meningioma presenting as an intraoral mass
TRANSCRIPT

Volume 41 Number 6
Meningioma presentivlg as intraoral mass 771
3. Chaudhry, A. P., Vickers, R. A., and Gorlin, R. J.: Intraoral Minor Salivary Gland Tumors, ORAL SURF. 14: 1194-1226, 1961.
4. Rosenfeld, L., Sessions, D. G., I&Swain, B., and Graves, H.: Malignant Tumors of Salivary Gland Origin, 37 Year Review of 184 Cases, Ann. Surg. 163: 726-735, 1966.
5. Frable, W. J., and Elzay, R. P.: Tumors of Minor Salivary Glands, A Report of 73 Cases, Cancer 25: 932-941, 1970.
6. Leafstedt, 5. W., Gaeta, J. R., Sako, Ii., Marchetta, F., and She&l, D.: Adenoid Cystic Carcinoma of Major and Minor Salivary Glands, Am. J. Surg. 122: 756-762,197l.
7. Berdal P., de Besche, A., and Mylius, E.: Cylindroma of the Salivary Glands, A Report of 80 eases, Acta Otolaryngol. 263: 170-173, 1970.
8. Moertel, C. G., and Velag, S.: A Case for Multicentricity of Origin of Malignant Neoplasms, ed. 1, New York, 1966, Springer Verlag, pp. 104-108.
9. Christ, T. F., and Cracker, D.: Basal Cell Adenoma of Minor Salivary Gland Origin, Cancer 30: 214-219, 1972.
10. Evans, R. W., and Cruickshank, A. H.: Epithelial Tumors of the Salivary Glands, ed. 1, Philadelphia 1970, W. B. Saunders Company, pp. 58-76, 142-165.
Il. Batsakis, J. G.: Tumors of the Head and Neck, ed. 1, Baltimore, 1974, Williams & Wilkins Company, pp. 25-26.
Reprint requests to: Dr. B. N. Appel Department of Pathology School of Dental Medicine University of Pittsburgh Pittsburgh, Pa. 15261
Meningioma presenting as an intraoral mass
Ashley M. Brown, D.D.S., M&x, Kenneth C. Pordham, D.D.S., and Edward T. Lally, D.D.S., Philadelphia, Pa.
UNIVERSITY OF PENNSYLVANIA SCHOOL OF DENTAL MEDICINE
The following case report illustrates a rather rare oral lesion, an extracranial meningioma. In the dental office the lesion was seen on a periapical x-ray film as a multilocular radiolucency. The patient, however, could not be convinced of the necessity of biopsy until several years later when clinical expansion of the maxillary buccal pIate was noted. Thereafter, clinical, radiographic, and histopathologic examination revealed a diffuse meningioma involving the maxillary sinus, the floor of the nose, and the maxillary gingiva. The patient has since refused complete surgical removal but remains alive and well 8 years after the lesion was first noted.
I n 1947 New and Devine,5 in a comprehensive review of neurogenic tumors of the nose and throat, reported only one meningioma, which occurred in a paranasal sinus (the frontal). Hill,4 in 1962, described a case arising in the maxillary sinus which presented as a palatal mass. In 1967 Suzuki and associate@ noted the extreme rarity of intraoral meningiomas and described a lesion which appeared to extend beneath the zygomatic arch to the maxillary gingiva from

