midgut carcinoid tumours
TRANSCRIPT

ACTAUNIVERSITATISUPSALIENSISUPPSALA2007
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 216
Midgut Carcinoid Tumours
New Diagnostic Procedures and Treatment
STAFFAN WELIN
ISSN 1651-6206ISBN 978-91-554-6773-9urn:nbn:se:uu:diva-7436


To my family,
Klara, Hampus and Ellen

List of Papers
I Staffan Welin, Mats Stridsberg, Janet Cunningham, Dan Gran-berg, Britt Skogseid, Kjell Öberg, Barbro Eriksson, Eva T. Jan-son. Elevated Plasma Chromogranin A is the First Indication of Recurrence in Radically Operated Midgut Carcinoid Tumours. (submitted)
II Staffan Welin, Kjell Öberg, Dan Granberg, Henrik Kindmark, Britt Skogseid, Eva T. Janson, Barbro Eriksson. Survival and Clinical Characteristics in 284 Patients with Malignant Midgut Carcinoid Tumors (Manuscript)
III Staffan V. Welin, Eva Tiensuu Janson, Anders Sundin, Mats Stridsberg, Erik Lavenius, Dan Granberg, Britt Skogseid, Kjell E. Öberg, Barbro K. Eriksson. High-dose treatment with a long-acting somatostatin analogue in patients with advanced midgut carcinoid tumours. European Journal of Endocrinology 151:107-112 (2004)
IV S Welin, M-L Fjällskog, J Saras, B Eriksson, E T Janson. Ex-pression of tyrosine kinase receptors in malignant midgut carci-noid tumours. Neuroendocrinology 84:42-48 (2006)

Contents
Introduction...................................................................................................11Midgut carcinoid tumours ........................................................................11The carcinoid syndrome ...........................................................................12Hormone analysis.....................................................................................13
Urinary 5-hydroxyindoleacetic acid ....................................................13Plasma chromogranin A ......................................................................13Tachykinins .........................................................................................13
Somatostatin receptors .............................................................................14Tyrosine kinase receptors.........................................................................15
PDGFR ................................................................................................15EGFR...................................................................................................15C-Kit ....................................................................................................16
Treatment .................................................................................................17Surgery.................................................................................................17Alpha-interferon ..................................................................................18Somatostatin and its analogues ............................................................19Liver embolisation ...............................................................................20Radiofrequency ablation......................................................................21Peptide receptor radionuclide therapy .................................................21
Aims of the investigation ..............................................................................22
Material and methods....................................................................................23Patients .....................................................................................................23Tumour tissue...........................................................................................24Immunohistochemistry.............................................................................24Biochemistry ............................................................................................26Radiology .................................................................................................26Somatostatin receptor scintigraphy ..........................................................27Positron emission tomography .................................................................27Definition of response ..............................................................................27Definition of recurrence ...........................................................................28Therapy ....................................................................................................28Statistics ...................................................................................................29
Results...........................................................................................................30Recurrences in radically operated midgut carcinoid tumors (paper I) .....30Survival and Clinical Characteristics in 284 Patients with Malignant Midgut Carcinoid Tumors (Paper II)........................................................31Treatment with high-dose octreotide pamoate (paper III)........................32
Biochemical and radiological responses..............................................32Immunohistochemistry ........................................................................32
Tyrosine kinase receptor expression (paper IV).......................................33
Summary.......................................................................................................35
Discussion.....................................................................................................37
Conclusion ....................................................................................................43
Acknowledgements.......................................................................................44
References.....................................................................................................46
Abbreviations
CgA Chromogranin A P-CgA Plasma chromogranin A U-5HIAA Urinary 5-hydroxyindoleacetic acid IFN Alpha-interferon RF Radiofrequency PDGFR Platelet derived growth factor receptor EGFR Epidermal growth factor receptor GH Growth hormone VEGF Vascular endothelial growth factor sst Somatostatin receptor sst-scan Somatostatin receptor scintigraphy Flt-1 FMS related tyrosine kinase 1 CT Computer tomography US Ultrasonography MRI Magnetic resonance investigation NPK Neuropeptide K PET Positron emission tomography 11C-5-HTP Carbon-11 labeled 5-Hydroxytryptophan CR Complete response PR Partial response SD Stable disease PD Progressive disease GIST Gastrointestinal stromal cell tumour LAR Long-acting release i.m. Intramuscular s.c. Subcutaneous PRRT Peptide Receptor Radionuclide Therapy 111In Indium 111 90Y Yttrium 90 177Lu Lutetium 177 TKR Tyrosine kinase receptors TKRI Tyrosine kinase receptors inhibitors EPT Endocrine pancreatic tumour CML Chronic myeloid lymphoma ASCO American Society of Clinical Oncology

11
Introduction
Midgut carcinoid tumours Carcinoid tumours were first described in 1907 by Oberndorfer and were initially believed to be benign tumours, originating in the intestine. Later, the carcinoid´s malignant potential was described as well as different possible locations for the primary tumour.
The previous classification that is still widely used among clinicians was proposed in 1963 by Williams and Sandler. They classified the tumours de-pending on the localisation of the primary tumour and the embryonic origin of that organ. The tumours were divided into foregut (bronchus, thymus, stomach, proximal duodenum and pancreas), midgut (distal duodenum, jeju-num, ileum, caecum and the mid-transverse part of colon) and hindgut (de-scending colon and rectum).
The different kinds of carcinoid tumours have common features such as originating from neuroendocrine cells, positive argyrophilic staining reaction and the presence of secretory granules. However, they differ in specific hor-mone production. The main hormone produced by midgut carcinoid tumours is serotonin.
One of the most common midgut carcinoid tumours is that of the appen-dix. It is usually benign, discovered at the tip of the appendix during appen-dectomy and is smaller than two cm. If the tumour is larger than two cm or located at the base, there is a higher risk for malignant behaviour and more extensive surgery should be considered (Moertel et al 1987). Midgut tu-mours outside the appendix are prone to be malignant and give rise to metas-tases. The incidence of malignant midgut carcinoids is 0.7-2.1/100.000 (Nor-heim et al 1987). The most common sites for metastases are regional and mesenteric lymph nodes and the liver. In the literature, about 80% of midgut carcinoids outside the appendix have lymph node metastases and 40% have liver metastases at diagnosis. The most common presenting symptom is the carcinoid syndrome which is present in about 50% of the patients. The sec-ond most frequent symptom is abdominal pain and/or intestinal obstruction which is present in about 40% of the patients at diagnosis (Janson et al 1997).
The survival of midgut carcinoid patients has improved over the years. In historical studies the median survival among those who died from their dis-ease was only about two years. In later studies, survival and prognosis has

12
been shown to correspond to certain factors. For instance, the ten-year sur-vival is 60% in the absence of liver metastases while, if present, only 15-25%. Five year survival has been reported to be 55% when localized or re-gional disease is present but only 35% in patients with distant metastases. In the largest material studied the five-year survival regardless of extent of disease was 60% (Strodel et al 1983, McDermott et al 1994 and Modlin et al 2003). In a study from Janson et al (1997), the median survival of midgut carcinoid tumours was 92 months, poor prognostic factors were, amongst others, old age, more than five liver metastases and high hormone levels. Zar et al (2004) showed in a large historical material that positive prognostic factors were young age at diagnosis and diagnosis in recent years. Removal of the primary tumour also seems to be of positive prognostic value (Hell-man et al 2002).
The carcinoid syndrome
Flush, diarrhoea, right-sided heart failure and bronchial constriction are the four symptoms included in the carcinoid syndrome, which was partly de-scribed by Isler and Hedinger in 1953 and fully by Thorson et al 1954. The carcinoid syndrome is most commonly associated with midgut carcinoid tumours and is present in about 50 % of patients recently diagnosed with a midgut carcinoid tumour. However, it might, in rare cases, occur in patients with bronchial carcinoids and endocrine pancreatic tumours. When a patient suffers from the carcinoid syndrome, multiple liver metastases are usually present. The diarrhoea is attributed to high serotonin production (Feldman and O´Dorisio 1986). However, recent data suggest that tachykinins may be involved as well. The flush has been regarded as induced by tachykinins such as neuropeptide K (NPK) (Norheim et al 1986). For many years, the cause of the carcinoid heart disease was unknown. However, in 2001, Raja-mannan et al showed that serotonin increased valvular proliferation in vitro in a dose-dependent manner. In 2005, Gustafsson et al showed that continu-ous infusion with serotonin induced carcinoid heart disease in rats. Previ-ously, there have been reports that some medical agents such as ergotamine, fenfluramine and phentermine involved in serotonin metabolism may also cause valvular dysfunction resembling the carcinoid heart disease (Connolly et al 1997).

13
Hormone analysis Urinary 5-hydroxyindoleacetic acid In 1953, Lembeck et al were able to extract serotonin from a carcinoid tu-mour. Two years later, Page et al reported increased levels of the serotonin metabolite 5-hydroxyindoleacetic acid (5HIAA) in the urine of carcinoid patients. It is still one of the most important markers in diagnosing and as-sessing midgut carcinoid patients.
Plasma chromogranin A Chromogranin A (CgA) belongs to a group of proteins that was found in the adrenal medulla during the 1960s, and, in 1967, Blaschko et al showed that it is a significant marker of neuroendocrine secretion. It has been shown to be present in almost all neuroendocrine organs such as, the pituitary, parathy-roid, adrenal medulla, endocrine pancreas and neuroendocrine cells of the gut. It is stored in large dense core vesicles in neuroendocrine cells. CgA is stored and released together with the more specific peptide hormones and might be increased and detected before the more bioactive hormones give symptoms.
Nowadays, it is used in the diagnosis of neuroendocrine tumours. CgA has 11 points where it may be cleaved depending on what organ that is in-volved. This results in several different fragments that are possible to meas-ure in the plasma. Stridsberg et al (2003) showed that commercial kits for measurement of P-CgA have different sensitivities depending on what epi-tope is targeted by the method.
Plasma levels of CgA have been shown to correlate with tumour burden in neuroblastoma (Hsiao et al 1990). It has also been shown to correlate with tumour burden in midgut carcinoid tumours, both in animal studies (Kolby et al et al 2004) and humans (Janson et al 1997). In midgut carcinoid tumours it has also been proven to be a better biochemical marker than U-5HIAA in patients with limited disease (Eriksson et al 1991).
There are some benign conditions that may cause increased levels of P-CgA without the presence of a neuroendocrine tumour. Among those are treatment with proton pump inhibitors (Sanduleanu et al 1999), chronic atro-phic gastritis (Borch et al 1997) and renal insufficiency (Hsiao et al 1990). These are common conditions and must be regarded when diagnosing new patients and evaluating treatments.
Tachykinins NPK and substance P can be found in high plasma concentrations in patients with midgut carcinoid tumours. When inducing a flush in midgut carcinoid

14
patients with pentagastrin, NPK increases two-fold and this test may there-fore be used as an indicator of carcinoid disease in early cases. Besides being suspected to induce the flush, NPK is often increased in patients with carci-noid heart disease (Norheim et al 1987). Substance P is not associated with increasing values during pentagastrin stimulation and does not seem to play a role in the carcinoid flush (Ahlman et al 1985). In dogs, substance P has been described to increase intestinal secretion of water and electrolytes (McFadden et al 1986). In recent studies, there is a correlation between lev-els of tachykinins and diarrhoea in midgut carcinoid tumours and all sero-tonin producing tumours express tachykinin in immunohistochemical inves-tigations (Cunningham et al manuscript).
Somatostatin receptors Somatostatin acts through specific membrane-bound receptors. Five differ-ent receptor subtypes have been characterised. Somatostatin receptor subtype 1 (sst1) and sst2 were identified by Yamada et al (1992), and the same group also reported the cloning of sst3-5 in 1993. The receptors belong to the G-protein coupled receptor family with seven trans-membrane spanning seg-ments (Bell et al 1993). The receptors are widely distributed in the body. All receptors are found in the brain, pancreas and stomach while sst1 is found in the liver, pituitary and kidney, sst2 in the pituitary and kidney, sst3 in the thyroid and pituitary, sst4 in the lungs and placenta and sst5 in the thyroid and pituitary (Schaer et al 1997, Caron et al 1997, Taniyama et al 2005).
The activation of the different receptors results in different actions. One of the most important actions is to inhibit hormone secretion and this is me-diated through sst2 and sst5 (Chen et al 1993). Both octreotide and lanreotide bind with high affinity to these two receptor subtypes explaining their effect on biochemical markers and symptoms in peptide hormone producing tu-mours (Lamberts et al 1996).
Anti-tumoural actions have been associated with all receptors in in vitro studies. Anti-proliferative effects have been shown for sst1-2 and sst4-5 (Reardon et al 1997, Florio et al 1999, Pages et al 1999 and Sharma et al 1999). Apoptosis have been shown to be mediated through sst2 and sst3(Sharma et al 1996 and Teijeiro et al 2002). Almost all of the studies have been made in vitro and in animals. Since there are species differences in somatostatin receptors, one should be careful in translating the results to humans. In clinical reality, radiological responses are rare and seen in only 5-10% of patients.
Since octreotide and lanreotide have a low binding affinity to sst1 andsst3-4 efforts have been made to develop an sst agonist with a broader recep-tor binding profile. SOM-230 binds with high affinity to all receptor sub-types except sst4 (Bruns et al 2002). It is hoped that treatment with SOM-230

