized care recommendations and evalu-ate the effectiveness of the system
ldquothis study aims to impact our patientsrsquo lives by reducing their cardiovascular risk and improving their quality of liferdquo said Daniel saman DrPH MPH cPH associ-ate research scientist at the essentia institute of rural Health
almost one-third of adults in the Us have prediabetes according to the Us centers for Disease control and Prevention and without intervention care 15 to 30 percent of them will develop type 2 diabetes within five years Patients with diabetes have health care costs that are 23 times higher than people who do not have diabetes according to the american Diabetes association
Hysterectomy Linked to Risks for Women Under Age 50researchers at Mayo clinic have shown that hysterectomy may be a marker of early cardiovascular risk and disease most notably for women less than 35 years of age
through the rochester epide-miology Project the researchers analyzed 3816 available records of women who had a hysterectomy with ovarian conservation in olmsted county between 1965 and 2002 they then determined a randomly selected control group of another 3816 women of the same age who had not undergone a hysterectomy and compared cardio-vascular risk factors and diseases for the women they discovered that the women who had a hyster-ectomy had slightly higher odds of having hyperlipidemia obesity and metabolic syndrome
ldquocardiovascular disease is the leading cause of death among women and women see primarily gynecologists between 18 years and 64 yearsmdasha time when early screening for cardiovascular disease would be importantrdquo said shannon laughlin-tommaso MD obstetri-ciangynecologist at Mayo clinic and lead author of the study ldquowe wanted to do this study to find a gynecologic screening method for cardiovascular diseaserdquo
in addition stroke was signifi-cantly more common among wom-en who had a hysterectomy before the age of 35 compared to women of the same age who did not have a hysterectomy women ages 35 to 40 that had a hysterectomy were more likely to have hypertension and women who had a hysterectomy at the age of 50 or older didnrsquot demon-strate any notable increases in risk factors and contrastingly were less likely to have had a stroke or congestive heart failure compared with women of the same age that did not have a hysterectomy
6 Minnesota HealtH care news September 2015
News from page 5
Zhi Halbach DO has joined Hutchinson Health as a family physician Halbach earned her doctor-ate in osteopathic medicine from the Des Moines University College of Osteopathic Medicine She is originally from Chaska and has moved back to Minnesota after completing her residency at St Lukersquos University Hospital in Pennsylvania Hal-bechrsquos special interests include womenrsquos health
preventive care and office procedures In addition Tiffany Trenda DO has joined Hutchinson Health as a pediatri-cian Trenda earned her doctorate in osteopathic medicine from Lake Erie College of Osteopathic Medicine in Pennsylvania and is moving back to her home state of Minnesota after completing her pediatric residency through Palmetto HealthUni-versity of South Carolina Trenda has spent time as a volunteer pediatrician in medically underserved communities in Nicaragua and El Salvador
Kevin Lindgren MD and Jaclyn Bailey MD have joined St Croix Orthopaedics as orthopedic surgeons Lindgren earned his medical degree from the Medical College of Wisconsin and completed an orthopaedic surgery residency at the University of Nebraska Medical CenterCreighton University where he received the Frank P Stone MD award for Outstanding Resident Lindgren completed his fellowship training at the University of Utah where
he specialized in hip and knee reconstruction and hip preservation surgery Bailey earned her doctor of medicine degree at the Univer-sity of Minnesota Medical School and completed an orthopaedic surgery residency at Grand Rapids Medical Education PartnersMichigan State University She completed her fellowship training in hand and upper extremity surgery at the University of California in San Francisco Lindgren will begin seeing patients at the Maplewood and Woodbury clinics in early September and at the new St Paul clinic when it opens later this fall Bailey will begin seeing patients at the Maplewood and Wyoming clinics at the end of September as well as at the new St Paul clinic
Samith Kochuparambil MD has joined Minne sota Oncology with the practice of medical oncology and hematology at the Minneapolis clinic Ko chu pa rambil earned his medical degree from the Madras Medical College Chennai India He completed a residency in internal medicine at the Medical College of Georgia where he received a STAR resident award and completed his fellowship in medical oncology and hematology at Mayo Clinic Kochuparambil specializes in treating pros-tate cancer kidney cancer bladder cancer multiple myeloma and general oncology
Peo Ple
September 2015 MINNESOTA HEALTH CARE NEWS 7
Kevin Lindgren MD
Samith Kochuparambil
MD
Zhi Halbach DO
Tiffany Trenda DO
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Young people experiencing their first psychotic episode wait an average of 72 weeks to seek treatment Other studies report that people
wait an average of 10 years before treatment
Half of all people living with a serious mental illness began experiencing symptoms before the age of 14 Three-quarters will develop a mental illness by age 24 So it is a ldquoyoung personrsquosrdquo illness during a prime time in their lives
For any health care condition early identifica-tion and treatment are critical The more we wait to treat a mental illness the more likely it is to become severe and for the individual to develop a substance use disorder as well So why is this happening
Building awarenessOne reason is that many people including youth are not aware of the symptoms of mental illness Teachers donrsquot receive much initial educa-tion about mental illnesses Limited access to treatment transportation insurance coverage and parent work schedules cause many to go without treatment
Minnesota schools do not require mental health education although there are mental health compo-nents in the National Health Education Standards However there are recommended free and low-cost programs available to schools including NAMI Minnesotarsquos free Ending the Silence program
Ending the Silence fits into 50-minute high school or middle school class periods and covers how common mental illnesses are signs and symptoms and the personal story of a young adult doing well in recovery Students receive resources to get help for themselves or a friend and information on how to fight the stigma of mental illnesses NAMI Minne-sota also developed a website for youth
In 2003 Minnesota became the first state to require continuing education for teachers on the key warning signs of early-onset mental illnesses in chil-dren and adolescents In 2013 trauma and autism were added These trainings help teachers under-stand the difference between willful behavior and symptomsmdashnot to have teachers diagnose students but to know when to talk to parents about a referral
In 2007 the Legislature funded school-linked mental health grants Grants are provided to mental health providers who then co-locate in the schools eliminating the barriers to treatment Funds pay for activities not funded by insurance such as collabo-ration with school support staff and teachers and for treatment of children who are uninsured and
underinsured Data from the first four years show that nearly half of the children had never received treatment and half of those had a serious mental illness While funding was doubled in 2013 only roughly 50 percent of schools have such a program
Reducing stigmaAnother issue is that parents and other adults work-ing with youth are not aware of the symptoms and frankly have stigmatizing attitudes Some believe that mental illnesses cannot occur in children and others believe that itrsquos just a ldquophaserdquo
We use slang words such as ldquocrazyrdquo and ldquonutsrdquo for people with mental illnesses but we donrsquot have slang words for other illnesses We never think to use the words ldquocourageousrdquo or ldquodeterminedrdquo to de-
scribe someone with schizo-phrenia or depression These are no ldquohot-dishrdquo or get-well card illnesses By harboring negative views we make it more difficult for people to seek treatment
Several strategies help to address this Mental Health First Aid an eight-hour class geared toward
youth or older adults increases mental health litera-cy It teaches people about the symptoms of mental illnesses and how to help when a person is in crisis or is suicidal The nation-wide class educates people about the signs and symptoms of mental illnesses
Another strategy is the Make It Ok campaign a one-hour presentation on how we talk and think about how mental illnesses impact peoplersquos lives Online videos of people with mental illnesses and their families present the impact of mental illnesses as well as personal stories of recovery The goal is to ldquomake it okrdquo to talk about mental illnesses
First Episode programs strive to identify psy-chosis early provide intensive treatment and help young people return to school or work so that they do not become disabled by their illness Early signs can include changing sleep patterns beginning to feel paranoid or having odd thought patterns hav-ing a hard time paying attention avoiding bathing and grooming and cognitive decline Efforts are underway to identify young people at closer to four weeks instead of 72 weeks But parents need to be watchful and not pass it off as a phase Funding was provided by the Legislature in 2015 For details visit the NAMI Minnesota website wwwnamihelpsorg
Progress and hopeWe are making progress that will lead to earlier identification and treatment but our work is not yet done Itrsquos important for everyone to learn about signs symptoms and what actions to take
Mental IllnessReaching out to youth in crisis
Pe RsPec t ive
Half of all people living with a serious mental illness began
experiencing symptoms before the age of 14
8 Minnesota HealtH care news September 2015
sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Ms Abderholden is the executive director of NAMI Minnesota (National Alliance on Mental Illness) a nonprofit organization that works to improve the lives of children and adults with mental illnesses and their families through its programs of education support and advocacy NAMI Minnesota offers more than 500 free classes and presentations and over 60 support groups each year
Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
September 2015 Minnesota HealtH care news 9
10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

North Memorial to Open Clinic on Nicollet Mall north Memorial Health care has announced plans for an 8000- square-foot clinic on nicollet Mall in the second-floor space former-ly occupied by the saks off 5th department store this will be the health care systemrsquos 16th location in the metro area
the primary care clinic will offer walk-in appointments advanced imaging mammography podiatry occupational medicine and lab services it will have direct access to Gaviidae common and the iDs center
ldquowith this new location we are bringing the north Memorial care that this community has come to trust and value close to where they live and workrdquo says Kelly Mack-en-Marble president of population health and ambulatory services at north Memorial Health care
United Properties and its joint venture capital partner capital real estate inc purchased the first few floors of the nicollet Mall site in December 2014 north Memorial signed a lease for the second-floor space in May and the clinic will open in november
Report Shows Effect of Air Pollution on Public Healthair pollution in the twin cities metro area contributed to an estimated 2000 deaths 400 hospitalizations and 600 visits to the emergency room in 2008 according to a new report from the Minnesota Department of Health (MDH) and Minnesota Pollution control agency (MPca)
the report called ldquolife and breath How air pollution affects public health in the twin citiesrdquo analyzed air quality data from MPca and public health data from MDH the agencies used mathematical modeling software to estimate the effects of air pollution
on public health for residents of the seven-county metro area in 2008 they found that fine particles or ground-level ozone the two most directly harmful air pollutants made conditions worse for an esti-mated 6 to 13 percent of residents in the area who died and 2 to 5 percent of residents who visited the hospital or emergency room for heart or lung issues
ldquothis report helps us see much more clearly than we could before just who is affected by air pollution how serious the effects are and where we have health disparities that need to be addressedrdquo said ed ehlinger MD Minnesota commissioner of health ldquothis report gives us a baseline by which we can measure the health impacts of future reductions in air pollutionrdquo
researchers analyzed data by ZiP codes and while there were no significant differences in air pollution levels between them the agencies did find that people residing in ZiP codes that had a higher percentage of people of color and residents in poverty had more health effects from the air pollution this is partially due to these areas having higher rates of preexisting heart and lung condi-tions in addition ldquoPlaces that have more elderly people with heart and lung conditions and children with uncontrollable asthma are places where air pollution has a greater impactrdquo according to ehlinger
ldquowe canrsquot control canadian wild fires or who is burning coal around the worldrdquo said John linc stine MPca commissioner ldquowe can look at our own choices every day we can choose the most fuel-efficient transportation we can afford or use mass transit small steps really do add up air pollution is a day-in-day-out cumulative problem we can all make a positive impact with the daily choices we makerdquo
according to ehlinger and stine data from 2014 indicate that air quality has improved since 2008 However it is not yet known whether health outcomes improved as well
September 2015 Minnesota HealtH care news 5
News to page 6
H2462_72596_01 Accepted 9252013 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
The real question
is
who can make
Medicare easier
Turn to HealthPartners Freedom and
let us help you nd the perfect plan to
meet your needs and budget
Visit healthpartnerscommedicare
INFORMATIONJob Number 245-13124 Trim 4w x 525h Modifi cation Date September 10 2014 1008 AM
Client HealthPartners Bleed Output Date 091014
Description Medicare 2014 Print Live Page 1
File Name 245-13124 Medicare [Home][4x525] r1
SIGN-OFF
[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
1
Did you knowbull Diabetic retinopathy can be controlled and
diabetic patients need regular eye exams tomaintain vision and good eye health
bull Diabetes Type ll can also cause vision changesbull Glaucoma must be diagnosed in early stages in
order to prevent vision lossbull All children entering school need a comprehen-
sive eye exam because vision screenings do notdetect a number of eye disorders
bull To maintain eye health everybody from babiesto boomers to older adults needs a regular eyeexam by a family eye doctor
To locate an optometrist near you and find comprehensive information about eye health visit
httpMinnesotaaoaorg
Minnesota Optometric Association
Doctors on the frontline of eye and vision care
HealthPartners to Study Improvements in Prediabetes CareHealthPartners institute for edu-cation and research has launched a five-year study to determine if web-based clinical decision support can help in the identification and treatment of patients with prediabe-tes to help reduce their chances of developing type 2 diabetes
ldquoclinical decision support in electronic medical records has improved care for diabetes and appropriate high-tech imaging and we hope to see if it can improve care for people at risk of developing diabetesrdquo said Jay Desai PhD MPH research fellow at Health-Partners institute for education and research and principal investigator of the study
researchers will study about 17000 patient participants with
prediabetes who receive care at 30 essentia Health clinics in northern Minnesota northwest wisconsin and eastern north Dakota they will implement a clinical decision support system to identify people with prediabetes give personalized care recommendations and evalu-ate the effectiveness of the system
ldquothis study aims to impact our patientsrsquo lives by reducing their cardiovascular risk and improving their quality of liferdquo said Daniel saman DrPH MPH cPH associ-ate research scientist at the essentia institute of rural Health
almost one-third of adults in the Us have prediabetes according to the Us centers for Disease control and Prevention and without intervention care 15 to 30 percent of them will develop type 2 diabetes within five years Patients with diabetes have health care costs that are 23 times higher than people who do not have diabetes according to the american Diabetes association
Hysterectomy Linked to Risks for Women Under Age 50researchers at Mayo clinic have shown that hysterectomy may be a marker of early cardiovascular risk and disease most notably for women less than 35 years of age
through the rochester epide-miology Project the researchers analyzed 3816 available records of women who had a hysterectomy with ovarian conservation in olmsted county between 1965 and 2002 they then determined a randomly selected control group of another 3816 women of the same age who had not undergone a hysterectomy and compared cardio-vascular risk factors and diseases for the women they discovered that the women who had a hyster-ectomy had slightly higher odds of having hyperlipidemia obesity and metabolic syndrome
ldquocardiovascular disease is the leading cause of death among women and women see primarily gynecologists between 18 years and 64 yearsmdasha time when early screening for cardiovascular disease would be importantrdquo said shannon laughlin-tommaso MD obstetri-ciangynecologist at Mayo clinic and lead author of the study ldquowe wanted to do this study to find a gynecologic screening method for cardiovascular diseaserdquo
in addition stroke was signifi-cantly more common among wom-en who had a hysterectomy before the age of 35 compared to women of the same age who did not have a hysterectomy women ages 35 to 40 that had a hysterectomy were more likely to have hypertension and women who had a hysterectomy at the age of 50 or older didnrsquot demon-strate any notable increases in risk factors and contrastingly were less likely to have had a stroke or congestive heart failure compared with women of the same age that did not have a hysterectomy
6 Minnesota HealtH care news September 2015
News from page 5
Zhi Halbach DO has joined Hutchinson Health as a family physician Halbach earned her doctor-ate in osteopathic medicine from the Des Moines University College of Osteopathic Medicine She is originally from Chaska and has moved back to Minnesota after completing her residency at St Lukersquos University Hospital in Pennsylvania Hal-bechrsquos special interests include womenrsquos health
preventive care and office procedures In addition Tiffany Trenda DO has joined Hutchinson Health as a pediatri-cian Trenda earned her doctorate in osteopathic medicine from Lake Erie College of Osteopathic Medicine in Pennsylvania and is moving back to her home state of Minnesota after completing her pediatric residency through Palmetto HealthUni-versity of South Carolina Trenda has spent time as a volunteer pediatrician in medically underserved communities in Nicaragua and El Salvador
Kevin Lindgren MD and Jaclyn Bailey MD have joined St Croix Orthopaedics as orthopedic surgeons Lindgren earned his medical degree from the Medical College of Wisconsin and completed an orthopaedic surgery residency at the University of Nebraska Medical CenterCreighton University where he received the Frank P Stone MD award for Outstanding Resident Lindgren completed his fellowship training at the University of Utah where
he specialized in hip and knee reconstruction and hip preservation surgery Bailey earned her doctor of medicine degree at the Univer-sity of Minnesota Medical School and completed an orthopaedic surgery residency at Grand Rapids Medical Education PartnersMichigan State University She completed her fellowship training in hand and upper extremity surgery at the University of California in San Francisco Lindgren will begin seeing patients at the Maplewood and Woodbury clinics in early September and at the new St Paul clinic when it opens later this fall Bailey will begin seeing patients at the Maplewood and Wyoming clinics at the end of September as well as at the new St Paul clinic
Samith Kochuparambil MD has joined Minne sota Oncology with the practice of medical oncology and hematology at the Minneapolis clinic Ko chu pa rambil earned his medical degree from the Madras Medical College Chennai India He completed a residency in internal medicine at the Medical College of Georgia where he received a STAR resident award and completed his fellowship in medical oncology and hematology at Mayo Clinic Kochuparambil specializes in treating pros-tate cancer kidney cancer bladder cancer multiple myeloma and general oncology
Peo Ple
September 2015 MINNESOTA HEALTH CARE NEWS 7
Kevin Lindgren MD
Samith Kochuparambil
MD
Zhi Halbach DO
Tiffany Trenda DO
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Young people experiencing their first psychotic episode wait an average of 72 weeks to seek treatment Other studies report that people
wait an average of 10 years before treatment
Half of all people living with a serious mental illness began experiencing symptoms before the age of 14 Three-quarters will develop a mental illness by age 24 So it is a ldquoyoung personrsquosrdquo illness during a prime time in their lives
For any health care condition early identifica-tion and treatment are critical The more we wait to treat a mental illness the more likely it is to become severe and for the individual to develop a substance use disorder as well So why is this happening
Building awarenessOne reason is that many people including youth are not aware of the symptoms of mental illness Teachers donrsquot receive much initial educa-tion about mental illnesses Limited access to treatment transportation insurance coverage and parent work schedules cause many to go without treatment
Minnesota schools do not require mental health education although there are mental health compo-nents in the National Health Education Standards However there are recommended free and low-cost programs available to schools including NAMI Minnesotarsquos free Ending the Silence program
Ending the Silence fits into 50-minute high school or middle school class periods and covers how common mental illnesses are signs and symptoms and the personal story of a young adult doing well in recovery Students receive resources to get help for themselves or a friend and information on how to fight the stigma of mental illnesses NAMI Minne-sota also developed a website for youth
In 2003 Minnesota became the first state to require continuing education for teachers on the key warning signs of early-onset mental illnesses in chil-dren and adolescents In 2013 trauma and autism were added These trainings help teachers under-stand the difference between willful behavior and symptomsmdashnot to have teachers diagnose students but to know when to talk to parents about a referral
In 2007 the Legislature funded school-linked mental health grants Grants are provided to mental health providers who then co-locate in the schools eliminating the barriers to treatment Funds pay for activities not funded by insurance such as collabo-ration with school support staff and teachers and for treatment of children who are uninsured and
