medicine release mechanisms in artificial organs of science radboud honours academy year: 2013-2014...
TRANSCRIPT
Faculty of Science Radboud Honours Academy
Year: 2013-2014
Date: 15-5-2014
Medicine release mechanisms in
artificial organs
Applied to the administration of insulin
Roel Maas
Eline Meijer
Roel Oldenkamp
Jelle Piepenbrock
Lonneke Slenders

1
Preface This report is the product of five students' work enrolled in the first-year Radboud Honours Academy of the
Science Faculty of the Radboud University Nijmegen. The Radboud Honours Academy is a programme of
excellence for 2nd and 3rd year Science Bachelor students. In the first year of the Honours programme (2nd
year Bachelor), an interdisciplinary group of five students write a research proposal on a topic of their
choice.
Our group consists of two biologists, two molecular life scientists (MLS) and one chemist. Together we
chose the research subject regarding artificial organs. To be able to work out an applicable example we
focused on an artificial pancreas that delivers insulin to help people suffering from diabetes type 1. We
started this year with the idea of optimizing the growth of cells grown in hydrogels. After a short time it
became clear we were more interested in the encapsulation of the cells. This encapsulation ensures that
exogenous cells remain functional and serve as an artificial organ inside a human body. During a literature
study, we discovered that the controlled release of a pharmaceutical product from the artificial organ to the
human body still is a challenge.
We would like to thank a number of people who have helped us during our research project. First of all, we
would like to thank both Prof. Hagen Bayley and Dr. Khuloud Al Jamal and their research groups who we
visited during our trip to Oxford. They answered most of our questions and helped us to realize our research
proposal. Secondly, we would like to thank the Radboud Honours Academy for giving us the opportunity to
write our research proposal and organize the trip to Oxford. Finally we would like to thank our supervisor
Dr. Paul Kouwer, who assisted us during the whole process this year.
Figure 1: London, March 7
th 2014. From left to right: Eline Meijer (Chemistry), Roel Maas (MLS), Roel
Oldenkamp (Biology), Jelle Piepenbrock (MLS), Lonneke Slenders (Biology)

2
Contents Preface ............................................................................................................................................................... 1
Contents ............................................................................................................................................................ 2
1. Introduction ................................................................................................................................................... 3
1.1 Problem indication .................................................................................................................................. 3
1.2 Problem statement .................................................................................................................................. 3
1.3 Scope ....................................................................................................................................................... 4
1.4 Research question ................................................................................................................................... 5
1.5 Reading guide .......................................................................................................................................... 5
2. Artificial insulin release mechanisms ............................................................................................................ 6
2.1 Insulin production .................................................................................................................................... 6
2.2 Cell survival .............................................................................................................................................. 8
2.3 Controlled release mechanism ................................................................................................................ 8
2.3.1 Release mechanisms......................................................................................................................... 9
2.3.2 Sensors ............................................................................................................................................ 12
2.4 Conclusion ............................................................................................................................................. 13
3. Setup and materials – Our model release mechanism................................................................................ 14
3.1 Carbon nanotubes ................................................................................................................................. 14
3.1.1 Single-walled carbon nanotubes .................................................................................................... 15
3.1.2 Multi-walled carbon nanotubes ..................................................................................................... 16
3.2 Functionalization ................................................................................................................................... 17
3.2.1 Molecular valve ............................................................................................................................. 17
3.2.2 Glucose sensor ................................................................................................................................ 19
3.3 Polymer-membranes for encapsulating cells ........................................................................................ 20
3.4 Possible experimental approaches ........................................................................................................ 21
4. Implementation ........................................................................................................................................... 23
5. Conclusion ................................................................................................................................................... 25
6. References ................................................................................................................................................... 26
3
1. Introduction
1.1 Problem indication
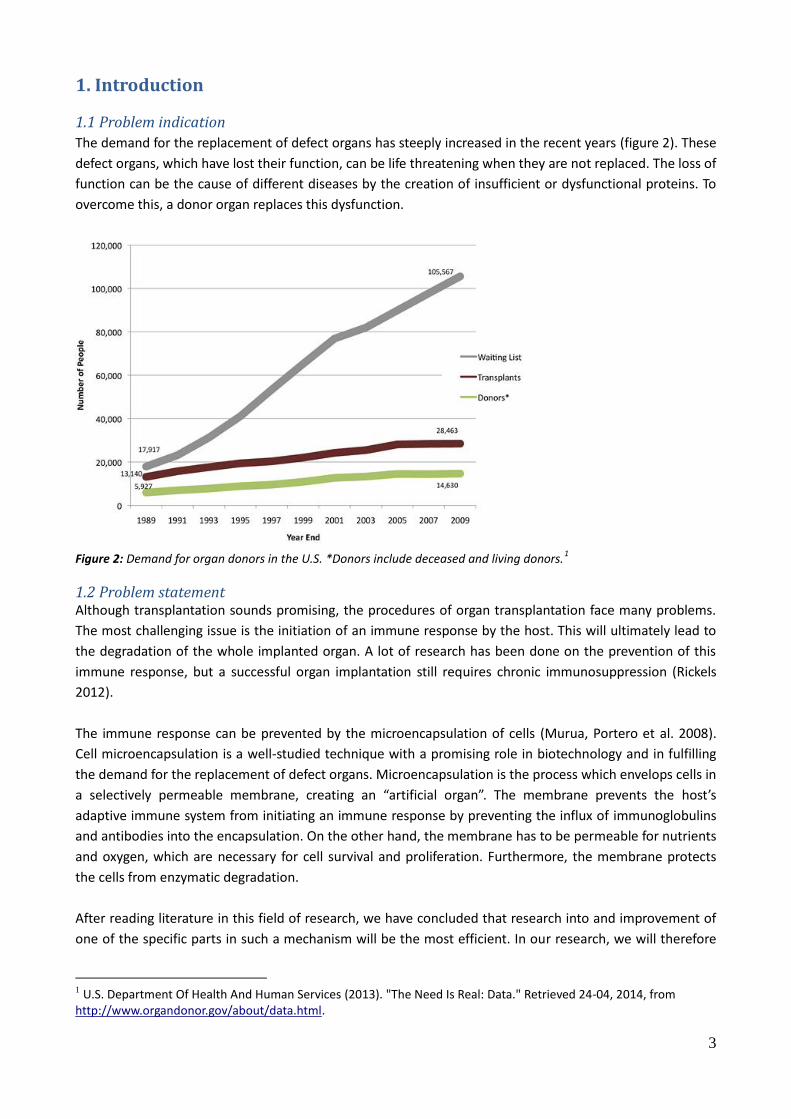
The demand for the replacement of defect organs has steeply increased in the recent years (figure 2). These
defect organs, which have lost their function, can be life threatening when they are not replaced. The loss of
function can be the cause of different diseases by the creation of insufficient or dysfunctional proteins. To
overcome this, a donor organ replaces this dysfunction.
Figure 2: Demand for organ donors in the U.S. *Donors include deceased and living donors.
1
1.2 Problem statement Although transplantation sounds promising, the procedures of organ transplantation face many problems.
The most challenging issue is the initiation of an immune response by the host. This will ultimately lead to
the degradation of the whole implanted organ. A lot of research has been done on the prevention of this
immune response, but a successful organ implantation still requires chronic immunosuppression (Rickels
2012).
The immune response can be prevented by the microencapsulation of cells (Murua, Portero et al. 2008).
Cell microencapsulation is a well-studied technique with a promising role in biotechnology and in fulfilling
the demand for the replacement of defect organs. Microencapsulation is the process which envelops cells in
a selectively permeable membrane, creating an “artificial organ”. The membrane prevents the host’s
adaptive immune system from initiating an immune response by preventing the influx of immunoglobulins
and antibodies into the encapsulation. On the other hand, the membrane has to be permeable for nutrients
and oxygen, which are necessary for cell survival and proliferation. Furthermore, the membrane protects
the cells from enzymatic degradation.
After reading literature in this field of research, we have concluded that research into and improvement of
one of the specific parts in such a mechanism will be the most efficient. In our research, we will therefore
1 U.S. Department Of Health And Human Services (2013). "The Need Is Real: Data." Retrieved 24-04, 2014, from
http://www.organdonor.gov/about/data.html.