15
will have a better anti-proliferative effect than the first generation soma-tostatin analogues which are used at present, but this still has to be evaluated in clinical trials.
Tyrosine kinase receptors With the knowledge that tyrosine kinase receptor (TKR) actions may play a role in inducing malignant transformation and promoting growth of several different malignancies, molecular targeting directed towards these receptors has become a hot topic in anti-cancer treatment. Some of the most interesting receptors are platelet derived growth factor receptor (PDGFR), epidermal growth factor receptor (EGFR) and c-kit.
PDGFRPDGFRs are abundant in connective tissue, bone marrow, endothelial and glia cells but are usually not present in epithelial cells. The expression of PDGF and PDGFR has been demonstrated in a number of neoplasms such as glioblastoma (Hermanson et al 1992), ovarian cancer (Henriksen et al 1993) and prostate cancer (Fudge et al 1994). Several studies implicate that PDGF has a role in solid tumour development. Several PDGF actions that may be of interest in tumour genesis are development of angiogenesis, autocrine stimulation of tumour cell growth and control of interstitial pressure of the stroma surrounding the tumour (Board et al 2005).
In midgut carcinoid tumours, Funa et al (1990) found a positive staining in 66% of tumours for PDGFR . Two years later, Chaudhry et al found the same receptor in 85% of midgut carcinoid tumours and 83% had positive staining for PDGFR in stoma cells. In endocrine pancreatic tumours (EPT), Fjällskog et al (2003) reported that all 38 investigated tumours expressed PDGFR while 74% expressed PDGFR . In tumour stroma surrounding the tissue, 57% were positive for PDGFR and 97% for PDGFR . This year, Kulke et al presented an abstract where they had treated 39 carcinoids and 52 endocrine pancreatic tumours with SU11248, a tyrosine kinase receptor in-hibitor (TKRI) targeting vascular endothelial growth factor receptor (VEGFR), PDGFR and c-kit. Radiological responses were seen in two of the carcinoid patients (5.1%) and seven (13.5%) of the EPTs and only mild side effects were noted.
EGFR EGF is known to increase cell proliferation, induce angiogenesis and de-crease apoptosis, actions which all may lead to increased mito-genesis and
16
cancer development (Schlessinger et al 2000 and Yarden et al 2001). Several malignancies have up-regulated EGFR, including breast, colon, non-small cell lung cancer and head-and-neck cancers. Over-expression also often cor-responds to a poor prognosis (Salomon et al 1995). Because of this the EGFR has drawn much attention during recent years and efforts to inhibit the receptor, and thereby hopefully find effective anti-tumour treatments, have been conducted. Both small molecules blocking the receptor and monoclonal antibodies have been tried. At the moment, a preparation of monoclonal antibodies against EGFR is registered in Sweden for treatment of breast, colon and head-and-neck cancer.
In neuroendocrine tumours, Nilsson et al (1995) reported a positive im-munohistochemical staining for EGFR in 27 out of 30 patients with neuro-endocrine tumours and, in another study, three out of nine midgut carcinoid tumours examined expressed EGFR (Wulbrand et al 1998). A recent study from Papouchado et al (2005) reported positive EGFR staining in 91% of midgut carcinoid tumours. In three different neuroendocrine tumour cell-lines, Höpfner et al (2003) showed that gefitinib, a small TKRI molecule induced growth inhibition, apoptosis and cell-cycle arrest. No studies or reports of midgut carcinoid patients treated with EGFR inhibitors have been published to our knowledge.
C-KitThe c-kit receptor is expressed in mast cells, melanocytes, spermatogonia and breast epithelium. C-kit belongs to class III TKR. The receptor contains an extra-cellular part, a single trans-membrane and a cytoplasmic part. The activated receptor is involved in several actions such as haematopoiesis, mast cell development and function, gametogenesis and melanogenesis (Rönnstrand et al 2004). In certain tumours such as germ cell tumours, gas-trointestinal stromal cell tumours (GIST), mast cell tumours, small cell lung cancer and breast cancer, dys-regulation of c-kit plays a role (Tsuura et al 1994, Hirota et al 1998, Tian et al 1999 and Palmu et al 2002). A c-kit muta-tion with a gain of function has been shown in mast-cell tumours, germ-cell tumours and GIST’s (Hirota et al 1998 and Tian et al 1999). We have not found any reports about the expression of c-kit in midgut carcinoid tumours. However, in endocrine pancreatic tumours, Fjällskog et al (2003) report a positive staining in 92% of the 38 investigated tumours.

17
Treatment Surgery One of the most important treatments in midgut carcinoid tumours is sur-gery. Abdominal pain due to intestinal obstruction is one of the most com-mon symptoms by which the midgut carcinoid tumour presents. The tumour itself is most often not large enough to obstruct the lumen of the intestine. Instead the lymph node metastases, located in the mesentery, cause a retrac-tion of the mesentery which eventually will give rise to an obstruction of the small bowel. Sometimes this arises before liver metastases have evolved and surgery with a radical approach may be performed. However, even in such cases, it has been shown that most patients will develop a recurrence of their disease though it might take decades before they are diagnosed and medical treatment is needed (Moertel et al 1987). The mesenteric lymph node metas-tases are sometimes difficult to remove since they often grow near the supe-rior mesenteric artery, surrounding it and giving rise to intestinal ischemia. Previously this ischemia was one of the major causes of death by carcinoid tumours and is still a problem. It has been shown that resection of the mesen-teric lymph node metastases with or without liver metastases improves sur-vival (Hellman et al 2002). A surgical procedure was described by Öhrvall et al in 2000, indicating how to remove the mesenteric lymph nodes, also those that seemed impossible to resect.
Most patients with midgut carcinoid tumours have multiple liver metas-tases at diagnosis. With new techniques, it has become more safe and feasi-ble to do liver surgery. It has been shown that aggressive surgery prolongs survival and liver resection is now recommended to perform in cases with uni-lobar disease or when 90% of the tumour volume can be excised. Today it is also common to combine surgery with radiofrequency (RF) ablation to reduce tumour volume (Hellman et al 2005).
Liver transplantations have been performed in a small number of cases of endocrine tumours. The reports that have been presented are heterogeneous regarding tumour diagnosis. In a study from Gothenburg, two midgut carci-noid patients were included. One had a recurrence after nine months and the second patient was still free of disease 24 months after transplantation (Ahlman et al 2004). In a study from France, five midgut carcinoid tumour patients had liver transplantation (Le Treut et al 1997). Two had recurrences while three were still free of disease 32, 70 and 77 months after surgery. Since most midgut carcinoid patients also have extra-hepatic disease, trans-plantation should be considered only in selected cases. Since modern imag-ing techniques such as PET with 11C-5-HTP find tumours less than five mm, it is recommended performing such investigations if available before consid-ering transplantation.

18
Alpha-interferonInterferon (IFN) was discovered almost fifty years ago (1957) by Isaacs and Lindmann. It is involved in the immune system for viral defence. There are three different types of IFN, alpha ( ), beta ( ) and gamma ( ) IFN, which bind to two different receptors. -IFN and -IFN bind to a common receptor and -IFN to a separate one. Recombinant IFN is used in the treatment of several different diseases. Alpha-IFN is most commonly used in tumours (myelom, hairy cell leukaemia, malignant melanoma, renal cell cancer and neuroendocrine tumours) and viral diseases such as hepatitis B and C. It acts by stimulating natural killer cells and, in neuroendocrine tumours, controls hormone secretion and tumour growth. This was shown by Öberg et al, who in 1983, reported the use of -IFN in nine patients with midgut carcinoid tumours. Eight of these responded with a reduction of both U-5HIAA and symptoms. In 1986, the same author reported an objective biochemical re-sponse in 47% of 36 patients treated with human leukocyte IFN after long-term treatment. These results have been confirmed by other authors (Biesma et al 1992, di Bartolomeo et al 1993). Radiological responses vary between 5-20% in most studies. In 1989, Moertel et al treated 24 patients with higher doses than previously had been done. The response rate was about the same but the patients experienced more side-effects. They also reported that the effect lasted for a median of only seven weeks. The frequent side-effects and the lack of evidence of an increased survival rate with IFN treatment have made the role of IFN in carcinoid treatment questionable. Large randomised trials have been difficult to perform. One study that randomised patients after embolisation to octreotide or octreotide + IFN could not show any sig-nificant difference regarding survival between the two treatment regimens (Kölby et al 2003). The study did however show an increase in time to pro-gression giving the advantage to the group given the combination. In a Nor-wegian, study, patients who responded to IFN treatment were randomized to continue with IFN or to stop the IFN treatment. There was a significantly improved survival in those patients who continued with IFN treatment (Jacobsen et al 1995). A few other randomized studies have been performed, however the study populations have been heterogeneous and therefore re-sults should be interpreted with care (Frank et al 1999 and Faiss et al 2003).
IFN interferes with the immune-system and this is also the cause for some of the side-effects induced by IFN treatment. A transient fever and flu-like symptoms arise when starting treatment. Other well-known side effects are myalgia, fatigue, anorexia and autoimmune diseases. Among the autoim-mune diseases, thyroid diseases are the most common (Rönnblom et al 1991).

19
Somatostatin and its analogues Somatostatin was first described in 1973 by Brazeau et al. It was described as a hypothalamic hormone that inhibited growth hormone (GH) secretion. Two biological active forms of somatostatin have been described, soma-tostatin-14 derived from the c-terminal of a propeptide in the hypothalamus and the amino terminally extended somatostatin-28 discovered in the gut by Pradayrol et al (1978). Somatostatin is found predominantly in the central nervous system and the gastrointestinal tract. However, somatostatin has also been found in the placenta, the kidney and cells of the immune system (Caron et al 1997, Reubi et al 1999, and Balster et al 2001).
One of the functions first described for somatostatin was inhibition of hormone secretion from endocrine cells and, therefore, it was soon consid-ered for treatment of endocrine disorders. In carcinoids, the first report came from Thulin et al, who, in 1978, reported successful use in a patient with severe carcinoid syndrome. However, native somatostatin has a very short half-life of about two to three minutes and it is therefore not practical for prolonged use. In 1982, the first long-acting somatostatin analogue, octreo-tide (SMS 201-995), was synthesized by Bauer et al. Its half-life was almost forty times longer (113 minutes) (Del Pozo et al 1986). In 1987, another compound, lanreotide (BIM-23014C), was synthesized by Heiman et al and both analogues are still the most frequently used in clinical practice.
One of the first reports concerning clinical use of octreotide came from Kvols et al in 1986 who reported a biochemical response in 72% of 25 pa-tients with a malignant midgut carcinoid tumour treated with octreotide three times a day. Even more patients had symptomatic improvement. The median duration of response was 12 months. During the years, several reports have shown about the same response rates (Ruzniewski et al 1996, and Wymenga et al 1999). In many patients, there is a recurrence in symptoms after some time of somatostatin analogue treatment. This phenomenon called tachyfy-laxis was described first by Wynick et al in 1989. The reason for its occur-rence is not yet known. When increasing doses, a new symptomatic response is often seen for a period of time.
Anti-proliferative effects by somatostatin have been studied by several groups. Arnold et al (1995), treated 53 patients in a German multicenter study with neuroendocrine tumours in a progressive phase with octreotide 200 µg 3 times daily. Stabilisation of tumour growth was achieved in 36.5% with a median duration of 18 months. However, tumour reduction is rarely seen at standard doses. There has been a discussion whether this lack of tu-mour shrinkage is a question of dosage. In a clinical study by Anthony et al (1993) they reported 31% radiological responses in a group of neuroendo-crine tumours treated with higher doses than normal, lanreotide 2250-9000 µg/day or octreotide 1500-6000 µg/day. In 1997, Eriksson et al presented a high-dose study with lanreotide up to 12 mg/day. Disappointingly, only 1