underinsured Data from the first four years show that nearly half of the children had never received treatment and half of those had a serious mental illness While funding was doubled in 2013 only roughly 50 percent of schools have such a program
Reducing stigmaAnother issue is that parents and other adults work-ing with youth are not aware of the symptoms and frankly have stigmatizing attitudes Some believe that mental illnesses cannot occur in children and others believe that itrsquos just a ldquophaserdquo
We use slang words such as ldquocrazyrdquo and ldquonutsrdquo for people with mental illnesses but we donrsquot have slang words for other illnesses We never think to use the words ldquocourageousrdquo or ldquodeterminedrdquo to de-
scribe someone with schizo-phrenia or depression These are no ldquohot-dishrdquo or get-well card illnesses By harboring negative views we make it more difficult for people to seek treatment
Several strategies help to address this Mental Health First Aid an eight-hour class geared toward
youth or older adults increases mental health litera-cy It teaches people about the symptoms of mental illnesses and how to help when a person is in crisis or is suicidal The nation-wide class educates people about the signs and symptoms of mental illnesses
Another strategy is the Make It Ok campaign a one-hour presentation on how we talk and think about how mental illnesses impact peoplersquos lives Online videos of people with mental illnesses and their families present the impact of mental illnesses as well as personal stories of recovery The goal is to ldquomake it okrdquo to talk about mental illnesses
First Episode programs strive to identify psy-chosis early provide intensive treatment and help young people return to school or work so that they do not become disabled by their illness Early signs can include changing sleep patterns beginning to feel paranoid or having odd thought patterns hav-ing a hard time paying attention avoiding bathing and grooming and cognitive decline Efforts are underway to identify young people at closer to four weeks instead of 72 weeks But parents need to be watchful and not pass it off as a phase Funding was provided by the Legislature in 2015 For details visit the NAMI Minnesota website wwwnamihelpsorg
Progress and hopeWe are making progress that will lead to earlier identification and treatment but our work is not yet done Itrsquos important for everyone to learn about signs symptoms and what actions to take
Mental IllnessReaching out to youth in crisis
Pe RsPec t ive
Half of all people living with a serious mental illness began
experiencing symptoms before the age of 14
8 Minnesota HealtH care news September 2015
sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Ms Abderholden is the executive director of NAMI Minnesota (National Alliance on Mental Illness) a nonprofit organization that works to improve the lives of children and adults with mental illnesses and their families through its programs of education support and advocacy NAMI Minnesota offers more than 500 free classes and presentations and over 60 support groups each year
Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
September 2015 Minnesota HealtH care news 9
10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

HealthPartners to Study Improvements in Prediabetes CareHealthPartners institute for edu-cation and research has launched a five-year study to determine if web-based clinical decision support can help in the identification and treatment of patients with prediabe-tes to help reduce their chances of developing type 2 diabetes
ldquoclinical decision support in electronic medical records has improved care for diabetes and appropriate high-tech imaging and we hope to see if it can improve care for people at risk of developing diabetesrdquo said Jay Desai PhD MPH research fellow at Health-Partners institute for education and research and principal investigator of the study
researchers will study about 17000 patient participants with
prediabetes who receive care at 30 essentia Health clinics in northern Minnesota northwest wisconsin and eastern north Dakota they will implement a clinical decision support system to identify people with prediabetes give personalized care recommendations and evalu-ate the effectiveness of the system
ldquothis study aims to impact our patientsrsquo lives by reducing their cardiovascular risk and improving their quality of liferdquo said Daniel saman DrPH MPH cPH associ-ate research scientist at the essentia institute of rural Health
almost one-third of adults in the Us have prediabetes according to the Us centers for Disease control and Prevention and without intervention care 15 to 30 percent of them will develop type 2 diabetes within five years Patients with diabetes have health care costs that are 23 times higher than people who do not have diabetes according to the american Diabetes association
Hysterectomy Linked to Risks for Women Under Age 50researchers at Mayo clinic have shown that hysterectomy may be a marker of early cardiovascular risk and disease most notably for women less than 35 years of age
through the rochester epide-miology Project the researchers analyzed 3816 available records of women who had a hysterectomy with ovarian conservation in olmsted county between 1965 and 2002 they then determined a randomly selected control group of another 3816 women of the same age who had not undergone a hysterectomy and compared cardio-vascular risk factors and diseases for the women they discovered that the women who had a hyster-ectomy had slightly higher odds of having hyperlipidemia obesity and metabolic syndrome
ldquocardiovascular disease is the leading cause of death among women and women see primarily gynecologists between 18 years and 64 yearsmdasha time when early screening for cardiovascular disease would be importantrdquo said shannon laughlin-tommaso MD obstetri-ciangynecologist at Mayo clinic and lead author of the study ldquowe wanted to do this study to find a gynecologic screening method for cardiovascular diseaserdquo
in addition stroke was signifi-cantly more common among wom-en who had a hysterectomy before the age of 35 compared to women of the same age who did not have a hysterectomy women ages 35 to 40 that had a hysterectomy were more likely to have hypertension and women who had a hysterectomy at the age of 50 or older didnrsquot demon-strate any notable increases in risk factors and contrastingly were less likely to have had a stroke or congestive heart failure compared with women of the same age that did not have a hysterectomy
6 Minnesota HealtH care news September 2015
News from page 5
Zhi Halbach DO has joined Hutchinson Health as a family physician Halbach earned her doctor-ate in osteopathic medicine from the Des Moines University College of Osteopathic Medicine She is originally from Chaska and has moved back to Minnesota after completing her residency at St Lukersquos University Hospital in Pennsylvania Hal-bechrsquos special interests include womenrsquos health
preventive care and office procedures In addition Tiffany Trenda DO has joined Hutchinson Health as a pediatri-cian Trenda earned her doctorate in osteopathic medicine from Lake Erie College of Osteopathic Medicine in Pennsylvania and is moving back to her home state of Minnesota after completing her pediatric residency through Palmetto HealthUni-versity of South Carolina Trenda has spent time as a volunteer pediatrician in medically underserved communities in Nicaragua and El Salvador
Kevin Lindgren MD and Jaclyn Bailey MD have joined St Croix Orthopaedics as orthopedic surgeons Lindgren earned his medical degree from the Medical College of Wisconsin and completed an orthopaedic surgery residency at the University of Nebraska Medical CenterCreighton University where he received the Frank P Stone MD award for Outstanding Resident Lindgren completed his fellowship training at the University of Utah where
he specialized in hip and knee reconstruction and hip preservation surgery Bailey earned her doctor of medicine degree at the Univer-sity of Minnesota Medical School and completed an orthopaedic surgery residency at Grand Rapids Medical Education PartnersMichigan State University She completed her fellowship training in hand and upper extremity surgery at the University of California in San Francisco Lindgren will begin seeing patients at the Maplewood and Woodbury clinics in early September and at the new St Paul clinic when it opens later this fall Bailey will begin seeing patients at the Maplewood and Wyoming clinics at the end of September as well as at the new St Paul clinic
Samith Kochuparambil MD has joined Minne sota Oncology with the practice of medical oncology and hematology at the Minneapolis clinic Ko chu pa rambil earned his medical degree from the Madras Medical College Chennai India He completed a residency in internal medicine at the Medical College of Georgia where he received a STAR resident award and completed his fellowship in medical oncology and hematology at Mayo Clinic Kochuparambil specializes in treating pros-tate cancer kidney cancer bladder cancer multiple myeloma and general oncology
Peo Ple
September 2015 MINNESOTA HEALTH CARE NEWS 7
Kevin Lindgren MD
Samith Kochuparambil
MD
Zhi Halbach DO
Tiffany Trenda DO
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Young people experiencing their first psychotic episode wait an average of 72 weeks to seek treatment Other studies report that people
wait an average of 10 years before treatment
Half of all people living with a serious mental illness began experiencing symptoms before the age of 14 Three-quarters will develop a mental illness by age 24 So it is a ldquoyoung personrsquosrdquo illness during a prime time in their lives
For any health care condition early identifica-tion and treatment are critical The more we wait to treat a mental illness the more likely it is to become severe and for the individual to develop a substance use disorder as well So why is this happening
Building awarenessOne reason is that many people including youth are not aware of the symptoms of mental illness Teachers donrsquot receive much initial educa-tion about mental illnesses Limited access to treatment transportation insurance coverage and parent work schedules cause many to go without treatment
Minnesota schools do not require mental health education although there are mental health compo-nents in the National Health Education Standards However there are recommended free and low-cost programs available to schools including NAMI Minnesotarsquos free Ending the Silence program
Ending the Silence fits into 50-minute high school or middle school class periods and covers how common mental illnesses are signs and symptoms and the personal story of a young adult doing well in recovery Students receive resources to get help for themselves or a friend and information on how to fight the stigma of mental illnesses NAMI Minne-sota also developed a website for youth
In 2003 Minnesota became the first state to require continuing education for teachers on the key warning signs of early-onset mental illnesses in chil-dren and adolescents In 2013 trauma and autism were added These trainings help teachers under-stand the difference between willful behavior and symptomsmdashnot to have teachers diagnose students but to know when to talk to parents about a referral
In 2007 the Legislature funded school-linked mental health grants Grants are provided to mental health providers who then co-locate in the schools eliminating the barriers to treatment Funds pay for activities not funded by insurance such as collabo-ration with school support staff and teachers and for treatment of children who are uninsured and
underinsured Data from the first four years show that nearly half of the children had never received treatment and half of those had a serious mental illness While funding was doubled in 2013 only roughly 50 percent of schools have such a program
Reducing stigmaAnother issue is that parents and other adults work-ing with youth are not aware of the symptoms and frankly have stigmatizing attitudes Some believe that mental illnesses cannot occur in children and others believe that itrsquos just a ldquophaserdquo
We use slang words such as ldquocrazyrdquo and ldquonutsrdquo for people with mental illnesses but we donrsquot have slang words for other illnesses We never think to use the words ldquocourageousrdquo or ldquodeterminedrdquo to de-
scribe someone with schizo-phrenia or depression These are no ldquohot-dishrdquo or get-well card illnesses By harboring negative views we make it more difficult for people to seek treatment
Several strategies help to address this Mental Health First Aid an eight-hour class geared toward
youth or older adults increases mental health litera-cy It teaches people about the symptoms of mental illnesses and how to help when a person is in crisis or is suicidal The nation-wide class educates people about the signs and symptoms of mental illnesses
Another strategy is the Make It Ok campaign a one-hour presentation on how we talk and think about how mental illnesses impact peoplersquos lives Online videos of people with mental illnesses and their families present the impact of mental illnesses as well as personal stories of recovery The goal is to ldquomake it okrdquo to talk about mental illnesses
First Episode programs strive to identify psy-chosis early provide intensive treatment and help young people return to school or work so that they do not become disabled by their illness Early signs can include changing sleep patterns beginning to feel paranoid or having odd thought patterns hav-ing a hard time paying attention avoiding bathing and grooming and cognitive decline Efforts are underway to identify young people at closer to four weeks instead of 72 weeks But parents need to be watchful and not pass it off as a phase Funding was provided by the Legislature in 2015 For details visit the NAMI Minnesota website wwwnamihelpsorg
Progress and hopeWe are making progress that will lead to earlier identification and treatment but our work is not yet done Itrsquos important for everyone to learn about signs symptoms and what actions to take
Mental IllnessReaching out to youth in crisis
Pe RsPec t ive
Half of all people living with a serious mental illness began
experiencing symptoms before the age of 14
8 Minnesota HealtH care news September 2015
sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Ms Abderholden is the executive director of NAMI Minnesota (National Alliance on Mental Illness) a nonprofit organization that works to improve the lives of children and adults with mental illnesses and their families through its programs of education support and advocacy NAMI Minnesota offers more than 500 free classes and presentations and over 60 support groups each year
Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
September 2015 Minnesota HealtH care news 9
10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Zhi Halbach DO has joined Hutchinson Health as a family physician Halbach earned her doctor-ate in osteopathic medicine from the Des Moines University College of Osteopathic Medicine She is originally from Chaska and has moved back to Minnesota after completing her residency at St Lukersquos University Hospital in Pennsylvania Hal-bechrsquos special interests include womenrsquos health
preventive care and office procedures In addition Tiffany Trenda DO has joined Hutchinson Health as a pediatri-cian Trenda earned her doctorate in osteopathic medicine from Lake Erie College of Osteopathic Medicine in Pennsylvania and is moving back to her home state of Minnesota after completing her pediatric residency through Palmetto HealthUni-versity of South Carolina Trenda has spent time as a volunteer pediatrician in medically underserved communities in Nicaragua and El Salvador
Kevin Lindgren MD and Jaclyn Bailey MD have joined St Croix Orthopaedics as orthopedic surgeons Lindgren earned his medical degree from the Medical College of Wisconsin and completed an orthopaedic surgery residency at the University of Nebraska Medical CenterCreighton University where he received the Frank P Stone MD award for Outstanding Resident Lindgren completed his fellowship training at the University of Utah where
he specialized in hip and knee reconstruction and hip preservation surgery Bailey earned her doctor of medicine degree at the Univer-sity of Minnesota Medical School and completed an orthopaedic surgery residency at Grand Rapids Medical Education PartnersMichigan State University She completed her fellowship training in hand and upper extremity surgery at the University of California in San Francisco Lindgren will begin seeing patients at the Maplewood and Woodbury clinics in early September and at the new St Paul clinic when it opens later this fall Bailey will begin seeing patients at the Maplewood and Wyoming clinics at the end of September as well as at the new St Paul clinic
Samith Kochuparambil MD has joined Minne sota Oncology with the practice of medical oncology and hematology at the Minneapolis clinic Ko chu pa rambil earned his medical degree from the Madras Medical College Chennai India He completed a residency in internal medicine at the Medical College of Georgia where he received a STAR resident award and completed his fellowship in medical oncology and hematology at Mayo Clinic Kochuparambil specializes in treating pros-tate cancer kidney cancer bladder cancer multiple myeloma and general oncology
Peo Ple
September 2015 MINNESOTA HEALTH CARE NEWS 7
Kevin Lindgren MD
Samith Kochuparambil
MD
Zhi Halbach DO
Tiffany Trenda DO
For a lifetime of healthy beautiful skinFrom advice on the best daily skin care to the most challenging skin conditions we can help Trusted since 1949 our 20 Board-certified dermatologists are the Twin Citiesrsquo Skin Care Experts
dermatologyconsultantscom
EAGAN | SAINT PAUL | VADNAIS HEIGHTS | WOODBURY 6512091600
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
bullHighbloodpressurebullHighcholesterolbullAsmokerbullOverweightbullDiabetes
bull Familyhistoryofcoronaryarterydisease
bull Femaleandpost-menopausebullMaleandover40yearsofage
ContactthestudyteamoraskyourphysicianaboutSAMURAItolearnmore
IfsoconsiderjoiningSamuraindashaclinicalstudytoassessapotentialnewmigrainemedicationforpeoplelikeyouWersquorelookingforpeopleover18yearsofagetotakepartWersquodespeciallyliketohearfrommigrainesuffererswithatleastoneofthefollowingcardivascularriskfactors(But aLL migraine sufferers are welcome to contact us)
Young people experiencing their first psychotic episode wait an average of 72 weeks to seek treatment Other studies report that people
wait an average of 10 years before treatment
Half of all people living with a serious mental illness began experiencing symptoms before the age of 14 Three-quarters will develop a mental illness by age 24 So it is a ldquoyoung personrsquosrdquo illness during a prime time in their lives
For any health care condition early identifica-tion and treatment are critical The more we wait to treat a mental illness the more likely it is to become severe and for the individual to develop a substance use disorder as well So why is this happening
Building awarenessOne reason is that many people including youth are not aware of the symptoms of mental illness Teachers donrsquot receive much initial educa-tion about mental illnesses Limited access to treatment transportation insurance coverage and parent work schedules cause many to go without treatment
Minnesota schools do not require mental health education although there are mental health compo-nents in the National Health Education Standards However there are recommended free and low-cost programs available to schools including NAMI Minnesotarsquos free Ending the Silence program
Ending the Silence fits into 50-minute high school or middle school class periods and covers how common mental illnesses are signs and symptoms and the personal story of a young adult doing well in recovery Students receive resources to get help for themselves or a friend and information on how to fight the stigma of mental illnesses NAMI Minne-sota also developed a website for youth
In 2003 Minnesota became the first state to require continuing education for teachers on the key warning signs of early-onset mental illnesses in chil-dren and adolescents In 2013 trauma and autism were added These trainings help teachers under-stand the difference between willful behavior and symptomsmdashnot to have teachers diagnose students but to know when to talk to parents about a referral
In 2007 the Legislature funded school-linked mental health grants Grants are provided to mental health providers who then co-locate in the schools eliminating the barriers to treatment Funds pay for activities not funded by insurance such as collabo-ration with school support staff and teachers and for treatment of children who are uninsured and
underinsured Data from the first four years show that nearly half of the children had never received treatment and half of those had a serious mental illness While funding was doubled in 2013 only roughly 50 percent of schools have such a program
Reducing stigmaAnother issue is that parents and other adults work-ing with youth are not aware of the symptoms and frankly have stigmatizing attitudes Some believe that mental illnesses cannot occur in children and others believe that itrsquos just a ldquophaserdquo
We use slang words such as ldquocrazyrdquo and ldquonutsrdquo for people with mental illnesses but we donrsquot have slang words for other illnesses We never think to use the words ldquocourageousrdquo or ldquodeterminedrdquo to de-
scribe someone with schizo-phrenia or depression These are no ldquohot-dishrdquo or get-well card illnesses By harboring negative views we make it more difficult for people to seek treatment
Several strategies help to address this Mental Health First Aid an eight-hour class geared toward
youth or older adults increases mental health litera-cy It teaches people about the symptoms of mental illnesses and how to help when a person is in crisis or is suicidal The nation-wide class educates people about the signs and symptoms of mental illnesses
Another strategy is the Make It Ok campaign a one-hour presentation on how we talk and think about how mental illnesses impact peoplersquos lives Online videos of people with mental illnesses and their families present the impact of mental illnesses as well as personal stories of recovery The goal is to ldquomake it okrdquo to talk about mental illnesses
First Episode programs strive to identify psy-chosis early provide intensive treatment and help young people return to school or work so that they do not become disabled by their illness Early signs can include changing sleep patterns beginning to feel paranoid or having odd thought patterns hav-ing a hard time paying attention avoiding bathing and grooming and cognitive decline Efforts are underway to identify young people at closer to four weeks instead of 72 weeks But parents need to be watchful and not pass it off as a phase Funding was provided by the Legislature in 2015 For details visit the NAMI Minnesota website wwwnamihelpsorg
Progress and hopeWe are making progress that will lead to earlier identification and treatment but our work is not yet done Itrsquos important for everyone to learn about signs symptoms and what actions to take
Mental IllnessReaching out to youth in crisis
Pe RsPec t ive
Half of all people living with a serious mental illness began
experiencing symptoms before the age of 14
8 Minnesota HealtH care news September 2015
sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Ms Abderholden is the executive director of NAMI Minnesota (National Alliance on Mental Illness) a nonprofit organization that works to improve the lives of children and adults with mental illnesses and their families through its programs of education support and advocacy NAMI Minnesota offers more than 500 free classes and presentations and over 60 support groups each year
Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
September 2015 Minnesota HealtH care news 9
10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Young people experiencing their first psychotic episode wait an average of 72 weeks to seek treatment Other studies report that people
wait an average of 10 years before treatment
Half of all people living with a serious mental illness began experiencing symptoms before the age of 14 Three-quarters will develop a mental illness by age 24 So it is a ldquoyoung personrsquosrdquo illness during a prime time in their lives
For any health care condition early identifica-tion and treatment are critical The more we wait to treat a mental illness the more likely it is to become severe and for the individual to develop a substance use disorder as well So why is this happening
Building awarenessOne reason is that many people including youth are not aware of the symptoms of mental illness Teachers donrsquot receive much initial educa-tion about mental illnesses Limited access to treatment transportation insurance coverage and parent work schedules cause many to go without treatment
Minnesota schools do not require mental health education although there are mental health compo-nents in the National Health Education Standards However there are recommended free and low-cost programs available to schools including NAMI Minnesotarsquos free Ending the Silence program
Ending the Silence fits into 50-minute high school or middle school class periods and covers how common mental illnesses are signs and symptoms and the personal story of a young adult doing well in recovery Students receive resources to get help for themselves or a friend and information on how to fight the stigma of mental illnesses NAMI Minne-sota also developed a website for youth
In 2003 Minnesota became the first state to require continuing education for teachers on the key warning signs of early-onset mental illnesses in chil-dren and adolescents In 2013 trauma and autism were added These trainings help teachers under-stand the difference between willful behavior and symptomsmdashnot to have teachers diagnose students but to know when to talk to parents about a referral
In 2007 the Legislature funded school-linked mental health grants Grants are provided to mental health providers who then co-locate in the schools eliminating the barriers to treatment Funds pay for activities not funded by insurance such as collabo-ration with school support staff and teachers and for treatment of children who are uninsured and
underinsured Data from the first four years show that nearly half of the children had never received treatment and half of those had a serious mental illness While funding was doubled in 2013 only roughly 50 percent of schools have such a program
Reducing stigmaAnother issue is that parents and other adults work-ing with youth are not aware of the symptoms and frankly have stigmatizing attitudes Some believe that mental illnesses cannot occur in children and others believe that itrsquos just a ldquophaserdquo
We use slang words such as ldquocrazyrdquo and ldquonutsrdquo for people with mental illnesses but we donrsquot have slang words for other illnesses We never think to use the words ldquocourageousrdquo or ldquodeterminedrdquo to de-
scribe someone with schizo-phrenia or depression These are no ldquohot-dishrdquo or get-well card illnesses By harboring negative views we make it more difficult for people to seek treatment
Several strategies help to address this Mental Health First Aid an eight-hour class geared toward
youth or older adults increases mental health litera-cy It teaches people about the symptoms of mental illnesses and how to help when a person is in crisis or is suicidal The nation-wide class educates people about the signs and symptoms of mental illnesses
Another strategy is the Make It Ok campaign a one-hour presentation on how we talk and think about how mental illnesses impact peoplersquos lives Online videos of people with mental illnesses and their families present the impact of mental illnesses as well as personal stories of recovery The goal is to ldquomake it okrdquo to talk about mental illnesses
First Episode programs strive to identify psy-chosis early provide intensive treatment and help young people return to school or work so that they do not become disabled by their illness Early signs can include changing sleep patterns beginning to feel paranoid or having odd thought patterns hav-ing a hard time paying attention avoiding bathing and grooming and cognitive decline Efforts are underway to identify young people at closer to four weeks instead of 72 weeks But parents need to be watchful and not pass it off as a phase Funding was provided by the Legislature in 2015 For details visit the NAMI Minnesota website wwwnamihelpsorg
Progress and hopeWe are making progress that will lead to earlier identification and treatment but our work is not yet done Itrsquos important for everyone to learn about signs symptoms and what actions to take
Mental IllnessReaching out to youth in crisis
Pe RsPec t ive
Half of all people living with a serious mental illness began
experiencing symptoms before the age of 14
8 Minnesota HealtH care news September 2015
sue Abderholden MPH
NAMI Minnesota (National Alliance on Mental Illness)
Ms Abderholden is the executive director of NAMI Minnesota (National Alliance on Mental Illness) a nonprofit organization that works to improve the lives of children and adults with mental illnesses and their families through its programs of education support and advocacy NAMI Minnesota offers more than 500 free classes and presentations and over 60 support groups each year
Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
September 2015 Minnesota HealtH care news 9
10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Is now offering you a cure for the common coverage
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
all
+One low monthly fee of $75
+Unlimited primary care access
+A personal doctor focused on your wellness
+No deductibles copays or surprise bills
Is your health plan making you SICKIntroducing PrimaCare Direct
a CURE for the COMMON
COVERAGE
+
+
MULTICAREDIRECTPrimaCare
Direct
+
wwwprimacaredirectcom Call Liz Reiter at 763-785-3330
Join Us612-444-6600
PrimaCaredirectcom
Are you SICK ofFeeling like you work for your insurance company
Constantly paying higher premiums
Avoiding care because of high deductibles
Limited physician networks
Pay one low monthly fee ndash see our doctors all you want
September 2015 Minnesota HealtH care news 9
10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

10 Questions
What is diabetes Diabetes or diabetes mellitus is a chronic metabolic disease involving high blood glucose It occurs either when a body doesnrsquot produce enough insulin or when the body does not respond properly to the insulin it does produce Insulin is a hormone the body needs to convert sugar starches and other food into energy Diabetes is rapidly becoming a national epidemic The American Diabetes Association says diabetes affects 29 million people in the US alonemdashbut only three out of four individuals have been diagnosed There are three types of diabetes type 1 type 2 and gestational diabetes which oc-curs in some women during pregnancy
What is the difference between type 1 and type 2 diabetes Type 1 diabetes is sometimes called insulin-dependent or juvenile diabetes It usually occurs in children or young adults when the bodyrsquos immune system destroys insulin-making cells that control blood glucose Patients with type 1 diabetes need to take insulin injections their entire lives
Type 2 or adult-onset diabetes is the most common form and accounts for more than 90 per-cent of all diabetes With type 2 diabetes either a personrsquos pancreas stops producing enough insulin for the body to function properly or the cells in the body become insulin resistant Type 2 diabetes can often be treated with lifestyle changes or medications before insulin is needed
What is prediabetes Prediabetes is a condition in which blood glucose levels are higher than normal but not high enough to be classified as diabetes At this stage cells in the body are starting to become resistant to insulin The majority of patients who develop type 2 diabetes start out with prediabetes Some patients with prediabetes benefit from medication including metformin Others respond well to medications that control cholesterol such as statins or those that lower blood pressure The best option for indi-viduals with prediabetes however is to make lifestyle changes in diet and exercise before the condition becomes full-blown diabetes
What are the common symptoms of the onset of diabetes The most common symptoms of diabetes include the following
Some people with type 2 diabetes have very mild symptoms that may not be noticed Pregnant women with gestational diabetes may not have any symptoms Phy-
sicians can determine if the symp-toms are signs of diabetes with one of three tests A1C fasting plasma glucose or oral glucose tolerance
The initial diagnosis of dia-betes can be overwhelming
What advice do you have for people facing this news Remem-
ber that most cases of diabetes can be well managed Individuals who suspect they or someone they love has diabetes should seek help from a medical professional right away Together they can begin to make lifestyle changes that will have a positive impact on the illness This might include a healthier diet with more fruits vegetables lean meats and low-fat dairy products It also might include 30 to 60 minutes of physical activity or exercise at least five days a week Individuals with diabetes should also have regular check-ups so their phy-sician can manage important diabetes indicators
What advice might you give parents of diabetic children Parents of children with diabetes have special issues Managing the disease affects the entire family and special precautions must be made for those times when the child is away from his or her parents School teachers for example must be made aware of dietary restric-tions and signs of distress should your childrsquos blood glucose level get too low In addition the American Diabetes Association suggests that parents develop a
written care plan such as those developed under fed-eral disability law (a Section 504 Plan or an Individu-
alized Education Program) to ensure their child is given the same educational opportunities as others despite his
or her diabetes
DiabetesScott Benson MDDr Benson is a board-certified family medicine physician at the Apple Valley Medical Center
10 MInnESOTA HEAlTH CARE nEWS September 2015
bull Increasedthirstbull Frequenturinationbull Extremehungerbull Unexplainedweightloss(withtype1)bull Ketonesintheurinebull Fatiguebull Irritabilitybull Blurredvisionbull Slow-healingsoresbull Frequentinfectionsbull Tinglingpainornumbnessinhands
and feet (with type 2)
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
What are common treatments and medications for both types of diabetes Individuals with type 1 diabetes almost always need insulin injections to manage their blood glucose levels Some people with type 2 diabetes can manage their disease with lifestyle changes involving diet and exercise Others may need medi-cations to stimulate their pancreas inhibit the production of glucose from their liver or block enzymes that make the body more sensitive to insulin Some may need insulin injections to control their diabetes Today there are exciting new products on the market to measure blood glucose and deliver insulin including blood glucose meters and implant-able insulin pumps There also are effective insulin medications available that act faster and last longer than thoseusedinthepastMetforminisafrequentlyprescribedmedica-tion for patients with type 2 diabetes
Please discuss recommended diet and exercise habits for diabetics Patients with diabetes need to watch their diet and eat healthy foods such as fruits vegetables lean meats whole grains and low-fat dairy products They should eat more foods with fiber and fewer with fat and salt A physician can help to create a meal plan that fits into a personrsquos lifestyle Exercise is also important Patients with diabetes should get between 30 and 60 minutes of physical activity at least five days a week Individuals with diabetes should also keep their blood pressure and cholesterol levels within a normal range and have them checked by a physician regularly
What can happen to patients who do not manage their diabetes Diabetes is serious and can lead to a number of complications including cardiovascular problems such as ischemic heart disease high blood pressure stroke and peripheral arterial disease It also can cause kidney disease and diseases of the nervous system such as neuropathy People with diabetes are more likely to develop infections slow-healing wounds hearing loss and
gum disease They also can develop eye problems such as glaucoma cataracts and diabetic retinopathy In extreme cases diabetes can lead to kidney transplants blindness or amputation of feet and legs
What does the future of diabetes research hold Recent scientific developments to address diabetes include a ldquosmart insulinrdquo patch that imitates the bodyrsquos beta cells by sensing blood glucose levels and releasing insulin Research is being conducted to develop new medications to learn about rare forms of diabetes caused by gene mutations to study the link between obesity and diabetes and to understand how to reduce cardiovascular complications in people with type 1 diabetes Medical device companies are conducting clin-ical trials on a closed loop insulin delivery system also known as an artificial pancreas This device links a continuous glucose monitor to an insulin pump in order to deliver insulin automatically
September 2015 MInnESOTA HEAlTH CARE nEWS 11
Most cases of diabetes can be well managed
Yoursquove always done things your own way And you still can with UCare for SeniorsSM a Medicare health plan that brings together great benefi ts at a great price
UCare for SeniorsSM lets you choose from plans that cover prescription drugs travel eyewear dental fi tness programs like Healthways SilverSneakersreg Fitness and more There are low or no co-pays for primary care visits with most plans And yoursquoll get to talk to a real person 247 when you call customer service Itrsquos just what yoursquod expect from health care that starts with you
Learn more about the benefi ts of UCare for Seniors in our new eGuide to Medicare at ucareplansorg Or call (toll free) 1-877-523-1518 (TTY) 1-800-688-2534 8 am to 8 pm daily
UCare for Seniors is an HMO-POS plan with a Medicare contract Enrollment in UCare for Seniors depends on contract renewal copy2015 UCare H2459_101512 CMS Accepted (10202012)
YOUrsquoRE STILL IN THIS THING TOGETHER WErsquoVE BEEN EXPECTING YOU
UC693 2015 Boomer MPP MN Health Care News_PeaceWeddingindd 1 82815 355 PM
Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Insurance
Open enrollment is just around the corner for people buying health care insurance under the Affordable Care Act and for employees facing annual renewals under their compa-
ny plans Picking the best coverage and asking the right questions is always challenging but for diabetics and those concerned about becoming diabetic it can be even more daunting
Thatrsquos because medical expenditures for people diagnosed as dia-betic can run 23 times higher than for non-diabetics according to the American Diabetes Association (ADA) Those costs make it even more important to pick the right plan The following guidelines are import-ant for diabetics and for all consumers of health care insurance
Costs of diabetesThe ADA reports that one in five US health care dollars is spent caring for the 29 million Americans diagnosed with diabetes In a study released in 2013 the ADA reported that people with diag-nosed diabetes incurred average annual medical expenditures of $13700 most of which ($7900) was attributed to their diabetes Most of those expenditures (90 percent) went to
bullHospital inpatient care 43 percent
bull Prescription medications to treat complications 18 percent
bullAnti-diabetic agents and diabetes supplies 12 percent
bullPhysician office visits 9 percent
bullNursingresidential facility stays 8 percent
If yoursquore in the market for a new health care plan yoursquoll need to consider all of these factors The least expensive plan could end up costing you more after you factor in costs for medications and testing supplies
Tips for selecting insuranceHealth care consumers face a world of new options including sub-sidies tax credits and new rules for MinnesotaCare and Medical Assistance Traditionally most consumers obtained insurance under group plans from their employer limiting their choices and services Employees and private consumers may now find more options for doctors hospitals clinics prescriptions and price
As a consumer you should view health insurance as an investment in your health and financial future Start by reading the fine print of both group plans and individual plans How do they differ with regard to your medications How do your yearly expenses for durable med-ical equipment test strips and other supplies affect your deductibles or maximum out-of-pocket expenses Does your current plan offer discounts to health clubs Are pre-diabetic screenings covered
Do your homeworkReady to start your research One place you can go to is a private exchange which is a marketplace that offers multiple plans multi-ple carriers and possibly other types of insurance such as dental vision and life insurance This marketplace may offer more options than traditional group plans but it can come with limitations Not all insurance products are available in these exchanges and the private exchange also does not allow consumers to use any public subsidies should they qualify for them
Diabetes care
Minimizing the costsBy Matthew Wicklund
12 MINNESOTA HEAlTH CARE NEwS September 2015
伀渀氀礀 㜀㔀
吀䴀
䄀洀瀀氀椀昀椀攀搀 䌀愀瀀琀椀漀渀攀搀 吀攀氀攀瀀栀漀渀攀
一攀瘀攀爀 洀椀猀猀 愀渀漀琀栀攀爀 眀漀爀搀 漀昀 礀漀甀爀 瀀栀漀渀攀 挀漀渀瘀攀爀猀愀琀椀漀渀猀 吀栀攀 䌀氀愀爀椀琀礀글 䔀渀猀攀洀戀氀攀∡ 椀猀 愀 焀甀愀氀椀琀礀 挀愀瀀琀椀漀渀攀搀 瀀栀漀渀攀 眀椀琀栀 琀栀攀 戀攀猀琀 愀洀瀀氀椀昀椀挀愀琀椀漀渀 愀瘀愀椀氀愀戀氀攀 䄀渀 㠀 琀漀甀挀栀猀挀爀攀攀渀 挀愀渀 攀渀氀愀爀最攀 琀攀砀琀 愀猀 渀攀攀搀攀搀 䄀琀 琀栀攀 氀漀眀 瀀爀椀挀攀 漀昀 㜀㔀 Ⰰ 礀漀甀 挀愀渀琀 愀昀昀漀爀搀 琀漀 瀀愀猀猀 琀栀椀猀 漀昀昀攀爀 甀瀀䘀爀攀攀 䤀渀猀琀愀氀氀愀琀椀漀渀 刀攀焀甀椀爀攀猀 戀漀琀栀 氀愀渀搀氀椀渀攀 愀渀搀 椀渀琀攀爀渀攀琀 挀漀渀渀攀挀琀椀漀渀 䘀爀攀攀 挀愀瀀琀椀漀渀椀渀最 猀攀爀瘀椀挀攀 琀栀爀漀甀最栀 琀栀攀 䘀䌀䌀
圀漀爀搀猀䴀愀琀琀攀爀
㠀 ⤀ 㠀㔀ⴀ㘀㜀㔀㠀
䘀椀渀搀 琀栀攀 䔀渀猀攀洀戀氀攀 愀琀眀眀眀栀愀爀爀椀猀挀漀洀洀挀漀洀眀漀爀搀猀
吀爀礀 漀甀琀 漀甀爀 瀀爀漀搀甀挀琀猀 昀漀爀 礀漀甀爀猀攀氀昀 嘀椀猀椀琀 漀甀爀 猀栀漀眀爀漀漀洀 㔀㔀㔀 吀攀挀栀渀漀氀漀最礀 䐀爀Ⰰ 䔀搀攀渀 倀爀愀椀爀椀攀Ⰰ 䴀一 㔀㔀㐀㐀
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
Minnesota residents may visit the MNsure public exchange to see whether they qualify for Medicaid MinnesotaCare or Qualified Health Plans (QHP) Consumers who qualify for a QHP might be eligible for tax credits cost sharing or premium relief Qualifications are based on a combination of income access to employer-sponsored plans and residence
The public exchange is similar to the private exchange where there can be multiple insurance companies offering products and some choice in plan offerings You may pick a deductible co-insurance and plan or network that is best for you Unlike a private exchange you can use pre-mium or tax credits (should you qualify) on this site like the private exchange not all carriers and plans are offered on a public exchange
Consumers may also go directly to the open market visiting the websites of insurance companies to shop for plans available in their area
Making sense of dollars and centsRegardless of your search strategy think beyond the monthly price tag You monthly premium is important but consumers need to make sure that they get what they pay for look at your needs and future plans and try to maximize the benefits while weighing the cost of premiums with the costs of deductibles and co-pays
I ask my clients several questions to help identify the best plan for them For example I ask how much money they could spend if something bad were to happen to them or to their family The pur-pose is to find out how high of a deductible that client could afford If you pick a plan based on the lowest premium you will likely have a very high deductible which is the portion of health coverage for which you are responsible If you have a $2000 deductible you will pay the first $2000 in medical expenses before the insurance company pays anything So if something bad happens to you or your family can you write a check for $2000
The next question is about co-insurance which means payments split between the insured and the insurance company You might have a plan with a $2000 deductible and 20 percent co-insurance what that means is once you have paid $2000 towards your health care the insurance company will cover 80 percent of expenses while you pay the remaining 20 percent Most people do not like unexpected bills so itrsquos worth seeing whether raising the premium a bitmdashperhaps by $10 per monthmdashmight reduce the co-insurance and save you money in the long run
Consumers also need to look at the Max out of Pocket (MOOP) which represents the most they will spend in one plan year If your plan has a Max Out Of Pocket of $6500 you will spend that amount in one plan year after which the insurance company will pay for all covered medical expenses at 100 percent There are plans that offer a deductible and a reduced price for services until you reach your MOOP
For diabetics this can be very important You might select a plan with a monthly premium of $500 a deductible of $1000 dollars co-insurance of 20 percent and a Max Out Of Pocket of $6500 per year This plan might appear to be the best for the client based solely on the monthly price But compare this to a plan with a
higher monthly premium of $590 a deductible of $3000 no co-in-surance and a Max Out Of Pocket of $3000 per year By choosing
the higher monthly premium plan you could save $2420 per year
People with type 1 or type 2 diabetes should also look for plans offering a discount on health club memberships Most plans today offer up to $20 off your monthly bill if you use the membership 12 times per month (Usage and reimbursement requirements vary by plan)
It is also important to look at the drug formu-lary to see if your insulin or medication is cov-ered Drug formularies change from year to year so check this regularly You should also see if you could obtain discounts directly from the manufac-turers of testing supplies
ConclusionIt is important to look at health insurance as an investment look at your wants and needs in insurance and maximize your premium co-pay and deductible Allow your money as well as the insurance to work for you and refer questions to a licensed health insurance broker or to your state exchange
Matthew Wicklund is a health insurance broker with Contego Capital Insur-ance Group MNsure and Medicare certified he focuses on individual family and Medicare clients
Think beyond the monthly
price tag
September 2015 MINNESOTA HEAlTH CARE NEwS 13INFORMATIONJob Number 245-13124 Trim 4rdquo x 525rdquo Modifi cation Date October 22 2014 233 PM
Client HealthPartners Bleed Output Date 102214
Description MN Health Care News Live Page 1
File Name 245-13124 Medicare [Carpenter][4x525]_3_
SIGN-OFF[shyshyshyshy] CD Peter Tressel
[shyshyshyshy] AD Anne Taylor
[shyshyshyshy] CW Terry Thomas
[shyshyshyshy] AS Mark Jenson
[shyshyshyshy] AM Linda Gogolin
[shyshyshyshy] PM Krista Kraabel
[shyshyshyshy] PA Tera Gilmore
Notes
3
Can I keep my doctor
Deductibles
H2462_77617 Accepted 01192014 HealthPartners is a Cost plan with a Medicare contract Enrollment in HealthPartners depends on contract renewal copy2013 HealthPartners
Deductibles
Can I keep my doctor
Deductibles
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Visit healthpartnerscommedicare
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
Let the friendly helpful people at
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
HealthPartners guide you to the perfect