772 Browx et (11. Oral Surg. Jnnr~, 1976
Pig. 1. Periapical roentgenograms, 1966. Note the multilocular soap-bubble radiolueencies which do not appear to be pulpal or periodontal in origin.
Fig. 1. Extensive lytic lesion aa seen in 1974. A lucency involving the cuspid, which was the site of the biopsy, is readily seen.
the pterygopalatine fossa. They distinctly noted the absence of osteolytic lesions of the maxilla in their patient. Wolff and Rankow8 reported on a parotid meningioma in 1971 and called attention to the rarity of this lesion in the soft tissues of the head and neck. Farr and co-workers3 found that in the total experience of Memorial Sloan Kettering from 1940 to 1970 only ten of 405 meningiomas presented in the paranasal sinuses and/or nasal cavity and none were reported in the oral cavity.
Therefore, we believe that the following case of a rare lesion, which first presented as a periapical radiolucency, is of importance to the general dental practitioner and specialist for diagnostic consideration and is worthy of report- ing.
Volume 41 Number 6
Meningioma presenting as intraoral mass 773
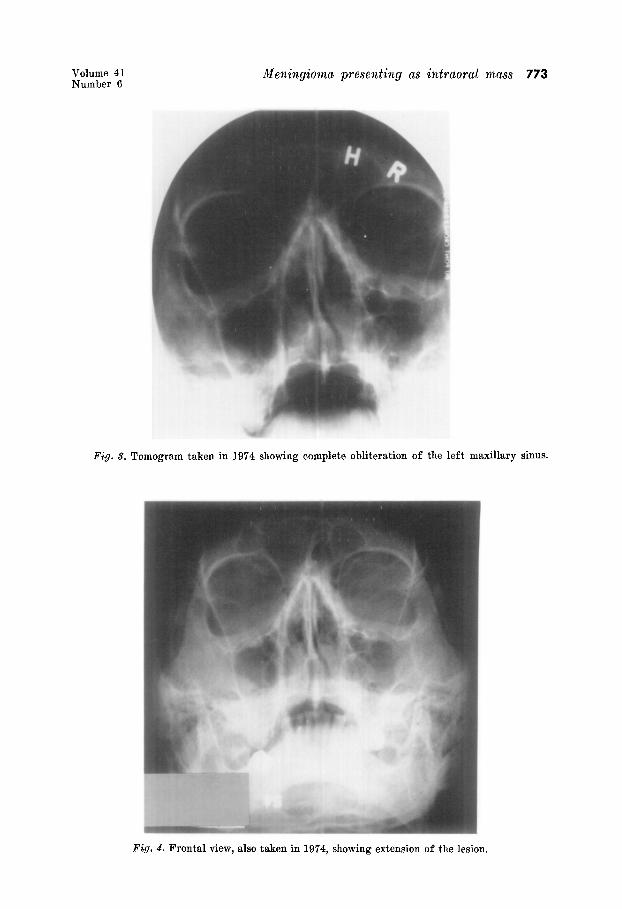
Fig. cc?. !I ‘omogram taken in 1974 showing complete obliteration of the left ma .xillai :Y sin lUS.
Fig. 4. Frontal view, also taken in 1974, showing extension of the lesion.

774 Brows et a,l. Oral Surg. June, 1976
Fig. 5. Histologic specimen showing the plump vesicular nuclei and swirling pattern characteristic of meningiomas. (Hematoxylin and eosin stain. Magnification, x140.)
Fig. 6. Histologic specimen showing nuclear pleomorphism and hyperchromatism. (Hema- toxylin and eosin stain. Magnification, x350.)
CASE REPORT The patient, a 69-year-old Caucasian man, first visited a periodontist in 1966, at which
time a peculiar soap-bubble type of radiolucency (Fig. 1) was noted in the area of the upper anterior teeth. The patient was advised to have the teeth treated and the lesions biopsied, but he refused, desiring only maintenance of the existing condition. Follow-up in 1968 revealed little or no change in the x-ray picture. A new lytic lesion of the left cuspid (not shown) was noted and again called to the patient’s attention.
In 1971, a Panorex film (not shown) failed to reveal any remarkable progression of these lesions. However, in May, 1974, the patient consented to have the anterior teeth removed and the “cystlike” lesion of the maxillary left cuspid area (Fig. 2) extirpated for diagnostic purposes. At surgery the lesion was noted to be poorly defined and was not completely removed. A diagnosis of an atypical neural lesion 1,s was made, and the specimen was sent to