20
patient (5%) had a partial tumour size response. However, in tumour tissue from the patients, apoptosis increased during treatment, a feature which is not seen when standard doses are used (Imam et al 1997).
Today slow release formulas of these compounds are most frequently used. They are administrated as intramuscular (i.m.) or deep subcutaneous (s.c.) injections once a month. The prolonged interval between injections has improved the quality of life for patients. Thirty mg of octreotide acetate and 120 mg of lanreotide are equipotent doses. In the late 1990´s, octreotide pamoate was produced. The difference between ordinary octreotide and this new compound was that you could load the pamoate with more octreotide, 160 mg. This compound was tested in several tumour groups. Treatment of breast cancer was studied in a randomized trial where tamoxifen was used with or without octreotide pamoate. The study was stopped in advance as there were no differences in response but there were more gastrointestinal side effects in the octreotide pamoate arm (Bajetta et al 2002). Another study was performed on a mixture of pancreatic, colonic and gastric adenocarci-nomas. No tumour responses were seen, however, the treatment was well tolerated (Helle et al 1998).
Octreotide and lanreotide both bind with high affinity to sst2 and sst5 andwith intermediate affinity to sst3, but not to sst1 and sst4. Some of the interest-ing effects such as apoptosis are believed to be mediated through sst3 and other cell-cycle inhibitory effects through sst1. Efforts have been made to develop a somatostatin analogue which binds with high affinity to more of the receptors. In 2002, Bruns et al succeeded in producing a new compound that binds with high affinity to sst1-3 and sst5, SOM230. The first results in midgut carcinoid patients who had symptoms, which were refractory to Oc-treotide LAR treatment were presented in an abstract at the ASCO gastroin-testinal meeting 2006. This showed that one patient (4%) had complete re-mission regarding symptoms and another 25% had partial response. Radio-logical and biochemical results were not reported.
In the gastrointestinal tract, somatostatin can induce reduction in blood-flow to the intestine, impaired gallbladder and intestinal motility and inhibi-tion of the secretion of the exocrine pancreas (Lembcke et al 1987). This is the cause to the usually mild adverse reactions seen during treatment with somatostatin analogues. The most common are nausea, transient abdominal pain, flatulence, diarrhoea and the development of gallstones which almost always remain asymptomatic (Trendle et al 1997).
Liver embolisation In patients with inoperable disseminated disease and multiple liver metasta-ses, hepatic artery embolisation can be performed to reduce tumour mass and hormone production. Usually, the embolisation is performed selectively in one of the liver lobes, reducing the risk of serious side effects. Overall radio-

21
logical response rates of about 50% have been seen in midgut carcinoid pa-tients with a median duration of 12 months. The procedure can be repeated several times. Side effects such as post-embolic pain, fever and nausea is seen in 50-90% of patients whereas severe side effects such as liver necrosis, renal failure, intestinal ischemia and cholecystitis is seen in less than 10% of the patients (Ruszniewski et al 1993, Ajani et al 1988 and Eriksson et al 1998).
Radiofrequency ablation Radiofrequency (RF) ablation is a local treatment using a needle which is placed within the liver metastases. Radiofrequency is used to heat the metas-tasis until it becomes necrotic. This is used in patients with limited disease in the liver (Elvin et al 2005). The impact of the procedure on survival has not been investigated in neuroendocrine tumours.
Peptide receptor radionuclide therapy In patients with high radio-ligand uptake at sst-scan, radionuclide therapy can be an option. Radionuclides that have been used are 111In-Pentetreotideor [111In-DTPA] Octreotide, 90Y-DOTATOC and [177Lu-DOTA0,Tyr3] Oc-treotate. Radiological partial responses (PR) for 111In-Pentetreotide have been 0-17% (Anthony et al 2002, Valkema et al 2002 and Buscombe et al 2003). Better responses have been obtained with 90Y-DOTATOC and [177Lu-DOTA0,Tyr3] Octreotate. In 90Y-DOTATOC studies a few patients (3-6%) have been reported to have complete remission (CR) (Waldherr et al 2002) and another 6-37% had PR (Otte et al 1999 and Waldherr et al 2002). There are few studies reporting the responses to [177Lu-DOTA0,Tyr3] Octreotate treatment. In one of the latest studies published, 2% had CR and 26% PR (Kwekkeboom et al 2005). Side effects reported are usually transient and include nephrotoxicity and bone marrow suppression. A few cases with myelo-dysplastic syndrome have been reported. Further studies to find opti-mal radionuclide and doses have to be performed.

22
Aims of the investigation
The aims of the present investigation were to:
Investigate the proportion of radically operated midgut carcinoid tumours that have a recurrence and which method first identifies the recurrences.
Evaluate overall and five-year survival in patients with malignant midgut carcinoid tumours and to identify factors that influence survival. To evaluate the effect of first-line medical treatment and the time to progres-sion.
Evaluate the effect on symptoms, hormone levels and tumour size of oc-treotide pamoate using a high-dose regime and to investigate changes in tumour biology during such treatment.
Investigate the expression of the tyrosine kinase receptors, PDGFR and , EGFR and c-kit in midgut carcinoid tumours in order to identify possi-
ble targets for future therapy studies.

23
Material and methods
Patients
Paper I We identified 61 patients referred to our centre between 1985 and 2004 who were considered radically operated by both the surgeon and the pathologist. There were 33 men and 28 women and their median age at diagnosis were 59 years (range 26-84). All had a histopathologically confirmed diagnosis of midgut carcinoid tumour not originating in the appendix. Ki-67 index was calculated in 24 patients and was less than two percent in all of them. All patients had lymph node metastases, two had single liver metastases that were removed at surgery. Acute surgery was performed in 43 patients (73%) whereas 18 (27%) underwent elective surgery by an experienced endocrine surgeon. Agreement in the surgical report and the pathology report on the radicality of the operation was an inclusion criterion.
Paper II All patients diagnosed with a malignant midgut carcinoid tumour and re-ferred to the Department of Endocrine Oncology, Uppsala University Hospi-tal from January 1990 until February 2006 were included in this retrospec-tive analysis. Medical records were reviewed and data collected for further analysis.
We identified 284 patients (133 women and 151 men) with a histopa-thologically confirmed midgut carcinoid tumour. Patients with tumours originating in the appendix were excluded. The median age at diagnosis was 61 years (range 25-84). All patients were evaluated for disease characteris-tics and other epidemiological factors. Sixteen patients were lost to follow-up but the remaining 268 patients were included in the calculation of overall survival. In another 41 patients, the primary medical treatment could not be evaluated due to change of therapy before evaluation (11), stop of treatment before evaluation (10) or no tumour visible at radiology and normal hormone levels (20). In the remaining 227 patients calculations of best response and time to progression were compared between groups of patients treated with only somatostatin analogue or IFN alone or the combination of the two.

24
Paper III Twelve patients, seven men and five women, with malignant midgut carci-noid tumours were included. The median age at diagnosis was 50 years and the median time from diagnosis to study inclusion was 64.5 months. All had a positive somatostatin receptor scintigraphy (sst-scan) and liver and lymph node metastases. Four had bone metastases and two had ovarian metastases. All had progressive disease during standard treatment at the time of inclu-sion. All but one had undergone debulking surgery and all had been treated with -IFN. Ten out of twelve were previously treated with somatostatin analogues. Three patients had undergone liver embolisation and two patients had been treated with [111In-DTPA] Octreotide.
Paper IV Tumour tissue was obtained from 36 patients, 24 women and 12 men, with malignant midgut carcinoid tumours. Their median age at diagnosis was 60 years. All had metastatic disease. Fifteen had received -IFN before the bi-opsy was taken and 21 had been treated with somatostatin analogues. Twenty-nine had performed an sst-scan and 83% had a pathological tracer uptake. Twenty-nine of the samples were from liver metastases, seven from lymph node metastases and one came from a primary tumour.
Tumour tissue Tumour tissue for histopathological diagnosis and immunohistochemical staining was collected using a 1.2 mm needle with ultrasound guidance. The tissue sample was immediately frozen in liquid nitrogen and kept at -70ºC until further use or was fixed in formalin and embedded in paraffin wax.
Paper III Tumour tissue was collected before treatment was initiated and thereafter every sixth month until end of study.
Paper IV Tumour tissue was gathered from the tumour tissue bank in our research department from 36 patients with a verified histopathological diagnosis of a malignant midgut carcinoid tumour.
ImmunohistochemistryImmunostaining was performed using the streptavidin-biotin complex tech-nique (Vector Laboratories, Burlinghame, CA, USA). Regarding antibodies,

25
purchasers and dilutions see Table 1. The immune reaction was visualised using Vectastatin Elite ABC kit (Vector Laboratories), 3-amino-9-ethylcarbazole was used as chromogen and 0.02% hydrogen peroxide as substrate. The sections were counterstained with Mayer’s haematoxylin (Apoteksbolaget, Stockholm, Sweden).
Table 1. Antibodies, dilutions and producers in immunohistochemical analysis in paper III and IV
Antibody Dilution Producer Paper CgA 1:2000 M Stridsberg Uppsala Sweden III, IV VEGF 1:50 Santa Cruz Biotech. Inc. CA USA III P27 1:100 Santa Cruz Biotech. Inc. CA USA III P16 1:40 Santa Cruz Biotech. Inc. CA USA III Flt-1 1:600 Santa Cruz Biotech. Inc. CA USA III Ki67 1:100 Dako Copenhagen Denmark III Cleavedcaspase 3
1:100 Cell Sign. Techn. Inc. MA USA III
PDGFR 1:400 Santa Cruz Biotech. Inc. CA USA IV PDGFR 1:100 Santa Cruz Biotech. Inc. CA USA IV EGFR 1:150 Santa Cruz Biotech. Inc. CA USA IV c-kit 1:250 Santa Cruz Biotech. Inc. CA USA IV Sst1 1:1200 M Stridsberg Uppsala Sweden III Sst2 1:5000 M Stridsberg Uppsala Sweden III Sst3 1:5000 M Stridsberg Uppsala Sweden III Sst4 1:1000 M Stridsberg Uppsala Sweden III Sst5 1:5000 M Stridsberg Uppsala Sweden III
Cell cultivation Human neuroendocrine pancreatic tumour cells, BON1, were cultivated in 50% Dulbecco´s modified Eagle´s medium and 50% F12 supplemented with 10% foetal bovine serum (FBS) and penicillin/streptomycin. Cells were cul-tivated at 37°C in a humified atmosphere containing 5% CO2.
Cell stimulation and fluorescence microscopy.Cells were seeded in chamber slides and cultivated for 48 hours. Prior to stimulation, the cells were incubated in medium devoid of FBS over night. Cells were stimulated with PDGF-BB (100 ng/ml) for 15 minutes at 37°C. After stimulation, the chamber slides were fixed in 3.8% formaldehyde in phosphate-buffered saline (PBS) for 30 minutes at 25°C and washed in PBS. The cells were permeabilized in 0.2% Triton X-100 in PBS for five minutes
26
and washed in PBS. Incubation with TRITC-labeled phalloidin (Sigma) in PBS was performed for one hour at 25°C and subsequently the cells were washed in PBS. The slides were mounted with cover slips by the use of Vec-tashields (Vector Laboratories). Cells were photographed by an Axiocam HRm camera employing the Axiovision Imaging Software using a 63x plan-apochromat objective and a Zeiss Axioplan2 microscope.
TunelFor apoptotic studies of tumour tissue in study III, we used the TUNEL method which is based on specific binding of terminal deoxynucleotidyl transferase to the 3'-OH ends of DNA breakage. The method was described by Gavrieli et al in 1992.
Biochemistry
Paper I-II At the patient’s first visit, P-CgA and two 24-hour collections of U-5HIAA were performed as well as routine biochemistry. During treatment and fol-low-up P-CgA and U-5HIAA as well as routine biochemistry were moni-tored every third to fourth month. Patients treated with IFN were examined for thyroid dysfunction, liver enzymes and bone marrow function at follow up.
Paper III P-CgA and U-5HIAA were analysed at screening and prior to first injection with octreotide pamoate. P-CgA was analysed before every injection during the treatment period. U-5HIAA was calculated as the mean of two 24-hour urine collections and measured every second month during treatment. In addition, haematology, liver enzymes, kidney function and electrolytes were checked before every injection.
Radiology
Paper I, II At the patient’s first visit after surgery, a contrast-enhanced computer tomo-graphy (CT) and ultra-sonography (US) were performed. At the following visits, these two investigations were usually alternately used at every second follow-up.