4
focus upon what we have identified as the main bottleneck: a release mechanism to accompany functional
cell microencapsulation. This mechanism releases a pharmaceutical product proportional to a substrate
concentration, for instance insulin release, proportional to the glucose concentration. The goal of this
research proposal is to try to find a self-regulating release mechanism that mimics the release of insulin by a
human pancreas in reaction to a high glucose concentration.
Ideally such release mechanism should work according to a general mechanism or principle that can be
used for the treatment of different kinds of diseases, so that it can be used as a blueprint for the treatment
of many diseases. This will save costs, resources and time.
By using the principle of cells growing inside a gel by microencapsulation the general approach of creating
an artificial organ becomes also possible for combating those diseases that have a need of pharmaceutical
products usually produced inside the body itself with a failure somewhere in the production pathway.
1.3 Scope
Despite the desire to develop a general artificial organ, we will use the pancreas as a model system. The
pancreas is an organ that produces insulin that can regulate the glucose concentration in the blood.
Diabetes is a disease that occurs when the body cannot use glucose properly because of certain defects in
the polysaccharide regulation. Glucose is needed to provide humans of energy (Brill 2012).
Normally, the human body precisely regulates the glucose concentration in the body. Long-term
hyperglycaemia2, a too high blood glucose concentration, can for example give complications like loss of
vision, nephropathy leading to renal failure, sexual dysfunction, cardiovascular diseases or a coma
(Association 2008).
The regulation of the blood glucose concentration is performed by beta-cells in the pancreas. These cells
release the hormone insulin proportional to the glucose concentration in the blood. Insulin is needed to
absorb glucose from the blood into tissue cells through GLUT-4 proteins and decrease in this way the blood
glucose level (Sherwood, Klandorf et al. 2012). Therefore, it binds insulin receptors (IR) like the growth
factors IGF-1 or IGF II to stimulate the glucose absorption (Ward and Lawrence 2009).
There are two common types of defects in this system that can cause hyperglycaemia. Firstly, tissue cells
become insensitive to insulin, which in turn causes blood sugar levels to rise. This disorder is called diabetes
type 2. Secondly, diabetes can be the result of an autoimmune disease. When the immune system destroys
beta-cells in the pancreas, the body is not able anymore to produce enough insulin to decrease the blood
glucose level. This is referred to as diabetes type 1.
2 The World Health Organisation defined hyperglycemia as blood glucose levels greater than 7.0 mmol/L when fasting
or blood glucose levels greater than 11.0 mmol/L 2 hours after meals. (Diabetes UK. (2014). "Diabetes and Hyperglycemia." Retrieved 1-05, 2014, from http://www.diabetes.co.uk/Diabetes-and-Hyperglycaemia.html.)

5
The number of diabetes patients is increasing rapidly. The World Health Organization estimated that the
number of diabetes patients worldwide was about 220 million in 2004 and in that year about 3.4 million
people died as a consequence of this pathology (Lombarte, Lupo et al. 2013). About 10% of the total
number of diabetes patients suffers from diabetes type 1 (Brill 2012). Especially this type of diabetes can be
troublesome because of the multiple injections of insulin per day. Researchers are trying to find new insulin
therapies like insulin analogues that can change diabetic care, but in this case the patients still have to inject
themselves (DeWitt and Hirsch 2003).
It would be more comfortable if the damaged beta-cells of diabetes type 1 patients could be replaced by an
artificial pancreas. Many researchers propose such an artificial organ, but the perfect insulin producing
artificial organ has not been found yet.
1.4 Research question
The major challenge in artificial organ research is to create a properly functioning release mechanism. This
report proposes a new solution for the designing of an artificial organ using different existing compounds to
create a new kind of release mechanism. It is not the purpose of this proposal to create a whole new
artificial organ, but the focus will be on the release mechanism especially of insulin. In further research this
could lead to a solution for diabetes type I. We formulate our research question as follows:
In what way can a controlled insulin release mechanism be created, that can stay in the human body for
prolonged periods of time and release insulin proportional to the blood glucose level?
1.5 Reading guide
In the next chapters we are going to search for answers to our research question. In chapter two already
researched artificial insulin release mechanisms will be discussed. We anticipate that one of these will
represent the basis of an artificial pancreas. The production and release of insulin will be described. In
chapter three we are actually going to discuss a setup for our release mechanism that we expect to be the
most efficient. This consists of the mechanisms for cell survival and for the controlled release of insulin.
At the end of our proposal we are going to discuss what the impact of our potential research could be and
anticipate what kind of problems could eventually arise. From all this we will draw a conclusion about our
designed release mechanism.

6
2. Artificial insulin release mechanisms
The goal of this proposal is to produce a so-called long-term closed-loop insulin releasing artificial organ. A
closed-loop system means that production, sensing and excretion processes all happen in the same device,
avoiding the need for an external input of insulin. To make such an artificial organ function properly, three
different components are needed. The first component is responsible for the production of insulin. To
make this possible, we want to encapsulate insulin producing cells in a hydrogel. These cells could be
bacteria, mammalian cells or yeast cells (section 2.1). The second component is responsible for the survival
of the cell, providing a way to control the matrix in which cells can thrive and to control the influx and efflux
of nutrients and waste products. The latter function is important to let the cells grow so they can live,
differentiate and produce insulin on a long-term base. (section 2.2). The last component is the controlled
release mechanism, a way to release insulin at a concentration proportional to the glucose concentration
(section 2.3). This mechanism itself can be divided into two subcomponents. The first of these is the actual
mechanism of release, for which a few criteria need to be met. The second subcomponent is a sensor which
can measure the glucose concentration and produces a signal proportional to the glucose concentration.
This sensor is therefore responsible for the controlled release of insulin. Two different types of sensors will
be discussed, namely the enzymatic and electro catalytic (nonenzymatic) glucose sensors. In the search for
a sensor it is important that the sensor gives a signal which can be used by the release mechanism to
excrete insulin.
2.1 Insulin production
To create an artificial organ that can regulate the insulin levels in the body active insulin production is
required. This process needs to take place in the enclosed space encapsulated by a membrane that is to be
the outer layer of the artificial organ. Three cell types were taken into consideration: bacterial E. coli cells, S.
cerevisiae yeast cells and human beta cells. Another way of producing insulin is by the use of cell free
systems. These systems work without a cell nucleus and other cell organelles. The only compounds that are
present in the cell free systems are the biological products and proteins needed for the production of
insulin. In the initial phase of the release mechanism it is much easier to use a storage of insulin, for
instance insulin capsules. By taking away the insulin production the insulin efflux only depends on the
efficiency of the release mechanism. However doing so the closed-loop property of the artificial organ
disappears.
Beta cells
For an artificial organ solely devoted to releasing insulin, the beta cells are probably the best option, as their
natural function is to produce insulin and deliver it into the bloodstream. As the goal of our work is to
design release mechanisms beyond the artificial pancreas and applicable to other organs, we will first look
into the application of other insulin producing cells or methods. Therefore, an effort will be made to shun
reliance on the function of beta cells for the artificial organ principle to work.
7
The human beta cells have an innate capability to sense the glucose concentration in the bloodstream and
the need for insulin. If we rely on the sensing capabilities of these cells, the translation to other organs is
limited to organs containing cells with an analogous mechanism to the beta cells. A way to overcome the
difficulties that our model system brings, while still being able to create a valid proof of concept, would be
the usage of beta cells that show an over expression of the insulin gene. If these cells continually produce a
steady amount of insulin, as bacteria ideally would do, we would be able to test the sensing capabilities and
the release mechanism of the membrane, while working around the fact that insulin is hard for bacteria to
produce.
Bacteria and yeast
The above goal of our work demands a certain variability and versatility from the producer cells. Bacterial
cells are most suited for overcoming these hurdles, because of their relatively undemanding nutrient
requirements and their customizability through genetic manipulation. However, the inability of bacterial
cells to fold complex proteins correctly through oxidation continues to pose a difficulty. This, in combination
with the absence of glycolysation in bacterial cells, has in the past led to a bottleneck in the road to mass
production of bioactive insulin. The heterodimeric nature of insulin, along with the need for sulfide bond
formation during protein folding, causes a major hurdle for the use of bacteria (Leibiger, Leibiger et al.
2008). More recent discoveries however, changed this paradigm somewhat. In a review of the possibilities
for bacterial protein production, James R Swartz highlights some new techniques that could eventually lead
to bacteria being able to produce bioactive insulin (Swartz 2001). The specific procedure by which the
bacteria in the artificial organ will produce insulin is not the focus of this research proposal. For now, it is
enough to know that it is already possible or will be in the near future.
Yeast cells are in many ways easy to manipulate, like bacteria, but are more complex. However, in yeast
cells, the same problems arise as in bacterial cells.
Cell free systems
Apart from the three aforementioned cell types, another avenue of research could also be explored in a
later stage: the usage of cell free systems. These are enzyme systems that have been isolated out of cells
that can perform certain biotransformation reactions. As there is no need for the reaction to deliver any
energy to the metabolic system of a cell, these reactions tend to be very energy-efficient. A challenge for
any such systems in this particular application would be setting up a cell free system that can produce
insulin out of molecules available in the inside of the artificial organ, getting the cell free system to work
inside of the human body and procuring a long lasting stability for the system (Zhang 2010).
Insulin Capsules
The expectation is that one of these four options will become a reality in the not too distant future. If an in
vivo method of producing insulin is not available at the time of the testing of this release mechanism,
insulin capsules could be used. With capsules of insulin that slowly degrade over time, we could still
demonstrate the mechanism of release, without being reliant on other research. Insulin capsules have been
created initially for oral delivery. For example, capsules that disintegrate in a glucose containing medium
could be used to fill the internal cavity of the artificial organ with insulin molecules, after which the release
mechanism can be activated (De Geest, Jonas et al. 2006).