Volume 41 Number 6
Meningionza presenting as intraoral mass 775
Fig. 7. Histologic specimen showing the focal hyalinization characteristic of meningiomas. (Hematoxylin and eosin stain. Magnification, x220.)
Fig. 8. Histologic specimen showing the characteristic swirling of the reticulin fibers in meningiomas. (Retieulin stain. Magnification, x220.)
Dr. L. Rorke of Philadelphia Ueneral Hospital for a neuropathologic consultation. The diagnosis was returned as “extracranial meningioma” and was subsequently confirmed by the Neuropathology Service of the Hospital of the University of Pennsylvania. The patient was then referred to the Otorhinolaryngology Service at the Hospital of the University of Pennsylvania, whereupon x-ray examination disclosed a diffuse lytic lesion of the left maxillary sinus (Figs. 3 and 4) which did not appear to involve the orbit. Physical examina- tion revealed no involvement of the tympanic membrane, orbit, or retropharyngeal structures. However, extension of the tumor mass to the floor of the nose was noted at this time. Other systems were negative. The patient refused further treatment at the University Hospital and referred himself to the American Oncologic Hospital in Fox Chase, Pennsylvania. A Caldwell-Luc procedure was performed at the American Oncologic Hospital, and a hard, tumorlike mass was found in the antrum. Curettage was performed, but again the patient

776 Brow?& et cxl. Oral Surg. .runc, 197(i
refused definitive therapy and has been followed on an outpatient basis by his local physician and dentist. He is alive and well 18 months after the definitive diagnosis of m(ningioma was made.
Pathology report
dficrosoopic description. The tumor is composed of varying-sized whorls of (ells wit11 fibers which are separated by sheets of plump-looking nuclei or fibrocollagenous stroma. Tim whorls resemble arachnoidal villi, and P.T.A.H.-positive fibers are found in many of them. Some portions of the tumor are extensively hyalinized, and the whorls in these places showed a striking lamellated pattern. Slight nuclear pleomorphism and hyperchromatism are noted, but mitotic figures are absent.
Diagnosis: Extracranial meningioma. Dr. Rorke added the following note to her report: “These are benign, slowly growing
tumors and do not require emergency therapy. I would recommend that consultation be obtained with an ENT specialist and neurosurgeon to plan the course of action.”
DISCUSSION
Extracranal meningiomas have been theorized to arise from ectopic embryonal sets of meningeal tissue which may have become heterotopic through developmental error or trauma.l It is alternatively possible that this meningioma arose from neural sheath cells along the course of the facial nerve.O Another important consideration is the possibility that the tumor was actually an extension of a cranial mass2 However, because of the patient’s reluctance to undergo definitive and complete removal, the issue cannot be completely resolved in this case. It is of interest to note that, despite the considered advice of the patient’s periodontist and medical therapists, he has consistently refused definitive therapy and has remained alive and well for 8 years.
REFERENCES
1.
2.
3.
2
6.
7.
8.
9.
Anderson, W. A. D. (editor) : Pathology, ed. 4, St. Louis, 1961, The C. V. Mosby Company, pp. 1327-1330. Ash, J. E., Beck, M. R., and Wilkes, J. D.: Tumors of the Upper Respiratory Tract and Ear, Atlas of Tumor Pathology, Washington, D.C., 1964, Armed Forces Institute of Path- ology, vol. 12, pp. 94-96. Farr, H. W., Gray, 0. F., Vrana, M., and Panio, M.: Extracranial Meningiomas, J. Surg. Oncol. 5: 411-420, 1973. Hill, C. I.: Meningioma of the Maxillary Sinus, Arch. Otolaryngol. 76: 547-549, 1962. New, G. B., and Devine, K. D.: Neurogenic Tumors of Nose and Throat, Arch. Otolaryngol. 46: 163-179. 1947. Pendergrass, E. P., and Hope, J. W.: An Extracranial Meningioma With No Apparent Intracranial Source, Am. J. Roentgenol. 70: 967-970, 1953. Suzuki, H., Gilbert, E. F., and Zimmerman, G.: Primary Extracranial Meningioma, Arch. Pathol. 84: 202-206, 1967. Wolff, M., and Bankow, R. R.: Meningioma of the Parotid Gland: An Insight Into the Pathogenesis of Extracranial Meningiomas, Hum. Pathol. 2: 453-459, 1971. Zachariae, L.: A Case of Extracranial Primary Meningioma, Acta Pathol. Microbial. Stand. 31: 58.60, 1952.
Reprint requests to: Dr. Ashley M. Brown National Cancer Institute Building 37, Room lB14 National Institutes of Health Bethesda, Md. 20014