27
Paper III A contrast-enhanced CT was performed at baseline and then every third month. The examinations were reviewed by a senior consultant in radiology. US was performed at baseline and every sixth month to monitor develop-ment of gallstones during treatment.
Somatostatin receptor scintigraphy Sst-scan was performed as previously described (Westlin et al 1992). In summary, [111In-DTPA-D-Phe1]-octreotide was injected. Twenty-four hours after injection, static anterior-posterior whole body images were taken. SPECT (Single Photon Emission Tomography) was also performed on the abdomen.
Paper I,II Since 1992, sst-scan has usually been performed at the first visit to our cen-tre. It has also been performed in radically operated patients having new symptoms, increased hormone levels or suspicious radiological findings and sometimes to follow treatment responses.
Paper III Sst-scan was done prior to start of treatment and every sixth month during treatment.
Positron emission tomography
Paper I PET-scan with 11C-5-HTP has been performed since 1991 in selected cases. Most often it has been used in radically operated patients to rule out remain-ing tumour tissue and before stopping adjuvant treatment for the same rea-son. It has also been used in patients with new symptoms, increased hor-mone levels or suspicious radiological findings and sometimes to follow treatment response.
Definition of response A radiological response was defined as a reduction by >50% in tumour size and was calculated as the sum of the products of the largest perpendicular diameters of measurable lesions. Stable disease was regarded as a reduction

28
by <50% or an increase of <25% in tumour size. Progressive disease was defined as >25% increase in tumour size and/or new lesions. Biochemical response was defined as >50% reduction in one tumour marker. Stable dis-ease was defined as <50% reduction but <25% increase of a tumour marker and progressive disease was thus defined as > 25% increase in one tumour marker.
Definition of recurrence Our current clinical praxis which was used in this study defines recurrent disease as one of the following events: 1) tumour cells are detected in a new tissue specimen obtained by surgery or biopsy 2) a tumour lesion is visual-ized by two radiological methods (US, CT, MRI, sst-scan or 11C-5-HTPPET) or 3) a tumour lesion is shown by one radiological method in combina-tion with at least one biochemical tumour marker increased above the upper reference level.
Therapy
Paper II In 254 patients, resection of the primary tumour had been performed. Twenty-nine patients were treated with octreotide 100-500 µg 1-3 times/day, octreotide LAR 10-30 mg/3-4week, lanreotide PR 30 mg/7-14 day or lanreo-tide autogel 60-120 mg/3-4 weeks alone as first-line medical treatment. Al-pha-IFN 3-5 MU s.c. 3-5 days/week was given to 85 patients and the combi-nation of the two treatments were given to 113 patients as first-line medical treatment.
Paper III The patients were treated with octreotide pamoate 160 mg i.m. every two weeks for two months and thereafter once a month. Treatment continued until progressive disease or any other reason for discontinuing the study.
lpha-IFN had to be withdrawn at least two months before the first injec-tion of octreotide pamoate. Long-acting somatostatin analogues were discon-tinued at least two months prior to study start. If the patient was unable to manage without somatostatin analogues, short-acting analogues could be used until 72 hours prior to the first injection in the study.
29
Statistics
Paper II Survival was calculated with the Kaplan Meier method with censoring for non-carcinoid related deaths. Proportional hazards were assumed and Cox regression method for uni- and multivariate analysis was performed.

30
Results
Recurrences in radically operated midgut carcinoid tumors (paper I) We found that 38/61 patients (62%) had disease recurrence during follow-up. The median follow-up of all patients was 90 months (range 15-270).
Five patients of those with recurrences had their recurrence already at the first follow-up after surgery. One patient was re-operated due to adherences and residual disease was found. He had an increased P-CgA but no radio-logical findings prior to surgery. The other four had radiological findings with at least one method. Three out of these four also had elevated P-CgA.
In the remaining 33 patients, the median time from surgery until a con-firmed recurrence was established was 35 months (range 6-217).
P-CgA was the first indicator in 28 of these 33 (84%) patients. Radiology was simultaneously positive in three and U-5HIAA in four patients. In the remaining patients, P-CgA continued to be elevated for a median time of 39 months before the recurrence was confirmed by radiology.
In only three patients, radiology was the first method to identify a recur-rence. In the remaining two patients, U-5HIAA was the first method to indi-cate recurrent disease.
The five-year survival for the whole group was 96%, whereas the ten- and 15-year survival rates were the same (92%).
31
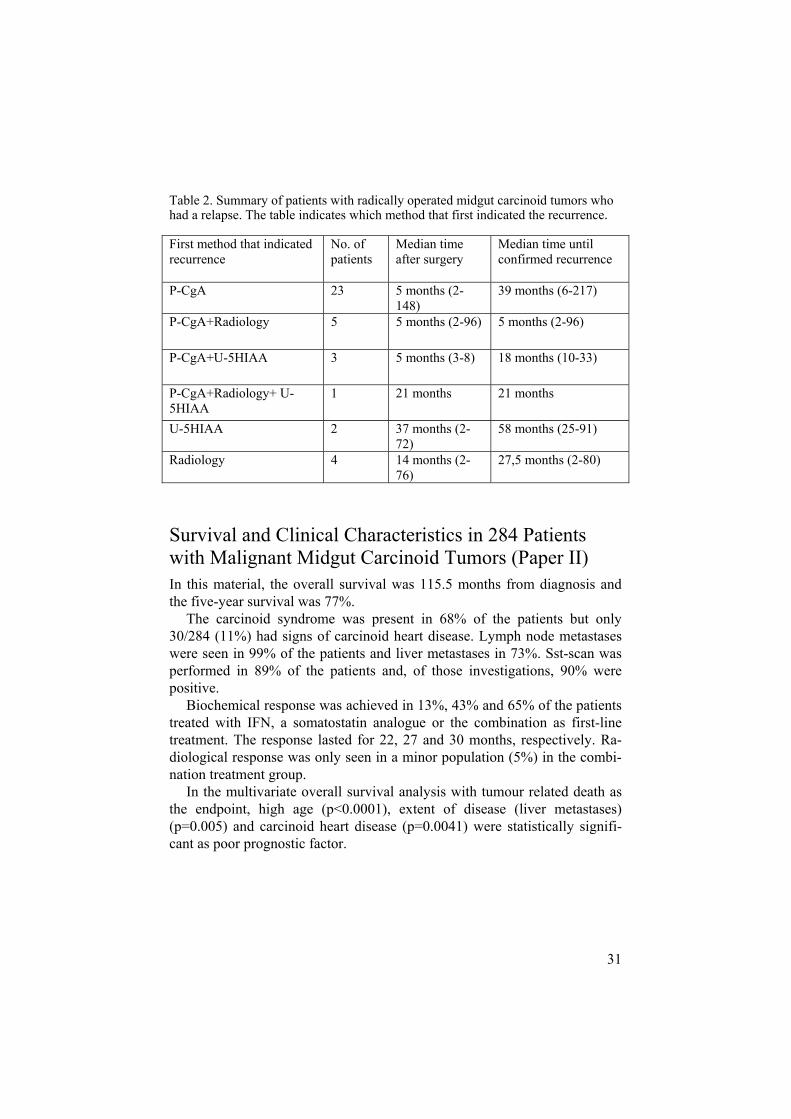
Table 2. Summary of patients with radically operated midgut carcinoid tumors who had a relapse. The table indicates which method that first indicated the recurrence.
First method that indicated recurrence
No. of patients
Median time after surgery
Median time until confirmed recurrence
P-CgA 23 5 months (2-148)
39 months (6-217)
P-CgA+Radiology 5 5 months (2-96) 5 months (2-96)
P-CgA+U-5HIAA 3 5 months (3-8) 18 months (10-33)
P-CgA+Radiology+ U-5HIAA
1 21 months 21 months
U-5HIAA 2 37 months (2-72)
58 months (25-91)
Radiology 4 14 months (2-76)
27,5 months (2-80)
Survival and Clinical Characteristics in 284 Patients with Malignant Midgut Carcinoid Tumors (Paper II) In this material, the overall survival was 115.5 months from diagnosis and the five-year survival was 77%.
The carcinoid syndrome was present in 68% of the patients but only 30/284 (11%) had signs of carcinoid heart disease. Lymph node metastases were seen in 99% of the patients and liver metastases in 73%. Sst-scan was performed in 89% of the patients and, of those investigations, 90% were positive.
Biochemical response was achieved in 13%, 43% and 65% of the patients treated with IFN, a somatostatin analogue or the combination as first-line treatment. The response lasted for 22, 27 and 30 months, respectively. Ra-diological response was only seen in a minor population (5%) in the combi-nation treatment group.
In the multivariate overall survival analysis with tumour related death as the endpoint, high age (p<0.0001), extent of disease (liver metastases) (p=0.005) and carcinoid heart disease (p=0.0041) were statistically signifi-cant as poor prognostic factor.

32
Table 3. Best response to treatment CR+PR Duration
(median) SD Duration
(median) PD
Interferon-alpha
11/85 (13%)
22 months (2-141)
67/85 (79%)
23 months (4-141)
7/85 (8%)
Somatostatin analogue
12/28 (43%)
27 months (4-60)
14/28 (50%)
27 months (5-60)
2/28 (7%)
Combination 74/113 (65%)
30 months (5-118)
38/113 (34%)
26.5 months (5-116)
1/113 (<1%)
CR = complete response, PR = partial response, SD = stable disease, PD =progressive disease
Treatment with high-dose octreotide pamoate (paper III) Biochemical and radiological responses Nine of twelve patients (75%) with progressive malignant midgut carcinoid tumour achieved stable disease for a median of 12 month. Minor tumour shrinkage was seen in five of the patients. Four patients (25%) had a PR of P-CgA with a median duration of five months, and two patients had PR of U-5HIAA for a median of 13.5 months. Another seven patients (58%) had stabilisation of P-CgA for a median duration of six month, whereas nine patients (75%) had stabilisation of U-5HIAA for a median of nine months. Ten of the 12 patients had symptomatic improvement. Few side-effects were noted.
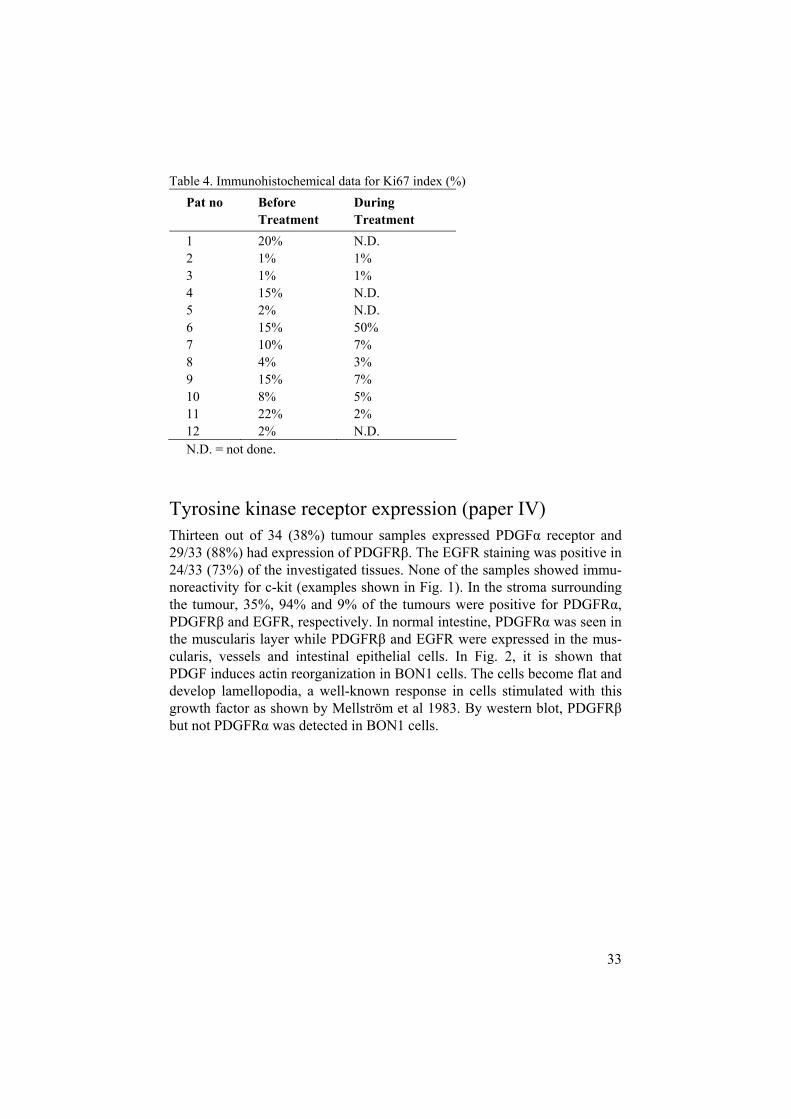
Immunohistochemistry All tumour specimens showed immunoreactivity for CgA. Sst1-3 and sst5 was also expressed in all tissues, while sst4 was expressed in nine out of twelve (75%) patients. The sst expression did not change during treatment. Apop-tosis, which was investigated by the TUNEL-method and cleaved caspase 3, as well as markers for angiogenesis, investigated by VEGF and FLT-1, and the expression of the cell-cycle regulating protein P16 remained unchanged during treatment. The expression of P27, a marker for cell cycle inhibition, showed a tendency to decrease during treatment. The proliferation marker Ki67 index was low (<2%) in four of 12 patients before treatment. Three patients had an unchanged Ki67 index for a median of 24 months. In those with Ki67 index >10%, two patients continued to progress, one of the two developed a severe carcinoid heart disease, and was withdrawn from the study and soon thereafter, he progressed. Two patients decreased their Ki67 index from high to low figures and were stabilized, see Table 4.
33
Table 4. Immunohistochemical data for Ki67 index (%) Pat no Before
Treatment During Treatment
1 20% N.D. 2 1% 1% 3 1% 1% 4 15% N.D. 5 2% N.D. 6 15% 50% 7 10% 7% 8 4% 3% 9 15% 7% 10 8% 5% 11 22% 2% 12 2% N.D. N.D. = not done.
Tyrosine kinase receptor expression (paper IV) Thirteen out of 34 (38%) tumour samples expressed PDGF receptor and 29/33 (88%) had expression of PDGFR . The EGFR staining was positive in 24/33 (73%) of the investigated tissues. None of the samples showed immu-noreactivity for c-kit (examples shown in Fig. 1). In the stroma surrounding the tumour, 35%, 94% and 9% of the tumours were positive for PDGFR ,PDGFR and EGFR, respectively. In normal intestine, PDGFR was seen in the muscularis layer while PDGFR and EGFR were expressed in the mus-cularis, vessels and intestinal epithelial cells. In Fig. 2, it is shown that PDGF induces actin reorganization in BON1 cells. The cells become flat and develop lamellopodia, a well-known response in cells stimulated with this growth factor as shown by Mellström et al 1983. By western blot, PDGFRbut not PDGFR was detected in BON1 cells.