8
2.2 Cell survival
The cells producing insulin need to be able to produce it for a long period of time. Therefore it is necessary
to encapsulate them inside a membrane (Orive, Maria Hernández et al. 2004). This is especially important
to prevent the potential immune response that can occur. Inside the membrane the cells can then be grown
in a hydrogel. For the growth of cells, nutrients and oxygen are needed and also the insulin has to be able to
be excreted out of the encapsulation to create a good working artificial pancreas. This means that both the
hydrogel and the membrane need to be porous and permeable.
A hydrogel, which is used to let the cells grow in, consists of hydrophobic polymer strains that are held
together by crosslinkers (Kopeček 2002). This network of strains can take up a large amount of water, but
because of the hydrophobic strains it will not dissolve and a gel is formed. The disorder of these strains
yields a porous gel. These pores can change in size according to the different proportion of water uptake of
the gel (Hoffman 2002). The proportion of water uptake by the gel is affected by its crosslinkers and the
effect of the environment on these connecting elements. By controlling the water uptake of the gel, the size
of the pores can be controlled. When the pores are small they will be able to let through oxygen and
nutrients for the cells to produce insulin and survive. When the gel has taken up a larger amount of water
the pores will be bigger and insulin would be able to diffuse through the gel. With an optimized pore size in
the gel it should however not be possible for antibodies like the smallest IgG immunoglobulin to come near
the cells producing insulin.
Antibodies are also prevented from coming near the cells by the encapsulating membrane, which is also a
polymer hydrogel. This membrane has pores for letting through nutrients and insulin but those pores will be
too small for antibodies to pass. Although an immune response is induced by all cells and particles that are
foreign to the body it can also be induced by the membrane itself which needs to prevent this immune
response. Therefore the membrane surrounding the cells in the hydrogel needs to be made biocompatible
by for instance placing specific proteins on the surface.
2.3 Controlled release mechanism
To create an artificial pancreas a self-controlling release mechanism is an important part of the design. The
first step in a good working release mechanism is sensing the glucose concentration of the blood. The
glucose concentration must be measured to allow insulin release in a controlled manner and in substantial
quantities. The measurement of the glucose concentration needs to give a signal to which the release
mechanisms can react in a way the efflux of insulin is proportional to the measured concentration. A high
concentration of glucose has to induce a high dose of insulin being released into the bloodstream whereas
there should be (nearly) no insulin released at a low concentration of insulin. This means that the release of
insulin requires control over time and response times to changing concentrations should be sufficiently fast.
Furthermore it has to be considered that the insulin must be released several times. This means that a fast,
stable and reversible shut-off mechanism is needed. This self-controlling shut-off mechanism is especially
important because the people suffering from diabetes type 1 would not have to measure their glucose
concentration constantly and several times a day. We are thus searching for a release mechanism that
reacts to changes of the concentration of glucose within several seconds to a few minutes.

9
2.3.1 Release mechanisms
In the literature a number of release mechanisms have been proposed. In the next paragraphs, we will
introduce and review them based on the requirements defined in the previous paragraph.
Hydrogels
The first option for a release mechanism was found in the use of hydrogels as membranes. Hydrogels
consist of hydrophobic polymer strains that are held together by crosslinkers. Because the glucose
concentration is the changing factor of the environment, the hydrogel needs to respond to this change by
taking up more water, swelling, when the concentration increases. This can be done in several manners, of
which two will be explained. The first method is to use pH transduction. Enzymes oxidize glucose and
change the local pH, which, in turn, can open the pores in pH-responsive hydrogel membranes. The most
often used enzymes to change the pH of the environment are glucose oxidases (GOs). GO oxidizes glucose
to gluconic acid thereby changing the pH of the environment. This change in pH can ionize polymers to
polycations, resulting in a repulsive Coulombic force between the chains. The chains will be repulsed by
each other, the gel swells and the pores become bigger (Qiu and Park 2001).
The second method is by using so called sol-gel phase hydrogels. To make these reversible sol-gel phase
hydrogels, crosslinks that react on glucose are needed. One such a crosslink is concanavalin A. Concanavalin
A is a tetramer that binds glucose reversibly. To make a sol-gel phase hydrogel, glucose-containing polymer
chains with concanavalin A as crosslinker can be used. The concanavalin A crosslinkers bind four glucose
molecules of different chains resulting in a gel phase hydrogel. The glucose molecules bound to the chain
will always compete with free glucose molecules. If the free glucose concentration rises, more and more of
the concanavalin A crosslinkers will bind the free glucose molecules. Thereby releasing the glucose bound to
the chains and the hydrogel turns into the solution phase (Qiu and Park 2001).
Looking at the list of criteria we see that the hydrogels are capable of releasing the insulin proportional to
the glucose level. They also have an opening and closing mechanism. Unfortunately the hydrogels does not
meet the other two criteria. The swelling and shrinking of the hydrogel takes too long after a change in the
glucose concentration. Furthermore, after the gel swells and shrinks a few times it becomes less and less
stable. Resulting in a continually opened membrane, letting the insulin through all the time. So the
durability of the hydrogels is pretty low.
Electrostatic membranes
A second potential release mechanism works with a selectively permeable membrane. The selectivity of the
membrane can be regulated with electrostatic properties. This can be achieved by placing charged
molecules on the outside of the membrane. Because these molecules are equipped with acidic or amino
groups they can change their charge and so the charge of the whole membrane (figure 3). A negatively
charged molecule, like insulin, will remain within the encapsulation and it will be held there when the
surrounding membrane is also negatively charged. When changing the charge of the membrane from
negative to positive the negatively charged insulin molecules will leave through the membrane.
Changes in the pH can protonate or deprotonate the amino and acidic groups. This is why a change in the
pH of the environment can lead to a change in charge of the membrane. This release mechanism is capable
of opening and closing with a long durability and the charges change quickly. A potential disadvantage is
that he charged groups could also block other substances like nutrients needed for the host cells to survive.
Another disadvantage is that the pores of the membrane are always open so molecules dangerous for the

10
host cells are able to go through the membrane all the time, if they can pass the polymer strands (Li,
Harbron et al. 2013). Because of these disadvantages an electrostatic membrane does not look like a perfect
release mechanism that can be used in the body.
Figure 3: “Chemical construction of water-dispersible aqueous inorganic microcompartments with self-activated gated
membrane permeability. Scheme that illustrates the design and construction of functionalized colloidosomes prepared
by TMOS-induced crosslinking and covalent grafting of a branched copolymer corona on the semipermeable outer
surface of a closely packed shell of silica nanoparticles. pH-induced changes in the net charge associated with cationic
dimethylamino (blue) and anionic carboxylate (red) groups of the TMSPMA23/DMAEMA40/MAA37–EGDMA8–DDT10
copolymer layer generate a gated response to the transfer of charged small molecules across the inorganic membrane.
The structure of the branched copolymer is shown (top right)” picture and capture taken from Li et al.(Li, Harbron et al.
2013).
Nanometersize channels
The third release mechanism works with channels with diameters in the nanometer range incorporated
into a silicon membrane (figure 4). Because these channels are so small the interaction of insulin with the
side walls has more influence on the efflux of insulin than the concentration gradient. These interactions
with the channel walls result in a baseline insulin efflux, independent of the concentration gradient. For this
kind of system to work as release mechanism, one would also need an active insulin efflux. This active
efflux can be realised by placing a potential over the nanochannels. Charged molecules will move along
with the potential or will be blocked by the potential dependent on the surface charge. By controlling the
potential over the membrane the efflux can be ten times higher than the baseline efflux. The stability, and
so the durability, of this release mechanism is high, due to the strength of the silicon membrane. The
membrane itself has no controlled release mechanism. For a peak efflux of insulin a device regulating the
membrane potential is needed that creates an electron flow that changes direction when the potential
changes direction. To achieve this a pre-programmed system is needed which includes a power supply for
the potential and a glucose sensor. During a time of low blood glucose level the device creates a potential
blocking the insulin efflux, by ensuring an electron flow in the opposite direction of the insulin efflux. When
the glucose sensor measures a high glucose concentration, the pre-programmed system changes the
direction of the potential (and thus the electron flow) resulting in a high insulin efflux. This looks promising
but the power supply reduces the lifetime of the release mechanism because the power supply may need
to be replaced after a period of time. The applied potential mechanism therefore has the same problem as
with the electrostatic membrane. Depending on the charge, the potential blocks the influx of nutrients or
other compounds needed for the insulin producing cells to survive (Grattoni, Parazynski et al. 2011).

