mark w linder, ph.d., dabcc, facb medical director, evp operations kristen k. reynolds ph.d....
TRANSCRIPT

Mark W Linder, Ph.D., DABCC, FACBMedical Director, EVP Operations
Kristen K. Reynolds Ph.D.Associate Medical Director, VP Laboratory Operations
Mark P. Borgman, Ph.D.Assistant Medical Director, Director of Laboratories
Copyright 2010-12 PGXL Laboratories LLC, Louisville KYAll materials herein are the exclusive property of PGXL laboratories

Enabling Personalized Medicine
IntuitiveMedicine
PrecisionMedicine
Indicators Suggest: Diagnostic services will trump therapeutics(Clayton M Christenson in: The Innovator’s Prescription, MaCGraw Hill, 2009)

~60% of meds in top 20 list causing ADRs are linked to a genetic variation
122 drugs have FDA box warnings related to genetics

4
Clinical Applications of Pharmacogenetic Information
• Anti-coagulation– Warfarin– Plavix (clopidogrel)
• Psychiatry– Anti-depressants
• Oncology– Thiopurines– Tamoxifen– EGFRi’s
• Pain management– Codeine– Methadone
• Epilepsy– Phenytoin– Carbamazepine
• Diabetes– Glipizide

Application of Pharmacogenomics to Anti-platelet therapy

6
• Clopidogrel (Plavix) activation.
PharmGKB.org

7
Antiplatelet Response
• ~ 30% of patients have deficiency in CYP2C19
– CYP2C19 *1/*2 (28%)
– CYP2C19 *2/*2 (2%)
• Decreased activation of clopidogrel – Decreased amount of active metabolite
– High on-treatment platelet reactivity

Influence of CYP2C19 on Clopidogrel Response
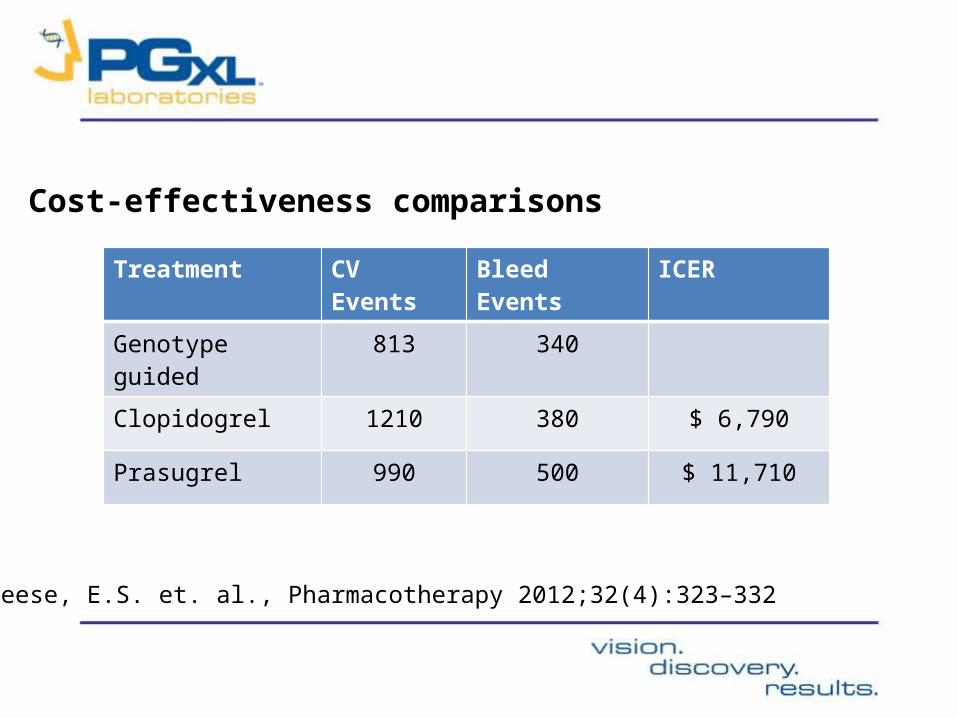
Treatment CV Events Bleed Events ICER
Genotype guided 813 340
Clopidogrel 1210 380 $ 6,790
Prasugrel 990 500 $ 11,710
Cost-effectiveness comparisons
Reese, E.S. et. al., Pharmacotherapy 2012;32(4):323–332

Application of Pharmacogenomics to warfarin therapy

11
The Problem
Reynolds et al. Pers Med 2007;4(1):11-31.

12
• 40% of population have deficient CYP2C9
• > 70% of population have decreased VKOR and are more sensitive to warfarin
Genetics of Warfarin metabolism and response

13
0 3 6 9 12 15 18 21 24 27 30
Ti me (days)
0. 00
0. 60
1. 20
1. 80
2. 40
3. 00
S-W
arfa
rin
(mg/
L) CYP2C9*1/*3
CYP2C9*1/*1
CYP2C9*1/*2
Accumulation
Steady-State
Linder et al. J Thrombosis & Thrombolysis 2002;14:227-232
CYP2C9 status increases magnitude of accumulation/unit dose as well as time to achieve steady-state
CONFIDENTIAL

14
VKORC1 -1639 G>A genotype dictates S-warfarin therapeutic concentration
Dose2.7 ± 1.2 mg
Dose4.2 ± 2.2 mg
Dose6.7 ± 3.3 mg
All within INR 2-3
Zhu Y et al. Clin Chem 2007;53(7):1199-1205.
CONFIDENTIAL


16
• Calculation of estimated maintenance dose• Modeling of individualized response to dose changes• Guidance for:
Monitoring strategy Dosing modifications Transition: induction to maintenance therapy
PerMIT:Warfarin©
Powered by PGXL Laboratories
CONFIDENTIAL

All; 66 y/o, female, 130 lbs

18
Concentration/Response Time Profile
Genotype: CYP2C9*1*2 // VKOR C1 GGEstimated Maintenance dose: 6.3 mg/d (5.7 – 7.0)Time to Steady-State; 11 to 15 daysTarget therapeutic concentration: 0.8 mg/L
. . . . . . 6 mg/d. . . . . . . 10, 10, 8, 6 mg/d
Linder MW et al. 2011 (unpublished results)CONFIDENTIAL

• State-of-the-art estimation of optimal warfarin doses, from induction to transitional, maintenance, and INR-adjustment dosing
• Dynamic and interactive tools that respond physician decisions
• Ongoing application of PGx results
• Minimized risk of out-of-range INRs

Randomized Control Pilot Trial • In collaboration with the University of Utah• Standard of care vs PerMIT:warfarin• Target enrollment of 15 subjects per arm• Outcomes• Time to first therapeutic INR• Time to stable therapy• Overall time in range• Incidence of above range INR’s

Outcomes

Fundamental Principles• Genetic variability in drug metabolism significantly increases risk of
ADRs and non-response• Genetic variation can be managed:
• Poor Metabolizers• Decreased maintenance dosing (20 – 70% )• Increased pro-drug dosing• Allow longer time to reach Steady-State• Allow longer time between medication changes• Increased observation • Choose alternative medication
• Rapid metabolizers• Increased dosages (50 – 200%)• Decreased pro-drug dosages

Clinical Implementation– Identify conflicts– Assess impact on care– Manage conflicts• Avoid pro-drugs in PM’s• Increase or decrease dosing• Alert/inform patient of potential side-effects

Thank You