plan to meet your needs and budget
plan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Deductiblesplan to meet your needs and budget
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
Medicare is less complex
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
if you simply choo
se the
best-built plan
best-built plan
best-built plan
OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

OptOmetry
ldquoWhat are we doing here Was I competing in slalom or GS (giant slalom)rdquo Adam asked while getting into the car Alarm bells were going off for Adamrsquos mom ldquoWas I
competing in slalom or GSrdquo he asked again repeatedly en-route to Childrenrsquos Hospital
Twelve-year-old Adam an avid downhill skier had fallen and suffered a concussion When his teammates found him he wasnrsquot making any sense Adam is one of the millions of adolescent athletes
who suffer concussions Contact sports such as football hockey basketball soccer lacrosse volleyball and wrestling are among those posing the highest risk for concussion
What is a concussionA concussion is a brain injury caused by a direct blow to the head or by any other force that can be transmitted to the head Ultimately this results in axonal (nerve) injury and lack of energy (glucose) to brain cells resulting in neurological symptoms Symptoms of a concussion are confusion headaches blurred or double vision nausea dizziness fatigue sensitivity to light and noise dazed feelings difficulty concentrating memory loss irritability and sleep disturbances Concussion symptoms may take days to be recog-nized underscoring the importance for anyone suspected of having a concussion to be evaluated by a medical professional
Diagnosis of concussion may be difficult and underreported as can be seen from the wide range of reported cases The Centers for Disease Control and Prevention (CDC) estimates between 17 million and 38 million sports-related concussions per year in the US School-age athletes may or may not have access to a medical professional who can assess whether a concussion has occurred and may rely on a trainer coach or even parents who may or may not be trained to identify concussions Some athletes may report feeling ldquofinerdquo and deny symptoms in order to remain in the game Unfortu-nately reliable valid cost-effective concussion testing methods that can be used by all athletes coaches and trainers have been difficult to find and standardize
Vision as the key in sideline concussion screeningIt would seem that vision would almost always be affected by con-cussion because vision is so embedded in the brain Vision involves more than 30 areas of the brain and is responsible for more than 70 percent of sensory processing The King-Devick Test used for years by eye care professionals is now used on the sidelines to screen athletes for concussions Administered to athletes in the preseason in less than two minutes by non-medical professionals the test includes verbally reading numbers in columns and rows Later if a concus-sion is suspected the test is administered in the same manner as the baseline testing If the response time is slower a concussion is highly
Sports- related
concussionsYour eye doctor may see the signs
By Jessica L Schara OD
14 MInneSoTA HeALTH CAre neWS September 2015
Psychiatric Care evolved888-9-prairie prairie-carecom
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
September 2015 MInneSoTA HeALTH CAre neWS 15
likely The science behind this test is that saccades or fine reading eye movements take place in over nine areas of the brain
After a concussionVisual symptoms that may occur after a concussion include light sensitivity double vision blurred vision (affecting nearby objects more than distant objects) focusing difficulty (such as reading and looking up to a blurred board and vice versa) headaches above the brow tracking diffi-culty skipping lines when reading omitting words illusions of movement decreased speed of processing and comprehension peripheral vision defects and balance and gait disturbances due to visual processing distortions
Vision can be blurred due to changes in nearsightedness farsightedness or astigmatism after a concussion which may be transient or may remain after healing Simple changes in spectacle prescription may be enough to improve the function of concussion patients allowing them to return to school or work
When we read our eyesrsquo internal focusing system is stimulated our eyes converge (both eyes turn inward as though looking towards our nose) and the pupil constricts The focusing system called ac-commodation can be disrupted after concussion and reading glasses are commonly prescribed to alleviate near vision blur eyestrain
headaches and visual fatigue over- or under-convergence can be affected after a concussion which can cause double vision eyestrain covering of an eye while reading and headaches Prisms andor vision therapy may be beneficial to patients with convergence issues
Pupils may enlarge after concussion causing increased light sensitivity or photophobia Tinted lenses may help
Tracking issues called pursuit dysfunction may be im-paired and may cause difficulty in tracking a moving object or reading Saccadesmdashfast fine-eye movements needed when reading from word to wordmdashmay be affected post-concussion causing patients to lose
place when reading skip lines or words and reread for comprehension Peripheral vision can be affected after a concussion which can cause part of peripheral vision to be ldquomissingrdquo This can be difficult for patient activities such as driving reading and playing sports (people may not see a ball coming at them or another player from the side view of the field)
How we move and navigate through space is determined in large part by visual processing eighty percent of fibers from the optic nerve go to the visual cortex however 20 percent will go to the su-perior colliculus part of the midbrain Those 20 percent are consid-ered ambient visual processing which can affect balance posture
Sports-related concussions to page 32
Vision is critical in concussion diagnosis
and management
Gambling problems can only be solved if you have the conversation Reach out and ask for help before you lose what is really important
Call 1-800-333-HOPEBefore you lose what really matters
GetGamblingHelpcom
Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Wound Care
Cuts and abrasions to the feet and lower extremities are com-mon occurrences in everyday life Usually these wounds heal quickly on their own with minimal intervention and basic
wound care including keeping the area clean and dry with perhaps a light bandage and some antibiotic ointment However wounds can sometimes turn into ulcers defined as wounds with a full thickness depth through the skin and a tendency for slow healing In order for these lower extremity ulcerations to heal the underlying causative factors need to be addressed Common causes of lower extremity ulcerations include venous insufficiency arterial insufficiency diabe-tes trauma or combinations of these factors
We will attempt to address some of the basic characteristics of these types of wounds and some of the treatments that may be required for healing
Venous insufficiency and ulcerationThese wounds sometimes occur due to problems with the veins that take the blood flow back up toward your heart This is known as venous insufficiency or venous reflux disease and may be related to weakened vein walls or damaged valves within the veins Patients with venous ulcerationmdashulcers related to restricted venous blood flowmdashmay have a history of venous blood clots varicose veins leg swelling or obesity Wounds themselves typically appear on their medial or lateral anklebones and can be very painful The surround-ing calf may be swollen and the skin may be stained red or brown and scaly in texture
In addition to local wound care treatment may include compres-sion of the legs with either a medicated bandage or compression hose Your primary care provider may refer you to a vascular specialist who may evaluate your venous blood flow with additional testing such as ultrasound If the ultrasound shows significant venous insufficiency in the superficial veins sometimes minimally invasive treatment of the bad superficial veins with some combination of laser or radiofrequen-cy ablation surgical removal or injection may be in order
In laser or radiofrequency ablation a catheter is placed into the legrsquos greater or small saphenous vein The abnormal refluxing vein is then taken out of circulation by clotting if off with laser or radiofre-quency energy Surgical vein removal may entail making some small incisions over the squiggly dilated superficial varicose veins which are often branches off the legrsquos main superficial saphenous veins Smaller branch veins can sometimes be handled with injection of medication that clots narrows and scars the vein shut (sclerother-apy) Often these procedures can be done with local anesthesia and minimal sedation in an outpatient setting
Arterial insufficiency and ulcerationThese wounds are due to poor blood flow down the legs Those at risk include smokers or patients with diabetes hypertension (high blood pressure) hyperlipidemia (high lipid levels) or kidney failure Patients with poor arterial circulation may have hairless skin that is very shiny tight and dry Wounds may appear on the toes between the toes or on the feet and may be very slow to heal Typically the
Your feet and lower extremities
Common risks and complicationsBy Nicole A Bauerly DPM FACFAS
and Michael Hu MD FACS
16 MInneSOTa HealTH Care neWS September 2015
Do You Suffer from 3 to 8 migraineS per month
radiant Clinical researchwwwradiantresearchcom
Contact the study team or ask your physician about SAMURAI to learn more
If so consider joining Samuraindasha clinical study to assess a potential new migraine medication for people like you Wersquore looking for people over 18 years of age to take part Wersquod especially like to hear from migraine sufferers with at least one of the following cardivascular risk factors (But aLL migraine sufferers are welcome to contact us)
bullHigh blood pressurebullHigh cholesterolbullA smokerbullOverweightbullDiabetes
bullFamily history of coronary artery disease
bullFemale and post-menopausebullMale and over
40 years of age
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
wounds may have a ldquopunched outrdquo appearance with a wound bed that may be pale or contain some dead tissue
The wounds may initially be small but if they are slow to heal or worsening and enlarging you must see your primary care provider He or she may refer you to a vascular specialist who will evaluate your blood flow down the legs and may order further testing to evaluate or improve blood flow which is important for healing Interventions to improve the blood flow down the leg may include same-day minimally invasive techniques including
bull angioplasty opening the artery with a balloon catheter placed through the skin (percutaneously) into the leg artery usually from one of the groin arteries
bull Stenting opening and holding the artery open with a cylindrical metal mesh tube also placed percutaneously if angioplasty is not enough or if the amount of narrowing is more extensive
bull atherectomy opening the artery with a percutaneously placed catheter that can cut and drill through narrowing in the arteries
Or in more severe cases
bull leg bypass surgery making incisions in the leg and sewing leg veins or artificial grafts into the arteries above and below the blockages allowing the blood flow to go around or to bypass more extensive blockages This type of surgery requires a hospital stay
Diabetic woundsDiabetic patients have up to a 25 percent lifetime risk of developing a foot ulcer Diabetic foot ulcer complications are the most com-mon cause of nontraumatic lower extremity amputations in the industrialized world These types of foot ulcers can form due to a combination of factors that include a lack of feeling in the foot (neuropathy) poor circulation foot deformities irritation (such as friction or pressure from shoes) and trauma Patients who have had diabetes for many years can develop a reduced or complete lack of
ability to feel pain in the feet due to nerve damage caused by elevated blood glucose levels over time The nerve damage often can occur without pain and you may not even be aware of the problem Keys to prevent-ing diabetic foot ulcers include
checking your feet daily avoiding going barefoot in or out of the home achieving good control of your diabetes to prevent further nerve and circulation damage and seeing a physician (primary and podiatric) on a regular basis If you develop a diabetic foot ulcer it is important to seek medical attention immediately Initial treatment may include local wound care offloading of the wound to decrease pressure vascular studies to evaluate your blood flow and other necessary tests depending on the severity of the wound
Your feet and lower extremities to page 19
September 2015 MInneSOTa HealTH Care neWS 17
Wounds to the feet are common
occurrences
This device should be worn at night and is not intended to replace the need to properly test your blood sugar levels with a blood glucose meter
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
National Recovery Month
Each September the Substance Abuse and Mental Health Services Administration (SAMHSA) works to spread the word that behavioral health is essential to health that prevention works and treatment is effective and that people can and do recover from mental andor substance use disorders
In 2013 about 438 million adults or 185 percent of the population had experienced a mental illness in the past year according to SAMHSA And about 216 million people age 12 or older were classified with a substance dependence or misuse disorder However many of these people are not getting the treatment they need
People facing mental and substance use disorders have the best chance of recovery when they realize they are not alone in how they feel Meeting with others who have ex-perienced recovery and being supported by their families peers and schools can bring hope and a sense of belonging to support long-term recovery
18 Minnesota HealtH care news September 2015
Calendar Sept-Oct 2015SEP9 Nutrition for Managing Lupus
The Lupus Foundation of Minne-sota hosts this free class to teach people with lupus and other chronic conditions how better nutritional choices can help manage inflamma-tion caused by these conditions Call Sandy at (952) 746-5151 to register by September 8
Wednesday Sept 9 12ndash1 pm Maple Grove Library 8001 Main St N Maple Grove
14 New Moms Support GroupPark Nicollet hosts this free support group
for women who have recently had a baby and are experiencing stress anxiety sadness or are feeling overwhelmed Join other women experiencing similar feelings for support and healing Registration is not required Call (952) 993-3307 for more information or other meeting dates
Monday Sept 14 12ndash1245 pm Park Nicollet Clinic 7th Floor 3800 Park Nicollet Blvd St Louis Park
16 Caregiver Support GroupNorth Memorial Medical Center hosts this
free support group for care partners of stroke survivors Come learn more about how to care for your loved one and feel support from others who understand Registration is not required Call (763) 581-3650 for more information or other meeting dates
Wednesday Sept 16 2ndash3 pm North Memorial Medical Center Plaza Level 3300 Oakdale Ave N Robbinsdale
28 Diabetes Insulin Pump Support GroupHealthEast hosts this free support
group for individuals who are interested in information about insulin pumps or are already using one Come learn more about how insulin pumps work and if one is right for you Call Diane at (651) 232-6322 to register
Monday Sept 28 6ndash730 pm Woodwinds Health Campus 1925 Woodwinds Dr Woodbury
OCt6 Grief amp Loss Support GroupThe Aliveness Project hosts this
free support group for people with HIV or their partners who have lost a loved one Come gain support and learn new strategies on how to cope Call Becca at (763) 253-2110 to sign up or learn about other meeting dates
tuesday Oct 6 1ndash2 pm the Aliveness Project Community Room 3808 Nicollet Ave S Minneapolis
10 Food Allergy Resource FairThe Food Allergy Support Group of
Minnesota hosts this free resource fair featur-ing allergy-friendly foods and products allergy safety information and doctors who will be available to answer questions No registration required but there is a $5 suggested donation per family Visit wwwfoodallergysupportmnorg for more information
Saturday Oct 10 9 amndash12 am Eisenhower Community Center 1001 Hwy 7 Hopkins
14 Colorectal Cancer Support GroupAllina Health hosts this support group for
those living with colorectal cancer and their caregivers Come to meet others on a similar path for support and to learn methods for coping with the physical and emotional impact of living with these cancers No registration required Call (763) 236-6060 with questions or to learn about other meeting dates
Wednesday Oct 14 6ndash730 pm Virginia Piper Cancer InstitutemdashMercy Hospital 11850 Blackfoot St NW Suite 130 Coon Rapids
17 Huntingtonrsquos Disease Support GroupThe Minnesota Chapter of the Huntingtonrsquos
Disease Society of America offers this free support group for those affected by Hunting-tonrsquos Disease Come make new connections in a safe caring environment Call Jessica at (612) 371-0904 or email jmarsolekhdsaorg for more information
Saturday Oct 17 1030 amndash1230 pm Oak Grove Lutheran Church 7045 Lyndale Ave S Richfield
SEP29 Mental Health First Aid
The National Alliance on Mental Illness hosts this free class to teach the basic skills needed to help a person who is experiencing a mental health problem or crisis Come learn how to identify under-stand and respond to signs of a mental illness and substance abuse disorders Registration required Call Kara at (651) 645-2948 ext 114 tuesday Sept 29 830 amndash530 pm Oak Grove Presbyterian Church 2200 W Old Shakopee Rd Bloomington
Send us your newsWe welcome your input If you have an event you would like to submit for our calendar please send your submission to MPPCalendar 2812 E 26th St Minneapolis MN 55406 Email submissions to amarlowmppubcom or fax them to (612) 728-8601 Please note We cannot guarantee that all submissions will be used CME CE and symposium listings will not be published
Americarsquos leading source of health
information online
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
Traumatic foot woundsTraumatic foot wounds are a common entity encountered by health care professionals The severity of these can vary widely and can include minor abrasions lacerations foreign bodies in the foot lead-ing to puncture wounds open fractures machinery injuries and degloving injuries where the skin is complete-ly removed from the underlying tissue Given that the feet are a weight-bearing surface and in con-stant ground contact preventing infection in open wounds of the feet is important to maintaining the ability to walk and bear weight local wound care is important to prevent infection antibioticsmdashtak-en orally or applied topicallymdashmay be necessary to prevent infection For puncture wounds and for more serious traumatic foot wounds in general it is important to make sure that your tetanus status is up to date Depending on wound severity surgery may be necessary to remove any devitalized (dead) tissue and to thoroughly irrigate and clean the area You should seek medical attention for deep puncture wounds or more serious trau-matic foot wounds in general but especially if there are any signs of the wound being infected Those signs of infection might include increased redness drainage swelling or pain
ComplicationsThe keys to successful wound healing include prompt recognition of the wound accurate diagnosis of the causative factors appropriate wound care and timely referral to a wound specialist or clinic while the wound is still small and easily treated Cooperation and com-mitment to a wound plan are vitally important especially in more difficult or extensive wounds Despite all the resources available in most modern hospitals and wound clinics late treatment of exten-
sive leg wounds especially in patients with multi-ple medical issues still can lead to problems with infection chronic pain and disability extended hospital stays for multiple procedures or opera-tions and in extreme cases amputation or death
ConclusionCuts abrasions and wounds to the feet are common occurrences and usually heal quickly However depending on the severity of the wound and your other underlying medical issues these injuries can become more serious Close observation and prompt evaluation of any slowly healing wounds by your medical providers is key to suc-cessful healing and prevention of more serious complications
nicole a Bauerly dPM FaCFaS is chief of the Department of Podiatry Surgery and assistant program director of the Podiatric Surgery Residency Program at Hennepin County Medical Center (HCMC) She is board-certified in foot surgery and reconstructive rearfootankle surgery Michael Hu Md FaCS is a vascular surgeon at HCMC His professional interests include aneurysm disease peripheral arterial and venous disease and carotid disease
Nerve damage often can occur without pain
September 2015 MInneSOTa HealTH Care neWS 19
Your feet and lower extremities from page 17
wwwstcroixorthocom
Tim Jackson has been a dairyman most of his life As the years passed his knees
wore out ldquoTwo years ago they were getting so bad that I could hardly navigate
anymorerdquo said Tim He began to get depressed because it was too painful to continue
his work and enjoy an active lifestyle Tim sought help from providers and had some
treatment before nding St Croix Orthopaedics (SCO) His treatment journey with SCO
helped him nd the solution he was looking for ldquoIt was a positive experience from the
beginningrdquo said Tim ldquoHe (the surgeon) painted a whole other picture for my liferdquo
Appointments Online or call 651-439-8807 | Multiple clinics in Minnesota and Wisconsin
Watch Timrsquos story online Go to httpbitly183Vlpc
B I L A T E R A L K N E ER E P L A C E M E N TH E L P S F A R M E RG E T H I S
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
About the RoundtableMinnesota Physician Publishingrsquos forty-third Minnesota Health Care
Roundtable examined the topic of The New Face of Health Care Expanding medical professional
relationships Seven panelists and our moderator met on April 23 2015 to
discuss this topic The next roundtable on Nov 12 2015 will address Behavioral health integration
New pathways to care
Mr starnes today we will talk about ex-panding medical professional relationships which can take many forms in somemdashan oncologist working with a radiologist for examplemdashthere is a well-defined protocol for communication and continuity of patient care We want to focus more on medical doctors working with medical professionals who are not Mds letrsquos start with a defini-tion What is a medical professional
Dr Hu It has to do with a degree of specif-ic medical training in some specific field as well as professional interest It has to involve some aspect of medicine however broadly you want to define that
Dr Sawyer In our institution we not only train chiropractic doctors but acupunc-turists and massage therapists and our definition of massage therapy is therapeutic massage We very much consider them to be medical professionals
Dr Desai When you define a medical pro-fessional you get into a lot of political dis-cussions and some people get their hackles up Folks who have gone through medical school or dental school or chiropractic school sometimes show an ingrained defen-siveness based on the school theyrsquove attend-ed and the education theyrsquove had Irsquom part of a multidisciplinary practice so I work very closely with behavioral health special-ists psychologists licensed social workers physical therapists and others Oftentimes I work with chiropractors or other medical professionals as well as with acupunctur-ists The value of that is undeniable