34
.
Figure 1. Immunohistochemical stainings in malignant midgut carcinoid tumours. Positive stainings for PDGFR (A), PDGFR (B), EGFR(C) and ChromograninA (E). Negative staining for c-kit (D).
Figure 2. PDGF induces cytoskeletal reorganization in BON1 cells. The actin cy-toskeleton of control cells and cells stimulated with PDGF-BB were visualized by using TRITC-phalloidin.
.

35
Summary
Study I In the first study, we retrospectively identified 61 patients who were consid-ered to have had radical surgery for their malignant midgut carcinoid tumour assessed both by the surgeon’s description and the pathology report. The patients were followed and different methods for detecting recurrent disease were evaluated. A recurrence was subsequently diagnosed in 38/61(62%) of the patients, the median time of observation being 90 months. P-CgA alone or in combination with other methods was the first method to detect recur-rence in 32/38 (84%) of the patients. Time to first sign of a recurrence was 35 months. However, this was a median of 39 months before the diagnosis of the recurrence was established.
Study II In the second study, we identified 284 patients diagnosed with a malignant midgut carcinoid tumour between 1990 and 2006 and referred to our national referral centre. We collected data concerning tumour characteristics, sur-vival, best response to first-line medical treatment and factors that could influence survival. We found, amongst other things, that carcinoid heart disease was present in 11% of the patients while carcinoid syndrome was present in 68% of the patients and liver metastases in 73%.
The median survival was 115.5 months and the five-year survival 77%. Biochemical responses to first-line medical treatment were for IFN 13%, somatostatin analogues 43% and for the combination 65%. Durations of biochemical response were 22, 27 and 30 months, respectively.
Carcinoid heart disease, liver metastases and old age were poor prognos-tic factors.
Study III In the third study, 12 patients with disseminated malignant midgut carcinoid tumours in a progressive phase were treated with ultra-high doses of octreo-tide pamoate; 160 mg twice a month for two months and after that, once a month. All patients had previously received several different treatments. Nine of twelve patients (75%) achieved stable radiological disease for a me-

36
dian of 12 months. The treatment was well tolerated and few side effects were observed.
Tumour cell biology studies on tumour specimens obtained before and during treatment could not identify any changes in apoptotic markers (TUNEL and cleaved caspase3), cell-cycle inhibition (p21 and p27) or an-giogenesis (VEGF, Flt1).
The sst subtype expression was analyzed by immunohistochemistry in all tumour specimens obtained in study III. All tumours expressed sst1-3 and sst5and 9/12 expressed sst4. There was no change in expression during treat-ment.
Study IV In the fourth study, we analyzed the expression of four different TKR with immunohistochemistry in 36 patients with malignant midgut carcinoid tu-mours. Thirty-eight percent of the patients had positive staining for PDGFRin tumour tissue. Corresponding figures for the other receptors were 88% for PDGFR , 73% for EGFR while none were positive for c-kit. Examples shown in Fig. 1. In Fig. 2, it is shown that PDGF induces actin reorganiza-tion in BON1 cells. The cells become flat and develop lamellopodia, a well known response in cells stimulated with this growth factor shown by Mell-ström et al (1983). By western blot, we could detect PDGFR but not PDGFR in BON1 cells. Thus, BON cells may be a good model in future studies of inhibition of PDGF stimulated tumour growth.

37
Discussion
Study I In the first study, we investigated which method that was the most sensitive for detecting recurrent disease in radically operated midgut carcinoid tumour patients. Retrospective data of biochemical markers (U-5HIAA and P-CgA) and radiological investigations (US, CT, sst-scan and 11C-5-HTP PET) were collected and evaluated.
Most patients with midgut carcinoid tumours have disseminated disease at diagnosis. One of the most common presenting symptoms at diagnosis is abdominal pain. Sometimes there is an indication for acute surgery. In a minority of patients, it is possible to perform surgery with a radical intent. From a previous study by Moertel (1987), we know that 77% of the 72 pa-tients with a malignant midgut carcinoid tumour who underwent curative surgery had a recurrence within a median of 16 years from surgery. In an-other study by Wängberg et al (1996) where 14 patients were operated with curative intent and had normal U-5HIAA postoperatively, 50% had a recur-rence when investigated with sst-scan. In our material of 61 patients who were reported by the surgeon and the pathologist to be radically operated, we identified 38 patients (62%) who had recurrent disease. The median follow-up time in our study was 90 months which is shorter than Moertel´s and this is probably the reason why there are a higher number of recurrences in his material.
We found that the most sensitive method for detecting a recurrence was P-CgA. It was the first method to indicate a recurrence alone in 23/38 (60.5%) patients and, in combination with other methods, in another 9/38 (23.7%) patients. Altogether, P-CgA was the first method to indicate recur-rent disease in 32/38 (84%) patients. In those cases where P-CgA was the only method to indicate a recurrence, it took a median of 39 months before the recurrence was confirmed either by radiology or, in one patient, by sur-gery due to adherences. P-CgA has previously been shown to be a better biochemical marker than U-5HIAA in patients with limited disease of a midgut carcinoid tumour (Eriksson et al 1991). It has also been shown to correlate with tumour volume in midgut carcinoid tumours both in animals (Kölby et al 2004) and humans (Janson et al 1997). However, to our knowl-edge, there are no studies comparing the efficacy of radiological and bio-

38
chemical investigations in detecting recurrences of midgut carcinoid tu-mours.
This study is retrospective and all radiological methods have not been performed at every check-up. However, CT and/or US was performed at the first follow-up and then every three to six month. Both radiological investi-gations were equally good as 11C-5-HTP PET in confirming recurrences. However, 11C-5-HTP PET was not performed in all patients and not repeat-edly and thus, may be superior to the other radiological investigations in detecting or confirming recurrences. We know from a previous study by Örlefors et al (2005) that 11C-5-HTP PET is superior to CT and sst-scan in detecting small lesions of endocrine tumours. However, 11C-5-HTP PET is a very expensive investigation and few centers have the possibility to synthe-size 11C-5-HTP. It is therefore not suitable to perform as a repeated investi-gation in the work-up of a radically operated midgut carcinoid patient. It should be restricted to selected cases where there is suspicion of a recurrence and where other methods have failed to detect a tumour. Sst-scans have been performed in almost all the patients, however not repeatedly, and therefore perhaps the efficacy of this method is underestimated in this study. However, one of the known situations where there is a problem with this method is in detection of small lesions (<1cm). Today many work-up schedules include biochemical and radiological investigations several times a year. With the knowledge that P-CgA is the most sensitive method to detect recurrences, we suggest that an asymptomatic patient with a radically operated malignant midgut carcinoid tumour should be monitored by P-CgA twice a year and, in suitable patients, US otherwise CT annually. In patients with increased P-CgA or symptoms of a carcinoid tumour (carcinoid syndrome or abdominal pain), available imaging techniques (US, CT, sst-scan and/or 11C-5-HTPPET) should be used in order to localize the tumour.
Study II The second study was performed to investigate if new treatment options have improved survival in malignant midgut carcinoid patients. Patient char-acteristics were recorded as well as response rate and duration of the re-sponses on first-line treatment. In previous studies from the 1960´s, median survival was five years from diagnosis (Moertel et al 1961). In studies from the 1990´s, the five-year survival in patients with liver metastases was re-ported to be 45-50% (Janson et al 1997, and Kölby et al 2003) whereas those with limited disease had a five-year survival of 100% (Wängberg et al 1996). In a recent study including more than 13 000 carcinoid patients comprising patients from 1959 to 2003, the five-year survival in small intestine midgut carcinoid tumours, regardless of extent of disease, was 60% (Modlin et al 2003). In a study from Pape et al 2004, they report of a five-year survival of 70%. However, in the study there are only 88 midgut carcinoid patients in-

39
cluded and the median duration of follow-up is only two years. Most studies have included patients diagnosed prior to the time when IFN and soma-tostatin analogues became available and therefore we chose to include pa-tients diagnosed when these compounds were available.
The five-year survival was 77% in our material which is better than re-ported in other homogenous malignant midgut carcinoid materials. The me-dian age at diagnosis is the same as in previous studies and earlier diagnosis is therefore probably not the cause of the improved survival rate. Instead, improved medical treatment is more likely to be one of the reasons for this prolonged survival. However, no study has been performed comparing sur-vival between treated and untreated patients. Other new treatment options have also become available during the observation time such as RF ablation of liver metastases and PRRT with 111In-Pentetreotide or [111In-DTPA] Oc-treotide, 90Y-DOTATOC and [177Lu-DOTA0,Tyr3] Octreotate. Resection of liver metastases has also become more feasible during the period of follow-up. The only method that has been shown to increase survival is surgery with removal of the primary tumour, removal of the mesenteric lymph node me-tastases and aggressive resection of liver metastases (Hellman et al 2002, and Yao et al 2001) and, even in these studies, there is no randomization. We have used all these methods in a multidisciplinary way and we believe that this concept is the reason for the increased survival.
Carcinoid heart disease is part of the carcinoid syndrome which usually develops when liver metastases are present. In our material, we have more patients with both liver metastases and the carcinoid syndrome than are usu-ally present in studies. Despite this fact, the frequency of carcinoid heart disease in our study (11%) is lower than in other studies (30-70%) (Norheim et al 1987, and Westberg et al 2001). Recently, a Norwegian group showed that continuous infusion of serotonin in rats gave pathological changes in the heart similar to that found in carcinoid heart disease (Gustafsson et al 2005). Both IFN and somatostatin analogues reduce serotonin production and, since almost all our patients had either of the compounds and often both, this might be the reason for the lower frequency in our study compared to previ-ous ones. However, in a multivariate analysis, presence of carcinoid heart disease is still an independent poor prognostic factor in carcinoid patients.
Comparison of responses between different first-line treatments in retro-spective studies is difficult. First-line treatment is often selected with regard to treatment side-effects, other concurrent diseases and preference of the doctor. In our material, patients with high age, autoimmune diseases, coro-nary heart disease and those with severe psychiatric disorders have received a somatostatin analogue as single treatment while patients with minimal disease and no carcinoid syndrome have received IFN. Those with more severe symptoms and probably with the largest tumour bulk have received the combination of alpha-IFN and a somatostatin analogue. There were no significant differences in survival between the treatment groups in our study.

40
However, it is interesting to note that the largest group of radiological re-sponders was found in the combination treatment group (5%) and that this group also had the highest frequency of biochemical responders (65%).
Previous randomized studies with IFN and somatostatin analogues have not shown any advantage in survival for IFN-treated patients as compared with those treated with a somatostatin analogue alone. However, in two of the studies there was a heterogeneous patient material with other tumors than midgut carcinoids included (Frank et al 1999 and Faiss et al 2003) and, in a sub-analysis, midgut carcinoid tumours responded better to IFN treatment than other tumours. In another patient material similar to ours with malig-nant midgut carcinoid tumours only, there was a significantly longer time to progression in patients treated with the combination than in those treated with octreotide alone (Kölby et al 2003). It has also been shown that, in pa-tients responding to IFN, survival is prolonged if treatment is continued with IFN compared to those who stopped treatment (Jacobsen et al 1995). As with all rare diseases, it is difficult to recruit patients to studies. Many centers collect patients with tumours that have different features and many of the patients should probably receive other kinds of treatments. Because of the heterogeneity of groups, it is difficult to identify differences in survival be-tween different treatments. In our material, we found a higher five-year sur-vival than has previously been described in a pure malignant midgut carci-noid tumour material. We cannot however say what causes this and therefore randomized multicentre studies with homogeneous materials need to be per-formed in order to answer the question of what treatment should be pre-ferred.
Study III In the third paper, a study was performed to explore if an ultra-high dose of octreotide could increase the response rate as compared to the response achieved by regular doses. Tumour biology studies of tumour tissues were also performed to investigate if octreotide affected tumour growth. In previ-ous studies, cell-cycle inhibition, apoptosis and anti-angiogenesis have been shown to be induced by octreotide (Imam et al 1997, Pages et al 1999, and Garcia de la Torre 2002).
In this study, there were no radiological responses. However, this study included patients with disseminated metastatic disease who had failed on several standard treatments; nine out of 12 achieved stable radiological dis-ease for a median of 12 months. The success of this treatment could of course be debated since there were no radiological responses. However, one should remember that all patients were in a progressive phase of their dis-ease at the time of inclusion in the study and most of them had received all

