medical practice (africa vs north america) dr louis uwaifo, md
TRANSCRIPT

Medical practice:Africa vs North America
Dr. Louis Uwaifo
Resident, Family Medicine,
University of Benin Teaching Hospital
(U.B.T.H.)

Outline• Introduction
• Definition
• Ideal medical practice model
• Reality check, comparison
• “Medicine is universal”
• Role of government
• Challenges facing medical practice in Africa and possible solutions
• Conclusion
• Thank you
Introduction
• Medical practice in Africa and North America have a
number of differences, and we will in this session
attempt to discuss some pieces of the puzzle.

Medical Practice
• Medical practice is a type of business in which a
medical practitioner or group of practitioners work with
patients in order to diagnose and treat illnesses,
injuries or other medical conditions that require care.
Ideal Medical Practice (IMP) model(L. Gordon Moore, MD, and John H. Wasson, MD, FAM PRACT MANAG. 2007)
• What is an Ideal Medical Practice?
Low overhead with high technology, wrapped around an excellent
physician-patient relationship.
• Ideal Medical Practice- A practice model designed to enhance doctor-
patient relationships, increase face-to-face time between doctors and
patients, reduce physician workloads, instill patients with a sense of
responsibility for their health and cut wasted dollars from the entire
system.

Ideal Medical Practice Typical Practice
Care is driven by the patient's needs, goals and
values- Patient Centered
Care is driven by the
practice's priorities-
Doctor Centered
Access is 24–7. Access is 9–5.
The care team uses technology to its fullest (e.g.,
electronic health records, e-mail, Internet scheduling).
The care team avoids new
technology.
Patients can see their own physician whenever they
choose.
Patients must see whoever
is available.
The majority of the office visit is spent with the
physician.
The majority of the office
visit is spent waiting.
Ideal Medical Practice
Overhead is low.
Typical Practice
Overhead is high.
Patients are seen the same day they call
the office.
Patients typically wait for an
appointment.
Physicians are able to see fewer
patients per day.
Physicians must generate high numbers
of visits per day to cover overhead.
Practices measure themselves regularly. Practices have little or no performance
data.
Practices are proactive in their care of
patients with chronic illnesses.
Practices are reactive in their care of
patients with chronic illnesses.
Physicians are satisfied and feel in
control.
Physicians feel harried and overbooked.

Reality Check: Case Scenarios (discussion)
Africa (Nigeria)
• A patient with an influential relative
as staff vs the average patient who
knows nobody
North America (US)
• Prof’s bilateral malleolar fracture
during a visit to the US

MEDICINE:
• is indeed universal, without special treatment to some, in other
words everyone should be treated with the same level of care
irrespective of who the know or their affiliations.
AFRICA (S.A) VS NORTH AMERICAN (CA) ER ACTIVITIES (VIDEOS)

ROLE OF GOVERNMENT
• United States (Population - 318.9million, United States Census Bureau, 2014);
Medicare, Medicaid, CHIP, and Marketplace Subsidies: Four health insurance
programs — Medicare, Medicaid, the Children’s Health Insurance Program (CHIP),
and Affordable Care Act (aca) marketplace subsidies — together accounted for
25 percent of the budget in 2015, or $938 billion. Nearly two-thirds of this
amount, or $546 billion, went to Medicare, which provides health coverage to
around 55 million people who are over age 65 or have disabilities. About $8,000
was spent per person, (The Center on Budget and Policy Priorities)
• It is estimated that approximately 62% of hospitals are non-profit, 20% are
government owned, and 18% are for-profit (Toronto Notes, 2015)

ROLE OF GOVERNMENT CONTD.
• Canada; (Population - 35.16 million, Statistics Canada 2013); In 2015, Total
health expenditure in Canada was expected to reach $219.1 billion, or
$6,105 per person. it is anticipated that, overall, health spending will
represent 10.9% of Canada’s gross domestic product, (Canadian Institute for
Health Information)
• Hospital services in Canada are publicly funded but delivered through
private, not-for-profit institutions owned and operated by communities,
religious organizations, and regional health authorities (Toronto Notes, 2015)

ROLE OF GOVERNMENT CONTD.
• Nigeria; (Population – 177.5 million, World Bank, 2014 )
N262b ($1.7billion) has been allocated to Health in Nigeria’s 2014
budget (Nigeria Health watch, 2014)

