mitral valve prolapse-click syndrome in twins
TRANSCRIPT

Anterior conduction delay
To the Editor: Anterior (left middle fascicular) delay is an important cause
of prominent right precordial R waves, and was properly diagnosed by Drs. Burchell and Reed (their Fig. 3) in their paper on machine processed electrocardiography diagnosis. 1
This phenomenon is often encountered in clinical electro- cardiography and vectorcardiography practice and should be reported as "large anterior QRS forces consistent with dorsal infarction or anterior conduction delay, if right ventricular hypertrophy is clinically ruled out."
The vectorcardiographic loops in such patients are indistin- guishable from some cases of right ventricular hypertrophy and from most cases of true dorsal infarction. When anglog- raphy and ventriculography are carried out in such patients (as in Burchell and Reed's reported case), the anterior descending artery is most commonly involved and indeed may be the only vessel involved.'-'
Of great interest in their case is the reporte d disappearance of the large anterior forces following bypass graft of the left anterior descending artery. This certainly is consistent with a conduction delay, o n an ischemic basis, improved after bypass.
Irwin Hoffman, M.D., F.A.C.C. Associate Professor of Medicine
State University of Ne w York a t Stony Brook
South Shore Cardiology Group 123 Grove Ave.
Cedarhurst, N. Y. 11516
REFERENCES 1.
2.
Burchell, H., and Reed, J.: A test experience with a machine-processed electrocardiography diagnosis: The recognition of "normal" and some specific patterns," AM. HEART J. 92:773, i976. Hoffman, I., Mehta, J., Hilsenrath, J., and Hamby, R. I.: Anterior conduction delay: A POSsible cause for promi- nent anterior QRS forces, J. Electrocardiol, 9"15, 1976.
Noise reduction in ambulatory monitoring
To the Editor: Monitoring the electrocardiogram for long periods has
become a standard and useful diagnostic procedure. Analysis by high sPeed scanning (H01ter technique) or computer is often impeded by the presence of artifacts due to electrode movement: Electronic filtering m a y improve the diagnostic yield at the price Of distorting the electrocardiogram. An expensive solutipn is offered by computer artifact recognition programs, but even these have shortcomings.
DU e t o the widesprea d use O f monitoring equipment we feel that drawing attention t o an inexpensive method of reducing artifacts a t source would be of value.
The origin of artifacts due to movement is complex but is mainly due to the presence of a direct potential of about 10 to 20 mV. across a skin electrode electrode interface, This potential is the resultant of electrolytic effects, possibl e leakage in the input circuitry of the amplifier, and the skin potentials of Tarchan0ff.
Letters to the Editor
Movement of the electrode on the skin causes a variation in contact resistance which is reflected as a changing potentia ! at the input terminal of the amplifier (Ohm's law). Removing the epidermis may reduce these skin potentials and resultant artifacts by a factor of 20.
We clean the skin with ether to ensure adhesion. A 5 mm. area is marked with a colored fiber tipped pen. A 6 ram. diamond abrasive dental bit in a high sPeed (30,000 r~p.m:) Dremel Moto-tool (Model 258, Dremel Mfg. Co . Racine, Wisc.; U.S.A.) i s briefly touched to the marked area, lea~ng a 2 to 3 mm. spot where the coloring and therefore Outer layers Of epidermis have been removed. Any pain"experienced or blood drawn indicates that the epidermis has been penetrated, and the procedure should then be repeated in an adjacent spot using less pressur e on the drill.
Clean silver-silver chloride cup electrodes (e.g., Hewlett- Packard, Cat. No. 14058) are carefully filled with electrocar- diographic paste and applied to the prepared skin area with standard double-sided adhesive discs. The discs are then further secured with an 8 cm. square self adhering foam pa d (Reston brand, Medical Products Division, 3M Company, Minnesota Mining & Manufacturing Co., 3M center, St. Paul, Minn. 55707).
