medical genetics - postgraduate medical journal · first time - edward's syndrome (trisomy...
TRANSCRIPT

Postgrad Med J (1991) 67, 613 - 631 ) The Fellowship of Postgraduate Medicine, 1991
Reviews in Medicine
Medical genetics
Maurice Super
Royal Manchester Children's Hospital, Pendlebury M27 JHA, UK
Introduction
The 1980s have seen a number of exciting andimportant developments in our knowledge ofhuman genetics. Instead of a rather empiricspeciality based on clinical and pedigree inform-ation alone, the locations of many genes have nowbeen discovered and the exact molecularconfiguration of the gene of some. Preclinical, evenprenatal diagnosis becomes feasible for disorderswhere this was previously not possible. Hopefullygeaetics in the 90s will include the rolling back ofthe frontiers of gene therapy.
Chromosomes
Advances in chromosome analysis have comeabout with great improvements in techniques, firstwith prometaphase banding allowing for muchlonger chromosomes with very clear banding pat-terns. This has allowed a number of microdeletiondisorders to be recognized including the interstitialdeletion of chromosome 11 associated with theWilm's tumour-aniridia syndrome, and ofchromo-some 15 with Prader-Willi and Angelman's syn-dromes.
The relationship of other chromosomal abnor-malities with tumour predisposition, e.g. retino-blastoma and deletion of part of chromosome 13(13q-), is better understood. Chromosomal re-arrangement found in clones in specific tumours isslightly beyond the remit of this article and will notbe discussed further.An important chromosome disorder, the fragile
X syndrome is now well recognized and requiresspecial culture techniques for its demonstration.Mosaic chromosome disorders, such as Killian-
Pallister syndrome which associates mental handi-cap, hypotonia, a high anterior hairline and thinupper lip, reveal the abnormal chromosome only in
tissues with a slow turnover of cells, such as incultured fibroblasts, while not being detectable inthe blood.A marriage ofmolecular genetic and cytogenetic
techniques allows increasingly refined in situ hy-bridization. Unfortunately, this powerful diagnos-tic tool remains very much at a research level.Studies in Down syndrome, some of which haveemployed in situ hybridization have concentratedon the minimum amount of trisomic materialnecessary for the phenotype, with accurate mapp-ing of the whole chromosome; localization of thegene for Alzheimer's disease to chromosome 21and the occurrence of presenile fibrillary tangles inDown syndrome have helped to shed light on this.
There has been much interest lately in theparental origin of chromosome disorders, withimprinting recognized in man for the first time.
Single gene disorders
A great leap forward in our knowledge of singlegene disorders has resulted from the somewhatunexpected success of reverse genetics - instead ofstarting off with a known protein or RNA, as waspossible for disorders ofhaemoglobin, for instance,application of markers to families with more thanone affected member has allowed accurate chromo-somal localization of a number of single genedisorders, notably myotonic dystrophy, Hunting-ton's disease, Duchenne and Becker musculardystrophies, cystic fibrosis, Friedreich's ataxia,neurofibromatosis I, facio-scapulo-humeral mus-cular dystrophy and spinal muscular atrophy.More recently, Marfan syndrome has been pro-visionally located on chromosome 15q.For some of these, notably Duchenne and
Becker muscular dystrophies and cystic fibrosis,the actual responsible genes have been found, withthe exact molecular abnormality identified in a highpercentage. Duchenne and Becker's are allelic andthe clinical picture can often be predicted from thetype of mutation and whether it results in a
Correspondence: M. Super, M.D., M.Sc., F.R.C.P.,D.C.H.
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

614 M. SUPER
catastrophic effect on the dystrophin molecule.For some disorders exact localization remains
difficult or puzzling. Although there seems to begood evidence of a locus for adult type polycystickidney disease linked to the alpha globin locus, onchromosome 16, in certain families an entirelydifferent locus is suggested by linkage studies.Similarly, the gene for tuberous sclerosis is linkedto a locus on chromosome 9 and British experiencefavours this localization of the gene. On the otherhand a number of American families show linkageto a locus on chromosome 11 and the Americanscannot confirm the British linkage experience. Bothgroups have families which seem to show linkage toneither locus. One difficulty in such studies, ondisorders very variable clinically, is assigning indi-viduals to affected or not affected categories, withinfamilies.
New DNA analysis techniques
A major development in analysis is the polymerasechain reaction (PCR) which shortens the analysistime and dispenses with the need for radio-activityrequired for more formal Southern blot analysis.PCR has extremely useful applications which
have been quickly realized. These include analysisof tiny samples, theoretically possible on the DNAof a single cell. There are many applications of thetechnique, by no means confined to genetic dis-orders. There has been some success in amplifyingDNA from single blastomeres, preimplantation,following in vitro fertilization as in ascertainingpresence of the Y chromosome in sex-linkeddisorders. Similarly there are early attempts tostudy the paternal contribution to fetal cells in themother's circulation. Such tests could avoidinvasive prenatal diagnosis.The discovery of great variability of the lengths
of satellite DNA between functioning genes is apowerful tool in distinguishing between individualsby genetic 'fingerprinting'. This has alreadyachieved widespread use in forensic and medico-legal work and by immigration authorities inchecking parentage.
Diseases which involve abnormalities ofDNA ofthe mitochondria have been discovered and therelationship of mitochondrial and nuclear DNA isbetter understood by studies in Kearns Sayerssyndrome.We still await clear elucidation of the genetic
components of various multifactorial disorders,such as neural tube defect, coronary heart diseaseand hypertension.
Prenatal tests
Prenatal testing earlier than that feasible byamniocentesis is now well established, though still
not nearly as widely available. Chorionic biopsyperformed at 9 weeks reflects the fetal status andallows chromosomal, DNA and enzyme analysis.Risks of miscarriage still exceed those ofamniocentesis and new technicians have highermiscarriage rates, during their learning curve.Where the risk of the disorder is high, thenchorionic villus sampling gives acceptably lowmiscarriage rates in experienced hands.
Screeningfor genetic disorders
Open neural tube defect screening by a combina-tion of serum a fetoprotein (AFP) and ultrasoundhas been used successfully in a number ofcentres inmany countries, notably in the United Kingdomand North America. Families need careful supportwhen screening tests prove positive. There is grow-ing enthusiasm for the introduction of pregnancyscreening for Down syndrome, using combinationsof tests including maternal age, serum AFP andserum human chorionic gonadotrophin (HCG).Such tests greatly increase the detection rates inyoung women to whom the majority ofbabies withDown syndrome are born. Currently about 60% ofDown syndrome is detectable by such screening.
Cystic fibrosis (CF) carrier screening wouldallow a greater disease detection rate in pregnancythan screening for Down syndrome, but the condi-tion is less well known by the public and lack ofnursing and medical awareness of the disorder andof the medical advances makes it premature tointroduce this on a wide scale now. Pilot cysticfibrosis carrier screening studies are in progress in anumber of centres.
Tay-Sachs disease and thalassaemia carrierscreening programmes have been very successful insome countries, whereas an early experience withsickle cell trait screening in New York is widelyregarded as having been very unsatisfactory, withscreened individuals feeling stigmatized and withresults and the implications of the results beingpoorly understood by many.The new genetics brings the emergence of a new
set of ethical and moral problems and theenthusiasm to introduce new techniques must bemade to keep time with medical, paramedical andlay education. New ways of treating geneticdisorders are being developed. Organ and bonemarrow transplantation have had some successes.
Specific gene therapy has the potential of beingmore effective with fewer side effects. Very earlyexperiments in Duchenne muscular dystrophy andin cystic fibrosis bring the hope that we are on thethreshold of a new era of treatment. Our capacityto recognize individuals at risk for certain disordersis likely to increase greatly at the same time.Pharmacogenetics will become more elegant andtreatments more tailored to the individual's genetic
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

MEDICAL GENETICS 615
background.Lastly, as described earlier, some of Mendel's
laws of segregation and inheritance need furtherscrutiny. Experiments have shown undoubtedexamples of molecular imprinting in mice, andclinical instances in man are being recognizedwhere inheritance of a maternal gene or portion ofchromosome gives a different phenotype to inheri-tance from the father. A yet more dramatic occur-rence is the existence of proven instances ofuniparental disomy, with both chromosomes in thecell inherited from one parent and with no evidenceof a contribution of that chromosome by the otherparent. The phenomenon has been observed twicein cystic fibrosis with a phenotypic effect of shortstature noted. Molecular analysis is certain touncover more instances of this phenomenon.
This introduction has briefly touched on themajority of important growth areas in genetics ofthe past decade. The individual topics will now beexpanded upon under the following headings:chromosomal advances - technical and clinical;advances in molecular biology: technical andclinical; screening for genetic disease; and ethicaland moral issues.
Chromosomes
It was only with the introduction in the 1950s ofcolchicine into chromosome cultures that cells were'frozen' in metaphase of mitosis and accurate coun-ting became possible. Before this it was thoughtthat there were 48 instead of 46 chromosomes pernormal human cell. Numerical abnormalities ofchromosome number were quickly discovered -Down syndrome' and later Klinefelter syndrome in1959.1 One rare disorder became dispropor-tionately famous - the cri du chat syndromeassociated with a significant deletion of the shortarm of chromosome 5 (5p-),3 visible even in therather short, dumpy chromosomes in karyotypespreads at that time. The incidence of majorstructural disorders of chromosomes in newbornswas established in a large four centre study, with56000 consecutive newborns analysed.4'5 Theincidences of the various aneuploidies and ofstructural rearrangements, including balanced andunbalanced chromosomes, were provided by thisvaluable study. Parts of it have been repeatedsubsequently and other studies have defined theincidence of chromosome abnormality in spon-taneous miscarriages and in stillbirths.6 A usefulrough reminder of these incidences emerged, witheach of the following being slight underestimates:chromosomal anomalies in spontaneous (recog-nized) miscarriage - 50%, in stillbirths- 5% and inlive newborns - 0.5%. Phenotypes of specificchromosome abnormalities were described for the
first time - Edward's syndrome (Trisomy 18),7Patau syndrome,8 to name but two. Klinefelter's9and Turner's syndrome'0 became better under-stood.
In the late 1960s Caspersson" introducedquinacrine banding which allowed differentiationof chromosomes of similar size from one anotherand Seabright's introduction of trypsin into cul-tures,'2 allowing partial digestion of the chromo-somal skeleton, is still an integral part of mostmajor banding techniques today. Quinacrinefluorescence which fades with time has been largelydiscarded in the standard chromosome laboratory.Caspersson was ahead of his time in the attemptedcomputerization of chromosome analysis alreadyin 1969. With the use of the fluorescent cell sorter,emissions from chromosome groups of varioussizes do allow some subtle chromosomal abnor-malities to be elucidated,'3 though the techniquedoes not form an important part of day-to-daypractice. Younis added methotrexate to chrom-osome cultures,'4 thus bringing cells into a uniformstate of mitototic division and allowing for 'freez-ing' in prometaphase, giving much longerchromosomes, capable of more accurate analysisand with more subtle abnormalities noticeable,especially tiny deletions. Breakpoints in structuralrearrangements can be defined more accurately andthis has been of value in focusing DNA investiga-tion when a gene site has been disrupted by atranslocation, as occurred for instance in locationof the gene for Duchenne muscular dystrophy.'5 Acertain amount of reinvestigation of peopleoriginally thought to be normal on chromosomeanalysis has proved necessary. This has appliedespecially to the fragile X syndrome, first noted byLubs in 196916 and then rediscovered by GillianTurner in 1979. ' Cells need to be cultured in a folicacid-deficient medium to demonstrate the fragilesite. Minor adjustments of the culture conditions'8allow for more regular detection.
Specific regions of the chromosome can behighlighted: for instance in C banding'9 the centro-meres show up while in telomeric staining20 withsilver stains, the ends of the chromosomes arehighlighted. Beautiful photographs of chromo-somes are possible on scanning electron micro-scopy and minute fragments can be accuratelyidentified as chromosomal or otherwise.2'
In situ hybridization
Combining the techniques ofchromosome analysisand molecular genetics by in situ hybridization hasplayed an important role in studies about the alphaand beta globin loci22 and was also helpful inidentifying the site ofmale sex determinates on theX chromosome in XX males.23 As techniquesbecome more powerful and smaller and smaller
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