Mr Hustvet I like the term ldquohealth care pro-fessionalrdquo Our current discipline is really pushing to alleviate some of the problems of having a limited number of physicians Would I take it personally if I were called a ldquomid-level providerrdquo I would really look more at what Irsquom able to do for the patient Am I able to meet a need in a timely fash-ion Am I able to assist and provide care where maybe there would have been a delay
Mr Starnes As science and training expands many health care professionals have the ability to make frontline diagnoses of conditions that could be shared with physicians Any examples of the ways in which these individuals could work with physicians
Dr Gulon Dental schools now include the team-based approach to care as part of the
curriculum Dentists are trained to not only work on prevention but disease treatment as wellmdashand like our physician colleagues to deliver care over the lifetime of our patients Itrsquos obvious that everything that goes into the mouth pretty much enters all the pathways of all the basic systems of the body Understanding that and applying dis-ciplines and approaches to care that impact andor prevent it are going to be useful in at least the teamwork process in health care
Mr Starnes Letrsquos talk about expanding the relationships between health care professionals and the benefits this can bring What are some of the existing barriers to this more collabora-tive approach
Dr Sawyer The biggest barriers really have to do with payment and the incentives in
payment When a patient walks in our door we manage that patient in a silo and we arenrsquot thinking of other providers that might be able to have a better impact or an additional impact on that patient
Mr Wingrove A lot of us are still getting to know each other and I think that is one of the keys to having successful interdisciplin-ary approaches Wersquore being forced now to look outside of our own box and collabo-rate with other people In the long run I think thatrsquos going to serve the patients well Itrsquos probably something we should have done a decade ago
Dr Desai Patient ownership is an area that we tend to ignore Itrsquos the most uncomfort-able of the areas to discuss The cultural issues surrounding patient ownership are the ones that are the hardest conversations to have
Dr Gulon I see this as an opportunity not as a barrier First of all 40 percent of the population seeks dental care in any given year Fifteen percent of those people donrsquot see a physician and thatrsquos a problem If wersquore presented with conditions in which we could be a source of referral to the physicians through appropriate screening whether itrsquos hypertension which we do rou-tinely oral cancer screening examinations diabetes screening or sleep apnea screen-ing there are windows andor opportuni-ties to collaborate at a higher level with our physician colleagues
Mr Starnes Are we are going to foster better relations between provider types if the consumers themselves broaden their approach to health
Mr Hustvet Changing a patientrsquos view on taking ownership of their health isnrsquot going to happen in a five-minute conversation at a physicianrsquos office It probably wonrsquot happen even after three or four five-minute conver-sations at the physicianrsquos office
Dr Hu Say you need to get a CT scan and an MRI Each costs different amounts at different places whether itrsquos inpatient outpatient or in hospitals Therersquos very little transparency so even if they want to be involved in making those decisions in a cost-effective manner based on their insur-ance or deductible they canrsquot do it
the new face of health care
Expanding medical professional relationships
20 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
Mr Johnson We all need to provide education to our patients about preven-tive care and following up with pre-ventive checkups because it canrsquot be a burden for just one profession
Dr Hu Irsquom a specialist a vascular surgeon so my view may be skewed towards specialty care Again wersquove been siloed for a long time We have radiologists who do angiograms and surgeons who do surgery but those barriers have changed and everyone wants to protect their turf I think the financial barriers are the first hurdle and probably the biggest hurdle in order to build a multidisciplinary team with a common goal
Mr Starnes We need to better understand the levels of training of different kinds of providers How early in onersquos health care career should this learning begin
Mr Johnson In the physical therapy program it happens early and for good reason Everybody is in learner mode I think it needs to be a little bit more robust actually so training would con-tinue beyond those initial few years
Mr Starnes What about health care pro-fessionals who are well into their careers and well removed from the academic or school environment
Mr Hustvet Sometimes itrsquos directed by a physician above everyone who pulls teams together to promote exposure and greater comfort levels with the different fields Being outside the facility itrsquos really a challenge for us We spend a lot of effort trying to track
people down and explain what kinds of services and offerings we have asking questions about their needs and where we can fill in the gaps
Mr Wingrove I represent the profes-sion that will literally decide for about 80 percent of you in the room today at least once whether you live or die Thatrsquos about 10 percent of what we do We have another 30 percent that deals with your urgent care needs and about 60 percent that involves your social needs Until recently we werenrsquot train-ing our professionals in how to deal with your social issues beyond some of the safety issues Thatrsquos one of the real promises of the new generation of community paramedics Itrsquos taking a professional that is super-sharp in life-saving skills and retraining them to do the majority of the work they actually perform each day which involves more psychosocial skills
Mr Starnes How can reimbursement mechanisms further collaboration
Dr Desai Therersquoll be a shortage of 90000 physicians within the next two to five years and certain states are suffering from it more acutely than others If we formed a care team with seven health care professionals and we all saw the patient together only one of us could get reimbursed We need to create incentives for people to want to be part of that team If you come to see me as a patient I will almost always refer you to a physical therapist possibly a behavioral health specialist an acupuncturist or a surgeon
Mehul Desai MD MPH practices at the Maple Grove and Fridley offices of Medical Advanced Pain Specialists (MAPS) Board-certified in pain medicine and physical medicine and rehabilitation (PMR) he has served as an assistant professor in the Depart-ment of Anesthesiology and Critical Care Medicine and of neurosurgery at George Washington Univer-sity (GWU) Medical Center Washington DC
John Gulon DDS has served at Eden Prairie-based Park Dental since 1987 In addition to seeing pa-tients at the group practicersquos Roseville clinic he has served as the president and CEO of Park Dental and its 37 practice locations since 2005 He graduated from the University of Minnesota School of Dentistry
Michael Hu MD practices at Hennepin County Medical Center He completed his medical degree and general surgery training at the University of Minnesota and his vascular surgery fellowship at Washington University in St Louis His professional interests include aneurysm disease peripheral arterial and venous disease carotid disease and dialysis access
Derek Hustvet RRT-NPS LRT is director of respi-ratory service at Pediatric Home Service (PHS) He earned a bachelorrsquos degree in respiratory therapy from North Dakota State University Fargo and is a licensed respiratory therapist and a neonatalpediatric respiratory care specialist
Craig Johnson PT MBA is president of the Minne-sota Physical Therapy Association (MNPT) where he is active in government affairs and payer relations as well as strategic repositioning efforts association payer forums and payer relation meetings He is also a partner and director of clinical integration at Therapy Partners
Charles Sawyer DC is senior vice president at Northwestern Health Sciences University in Bloom-ington Minnesota During his 35-year career he has been a leader in the chiropractic profession and a member of the faculty and administration at Northwestern Health Sciences University
Gary Wingrove is director of government relations and strategic affairs for Gold Cross AmbulanceMayo Clinic Medical Transport in Minnesota and Western Wisconsin He is a former Minnesota state EMS director who was awarded the Minnesota De-partment of Healthrsquos Jim Parker Leadership Award for Community Health Services
about the ModeratorMike starnes has been the publisher at Minnesota Physician Publishing since 1986 His duties include the production of MedFax Minnesota Physician Employee Benefits Planner and Minnesota Health Care News directing the Minnesota Health Care Consumer Association and hosting the Minnesota Health Care Roundtable
September 2015 Minnesota HealtH care news 21
ldquo You want to do the best thing for the patientrdquo
Michael Hu MD
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to promote innovative clinical pathwaysrdquo
Craig Johnson PT MBA
Dr Sawyer Right now with the fee-for-service reimbursement formula we donrsquot have any incentive to talk about team-based care If and when the payment shifts to focus on the value that the team provides it will be more productive
Dr Desai In 2018 it shifts as Medicare makes the majority of payments based on value as opposed to fee-for-service
Mr Starnes What could be gained by better relationships between health care professional relationships
Dr Desai Low-back pain is the single most expensive medical condition with costs approaching around $100 billion annu-ally in the United States Itrsquos three times more expensive than cardiac care services and itrsquos more expensive than diabetes and cardiac care combined Eighty percent of Americans will have an episode of low-back pain However it turns out that 7 percent of those patientsmdasharound 15 to 25 million Americansmdashare using up 85 to 97 percent of that $100 billion If the different health care professionals treating these patients operated more collaboratively there could be huge cost savings
Mr Johnson I think that many of our current outcome measurements are really process measurements Theyrsquore not quality-
of-life measurements like those used in Europe and theyrsquore not functionally based either An outcome thatrsquos worth measuring in my mind one that moves the health of the population higher requires a functional measure and a quality-of-life measure I think we do need to address that and not go with just process measures or measuring whether we get the person from point A to point B and theyrsquore happy and out the door but rather on their ability to function in society and their quality of life
Dr Hu In the large medical groups Irsquove worked in patient satisfaction is different from measuring the real outcomesmdashfor example that theyrsquore functioning better theyrsquore able to walk and theyrsquore pain free At the same time yoursquore getting these little management metricsmdashfor example what would you as a physician do Is the pa-tient satisfied and happy All of those are not necessarily the same as treating the problem I think that trying to have patient satisfaction is a tremendous problem that a lot of physicians complain about in these large care systems but it doesnrsquot necessarily correlate with better care
Dr Desai I agree with you because when you look at the HCAHPS (Hospital Consum-er Assessment of Healthcare Providers and Systems) scores patients who are more like-ly to be satisfied are more likely to die ear-lier Patient satisfaction and outcomes are not correlated Yoursquore more likely to provide more tests more medications more inter-ventions for someone because then they feel
as if something happened to them and they report being more satisfiedmdashbut thatrsquos not the same as actually getting better
Dr Hu At HCMC (Hennepin County Medical Center) wersquore working on a so-called Limb Salvage Center where we have people from different specialtiesmdashradiology vascular surgery hyperbaric oxygen dietarymdashtry-ing to save limbs All of us bring different perspectives and maybe we have different tools The whole goal is not to have two different ideas about how to treat this but to have one consensus idea of how to treat the patient
Dr Gulon Certainly wersquod see some ad-vantages of interoperability between the medical record and the dental record That doesnrsquot exist today Instead we do it the old-fashioned way with a call or paper referral One challenge is to follow up to ensure that the patient did follow through with the referral with the physician The other challenge is getting the results of that referral andor the tests or evaluation back to the dentist
Mr Starnes Any other thoughts on how we could improve care by improving relationships between provider types
Dr Gulon One for example is periodon-tal disease Itrsquos present in roughly half the population today and there are certain clear associations between periodontal disease and its management and cardio-vascular health Today roughly 80 million people have some form of hypertension and 145 million people go undiagnosed or are unaware of the associated risks
Mr Starnes Are there examples from within your own organizations of how expanded rela-tionships between different kinds of health care providers are producing good results
Mr Wingrove Within paramedic service we have some high-utilizer groups of patients The people that abuse our system tend to call on different days and at different times so theyrsquoll see nurse Judy on Monday and nurse Tammy on Wednesday and nurse Steve on Friday North Memorialrsquos com-munity paramedics now follow patients at home who have 10 or more medications three or more comorbidities and time-sen-sitive medications The paramedics use the same electronic medical record so they can see all the hospital visits all the clinic visits and can issue a request for a physical
22 Minnesota HealtH care news September 2015
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
ldquo We are trying to have more proactive team involvementrdquo
Derek Hustvet RRT-NPS LRT
therapy service or a secure message to the physician Itrsquos part of a Medicaid shared savings ACO (Accountable Care Organiza-tion) so the state gave them a significant portion of shared savings last fall Of course 80 percent of it should go to the paramedic and 20 percent be shared by the rest of you but that model is a shining star in the country
Dr Sawyer The Hennepin Health initiative is extremely novel It combines the clinical services that we all think about but then it adds social services and throws a big net over the most complicated vulnerable population of patients where the costs are high and the access is not good Theyrsquore bringing mental health professionals and social workers in and dealing with poverty and homelessness
Mr Hustvet We are trying to have more pro-active team involvement We are also trying to prevent emergency room visits and the expense of Medicare dollars We do this not just with asthma and obesity but also with our general patient population The bigger challenge is when we have to communicate with four different physicians from two dif-ferent hospitals with one to four involved parents and three four or five different primary nurses Care conferences are probably a great example as well We get to sit with the physicians with the family with everybody involved and have a conver-sation These meetings can sometimes raise really important crucial questions If the discharge is tomorrow what happens how do we fix this do we rush through things If the team does save dollars itrsquos hospi-tal-based versus home care versus maybe an extended living facility that determines where that benefit goes
Mr Johnson Whatrsquos going well Here are a few examples One is a primary spine pro-gram in Mankato The primary care clinic is a medical home and theyrsquore using a tool to risk-adjust patients in terms of the risk of accessing services and making referrals to physical therapy Another therapy clinic in our network is working with a primary care clinic and when a patient is identified with prediabetes based on blood work they refer them to physical therapy for education Theyrsquove shown very good results in reducing blood sugar levels over a six-month period Finally Courage Kenny set up a pilot program a couple of years ago as a medical
home with about 200 patients The patient population was essentially defined as dual eligible which means they are eligible for Medicaid and Medicare By being very preventive- focused and helping manage their health I believe they saved the state about $2 million
Mr Starnes Why are health plans so unwilling to offer fair compensation to non-physician health care professionals
Dr Sawyer Itrsquos all about coding and chasing the money Wersquore starting to ditch the terms complementary and alternative because they donrsquot mean anything If acupuncture is the best early treatment to use along with reasonable medication management for a patient with acute or chronic pain then that should be put into effect right from the start Typically to qualify for reim-bursement for acupuncture the pain has to be four months of chronicity or longer This delays the use of a therapy that has no downside to it whatsoever Then once pay-ment is approved reimbursement is so low that itrsquos not feasible to provide the care in a pain clinic or large health system
Mr Johnson In our current fee-for-service system itrsquos obvious that the current pathway for most disease processes is too costly Wersquove done a fair amount of research into payer data of delivery partners and timing of care in relation to physical therapy and particularly musculoskeletal conditions and therersquos a huge amount of care thatrsquos provided upstream There have been a couple of very good research articles from Spine magazine and Health Affairs demonstrating that early access to physical therapy for low back painmdashwithin 14 days of seeing a primary or a medical providermdashhas reduced the total episode cost for that back episode by 40 percent
Mr Starnes Dental insurance reimbursement seems to differ from other reimbursement models Why is this
Dr Gulon Irsquom not sure that dental is doing it any better In fact in dental we get paid by procedures In the dental world we donrsquot operate with diagnostic codes but that world is evolving On the other hand wersquore working on a couple of novel projects with integrated physician networks including some sleep studies right in our practice Wersquove worked out some reimbursement mechanisms between the physician network and our group
Mr Starnes One of the biggest challenges comes from corporate culture and senior leadership In some systems individuals wonrsquot change regardless of evidence that suggests they should and in some systems senior leadership is very proactive about change but it somehow gets bogged down in mid-level management Any comments on this
Dr Desai We do have progressive-thinking leadership and wersquore doing some things that are progressive and innovative on the training level People who have been trained already and have been out of school for five 10 or 15 years is where the gap is What we really need is to identify and mentor and support great clinical leaders What I mean is that health care is not going to change until health care providers buy in You can have a great administrator you can force it down someonersquos throat but you need a foil to that with great health care
September 2015 Minnesota HealtH care news 23
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
leadership Getting folks who are mid-ca-reer to change their practice patterns as wersquove all been talking about is a signifi-cantly greater challenge because theyrsquore set in their ways Those are the folks running the show so to speak
Dr Gulon Irsquom really optimistic that the ears are open from the medical administratorsrsquo point of view Many of us have been proud that in Minnesota overall wersquore pretty progressive with regards to health care Unfortunately when it comes to the pedi-atric dental benefit Minnesota is dead last 50th out of 50 in terms of reimbursement Switching gears for a moment from the conversations wersquove had with chief med-ical officers therersquos a significant amount of waste in terms of the access for dental care through emergency departments with roughly $50 million each year being spent on dental care in emergency rooms Inter-estingly enough wersquove been able to partner with a physician group to leverage some of the synergies so that we can actually have those patients access the care through the dental practice rather than through the emergency room
Mr Wingrove When we encounter a patient who has congestive heart failure and has significant breathing difficulty we have two choices We can intubate them or we can put them on CPAP (continuous positive airway pressure) If we intubate them what do you suppose happens to the hospital-
acquired infection rate It has nothing to do with the hospital but itrsquos in an unsterile environment and itrsquos an invasive proce-dure On the other hand if we use CPAP and maybe even get a better result than intubation we can drive the hospital score into a better position Those are some of the things that have value to patients as well as to the payers
Mr Starnes Under the Accountable Care Act (ACA) reimbursement for health care services will migrate from a volume- to a value-based methodology How does expanded collabora-tion between health care professionals respond to this migration
Mr Johnson The whole notion of collabora-tion has been spurred on by the ACA The Centers for Medicare amp Medicaid Services (CMS) has announced that theyrsquore moving towards 50 percent of their payment being value-based by 2018 and that will certainly foster innovation around collaboration I am a firm believer that we should manage what we measure so measuring outcome is going to be very critical in this collab-oration Financial incentives when they are aligned will also drive collaboration and financial incentives really do drive our provider behavior
Mr Starnes Part of the health care reform is going to deal with attempts to reduce rehospi-talization How can penalties for rehospitaliza-tion drive better collaboration
Mr Hustvet From a home care perspective we actually have some incentive right now to keep patients out of the hospital We canrsquot bill for our equipment and we canrsquot bill for the pieces or parts or supplies they use if theyrsquore in the hospital We have a clinical piece that often does not get reimbursed If it does get reimbursed itrsquos not a full reim-bursement but that piece of equipment is necessary to keep that patient out of the hospital Wersquove noticed in the last three years more focus from the hospital facility level at care management and discharge planning Therersquos a lot more focus on providing 24-hour 7-day-a-week support There used to be just a daily discharge plan after which you didnrsquot have a lot of com-munication and cooperation I think from our perspective wersquove been trying to do this because itrsquos good for our business model and itrsquos good for our patients
Mr Starnes Can an increased emphasis on prevention foster improved collaborations