The electrode wires are taped to the skin with a Reston foam pad some distance from the electrode to prevent traction being transmitted to the electrode. A further precaution against displacement of the electrodes during the summer months is to harness the patient With a disposable tight fitting ~est, quickly an d easily made from Elastomesh, No. 5, Smith and Nephew, Ltd.
Using this method we have performed over 1500 6-hour ambulant Holter tape recordings to analyze ventricular ectopic beats in postmyocardial infarction patients,' with l~ss than 5 per cent of tapes showing artifacts that impede recognition of arrhythmias.
A.L. van Gelder, M.B.Ch.B. D.P. Myburgh M.B.Ch.B., F.A.C.C.
Military Medical Institute Verwoerdburg P.O. Tek 0133
Republic of South Africa
REFERENCE 1. Myburgh, D. P., and van Gelder, A. L.: Ventricular
ectopic activity in chronic ischaemic heart disease, S. Aft. Med. J. 50:1856, 1976.
Mitral valve prolapse-click syndrome in twins
To the Editor: W e recently have been involved personally and profession-
ally in the evaluation of identical twin subjects with echocar- diographically documented mitraI valve prolapse-click syn- drome. Rarely has this problem been reported in twins and not previously with echocardiographic confirmation. Case reports
Case 1: J. B. G., an asymptomatic, currently healthy 32- year-old physician, without history of cardiovascular illness, Underwent a routine physical examination on discharge fro m the armed services. Numerous previous physical examinations
American Hear t Journal 81 3
Letters to the Editor
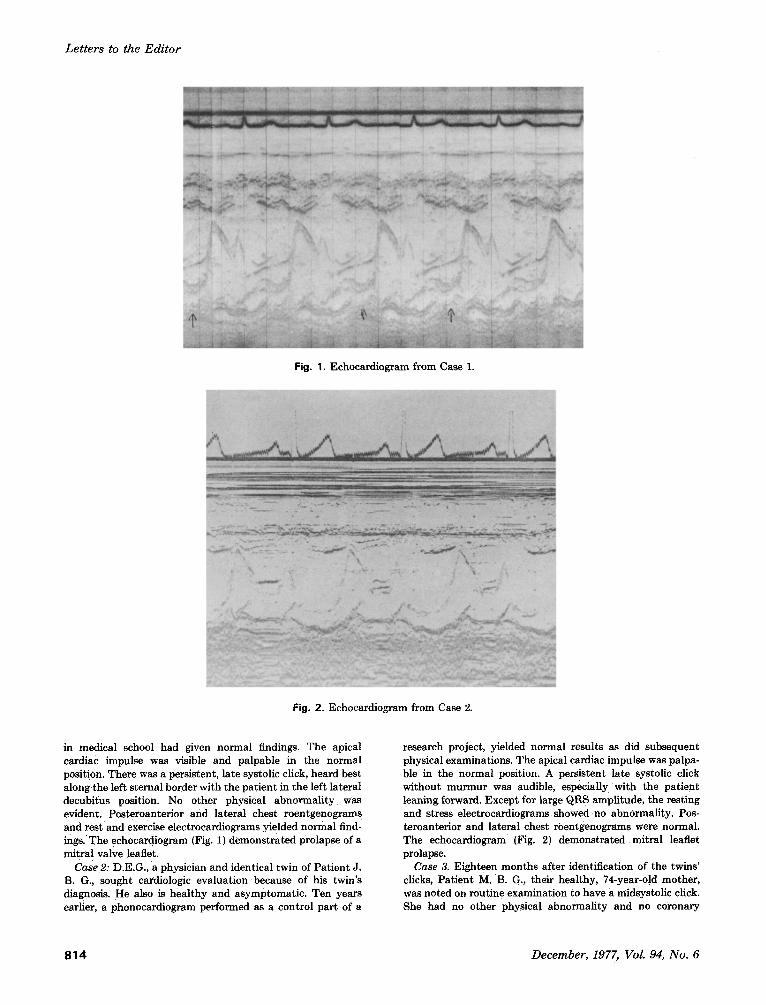
Fig. 1. Echocardiogram from Case 1.