616 M. SUPER
stretches of DNA are amplified to measurableproportions, these techniques will become increas-ingly important in the future and will help greatly inchromosome analysis.
Such techniques are useful in determining thechromosomal origin of additional material on achromosome and carriers of small chromosometranslocations can be detected with greateraccuracy.
Chromosome nomenclature
An international agreement on chromosomenomenclature and description of defects exists.24The autosomes pairs are numbered according tosize, from I to 22, with the sex chromosomesmaking up the normal complement of 46. The longarm, q, and the short arm, p, are divided into largemapping regions and two further subdivisionsexist. Thus Xq27.3 denotes subregion 3 of sub-division 7 of major mapping region 2 on the longarm of the X chromosome, the site of the visibleabnormality of the fragile X syndrome - in fact FraXq27.3 describes it completely.Chromosome disorders are of number (aneu-
ploidy), or of structure, with inversions, transloca-tions both balanced and unbalanced, deletions,duplications and rings possible. They may arise byinheritance or mutation. The relationship of newmutations ofapparently balanced translocations tophenotypic expression is currently under review.Theoretically, ifthere has been no gain or loss in thetranslocation event then there should be nophenotypic effect. However, empiric observationshows a finite increase in mental handicap.25 Samp-ling bias is admitted26 and a multicentre study bythe Clinical Genetic Society is currently in progressand hopes to define the problem more accurately.A valuable textbook on chromosome disorders is
that by Schintzel,27 and the interested reader isreferred there for detailed clinical information onmost described chromosome abnormalities. Thewhole of a recent supplement of the AmericanJournal of Medical Genetics is devoted to Downsyndrome.29 An earlier monograph on Down's byLubs is interesting.28
Some specific recently described chromosomalsyndromes
Fragile X, Killian Pallister syndrome, Prader-Williand Angelman syndromes will be described ingreater detail.
The fragile X syndrome (Fra Xq27.3) The namederives from a visible constriction in the body ofthechromosome. 'Fragile' is a misnomer, for thechromosome very seldom breaks there. Thoughfragile sites are recognized on many
chromosomes,29 only fragile X is known to beassociated with clinical abnormality. The disorderis an important cause ofmental handicap in males,affecting 1 in 1000.30 About one third of carrierfemales are also mentally handicapped, thoughoften to a lesser extent.3' The condition may ariseby inheritance or new mutation - thought to beabout 60%.32 Affected boys especially have in-creased head circumference, delay in the onset ofspeech, disruptive behaviour in childhood andbecome very shy as adults when they are usuallygentle. True autism is not usually typical of fragileX. Macro-orchidism was an early described featureof the syndrome and is usually present in adult-hood. On the other hand it proved a poor markerfor the disorder in a study of males in mentalinstitutions.33 There is by now a very extensiveliterature on fragile X with whole issues of geneticsjournals devoted to it.34-36 Because of the specialfolic acid-poor culture conditions required todefine the fragile site, it is important to remember torequest the investigation specifically - it will usuallybe missed on standard culture. Folic acid therapyhas been attempted but found to be of no benefiteither to the degree of mental handicap orbehaviour.37'38 The actual fragile site is very closelylinked to the responsible gene in that families havebeen described with a number of affected maleswho show fragile sites, yet other males who arehandicapped without abnormal chromsomes andmales with the fragile site who are normal mentally.DNA analysis around the site has proved especiallydifficult because of the large amount of meioticcross-over activity in that region of the X.39 Thevery frequency of the disorder and high mutationrate are probably also reflections of the activity ofthe site. Definitive prenatal diagnosis of fragileX ispossible but it needs cordocentesis with examina-tion of fetal lymphocytes,40 since chorionic villusexamination seldom shows the site.
Killian Pallister mosaic4' This rare, thoughunderdiagnosed, cause of severe mental handicapoccurs on the basis of an isochromosome of theshort arm of chromosome 12 occurring at an earlystage of mitosis, giving rise to a mosaic situation,with the aneuploid cells containing, in effect,terasomy for 12p. The karyotype ofan affected boymay be described as 46XY/47XYil2p. The tetra-somic cells in lymphocytes are selected against, sothat even in the newborn the blood will be reportedas simply 46XY. Skin biopsy and fibroblast cultureare needed to demonstrate the mosaicism. Thephenotype includes high birth weight, a highanterior hairline with thin hair anteriorly, a thinupper lip with long frenulum and thick lower lip(Figure 1). Features become coarse with age. Thecondition has been described in a 38 year old man.42
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

MEDICAL GENETICS 617
Figure 1 Child with Killian-Pallister mosaic (Tetrasomy12p in fibroblast culture). Note high hairline with finetemporal hair, thin upper lip, full lower lip. There ismarked hypotonia and retardation. Permission has beenreceived from the parents for this photograph to bepublished.
Other chromosome mosaics One relatively com-mon somatic mosaic is trisomy 8 mosaic in whichmarfanoid body habitus may be associated withmental handicap and deep longitudinal creasing ofthe anterior sole.43 One should also suspectmosaicism when mental handicap is associatedwith asymmetry or patchy hypopigmentation ofthe skin." Sometimes the mosaic can be demon-strated in cultured lymphocytes but skin biopsyshould be done where suspicion remains highfollowing a normal karyotype report. Finding ofsomatic mosaicism allows for a definitive diagnosisand for very low recurrence risk figures to be givento parents, instead of an empiric intermediate oreven high figure with no diagnosis and the sus-picion of a genetic disorder.
Prader- Willi and Angelman 's syndromes Theseare possibly examples of imprinting.45 The samechromosome deletion, visible on good chromo-some cultures, e.g. 46XX del 15qll, has beendescribed in these two disorders with very littleoverlap in their clinical phenotype. In Prader-Willisyndrome the deletion is de novo and paternal inorigin, or the paternal contribution is missing' and
thus there is maternal imprinting, while in Angel-man's syndrome the opposite situation seems toapply.47 Prader-Willi syndrome is a mentally handi-capping disorder in which there is spectacularneonatal hypotonia with tube feeding needed atfirst too and later there is hypogenitalism andmarked truncal obesity.48Angelman's syndrome49 also shows hypotonia
but the disorder is characterized by marked mentalhandicap, jerky movements, which earned it theunfortunate title of the 'Happy Puppet' syndrome,tongue thrusting and a characteristically abnormalsleep electroencephalogram. Early in childhood thecondition may be difficult to tell from Rett syn-drome,50 a recently recognized condition of girlswho become markedly autistic and develop hand-wringing after a seemingly normal start to life. Thebasis of Rett syndome awaits elucidation.
Chromosome stress tests
Specific stress techniques may be employed in thestudy of certain disorders, particularly those ofDNA repair. These include exposure to irradiationin ataxia telangiectasia5' and to U-V light inCockayne syndrome,52 with an increase in breaksseen in both. Sister chromatid exchange shows anincrease in spontaneous activity in Bloom syn-drome53 and the technique has been used as amonitor of subtle chromosome damage fromenvironmental insult.54
Down syndrome
Down syndrome has been the subject of intensivestudy which has become more and more sophisti-cated as new analytical techniques have beenapplied. The whole of a recent supplement ofAmerican Journal ofMedical Genetics is devoted tothe disorder.28
Analysis of families in which partial transloca-tion had occurred and careful molecular mappinghas shown that the Down phenotype will occurwhen there is trisomy of band Xq22 and work isafoot to subdissect the bands still further.54'55Similarly, the pathogenesis of the mental deficiencyhas been studied.56 Prenatal and postnatal neuro-genesis and synaptogenesis, with significant reduc-tion in neurones and synapses and a quantitativedeficiency ofmyelin, have been described.57'58 Thereare significant quantitative alterations of a numberof neurotransmitters involving dopamine,serotonin and acetyl choline.59 Alzheimer's diseasechanges occur very early in the brain in Downsyndrome - 88.9% by the age 30 and 100% after50' show the amyloid plaques and fibrillary tang-les. The gene for Alzheimer's disease has beenlocated to chromosome 21 as has the gene for theprecursor amyloid protein.61
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