PERCENTAGE OF GDP SPENT ON HEALTHCARE, (World Bank, 2015)
Country Name Health expenditure, total (% of
GDP)
United States 17.1%
Canada 10.9%
South Africa 8.9%
Ghana 5.4%
Nigeria 3.9%
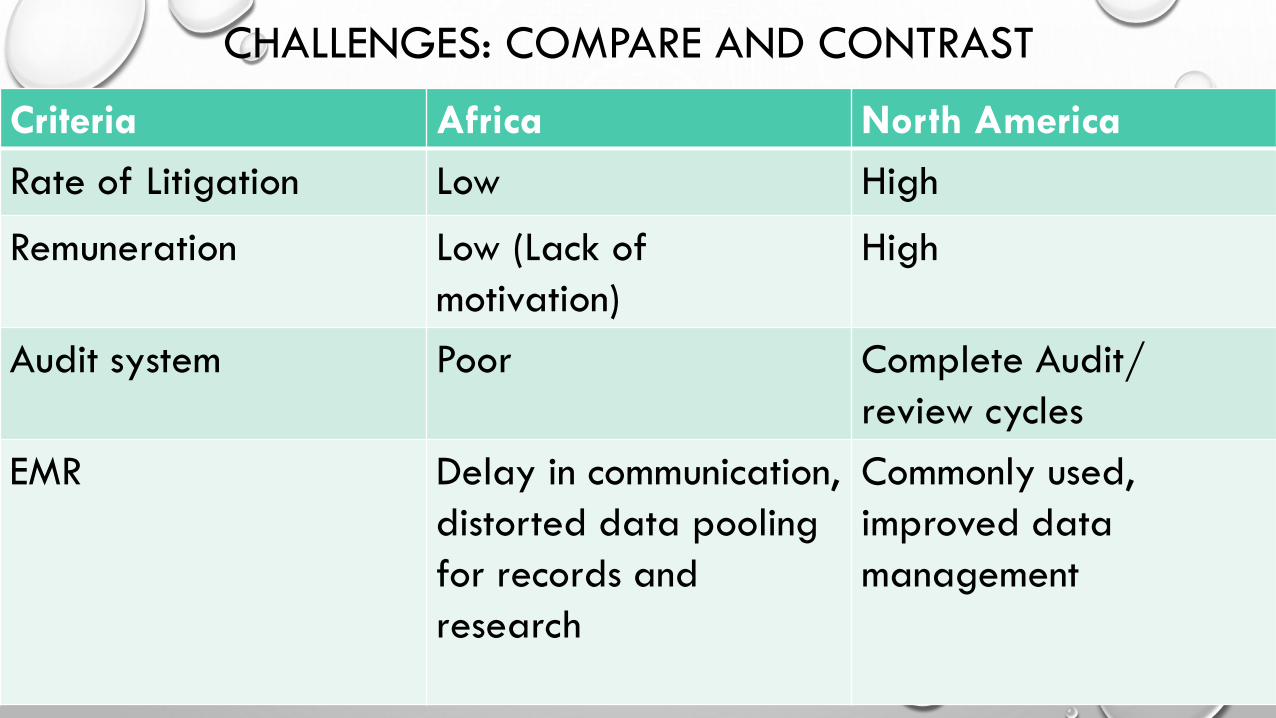
CHALLENGES: COMPARE AND CONTRAST
Criteria Africa North America
Rate of Litigation Low High
Remuneration Low (Lack of
motivation)
High
Audit system Poor Complete Audit/
review cycles
EMR Delay in communication,
distorted data pooling
for records and
research
Commonly used,
improved data
management
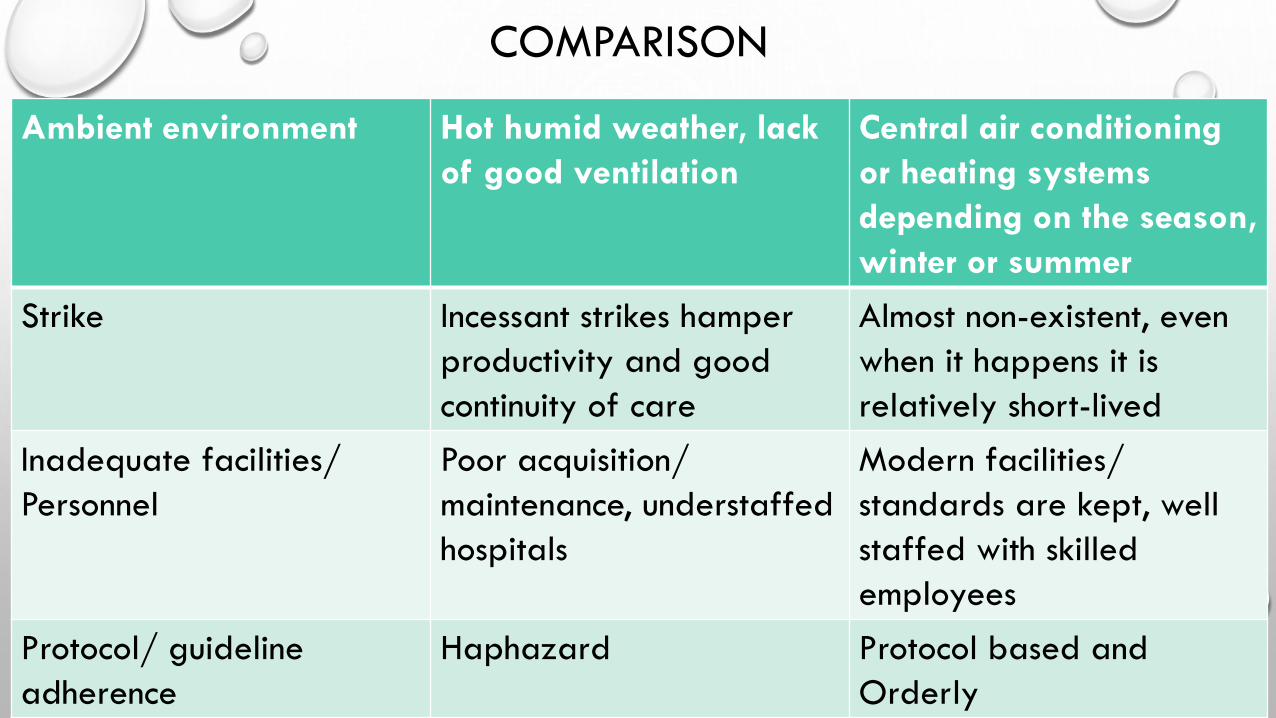
COMPARISON
Ambient environment Hot humid weather, lack
of good ventilation
Central air conditioning
or heating systems
depending on the season,
winter or summer
Strike Incessant strikes hamper
productivity and good
continuity of care
Almost non-existent, even
when it happens it is
relatively short-lived
Inadequate facilities/
Personnel
Poor acquisition/
maintenance, understaffed
hospitals
Modern facilities/
standards are kept, well
staffed with skilled
employees
Protocol/ guideline
adherence
Haphazard Protocol based and
Orderly