11
Figure 4: A silicon membrane which contains micro(M)- and nanochannels (N). The molecules move freely through the
microchannels but interact with the sidewalls of the nanochannels. The picture on the right shows how the molecules,
moving from the inside (A) to the outside (B), interact with the sidewalls of the nanochannels (Grattoni, Parazynski et
al. 2011).
Molecular valve
The fourth and last release mechanism works with a molecular valve. A molecular valve is a controllable
valve working on the molecular level. One such a molecular valve is the bistable [2]rotaxane (figure 5). A
bistable [2]rotaxane works as a door mechanism. A CPBQT4+ ring can shuttle between two different binding
sites on the bistable [2]rotaxane. This shuttling occurs by redox reactions of one of the two binding sites.
When the bistable [2]rotaxane is placed on the outside of a pore, than the ring can either block the opening
of the pore or open it by shuttling of the ring. The stability of the bistable [2]rotaxane seems to be pretty
good. It is strong enough to bend a golden plate several times. But the precise durability of the bistable
[2]rotaxane is still not clear. For the controlled release of insulin a sensor with an electrical current as
output is needed. This electrical current can be used for the redox reactions for the shuttling of the ring. So
when this molecular valve can be successfully coupled to a sensor a good working release mechanism can
be made which meets all the considerations (Fahrenbach, Warren et al. 2013).
Figure 5: Bistable [2]rotaxanes placed on the outside of the pores in a mesoporous silica nanoparticle. When the
CPBQT4+
shuttles to the distant position from the membrane the pore opens and the trapped molecules come free
(Nguyen, Liu et al. 2007).
12
2.3.2 Sensors
The second important part of the release mechanism is the sensor. There are two general types of sensors
to measure the glucose concentration. These are enzymatic and nonenzymatic (electro catalytic) glucose
sensors which will both be discussed in the following.
Enzymatic sensors
The enzymatic sensors are widely used because of the high sensitivity and selectivity with a low detection
limit for glucose (Wang, Zhang et al. 2003). Furthermore, these sensors do not induce an immune response.
The enzyme used is glucose oxidase (Jiang, Yu et al. 2013) which catalyzes the oxidation of glucose to
gluconolactone (Ye, Wen et al. 2004). The reaction hereby taking place is the following (Guiseppi-Elie, Lei et
al. 2002):
glucose + O2 → gluconolacetone + H2O2
Some examples of enzymatic sensors are the pH-sensitivity of membranes or enzymes like concanavalin A
which binds insulin and oxidized-glucose competitively (Qiu and Park 2001). These membranes would
require some extra groups or certain compositions of hydrogels to have the sensor build inside the
membrane.
The disadvantages of these sensors are though that they usually respond very slowly. The gel or membrane
around the cells cannot stay in the same stable conformation for a long time because the strength will
change and degrade after some time of use. In addition to the stability of the membrane the stability of the
enzyme causes problems, too. The stability of the sensor causes inevitable drawbacks. The chemical and
thermal instabilities derive from the nature of enzymes (Jiang, Yu et al. 2013).
Nonenzymatic sensors
Nonenzymatic sensors are nowadays used to measure glucose concentrations for continuous glucose
monitoring. The oxidization of glucose takes place on expensive noble metal electrodes, like gold or
platinum. These metals are necessary, because the sensors are based on direct electro catalytic oxidization,
which produces free electrons. Therefore, a current proportional to the glucose concentration is created
which can be used as a signal (Jiang, Yu et al. 2013).
Nonenzymatic sensors have both advantages as disadvantages. Advantages like simplicity and good stability
are of great importance for this research proposal. However, the sensors have a low sensitivity and
selectivity towards glucose because of surface poisoning due to electroactive interfering species in the
blood. For instance, chloride ions (Ye, Wen et al. 2004), 4-acentamidophenol, asorbic acid (AA) and uric acid
(UA) reduce both the selectivity and sensitivity (Cui, Ye et al. 2007). The level of reduction is dependent on
the noble metal electrodes.
Nonetheless, in combination with carbon nanotubes, which possess a high surface area and good
mechanical properties like stability and conductivity (Jiang, Yu et al. 2013), these nonenzymatic sensors
appeared to be promising for the glucose detection. Furthermore carbon nanotubes also have extremely
high mechanical strength (Ye, Wen et al. 2004). Because of the better stability and the coupling with carbon
nanotubes we thus decided to use a nonenzymatic glucose sensor.

13
2.4 Conclusion
This chapter has described different ideas and mechanisms regarding artificial organs. It has become clear
that many ways of insulin production inside the cavity are possible. Insulin production by bacteria or yeast
cells are most favourable, because of their relatively undemanding nutrient requirements and their
customizability through genetic manipulation. Besides, some controlled release mechanisms are discussed,
with a focus on membranes and sensors. This research proposal will look further into molecular valves,
coupled to a nonenzymatic sensor which oxidizes glucose, because this setup meets our requirements.
Firstly, the valve will open and close the pore proportional to the glucose concentration because of the
glucose sensor. Secondly, this setup creates a shut-off mechanism, which is necessary for terminating the
insulin efflux when the blood glucose level has been sufficiently lowered. Thirdly, the molecular valve is
quite stable and the opening and closing occurs quite fast.
14
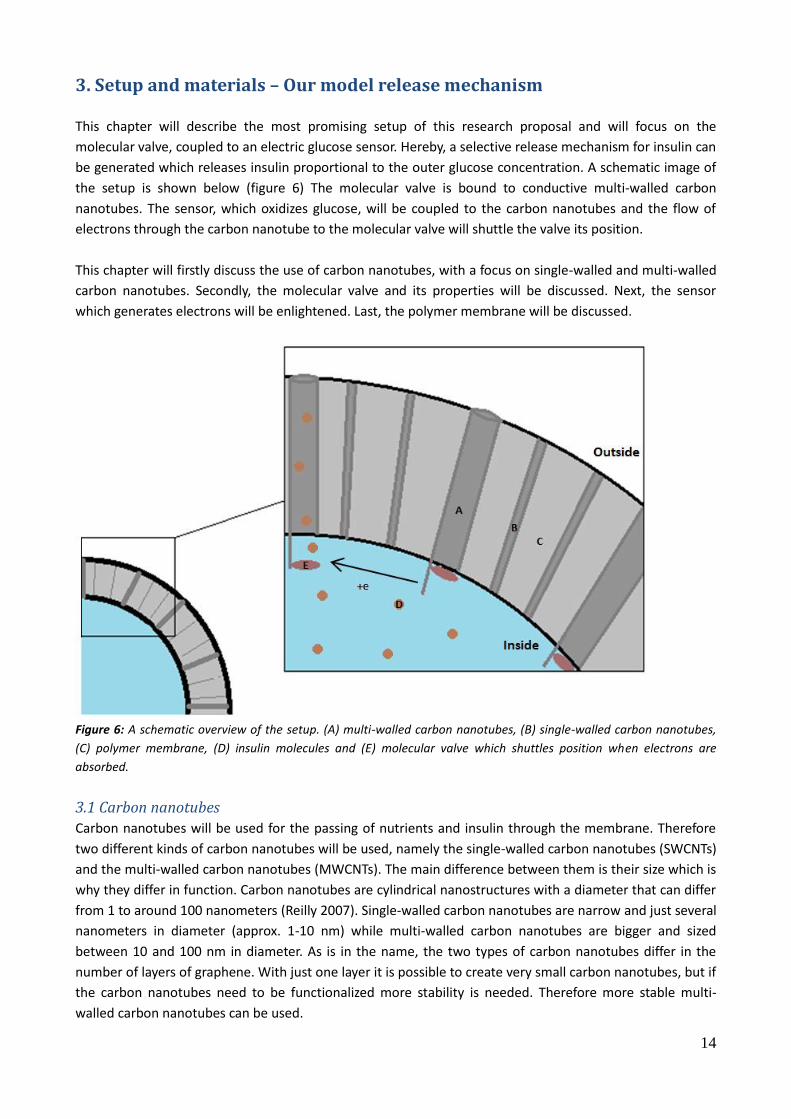
3. Setup and materials – Our model release mechanism This chapter will describe the most promising setup of this research proposal and will focus on the
molecular valve, coupled to an electric glucose sensor. Hereby, a selective release mechanism for insulin can
be generated which releases insulin proportional to the outer glucose concentration. A schematic image of
the setup is shown below (figure 6) The molecular valve is bound to conductive multi-walled carbon
nanotubes. The sensor, which oxidizes glucose, will be coupled to the carbon nanotubes and the flow of
electrons through the carbon nanotube to the molecular valve will shuttle the valve its position.
This chapter will firstly discuss the use of carbon nanotubes, with a focus on single-walled and multi-walled
carbon nanotubes. Secondly, the molecular valve and its properties will be discussed. Next, the sensor
which generates electrons will be enlightened. Last, the polymer membrane will be discussed.
Figure 6: A schematic overview of the setup. (A) multi-walled carbon nanotubes, (B) single-walled carbon nanotubes,
(C) polymer membrane, (D) insulin molecules and (E) molecular valve which shuttles position when electrons are
absorbed.
3.1 Carbon nanotubes
Carbon nanotubes will be used for the passing of nutrients and insulin through the membrane. Therefore
two different kinds of carbon nanotubes will be used, namely the single-walled carbon nanotubes (SWCNTs)
and the multi-walled carbon nanotubes (MWCNTs). The main difference between them is their size which is
why they differ in function. Carbon nanotubes are cylindrical nanostructures with a diameter that can differ
from 1 to around 100 nanometers (Reilly 2007). Single-walled carbon nanotubes are narrow and just several
nanometers in diameter (approx. 1-10 nm) while multi-walled carbon nanotubes are bigger and sized
between 10 and 100 nm in diameter. As is in the name, the two types of carbon nanotubes differ in the
number of layers of graphene. With just one layer it is possible to create very small carbon nanotubes, but if
the carbon nanotubes need to be functionalized more stability is needed. Therefore more stable multi-
walled carbon nanotubes can be used.

15
Small molecules like nutrients and oxygen will be transported through the small single-walled carbon
nanotubes. Furthermore multi-walled carbon nanotubes will be used for the release of insulin after
functionalization, which all will be discussed in the following paragraphs.
3.1.1 Single-walled carbon nanotubes
The single-walled carbon nanotubes (SWCNTs) will be used for providing the insulin producing cells inside
the polymer membrane with enough nutrients and oxygen. Therefore the characteristics and synthesis of
SWCNTs will be discussed in this paragraph.
Characteristics of single-walled carbon nanotubes
Single-walled carbon nanotubes have a very small diameter in nanometer scale, while the length of the
carbon nanotubes is several micrometers (Reilly 2007). Those tubes are made of hexagons of carbon atoms
bound together, forming a honeycomb structure (figure 7).
Because of the nanometre scale, large molecules cannot pass the tube
and reach the cells inside the membrane. More specifically, the smallest
immunoglobin IgG (150 KDa) with a diameter of approximately 15 nm
cannot diffuse through the SWCNT (Randall, Kalinin et al. 2011). On the
other hand, smaller molecules like glucose, oxygen and small proteins
will be able to diffuse through the tubes, maintaining the living cells.
The pharmaceutical product insulin, with a diameter of approximately 5
nm and height of approximately 3.5 nm (Brange, Owens et al. 1990), will
not pass the SWCNT.
Synthesis of single-walled carbon nanotubes
There are different ways of SWCNTs synthesises. Firstly, SWCNT
synthesis, compared to MWCNT synthesis, is harder because SWCNTs
are more fragile. Secondly, there is a difference in the deposition of
carbon nanotubes in the polymer membranes. Carbon nanotubes can be
randomly orientated or vertically aligned (figure 8) (Ahn, Baek et al.
2012). The SWCNTs in vertically aligned membranes are all
perpendicular to the membrane,
whereas SWCNTs in randomly
orientated membranes are not. In
this research proposal the single-walled carbon nanotubes will initially
be randomly orientated, because it is much easier to synthesize than
vertically aligned SWCNTs. Besides it is not necessary that all the
SWCNTs face the in- or outside, because enough molecules will diffuse
through SWCNTs if the concentration of carbon nanotubes is high
enough. In a later stage the single-walled carbon nanotubes can still be
synthesized in a vertically aligned manner as a prospect of higher
efficiency.
Figure 7: Conceptual diagram of a single-walled carbon nanotube with typical dimensions of length and width. (Raymond M. Reilly, 2007)
Figure 8: Conceptual diagram of CNT membranes. (a) Vertically aligned CNT membrane and (b) randomly orientated CNT membrane (Ahn, Baek et al. 2012).