618 M. SUPER
Advances in molecular biology
Large tracts of DNA on the chromosomes consistof non-coding, often highly repetitive regions.Some ofthese may represent genes once active, nowtermed pseudogenes; others may act as spacers,perhaps playing a role in keeping the species apart.Active genes themselves consist of expressedregions or exons, and intervening sequences or
introns which are not translated.Abnormalities in the exons are far more likely to
result in disease, than in the introns, thoughabnormalities at intron-exon boundaries maysignificantly alter characteristics of the RNA byincreasing or decreasing the length of the exon.Alterations in the base pairs may alter the func-tional triplets or codons which code for the amino-acids of the final protein.Thus a single base change or point mutation may
have a profound effect if it affects a critical part of afunctional molecule, as in sickle cell haemoglobin,where valine is substituted for glutamic acidbecause of a substitution of adenine for thymine,CAC for CTC in the relevant triplet from codon6.62
Deletions or duplications may or may not alterthe normal triplet progression of the reading frame(depending simply on whether an exact multiple ofthree, counting from the reading end of the exon, isinvolved or not - when there is a frameshift, thenthere will generally be a more catastrophic effect onthe final protein).When a point mutation results in a prematurely
occurring stop codon then a truncated proteinresults, whilst a mutation may alter a normallyoccurring stop sequence and result in a longer thannormal protein, as in Haemoglobin ConstanceSpring.63 The textbooks by Harry Harris ThePrinciples of Biochemical Genetics' and by SirDavid Weatherall,65 The New Genetics and ClinicalPractice give very useful introductions to thegenetic code, its working and its relation to genes.Although the genetic code was cracked in 1953,66
it took a considerable length of time before thebenefits to medical science became evident. Manylaboratory technical advances combined to makethis possible. Most of these make use of thecomplementary nature of matching DNA strands,where guanine is always matched with cytosine orvice versa and thymine always matched withadenine. Restriction enzymes, generally derivedfrom micro-organisms, were discovered, capable ofcutting DNA at particular sites according to thebase pair composition into fragments of differingsize and charge.67'68 Southern's blotting technique69was at first one of the few reliable methods ofanalysis, where DNA digested by restrictionenzymes and separated by electrophoresis onagarose gel is blotted onto nitrocellulose paper or,
more recently, onto charged nylon membranes70and then incubated with radio-active probes com-prising a stretch of (human) DNA grown up in amicro-organism, often phage or lambda. TheDNAprobe on incubation anneals to DNAs ifpresent onthe blot which contains the partnering complement-ary strand. This technique has many applications,including testing for the presence of a particularDNA fragment in somatic cell hybrids of mouseand human cells. Such hybrids shed humanchromosomes during each passage and the tech-nique has been very valuable in the mapping ofgenes to particular chromosomes.7' DNA digestionby restriction enzymes has allowed discovery of agreat number of polymorphisms, i.e. normaldiffering forms which help to differentiate DNAfrom homologous chromosomes in regions ofinterest from one another - restriction fragmentlength polymorphisms (RFLP). Polymorphismsare necessary in mapping studies and in the track-ing of disease genes within families.Methods of obtaining very long fragments of
DNA by a combination of the use of 'rare cutters',restriction enzymes for seldom encountered DNAsequences, combined with pulsed field gel electro-phoresis (making DNA travel on a gel in whichdifferent current vectors are being applied),72'73have proved of value in narrowing down searchesby excluding or including large tracts ofDNA at atime.
Reliable methods of DNA extraction from cel-lular material have been developed74 with theproduct capable of long-term storage at - 70°Cand with such DNA suitable for most experiments.Methods of RNA extraction require very freshtissues before study by 'Northern' blotting75 andcertain laboratories have more technical successthan others.An important development in genetic analysis of
DNA and RNA has been the introduction of thepolymerase chain reaction (PCR),76'77 where primersequences developed from complementary strandsof DNA flanking a DNA region of interest areincubated with a sample for study. If the interven-ing sequences are present in the sample, then, underthe influence of an enzyme capable of existing atvery high temperatures - Taq polymerase (derivedfrom the organism Thermus aquaticus), theintervening sequence is made good from basesadded to the mixture and in a series of separation,polymerizing and annealing steps at differingtemperatures, great amplification of the DNAtakes place. The technique dispenses with the needfor radio-activity because of the much greaterquantities and specificity of the end product. Amodification of PCR is artificial restriction muta-tion system (ARMS), where errors are built intoone of the primers, allowing development of apositive-negative system of analysis. The technique
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from
MEDICAL GENETICS 619
has been used successfully in studies of alpha-I -antitrypsin,78 cystic fibrosis79 and haemoglobin-opathies.80
Tiny samples are capable of analysis by PCRmethods, including blood from Guthrie spots8' andsingle blastomeres following in vitro fertilization.82There has been limited success in attempting todetect DNA from fetal cells in the maternal circula-tion, by searching for the paternal contribution.83
Incorporation ofhuman chromosomes into yeast,so called 'YAC' clones (yeast artificial chromo-somes)84 are likely to prove of great use in genelocalizing experiments, being far less laboriousthan maintenance of somatic cell hybrids.
Tracts of DNA can be sequenced according tothe order of occurrence of the bases adenosine,cytosine, guanine, thymine in vertical electro-phoresis.85 For some smaller genes with differentabnormalities in different families being responsi-ble for the disease state, direct sequencing may bethe analytical method of choice - this applies forexample to factor IX abnormalities.86 Ways ofincorporating normal or diseased genes into viralvectors and thence into human tissues, either inculture or in vivo will allow more detailed study ofpathophysiology and will also presage gene treat-ment.87Mapping of the human genome is thought to be
so worthwhile that there are now major NorthAmerican and European initiatives. McKusick'sinvaluable catalogue of mendelian inheritance88 isregularly updated and contains information on theknown locations of human genes, either as C(confirmed), P (provisional) or L (limbo). Anup-to-date human gene map is also regularlypublished in the Proceedings of the NationalAcademy of Sciences.89
Specific single gene disorders
The principles of DNA research and analysis byreverse genetics can best be understood by adetailed summary of the highlights of research inDuchenne and Becker's muscular dystrophies andin cystic fibrosis. In both of these the normal genesimpaired in the disease states have now beendefined. Readers are referred to Weatherall65 for adescription of classical genetic analysis applicablefor example to the haemoglobinopathies and wherethe molecular configuration of the DNA wasderived from a knowledge of the amino-acidscomprising the globin chains.
Duchenne and Becker's muscular dystrophies(DMD and BMD)
Despite the 'head start' which the X-linkeddisorders enjoy over the autosomal disorders in
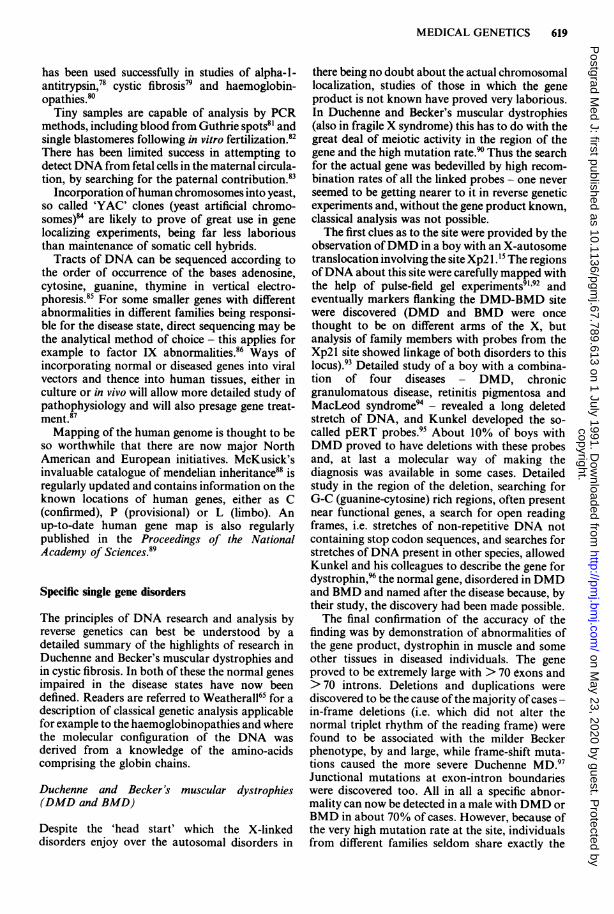
there being no doubt about the actual chromosomallocalization, studies of those in which the geneproduct is not known have proved very laborious.In Duchenne and Becker's muscular dystrophies(also in fragile X syndrome) this has to do with thegreat deal of meiotic activity in the region of thegene and the high mutation rate.?' Thus the searchfor the actual gene was bedevilled by high recom-bination rates of all the linked probes - one neverseemed to be getting nearer to it in reverse geneticexperiments and, without the gene product known,classical analysis was not possible.The first clues as to the site were provided by the
observation ofDMD in a boy with an X-autosometranslocation involving the site Xp2l .15 The regionsofDNA about this site were carefully mapped withthe help of pulse-field gel experiments9l'92 andeventually markers flanking the DMD-BMD sitewere discovered (DMD and BMD were oncethought to be on different arms of the X, butanalysis of family members with probes from theXp2l site showed linkage of both disorders to thislocus).93 Detailed study of a boy with a combina-tion of four diseases - DMD, chronicgranulomatous disease, retinitis pigmentosa andMacLeod syndrome94 - revealed a long deletedstretch of DNA, and Kunkel developed the so-called pERT probes.95 About 10% of boys withDMD proved to have deletions with these probesand, at last a molecular way of making thediagnosis was available in some cases. Detailedstudy in the region of the deletion, searching forG-C (guanine-cytosine) rich regions, often presentnear functional genes, a search for open readingframes, i.e. stretches of non-repetitive DNA notcontaining stop codon sequences, and searches forstretches of DNA present in other species, allowedKunkel and his colleagues to describe the gene fordystrophin,96 the normal gene, disordered in DMDand BMD and named after the disease because, bytheir study, the discovery had been made possible.The final confirmation of the accuracy of the
finding was by demonstration of abnormalities ofthe gene product, dystrophin in muscle and someother tissues in diseased individuals. The geneproved to be extremely large with > 70 exons and> 70 introns. Deletions and duplications werediscovered to be the cause of the majority ofcases -in-frame deletions (i.e. which did not alter thenormal triplet rhythm of the reading frame) werefound to be associated with the milder Beckerphenotype, by and large, while frame-shift muta-tions caused the more severe Duchenne MD.97Junctional mutations at exon-intron boundarieswere discovered too. All in all a specific abnor-mality can now be detected in a male with DMD orBMD in about 70% of cases. However, because ofthe very high mutation rate at the site, individualsfrom different families seldom share exactly the
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

620 M. SUPER
same mutation or deletion.Analysis of some potential female carriers has
proved difficult. It may be easy to classify a femaleat risk as being a carrier, on the basis of a familystory with a significantly raised creatine kinase(with the tests done in a laboratory with its ownbank ofnormal results for females). However, only70% of obligatory carriers have a raised creatinekinase.98 DNA based experiments which give asingle band may indicate that the DNA from bothX chromosomes is giving the same pattern (and thewoman is not a carrier), or may in fact be giving thesignal from one chromosome only, with a deletionfor the probe on the other. Assessing one dose ortwo from the heaviness of the band is subject toexperimental or reader error. Figure 2 provides agood example of the practical difficulties. It isdifficult to know whether the mother has both Xchromosomes giving the pattern or whether thesignal is only coming from one, The apparent'non-maternity' in her daughter provides the an-swer. This is because her mother is deleted withinthe dystrophin locus ofone ofherX chromosomes.The pattern which the daughter shows must bepaternally derived, since her mother does not havethis polymorphism at all. The daughter's male fetuswas found to show the deletion like her brother and
she opted for termination. Creatine kinase in thesame family some years earlier had been seriouslymisleading, suggesting a 5% carrier risk.
Very recently, by using a number of overlappingRNA probes for the dystrophin molecule, there hasbeen success in telling female relatives of indivi-duals with deletions apart from one another interms of carrier status.99
Staining of muscle biopsy tissue with antibodiesto the dystrophin molecule has application inanalysis of such tissues and may even be applicableto fetal muscle biopsy tissue in the 30% of familieswhere no molecular abnormality has been dis-covered."°°RNA for dystrophin has recently been success-
fully incorporated into the extensor digitorumbrevis muscle of an individual with DMD.101 Thiswas followed by an increase in the strength of themuscle and dystrophin could be demonstrated inthe muscle after biopsy. Hopefully, this successfulexperiment will be followed by others on largermuscles, and a definitive treatment.
Cysticfibrosis
Siblings of people with CF, having been shown tobe free of CF by standard sweat test, have a 2 in 3
Deleted
Figure 2 The female I12 shows apparent 'non-maternity,' i.e. she has not inherited the I allele from her mother.Therefore her mother and she must be deleted for what she has inherited and passed on to her male fetus. Therefore thefetus is affected.
Results of Southern blot analysis with intragenic probe from dystrophin locus.
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