Fig. 2. Echocardiogram from Case 2.
in medical school had given normal findings. The apical cardiac impulse was visible and palpable in the normal position. There was a persistent, late systolic click, heard best along the left sternal border with the patient in the left lateral decubitus position. No other physical abnormality was evident. Posteroanterior and lateral chest roentgenogram s and rest and exercise electrocardiograms yielded normal find- ings.'The echocardiogram {Fig. 1) demonstrated prolapse of a mitral valve leaflet.
Case 2: D.E.G., a physician and identical twin of Patient J. B. G:, sought cardiologic evaluat ion because of his twin's diagnosis. He also is healthy and asymptomatic. Ten years earlier, a phonocardiogram performed as a control part of a
research project, yielded normal results as did subsequent physical examinations. The apical cardiac impulse was palpa- ble in the normal position. A persistent late systolic click without murmur was audible, especially with the patient leaning forward. Except for large QRS amplitude, the resting and stress electrocardiograms showed no abnormality. Pos- teroanterior and lateral Chest roentgenograms were normal. The echocardiogram (Fig. 2)demonstra ted mitral leaflet prolapse.
Case 3. Eighteen months after identification of the twins' clicks, Patient M. B. G., their healthy, 74-year-old mother, was noted on routine examination to have a midsystoiic click. She had no other physical abnormality and no coronary
8 1 4 December, 1977, Vol. 94, No. 6

Letters to the Editor
artery disease. The electrocardiogram and posteroanterinr and lateral chest roentgenograms were normal. An echocardio- gram showed mitral leaflet prolapse. The twin's father, now dead, had no known evidence of cardiac click, or murmur. There are no other siblings.
Discussion. Only two previous reports of mitral valve prolapse-click syndrome involve twins. In both sets, associated congenital defects may have been present. The first report 1 concerned 17-year-old girls, both with midsystolic clicks. One had a late systolic murmur, and the other had aortic insuffi- ciency. Their mother also had a midsystolic click. The second twinship 2 involved 18-year-old girls; the first had a midsystolic click alone, and the second had a midsystolic crick and a late systolic murmur. Both had high-arched palates. Neither parent was affected. Echocardiographic data were not mentioned in either of the two accounts. 1 ~
In the patients presented here, the late discovery of clicks, the fact tha t both twins had been examined previously on multiple occasions without auscultatory abnormalities, and the previously normal phonocardiographic s tudy in Pat ient D. E. G. are consistent with the na tura l history of the disorder. 2-~ Uncommon and of greater note is the absence of associated skeletal abnormalities, of other cardiac auscultatory or elec-
trocardiographic findings (other than QRS ampli tude in Pat ient D. E. G.), and of exercise-induced a~rhythmias. ~
Donald E. Girard, M.D. Department of Medicine
University of Oregon Health Sciences Center
3181 S.W. Sam Jackson Blvd. Portland, Ore. 97201
John B. Girard, M.D. Department of Obstetrics-Gynecology
University of California San Francisco, Calif.
REFERENCES
1. Rizzon, P., Biascon, G., Brindicci, G., et al: Familial syndrome of midsystolic click and late systolic murmur, Br. Heart J. 35:245, 1973. Jeresaty, R. M.: Mitral valve prolapse-click syndrome, Progr. Cardiovasc. Dis. 15:623, 1973. Devereux, R. B., Perloff, J. K., Reichel N., et al: Mitral valve prolapse, Circulation 54.'3, 1976. Aranda, J. M., Befeler, B., El*Sherif, N., et al: Mitral valve prolapse: Recent concepts and observations, Am. J. Med. 60:997, 1976.
American Hear t Journal 815