maximizing treatment effectiveness for dwi … · maximizing treatment effectiveness for dwi...
TRANSCRIPT

MAXIMIZING TREATMENT EFFECTIVENESS FOR DWI OFFENDERS
Sharon L. Franklin, M.A.Alcohol Countermeasures Probation, Fort Wayne, Indiana, U.S.A.
Summary.
Group intensive treatment strategies for DWI offenders offer promising alternatives to traditional treatment formats. Group intensive treatment offers higher rates of therapeutic contacts combined with lower fees for offenders and requires less time to complete. When group intensive treatment was instituted for DWI offenders in Allen County, Indiana, more offenders successfully completed treatment and paid their fees. More hours of treatment services became available to offenders while caseloads for probation and therapeutic staff dropped dramatically.Introduction.
Evaluation studies (Nichols et al., 1978 a; Nichols et al., 1978 b) conducted on the Alcohol Safety Action Projects (ASAPs) of the 1970s indicated the following: (a) short term rehabilitation (STR) did not change the drinking driving behavior of problem drinking DWI drivers and (b) didactic education seemed harmful to these same drivers. However, almost any intervention applied to social drinker DWI drivers resulted in a reduction in subsequent DWI behavior; and small, interactive groups were more effective than larger groups (Nichols et al., 1978 b). License suspension was the only single countermeasure that resulted in a reduction of DWI rearrests among problem drinking drivers (Hagen, 1981; McGuire and Peck, 1977).These evaluation outcomes implied that programs designed to combine countermeasures and to provide long term treatment to DWI offenders might prove more effective. Subsequent research defines a comprehensive DWI program as one that "interlocks" legal sanctions and treatment sanctions with management functions insuring accountability (U. S. Department of Transportation [DOT], 1987).Materials and Methods.
The notion that long term treatment is required to effectively impact the drinking driving behavior of problem drinking drivers may be critical to DWI intervention programs. Unfortunately, definitions of "long-term" and "treatment" are sufficiently murky to require separate analysis.Treatment for the purposes of this discussion refers to outpatient or inpatient services provided by professional therapists certified as addictions specialists. Traditional treatment refers to services applied at a rate of one session per week for one to two hours per session. Group intensive treatment refers to services provided at a rate of two or more sessions per week for two or more hours per session. Treatment services include: group addictions psychotherapy, family therapy, and individual therapy.
965
Most addictions treatment programs providing the above services also include an educational component which typically covers AIDS awareness, addiction, the disease concept, co-dependency, and other relevant issues.Educational interventions that are appropriate for social drinker drivers are not considered to be treatment within these definitions."Long-termness" is more difficult to define. Most definitions refer to length of time in treatment. In general, a year or more in treatment is considered to be long-term treatment. However, length of time in treatment as a measure does not address the issue of service provision.Is one meeting per week as effective as three meetings per week? Are Intensive Outpatient Programs (IOP) more effective for multiple offenders than traditional outpatient programs?It seems necessary to define a measure that relates service provision to length of time in treatment. Let the ratio of the number of hours of outpatient services to the number of weeks in a year be defined as a "treatment intensity score". This measure can be used to establish a definition of long term treatment that relates service provision to time in treatment.Define long-term treatment as a treatment intensity score of .75. The selection of this standard for use as a measure of long termness is arbitrary but intuitively defensible. The .75 treatment intensity score was selected given a traditional treatment format: one hour meetings once per week for 52 weeks minus thirteen weeks for therapist training, vacation, and sick time leaves 39 weeks. Given a traditional format, 39 weeks is a reasonable number of weeks to expect a therapist to see a client that has been assigned to a program lasting one year. Hence, it would be reasonable to expect around 39 hours of treatment services to be provided to offenders in such a program. Results.A model Alcohol Countermeasures Program (ACP) dealing exclusively with DWI offenders was designed and implemented in Allen County, Indiana in 1979. The program was a model in the sense that its design incorporated the attributes implied by the ASAP evaluation data: all available countermeasures were combined (jail, probation, fines, license probation/suspension), one year of addictions treatment was required, and an effective probationer tracking system was combined with strong legal accountability. The treatment and statistical information utilized in this study was collected as a routine function of ACP's probation monitoring.The "treatment" originally provided by the local mental health center was sixteen hours of alcohol awareness education, one half of which was didactic and one half of which was small group processing of the information provided in the didactic component. Individual treatment augmented the education. The groups provided in this programming were not therapy groups.In less than a year, the numbers of offenders referred by the court and the program to treatment had increased to the degree that the group processing component to the program was dropped. The education became strictly didactic, which as indicated above, is contraindicated for problem drinker drivers.