MEDICAL GENETICS 621
chance of being carriers, while siblings of theparents have a risk slightly greater than 1 in 2 (thistakes account of the 50:50 chance of havinginherited carrier status from the one grandparentof the CF individual and the 1 in 25 chance that theother grandparent is a carrier too.) Spouses ofEuropean origin. without a family history, have a 1in 25 chance and thus odds for family members oftheir having affected offspring can be calculated(Table I).For a long time these odds were all that one
could offer in genetic counselling and there was noaccurate prenatal test. An early marker for the CFgene, cystic fibrosis antigen,'02 present in the serumof most people with CF and most of their obligatecarrier parents, allowed a recalculation with moreaccurate carrier odds possible.'03 The technique ofthe test based on iso-electric focusing of serumproved technically difficult and subject to observerbias and thus was never introduced on a wide scale.
In 1982, Jalanko discovered reduced microvillarenzymes in the amniotic fluid in pregnancies inwhich the fetus was trisomicl"4 and an extension ofthis work showed similar findings when the fetushad CF. Brock developed a microvillar enzyme testbased on residual alkaline phosphatase (afterinhibition by amino-acids), gammaglutamyl trans-peptidase (GGT) and aminopeptidase M inamniotic fluid taken at 18 weeks.'05 This work didprove reproducible. However, error rates in bothdirections were found. Thus a diagnosis of CF inthe fetus had a chance of being incorrect andreassurance offreedom from CF sometimes provedfalse. For a couple at a 1 in 4 risk of havingoffspring with CF, false positive error rates of 8%were quoted, with a 5% false negative rate.'06 Forcouples at a much lower prior risk of having CFoffspring, e.g. siblings of CF subjects or of theirparents, the prediction would be wrong more oftenthan correct when an affected fetus was forecast.Negative tests, with the low prior carrier odds didallow further reassurance. The risk of becominginvolved in a situation of wishing to ignore apositive test, because ofits chances ofbeing wrong,reduced the demand for tests in people at low priorrisk. Even those at a high (1 in 4) risk were worried,
Table I Risk of having CF offspring where spouse hasno family history of CF
Risk
No family story in either parent I in 2500Same but first cousin marriage I in 800Sibling has child with CF I in 200Sibling has CF 1 in 150Divorced parent ofCF child -remarried I in 100Woman has CF I in 50
firstly, by the chances of a wrong prediction and,secondly, by the need for the amniocentesis to beperformed well into the second trimester. Thusmany such couples took decisions not to add to thefamily. Some ofthem felt it worthwhile to wait for amore accurate test which could be applied earlier inthe pregnancy.
In 1985, Eiberg found linkage between a poly-morphic enzyme, paraoxinase, and CF by studyingnuclear families with more than one child withCF.'07 Whatever paraoxinase polymorphism wasfound in one child was very likely to be repeated inthe other. Thus a lod score (logarithm of the odds)in excess of 4 of linkage between paraoxinase andCF became possible, i.e. odds of 10,000 to 1 thatthey were linked. From the number of affectedsibling pairs showing differing polymorphisms,indicative of meiotic crossover between paraox-inase and CF in one or other parent, a recombina-tion fraction, or theta, of 10% was calculated (i.e.the crossover 'distance' between the two markers is10 centiMorgans). At this stage there was no idea ofwhere the gene for paraoxinase was. A negativegene map for CF had been constructed fromstudies of families with more than one CF childwith a host of polymorphic markers.'08 Lap CheeTsui, using information from the negative genemap, found linkage between paraoxinase and ananonymous DNA marker, DOCRI-917,19 whichproved to be 5 centiMorgans from paraoxinase and15 centiMorgans from CF. In a series of somaticcell mouse-human experiments his team rapidlyshowed that DOCR-917 was only present whenhuman chromosome 7 was present in the culture."0Research workers could then simply 'go to thefridge' to find other chromosome 7 markers. Twoof these, discovered about 1 year earlier, proved tobe extremely close to CF when tested in the familieswith more than 1 CF child. These were the Metoncogene"' and an anonymous probe pJ3.11.'12Distances of about 1.5 centiMorgans were quotedon the basis of 15 meiotic crossovers in 1000chromosomes analysed.
In fact, when the study group was reinvestigated,the CF diagnosis proved wrong in a number andnew distances of 0.3 cM between pJ3. 11 and CF,and 0.4 cM between Met and CF were calculated.Virtually overnight a very accurate prenatal testhad become available, with very low error rates,considered acceptable both by couples taking thetests up and by those offering them. The test wasavailable on chorionic material and thus at 9 weeks.The first tests were described in early 1986. '1'1314Between 1986 and 1990, a United Kingdom surveyof prenatal diagnosis in CF showed 398 womenwho had undergone the test."5 Results of affecteds,carriers and those with no CF genes were found toobey the rules of mendelian recessive segregation.Accurate carrier detection tests became available
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

622 M. SUPER
immediately for the healthy siblings. Interestingly,an analysis of findings in many laboratories world-wide showed that males found to be carriers were
more often found to have inherited their carrierstatus from their fathers - thought to be an instanceof meiotic drive and possibly linked to theheterozygote advantage thought to account for CFbeing so common.'"6
For prenatal tests to be applicable in a particularfamily one needed to be able to tell the polymor-phisms of the linked probes apart in the parentsand which each had passed on to the affectedperson. Since Met and pJ3.11 are normal poly-morphic probes simply linked to CF, of course
analysing them in a family in which CF had neveroccurred would not help in the slightest in predict-ing whether CF was likely to happen. The polymor-phisms can track the CF gene in a family in which itis known to be occurring. One still had the problemin families then of not being able to tell whether thespouse marrying into a family with CF was a
carrier.Studies employing pulse-field gel electrophoresis
suggested that Met and pJ3.11 were flanking theCF gene, with a probable distance of 1.5 Mega-bases between the two."7 The search for the gene
between these two sites threw up a candidate geneCS7.1"8 Although the claim to have found the gene
proved premature, strong linkage disequilibriumwas found betwen CF and CS7, and between thedisease locus and two nearby probes XV2c andKml9."9 Thus a particular polymorphism or re-
striction fragment size was found far more oftenwith the CF bearing chromosome of the parentthan with non-CF chromosome. Application ofinformation using linkage disequilibrium proved ofsome value in increasing or decreasing the chancesof there being a CF gene nearby in family testswhere the child with CF had died, in the cases ofspouses marrying into families with CF and in thetesting of sperm donor panels where one couldselect a favourable haplotype in the face of a CFfamily history. Carrier odds of 1 in 4 could be givento a member ofthe general public in Britain with arunfavourable pattern on both chromosomes versusodds of 1 in 250 with favourable patterns on
both."9Interestingly, when eventually the CF gene was
discovered, the majority of CF chromosomesshowing the commonest mutation were found toshow the unfavourable XV2c, Kml9 haplotype,with the next commonest mutations also showingthis haplotype.
Uniparental disomy in cysticfibrosis
Molecular analysis has allowed analysis of twochildren with cystic fibrosis and disproportionate
short stature. 120-121 In both, analysis proved pater-nity, yet showed that there was a double represent-ation ofone ofthe maternal chromsome 7s, with nopaternal contribution for this chromosome. Thisintriguing example of an imprinting effect mustcause us to wonder how many unexplained unusualpresentations of common diseases may be causedby the phenomenon. At last we have the tools to beable to realize the existence of so unexpected afinding and to search for it.
Discovery ofthe cysticfibrosis gene, CFTR
In September 1989 a series of three brilliant articlesdescribed the CF gene,'23-125 termed cystic fibrosistransmembrane conductance regulator (CFTR).By a process of jumping over stretches of DNAsituated between Met and pJ3. 11 which gavetechnical difficulty in cloning experiments in thelaboratory, a stretch was discovered rich in G-Cfragments, with open reading frames and present inmany different species. By the chemical composi-tion ofthe protein which could be deduced from theDNA sequences of the exons, a protein with twonucleotide binding folds, thought capable of bind-ing ATP and a highly charged R domain, could bepredicted and hydropathy plots of the proteinshowed these regions to be hydrophilic (and intra-cytoplasmic) as opposed to the hydrophobic mem-brane portion of the protein. A deletion at position508 of the 1480 amino-acid CFTR was discoveredwith an 'in-frame' three base-pairs AAG missing,resulting in a missing phenylalanine, thus DeltaF508, in the first nucleotide binding fold and inexon 10 of the DNA in the gene. The majority ofsubjects showing this mutation also were found tobe pancreatic insufficient (about 10% of patientswith CF have normal pancreatic functions and aretermed sufficient). In fact, while this finding de-scribed in the original articles remains substantiallytrue, clinical variability and CF cannot be simplyexplained on DNA findings.125An international CF genetic analysis consortium
has been set up and is a wonderful example of howrapid progress can be when there is free exchange.A map of the Delta F508 gene in Europe has beendrawn,'26 showing an increase in incidence fromsouth east to north west and with the highestproportion described in Denmark.
In the UK, a Delta F508 incidence of 80% incarriers has been described.'27 More than 60 furthermutations have been found. One, G55 1 D, accountsfor about 5% ofCF genes in people of Celtic originand is common in the West of Britain and in Eire(glycine substituted for by aspartic acid at position551 - a point mutation). Deletions, point muta-tions, 'nonsense' mutations, with a stop codon
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

MEDICAL GENETICS 623
occurring prematurely, frame-shift mutations andmutations at intron-exon boundaries have beendescribed. 128-133Twelve separate mutations have been found in
Britain and these account for more than 92% ofCFchromosomes. Thus the carrier risk for someonewithout a family story of CF, negative for all 12would be about 1 in 300 instead of 1 in 25. Odds likethis make general carrier screening seem attractive,especially since those positive on testing are estab-lished as definite carriers. Two people from thegeneral population, both negative on testing,would have a 1/300 x 1/300 x 1/4 or a 1/360,000chance of having offspring with CF and even anestablished carrier with someone negative for all 12would only have a 1/1200 chance of affectedoffspring.'34 More importantly, a good carrierdetection test exists now for people marrying afamily where CF has occurred and for sperm or
oocyte donor situations.The CFTR has been shown to share characteris-
tics with P-glycoproteins of multiple drug resist-ance and also to share similarities with a number ofbacterial wall transport systems.'23 These havehelped to derive hypotheses for the function of theprotein. From its form it is likely to allow move-ment in only one direction, either into or out of thecell'35 and thus CFTR cannot itself be the chloridechannel, since these channels allow bi-directionalmovement. Even if it is a secondary phenomenon,some blockage ofchloride movement does occur inCF and manipulation of this, or of CFTR itself,could ameliorate conditions in the lung withclinical improvement. Amiloride has been used inthis way'36 and is the subject now of a multicentrestudy in North America.The final step in establishing that CFTR is the
gene disordered in CF is contained in theexperiments of Rich'39 and of Gregory'40 who havecorrected the biochemical defect of CF tissues inculture by incorporating the normal gene.Experiments are afoot to incorporate the CFmRNA into modified adenovirus'39 or adeno-associated virus,'14 hopefully capable of safeadministration by nebulizer on an intermittentbasis, with a proportion oflung cells being returnedto normal function. To make a significant (genetic)disorder something minor, as has been achieved insome bacterial infections, is an exciting but notimpossible dream. Most people believe that geneticcounselling, detection of those at risk, and termina-tion ofaffected pregnancies, will continue to have asignificant place in medical practice in CF for sometime to come, to express a more sober view.With more than 92% of CF genes now identi-
fiable, testing can be very useful in confirming a CFdiagnosis or in casting doubt where the subjectproves negative on testing for all the discoveredmutations.
Other genetic disorders
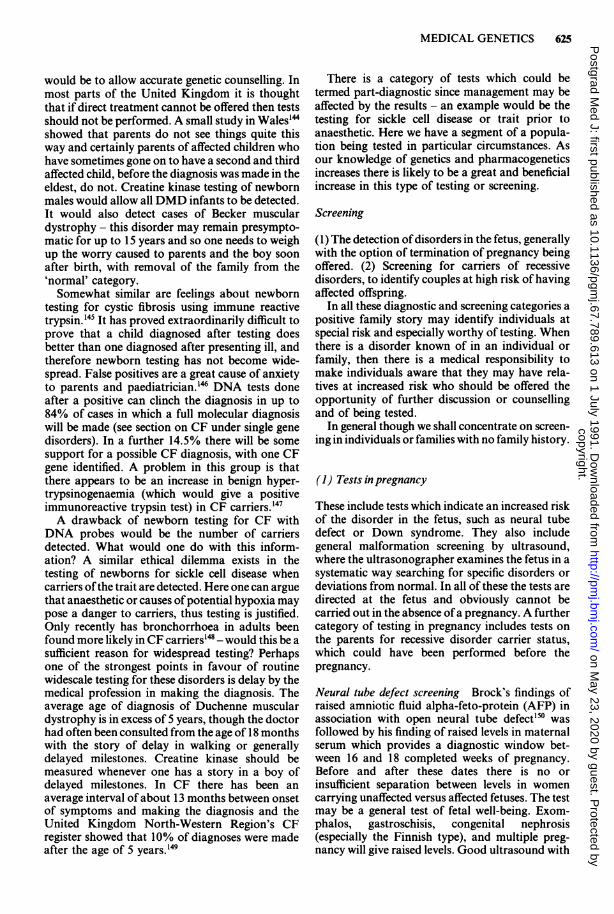
The genes for many of the known proteins orenzymes have been fully identified. The loci ofmany others have been derived from family studies.An ideogram gene map is shown in Figure 3 withthe established gene placements of some of thebetter known genetic disorders. Applications ofDNA technology to their study within familiesdepend on the particular disorder and the accuracyof any predictive testing.
Screening and diagnostic 'screening' for geneticdisease
A differentiation between screening and diagnostictests is made, according to Wald and Cuckle'susage of the terms.'4' They define screening as theidentification in apparently healthy individuals ofthose who are sufficiently at risk of a specificdisorder to justify a subsequent diagnostic test orprocedure, or direct preventative action. Theyreserve the term diagnostic for those tests whichwould be followed by a therapeutic intervention.Wald and Cuckle outline a checklist of29 questionsapplicable to screening and diagnostic tests. Tothese must be added an adequate general knowledgeofthe disorder tested for in the individual and in themedical and involved paramedical professions, i.e.there needs to be an adequate level of publicawareness before any widespread tests are applied.We can divide such tests into three categories,
one diagnostic and two screening.
Diagnostic
Tests for phenylketonuria in the newborn haveallowed countless thousands of people to achieve anormal range of intelligence on diets low inphenylalanine. In some centres other, rarer, inbornerrors of metabolism are tested for automaticallysince they are detected by the paper chromato-graphy test used. Nowadays, as part of 'Smack'tests, many adults have tests for hypercholesterol-aemia. Diet and cholesterol lowering agents candelay the onset of coronary heart disease. One in500 have the gene for Type 2 hypercholesterol-aemia, an autosomal dominant. The responsiblegene is on chromosome 19 and DNA markers canalso be used in preclinical diagnosis.'42"143
There is a group of genetic disorders in whichdiagnostic tests in infancy would provide a pre-clinical diagnosis but where the case for improvedmanagement of the child, based on the diagnosis isnot made. Included here is Duchenne musculardystrophy - making the diagnosis would notimprove management or prognosis and thus theonly rationale for testing of all newborn males
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