16
The production of the SWCNTs is explained by Takagi et al. in 2006 (Takagi, Homma et al. 2006) . Metal
catalysts are used at high temperatures for the molecular self-assembly. The size of these catalyst particles
determine the diameter of the tubes which is why they can be varied. Chang et al. showed in 2013 that it is
also possible to covalently bind the SWCNTs to the polymer matrix present in the membrane (Chang, Jeon
et al. 2013). Therefore the exterior of the nanotubes needs to be modified. This covalently binding will
increase the lifetime of the carbon nanotube membrane and lower the toxicity, because the tubes will not
dissolve from the membrane into the human body.
3.1.2 Multi-walled carbon nanotubes
Next to the single-walled carbon nanotubes (SWCNTs) multi-walled carbon nanotubes (MWCNTs) will be
placed into the membrane. These multi-walled carbon nanotubes, which consist of concentrically organized
cylindrically formed graphene sheets, will be the portal through which insulin will flow out of the artificial
organ.
During the last few years, much research has focused on the functionalization of multi-walled carbon
nanotubes. For our purposes, the multi-walled carbon nanotubes need to be able to:
conduct the electrical current from the sensor molecules to the gate molecule.
be covalently bound to a sensor material, which can create an electrical current.
be covalently bound to a gate molecule, which can respond to the aforementioned current.
be covalently bound to the membrane polymers if needed.
be large enough to transport insulin but small enough to exclude any larger compounds.
The first property should be relatively easy to accomplish, as carbon nanotubes are highly conductive. The
exact properties of the nanotubes can also be tuned to produce the exact amount of conductivity needed to
activate all components (Bandaru 2007). The other requirements all have to be realized through
functionalization of both tips and the sidewalls of the carbon nanotubes. A consideration however is that
the conductivity of the nanotube could be reduced or hindered by the functionalization of the outer walls.
As insulin has a globular size of around 5 nanometers, the diameter of the multi-walled carbon nanotube
should be slightly larger. It should be less than 15 nm in diameter, though, to prevent immunoglobulins from
entering the artificial pancreas. With a simple side-by-side comparison of insulin diffusion rates, an optimal
inner carbon nanotube radius could be found. Multi-walled carbon nanotubes with a 4 nm to a 80 nm inner
diameter are commercially available. Producing or gaining access to nanotubes with a correct size for insulin
transport seems likely.3,4
3 Sigma-aldrich (2014). "Properties and Applications of Single-, Double- and Multi-Walled Carbon Nanotubes."
Retrieved 16-04, 2014, from http://www.sigmaaldrich.com/technical-documents/articles/materials-science/single-double-multi-walled-carbon-nanotubes.html]. 4 Cheap Tubes Inc (2014). "COOH Functionalized Nanotubes-COOH CNTs." Retrieved 16-04, 2014, from
http://www.cheaptubesinc.com/coohfunctionalizedcnts.htm#COOH_Functionalized_Nanotubes_8nm_Specifications.

17
3.2 Functionalization
This paragraph will handle the functionalization of the multi-walled carbon nanotubes with the molecular
valve and the glucose sensor. Both molecular valve and sensor will separately be discussed.
To determine what kind of functionalization we have to consider, we have to know what kind of gate
molecule we are planning to use (section 3.2.1). For the gate molecule, we are looking into the possibility of
using a bistable [2]rotaxane as a redox-sensitive mechanism which can be opened and closed. The tip of the
carbon nanotube on the inner side of the artificial organ can be functionalized through several different
kinds of reactions, namely 1,3-dipolar cycloaddition, reactions with nitrenes, radicals and carbenes, or
through a Birch reduction (Kuzmany, Kukovecz et al. 2004), (Georgakilas, Kordatos et al. 2002). It should be
possible to place the chosen gate molecules on the tip of the nanotubes with one of these reaction
methods.
Also a sensor needs to be chosen (section 3.2.2). As the most compatible sensors seems to be
nonenzymatic sensors we will consider these. It should be possible to coat a part of the nanotubes with a
metaloxide, which will produce a redox reaction when coming in contact with glucose, thus supplying
electrons which can be used to produce a releasing response. Something comparable has been done by Sun
et al. (Sun, Zhang et al. 2007). This coating should preferably only be on the side of the nanotube that is in
contact with the bloodstream or the tissue fluids.
3.2.1 Molecular valve
A bistable [2]rotaxane (figure 9) consists of two π-electron rich groups, most
frequently 1,5-dioxynaphthalene (DNP) and tetrathiafulvalene (TTF). Next to it, it
contains an electron-deficient cyclobis (paraquat-p-phenylene) (CBPQT4+) ring. The
CBPQT4+ ring prefers a binding for TTF, because the ring has a 1.4 kcal mol-1 better
binding affinity with TTF then with DNP. When TTF is oxidized to the radicals TTF+
or TTF2+, the ring switches to the DNP group due to the Coulombic repulsion
between the oxidized TTF with the CBPQT4+ ring. After reducing TTF2+ the ring
slowly moves back to the TTF group (Dey, Coskun et al. 2011).
The shuttling of the ring between the two π-electron rich groups makes it possible
to open or close multi-walled carbon nanotubes. The opening/closing of the pore
will be the result of reduction/oxidation of the TTF group.
Placing the rotaxanes on CNT’s
The bistable [2]rotaxane has to be placed on the tip of the carbon nanotubes to
manage the efflux of insulin. The carbon nanotubes we want to close have a
diameter of ±10 nm. Nguyen et al. used bistable rotaxanes as valves working on
pores of mesoporous silica nanoparticles, in which one bistable [2]rotaxane
completely closed 3 nm diametric pores (Nguyen, Liu et al. 2007). The closure of 10
nm diametric pores thus needs multiple bistable [2]rotoxanes.
Figure 9: Bistable [2]rotaxane consisting of a DNP group (red), a TTF group (green) and a CBPQT
4+ ring (blue).
18
It is very important that the bistable [2]rotaxanes are scattered around the opening of the pores.
Interactions between bistable [2]rotaxanes can result in blocking or slowing down the opening and closing
process. To ensure that the bistable [2]rotaxanes are scattered around the opening of the pore, the best
reaction conditions must be elected. The best conditions have to ensure that the bistable [2]rotaxanes only
bind to most energetically favourable positions. Due to the Coulombic repulsive force of the CPBQT4+ ring
these positions will be distant from the already placed bistable [2]rotaxanes, so the negative interactions
will be reduced.
Another way to close pores that are larger than 3 nm is by magnifying the ring. This can be done by placing
side groups on the CPBQT4+ ring. The effects of the magnification of the ring on the shuttling rate needs to
be investigated, though.
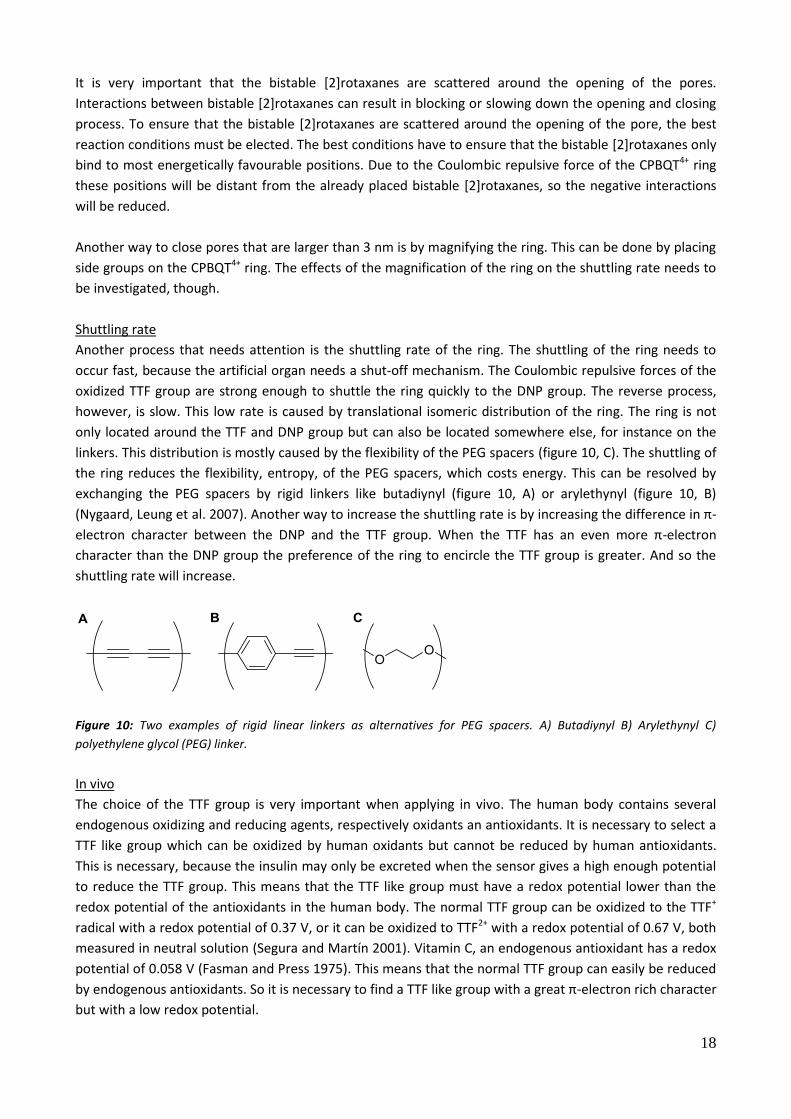
Shuttling rate
Another process that needs attention is the shuttling rate of the ring. The shuttling of the ring needs to
occur fast, because the artificial organ needs a shut-off mechanism. The Coulombic repulsive forces of the
oxidized TTF group are strong enough to shuttle the ring quickly to the DNP group. The reverse process,
however, is slow. This low rate is caused by translational isomeric distribution of the ring. The ring is not
only located around the TTF and DNP group but can also be located somewhere else, for instance on the
linkers. This distribution is mostly caused by the flexibility of the PEG spacers (figure 10, C). The shuttling of
the ring reduces the flexibility, entropy, of the PEG spacers, which costs energy. This can be resolved by
exchanging the PEG spacers by rigid linkers like butadiynyl (figure 10, A) or arylethynyl (figure 10, B)
(Nygaard, Leung et al. 2007). Another way to increase the shuttling rate is by increasing the difference in π-
electron character between the DNP and the TTF group. When the TTF has an even more π-electron
character than the DNP group the preference of the ring to encircle the TTF group is greater. And so the
shuttling rate will increase.
Figure 10: Two examples of rigid linear linkers as alternatives for PEG spacers. A) Butadiynyl B) Arylethynyl C)
polyethylene glycol (PEG) linker.
In vivo
The choice of the TTF group is very important when applying in vivo. The human body contains several
endogenous oxidizing and reducing agents, respectively oxidants an antioxidants. It is necessary to select a
TTF like group which can be oxidized by human oxidants but cannot be reduced by human antioxidants.
This is necessary, because the insulin may only be excreted when the sensor gives a high enough potential
to reduce the TTF group. This means that the TTF like group must have a redox potential lower than the
redox potential of the antioxidants in the human body. The normal TTF group can be oxidized to the TTF+
radical with a redox potential of 0.37 V, or it can be oxidized to TTF2+ with a redox potential of 0.67 V, both
measured in neutral solution (Segura and Martín 2001). Vitamin C, an endogenous antioxidant has a redox
potential of 0.058 V (Fasman and Press 1975). This means that the normal TTF group can easily be reduced
by endogenous antioxidants. So it is necessary to find a TTF like group with a great π-electron rich character
but with a low redox potential.