41
available treatments for midgut carcinoid tumours. Eight of twelve had a Ki67 index that was much higher than is usually seen in midgut carcinoid tumours (>1%). This indicates that the patients included had tumours with a high proliferation. In this severely ill group of patients octreotide pamoate 160 mg was able to stabilize the tumour growth in 75% of the patients for a median of 12 months. Regarding the biochemical responses, all but two con-tinued on high doses of somatostatin analogues until three days prior to base-line. It is therefore possible that there was a suppression of the biochemical markers still present due to that medication. Still, an positive effect for most of the patients was obtained. The Ki67 index decreased in several patients while tumour growth was stabilized. To obtain such good results in this group of late stage patients with almost no side-effects may be considered as an important step forward in the management of midgut carcinoid tumours.
Study IV In paper four, we identified TKRs that could be targeted with TKRI. Several different tumours have been reported to respond to TKRI treatment (colon, head-and-neck, GIST and CML). It has been shown that for small molecules such as imatinib you do not only need the expression but also a mutation in the receptor to achieve a response. This also seems to be true for gefitinib in non-small cell lung cancer where it was shown that responders had a muta-tion in the EGFR. However, on the other hand, some of the monoclonal anti-bodies used do not seem to need the EGFR expression to be effective in treatment. An example of this is colon cancer. There is only scattered infor-mation about TKR expression in midgut carcinoid tumours in the literature and most studies performed so far have included few patients. In our study, we showed that 38% of the tumours had expression of PDGFR , 88% of PDGFR , 73% of EGFR while none expressed c-kit. This indicates, together with previous observations, that midgut carcinoid tumours express at least three out of the four receptors tested. The expression of c-kit receptor has not yet been reported in any other studies but our results indicate that it is proba-bly not frequently expressed in midgut carcinoid tumours.
Treatment studies with TKRI in midgut carcinoid tumours have not been published. In an abstract, Yao et al (2003) reported early data of 15 unde-fined carcinoids treated with imatinib. No radiological responses were re-ported but ten patients had stable disease. In paper four, we report of a pa-tient who was in a progressive phase although treated with several of the available treatments. He was stabilized for more than a year when treated with imatinib in addition to -IFN and octreotide. Unfortunately, the TKR expression in his tumour could not be investigated due to complicating dis-ease making it impossible to take a biopsy. Thus, we can only speculate about how imatinib acted on the tumour. One mechanism could of course be a direct effect on the receptor, inhibiting further cell proliferation. Another possible mechanism could be that imatinib through binding to PDGFR in the

42
tumour stroma, might reduce the intra-tumoural stromal pressure and thereby allow more of the anti-tumoural treatment to reach the tumour cells. Such an effect has been proposed by Pietras et al (2002) in animal experiments. It is still unknown if there are mutations in the EGFR in midgut carcinoid tu-mours. However, in a study from Höpfner et al (2003), three different neuro-endocrine tumour cell-lines responded to gefitinib treatment. In a study by Papouchado et al (2005), an activated EGFR was reported to occur in a high frequency in midgut carcinoid tumours. They claimed to have started clinical trials with gefitinib in midgut carcinoid patients but there is no report on the outcome of such treatment yet. If midgut carcinoid tumours fail to respond to small molecules, it would also be interesting to try monoclonal antibodies directed towards EGFR, since these have shown responses in several tu-mours also without the expression of EGFR.

43
Conclusion
P-CgA is more sensitive than U-5HIAA and imaging techniques (US, CT, sst-scan) to detect recurrent disease in radically operated malignant mid-gut carcinoid tumours.
The median survival in 284 malignant midgut carcinoid tumours treated at our centre 1990-2006 is 115.5 months and the five-year survival rate is 77%. These figures are higher than those previously reported for malig-nant midgut carcinoid tumours.
Carcinoid heart disease seems to be less common in our material as com-pared with historical reports.
Carcinoid heart disease, liver metastases and old age were identified as independently poor prognostic factors in the multivariate analysis.
Treatment with octreotide pamoate in advanced malignant midgut carci-noid tumours stabilised the disease for a long period of time without any severe side effects and may be an important addition to the therapeutic ar-senal for patients with advanced disease.
Malignant midgut carcinoid tumours express PDGFR and EGFR in more than 70% of cases. PDGFR was expressed in 38% of the examined tu-mours. C-kit was not expressed in any midgut carcinoid tumour.
BON-1 cells expressed PDGFR in western blot analysis and, after stimu-lation with PDGF, there was an activation of the receptor, indicating that it is a possible target for anti-tumoural treatment. This will have to be ex-plored in future studies.
44
Acknowledgements
During my time at the Department of Endocrine Oncology I have met and worked with several people that have made these last ten years joyful, inter-esting and stimulating. They have inspired, taught, guided, helped, criticised and supported me. There are so many that I can not mention everyone but I would like to mention:
Eva T. Janson, my supervisor, for your enthusiasm, incredible working ca-pacity, guidance and assistance during my research work, for your energy, for knowing when to put pressure on me and when to let go.
Barbro Eriksson, my co supervisor, boss and clinical mentor for always be-lieving in me and for always having time when needed, for your assistance and help during my research, especially your exquisite language. Thank you for the nice trips in business, for drinking Margaritas and smoking Cuban cigars.
Britt Skogseid, my co author, for introducing me to research, for sharing your vast knowledge in the fascinating world of hereditary diseases, for all stimulating rounds and discussions about anything from difficult medical problems to figure skating. For walks in the red light district and an astonish-ing van Gogh exhibition.
Kjell Öberg, the Dean of the Medical Faculty and the founder of the unit of Endocrine Oncology in Uppsala. Thank you for your never ending enthusi-asm, curiosity and for sharing your vast knowledge in endocrine tumours. Special thanks for the snow scooter trip among hungry polar bears.
Dan Granberg, co author and colleague, for your loyalty, working capacity and friendship.
Janet Cunningham, Marie-Louise Fjällskog, Henrik Kindmark, Jan Saras, Mats Stridsberg, and Anders Sundin, my co authors and colleagues for good collaboration and sharing valuable knowledge to make this work possible.
Christina Kampanellou, Gordana Kozvolacki, Ylva Nordgren, Mattias Sigurd, Apostolos Tsolakis, Håkan Örlefors and all colleagues who have worked at 70CM, 30B2 and 78D, for good collaboration and making the ward a pleasant place to be.
45
Monica Hurtig, retired, but not tired, research nurse and former head of the ward, for your caring of every staff, patient or relative. For all the social activities you arranged, the good care of my children and for your great commitment in the Department.
Åsa Forsberg and Margareta Halin Lejonklou, for teaching me the technique of immunohistochemistry and for giving me technical assistance when any-thing went wrong.
Gunnel Larsson, for guiding me in my first fumbling statistical manoeuvres and for being such a nice person.
Annette Hägg, for all your enormous help with papers, Endnote, copying and everything around the dissertation. For our many discussions (although I am a no good rheumatologist or gastro enterologist).
Mikael Björk, for all your help with computers and programs, good talks about life and for accompanying me, sleeping in the stable at planning meet-ings.
All the staff at 70CM, 30B2 and 78D, for making the ward such a nice place to spend working and spare time. Special thanks to Gertrud Fredriksson for always having a helping hand when needed.
All our friends, who make spare time (whatever that is) more enjoyable, for dinners, parties, swimming and travelling company.
Arne, Ulla, John and Viktoria, my second family, for always helping out when we need you.
Björn and Charlotte, my brother and sister with families, for always being there when needed.
Lars and Maj-Britt, my parents, for your love and support through life.
Hampus and Ellen, for being the joy of my life, always and forever.
Klara, whom without I would be a general practioner in Jämtland. You are everything to me and nothing of this had been possible without you and your help. I love you!
And finally all the patients, whom without this work never would have been possible.
…………………………………. For those who I forgot and should have been mentioned, please sign your name.

46
References
Ahlman H, Dahlstrom A, Gronstad K, Jaffe BM, Nilsson O, Oberg K 1985 The pentagastrin test in the diagnosis of the carcinoid syndrome. J Cardiovasc Phar-macol 7 Suppl 7:S86-88
Ahlman H, Friman S, Cahlin C, Nilsson O, Jansson S, Wangberg B, Olausson M 2004 Liver transplantation for treatment of metastatic neuroendocrine tumors. Ann N Y Acad Sci 1014:265-269
Ajani JA, Carrasco CH, Charnsangavej C, Samaan NA, Levin B, Wallace S 1988 Islet cell tumors metastatic to the liver: effective palliation by sequential hepatic artery embolization. Ann Intern Med 108:340-344
Anthony L, Johnson D, Hande K, Shaff M, Winn S, Krozely M, Oates J 1993 Somatostatin analogue phase I trials in neuroendocrine neoplasms. Acta Oncol 32:217-223
Anthony LB, Woltering EA, Espenan GD, Cronin MD, Maloney TJ, McCarthy KE 2002 Indium-111-pentetreotide prolongs survival in gastroenteropancreatic ma-lignancies. Semin Nucl Med 32:123-132
Arnold R, Benning R, Neuhaus C, Rolwage M, Trautmann ME 1993 Gastroentero-pancreatic endocrine tumours: effect of Sandostatin on tumour growth. The German Sandostatin Study Group. Digestion 54 Suppl 1:72-75
Bajetta E, Procopio G, Ferrari L, Martinetti A, Zilembo N, Catena L, Alu M, Della TS, Alberti D, Buzzoni R 2002 A randomized, multicenter prospective trial as-sessing long-acting release octreotide pamoate plus tamoxifen as a first line therapy for advanced breast carcinoma. Cancer 94:299-304
Balster DA, O'Dorisio MS, Summers MA, Turman MA 2001 Segmental expression of somatostatin receptor subtypes sst(1) and sst(2) in tubules and glomeruli of human kidney. Am J Physiol Renal Physiol 280:F457-465
Bauer W, Briner U, Doepfner W, Haller R, Huguenin R, Marbach P, Petcher TJ, Pless 1982 SMS 201-995: a very potent and selective octapeptide analogue of somatostatin with prolonged action. Life Sci 31:1133-1140
Bell GI, Reisine T 1993 Molecular biology of somatostatin receptors. Trends Neu-rosci 16:34-38
Biesma B, Willemse PH, Mulder NH, Verschueren RC, Kema IP, de Bruijn HW, Postmus PE, Sleijfer DT, de Vries EG 1992 Recombinant interferon alpha-2b in patients with metastatic apudomas: effect on tumours and tumour markers. Br J Cancer 66:850-855
Blaschko H, Comline RS, Schneider FH, Silver M, Smith AD 1967 Secretion of a chromaffin granule protein, chromogranin, from the adrenal gland after splanchnic stimulation. Nature 215:58-59
Board R, Jayson GC 2005 Platelet-derived growth factor receptor (PDGFR): a tar-get for anticancer therapeutics. Drug Resist Updat 8:75-83
Borch K, Stridsberg M, Burman P, Rehfeld JF 1997 Basal chromogranin A and gastrin concentrations in circulation correlate to endocrine cell proliferation in type-A gastritis. Scand J Gastroenterol 32:198-202