Dr Desai Itrsquos very unlikely that prevention can be achieved with just one provider Itrsquos unlikely that just one specialist or one primary care provider could achieve pre-vention I think that in itself provides the foundation for greater collaboration One of the things I tell patients all the time is I donrsquot have to be the one to fix you I donrsquot have to be the one to make you better but if I can get you to the right person it still makes me look good
Dr Sawyer Irsquom not sure who is able by virtue of their training and experience to actually provide preventive services Irsquom not talking about pap smears and mammo-grams Irsquom talking about the discussions the coaching and visiting with the patient Wersquove got a mixed bag and I think itrsquos too early to know for sure how thatrsquos going to work but we certainly have to put that in place because itrsquos now mandated
Mr Starnes Are there future legislative actions at the state or federal level that might drive collaboration
Mr Johnson It can be demonstrated that silo management mentality is ineffective From our associationrsquos standpoint we are trying to promote innovative clinical path-ways and research has shown that early access to physical therapy is key to saving dollars throughout that whole episode We have a very innovative national association
24 Minnesota HealtH care news September 2015
ldquo everybody ought to be right at the top of their licenserdquo
Charles Sawyer DC
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
I applied for a grant from them to run a pilot study around workerrsquos compensation patients directly accessing physical therapy We have had discussions with stakehold-ers at high levels including the Chamber of Commerce the Department of Labor brokers and the workerrsquos compensation in-surer for the state I think this is definitely beginning to show up on their radar I think that will obviously affect future legislation and the way that the workerrsquos compensa-tion fee schedule works Ultimately we are hoping to change legislation
Mr Starnes We recently had landmark approval from the House and Senate on new Medicare reform Is Medicare reform going to help foster better relationships between health care professionals
Mr Hustvet I think itrsquos a good start I think anytime yoursquore getting physicians involved with alternative providers therersquos going to be more collaboration Therersquos a push right now on both physicians and even physician assistants to see how much work they can get done If we can spend 10 minutes 20 minutes or a half hour with the patient and then have a five-minute conversation with the physicianmdashversus the physician only getting five minutes with the patientmdash I think thatrsquos going to drive a little more col-laboration and offer a little more exposure The physician I think will end up ultimate-ly being more of a coordinator and manag-er of the other therapies and services
Mr Starnes In every legislative session there are bills introduced that redefine the scope of practice for specific provider types and there are always ldquoturf-warrdquo conflicts over their pas-sage How do we best address this
Mr Wingrove Sometimes thatrsquos healthy tension and sometimes thatrsquos not healthy tension Wersquore in a time when change is here and itrsquos being made everywhere and I think we just have to recognize there have been changes over time in all of our professions and those are cyclic This is a new time when the professions will change Technology also plays a role in how safely different providers can do different things The professional protection I donrsquot think will ever go away but wersquoll have to respond to it based on what the payment system forces on us
Mr Johnson We donrsquot really like this licen-sure turf battle but it does happen Therersquos
a filter that describes scope and helps leg-islators make decisions Legislators make decisions about scope for every profession in this state and theyrsquore not really the experts most of the time Theyrsquove actually appreciated that herersquos something that you can measure when somebody comes to you and they want to expand in a certain area I think we need to get beyond that as well and be very proactive because the time that it takes and the resources it takes to fight those battles are pretty wasted I think we need to recognize that and try to maximize the training level of each provider on the care team and not have legislative turf bat-tles about scope
Dr Sawyer The real issue is that everybody ought to be right at the top of their license and if these care models can change and the reimbursement can change then the commercial payers will follow what Medi-care is doing Getting this shift to value would allow clinicians like Gary and me to sit down at the table and say well if wersquore in the shop together if wersquore in the same practice together what can we do to elevate the model of care and the delivery of it and the efficiency of it and go right to a payer along with nurse practitioners pain spe-cialists and acupuncturists and say wersquove got a proposal from you and itrsquos too good to turn down
Dr Gulon Dentistry as I mentioned earlier has added mid-level practitioners in the form of dental therapists and advanced dental therapists with expanded functions Dentistry was not un-like other professions that were slow to recognize the shortag-es that we are encoun-tering We have to be more creative and I think thatrsquos driving a lot of the behaviors out there
Dr Hu If you can get the collaborations to work is it going to be revenue neutral If itrsquos revenue neutral basically yoursquore redistributing income from one group to another group From a practical stand-
point I believe that fee-for-service can be a very powerful motivator sometimes just to do the work Will people work as hard when you take away some of that financial incentive I know that under different health care models and within different health care groups when you incentivize doing a procedure and yoursquore a subspecial-ist you do make your people work harder When you take that incentive away they donrsquot work as hard
Dr Sawyer I do worry a little bit about the fact that maybe wersquore over-vilifying fee-for-service reimbursement If we shift into value-based reimbursement and shared savings and shared risk I wonder if therersquos going to be another perverse incentive If I do less the team that Irsquom on the hospital that I practice in and the system that Irsquom a health care provider in is going to do bet-ter and by extension I will do better if my contract shows some performance
Mr Hustvet I think therersquos also potential for cost savings If Irsquom a respiratory therapist and Irsquom allowed to manage an asthma pa-tient more than likely Irsquom going to get reim-bursed less than the pulmonologist would I could be working for a pulmonologist or a physician or a primary pediatrician through their office Irsquom getting reimbursed less but theyrsquore seeing three times as many asthma patients because Irsquom there as well I think therersquos some potential to shift some
September 2015 Minnesota HealtH care news 25
ldquo Wersquore in a time when change is hererdquo
Gary Wingrove
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
of the work to me or other folks that arenrsquot billing quite as much and still see quali-ty patients and allow the physician to see the higher-needs patients that maybe are getting delayed or pushed off or even going into the hospital
Mr Starnes An emerging model involves com-munity-based initiatives many of which could be duplicated and expanded Can you give some examples
Mr Wingrove Our state got a grant from CMS to work on different sorts of models and one of the ones theyrsquove chosen is to create opportunities to expand three emerg-ing professions community paramedics community health workers and dental therapists They are contracting now for each of these to create tool kits for potential employers The goal is to speed the adop-tion of the professions by employers It will set the stage for the employer to learn about the training they come in with the sorts of things you can expect them to do and how reimbursement worksmdashif it works at all They are also at least in our case subsidiz-ing the employment of a handful of pro-fessionals so that employers can test it out and make sure it works and learn about the intricate details of actually putting the pro-fession into practice
Dr Sawyer Irsquom not sure that the innova-tions would have happened in either the state innovation model initiative or the Hennepin Health initiative if there hadnrsquot been legislation and direct involvement by state agencies with provider groups In other words Irsquom not sure that would have evolved or happened if the payers werenrsquot the ones responsible for it and I donrsquot think they wouldrsquove taken the initiative
Mr Johnson Under one community-based program that in its original form our asso-ciation worked on we developed an educa-tion program that assessed seniors for their risk of falling Reducing the number of falls has an impact on that individualrsquos health as well as on the health of those in the com-munity The program was first developed for assessment and then for intervention and oftentimes the assessment revealed that a community-based strengthening program would help to reduce the risk of falls This was a grant-funded initiative with a train-the-trainer model which trained commu-nity health nurses and others to assess and then to address the issue Now the Depart-ment of Health is reviving this initiative with about a dozen health care providers and community organizations working on reducing falls by seniors in the community
Mr Starnes How could a value-based care model promote interprofessional relationships or address the turf or silo mentality
Dr Desai The greatest advantage of a value-based reimbursement model is that for the most part the value of a personrsquos contribution to the care team gets equalized a little bit better The traditional system is quite hierarchal with certain people on the top and others along the way By bundling care and by providing reimbursement in a value-based system long-term manage-ment becomes more important than inci-dent-based management which also then shifts away from the silo effect
Mr Starnes If we increased the focus on the patient experience might we break down some of that silo mentality
Dr Hu I think so Like anything you want to do the best thing for the patient and itrsquos rare that yoursquore the only one who can do it I think centering on the patients giving them the best experience requires you to seek out all the other things that they need I think yes that will help break down some of the silos
Dr Gulon Patients who go through different levels of caremdashwhether itrsquos with a dentist or a physician or a chiropractor or whom-evermdashwill benefit if therersquos a high level of transparency communication and coordi-nation within the care team Certainly we recognize the challenges of achieving that but also itrsquos pretty obvious how that might feel to the patient
Mr Starnes Even though different types of providers have similar goals they may not talk to each other Why not
Dr Desai Synergies are often unrealized because of time and malaligned financial incentives Those are the two primary rea-sons Right now therersquos no incentive to learn what the other guys do He might be the specialist in this I might be the specialist in that In order to get that 360-degree view or that spherical view of what the patientrsquos going through you need to get all partners involved If you do that then the value of your partnership increases and your incen-tive to learn about what others do at least to some extent increases
Dr Sawyer If wersquore in the same practice business together we sit down at the table and figure out how are we going to be
26 Minnesota HealtH care news September 2015
ldquo i see this as an opportunity not a barrierrdquo
John Gulon DDS
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e sponsored by
M i n n e s o t a h e a l t h c a r e r o u n d t a b l e
successful because wersquod like to approach this particular payer public or private with a proposal to do X for a new model of care and delivery Wersquove got to get to know each other on both a professional level and a personal level so we have some trust and assurance that wersquore watching each otherrsquos backs Being in business together is a big deal
Mr Hustvet We lack easy communication and easy access tools Just because Irsquom only free at noon and yoursquore only free at one doesnrsquot mean I couldnrsquot have gone into a shared system and put in a note or a com-ment for you Thatrsquos better than a system in which one physician calls one emails and one faxes or leaves a note on the nursersquos desk I canrsquot communicate with three or four of the hospitals that use different electronic records and one physician who prefers to use a pager and calls me back when Irsquom already out on the road seeing somebody else
Mr Starnes Do patients need to be educated not to fear being part of a collaborative process
Dr Desai I think so I think increasingly you have patients who have been exposed to advocacy groups Also patients are increas-ingly more educated about their disease states Patients come to me all the time and say well PT (physical therapy) doesnrsquot work for me or chiropractic doesnrsquot work for me or acupuncture doesnrsquot work for me That ties back into that initial conversation we had about training and understanding what your collaborators bring to the table I say to the patient well itrsquos not that PT doesnrsquot work for you but itrsquos that therapist
Mr Johnson I think thatrsquos exactly right We have a joke in physical therapy about a patient making a comment to the doctor ldquoI tried physical therapy and it didnrsquot workrdquo The comeback is ldquoHave you tried doctoringrdquo Itrsquos the individual There is a provider in town that is absolutely selective about which therapist he sends his patients to because hersquos taken the time to build a relationship Understanding the person whorsquos delivering the care is really critical and I think thatrsquos a great point
Dr Desai A lot of us who believe in multidis-ciplinary or interdisciplinary care have tak-en the time to create our own networks I have already identified the folks Irsquom going to
send people to I have preferred providers and those are the only people Irsquom interested in sending patients to if I have a choice I know at the end of the day the patients are going to get better and itrsquos going to make me look good and everyone so to speak is happy at the end of that experience
Mr Starnes What must be done to expand interprofessional relationships in health care delivery
Mr Wingrove I think it centers on the people and the relationships between the professionals It will go faster if we spend time on the front end managing that process well
Mr Hustvet I think the most basic piece is just increased communication whether that involves meetings discussions or elec-tronic communications Thatrsquos really going to be the main driver
Dr Desai In my estimation itrsquos financial misalignment Until we align the financial incentives to collaborate therersquos going to be some resistance I think that with the Accountable Care Act and with value-based reimbursement wersquore moving in the right direction and I think there are some really creative ideas with regards to that but finances need to be aligned
Dr Sawyer I think it has to be initiative and motivation In other words when Irsquove got a reason to reach out I should make that phone call or send that email and ask if we can have lunch so we can start talking about some different ways of working together
Dr Gulon From the consumer point of view I would ask patients to continue to access the system and to understand how relation-ships and overall health are interconnected and to continue to demand from the med-ical care system that which seems obvious but which may be more difficult to achieve I think that with continued persistence that will happen
Dr Hu If I had to pick one I would say good communication between the different specialties and the different providers Concurrent with that would be a good understanding of the capabilities of every-one on the team and what they can do for the patient
Mr Johnson I would echo those Itrsquos a long list but I believe that aligning the financial incentives and relationships and under-standing what each provider does are most important
September 2015 Minnesota HealtH care news 27
ldquo I tell patients all the time lsquoI donrsquot have to be the one to fix yoursquordquo
Mehul Desai MD MPH
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
Urology
Overactive bladder (OAB) is not a disease but a condition with symptoms of increased urinary frequency and urgency OAB may also include urinary leakage associated with a
bothersome degree of urge to get to the bathroom It is a common condition afflicting more than 33 million Americans It may occur among both sexes of all ages but is more common in female adults
Is it really a problemYes it is The normal frequency of urination is around six to eight times per day and up to two times per night Urinary leakage due
to urgency is also abnormal While having an increase in frequency every once in awhile is not necessarily a problem when the symp-toms of OAB start to have a consistent negative effect on a patientrsquos quality of life it becomes a medical condition Patients with OAB suffer physical and emotional harm from the problem They have been shown to have a significantly decreased quality of life causing extreme embarrassment that limits their social interactions employ-ment opportunities and trips outside the home It also promotes social isolation and depression It is not unusual for patients to dehydrate themselves in order to minimize the symptoms of OAB which may have other unintended health consequences such as falls and hip fractures among the elderly Patients often spend hundreds of dollars annually on pads and diapers in order to contain the leakage As one of our 20-something patients once told us ldquoItrsquos not like you put a diaper on and then you are normalrdquo
How is it diagnosedThe patientrsquos history is key Amounts and type of fluid intake other medical conditions and current medications need to be understood We ask them to recount how many times per day they void what is the degree of urgency and whether or not there are accidents before reaching the bathroom We need to know if the degree of leakage may require pad use and if so what type and how many pads per day are usually required It is often hard for patients to answer these types of questions without giving them some forethought A urinary diary used by the patient to count these events can be very helpful in zeroing in on the symptoms and often can be a surprise to the patient who may have been dealing with the problem by trying to ignore or minimize the symptoms
We also need to know how much bother each individual patient experiences from these complaints It does not always follow that a patient who leaks more is more troubled Some patients can cope well with a lot of leakage and some find small amounts extremely bothersome We usually use surveys that include a score based on a series of questions that have been validated to measure the impact on quality of life for OAB Not only can these be helpful on initial assessment but along with voiding diaries they can help us to assess the impact of treatments and the need for further measures should the problem remain
Overactive bladder
When going too often becomes a problemBy Steven Siegel MD
28 MINNeSOTA HeAlTH cAre NeWS September 2015
In the next issue
bullEczema
bullMale osteoporosis
bullNeuropathy
Your Guide to Consumer Information
It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

It is not unusual for the problem of OAB to coexist with other conditions such as leakage with cough or sneeze or other physical exertions (stress urinary incontinence) vaginal bulges due to pelvic prolapse in which pelvic organs slip out of place urinary tract infection and slow stream or incomplete bladder emptying which could be related to prostate problems in men Bowel symptoms such as constipation or lack of control (fecal incontinence) can also be present and need to be assessed On physical exam we need to check for vaginal support and visible leakage in females prostate size in men pelvic muscle tone and control changes that may affect hip function swelling in the lower extremities and neurological signs that may be associated with urinary symptoms We also check a urine sample to rule out blood or infection and measure how much remains in the bladder after urination to understand the patientrsquos ability to empty This type of workup is usually enough to get started for most patients In some cases cystoscopy testing (which uses a thin lighted tube equipped with a lens to inspect the bladder) or a nerve test of bladder function (urodynamics exam) may be needed
What can be done about OABlots Most people are aware that there are medications for the woman who has ldquogotta go gotta go gotta go right nowrdquo However while many brands of medication have been available for decades they mostly work about the same and for most patients particularly younger ones with few other health concerns they may prove to be a limited and unsustainable solution due to incomplete benefits and side effects including dry mouth and constipation Plus medications donrsquot solve the problem they simply attempt to minimize the symptoms While medications are an option for all of our patients other options are often more successful and desirable We use a ldquoroadmaprdquo or pathway of conservative and advanced options to help the patient visualize where they stand with their problem which treatments have been tried and which additional options remain should they still be bothered by their OAB symptoms
Conservative options Many of our patients arrive ready to start with the first conservative steps that in addition to drugs include behavioral therapies biofeedback or physical therapy As an exam-ple types and patterns of fluid intake can be related to the problem Too much caffeine pop and even excessive water consumption may be contributing factors Alternatively severe restriction of fluid and lack of dietary fiber may contribute to constipation which also could have a negative impact on symptoms Dietary changes are a basic behavioral measure that carries little risk and can offer a big reward Patients are often surprised at how well these conservative options can impact their condition and we are always satisfied when something simple inexpensive safe and reversible proves to be the right solution for a particular patient linking the patient to an appropriate resource such as physical therapy or a biofeedback therapist is critical in making the most out of these options
Advanced options Some of our patients will have already tried and failed conservative options and this provides a starting point
for advanced options for OAB They include nerve stimulation therapies similar to acupuncture (Urgent Pc) or implantable devices that work like a pacemaker (InterStim) Injection of the bladder
with Botox can also be used to successfully treat OAB symptoms each option has pros and cons for
an individual patient and providers need to help the patient understand them in order to weigh them and decide what may work best in each case
SummaryOAB is a common problem of both men and women and can have a significant impact on overall health Specialists in OAB are dedicated to helping patients with this problem and will continue to work to im-prove symptoms with the increasingly wide range of options that are currently available Since this is a problem of symptoms and quality of life when our patients are happy
we are happy If they are still being bothered by symptoms we will continue to offer appropriate solutions There is rarely a patient with this problem who cannot be helped