19
3.2.2 Glucose sensor
To reduce the TTF molecule of the molecular valve proportional to the glucose concentration, the
nonenzymetic glucose sensor will be coupled to the other end of the carbon nanotube than the molecular
valve. The electrons which are formed by the oxidization of glucose can be transferred to the TTF molecule
over the carbon nanotubes, because of their high electrical conductivity (Guiseppi-Elie, Lei et al. 2002).
The sensors will work as redox electrodes, rather than current measuring device when being coupled to
carbon nanotubes. As sensors they work with an applied potential, which is needed if a current is to be
measured. In this research proposal, the produced current is not essential to know, because it only has to
act as a redox electrode to reduce the molecular valve. Only the concentration to which the sensor reacts
has to be on the same order of magnitude as the glucose levels in the blood. The 'fine-tuning' can still be
done later by placing several different barriers in the multi-walled carbon nanotubes so that the insulin can
be released proportionally to the glucose concentration.
Nickelhydroxide sensor
This sensor is based on a nickelhydroxide layer on a polymide/CNT membrane. Nickelhydroxide is a good
glucose electrocatalyst and synthesized as a nanosphere on the polymide/CNT membrane, with the growth
mechanism shown in figure 11, performes well as a glucose sensor.
Growing Ni(OH)2 on the CNT membrane takes place by the electrochemical reduction of NO3- which
produces OH- in aqueous solutions. Nickelhydroxide is then formed by combining OH- with Ni2+. The
generation of hydroxide ions controls the crystal growth of Ni(OH)2 in the reaction system.
Figure 11: Proposed growth mechanism for the nanostructures of Ni(OH)2 (Jiang, Yu et al. 2013).
By oxidizing glucose, the reaction for the formation of nickelhydroxide is the following:
Ni(OH)2 + OH- → NiO(OH) + H2O + e-
NiO(OH) + glucose → Ni(OH)2 + glucolactone
The glucose concentration is thus mainly measured in basic solutions, as OH- ions are needed. Still the
measurement takes place by oxidizing glucose by the active Pl/CNT- Ni(OH)2 nanospheres. The reaction is
catalyzed by the Ni3+/Ni2+ species on the film surface. By the diffusion of glucose to the film surface it is
rapidly oxidized to glucolacetone by the Ni3+. This is a typical mediated catalytic oxidation.
The sensor acts rapidly, 95% of the steady state current is reached within 5 seconds. The current shows an
extended linear range from 1.0 µM to 0.8 mM with a very low detection limit and a high sensitivity. The
glucose concentration in blood though varies from 4 to 8 mM – the measurement here still has to be

