miliary mottling -- rare cause - cpa chennai a andal department of pediatrics ... kanchi kamakoti...
TRANSCRIPT
DR ARATHI SRINIVASAN
FELLOW IN PEDIATRIC HEMATO ONCOLOGY
DR A ANDAL
DEPARTMENT OF PEDIATRICS
DR JULIUS XAVIER SCOTT
DEPARTMENT OF PEDIATRIC HEMATO ONCOLOGY
KANCHI KAMAKOTI CHILDS TRUST HOSPITAL
*MILIARY MOTTLING --
RARE CAUSE
*3 yrs old female child
*Intermittent fever of six months duration
*Respiratory symptoms like recurrent cough, fever and wheeze.
*Suspected history of contact with tuberculosis
*Preliminary work up for tuberculosis were negative
(erythrocyte sedimentation rate, Mantoux test, Chest X ray,
gastric juice for Acid Fast Bacilli)
*Started on preventers for recurrent wheeze
1 year later
Fever and respiratory symptoms like cough
and wheezing
splenohepatomegaly ( liver 3 cms below right
costal margin, spleen 5 cms below left costal
margin)
RS: bilateral diffuse crepitations
Chest x ray
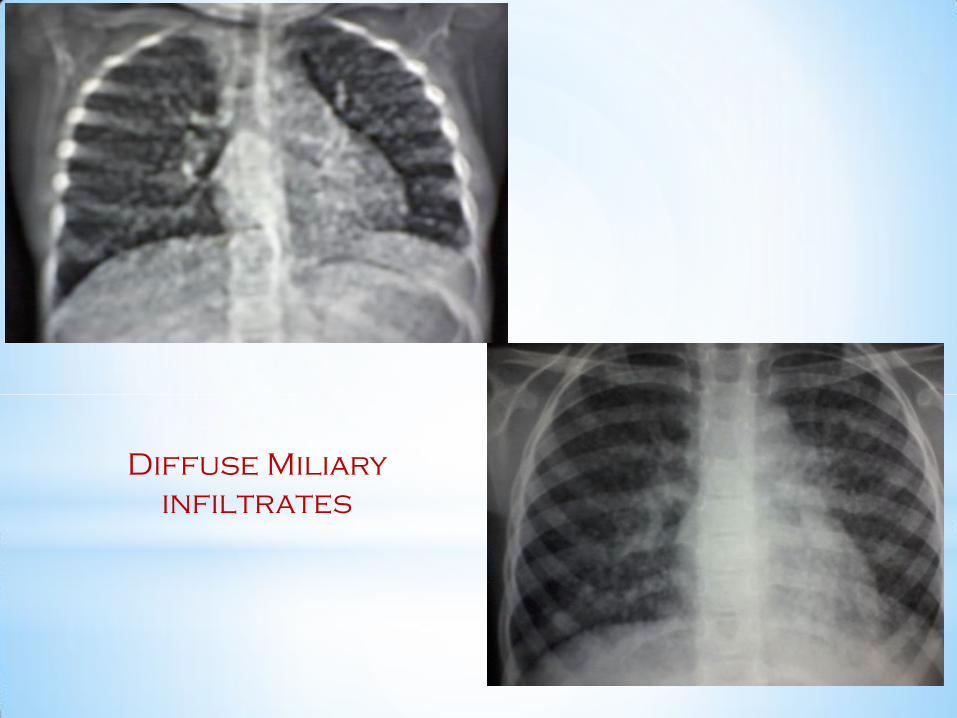
Diffuse Miliary
infiltrates
*Re work up:
• Neutrophilic leucocytosis/ AEC: normal
• Normal immunoglobulin levels
• HIV: negative
*Treated with antibiotics
*Planned for bronchoscopy /lung biopsy
*Started on ATT
6 months later
Recurrent cough, fever and
progressive respiratory distress
Crepitations and splenohepatomegaly
• Neutrophilic leucocytosis (40400 cells/cumm)
• C-Reactive Protein: raised/ ESR: raised
• Chest radiograph : bilateral pulmonary
infiltrates worsening than before

*High Resolution
chest CT ---
bilateral diffuse
pulmonary
*Broncho alveolar lavage fluid analysis
for tuberculosis/other infections -- negative
*Bone marrow aspiration – normal
Thoracoscopic lung biopsy
Non Hodgkins
Lymphoma -- Diffuse
large B cell lymphoma
Risk stratified – Group B NHL
Chemotherapy – COP
reduction
Repeat chest X ray…….