Steven Siegel MD is the director of the Centers for Urinary Incontinence and Female Urology at Metro Urology He is board-certified in urology and female pelvic medicine and reconstructive surgery He practices in Woodbury Minn
September 2015 MINNeSOTA HeAlTH cAre NeWS 29
Normal frequency of urination is around six to eight times per day
More than 2400 families have found a place to belong at St Davidrsquos Center
FIND YOUR PLACE
stdavidscenterorg9525488700
YOU belongHERE
Early Childhood Education bull Autism ServicesPediatric Speech Music and Occupational Therapy
Childrenrsquos Mental Health bull Foster CareServices for Individuals with Lifelong Special Needs
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
ChroniC Conditions
Lupus is a chronic autoimmune disease where the immune system turns against parts of the body itrsquos designed to protect This leads to inflammation and can affect many
different body systems including joints blood cells and organs Although one in 200 people is diagnosed with lupusmdash90 percent of whom are womenmdashit remains one of the least well-known chronic illnesses
Lupus can occur at any age and in either sex Women are most often diagnosed during the childbearing years between the ages of 15 and 45 African American Latino Asian and Native American women have a significantly higher risk for lupus and tend to develop the disease earlier and have more complications than Caucasians Yet statistics of individuals with lupus over the age of 50 show a significant increase in the number of males diagnosed
There are four different types of lupus
bull Systemic lupus erythematosus (SLE) is generally considered more serious than the other three forms SLE can affect many parts of a personrsquos body including kidneys heart lungs brain blood and skin
bull Discoid is a form of lupus that only affects the skin and causes rashes typically found on the face neck and scalp but can appear anywhere on the body This type of lupus does not affect any of the internal body organs although one in 10 people living with discoid lupus will develop systemic lupus
bull Drug-induced lupus occurs after a person takes certain types of medication The symptoms are similar to SLE but they usually disappear when a person stops taking the medicine
bull Neonatal lupus occurs rarely in newborns of mothers with lupus This condition can cause skin rashes anemia or liver problems and symptoms usually go away after a few months and donrsquot cause permanent damage
Cause of lupusWhile the cause is unknown scientists suspect that individuals are genetically predisposed to lupus and that the disease remains quiet until a trigger sets the disease process in motion Some outside environmental factor(s) create the right conditions for the disease to become active The conditions that trigger lupus vary from person to person
Only 10 percent of those with lupus will have a parent or sibling who already has or may develop lupus The chance increases to 50 percent if one has an identical twin with lupus About 5 percent of the children born to individuals with lupus will develop the illness
Living with
Managing an autoimmune diseaseBy Jennifer Monroe MA MPH
and Timothy Niewold MD
30 MiNNESOTA HEALTH CArE NEWS September 2015
We are so sure the BioMat will improve your health that we accept returns for full refund if you are not satisfied for any reason If you order through us you will also receive a 30 year repair guarantee and lifetime trade-in policy
This amazing medical-grade infrared heating mat can change your life for the better It is used in homes and professional healing practices all over the world The BioMat provides immediate and dramatic relief for people suffering from a wide variety of chronic
conditions that have not responded well to medication therapy A brief overview of benefits from using the BioMat
bull Stress and anxiety reliefbull Improved mobility and flexibilitybull Chronic and acute pain reliefbull Arthritis neuropathy and
fibromyalgia reliefbull Detoxification
bull Core body temperature supportbull Improved circulationbull Lymphatic drainagebull Relief from persistent infectionbull Speeds healing of soft tissue injuries
Have You heardabout the BioMat
Mini BioMat 33x20$65000
BioMat Professional 74x28$165000
For more details please visit wwwcrystalbiomatcom
8666897336
Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Symptoms and diagnosis Each person with lupus has different symptoms that can range from mild to severe and may come and go over time New symptoms may continue to appear years after the initial diagnosis and different symptoms can occur at different times in some only one system of the body such as the skin or joints is affected Other people experience symptoms in many parts of their body Just how seriously a body system is affected varies from person to person
Some of the most common symptoms include extreme fatigue arthritis unexplained fever skin rashes and kidney problems Other symptoms include chest pain upon breathing unusual loss of hair pale or purple fingers or toes from cold or stress (also known as raynaudrsquos phenom-enon) sensitivity to the sun swelling in legs or around the eyes mouth ulcers and swollen glands
Lupus can be difficult to diagnose and it may take months or years because the symptoms are usually not present all the time When the symptoms are present they can mimic other diseas-es resulting in misdiagnosis Additionally there is no single test to diagnose lupus The process of diagnosis requires a patientrsquos entire medical history details on the frequency and severity of symptoms and an analysis of lab test results
Flares and remissionsLupus is unpredictable and patients often suffer flares (active symptoms) followed by periods of remission (symptoms disappear) For those who have not been diagnosed with lupus this continued recurrence of symptoms might be the first clue that lupus is the cause
Lupus flares can be classified as mild moderate or severe An example of a milder flare might be the appearance of a rash while an example of a very severe flare could cause fluid collection around the heart or even kidney failure
What causes a flare is almost as unpredictable as when the flare will occur There is no definitive way to predict when a flare will happen how bad it will be or how long it will last When patients experience a lupus flare they may have different symptoms than those they have had in the past
The best way to manage lupus and avoid flares is to listen to the body learn what the personal triggers and early warning signs are and talk with a physician about them Additionally individuals and families whose lives are impacted by lupus can better educate themselves and learn about the different resources that exist through organizations such as the Lupus Foundation of Minnesota Mayo Clinic and the University of Minnesotarsquos Lupus Clinic to help them live well with the disease However if an individual with lupus thinks a flare is starting itrsquos best to see a physician as soon as possible
Treatment and managementAlthough therersquos no cure for lupus yet medications can control symptoms and prevent or slow organ damage While some minor lupus cases can be handled without medication most people with
lupus require medication to minimize symptoms and maintain normal functions The goals of an individualrsquos treatment plan are to prevent flares control symptoms and treat flares when they occur and to reduce organ damage and other problems
Common medications used to treat lupus include Benlysta aspirin and nonsteroidal
anti-inflammatory drugs (NSAiDs) anti-malarial drugs such as Avloclor or Malarivon (chloroquine phosphates) or Nivaquine
(chloroquine sulfate) Atabrine or Mepacrine (Quinacrine Hydrocholorides) Plaquenil (hydroxychloroquine) or corticosteroids in serious cases immunosuppressive drugs
may also be prescribed
The treatment of lupus is still challeng-ing and because patients are not able to predict flares in advance vigilance and communication between patient and physician are critical in managing lupus and controlling symptoms
rest stress reduction and a healthy diet and lifestyle are also important in addition the use of sunscreens is advocated in all patients even in non-tropical regions as ultraviolet light may exacerbate lupus
Living with lupus to page 34
September 2015 MiNNESOTA HEALTH CArE NEWS 31
People living with lupus can lead active
healthy lives
the bene ts of yogaDiscoverRight now new students get a FREE WEEK of unlimited yoga
See you soon at any one of our 8 Minnesota locations
Eden Prairie bull Edina bull Minneapolis bull Minnetonka
St Louis Park bull St Paul bull Stadium Village bull Uptown
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
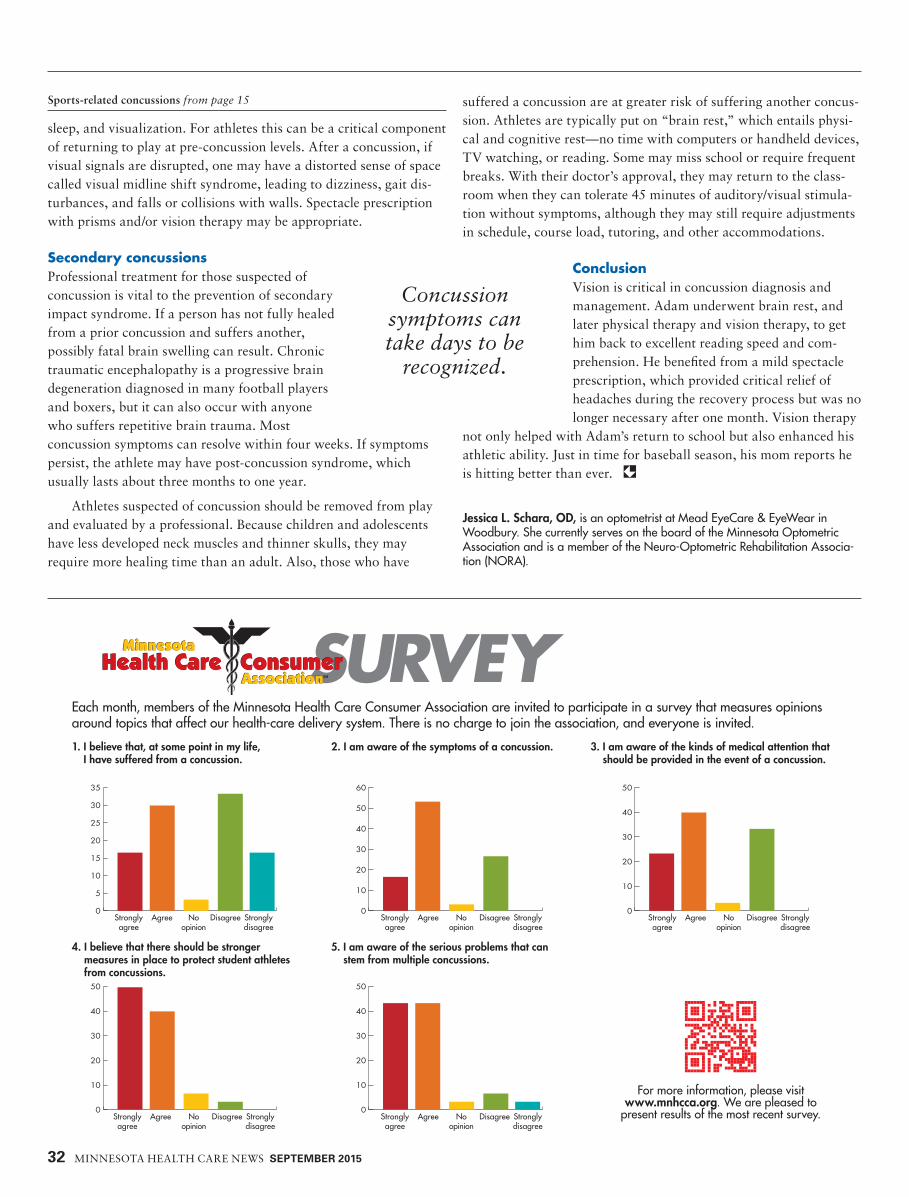
32 MInneSoTA HeALTH CAre neWS September 2015
sleep and visualization For athletes this can be a critical component of returning to play at pre-concussion levels After a concussion if visual signals are disrupted one may have a distorted sense of space called visual midline shift syndrome leading to dizziness gait dis-turbances and falls or collisions with walls Spectacle prescription with prisms andor vision therapy may be appropriate
Secondary concussionsProfessional treatment for those suspected of concussion is vital to the prevention of secondary impact syndrome If a person has not fully healed from a prior concussion and suffers another possibly fatal brain swelling can result Chronic traumatic encephalopathy is a progressive brain degeneration diagnosed in many football players and boxers but it can also occur with anyone who suffers repetitive brain trauma Most concussion symptoms can resolve within four weeks If symptoms persist the athlete may have post-concussion syndrome which usually lasts about three months to one year
Athletes suspected of concussion should be removed from play and evaluated by a professional Because children and adolescents have less developed neck muscles and thinner skulls they may require more healing time than an adult Also those who have
suffered a concussion are at greater risk of suffering another concus-sion Athletes are typically put on ldquobrain restrdquo which entails physi-cal and cognitive restmdashno time with computers or handheld devices TV watching or reading Some may miss school or require frequent breaks With their doctorrsquos approval they may return to the class-room when they can tolerate 45 minutes of auditoryvisual stimula-tion without symptoms although they may still require adjustments in schedule course load tutoring and other accommodations
ConclusionVision is critical in concussion diagnosis and management Adam underwent brain rest and later physical therapy and vision therapy to get him back to excellent reading speed and com-prehension He benefited from a mild spectacle prescription which provided critical relief of headaches during the recovery process but was no longer necessary after one month Vision therapy
not only helped with Adamrsquos return to school but also enhanced his athletic ability Just in time for baseball season his mom reports he is hitting better than ever
Jessica L Schara OD is an optometrist at Mead EyeCare amp EyeWear in Woodbury She currently serves on the board of the Minnesota Optometric Association and is a member of the Neuro-Optometric Rehabilitation Associa-tion (NORA)
Sports-related concussions from page 15
Concussion symptoms can take days to be
recognized
0
5
10
15
20
25
30
35
0
10
20
30
40
50
0
10
20
30
40
50
60
0
10
20
30
40
50
0
10
20
30
40
50
Each month members of the Minnesota Health Care Consumer Association are invited to participate in a survey that measures opinions around topics that affect our health-care delivery system There is no charge to join the association and everyone is invited
1 I believe that at some point in my life I have suffered from a concussion
3 I am aware of the kinds of medical attention that should be provided in the event of a concussion
5 I am aware of the serious problems that can stem from multiple concussions
2 I am aware of the symptoms of a concussion
4 I believe that there should be stronger measures in place to protect student athletes from concussions
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
Strongly agree
Agree No opinion
Disagree Strongly disagree
For more information please visit wwwmnhccaorg We are pleased to
present results of the most recent survey
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks
ldquoA way for you to make a diff erencerdquo
Join now
SM
Welcome to your opportunity to be heard in debates and discussions that shape the futureof health care policy There is no cost to joinand all you need to become a member is access to the Internet
Members receive a free monthly electronicnewsletter and the opportunity to participate in consumer opinion surveys
wwwmnhccaorg
Health Care ConsumerAssociation
Minnesota
NOVEMBER 2012 MINNESOTA HEALTH CARE NEWS 33September 2015 Minnesota HealtH care news 33
All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

All in all treatment options for lupus have begun to improve with more potential treatments in the pipeline than ever before and people with the disease are living longer Studies have shown that people who are informed and involved in their own care have less pain make fewer visits to the doctor feel better about themselves and remain more active
Advancements This is an exciting time for lupus research Scientists are at the threshold of a number of new treatment possibilities at various stages of clinical development For instance in Minneso-ta studies are currently in process focusing on a myriad of critical areas including genetics measuring and evaluating clinical disease development against normal biological process-es using biological markers (or biomarkers) monitoring the lupus disease process exploring treatment options and overcoming barriers that tend to keep some populations from complying with prescribed treatment
Great progress is being made in understand-ing the cause of lupus Studies are mapping the
genetic architecture of the disease as well as the immune system abnormalities that characterize lupus This is leading to ideas for new therapeutic targets and many of these are being worked on in academic research centers and pharmaceutical companies Many other autoimmune diseases such as rheumatoid arthritis and
psoriasis have seen a number of new effective immune system-based treatments providing hope that lupus will enjoy the same type of progress in the coming years
Although the cause of lupus remains unknown and a cure is yet to be discovered people living with lupus can lead active healthy lives Support systems are in place and public awareness is higher than itrsquos ever been Signif-icant progress also continues to be made year after year in the area of medical research From new drugs to cutting-edge genetic research the dynamic growth in clinical efforts to under-stand and treat lupus is encouraging
Jennifer Monroe MA MPh is president of the Lupus Foundation of Minnesota an independent nonprofit charitable organization based in Bloomington timothy niewold Md is an associate professor of medicine at the Mayo Clinic in Rochester and a 2015 Lupus Foun-dation of Minnesota research grant recipient
This is an exciting time for lupus research
Living with lupus from page 31
34 MiNNESOTA HEALTH CArE NEWS September 2015
Elizabeth Klodas MDFASCC is a preventive
cardiologist She isthe founding Editor inChief of CardioSmart
for the AmericanCollege of Cardiologywwwcardiosmartorg
a published authorand medical editor for
webMD She is a memberof several national
committees on improvingcardiac health and afrequent lecturer on
the topic
Preventive Cardiology Consultants isfounded on the fundamental belief thatmuch of heart disease can be avoidedin the vast majority of patients andsignificantly delayed in the rest by prudentmodification of risk factors and attainablelifestyle measures
We are dedicated to creating a true part-nership between doctor and patient workingtogether to maximize heart health Wespend time getting to know each patientindividually learning about their lives andlifestyles before customizing treatmentprograms to maximize their health
Whether you have experienced any typeof cardiac event are at risk for one or
are interested in learning how to preventone we can design a set of just-for-yousolutions
Among the services we provide
bull One-on-one consultations withcardiologists
bull In-depth evaluation of nutrition andlifestyle factors
bull Advanced and routine blood analysis
bull Cardiac imaging including (as required)stress testing stress echocardiographystress nuclear imaging coronary calciumscreening CT coronary angiography
bull Vascular screening
bull Dietary counselingExercise prescriptions
Now accepting new patients
A unique perspective on cardiac care
To schedule an appointment or to learn more about becominga patient please contact
Preventive Cardiology Consultants6545 France Avenue Suite 125 Edina MN 55435
phone 9529295600 fax 9529295610 wwwpccmncom
Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

Victozareg (liraglutide [rDNA origin] injection) Rx Only BRIEF SUMMARY Please consult package insert for full prescribing information
WARNING RISK OF THYROID C-CELL TUMORS Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carci-noma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitor-ing with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumors [see Contraindications and Warnings and Precautions]
INDICATIONS AND USAGE Victozareg is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus Important Limitations of Use Because of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exercise Based on spon-taneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitis Victozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settings The concurrent use of Victozareg and prandial insulin has not been studiedCONTRAINDICATIONS Do not use in patients with a personal or family history of medullary thyroid car-cinoma (MTC) or in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Do not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsWARNINGS AND PRECAUTIONS Risk of Thyroid C-cell Tumors Liraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors (adenomas andor carcinomas) at clinically rele-vant exposures in both genders of rats and mice Malignant thyroid C-cell carcinomas were detected in rats and mice A statistically significant increase in cancer was observed in rats receiving liraglutide at 8-times clinical exposure compared to controls It is unknown whether Victozareg will cause thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as the human relevance of liraglutide-induced rodent thyroid C-cell tumors could not be determined by clinical or nonclinical studies In the clinical trials there have been 6 reported cases of thyroid C-cell hyperplasia among Victozareg-treated patients and 2 cases in comparator-treated patients (13 vs 10 cases per 1000 patient-years) One comparator-treated patient with MTC had pre-treatment serum calcitonin concentrations gt1000 ngL suggesting pre-existing disease All of these cases were diagnosed after thyroidectomy which was prompted by abnormal results on routine protocol-specified measurements of serum calcitonin Five of the six Victozareg-treated patients had elevated calcitonin concentrations at baseline and throughout the trial One Victozareg and one non-Victozareg-treated patient developed elevated calcitonin concentrations while on treatment Calcitonin a biological marker of MTC was measured throughout the clinical development program The serum calcitonin assay used in the Victozareg clinical trials had a lower limit of quantification (LLOQ) of 07 ngL and the upper limit of the refer-ence range was 50 ngL for women and 84 ngL for men At Weeks 26 and 52 in the clinical trials adjusted mean serum calcitonin concentrations were higher in Victozareg-treated patients compared to placebo-treated patients but not compared to patients receiving active comparator At these timepoints the adjusted mean serum calcitonin values (~10 ngL) were just above the LLOQ with between-group differences in adjusted mean serum calcitonin values of approximately 01 ngL or less Among patients with pre-treatment serum calcitonin below the upper limit of the reference range shifts to above the upper limit of the reference range which persisted in subsequent measurements occurred most frequently among patients treated with Victozareg 18 mgday In trials with on-treatment serum calcitonin measurements out to 5-6 months 19 of patients treated with Victozareg 18 mgday developed new and persistent calcitonin elevations above the upper limit of the reference range compared to 08-11 of patients treated with control medication or the 06 and 12 mg doses of Victozareg In trials with on-treatment serum calcitonin measurements out to 12 months 13 of patients treated with Victozareg 18 mgday had new and persistent elevations of calcitonin from below or within the reference range to above the upper limit of the reference range compared to 06 0 and 10 of patients treated with Victozareg 12 mg placebo and active control respectively Otherwise Victozareg did not produce consistent dose-dependent or time-dependent increases in serum calcitonin Patients with MTC usually have calcitonin values gt50 ngL In Victozareg clinical trials among patients with pre-treatment serum calcitonin lt50 ngL one Victozareg-treated patient and no comparator-treated patients developed serum calcitonin gt50 ngL The Victozareg-treated patient who developed serum calcitonin gt50 ngL had an elevated pre-treatment serum calcitonin of 107 ngL that increased to 307 ngL at Week 12 and 535 ngL at the end of the 6-month trial Follow-up serum calcitonin was 223 ngL more than 25 years after the last dose of Victozareg The largest increase in serum calcitonin in a comparator-treated patient was seen with glimepiride in a patient whose serum calcitonin increased from 193 ngL at baseline to 448 ngL at Week 65 and 381 ngL at Week 104 Among patients who began with serum calcitonin lt20 ngL calcitonin elevations to gt20 ngL occurred in 07 of Victozareg-treated patients 03 of placebo-treated patients and 05 of active-comparator-treated patients with an incidence of 11 among patients treated with 18 mgday of Victozareg The clinical significance of these findings is unknown Counsel patients regarding the risk for MTC and the symptoms of thyroid tumors (eg a mass in the neck dysphagia dyspnea or persistent hoarseness) It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate the potential risk of MTC and such monitoring may increase the risk of unnecessary procedures due to low test specificity for serum calcitonin and a high background incidence of thyroid disease Patients with thyroid nodules noted on physical examination or neck imaging obtained for other reasons should be referred to an endocrinologist for further evaluation Although routine monitoring of serum calcitonin is of uncertain value in patients treated with Victozareg if serum calcitonin is measured and found to be elevated the patient should be referred to an endocrinologist for further evaluation Pancreatitis Based on spontaneous post-marketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg After initia-tion of Victozareg observe patients carefully for signs and symptoms of pancreatitis (including persistent severe abdominal pain sometimes radiating to the back and which may or may not be accompanied by vomiting) If pancreatitis is suspected Victozareg should promptly be discontinued and appropriate management should be initiated If pancreatitis is confirmed Victozareg should not be restarted Consider antidiabetic therapies other than Victozareg in patients with a history of pancreatitis In clinical trials of Victozareg there have been 13 cases of pancreatitis among Victozareg-treated patients and 1 case in a comparator (glimepiride) treated patient (27 vs 05 cases per 1000 patient-years) Nine of the 13 cases with Victozareg were reported as acute pancreatitis and four were reported as chronic pancreatitis In one case in a Victozareg-treated patient pancre-atitis with necrosis was observed and led to death however clinical causality could not be established Some patients had other risk factors for pancreatitis such as a history of cholelithiasis or alcohol abuse Use with Medications Known to Cause Hypoglycemia Patients receiving Victozareg in combination with an insulin secretagogue (eg sulfonylurea) or insulin may have an increased risk of hypoglycemia The risk of hypoglycemia may be lowered by a reduction in the dose of sulfonylurea (or other concomitantly admin-istered insulin secretagogues) or insulin Renal Impairment Victozareg has not been found to be directly nephrotoxic in animal studies or clinical trials There have been postmarketing reports of acute renal failure and worsening of chronic renal failure which may sometimes require hemodialysis in Victozareg-treated patients Some of these events were reported in patients without known underlying renal disease A majority of the reported events occurred in patients who had experienced nausea vomiting diarrhea or dehydration Some of the reported events occurred in patients receiving one or more medications known to affect renal function or hydration status Altered renal function has been reversed in many of the reported cases with supportive treatment and discontinuation of potentially causative agents including Victozareg Use caution when initiating or escalating doses of Victozareg in patients with renal impairment Hypersensitivity Reac-tions There have been postmarketing reports of serious hypersensitivity reactions (eg anaphylactic reactions and angioedema) in patients treated with Victozareg If a hypersensitivity reaction occurs the patient should discontinue Victozareg and other suspect medications and promptly seek medical advice Angio-edema has also been reported with other GLP-1 receptor agonists Use caution in a patient with a history of angioedema with another GLP-1 receptor agonist because it is unknown whether such patients will be pre-disposed to angioedema with Victozareg Macrovascular Outcomes There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugADVERSE REACTIONS Clinical Trials Experience Because clinical trials are conducted under widely varying conditions adverse reaction rates observed in the clinical trials of a drug cannot be directly com-pared to rates in the clinical trials of another drug and may not reflect the rates observed in practice The safety of Victozareg has been evaluated in 8 clinical trials A double-blind 52-week monotherapy trial com-pared Victozareg 12 mg daily Victozareg 18 mg daily and glimepiride 8 mg daily A double-blind 26 week add-on to metformin trial compared Victozareg 06 mg once-daily Victozareg 12 mg once-daily Victozareg 18