20
investigated. The sensor is in fact highly reproducible which is also an important factor. Also the selectivity
for glucose has been tested by adding other interfering substances. These show negligible responses for the
glucose concentration so the sensor is considered to be selective.
Jiang et al. conclude from their results that the glucose sensor has potential applications for the analysis of
glucose in real biological samples because the sensor performs well for the detection of glucose in human
blood serum samples. The samples still have to be made basic, though, so there still has to be done some
research.
The sensor exhibits a high sensitivity and a long-term stability. In addition to this it is also easily
reproducible and performs not yet optimal for the detection of glucose in human blood serums but it is
possible (Jiang, Yu et al. 2013).
Platinum-lead sensor
Another sensor, researched by Cui et al., is created by the electrodeposition of platinum and lead to a multi-
walled carbon nanotube. The resulting nanocomposite was stable with high electrocatalytic activity to
glucose oxidation. After a slight modification the sensor was made highly sensitive and selective with a low
detection limit in amperometric glucose sensing. The sensor exhibits linearity up to 11 mM of glucose and
thus it would be able to measure glucose concentrations in human blood. The electroactive species like
ascorbic acid, uric acid and fructose invoked the current response for 9 to 23%. The sensor is stable and
reproducible but it also can be toxic because of the lead being placed into the body. Therefore this sensor is
considered as an option if the toxicity can be controlled in any way, for it shows good responses concerning
the glucose concentrations in blood (Cui, Ye et al. 2007).
The platinum-lead sensor seems to be the most suitable sensor for our release mechanism. Because of the
unknown toxicity of lead it would though be better to use the nickelhydroxide sensor if it is also useable
without the alkalinity.
3.3 Polymer-membranes for encapsulating cells
The carbon nanotubes have to be placed in a functional membrane with several characteristics. This
membrane has to be insoluble, because the artificial organ will be placed in the tissue, in contact with tissue
fluids, for optimal glucose measuring. Also the membrane has to be non-porous, so cells and
immunoglobins from the immune system are not able to reach insulin-producing cells inside the artificial
organ. Furthermore insulin needs to flow only through the multi-walled carbon nanotubes so that its flow
rate can be regulated. Because the membrane contacts the constituents of blood directly, the membrane
must be biocompatible and able to avoid causing thrombus formation, immune reaction and inflammation
(Kawakami 2008).
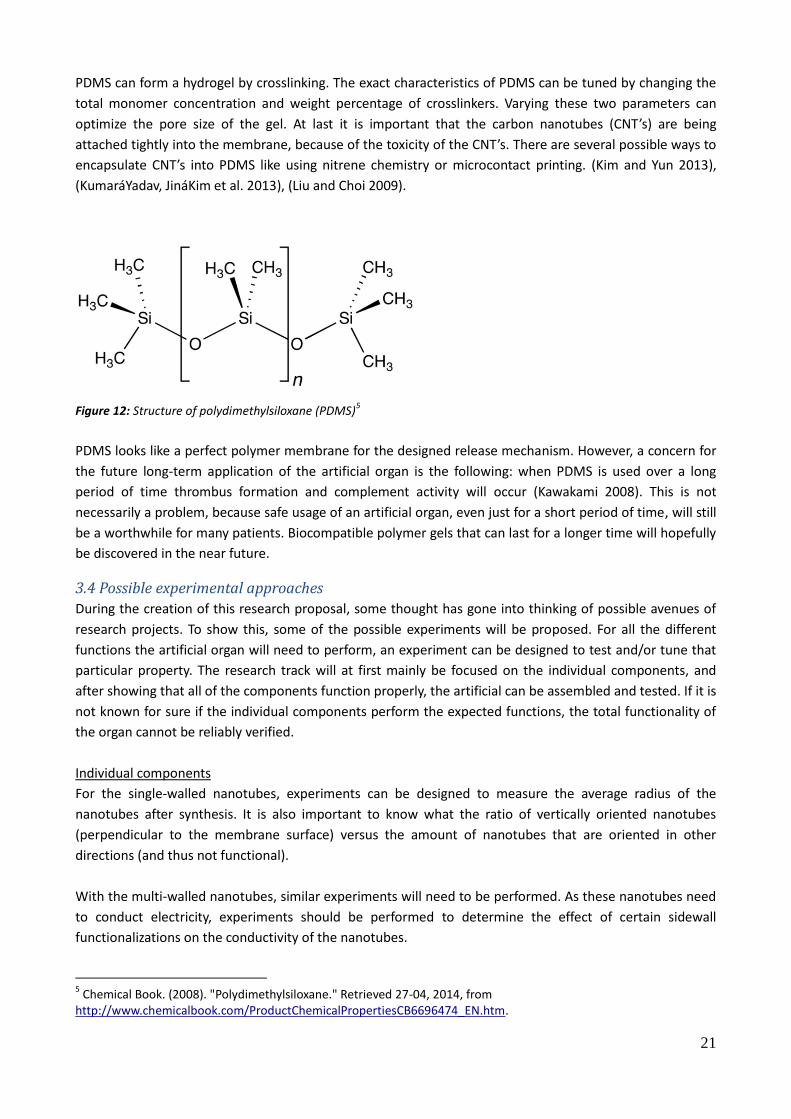
Polydimethylsiloxane membrane
A possible membrane that includes all these properties could be a hydrogel of the polymer
polydimethylsiloxane (PDMS) (figure 12). This is a typical polymer that is often used for membrane
materials in artificial organs (Kawakami 2008). Because PDMS has a hydrophobic surface the absorption of
proteins and biogenic substances into the surface of the membrane is inhibited. This is important because
this avoids the aforementioned biocompatibility issues. In this way PDMS is more biocompatible than most
other polymer membranes.
21
PDMS can form a hydrogel by crosslinking. The exact characteristics of PDMS can be tuned by changing the
total monomer concentration and weight percentage of crosslinkers. Varying these two parameters can
optimize the pore size of the gel. At last it is important that the carbon nanotubes (CNT’s) are being
attached tightly into the membrane, because of the toxicity of the CNT’s. There are several possible ways to
encapsulate CNT’s into PDMS like using nitrene chemistry or microcontact printing. (Kim and Yun 2013),
(KumaráYadav, JináKim et al. 2013), (Liu and Choi 2009).
Figure 12: Structure of polydimethylsiloxane (PDMS)5
PDMS looks like a perfect polymer membrane for the designed release mechanism. However, a concern for
the future long-term application of the artificial organ is the following: when PDMS is used over a long
period of time thrombus formation and complement activity will occur (Kawakami 2008). This is not
necessarily a problem, because safe usage of an artificial organ, even just for a short period of time, will still
be a worthwhile for many patients. Biocompatible polymer gels that can last for a longer time will hopefully
be discovered in the near future.
3.4 Possible experimental approaches
During the creation of this research proposal, some thought has gone into thinking of possible avenues of
research projects. To show this, some of the possible experiments will be proposed. For all the different
functions the artificial organ will need to perform, an experiment can be designed to test and/or tune that
particular property. The research track will at first mainly be focused on the individual components, and
after showing that all of the components function properly, the artificial can be assembled and tested. If it is
not known for sure if the individual components perform the expected functions, the total functionality of
the organ cannot be reliably verified.
Individual components
For the single-walled nanotubes, experiments can be designed to measure the average radius of the
nanotubes after synthesis. It is also important to know what the ratio of vertically oriented nanotubes
(perpendicular to the membrane surface) versus the amount of nanotubes that are oriented in other
directions (and thus not functional).
With the multi-walled nanotubes, similar experiments will need to be performed. As these nanotubes need
to conduct electricity, experiments should be performed to determine the effect of certain sidewall
functionalizations on the conductivity of the nanotubes.
5 Chemical Book. (2008). "Polydimethylsiloxane." Retrieved 27-04, 2014, from
http://www.chemicalbook.com/ProductChemicalPropertiesCB6696474_EN.htm.

22
The molecular valves need to fully stop insulin from crossing the membrane. Experiments need to be
performed to determine the optimal amount of tip functionalizations, for example the amount of rotaxanes
needed to close the nanotubes efficiently. Another possible experiment could be testing the effect of
changing the part of the rotaxanes between the two charged rings, to see if the ring shifting can be
performed over larger distances. This would in turn create more options for optimizing the insulin release
rate.
With the glucose sensors, the main concerns are biocompatibility and sensitivity/selectivity. The toxicity of
the sensors needs to be researched, as these molecules are the only part of the artificial organ that is
directly in contact with the bodily fluids. The sensitivity and the selectivity of the sensors in biological
circumstances need to be verified.
The last main component on which experiments can be performed is the polymer membrane, with
structural integrity as the main concern. The integrity and durability of the membrane could be tested
holding into account the fluctuating levels of pH and temperature in the human body.
Combined components
If all these components work as planned and as efficiently as possible, the artificial organ can be fully
assembled and tested as a full-scale system. At this point, more macro-scale concepts come into play, for
example, the structural degradation and the efficiency of the entire system (the speed and size of the
insulin response to certain signals) can be measured. The function of the artificial organ can at first be
tested in vitro, by placing the artificial organ in a medium with shifting glucose levels, while measuring the
insulin release rate into the external medium. Experiments in vitro can also enlighten doubts about the
durability of the organ. If all goes well, experiments in vivo can be performed, in which testing the toxicity
and biocompatibility of the organ becomes the most important aspect.

23
4. Implementation
In the preceding chapters the aspects of a proposed artificial organ are described. This artificial organ
consists of several aspects: a molecular valve, a sensor, carbon nanotubes and a membrane. The biggest
challenge of this research proposal is to let all the different parts of the release mechanism work together
as a well-functioning system. First of all the release mechanism has to be synthesized and after this tests
must be done to make sure the release mechanism actually produces the expected results.
The main aim is to create an artificial organ that can be used to control the blood glucose by measuring
glucose and releasing insulin at the right moment, but a long term goal will be to use the release
mechanism for other releasing processes in the body. The design of such a device needs a mathematical
model, which represents the glucose-insulin feedback system. In this research proposal it is not the aim to
make a model of the glucose-insulin feedback system, but it is essential to compare the designed release
mechanism with the model of a healthy pancreas. Also it is necessary to understand the disorders that can
occur in the pancreas and lead to diabetes, so the release mechanism can be used in the right way and
location.
There are several possible models described by Palumbo et al., which can be compared to the eventual
results of our release mechanism. The most well-suited models are aiming to describe glucose homeostasis
from a phenomenological point of view, at organ and tissue levels without getting too deep into the
metabolic details. In these models glucose concentration in the blood induces an insulin release of the
pancreas consisting of two contributions. The first phase is quick response to a sudden glycaemia change.
The second phase is a release of insulin after about ten minutes. Also a number of hormones like adrenalin,
glucagon, growth hormones and cortisol contribute to rescuing the body form hypoglycaemia. However,
since clinical procedures are normally used at inappropriately high glycaemia because of a lack of insulin,
most of the existing models consider a simplified system in which glucose is only controlled by insulin. It will
become a challenge to adjust the designed release mechanism to the models of glucose-insulin
homeostasis in the human body (Palumbo, Ditlevsen et al. 2013).
Nevertheless the independent parts of the release mechanism are not perfect either. First of all the system
has to be biocompatible. The membrane is biocompatible, but the carbon nanotubes are not
biocompatible, if they come into contact with the bodily fluids or the bloodstream. The toxicity of the
compartments plays an important role. Specific testing has shown that PDMS is not toxic and does not bio-
accumulate in organisms (Kukkonen and Landrum 1995). On the other hand CNT’s are actually rather toxic.
It is known that under some conditions carbon nanotubes can cross the membrane barriers and that if raw
materials reaches the organs they can induce harmful effects as inflammatory and fibrotic reactions
(Kolosnjaj, Szwarc et al. 2007). However these carbon nanotubes are only toxic while they are released to
the body, so it is really important to attach the carbon nanotubes tightly into the membrane.
The sensor mechanism is a component that will be in contact with the patient’s body, which is why it is
important to consider its toxicity. In the section dedicated to the sensors, several different options are
considered, with varying degrees of expected toxicity. The gate mechanism should in principle not come
into direct contact with the patient’s blood or immune system, so toxicity is less of a concern than it is with
the sensors.
24
A location for the artificial organ has to be decided upon. It is important that the release mechanism is
placed in the tissue fluid because this way the glucose concentration can be measured. The most logical
location to place the artificial organ would be near the pancreas, because this place has the same
conditions as the normal beta cells that normally produce insulin in healthy people. However this would
mean the patient has to undergo an invasive surgery each time the artificial organ has to be replaced. A less
invasive method would be to bring the artificial organ under the skin. It is not possible to inject the artificial
organ into the veins because it would get stuck in the capillaries. So it would be a solution to bind the
artificial organ to the connective tissue under the skin, adjacent to a blood vessel. There must be done
further research in this area.
Also the durability of the artificial organ could become a concern. The parts of the artificial organ have to
last for a certain time so the patient has to come to the hospital as infrequently as possible. However it
would already be an improvement if the artificial organ has a durability of only one or a few weeks to
months, because at the moment these patients have to inject themselves with insulin several times a day.
The membrane material PDMS looks like a perfect polymer membrane for the designed release
mechanism. However when PDMS is used over a long period of time thrombus formation and complement
activity will occur (Kawakami 2008). The durability of the other components, employed in this new way,
needs to be determined through experiments.
Finally, when all these problems are solved the release mechanism could be used as an artificial organ for
diabetic patients. However this stage has not been reached and a lot of research is necessary to make the
release mechanism and the artificial pancreas a reality.