47
Brazeau P, Vale W, Burgus R, Ling N, Butcher M, Rivier J, Guillemin R 1973 Hypothalamic polypeptide that inhibits the secretion of immunoreactive pitui-tary growth hormone. Science 179:77-79
Bruns C, Lewis I, Briner U, Meno-Tetang G, Weckbecker G 2002 SOM230: a novel somatostatin peptidomimetic with broad somatotropin release inhibiting factor (SRIF) receptor binding and a unique antisecretory profile. Eur J Endo-crinol 146:707-716
Buscombe JR, Caplin ME, Hilson AJ 2003 Long-term efficacy of high-activity 111in-pentetreotide therapy in patients with disseminated neuroendocrine tu-mors. J Nucl Med 44:1-6
Caron P, Buscail L, Beckers A, Esteve JP, Igout A, Hennen G, Susini C 1997 Ex-pression of somatostatin receptor SST4 in human placenta and absence of oc-treotide effect on human placental growth hormone concentration during preg-nancy. J Clin Endocrinol Metab 82:3771-3776
Chaudhry A, Papanicolaou V, Oberg K, Heldin CH, Funa K 1992 Expression of platelet-derived growth factor and its receptors in neuroendocrine tumors of the digestive system. Cancer Res 52:1006-1012
Chen F, O'Dorisio MS, Hermann G, Hayes J, Malarkey WB, O'Dorisio TM 1993 Mechanisms of action of long-acting analogs of somatostatin. Regul Pept 44:285-295
Connolly HM, Crary JL, McGoon MD, Hensrud DD, Edwards BS, Edwards WD, Schaff HV 1997 Valvular heart disease associated with fenfluramine-phentermine. N Engl J Med 337:581-588
Cunningham J, Janson ET, Agarwal S, Grimelius L, Stridsberg M. Expression of tachykinins in neuroendocrine tumours and their possible role for carcinoid diar-rhea. (manuscript)
del Pozo E, Neufeld M, Schluter K, Tortosa F, Clarenbach P, Bieder E, Wendel L, Nuesch E, Marbach P, Cramer H, et al. 1986 Endocrine profile of a long-acting somatostatin derivative SMS 201-995. Study in normal volunteers following subcutaneous administration. Acta Endocrinol (Copenh) 111:433-439
Di Bartolomeo M, Bajetta E, Zilembo N, de Braud F, Di Leo A, Verusio C, D'Aprile M, Scanni A, Barduagni M, Barduagni A, et al. 1993 Treatment of car-cinoid syndrome with recombinant interferon alpha-2a. Acta Oncol 32:235-238
Elvin A, Skogseid B, Hellman P 2005 Radiofrequency ablation of neuroendocrine liver metastases. Abdom Imaging 30:427-434
Eriksson B, Oberg K 1991 Peptide hormones as tumor markers in neuroendocrine gastrointestinal tumors. Acta Oncol 30:477-483
Eriksson B, Renstrup J, Imam H, Oberg K 1997 High-dose treatment with lanreo-tide of patients with advanced neuroendocrine gastrointestinal tumors: clinical and biological effects. Ann Oncol 8:1041-1044
Eriksson BK, Larsson EG, Skogseid BM, Lofberg AM, Lorelius LE, Oberg KE 1998 Liver embolizations of patients with malignant neuroendocrine gastroin-testinal tumors. Cancer 83:2293-2301
Faiss S, Pape UF, Bohmig M, Dorffel Y, Mansmann U, Golder W, Riecken EO, Wiedenmann B 2003 Prospective, randomized, multicenter trial on the antipro-liferative effect of lanreotide, interferon alfa, and their combination for therapy of metastatic neuroendocrine gastroenteropancreatic tumors--the International Lanreotide and Interferon Alfa Study Group. J Clin Oncol 21:2689-2696
Feldman JM, O'Dorisio TM 1986 Role of neuropeptides and serotonin in the diag-nosis of carcinoid tumors. Am J Med 81:41-48
48
Ferjoux G, Bousquet C, Cordelier P, Benali N, Lopez F, Rochaix P, Buscail L, Susini C 2000 Signal transduction of somatostatin receptors negatively control-ling cell proliferation. J Physiol Paris 94:205-210
Fjallskog ML, Lejonklou MH, Oberg KE, Eriksson BK, Janson ET 2003 Expres-sion of molecular targets for tyrosine kinase receptor antagonists in malignant endocrine pancreatic tumors. Clin Cancer Res 9:1469-1473
Florio T, Yao H, Carey KD, Dillon TJ, Stork PJ 1999 Somatostatin activation of mitogen-activated protein kinase via somatostatin receptor 1 (SSTR1). Mol En-docrinol 13:24-37
Frank M, Klose KJ, Wied M, Ishaque N, Schade-Brittinger C, Arnold R 1999 Combination therapy with octreotide and alpha-interferon: effect on tumor growth in metastatic endocrine gastroenteropancreatic tumors. Am J Gastroen-terol 94:1381-1387
Fudge K, Wang CY, Stearns ME 1994 Immunohistochemistry analysis of platelet-derived growth factor A and B chains and platelet-derived growth factor alpha and beta receptor expression in benign prostatic hyperplasias and Gleason-graded human prostate adenocarcinomas. Mod Pathol 7:549-554
Funa K, Papanicolaou V, Juhlin C, Rastad J, Akerstrom G, Heldin CH, Oberg K 1990 Expression of platelet-derived growth factor beta-receptors on stromal tis-sue cells in human carcinoid tumors. Cancer Res 50:748-753
Garcia de la Torre N, Wass JA, Turner HE 2002 Antiangiogenic effects of soma-tostatin analogues. Clin Endocrinol (Oxf) 57:425-441
Gavrieli Y, Sherman Y, Ben-Sasson SA 1992 Identification of programmed cell death in situ via specific labeling of nuclear DNA fragmentation. J Cell Biol 119:493-501
Gustafsson BI, Tommeras K, Nordrum I, Loennechen JP, Brunsvik A, Solligard E, Fossmark R, Bakke I, Syversen U, Waldum H 2005 Long-term serotonin ad-ministration induces heart valve disease in rats. Circulation 111:1517-1522
Heiman ML, Murphy WA, Coy DH 1987 Differential binding of somatostatin ago-nists to somatostatin receptors in brain and adenohypophysis. Neuroendocrinol-ogy 45:429-436
Helle SI, Geisler J, Poulsen JP, Hestdal K, Meadows K, Collins W, Tveit KM, Holly JM, Lonning PE 1998 Microencapsulated octreotide pamoate in advanced gastrointestinal and pancreatic cancer: a phase I study. Br J Cancer 78:14-20
Hellman P, Lundstrom T, Ohrvall U, Eriksson B, Skogseid B, Oberg K, Tiensuu Janson E, Akerstrom G 2002 Effect of surgery on the outcome of midgut carci-noid disease with lymph node and liver metastases. World J Surg 26:991-997
Hellman P, Ladjevardi S, Skogseid B, Akerstrom G, Elvin A 2002 Radiofrequency tissue ablation using cooled tip for liver metastases of endocrine tumors. World J Surg 26:1052-1056
Henriksen R, Funa K, Wilander E, Backstrom T, Ridderheim M, Oberg K 1993 Expression and prognostic significance of platelet-derived growth factor and its receptors in epithelial ovarian neoplasms. Cancer Res 53:4550-4554
Hermanson M, Funa K, Hartman M, Claesson-Welsh L, Heldin CH, Westermark B, Nister M 1992 Platelet-derived growth factor and its receptors in human glioma tissue: expression of messenger RNA and protein suggests the presence of autocrine and paracrine loops. Cancer Res 52:3213-3219
Hirota S, Isozaki K, Moriyama Y, Hashimoto K, Nishida T, Ishiguro S, Kawano K, Hanada M, Kurata A, Takeda M, Muhammad Tunio G, Matsuzawa Y, Kana-kura Y, Shinomura Y, Kitamura Y 1998 Gain-of-function mutations of c-kit in human gastrointestinal stromal tumors. Science 279:577-580
49
Hopfner M, Sutter AP, Gerst B, Zeitz M, Scherubl H 2003 A novel approach in the treatment of neuroendocrine gastrointestinal tumours. Targeting the epidermal growth factor receptor by gefitinib (ZD1839). Br J Cancer 89:1766-1775
Hsiao RJ, Mezger MS, O'Connor DT 1990 Chromogranin A in uremia: progressive retention of immunoreactive fragments. Kidney Int 37:955-964
Hsiao RJ, Seeger RC, Yu AL, O'Connor DT 1990 Chromogranin A in children with neuroblastoma. Serum concentration parallels disease stage and predicts sur-vival. J Clin Invest 85:1555-1559
Imam H, Eriksson B, Lukinius A, Janson ET, Lindgren PG, Wilander E, Oberg K 1997 Induction of apoptosis in neuroendocrine tumors of the digestive system during treatment with somatostatin analogs. Acta Oncol 36:607-614
Isaacs A, Lindenmann J 1957 Virus interference. I. The interferon. Proc R Soc Lond B Biol Sci 147:258-267
Isler P, Hedinger C 1953 Metastatic carcinoid of the small intestine with severe valvular defects especially in the right part of the heart and with pulmonary stenosis; a peculiar symptom complex. Schweiz Med Wochenschr 83:4-7
Jacobsen MB, Hanssen LE, Kolmannskog F, Schrumpf E, Vatn MH, Bergan A 1995 Interferon-alpha 2b, with or without prior hepatic artery embolization: clinical response and survival in mid-gut carcinoid patients. The Norwegian car-cinoid study. Scand J Gastroenterol 30:789-796
Janson ET, Holmberg L, Stridsberg M, Eriksson B, Theodorsson E, Wilander E, Oberg K 1997 Carcinoid tumors: analysis of prognostic factors and survival in 301 patients from a referral center. Ann Oncol 8:685-690
Kolby L, Bernhardt P, Sward C, Johanson V, Ahlman H, Forssell-Aronsson E, Stridsberg M, Wangberg B, Nilsson O 2004 Chromogranin A as a determinant of midgut carcinoid tumour volume. Regul Pept 120:269-273
Kolby L, Persson G, Franzen S, Ahren B 2003 Randomized clinical trial of the effect of interferon alpha on survival in patients with disseminated midgut car-cinoid tumours. Br J Surg 90:687-693
Kwekkeboom DJ, Teunissen JJ, Bakker WH, Kooij PP, de Herder WW, Feelders RA, van Eijck CH, Esser JP, Kam BL, Krenning EP 2005 Radiolabeled soma-tostatin analog [177Lu-DOTA0,Tyr3]octreotate in patients with endocrine gas-troenteropancreatic tumors. J Clin Oncol 23:2754-2762
Kvols L Oberg K, de Herder W, Anthony L, Glusman J, Tran LL, Widenmann B 2005 Early data on the efficacy and safety of the novel multi-ligand soma-tostatin analog, SOM230, in patients with metastatic carcinoid tumors refractory or resistant to octreotide LAR. ASCO Annual Meeting Proceedings Vol 23:8024
Kvols LK, Moertel CG, O'Connell MJ, Schutt AJ, Rubin J, Hahn RG 1986 Treat-ment of the malignant carcinoid syndrome. Evaluation of a long-acting soma-tostatin analogue. N Engl J Med 315:663-666
Lamberts SW, van der Lely AJ, de Herder WW, Hofland LJ 1996 Octreotide. N Engl J Med 334:246-254
Lembcke B, Creutzfeldt W, Schleser S, Ebert R, Shaw C, Koop I 1987 Effect of the somatostatin analogue sandostatin (SMS 201-995) on gastrointestinal, pancre-atic and biliary function and hormone release in normal men. Digestion 36:108-124
Lembeck F 1953 5-Hydroxytryptamine in a carcinoid tumour. Nature 172:910-911 Le Treut YP, Delpero JR, Dousset B, Cherqui D, Segol P, Mantion G, Hannoun L,
Benhamou G, Launois B, Boillot O, Domergue J, Bismuth H 1997 Results of liver transplantation in the treatment of metastatic neuroendocrine tumors. A 31-case French multicentric report. Ann Surg 225:355-364
50
Lundin L, Norheim I, Landelius J, Oberg K, Theodorsson-Norheim E 1988 Carci-noid heart disease: relationship of circulating vasoactive substances to ultra-sound-detectable cardiac abnormalities. Circulation 77:264-269
McDermott EW, Guduric B, Brennan MF 1994 Prognostic variables in patients with gastrointestinal carcinoid tumours. Br J Surg 81:1007-1009
McFadden D, Zinner MJ, Jaffe BM 1986 Substance P-induced intestinal secretion of water and electrolytes. Gut 27:267-272
Mellstroom K, Hoglund AS, Nister M, Heldin CH, Westermark B, Lindberg U. The effect of platelet-derived growth factor on morphology and motility of human glial cells. J Muscle Res Cell Motil 1983; 4:589-609.
Mengel C, R S The Carcinoid Syndrome. In: Alimentary Tract Cancer; 1584-1594 Modlin IM, Lye KD, Kidd M 2003 A 5-decade analysis of 13,715 carcinoid tumors.
Cancer 97:934-959 Moertel CG 1987 Karnofsky memorial lecture. An odyssey in the land of small
tumors. J Clin Oncol 5:1502-1522 Moertel CG, Johnson CM, McKusick MA, Martin JK, Jr., Nagorney DM, Kvols
LK, Rubin J, Kunselman S 1994 The management of patients with advanced carcinoid tumors and islet cell carcinomas. Ann Intern Med 120:302-309
Moertel CG, Rubin J, Kvols LK 1989 Therapy of metastatic carcinoid tumor and the malignant carcinoid syndrome with recombinant leukocyte A interferon. J Clin Oncol 7:865-868
Moertel CG, Sauer WG, Dockerty MB, Baggenstoss AH 1961 Life history of the carcinoid tumor of the small intestine. Cancer 14:901-912
Moertel CG, Weiland LH, Nagorney DM, Dockerty MB 1987 Carcinoid tumor of the appendix: treatment and prognosis. N Engl J Med 317:1699-1701
Nilsson O, Wangberg B, Kolby L, Schultz GS, Ahlman H 1995 Expression of trans-forming growth factor alpha and its receptor in human neuroendocrine tumours. Int J Cancer 60:645-651
Norheim I, Oberg K, Theodorsson-Norheim E, Lindgren PG, Lundqvist G, Mag-nusson A, Wide L, Wilander E 1987 Malignant carcinoid tumors. An analysis of 103 patients with regard to tumor localization, hormone production, and sur-vival. Ann Surg 206:115-125
Norheim I, Theodorsson-Norheim E, Brodin E, Oberg K 1986 Tachykinins in car-cinoid tumors: their use as a tumor marker and possible role in the carcinoid flush. J Clin Endocrinol Metab 63:605-612
Oberg K, Funa K, Alm G 1983 Effects of leukocyte interferon on clinical symp-toms and hormone levels in patients with mid-gut carcinoid tumors and carci-noid syndrome. N Engl J Med 309:129-133
Oberg K, Norheim I, Lind E, Alm G, Lundqvist G, Wide L, Jonsdottir B, Magnus-son A, Wilander E 1986 Treatment of malignant carcinoid tumors with human leukocyte interferon: long-term results. Cancer Treat Rep 70:1297-1304
Oberndorfer S 1907 Karzinoide Tumoren des Dünndarms. In: Frankfurter Zeitschrift für Pathologie; 426-432
Ohrvall U, Eriksson B, Juhlin C, Karacagil S, Rastad J, Hellman P, Akerstrom G 2000 Method for dissection of mesenteric metastases in mid-gut carcinoid tu-mors. World J Surg 24:1402-1408
Orlefors H, Sundin A, Garske U, Juhlin C, Oberg K, Skogseid B, Langstrom B, Bergstrom M, Eriksson B 2005 Whole-body (11)C-5-hydroxytryptophan posi-tron emission tomography as a universal imaging technique for neuroendocrine tumors: comparison with somatostatin receptor scintigraphy and computed to-mography. J Clin Endocrinol Metab 90:3392-3400