mg once-daily placebo and glimepiride 4 mg once-daily A double-blind 26 week add-on to glimepiride trial compared Victozareg 06 mg daily Victozareg 12 mg once-daily Victozareg 18 mg once-daily placebo and rosiglitazone 4 mg once-daily A 26 week add-on to metformin + glimepiride trial compared double-blind Victozareg 18 mg once-daily double-blind placebo and open-label insulin glargine once-daily A double-blind 26-week add-on to metformin + rosiglitazone trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and placebo An open-label 26-week add-on to metformin andor sulfonylurea trial com-pared Victozareg 18 mg once-daily and exenatide 10 mcg twice-daily An open-label 26-week add-on to metformin trial compared Victozareg 12 mg once-daily Victozareg 18 mg once-daily and sitagliptin 100 mg once-daily An open-label 26-week trial compared insulin detemir as add-on to Victozareg 18 mg + metformin to continued treatment with Victozareg + metformin alone Withdrawals The incidence of withdrawal due to adverse events was 78 for Victozareg-treated patients and 34 for comparator-treated patients in the five double-blind controlled trials of 26 weeks duration or longer This difference was driven by withdrawals due to gastrointestinal adverse reactions which occurred in 50 of Victozareg-treated patients and 05 of comparator-treated patients In these five trials the most common adverse reactions leading to with-drawal for Victozareg-treated patients were nausea (28 versus 0 for comparator) and vomiting (15 versus 01 for comparator) Withdrawal due to gastrointestinal adverse events mainly occurred during the first 2-3 months of the trials Common adverse reactions Tables 1 2 3 and 4 summarize common adverse reactions (hypoglycemia is discussed separately) reported in seven of the eight controlled trials of 26 weeks duration or longer Most of these adverse reactions were gastrointestinal in nature In the five double-blind clinical trials of 26 weeks duration or longer gastrointestinal adverse reactions were reported in 41 of Victozareg-treated patients and were dose-related Gastrointestinal adverse reactions occurred in 17 of comparator-treated patients Common adverse reactions that occurred at a higher incidence among Victozareg-treated patients included nausea vomiting diarrhea dyspepsia and constipation In the five dou-ble-blind and three open-label clinical trials of 26 weeks duration or longer the percentage of patients who reported nausea declined over time In the five double-blind trials approximately 13 of Victozareg-treated patients and 2 of comparator-treated patients reported nausea during the first 2 weeks of treatment In the 26-week open-label trial comparing Victozareg to exenatide both in combination with metformin andor sulfo-nylurea gastrointestinal adverse reactions were reported at a similar incidence in the Victozareg and exenatide treatment groups (Table 3) In the 26-week open-label trial comparing Victozareg 12 mg Victozareg 18 mg and sitagliptin 100 mg all in combination with metformin gastrointestinal adverse reactions were reported at a higher incidence with Victozareg than sitagliptin (Table 4) In the remaining 26-week trial all patients received Victozareg 18 mg + metformin during a 12-week run-in period During the run-in period 167 patients (17 of enrolled total) withdrew from the trial 76 (46 of withdrawals) of these patients doing so because of gastrointestinal adverse reactions and 15 (9 of withdrawals) doing so due to other adverse events Only those patients who completed the run-in period with inadequate glycemic control were randomized to 26 weeks of add-on therapy with insulin detemir or continued unchanged treatment with Victozareg 18 mg + metformin During this randomized 26-week period diarrhea was the only adverse reaction reported in ge5 of patients treated with Victozareg 18 mg + metformin + insulin detemir (117) and greater than in patients treated with Victozareg 18 mg and metformin alone (69)Table 1 Adverse reactions reported in ge5 of Victozareg-treated patients in a 52-week monotherapy trial
All Victozareg N = 497 Glimepiride N = 248Adverse Reaction () ()Nausea 284 85Diarrhea 171 89Vomiting 109 36Constipation 99 48Headache 91 93
Table 2 Adverse reactions reported in ge5 of Victozareg-treated patients and occurring more frequently with Victozareg compared to placebo 26-week combination therapy trials
Add-on to Metformin TrialAll Victozareg + Metformin
N = 724Placebo + Metformin
N = 121Glimepiride + Metformin
N = 242Adverse Reaction () () ()Nausea 152 41 33Diarrhea 109 41 37Headache 90 66 95Vomiting 65 08 04
Add-on to Glimepiride TrialAll Victozareg +
Glimepiride N = 695Placebo + Glimepiride
N = 114Rosiglitazone +
Glimepiride N = 231Adverse Reaction () () ()Nausea 75 18 26Diarrhea 72 18 22Constipation 53 09 17Dyspepsia 52 09 26
Add-on to Metformin + GlimepirideVictozareg 18 + Metformin + Glimepiride N = 230
Placebo + Metformin + Glimepiride N = 114
Glargine + Metformin + Glimepiride N = 232
Adverse Reaction () () ()Nausea 139 35 13Diarrhea 100 53 13Headache 96 79 56Dyspepsia 65 09 17Vomiting 65 35 04
Add-on to Metformin + RosiglitazoneAll Victozareg + Metformin +
Rosiglitazone N = 355Placebo + Metformin + Rosiglitazone
N = 175Adverse Reaction () ()Nausea 346 86Diarrhea 141 63Vomiting 124 29Headache 82 46Constipation 51 11
Table 3 Adverse Reactions reported in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Exenatide
Victozareg 18 mg once daily + metformin andor sulfonylurea
N = 235
Exenatide 10 mcg twice daily + metformin andor sulfonylurea
N = 232Adverse Reaction () ()Nausea 255 280Diarrhea 123 121Headache 89 103Dyspepsia 89 47Vomiting 60 99Constipation 51 26
Table 4 Adverse Reactions in ge5 of Victozareg-treated patients in a 26-Week Open-Label Trial versus Sitagliptin
All Victozareg + metformin N = 439
Sitagliptin 100 mgday + metformin N = 219
Adverse Reaction () ()Nausea 239 46Headache 103 100Diarrhea 93 46Vomiting 87 41
Immunogenicity Consistent with the potentially immunogenic properties of protein and peptide pharma-ceuticals patients treated with Victozareg may develop anti-liraglutide antibodies Approximately 50-70 of Victozareg-treated patients in the five double-blind clinical trials of 26 weeks duration or longer were tested for the presence of anti-liraglutide antibodies at the end of treatment Low titers (concentrations not requiring dilution of serum) of anti-liraglutide antibodies were detected in 86 of these Victozareg-treated patients Sampling was not performed uniformly across all patients in the clinical trials and this may have resulted in an underestimate of the actual percentage of patients who developed antibodies Cross-reacting anti-liraglutide antibodies to native glucagon-like peptide-1 (GLP-1) occurred in 69 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 48 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials These cross-reacting antibodies were not tested
for neutralizing effect against native GLP-1 and thus the potential for clinically significant neutralization of native GLP-1 was not assessed Antibodies that had a neutralizing effect on liraglutide in an in vitro assay occurred in 23 of the Victozareg-treated patients in the double-blind 52-week monotherapy trial and in 10 of the Victozareg-treated patients in the double-blind 26-week add-on combination therapy trials Among Victozareg-treated patients who developed anti-liraglutide antibodies the most common category of adverse events was that of infections which occurred among 40 of these patients compared to 36 34 and 35 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively The specific infections which occurred with greater frequency among Victozareg-treated anti-body-positive patients were primarily nonserious upper respiratory tract infections which occurred among 11 of Victozareg-treated antibody-positive patients and among 7 7 and 5 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Among Victozareg-treated antibody-negative patients the most common category of adverse events was that of gastrointestinal events which occurred in 43 18 and 19 of antibody-negative Victozareg-treated placebo-treated and active-control-treated patients respectively Antibody formation was not associated with reduced efficacy of Victozareg when comparing mean HbA1c of all antibody-positive and all antibody-negative patients However the 3 patients with the highest titers of anti-liraglutide antibodies had no reduction in HbA1c with Victozareg treatment In the five double-blind clinical trials of Victozareg events from a composite of adverse events potentially related to immunogenicity (eg urticaria angioedema) occurred among 08 of Victozareg-treated patients and among 04 of comparator-treated patients Urticaria accounted for approximately one-half of the events in this composite for Victozareg-treated patients Patients who developed anti-liraglutide antibodies were not more likely to develop events from the immunogenicity events composite than were patients who did not develop anti-liraglutide antibodies Injection site reactions Injection site reactions (eg injection site rash erythema) were reported in approximately 2 of Victozareg-treated patients in the five double-blind clinical trials of at least 26 weeks duration Less than 02 of Victozareg-treated patients discontinued due to injection site reactions Papillary thyroid carcinoma In clinical trials of Victozareg there were 7 reported cases of papillary thyroid carcinoma in patients treated with Victozareg and 1 case in a comparator-treated patient (15 vs 05 cases per 1000 patient-years) Most of these papillary thyroid carcinomas were lt1 cm in greatest diameter and were diagnosed in surgical pathology specimens after thyroidectomy prompted by findings on protocol-specified screening with serum calcitonin or thyroid ultrasound Hypoglycemia In the eight clinical trials of at least 26 weeks duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients (23 cases per 1000 patient-years) and in two exenatide-treated patients Of these 11 Victozareg-treated patients six patients were concomitantly using metformin and a sulfonylurea one was concomitantly using a sulfonylurea two were concomitantly using metformin (blood glucose values were 65 and 94 mgdL) and two were using Victozareg as monotherapy (one of these patients was undergoing an intravenous glucose tolerance test and the other was receiving insulin as treat-ment during a hospital stay) For these two patients on Victozareg monotherapy the insulin treatment was the likely explanation for the hypoglycemia In the 26-week open-label trial comparing Victozareg to sitagliptin the incidence of hypoglycemic events defined as symptoms accompanied by a fingerstick glucose lt56 mgdL was comparable among the treatment groups (approximately 5)Table 5 Incidence () and Rate (episodespatient year) of Hypoglycemia in the 52-Week Monotherapy Trial and in the 26-Week Combination Therapy Trials
Victozareg Treatment Active Comparator Placebo ComparatorMonotherapy Victozareg (N = 497) Glimepiride (N = 248) NonePatient not able to self-treat 0 0 mdashPatient able to self-treat 97 (024) 250 (166) mdashNot classified 12 (003) 24 (004) mdashAdd-on to Metformin Victozareg + Metformin
(N = 724)Glimepiride +
Metformin (N = 242)Placebo + Metformin
(N = 121)Patient not able to self-treat 01 (0001) 0 0Patient able to self-treat 36 (005) 223 (087) 25 (006)Add-on to Victozareg + Metformin
Insulin detemir + Victozareg + Metformin
(N = 163)
Continued Victozareg + Metformin alone
(N = 158)
None
Patient not able to self-treat 0 0 mdashPatient able to self-treat 92 (029) 13 (003) mdashAdd-on to Glimepiride Victozareg +
Glimepiride (N = 695)Rosiglitazone +
Glimepiride (N = 231)Placebo +
Glimepiride (N = 114)Patient not able to self-treat 01 (0003) 0 0Patient able to self-treat 75 (038) 43 (012) 26 (017)Not classified 09 (005) 09 (002) 0Add-on to Metformin + Rosiglitazone
Victozareg + Metformin + Rosiglitazone
(N = 355)
None
Placebo + Metformin + Rosiglitazone
(N = 175)Patient not able to self-treat 0 mdash 0Patient able to self-treat 79 (049) mdash 46 (015)Not classified 06 (001) mdash 11 (003)Add-on to Metformin + Glimepiride
Victozareg + Metformin + Glimepiride
(N = 230)
Insulin glargine + Metformin +
Glimepiride (N = 232)
Placebo + Metformin + Glimepiride
(N = 114)Patient not able to self-treat 22 (006) 0 0Patient able to self-treat 274 (116) 289 (129) 167 (095)Not classified 0 17 (004) 0
One patient is an outlier and was excluded due to 25 hypoglycemic episodes that the patient was able to self-treat This patient had a history of frequent hypoglycemia prior to the studyIn a pooled analysis of clinical trials the incidence rate (per 1000 patient-years) for malignant neoplasms (based on investigator-reported events medical history pathology reports and surgical reports from both blinded and open-label study periods) was 109 for Victozareg 63 for placebo and 72 for active comparator After excluding papillary thyroid carcinoma events [see Adverse Reactions] no particular cancer cell type predominated Seven malignant neoplasm events were reported beyond 1 year of exposure to study medica-tion six events among Victozareg-treated patients (4 colon 1 prostate and 1 nasopharyngeal) no events with placebo and one event with active comparator (colon) Causality has not been established Laboratory Tests In the five clinical trials of at least 26 weeks duration mildly elevated serum bilirubin concentrations (elevations to no more than twice the upper limit of the reference range) occurred in 40 of Victozareg-treated patients 21 of placebo-treated patients and 35 of active-comparator-treated patients This finding was not accompanied by abnormalities in other liver tests The significance of this isolated finding is unknown Vital signs Victozareg did not have adverse effects on blood pressure Mean increases from baseline in heart rate of 2 to 3 beats per minute have been observed with Victozareg compared to placebo The long-term clinical effects of the increase in pulse rate have not been established Post-Marketing Experience The following additional adverse reactions have been reported during post-approval use of Victozareg Because these events are reported voluntarily from a population of uncertain size it is generally not possible to reli-ably estimate their frequency or establish a causal relationship to drug exposure Dehydration resulting from nausea vomiting and diarrhea Increased serum creatinine acute renal failure or worsening of chronic renal failure sometimes requiring hemodialysis Angioedema and anaphylactic reactions Allergic reactions rash and pruritus Acute pancreatitis hemorrhagic and necrotizing pancreatitis sometimes resulting in deathOVERDOSAGE Overdoses have been reported in clinical trials and post-marketing use of Victozareg Effects have included severe nausea and severe vomiting In the event of overdosage appropriate supportive treat-ment should be initiated according to the patientrsquos clinical signs and symptomsMore detailed information is available upon request For information about Victozareg contact Novo Nordisk Inc 800 Scudders Mill Road Plainsboro NJ 08536 1minus877-484-2869Date of Issue April 16 2013 Version 6Manufactured by Novo Nordisk AS DK-2880 Bagsvaerd DenmarkVictozareg is covered by US Patent Nos 6268343 6458924 7235627 8114833 and other patents pending Victozareg Pen is covered by US Patent Nos 6004297 RE 43834 RE 41956 and other patents pendingcopy 2010-2013 Novo Nordisk 0513-00015682-1 52013
S975rdquo
S1
22
5rdquo
VICU3X1498_B_2_0_Journal_Ad_Tabloid_Resize_BS_r5indd 1 111913 809 PM
The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks

The change begins at VictozaProcom
Victozareg is a registered trademark of Novo Nordisk AScopy 2013 Novo Nordisk All rights reserved 1013-00018617-1 December 2013
Indications and UsageVictozareg (liraglutide [rDNA origin] injection) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitusBecause of the uncertain relevance of the rodent thyroid C-cell tumor findings to humans prescribe Victozareg only to patients for whom the potential benefits are considered to outweigh the potential risk Victozareg is not recommended as first-line therapy for patients who have inadequate glycemic control on diet and exerciseBased on spontaneous postmarketing reports acute pancreatitis including fatal and non-fatal hemorrhagic or necrotizing pancreatitis has been observed in patients treated with Victozareg Victozareg has not been studied in patients with a history of pancreatitis It is unknown whether patients with a history of pancreatitis are at increased risk for pancreatitis while using Victozareg Other antidiabetic therapies should be considered in patients with a history of pancreatitisVictozareg is not a substitute for insulin Victozareg should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis as it would not be effective in these settingsVictozareg has not been studied in combination with prandial insulin
Important Safety InformationLiraglutide causes dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures in both genders of rats and mice It is unknown whether Victozareg causes thyroid C-cell tumors including medullary thyroid carcinoma (MTC) in humans as human relevance could not be ruled out by clinical or nonclinical studies Victozareg is contraindicated in patients with a personal or family history of MTC and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) Based on the findings in rodents monitoring with serum calcitonin or thyroid ultrasound was performed during clinical trials but this may have increased the number of unnecessary thyroid surgeries It is unknown whether monitoring with serum calcitonin or thyroid ultrasound will mitigate human risk of thyroid C-cell tumors Patients should be counseled regarding the risk and symptoms of thyroid tumorsDo not use in patients with a prior serious hypersensitivity reaction to Victozareg or to any of the product componentsPostmarketing reports including fatal and non-fatal hemorrhagic or necrotizing pancreatitis Discontinue promptly if pancreatitis is suspected Do not restart if
pancreatitis is confirmed Consider other antidiabetic therapies in patients with a history of pancreatitisWhen Victozareg is used with an insulin secretagogue (eg a sulfonylurea) or insulin serious hypoglycemia can occur Consider lowering the dose of the insulin secretagogue or insulin to reduce the risk of hypoglycemiaRenal impairment has been reported postmarketing usually in association with nausea vomiting diarrhea or dehydration which may sometimes require hemodialysis Use caution when initiating or escalating doses of Victozareg in patients with renal impairmentSerious hypersensitivity reactions (eg anaphylaxis and angioedema) have been reported during postmarketing use of Victozareg If symptoms of hypersensitivity reactions occur patients must stop taking Victozareg and seek medical advice promptlyThere have been no studies establishing conclusive evidence of macrovascular risk reduction with Victozareg or any other antidiabetic drugThe most common adverse reactions reported in ge5 of patients treated with Victozareg and more commonly than in patients treated with placebo are headache nausea diarrhea dyspepsia constipation and anti-liraglutide antibody formation Immunogenicity-related events including urticaria were more common among Victozareg-treated patients (08) than among comparator-treated patients (04) in clinical trialsVictozareg has not been studied in type 2 diabetes patients below 18 years of age and is not recommended for use in pediatric patientsThere is limited data in patients with renal or hepatic impairment In a 52-week monotherapy study (n=745) with a 52-week extension the adverse reactions reported in ge 5 of patients treated with Victozareg 18 mg Victozareg 12 mg or glimepiride were constipation (118 84 and 48) diarrhea (195 175 and 93) flatulence (53 16 and 20) nausea (305 287 and 85) vomiting (102 131 and 40) fatigue (53 32 and 36) bronchitis (37 60 and 44) influenza (110 92 and 85) nasopharyngitis (65 92 and 73) sinusitis (73 84 and 73) upper respiratory tract infection (134 143 and 89) urinary tract infection (61 104 and 52) arthralgia (24 44 and 60) back pain (73 72 and 69) pain in extremity (61 36 and 32) dizziness (77 52 and 52) headache (73 112 and 93) depression (57 32 and 20) cough (57 20 and 44) and hypertension (45 56 and 69)
Please see brief summary of Prescribing Information on adjacent page
Victozaregmdasha force for change in type 2 diabetes
Weight loss up to 55 lbab
Low rate of hypoglycemiac
Reductions up to -11a
A change with powerful long-lasting benefits
a18 mg dose when used alone for 52 weeks bVictozareg is not indicated for the management of obesity Weight change was a secondary end point in clinical trials cIn the 8 clinical trials of at least 26 weeksrsquo duration hypoglycemia requiring the assistance of another person for treatment occurred in 11 Victozareg-treated patients
A 52-week double-blind double-dummy active-controlled parallel-group multicenter study Patients with type 2 diabetes (N=745) were randomized to receive once-daily Victozareg 12 mg (n=251) Victozareg 18 mg (n=246) or glimepiride 8 mg (n=248) The primary outcome was change in A1C after 52 weeks