624 M. SUPER
.}a, . ..
jeOO
.I . ;
t
k' it
m. :-
CL
ra5LCL#.
as
an s.z
I IIt
a_ ! a
.*F q
Li.t'1.. lib,e
IC W
Za
*L W7
ffi 4
an 'a
ra
aL a scgOg
EL
w l ~~~~~~tvItAuj 02 .1 1`0 0 fi
,,
C)
0Le
00r-
220C)
ua)20
C4
._
C.
CX
Co00
et
CoDC(A
a a
IIiia p
- _
C Vr
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from
MEDICAL GENETICS 625
would be to allow accurate genetic counselling. Inmost parts of the United Kingdom it is thoughtthat if direct treatment cannot be offered then testsshould not be performed. A small study in Wales'"showed that parents do not see things quite thisway and certainly parents of affected children whohave sometimes gone on to have a second and thirdaffected child, before the diagnosis was made in theeldest, do not. Creatine kinase testing of newbornmales would allow all DMD infants to be detected.It would also detect cases of Becker musculardystrophy - this disorder may remain presympto-matic for up to 15 years and so one needs to weighup the worry caused to parents and the boy soonafter birth, with removal of the family from the'normal' category.Somewhat similar are feelings about newborn
testing for cystic fibrosis using immune reactivetrypsin. 145 It has proved extraordinarily difficult toprove that a child diagnosed after testing doesbetter than one diagnosed after presenting ill, andtherefore newborn testing has not become wide-spread. False positives are a great cause of anxietyto parents and paediatrician.'46 DNA tests doneafter a positive can clinch the diagnosis in up to84% of cases in which a full molecular diagnosiswill be made (see section on CF under single genedisorders). In a further 14.5% there will be somesupport for a possible CF diagnosis, with one CFgene identified. A problem in this group is thatthere appears to be an increase in benign hyper-trypsinogenaemia (which would give a positiveimmunoreactive trypsin test) in CF carriers.'47A drawback of newborn testing for CF with
DNA probes would be the number of carriersdetected. What would one do with this inform-ation? A similar ethical dilemma exists in thetesting of newborns for sickle cell disease whencarriers ofthe trait are detected. Here one can arguethat anaesthetic or causes of potential hypoxia maypose a danger to carriers, thus testing is justified.Only recently has bronchorrhoea in adults beenfound more likely in CF carriers'48 - would this be asufficient reason for widespread testing? Perhapsone of the strongest points in favour of routinewidescale testing for these disorders is delay by themedical profession in making the diagnosis. Theaverage age of diagnosis of Duchenne musculardystrophy is in excess of 5 years, though the doctorhad often been consulted from the age of 18 monthswith the story of delay in walking or generallydelayed milestones. Creatine kinase should bemeasured whenever one has a story in a boy ofdelayed milestones. In CF there has been anaverage interval of about 13 months between onsetof symptoms and making the diagnosis and theUnited Kingdom North-Western Region's CFregister showed that 10% of diagnoses were madeafter the age of 5 years. "'
There is a category of tests which could betermed part-diagnostic since management may beaffected by the results - an example would be thetesting for sickle cell disease or trait prior toanaesthetic. Here we have a segment of a popula-tion being tested in particular circumstances. Asour knowledge of genetics and pharmacogeneticsincreases there is likely to be a great and beneficialincrease in this type of testing or screening.
Screening
(1) The detection ofdisorders in the fetus, generallywith the option of termination of pregnancy beingoffered. (2) Screening for carriers of recessivedisorders, to identify couples at high risk of havingaffected offspring.
In all these diagnostic and screening categories apositive family story may identify individuals atspecial risk and especially worthy of testing. Whenthere is a disorder known of in an individual orfamily, then there is a medical responsibility tomake individuals aware that they may have rela-tives at increased risk who should be offered theopportunity of further discussion or counsellingand of being tested.
In general though we shall concentrate on screen-ing in individuals or families with no family history.
(1) Tests in pregnancy
These include tests which indicate an increased riskof the disorder in the fetus, such as neural tubedefect or Down syndrome. They also includegeneral malformation screening by ultrasound,where the ultrasonographer examines the fetus in asystematic way searching for specific disorders ordeviations from normal. In all of these the tests aredirected at the fetus and obviously cannot becarried out in the absence ofa pregnancy. A furthercategory of testing in pregnancy includes tests onthe parents for recessive disorder carrier status,which could have been performed before thepregnancy.
Neural tube defect screening Brock's findings ofraised amniotic fluid alpha-feto-protein (AFP) inassociation with open neural tube defect'50 wasfollowed by his finding of raised levels in maternalserum which provides a diagnostic window bet-ween 16 and 18 completed weeks of pregnancy.Before and after these dates there is no orinsufficient separation between levels in womencarrying unaffected versus affected fetuses. The testmay be a general test of fetal well-being. Exom-phalos, gastroschisis, congenital nephrosis(especially the Finnish type), and multiple preg-nancy will give raised levels. Good ultrasound with
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

626 M. SUPER
real time was introduced on a wide scale in the 80sand the test has proved a very valuable adjunct toserum AFP screening. False reassurance in in-stances where ultrasound alone has been used asthe screening tool,'5' lead most centres to wish torely on both tests used together. The finding of araised serum AFP between 16 and 18 weeks ofpregnancy gives odds of about 1 in 8 that there willbe an open neural tube defect. Amniocentesis andAFP measurement in the amniotic fluid will giveodds of 20:1 in favour of the fetus having thedefect. The finding of a band for acetyl-cholinesterasel52 in amniotic fluid in someone inwhom there was a raised serum AFP and raisedamniotic AFP gives odds of 250:1 of an openneural tube defect in a region where there is a highbackground incidence of neural tube defect.'53Where open neural tube defect has been de-
tected, genetic counselling will need to include anexplanation of the likely severity at birth. Manycouples opt to end the pregnancy. The odds of arecurrence in a future pregnancy can be reduced byadministration of periconceptual Pregnavite forteF, a multivitamin preparation,'54 though puristsargue that the cause and beneficial effect is notproven.
Screening for specific disorders may have usefulspin-off. Mentioned above is detection of gastro-schisis or infantile kidney disease following on AFPscreening. Absence of the normal cholinesteraseband in amniotic fluid may allow detection ofatypical cholinesterase in the mother for whomsuccinyl choline, as given during anaesthetic,would pose dangers.'55 Cholinesterase in amnioticfluid is of maternal origin, while acetyl-cholinesterase is fetal in origin.
Screening for Down syndrome A further spin-offof AFP screening was the observation that mostwomen carrying a fetus who turned out to haveDown syndrome had had lower than normal serumAFP levels at 16- 18 weeks.'56 It seems that the fetalliver, the origin of AFP, matures late in Downsyndrome. Screening by using a combination ofmaternal age, serum AFP and serum HCG (humanchorionic gonadotrophin, often raised in thepresence of Down syndrome) allows recalculationof the odds ofhaving an affected fetus - thus, ifoneallows for 5% of women to have amniocentesisthen using specific cut-off points for serum AFPand HCG one can give odds greater or less than 1 in250 of having an affected fetus, with amnio-centesis,'57 the definitive test offered to those athigher risk. Sixty per cent of fetuses affected byDown syndrome could be detected in this way.Because the tests are independent of one another,risk figures derived for each of age, AFP and HCGare additive and more accurate than any of themalone.
The search continues for other tests which couldresult in an even higher pick-up rate and higherspecificity, allowing fewer amniocenteses. Testssuch as maternal serum oestriol (lowered in thepresence of Down syndrome) and reduced fetalfemur length could further refine the odds but addconsiderably to problems of organization andco-ordination.
All of these tests could be replaced if a reliablemethod of detecting trisomic fetal cells in maternalblood were to be developed by an advance inpolymerase chain reaction, especially were reliablemethods to measure gene dosage to be discovered.Down's screening is not generally available in theUnited Kingdom on the NHS but the tests arebeing offered increasingly on a payment basis.
Ultrasound screening Many ultrasound special-ists now screen each fetus at least twice: once, as ameasure of the length of gestation, at about 12weeks, an adjunct to serum AFP screening, and asecond time at about 18 weeks when specificanatomical details are studied carefully, especiallythe central nervous system, spine, bladder andkidneys, diaphragms and four-chamber view of theheart. Normal findings provide for reassurance andreduce greatly the chances of a significant malfor-mation.'52 However, false positive diagnosis offetalabnormality is possible and so is false reassurance.The normal fetal cerebral ventricles and the fetalurinary collecting systems can contain generousamounts of fluid resulting in wrong diagnosis ofhydrocephalus or of hydronephrosis. Sometimespathological alteration may not yet be evident inthe second trimester - an example is autosomalrecessive microcephaly, when even specific searchesin the face of a family story are unable to provideregular reassurance; in hypoplastic left heart synd-rome, the hypoplastic process may start later thanthe scan date. With adequate counselling, thebenefits of routine ultrasound scanning of everyfetus should far outweigh the disadvantages ofoccasional wrong diagnosis. Spin-off includesearly diagnosis of multiple pregnancy and accuratepositioning of the placenta. New technology, in-cluding Doppler studies of placental blood flow,will bring new advantages. Those who talk againstscreening, stressing the mental harm which mayresult, should keep in mind the enormous increasein our knowledge which has followed from screen-ing tests. 'If you don't look you can't find.'
(2) Carrier screening tests
Two carrier screening programmes, widely re-garded as successful, involve Tay-Sachs disease inthe United States and Canada'58 and thalassaemiain Sardinia and Cyprus.'59"'60 In each instance there
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