966
Discussions concerning the appropriateness of group therapy for DWI offenders produced no changes in treatment format from 1979 to 1985. Time in treatment for most offenders ranged from three months for social drinkers to five to eight months for problem drinker drivers.From 1980 to 1982 services were brokered for 781 offenders, 676 offenders, and 640 offenders respectively. During the last quarter of 1982, a selective enforcement program against drunk driving (SEPADD) resulted in 719 DWI offenders being convicted and assigned to ACP. The impact of this program was felt in 1983 when ACP brokered services for 1106 offenders. ACP's active monthly caseload increased from 400 in August of 1982 to 785 in 1983. So many offenders were referred to the program that some offenders had to wait for two months to be screened for admission to ACP and for as long as three months to enter treatment after admission to ACP.The selective enforcement program so overloaded the system that the mental health center designed special programs that consisted solely of didactic education for resistant alcoholic clients. No pretense was made of giving these offenders any treatment. Under the circumstances, ACP staff did not confront the use of this strategy even though these clients are the ones for whom education is harmful. When the same "temporary strategy" was carried over into 1984, the service provider was confronted by court administrators about the failure to provide adequate treatment both in terms of type of treatment and in the number of hours of services provided.The average number of services provided to offenders was 21 hours. These hours represented sixteen hours of didactic education and five individual therapy sessions with neither intervention being recommended for substance abusing offenders (Lowinson and Zwerling, 1981; Stein and Friedman, 1981). Once again the need for group addictions psychotherapy for these offenders was reviewed with the service provider. This discussion included the utilization of group therapy as a tool to increase the number of treatment contact hours while potentialy reducing the therapists' caseloads. Intensive Outpatient Programming (IOP) was suggested as a possible method for caseload reduction.Rather than explore the potential of instituting group intensive treatment, the mental health center developed a 40 to 50 hour traditional treatment program in September of 1984. Treatment intensity increased from .41 (21 hours per year) to .86. With no increase in the use of group therapy or an increase in staff, the length of time required to provide the services doubled. Moveover, the numbers of offenders arrested for DWI and referred to ACP did not return to pre-SEPADD levels. Since caseload is a function of the number of clients and the duration of treatment(Ludwin, 1988), caseloads for both the mental health center and ACP increased alarming. ACP's monthly, active caseload increased from 793 in September of 1984 to 1003 in March of 1985.In April of 1985, a private service provider decided to explore the practicality of IOP. Allen Superior Court immediately approved the creation of a multiple offender program wherein any offender convicted of DWI and having a prior alcohol or drug conviction was assigned to IOP.The IOP met three sessions per week for three hours per session for eight weeks
967

and was followed by six weeks of aftercare for a total of 84 hours. All multiple offenders were assigned to this program.Within a matter three months the private provider developed a forty to fifty hour Accelerated Program for first offenders as well. This group intensive program met two times per week for one and a half to two hours per group for ten to twelve weeks. The treatment intensity for this program was also .86 and consistent with the .75 definition of long-termtreatment.First offenders were thereafter offered the choice of attending either the traditional (one year) program or the group intensive program which required half the time to complete. The costs of the the accelerated programs were lower than traditional programs. Offenders began to choose the group intensive programs to the exclusion of thetraditional program.