Suggestions to problems with medical practice in Africa
• Ambient environment: a conducive working environment is essential to enhancing
doctors’ efficiency and productivity; preventing us from wanting to rush through our
work to go get some fresh air
• Management Protocols/ guidelines: should be made readily available both physically
and in electronic format for doctors easy perusal; access to up-to-date journals,
attending training conferences
• Facilities: acquisition and maintenance of facilities ensures sustenance of otherwise
expensive machines, as it is cheaper to maintain than replace
• Electronic health/ medical records: introduction and training of doctors to use the EMR;
a systematized collection of patient and population electronically-stored health
information in a digital format

Suggestions contd.
• Remuneration: health professionals work passionately for long hours no doubt,
medicine is not all about money but cash and noncash incentives for work done is an
important motivating factor
• Audit: complete weekly audit cycles, with appraisals of targets and outcomes to see
where adjustments are needed, to ensure protocols are adhered to
• Strike: ‘excellent patient care’, our ideal model’s goal can be protected by promptly
addressing concerns health workers may have to prevent industrial actions that
disrupts our practice and jeopardise continuity of care
• Litigation: getting law enforcement involved when necessary and implementation
committees for existing laws; also education of the citizenry on their rights and
privileges

CONCLUSION
• Is there hope for an Ideal Medical Practice in Africa?
• There is hope! The largest room in the world is the room for improvement (Brian Tracy).
The reasons there are so many disparities between Africa and North American medical
practice is multifactorial and the fix wont be overnight; we will get there as long as we
“become addicted to constant and never ending self improvement” (M. Gandhi)

THANK YOU