MEDICAL GENETICS 627
was an intensive education programme beforescreening started. Many couples and individualswere screened after publicity campaigns, attendanton the initial introduction of tests. Thereafternumbers tested fell off rather so that a recentpublication on Tay-Sachs carrier screening inToronto found that most people screened camefrom a population of pregnant Jewish women andtheir spouses.'6' Thus, although pre-pregnancy,even pre-marriage screening is available, it ispregnancy which may concentrate the mind. Acertain amount of premarital screening does occurat the request of orthodox Rabbis who see mar-riages arranged to avoid the risk of Tay-Sachsentirely as an infinitely better option than fetaltesting and termination of pregnancy. Otherreligious groups where arranged marriage is com-mon could see things in the same light.
Carrier testing is likely to become much morecommon and will include more than one disorder,thus helping to remove the stigma ofbeing found tobe a carrier. Studies demonstrating the great in-crease in autosomal recessive disorders, mentalhandicap and congenital malformations in theproducts of incest indicate that we all must carryfour or five recessive genes capable of resulting insignificant disease if our offspring inherits one ofthem from us and also from our partner whohappens to have that one too. Children born as aresult of incest are homozygous for at least onequarter of their genes; products of uncle-niece ordouble first cousin marriages are homozygous for 1in 8 genes and first cousins for 1 in 16. This fractionis termed the coefficient of inbreeding.Once an individual had taken a decision to wish
to be screened, he or she would naturally beinterested if carrier status for other potentiallyunpleasant disorders could be carried out on thesame test specimen;. diagnostic testing, for exam-ple, for hypercholesterolaemia or alpha 1 antitryp-sin status could also be undertaken on the sample.Examples of disorders where there could be greatinterest in carrier detection screening programmescould be muscular dystrophy, cystic fibrosis, fragileX syndrome in females and severe forms of spinalmuscular atrophy.The debate on exactly when to introduce popula-
tion screening for CF is well advanced. Ten Kate'62has argued that one needs to be able to leave acouple with as low a risk as when they opted to bescreened, except for those in whom you find bothpartners carriers. Thus, he suggests that one waituntil 96% ofCF genes have been detected, when aproven carrier would only have a 1 in 2000 risk ofhaving a child with CF if the partner is negative onall tests (this would imply testing for about 12mutations). We have argued that where back-upfacilities to educate and support families exist oneneed not wait quite that long'63 and feel that with
92% of mutations identified in our population wecan get ready to introduce screening.
Ethics and genetics
Though there are deep personal differences aboutthe acceptability of prenatal diagnosis leading totermination of pregnancy, such matters are ones ofpersonal preference and opinion, rather than ofethics when one is dealing with termination follow-ing the diagnosis of a severe disabling disorder inthe embryo or fetus."M The ethical issues surroundthe accuracy of advice given and the safety ofuntried prenatal diagnostic techniques for themother and the unborn. We are dealing with aproblem of degree in acceptibility by couples,medical practitioners and society. It is the latterwhich makes the loudest disapproving noises, oftenwishing to impose a viewpoint on the individual.Allowing a child to die untreated may break thelaw. Under French law a termination of pregnancyis permitted right up until full-term whensignificant disability is certain; in Britain suchtermination is legal up to 24 weeks and some see ahypocrisy in this differentiation. Terminationbefore 12 weeks is more acceptable to couple andpractitioner and is safer for the mother than givingbirth at full-term. Diagnosing a diseased zygote inthe test tube with selective re-implantation is leastunattractive but also the least available method ofprenatal diagnosis.How does one gauge whether a medical geneti-
cist is doing his or her work well? Clarke has writtenwarning those who would wish to see successmeasured in financial terms by the savings forsociety in terminations ofpregnancies where disab-ling disability was forecast.'65The recommendations of the Warnock enquiry
in respect of experimentation which may be under-taken on the embryo up to 14 days after fertiliza-tion in vitro has become law. Experiments on genesand how they may work in this 14 day period maybring great benefit to mankind. The ethical prob-lem is that the research does not benefit thatparticular early potential human being. It has beenlegislated that a genetic engineering experiment,such as the introduction of a normal gene into theearly embryo before re-implantation, is not to bepermitted. This would alter the basic genetic make-up ofthe individual and alter the genes passed on inprocreation. Creation of a chimeric population ofcells by introducing dystrophin into muscle orCFTR into lung cells is not seen as being unethical.Permission for the first genetic implantationexperiments has been granted by the NationalInstitutes of Health.
There is no obligation to reveal the results ofpreclinical diagnosis by means of predictive tests in
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

628 M. SUPER
filling in an insurance form, though there would bean obligation to mention a positive family historyof symptomatic individuals.Though paternity tests are technically feasible,
there could be some ethical issues involved infathers wishing to check on their paternity of theirchilden - one might need to consider the welfare ofthe child in offering such tests and marriage
guidance might be a better option. In any eventthere should be careful counselling before suchtests are performed.The 80s proved very exciting in terms of genetic
discoveries and applications of the new-foundknowledge. The 90s should prove even moreexciting and the genetic text-book is likely to berewritten by 2001.
References
Chromosomes
1. Lejeune, J., Gautier, M. & Turpin, M.R. Etudes deschromosomes somatique de neuf enfants mongoliens. CRAcad Sci (Paris) 1959, 248: 1721-1722.
2. Jacobs, P.A. & Strong, J.A. The somative chromosomes inmongolism Lancet 1959, i: 710-712.
3. Lejeune, J., Lafourcade, J., Berger, R. et al. Trois cas dedeletion partielle du bras court d'un chromosome 5. CRAcad Sci (Paris) 1963, 257: 3098-3102.
4. Hamerton, J.L., Ray, M., Abbot, J. et al. Chromosomestudies in a neonatal population. Can Med Assoc J 1972,106: 776-779.
5. Evans, H.J. Chromosome anomalies among liveborns. JMed Genet 1977, 14: 309.
6. Creasy, M.R., Crolla, J.A. & Alberman, E. A cytogeneticstudy of human spontaneous abortions using bandingtechniques. Hum Genet 1976, 31: 177-196.
7. Edwards, J.H., Harnden, D.G., Cameron, A.H. et al. A newtrisomic syndrome. Lancet 1960, i: 787.
8. Patau, K., Smith, D.W., Therman, E. et al. Multiplecongenital anomaly caused by an extra autosome. Lancet1960, i: 790-793.
9. Froland, A. Klinefelter Syndrome. Costers Bogtrykkeri,Copenhagen, 1969.
10. Ferguson-Smith, M.A. A collaborative study of theaetiology of Turner syndrome. Ann Hum Genet 1980, 43:355-368.
11. Caspersson, T., De la Chapelle, A. Schroder, J. et al.Quinacrine fluorescence ofmetaphase chromosomes: identi-cal patterns in different tissues. Exp Cell Res 1972, 72: 56.
12. Seabright, M. A rapid technique for human chromosomebanding. Lancet 1971, fi: 971-972.
13. Carrano, A.V., Gray, J.W., Langlois, R.G. et al. Measure-ment and purification of human chromosomes by flowcytometry and sorting. Proc Natl Acad Sci 1979, 76: 1382.
14. Younis, J.J. High resolution of human chromosomes.Science 1976, 191: 1268-1270.
15. Lindenbaum, R.H, Clarke, G., Patel, C. et al. Musculardystrophy in an X-translocation female suggests thatDuchenne locus is on X chromosome short arm. J MedGenet 1979, 16: 389-392.
16. Lubs, A. A marker chromosome. Am JHum Genet 1969, 21:231.
17. Turner, F., Daniel, A. & Frost, M. X-linked mentalretardation, macro-orchidism and Xq27 fragile site. JPediatr 1980, 96: 837.
18. Glover, T.W. FUdR induction ofthe X-chromosome fragilesite: evidence of mechanism of folic acid and thymidineinhibition. Am J Hum Genet 1981, 33: 234-242.
19. Pardue, M.L. & Gall, J.G. Chromosome localisation ofmouse satellite DNA. Science 1970, 168: 1356-1358.
20. Dutrillaux, B. Nouveau system marquage chromosomiqueavec bandes T. Chromosoma 1973, 41: 395-402.
21. Harrison, C., Jack, E.M. & Allen, T.D. Light and simul-taneous scanning electron microscopy of the samemetaphase chromosomes. In: Hayat, M.A. (ed.) Correla-tional Microscopy in Biology. Academic Press, London,1987, pp. 190-249.
22. Buckle, V.J. & Craig, I.W. In situ hybridisation. In: Davies,K.E. (ed.) Human Genetic Diseases: a practical approach.IRL Press, Oxford, 1986.
23. Sinclair, A.H., Berta, P., Palmer, S. et al. A gene from thehuman sex-determining region encodes a protein withhomology to a conserved DNA binding motif.
24. Lubs, H.A. & Ing, P.S. Human cytogenetic nomenclature.In: Emery, A.E.H. & Rimoin, D.L. (eds) Principles andPractices of Medical Genetics. Churchill Livingstone, Edin-burgh, 1983.
25. Funderburk, S.J., Spence, M.A. & Sparkles, R.S. Mentalretardation associated with 'balanced' chromosome rear-rangements. Am J Med Genet 1977, 29: 136-141.
26. Warburton, D. Outcome of cases of structural rearrange-ments diagnosed at amniocentesis. Prenatal Diagnosis 1984,4: 69-80.
27. Schintzel, A. Catalogue of Unbalanced Chromosomal Aber-rations in Man. Walter de Gruyer, New York, 1984.
28. De La Cruz, F.F. & Gerald, P.S. Trisomy 21 (Downsyndrome) research perspectives. University Park Press,Baltimore, USA, 1981.
29. Down's Syndrome Supplement. Am J Med Genet 1990.30. Sutherland, G.R. & Hecht, F. Fragile Sites on Human
Chromosomes. Oxford University Press, Oxford, 1985.31. Turner, G. & Jacobs, P. Marker (X) linked mental retarda-
tion. Adv Hum Genet 1986, 13: 83-112.32. Partington, M.W. Females in fragile X families. Am J Med
Genet 1986, 23: 111-126.32a.Davies, K.E., Mattei, M.G., Mattei, J.F. et al. Linkage
studies of x-linked mental retardation. Hum Genet 1985, 70:249-255.
33. Webb, T., Bundy, S.E., Thake, A.I. & Todd, J. Populationincidence and segregation ratios in the Martin-Bell syn-drome. Am J Med Genet 1986, 23: 573- 580.
34. Fragile, X: Special Issue: X-linked mental retardation 2. AmJ Med Genet 1986, 23: 1- 736.
35. Fragile, X: Special Issue: X-linked mental retardation. Am JMed Genet 1988, 30: 1-702.
36. Turner, G. Conference report: second international work-shop on fragile X and on X-linked mental retardation. Am JMed Genet 1986, 23: 1 1.
37. Brown, W.T., Jenkins, E.C., Friedman, E. et al. Folic acidtherapy in the fragileX syndrome. AmJMed Genet 1984, 17:299-302.
38. Hagerman, R.J., Jackson, A.W. & Levitas, A. Folic acidversus placebo in the treatment of males with fragile Xsyndrome. Am J Med Genet 1986, 23: 241-262.
39. Suthers, G.K., Hyland, V.J. & Callen, D.F. Physical mapp-ing of new DNA probes near the fragile X mutation(FRAXA) by using a panel of cell lines. Am J Hum Genet1990, 47: 187- 195.
40. Shapiro, L.R., Wilmot, P.L., Murphy, P.D. & Breg, W.R.Experience with multiple approaches to the prenatal diag-nosis of the fragile X syndrome: amniotic fluid, chorionicvilli, fetal blood and molecular methods. Am J Med Genet1988, 30: 347-354.
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