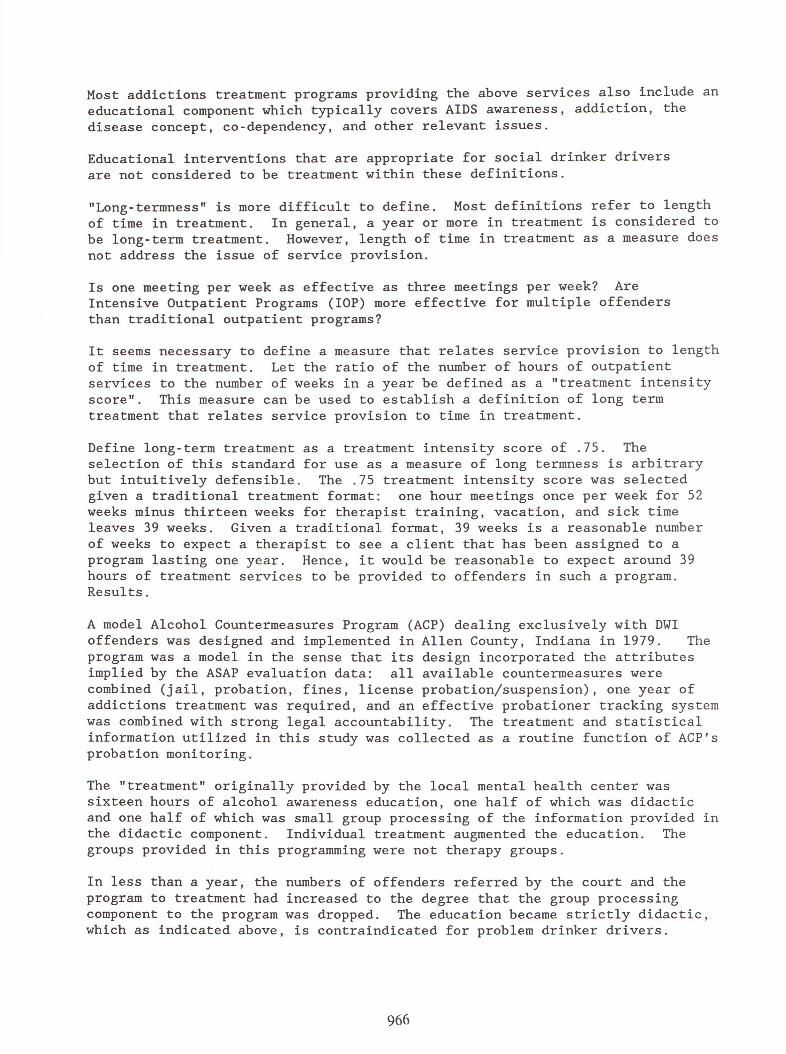
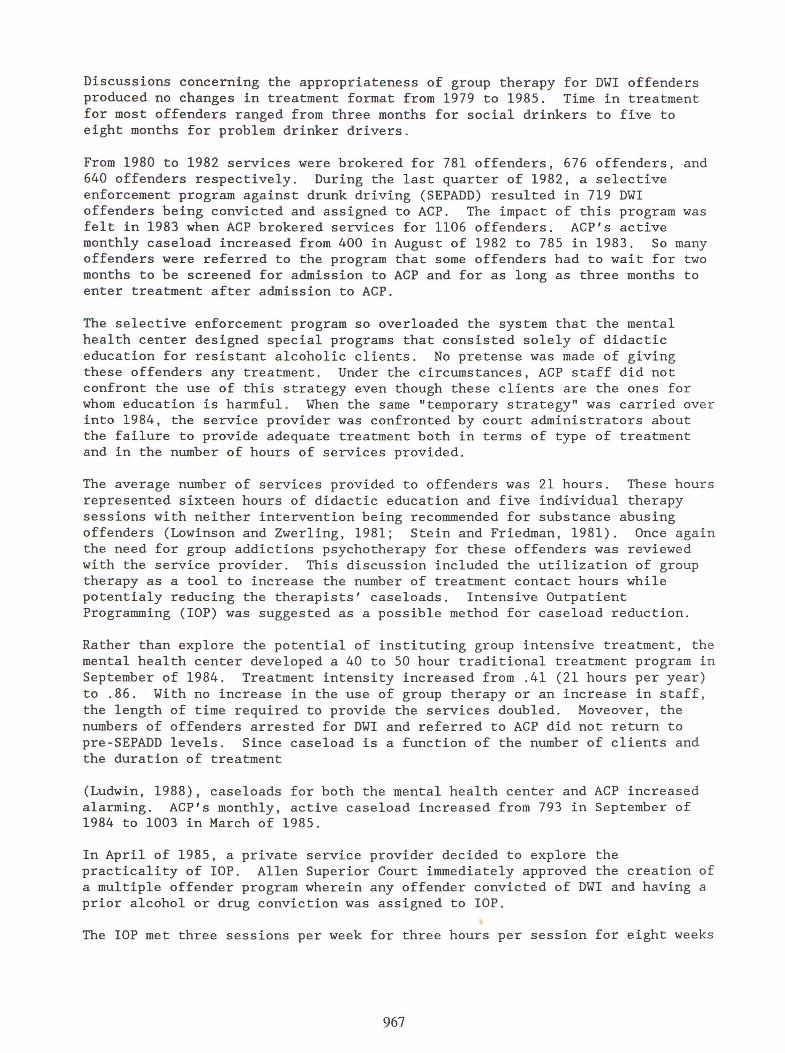
Discussion.The Impact of Treatment Style on Probation's Caseload is depicted in Figure 1. The steep rise in monthly caseload resulting from doubling treatment intensity from .41 to .86 while utilizing the traditional format is obvious during the last quarter of 1984 and the first quarter of 1985.Equally apparent is the decline in probation's caseload subsequent to the implementation of group intensive treatment in April of 1985. The private service provider was not overloaded in spite of a treatment intensity of .86 for the Accelerated Program and 1.61 for IOP.Probation's caseload stablized during the last quarter of 1987 and has remained stable with an average monthly caseload of 468 probationers. Significantly, the introduction of group intensive treatment affected the rate of successful treatment completions among DWI offenders.To successfully complete treatment, a probationer must attend all treatment sessions and be paid in full at the time of probation release, otherwise failure to pay procedures are filed with Allen Superior Court. In 1984, only 54.9% of first time ACP probationers were successfully completing treatment. After the implementation of group intensive treatment, a steady increase in the percentage of successful completions was observed as indicated in Figure 2, despite allowing multiple DWI offenders back into the program. By the end of 1988, 70.9% of all probationers were successfully completing treatment.In conclusion, the implementation of group intensive treatment maximizes treatment effectiveness for DWI offenders by increasing the service delivery capacity of the addictions treatment system. Treatment intensity increased from .41 to .86 for first offenders and from .41 to 1.61 for multiple offenders. In the program cited, this change resulted in a significant increase in successful treatment completions among both first and multiple offenders.