25
5. Conclusion
A concept for making an artificial organ which is applied to insulin production is proposed. The artificial
pancreas has a great social interest because it can be used by people suffering from the disease diabetes
(type 1). The proposed pancreas is also just a model system for the treatment of many diseases which act in
a similar way to glucose. This organ ideally consists of insulin producing cells in a hydrogel, encapsulated by
a membrane. In this membrane small single-walled carbon nanotubes are placed to provide the cells of
oxygen and nutrients. Furthermore, the thicker multi-walled carbon nanotubes, also placed in the
membrane, are functionalized with a gate mechanism, the molecular valve, and a glucose sensor. The
glucose sensor measures the glucose concentration in the blood, thereby producing an electrical current.
This current is conducted through the carbon nanotubes to the molecular valve. Here a reduction reaction
takes places which opens the gate so insulin can pass the membrane and leave into the bloodstream. We
expect that it is possible to actually create and implant this proposed organ. Research has to be done to
couple the working mechanisms of the molecular valve and the glucose sensor to each other and to the
carbon nanotube. After the concept has proven viable, optimization will be the next step on the road to
treating a wide array of diseases.

26
6. References
Ahn, C. H., Y. Baek, et al. (2012). "Carbon nanotube-based membranes: Fabrication and application to desalination." Journal of Industrial and Engineering Chemistry 18(5): 1551-1559. Association, A. D. (2008). "Diagnosis and classification of diabetes mellitus." Diabetes care 31(Supplement 1): S55-S60. Bandaru, P. R. (2007). "Electrical properties and applications of carbon nanotube structures." Journal of nanoscience and nanotechnology 7(4-5): 4-5. Brange, J., D. R. Owens, et al. (1990). "Monomeric insulins and their experimental and clinical implications." Diabetes care 13(9): 923-954. Brill, M. T. (2012). Diabetes. Minneapolis, MN, Twenty-First Century Books. Chang, D. W., I.-Y. Jeon, et al. (2013). "Mild and Nondestructive Chemical Modification of Carbon Nanotubes (CNTs): Direct Friedel-Crafts Acylation Reaction." Cui, H.-F., J.-S. Ye, et al. (2007). "Selective and sensitive electrochemical detection of glucose in neutral solution using platinum–lead alloy nanoparticle/carbon nanotube nanocomposites." Analytica chimica acta 594(2): 175-183. De Geest, B. G., A. M. Jonas, et al. (2006). "Glucose-responsive polyelectrolyte capsules." Langmuir 22(11): 5070-5074. DeWitt, D. E. and I. B. Hirsch (2003). "Outpatient insulin therapy in type 1 and type 2 diabetes mellitus: scientific review." Jama 289(17): 2254-2264. Dey, S. K., A. Coskun, et al. (2011). "A redox-active reverse donor–acceptor bistable [2] rotaxane." Chemical Science 2(6): 1046-1053. Fahrenbach, A. C., S. C. Warren, et al. (2013). "Organic Switches for Surfaces and Devices." Advanced Materials 25(3): 331-348. Fasman, G. D. and C. Press (1975). Handbook of biochemistry and molecular biology, CRC press Cleveland, Ohio. Georgakilas, V., K. Kordatos, et al. (2002). "Organic functionalization of carbon nanotubes." Journal of the American Chemical Society 124(5): 760-761. Grattoni, A., S. Parazynski, et al. (2011). "Building Nanoglands." Mechanical engineering 133(2): 22-26. Guiseppi-Elie, A., C. Lei, et al. (2002). "Direct electron transfer of glucose oxidase on carbon nanotubes." Nanotechnology 13(5): 559. Hoffman, A. S. (2002). "Hydrogels for biomedical applications." Advanced Drug Delivery Reviews 54(1): 3-12. Jiang, Y., S. Yu, et al. (2013). "Improvement of sensitive Ni (OH)2 nonenzymatic glucose sensor based on carbon nanotube/polyimide membrane." Carbon 63: 367-375.
27
Kawakami, H. (2008). "Polymeric membrane materials for artificial organs." Journal of Artificial Organs 11(4): 177-181. Kim, D. and K.-S. Yun (2013). "Patterning of carbon nanotube films on PDMS using SU-8 microstructures." Microsystem technologies 19(5): 743-748. Kolosnjaj, J., H. Szwarc, et al. (2007). Toxicity studies of carbon nanotubes. Bio-Applications of Nanoparticles, Springer: 181-204. Kopeček, J. (2002). "Polymer chemistry: swell gels." Nature 417(6887): 388-391. Kukkonen, J. and P. F. Landrum (1995). "Effects of sediment‐bound polydimethylsiloxane on the bioavailability and distribution of benzo [a] pyrene in lake sediment to Lumbriculus variegatus." Environmental Toxicology and Chemistry 14(3): 523-531. KumaráYadav, S., I. JináKim, et al. (2013). "PDMS/MWCNT nanocomposite actuators using silicone functionalized multiwalled carbon nanotubes via nitrene chemistry." Journal of Materials Chemistry C 1(35): 5463-5470. Kuzmany, H., A. Kukovecz, et al. (2004). "Functionalization of carbon nanotubes." Synthetic Metals 141(1): 113-122. Leibiger, I. B., B. Leibiger, et al. (2008). "Insulin Signaling in the Pancreatic β-Cell." Annual Review of Nutrition 28(1): 233-251. Li, M., R. L. Harbron, et al. (2013). "Electrostatically gated membrane permeability in inorganic protocells." Nat Chem 5(6): 529-536. Liu, C.-X. and J.-W. Choi (2009). "Patterning conductive PDMS nanocomposite in an elastomer using microcontact printing." Journal of Micromechanics and Microengineering 19(8): 085019. Lombarte, M., M. Lupo, et al. (2013). "Mathematical model of glucose–insulin homeostasis in healthy rats." Mathematical biosciences 245(2): 269-277. Murua, A., A. Portero, et al. (2008). "Cell microencapsulation technology: towards clinical application." Journal of Controlled Release 132(2): 76-83. Nguyen, T. D., Y. Liu, et al. (2007). "Design and optimization of molecular nanovalves based on redox-switchable bistable rotaxanes." Journal of the American Chemical Society 129(3): 626-634. Nygaard, S., K. C.-F. Leung, et al. (2007). "Functionally rigid bistable [2] rotaxanes." Journal of the American Chemical Society 129(4): 960-970. Orive, G., R. Maria Hernández, et al. (2004). "History, challenges and perspectives of cell microencapsulation." TRENDS in Biotechnology 22(2): 87-92. Palumbo, P., S. Ditlevsen, et al. (2013). "Mathematical modeling of the glucose–insulin system: A review." Mathematical biosciences 244(2): 69-81. Qiu, Y. and K. Park (2001). "Environment-sensitive hydrogels for drug delivery." Advanced Drug Delivery Reviews 53(3): 321-339.

28
Randall, C. L., Y. V. Kalinin, et al. (2011). "Self-folding immunoprotective cell encapsulation devices." Nanomedicine: Nanotechnology, Biology and Medicine 7(6): 686-689. Reilly, R. M. (2007). "Carbon nanotubes: potential benefits and risks of nanotechnology in nuclear medicine." Journal of Nuclear Medicine 48(7): 1039-1042. Rickels, M. R. (2012). "Recovery of endocrine function after islet and pancreas transplantation." Current diabetes reports 12(5): 587-596. Segura, J. L. and N. Martín (2001). "New concepts in tetrathiafulvalene chemistry." Angewandte Chemie International Edition 40(8): 1372-1409. Sherwood, L., H. Klandorf, et al. (2012). Animal physiology: from genes to organisms, Cengage Learning. Sun, Z., X. Zhang, et al. (2007). "Coating carbon nanotubes with metal oxides in a supercritical carbon dioxide–ethanol solution." Carbon 45(13): 2589-2596. Swartz, J. R. (2001). "Advances in Escherichia coli production of therapeutic proteins." Current Opinion in Biotechnology 12(2): 195-201. Takagi, D., Y. Homma, et al. (2006). "Single-walled carbon nanotube growth from highly activated metal nanoparticles." Nano letters 6(12): 2642-2645. Wang, S., Q. Zhang, et al. (2003). "A novel multi-walled carbon nanotube-based biosensor for glucose detection." Biochemical and biophysical research communications 311(3): 572-576. Ward, C. W. and M. C. Lawrence (2009). "Ligand‐induced activation of the insulin receptor: a multi‐step process involving structural changes in both the ligand and the receptor." Bioessays 31(4): 422-434. Ye, J.-S., Y. Wen, et al. (2004). "Nonenzymatic glucose detection using multi-walled carbon nanotube electrodes." Electrochemistry Communications 6(1): 66-70. Zhang, Y. H. P. (2010). "Production of biocommodities and bioelectricity by cell‐free synthetic enzymatic pathway biotransformations: Challenges and opportunities." Biotechnology and bioengineering 105(4): 663-677.