MEDICAL GENETICS 629
41. Raffel, L.J., Mohaudus, T. & Rimoin, D.L. Chromosomemosaicism in the Killian/Teschler-Nicola syndrome. Am JMed Genet 1986, 24: 607-611.
42. Quarrel, O.W.J., Hamill, M.A. & Hughes, H.E. Pallister-Killian mosaic syndrome with the emphasis on the adultphenotype. Am J Med Genet 1988, 31: 841-844.
43. Schintzel, A. Trisomy 8 mosaicism syndrome. Helv PediatrActa 1974, 29: 531.
44. Thurleau, C., Taillard, F., de Bazigan, M.D. et al.Hypomelanosis of Ito (incontinentio pigmentaeachromians) and mosaicism for a microdeletion of 1 5q. HumGenet 1986, 74: 185-187.
45. Hall, J.G. Genomic imprinting - review and relevance tohuman disease. Am J Hum Genet 1990, 46: 103-123. AlsoHall, J.G. Genomic imprinting. Arch Dis Child 1990, 65:1013-1015.
46. Nicholls, R.D., Knoll, J.H.M., Butler, M.G. et al. Geneticimprinting suggested by maternal heterodisomy in non-deletion Prader-Willi syndrome. Nature 1989, 342: 281-285.
47. Magenis, E.R, Brown, M.G., Lacy, D.A. et al. Is Angelmansyndrome an alternative result of del(l5Xql 1q13)? Am JMed Genet 1987, 28: 829-838.
48. Hall, B.D. & Smith, D.W. Prader-Willi Syndrome. J Pediatr1972, 81: 286.
49. Angelman, H. "Puppet children": a report on three cases.Dev Med Child Neurol 1965, 7: 681-688.
50. Rett Syndrome. Am J Med Genet 1986, Suppl 1: 1-402.51. Arlett, C.F. Human DNA repair defects. J Inher Metab Dis
1986, 9 (Suppl I): 69-84.52. Lehman, A.R., Francis, A.J. & Gianelli, F. Prenatal diag-
nosis of Cockayne's Syndrome. Lancet 1985, i: 486.53. German, J., Bloom, D. & Passarge, E. Bloom's Syndrome
XI. Progress report for 1983. Clin Genet 1984, 25: 166.54. Brewer, J.G. & Preston, R.J. Cytogenetic effects of
environmental mutagens. Mutat Res 1974, 26: 297-305.55. Korenberg, J.R., Kawashima, H., Pulst, S.M. et al.
Molecular definition of a portion of chromosome 21 thatcauses features of Down syndrome phenotype. Am J HumGenet 1990, 47: 236-246.
56. Lejeune, J. Pathogenesis of mental deficiency in Downsyndrome. Am J Med Genet 1990, Suppl 7: 20-30.
57. Wisniewski, K.E., Laure-Kaminowska, M., Connell, F. &Wen, G.Y. Neuronal density and synaptogenesis in thepostnatal stage of brain maturation in Down syndrome. In:Epstein, C.J. (ed.) The Neurobiology of Down Syndrome.Raven Press, New York, 1986, pp. 29-44.
58. Balasz, R. & Brooksbank, B.W.L. Certain neurochemicalaspects of the pathogenesis of Down syndrome. In: Epstein,C.J. (ed.) The Neurobiology of Down Syndrome. RavenPress, New York, 1986, pp. 57-92.
59. McCoy, E.E. & Enns, L. Current status of neurotransmitterabnormalities in Down syndrome. In: Epstein, C.J. (ed.) TheNeurobiology ofDown Syndrome. Raven Press, New York,1986, pp. 73-87.
60. St George Hislop, P.H., Tanzi, R.E., Polinsky, R.J. et al.The genetic defect causing familial Alzheimer's disease mapsto chromosome 21. Science 1987, 235: 885-890.
61. Owen, M.J., James, L.A., Hardy, J.A. et al. Physicalmapping around the Alzheimer locus on the proximal longarm ofchromosome 21. AmJHum Genet 1990,46:316-322.
Advances in Molecular Biology62. Ingram, V.M. Abnormal human hemoglobins. III: The
chemical difference between normal and sickle hemoglobins.Biochem Biophys Acta 1959, 36: 402.
63. Milner, P.F., Clegg, J.B. & Weatherall, D.J. Haemoglobin Hdisease due to a unique variant with an elongated alphachain. Lancet 1971, i: 729.
64. Harris, H. The Principles of Human Biochemical Genetics.Elsevier, Amsterdam, 1980.
65. Weatherall, D.J. The New Genetics and Clinical Practice,2nd edition. Oxford Medical Publications, Oxford, 1985.
66. Watson, J.D. & Crick, F.H.C. Genetic implications of thestructure of deoxyribosenucleic acid. Nature 1953, 171:964-967.
67. Orkin, S.H., Alter, B.P., Altay, C. et al. Application ofendonuclease mapping to the analysis and prenatal diag-nosis of thalassaemias caused by globin gene deletions. NEngl J Med 1978, 229: 166-172.
68. Smith, H.O. & Wilcox, K.W. A restriction enzyme fromHaemophilus influenzae. J Mol Biol 1970, 51: 379-391.
69. Southern, E.M. Detection of specific sequences amongDNA fragments by gel electrophoresis. J Mol Biol 1975, 98:503-517.
70. Old, J.M. In: Davis, K.E. (ed.) Fetal DNA Analysis inHuman Genetic Diseases: a practical approach. IRL Press,Oxford, 1986, pp. 1-17.
71. Ruddle, F.H. & Creagan, R.P. Parasexual approaches to thegenetics of man. Ann Rev Genet 1975, 9: 407-486.
72. Anand, R. Pulsed field gel electrophoresis: a technique forfractionating large DNA molecules. Trends Genet 1986, 2:278-283.
73. Brown, W.R.A. & Bird, A.P. Long range restriction mapp-ing of mammalian genomic DNA. Nature 1986, 322:477-481.
74. Maniatis, T., Fritsch, E.F. & Sambrook, J. MolecularCloning. A Laboratory Manual. Cold Spring HarborLaboratory Press, New York, 1982.
75. Antoniou, M., de Boer, E. & Grosveld, F. Fine mapping ofgenes: the characterisation of the transcriptional unit. In:Davies, K.E. (ed.) Human Genetic Disease: A practicalapproach. IRL Press, Oxford, 1986, pp. 65-84.
76. Saiki, R.K., Scharf, S., Faloona, F. et al. Enzymaticamplification of B-globin genomic sequences and restrictionsite analysis for diagnosis of sickle cell anaemia. Science1985, 230: 1350-1354.
77. Eisenstein, B. The polymerase chain reaction: a new methodof using molecular genetics for medical diagnosis. N Engl JMed 1990, 322: 178-183.
78. Newton, C.R., Summers, C., Heptinstall, L.E. et al., Diag-nosis of Alpha- I-antitrypsin deficiency by enzymaticamplification of human genomic DNA and direct sequenc-ing of DA products. Nucl Acids Res 1988, 16: 16:8233-8243.
79. Newton, C.R., Heptinstall, L.E., Summers, C. et al.Amplification Refractory Mutation System for prenataldiagnosis and carrier Lancet 1989, ii: 1481-1485.
80. Old, J.M., Varawalla, N.W., Weatherall, D.J. Rapid detec-tion and prenatal diagnosis of B-thalassaemia: studies inIndian and Cypriot populations in the UK. Lancet 1990,336: 834-837.
81. Jinks, D.C., Minter, M., Tarver, D. et al. Moleculardiagnosis of sickle cell disease using dried blood specimenson blotters used for newborn screening. Hum Genet 1989,81:363-366.
82. Handyside, A.H., Pallinson, J.K., Penketh, R.J.A. et al.Biopsy of human re-implantation embryos and sexing byDNA amplification. Lancet 1989, i: 347-349.
83. Lo, Y.-M.D., Patel, B., Wainscoat, J.S. et al. Prenatal sexdetermination by DNA amplification from maternal blood.Lancet 1989, ii: 1363-1365.
84. Imai, T. & Olsen, M.V. Second generation approach to theconstruction of yeast artificial chromosome libraries.Genomics 1990, 8: 297-303.
85. Sanger, F., Nicklen, S. & Coulson, A.R. DNA sequencingwith chain-terminating inhibitors. Proc Natl Acad Sci 1977,74: 5463.
86. Green, P.M., Bentley, D.R., Mibashan, R.S. et al.Molecular pathology of haemophilia D. EMBO J 1989, 8:1067-1072.
87. Crystal, R.G., Rosenfeld, M., Siegfried, W. et al. New viraltransfer systems. Pediatr Pulmonol 1990, Suppl 5: 1023.
88. McKusick, V.A. Mendelian Inheritance in Man. 9th Ed.Johns Hopkins University Press, Baltimore, 1990.
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