968

References.
Hagen, R. E. (1981). The sanctioning process and the DUI offender. Abstracts and reviews. Alcohol and Driving, 2, 1-5.Lowinson, J. & Zwerling, I. (1981). Group therapy with narcotic addicts.In Kaplan, H., & Sadock, B., Comprehensive Group Psychotherapy (pp. 602 -621). Baltimore, MD: The Williams and Wilkins Company. Ludwin, W. G. (1988). Simple model for powerful results. Administration and Society, 19(4), 479 - 492.Nichols, J. L., Ellingstad, V. S., & Struckman-Johnson, D. L. (1978 a, May).An experimental evaluation of the effectiveness of short-term education and rehabilitation programs for convicted drinking drivers.Paper presented at the Annual Forum of the National Council on Alcoholism,St. Louis, Missouri.Nichols, J. L., Weinstein, E. B., Ellingstad, V. S., & Struckman-Johnson,D. L. (1978 b). The specific deterrent effect of ASAP education and rehabilitation programs. Journal of Safety Research, 10, 177-187.Stein, A., & Friedman, E. (1981). Group therapy with alcoholics. In Kaplan, H., & Sadock, B., Comprehensive Group Psychotherapy (pp. 652 - 689).Baltimore, MD: The Williams and Wilkins Company.McGuire, J. P., & Peck, R. C., (1977). Traffic offense sentencing processes and highway safety, II (DOT Report No. DOT HS 802 327). Washington, DC:National Highway Traffic Safety Administration.U. S. Department of Transportation (1987). Treatment for the drunk driver (Contract No. DTNH22-85-C-05100) Springfield, Virginia: National Technical Information Service.
969
M P A C T O F T R E A T M E N T S T Y LE ON P R O B A T I O N 'S C A S E L O A D
L E G E N D
____ CASELOAD
1 9 8 4 1 9 8 5 1 9 8 6 1 9 8 7 F i g u r e 1 .
1 9 8 8
ALCOHOL COUNTERMEASURES PROBATION BUSINESS TRENDS: 1985 - 1988
CLOSURES
SATISFACTORYJAIL OPTIONS 2 .3X
UNSATISFACTORY 6.7%
FALURES TO PAY 7.9%
MISCaLANEOUS OS
REVOCATIONS 12.2%
Figure 2.970