*Repeat chest X ray: clearance of the pulmonary infiltrates
*
*Completed 9 cycles of chemotherapy
*PET scan negative at end of treatment
*Doing well
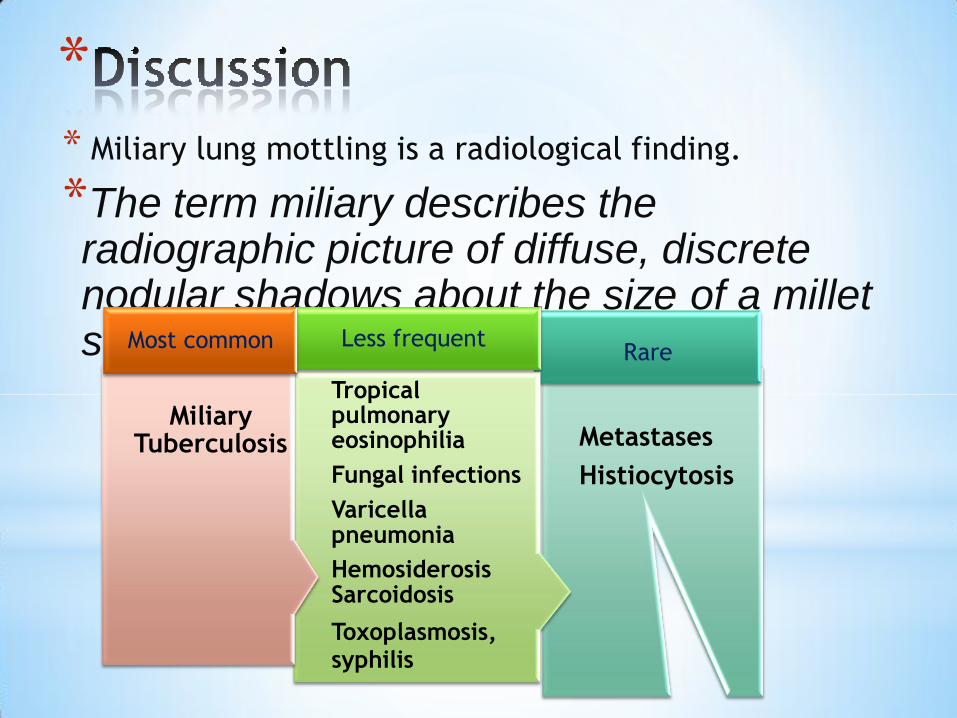
** Miliary lung mottling is a radiological finding.
*The term miliary describes the radiographic picture of diffuse, discrete nodular shadows about the size of a millet seed (2mm)
Metastases
Histiocytosis
Rare
Tropical pulmonary eosinophilia
Fungal infections
Varicella pneumonia
HemosiderosisSarcoidosis
Toxoplasmosis, syphilis
Less frequent
Miliary Tuberculosis
Most common
* Chest X ray and Miliary TB
*Localizes the site of pathology
*Relevant clinical setting + radiological lesions
( miliary, hilar/paratracheal lymphadenopathy /
fibrocaseous cavitatory lesions ) ----
may strongly suggest TB
*Clinical presentations of Childhood
Non Hodgkins Lymphoma*Precursor lymphoid neoplasms
T-lymphoblastic lymphoma --- Anterior mediastinal mass
B-lymphoblastic lymphoma --- Cutaneous masses,
isolated lymph node masses,
primary bone lymphoma
*Mature B-cell neoplasms
Burkitt lymphoma --- Abdominal masses,GIT
Waldeyer's ring
Diffuse large B-cell lymphoma --- Nodes, abdominal masses,
bone
*Mature T-cell neoplasms
Anaplastic large cell lymphoma --- Skin, nodes, bone
Peripheral T-cell lymphoma
*
*Miliary infiltrates in Non-Hodgkin's lymphoma are
extremely rare.
*Primary pulmonary Non Hodgkins lymphoma is very rare and
accounts 0.4% of all lymphomas
*Involvement of the lung with the lymphomatous process occurs
in 5-20% of patients at diagnosis and eventually in 20-60%.

*Review of literature*Miyake S, Yoshizawa Y, Ohkouchi Y, Kurashima A, Hebisawa A. Non-
Hodgkin's Lymphoma with Pulmonary Infiltrates Mimicking Miliary
Tuberculosis. Internal Medicine. 1997; 36: 420-423.\
*Wrobel T, Dzietczenia J, Sobieszek MP, Mazur G, Piwkowski P. Primary
pulmonary diffuse large B-cell lymphoma. Am. J. Hematol. 2011;
00:000–000. Published online in Wiley Online Library
(wileyonlinelibrary.com). DOI: 10.1002/ajh.22116.
*Close PM, Macrae MB, Hammond JM, Aronson I, Johnson CA, Potgieter
PD,et al. Anaplastic large-cell Ki-1 lymphoma. Pulmonary presentation
mimicking miliary tuberculosis. Am J Clin Pathol. 1993; 99:631-6.
*Scott JX, Gnananayagam EJ, Sundaravalli EKR,Thomas G, Shanthly N,
Kirubakaran C. Unusual Cause for Miliary Lung Mottling in a Child.
Indian J Chest Dis Allied Sci 2004; 46 : 291-293
* Take home messagePediatrician’s Perspective Miliary TB is the most common cause for miliary mottling in a developing country, but not the only cause, especially when there is no bacteriological evidence of tuberculosis or if there is no expected response.
The importance of obtaining tissue diagnosis rather than empirical ATT and missing occult malignancies needs to be emphasized. Pediatric Oncologist’s Perspective Non Hodgkins lymphoma presents commonly as tumors in abdomen.
Though Diffuse large B cell lymphoma occurs only in 10% cases of primary pulmonary NHL, rare possibility of B Type NHL should be considered.
Miliary
infiltrates

*THANK YOU