630 M. SUPER
89. Proceedings of Human Gene Mapping Workshop 10.Cytogenet Cell Genet, 1989, 51: 1-1147.
90. Davies, K.E. Molecular genetics of the human X-chromosome. J Med Genet 1985, 22: 243-249.
91. Wapenaar, M.C., Hoffman, E.P., Slayter, H.S. et al. Adeletion hotspot in the Duchenne muscular dystrophy gene.Genomics 1988, 2: 101-108.
92. Van Ommen, G.J.B., Bertelson, C., Ginjaar, H.B. et al.Long range genomic mapping of the Duchenne musculardystrophy (DMD) gene: Isolation and use ofJ66 (DXS268),a distal intragenic marker. Genomics 1987, 1: 329-336.
93. Kingston, H.M., Sarfarazi, M., Thomas, N.S.T. & Harper,P.S. Localisation of the Becker muscular dystrophy gene onthe short arm of the X chromosome by linkage to clonedDNA sequences. Hum Genetic 1984, 67: 6-17.
94. Fraencke, U., Ochs, H.D., de Martinville, B. et al. MinorXp2 1 chromosome deletion in a male associated withexpression of Duchenne muscular dystrophy, chronicgranulomatous disease, retinitis pigmentosa and McLeodsyndrome. Am J Hum Genet 1985, 37: 250-267.
95. Kunkel, L.M., Monaco, A.P., Middlesworth, W. et al.Specific cloning ofDNA fragments absent from theDNA ofa male patient with an X chromosome deletion. Proc NatlAcad Sci 1985, 82: 4778-4782.
96. Monaco, A., Neve, R., Coletti-Feener, C. et al. Isolation ofcandidate cDNAs for portions of the Duchenne musculardystrophy gene. Nature 1986, 323: 646-650.
97. Koenig, M., Beggs, A.H., Moyer, M. et al. The molecularbasis for Duchenne versus Becker muscular dystrophy:correlation of severity with type of deletion. Am J HumGenet 1989, 45: 498-506.
98. Emery, A.E.H. & Holloway, S. Use of normal daughters'creatine kinase in estimating heterozygosity in Duchennemuscular dystrophy. Hum Heredity 1977, 27: 118-126.
99. Roberts, R.G., Bentley, D.R., Barby, T.F.M. et al. Directdiagnosis of Duchenne and Becker muscular dystrophy byamplification of lymphocyte RNA. Lancet 336: 1523-1526.
100. Boelter, W.D., Burt, B.A. & Spector, E.B. Dystrophinprotein and RFLP analysis for fetal diagnosis and carrierconfirmation of Duchenne muscular dystrophy. PrenatalDiagnosis 1990, 10: 703-715.
101. Law, P.K., Bertorini, T.E., Goodwin, T.G. et al. Dystrophinproduction induced by myoblast transfer therapy inDuchenne muscular dystrophy. Lancet 1990, 336: 114-115.
102. Wilson, G.B., Monsher, M.T. & Fudenberg, H.H. Addi-tional notes on the use of isoelectric focusing for thedetection of cystic fibrosis protein. Pediatr Res 1977, 11:139-141.
103. Super, M. & Swindlehurst, C. Isoelectric focusing in geneticcounselling of families with cystic fibrosis. Am J Med Genet1984, 18: 449-453.
104. Jalanko, H. & Aula, P. Decrease in gamma-glutamyltranspeptidase activity in early amniotic fluid in fetaltrisomy 18. Br Med J 1982, 284: 1593-1594.
105. Brock, D.J.H. Amniotic fluid alkaline phosphatase in earlyprenatal diagnosis of cystic fibrosis. Lancet 1983, ii:941 -943.
106. Brock, D.J.H. Cystic fibrosis: prenatal diagnosis of I in 4risk pregnancies. Pediatr Pulmonol 1989, Suppl. 4: 35-36.
107. Eiberg, H., Mohr, J. & Smigolow, K. Linkage relationshipsof paraoxinase (PON) with other markers: indication ofPON-cystic fibrosis synteny. Clin Genet 1985, 28: 265-271.
108. Tsui, L.-C., Cox, C.W., McAlpine, C.J. & Buchwald, M.Cystic fibrosis: analysis of linkage of the disease locus to redcell and plasma markers. Cytogenet Cell Genet 1985, 39:238-239.
109. Tsui, L.-C., Buchwald, M., Barker, D. et al. Cystic fibrosislocus defined by a genetically linked polymorphic marker.Science 1985, 230: 1054- 1057.
110. Knowlton, R.G., Cohen, O., Van Cong, H. et al. Apolymorphic DNA marker linked to cystic fibrosis is onchromosome 7. Nature 1985, 318: 380-382.
11. White, R., Woodward, S., Leppert, M. et al. A closely linkedmarker for cystic fibrosis. Nature 1985, 318: 382-384.
112. Wainwright, B., Scambler, P.J., Schmidtke, J. et al.Localisation ofthe cystic fibrosis locus to 7 cen-7q22. Nature1985, 318: 384-385.
113. Farrall, M., Law, H.-Y. & Rodeck, C.H. First trimesterprenatal diagnosis of cystic fibrosis with linked DNAprobes. Lancet 1986, i: 1402-1405.
114. Super, M., Ivinson, A., Schwarz, M.J. et al. Clinicexperience: prenatal diagnosis ofcystic fibrosis. Lancet 1987,ii: 782-784.
115. Super, M. A United Kingdom cystic fibrosis register. CysticFibrosis Research Workers Conference, Warwick April1991.
116. Kitzis, A., Chomel, J.C. & Kaplan, J.C. Unusual segrega-tion of cystic fibrosis alleles to males. Nature 1988, 333: 215.
117. Estivill, X., Scambler, P.J., Wainwright, B. et al. Patterns ofpolymorphism and linkage disequilibrium tofor cysticfibrosis. Genomics 1987, i: 257-263.
118. Estivill, X., Farrall, M., Scambler, P.J. et al. A candidate forthe cystic fibrosis locus isolated by selection for methylationfree islands. Nature 1987, 326: 840-845.
119. Engel, E. A new genetic concept: uniparental disomy and itspotential effect isodisomy. Am J Med Genet 1980, 6:137-144.
120. Voss, R., Ben-Simon, E., Avital, A. et al. Isodisomy ofchromosome 7 in a patient with cystic fibrosis: coulduniparental disomy be common in humans? Am J HumGenet 1989, 45: 373-380.
121. Super, M. & Schwarz, M.J. Genetic counselling experiencesin cystic fibrosis. Pediatr Pulmonol 1989, Suppl 4: 113.
122. Rommens, J.M., Ianuzzi, M.C., Kerem, B. et al.Identification of the cystic fibrosis gene: chromosome walk-ing and jumping. Science 1989, 245: 1059-1065.
123. Riordan, J.R., Rommens, J.M., Kerem, B.-S. et al.Identification ofthe cystic fibrosis gene: cloning and charac-terisation of complementary DNA. Science 1989, 245:1066-1072.
124. Kerem, B.-S., Rommens, J.M., Buchanan, J.A. et al.Identification of the cystic fibrosis gene: genetic analysis.Science 1985, 245: 1073-1080.
125. Santis, G., Osborne, L., Knight, R. & Hodson, M.E.Independent genetic determinates of pancreatic and pul-monary status in cystic fibrosis. Lancet 1990, 336:1081-1084.
126. European Working Group on CF Genetics. Populationanalysis of the major mutation ofcystic fibrosis. Hum Genet1990, 85: 391-453.
127. Schwarz, M.J., Super, M., Wallis, C. et al. Delta F508 testingof the DNA bank of the Royal Manchester Children'sHospital. Hum Genet 1990, 85: 428-430.
128. Schwarz, M.J., Summers, C., Heptinstall, L. et al. A deletionmutation of the cystic fibrosis transmembrane conductanceregulator delta I507. In: Tsui, L.-C., Romeo, G. (eds)Identification ofthe Cystic Fibrosis Gene. Plenum Press, NewYork, 1991.
129. Cutting, G., Kascoli, L.M., Rosenstein, B.J. et al. A clusterof cystic fibrosis mutations in the first nucleotide bindingfold of the cystic fibrosis conductance regulator protein.Nature 1990, 246: 366-369.
130. Kerem, B.-S., Zielenski, J., Markiewicz, D. et al.Identification of cystic fibrosis mutations in regions corre-sponding to two putative binding folds of the cystic fibrosisgene. Proc Natl Acad Sci 1990, 87: 8117-8151.
131. Dean, M., White, M., Amos, J. et al. Multiple mutations inhighly conserved residues are found in mildly affected cysticfibrosis patients. Cell 1990, 61: 863-870.
132. Osborne, L., Knight, R.A., Santis, G., Hodson, M. Anon-conservative mutation in the second nucleotide bindingfold of the cystic fibrosis transmembrane regulator. Am JHum Genet in press.
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from

MEDICAL GENETICS 631
133. Zielenski, J., Bozon, D., Kerem, B. et al. Identification ofmutations in exon 1 through 8 of the cystic fibrosistransmembrane conductance regulator. Genomics 1991, 10:214-228.
134. Super, M. & Schwarz, M.J. Mutations of the cystic fibrosisgene in North-West England. Cystic Fibrosis ResearchWorker's Conference, Warwick, 1991.
135. Hyde, S.C., Emsley, P., Hartshorn, M.J. et al. Structural andfunctional relationships of ATP-binding protein associatedwith cystic fibrosis, multiple drug resistance and bacterialtransport. Nature 1990, 346: 362-365.
136. Knowles, M.R., Church, N.L. & Waltner, W.E. A pilotstudy of aerosolised amiloride for the treatment of lungdisease in cystic fibrosis. N Engl J Med 1990, 322:1189-1194.
137. Rich, D.P., Anderson, M.P., Gregory, R.J. et al. Expressionof cystic fibrosis transmembrane conductance regulatorcorrects defective chloride channel regulation in cysticfibrosis airway epithelial cells. Nature 1990, 347: 358-363.
138. Gregory, R.J., Cheng, S.H., Rich, O.P. et al. Expression andcharacterisation of the cystic fibrosis transmembrane con-ductance regulator. Nature 1990, 347: 382-386.
139. Crystal, G., Trapnell, B.C., Yoshimura, K. et al. Genetherapy for cystic fibrosis: modulation of the respiratoryepithelial cell target by gene transfer. Pediatr Pulmonol 1990,Suppl 5: 59-61.
140. Carter, B., Flotte, T.R., Owens, R.A. et al. Adeno-associated virus for gene transfer. Pediatr Pulmonol 1990,SupplS: 104.
Screening in genetic disease141. Cuckle, H. & Wald, N. Reporting the assessment of
screening and diagnostic tests. Br J Obstet Gynaecol 1989,96: 389-396.
142. Francke, U., Brown, M.S. & Goldstein, J.L. Assignment ofthe human gene for the low density lipoprotein receptor tochromosome 19: synteny ofa receptor, a ligand and a geneticdisease. Proc Nat! Acad Sci 1984, 81: 2826-2830.
143. Horstemke, B., Dunning, A. & Humphries, S. Identificationof deletions in the human low density lipoprotein receptorgene. J Med Genet 1987, 24: 144-147.
144. Smith, R.A., Williams, D.K., Silbert, J.R., Harper, P.S.Attitudes of mothers to neonatal screening for Duchennemuscular dystrophy. Br Med J 1990, 300: 1112.
145. Wilcken, B., Brown, A.R.D., Urwin, R. & Brown, D.A.Cystic fibrosis screening by dried blood spot trypsin assay. JPediatr 1983, 102: 383-387.
146. Perobelli, S., Faraguna, D., Giglio, L. et al. False positivescreening tests for cystic fibrosis: psychological reactions inthe parents and attitudes of the professionals. 10th Interna-tional Cystic Fibrosis Conference. Exerpta Medica, Amster-dam, 1988, p. 24.
147. Laroche, D. & Travert, G. Abnormal frequency of deltaF508 mutation in neonatal transitory hypertrypsinaemia.Lancet 1991, 337: 55.
148. Dumur, V., Lafitte, J.-J. & Gervais, R. Abnormal distribu-tion of cystic fibrosis delta F508 allele in adults with chronicbronchial hypersecretion. Lancet 1990, 336: 1340.
149. Hambleton, G., Super, M. & Walsworth-Bell, J. PaediatricCystic Fibrosis Register of the North-West Regional HealthAuthority 1986.
150. Brock, D.J.H. & Sutcliffe, R.G. Alpha-fetoprotein in theantenatal diagnosis of anencephaly and spina bifida. Lancet1972, ii: 197-199.
151. Bernard, S., Walsworth-Bell, J. & Super, M. A survey ofneural tube defects in the North-West ofEngland. Surgery ininfancy and childhood 198, ii: 15- 16.
152. Smith, A.D., Wald, N.J. & Cuckle, H.S. Amniotic fluidacetylcholinesterase as a possible diagnostic test for neuraltube defect in early pregnancy. Lancet 1979, i: 665-668.
153. Wald, N.J. & Cuckle, H.S. Recent advances in screening forneural tube defects and Down syndrome. In: Rodeck, C. (ed.)Prenatal Diagnosis. Bailliere-Tindall, London, 1987.
154. Smithells, R.W., Sheppard, S., Scorah, C. et al. Possibleprevention of neural tube defects by periconceptual vitaminsupplementation. Lancet 1980, i: 339-340.
155. Super, M., Fennell,, Schwarz, M.J. & Boyd, R.A. Investiga-tion of cholinesterase in amniotic fluid. Br Med J 1986, 293:17-18.
156. Cuckle, H.S., Wald, N.J. & Thompson, S.J. Estimating awoman's risk of having a pregnancy associated with Downsyndrome using her age and serum alpha-feto-protein. Br JObstet Gynaecol 1987, 94: 387-402.
157. Cuckle, H.S. & Wald, N.J. Screening for Down syndrome.In: Lilford, R.J. (ed.) Prenatal Diagnosis and Prognosis.Butterworths, London, 1990, pp. 67-92.
158. Kaback, M.M., Nathan, T.J. & Greenwald, S. Tay-Sachsdisease: heterozygote screening and prenatal diagnosis - USexperience and world perspective in Tay-Sachs. In: Kaback,M.M. (ed.) Progress in Clinical and Biological Research inTay-Sachs. Alan Liss, New York, 1977.
159. Modell, M. & Modell, B. Genetic screening for ethnicminorities. Br Med J 1990, 300: 1702- 1704.
160. Cao, A.L., Pintus, U., Lecca, C. et al. Control of Beta-thalassaemia by carrier screening and antenatal diagnosis inSardinians. Clin Genet 1984, 26: 12-22.
161. Clarke, J.T.R., Skomorowski, M.A. & Zuker, S. Tay Sachscarrier screening: follow-up ofa case finding approach. Am JMed Genet 1989, 34: 601-605.
162. Ten Kate, L. Carrier screening for cystic fibrosis. Lancet1989, ii: 973-974.
163. Super, M., Schwarz, M.J. & Sardharwalla, I.B. CF screen-ing. Nature 1989, 344: 113-114.
Ethics and genetics164. Royal College of Physicians report: Prenatal diagnosis and
genetic screening: community and service implications. RoyalCollege of Physicians, London, 1989.
165. Clarke, A. Genetics, ethics and audit. Lancet 1990, 335:1145-1147.
copyright. on M
ay 23, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.67.789.613 on 1 July 1991. D
ownloaded from