51
Otte A, Herrmann R, Macke HR, Muller-Brand J 1999 [Yttrium 90 DOTATOC: a new somatostatin analog for cancer therapy of neuroendocrine tumors]. Schweiz Rundsch Med Prax 88:1263-1268
Page IH, Corcoran AC, Udenfriend S, Szoedsma A, Weissbach H 1955 Argentaffi-noma as endocrine tumour. Lancet 268:198-199
Pages P, Benali N, Saint-Laurent N, Esteve JP, Schally AV, Tkaczuk J, Vaysse N, Susini C, Buscail L 1999 sst2 somatostatin receptor mediates cell cycle arrest and induction of p27(Kip1). Evidence for the role of SHP-1. J Biol Chem 274:15186-15193
Palmu S, Soderstrom KO, Quazi K, Isola J, Salminen E 2002 Expression of C-KIT and HER-2 tyrosine kinase receptors in poor-prognosis breast cancer. Antican-cer Res 22:411-414
Pape UF, Bohmig M, Berndt U, Tiling N, Wiedenmann B, Plockinger U 2004 Sur-vival and clinical outcome of patients with neuroendocrine tumors of the gastro-enteropancreatic tract in a german referral center. Ann N Y Acad Sci 1014:222-233
Papouchado B, Erickson LA, Rohlinger AL, Hobday TJ, Erlichman C, Ames MM, Lloyd RV 2005 Epidermal growth factor receptor and activated epidermal growth factor receptor expression in gastrointestinal carcinoids and pancreatic endocrine carcinomas. Mod Pathol 18:1329-1335
Pietras K, Rubin K, Sjoblom T, Buchdunger E, Sjoquist M, Heldin CH, Ostman A 2002 Inhibition of PDGF receptor signaling in tumor stroma enhances antitumor effect of chemotherapy. Cancer Res 62:5476-5484
Pradayrol L, Chayvialle J, Mutt V 1978 Pig duodenal somatostatin: extraction and purification. Metabolism 27:1197-1200
Rajamannan NM, Caplice N, Anthikad F, Sebo TJ, Orszulak TA, Edwards WD, Tajik J, Schwartz RS 2001 Cell proliferation in carcinoid valve disease: a mechanism for serotonin effects. J Heart Valve Dis 10:827-831
Reardon DB, Dent P, Wood SL, Kong T, Sturgill TW 1997 Activation in vitro of somatostatin receptor subtypes 2, 3, or 4 stimulates protein tyrosine phosphatase activity in membranes from transfected Ras-transformed NIH 3T3 cells: coex-pression with catalytically inactive SHP-2 blocks responsiveness. Mol Endocri-nol 11:1062-1069
Reubi JC, Laissue JA, Waser B, Steffen DL, Hipkin RW, Schonbrunn A 1999 Im-munohistochemical detection of somatostatin sst2a receptors in the lymphatic, smooth muscular, and peripheral nervous systems of the human gastrointestinal tract: facts and artifacts. J Clin Endocrinol Metab 84:2942-2950
Rindi G, Capella C, Solcia E 2000 Introduction to a revised clinicopathological classification of neuroendocrine tumors of the gastroenteropancreatic tract. Q J Nucl Med 44:13-21
Ronnblom LE, Alm GV, Oberg KE 1991 Autoimmunity after alpha-interferon therapy for malignant carcinoid tumors. Ann Intern Med 115:178-183
Ronnstrand L 2004 Signal transduction via the stem cell factor receptor/c-Kit. Cell Mol Life Sci 61:2535-2548
Ruszniewski P, Ducreux M, Chayvialle JA, Blumberg J, Cloarec D, Michel H, Raymond JM, Dupas JL, Gouerou H, Jian R, Genestin E, Bernades P, Rougier P 1996 Treatment of the carcinoid syndrome with the longacting somatostatin analogue lanreotide: a prospective study in 39 patients. Gut 39:279-283
Ruszniewski P, Rougier P, Roche A, Legmann P, Sibert A, Hochlaf S, Ychou M, Mignon M 1993 Hepatic arterial chemoembolization in patients with liver me-tastases of endocrine tumors. A prospective phase II study in 24 patients. Cancer 71:2624-2630
52
Salomon DS, Brandt R, Ciardiello F, Normanno N 1995 Epidermal growth factor-related peptides and their receptors in human malignancies. Crit Rev Oncol Hematol 19:183-232
Sanduleanu S, Stridsberg M, Jonkers D, Hameeteman W, Biemond I, Lundqvist G, Lamers C, Stockbrugger RW 1999 Serum gastrin and chromogranin A during medium- and long-term acid suppressive therapy: a case-control study. Aliment Pharmacol Ther 13:145-153
Sauer WG, Dearing WH, Flock EV 1958 Diagnosis and clinical management of functioning carcinoids. J Am Med Assoc 168:139-147
Schaer JC, Waser B, Mengod G, Reubi JC 1997 Somatostatin receptor subtypes sst1, sst2, sst3 and sst5 expression in human pituitary, gastroentero-pancreatic and mammary tumors: comparison of mRNA analysis with receptor autoradio-graphy. Int J Cancer 70:530-537
Schlessinger J 2000 Cell signaling by receptor tyrosine kinases. Cell 103:211-225 Sharma K, Patel YC, Srikant CB 1999 C-terminal region of human somatostatin
receptor 5 is required for induction of Rb and G1 cell cycle arrest. Mol Endocri-nol 13:82-90
Sharma K, Patel YC, Srikant CB 1996 Subtype-selective induction of wild-type p53 and apoptosis, but not cell cycle arrest, by human somatostatin receptor 3. Mol Endocrinol 10:1688-1696
Stridsberg M, Eriksson B, Oberg K, Janson ET 2003 A comparison between three commercial kits for chromogranin A measurements. J Endocrinol 177:337-341
Strodel WE, Talpos G, Eckhauser F, Thompson N 1983 Surgical therapy for small-bowel carcinoid tumors. Arch Surg 118:391-397
Taniyama Y, Suzuki T, Mikami Y, Moriya T, Satomi S, Sasano H 2005 Systemic distribution of somatostatin receptor subtypes in human: an immunohistochemi-cal study. Endocr J 52:605-611
Teijeiro R, Rios R, Costoya JA, Castro R, Bello JL, Devesa J, Arce VM 2002 Acti-vation of human somatostatin receptor 2 promotes apoptosis through a mecha-nism that is independent from induction of p53. Cell Physiol Biochem 12:31-38
Thorson A, Biorck G, Bjorkman G, Waldenstrom J 1954 Malignant carcinoid of the small intestine with metastases to the liver, valvular disease of the right side of the heart (pulmonary stenosis and tricuspid regurgitation without septal defects), peripheral vasomotor symptoms, bronchoconstriction, and an unusual type of cyanosis; a clinical and pathologic syndrome. Am Heart J 47:795-817
Thulin L, Samnegard H, Tyden G, Long DH, Efendic S 1978 Efficacy of soma-tostatin in a patient with carcinoid syndrome. Lancet 2:43
Tian Q, Frierson HF, Jr., Krystal GW, Moskaluk CA 1999 Activating c-kit gene mutations in human germ cell tumors. Am J Pathol 154:1643-1647
Trendle MC, Moertel CG, Kvols LK 1997 Incidence and morbidity of cholelithiasis in patients receiving chronic octreotide for metastatic carcinoid and malignant islet cell tumors. Cancer 79:830-834
Tsuura Y, Hiraki H, Watanabe K, Igarashi S, Shimamura K, Fukuda T, Suzuki T, Seito T 1994 Preferential localization of c-kit product in tissue mast cells, basal cells of skin, epithelial cells of breast, small cell lung carcinoma and semi-noma/dysgerminoma in human: immunohistochemical study on formalin-fixed, paraffin-embedded tissues. Virchows Arch 424:135-141
Waldherr C, Pless M, Maecke HR, Schumacher T, Crazzolara A, Nitzsche EU, Haldemann A, Mueller-Brand J 2002 Tumor response and clinical benefit in neuroendocrine tumors after 7.4 GBq (90)Y-DOTATOC. J Nucl Med 43:610-616

53
Valkema R, De Jong M, Bakker WH, Breeman WA, Kooij PP, Lugtenburg PJ, De Jong FH, Christiansen A, Kam BL, De Herder WW, Stridsberg M, Lindemans J, Ensing G, Krenning EP 2002 Phase I study of peptide receptor radionuclide therapy with [In-DTPA]octreotide: the Rotterdam experience. Semin Nucl Med 32:110-122
Wangberg B, Westberg G, Tylen U, Tisell L, Jansson S, Nilsson O, Johansson V, Schersten T, Ahlman H 1996 Survival of patients with disseminated midgut car-cinoid tumors after aggressive tumor reduction. World J Surg 20:892-899; dis-cussion 899
Westberg G, Wangberg B, Ahlman H, Bergh CH, Beckman-Suurkula M, Caidahl K 2001 Prediction of prognosis by echocardiography in patients with midgut car-cinoid syndrome. Br J Surg 88:865-872
Westlin JE, Janson ET, Ahlstrom H, Ohrvall U, Arnberg H, Nilsson S, Akerstrom G, Oberg K 1992 [A new diagnostic method: somatostatin receptor scintigraphy of neuroendocrine tumors]. Lakartidningen 89:4377-4379
Williams ED, Sandler M 1963 The classification of carcinoid tum ours. Lancet 1:238-239
Wulbrand U, Wied M, Zofel P, Goke B, Arnold R, Fehmann H 1998 Growth factor receptor expression in human gastroenteropancreatic neuroendocrine tumours. Eur J Clin Invest 28:1038-1049
Wymenga AN, Eriksson B, Salmela PI, Jacobsen MB, Van Cutsem EJ, Fiasse RH, Valimaki MJ, Renstrup J, de Vries EG, Oberg KE 1999 Efficacy and safety of prolonged-release lanreotide in patients with gastrointestinal neuroendocrine tumors and hormone-related symptoms. J Clin Oncol 17:1111
Wynick D, Anderson JV, Williams SJ, Bloom SR 1989 Resistance of metastatic pancreatic endocrine tumours after long-term treatment with the somatostatin analogue octreotide (SMS 201-995). Clin Endocrinol (Oxf) 30:385-388
Yamada Y, Kagimoto S, Kubota A, Yasuda K, Masuda K, Someya Y, Ihara Y, Li Q, Imura H, Seino S, et al. 1993 Cloning, functional expression and pharmacol-ogical characterization of a fourth (hSSTR4) and a fifth (hSSTR5) human soma-tostatin receptor subtype. Biochem Biophys Res Commun 195:844-852
Yamada Y, Post SR, Wang K, Tager HS, Bell GI, Seino S 1992 Cloning and func-tional characterization of a family of human and mouse somatostatin receptors expressed in brain, gastrointestinal tract, and kidney. Proc Natl Acad Sci U S A 89:251-255
Yamada Y, Reisine T, Law SF, Ihara Y, Kubota A, Kagimoto S, Seino M, Seino Y, Bell GI, Seino S 1992 Somatostatin receptors, an expanding gene family: clon-ing and functional characterization of human SSTR3, a protein coupled to ade-nylyl cyclase. Mol Endocrinol 6:2136-2142
Yao KA, Talamonti MS, Nemcek A, Angelos P, Chrisman H, Skarda J, Benson AB, Rao S, Joehl RJ 2001 Indications and results of liver resection and hepatic chemoembolization for metastatic gastrointestinal neuroendocrine tumors. Sur-gery 130:677-682; discussion 682-675
Yarden Y 2001 The EGFR family and its ligands in human cancer. signalling mechanisms and therapeutic opportunities. Eur J Cancer 37 Suppl 4:S3-8
Zar N, Garmo H, Holmberg L, Rastad J, Hellman P 2004 Long-term survival of patients with small intestinal carcinoid tumors. World J Surg 28:1163-1168

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 216
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-7436
ACTAUNIVERSITATISUPSALIENSISUPPSALA2007