marine poisoning - emergpa · web viewmarine toxin toxin origin food source clinical syndrome and...
TRANSCRIPT

http://neurology.thelancet.com Vol 4 April 2005 219
Review
Neurotoxic marine poisoningGeoffrey K Isbister, Matthew C Kiernan
Marine poisoning results from the ingestion of marine animals that contain toxic substances and causes substantial illness in coastal regions. Three main clinical syndromes of marine poisoning have important neurological symptoms—ciguatera, tetrodotoxin poisoning, and paralytic shellfish poisoning. Ciguatera is the commonest syndrome of marine poisoning and is characterised by moderate to severe gastrointestinal effects (vomiting, diarrhoea, and abdominal cramps) and neurological effects (myalgia, paraesthesia, cold allodynia, and ataxia), but is rarely lethal. Tetrodotoxin poisoning and paralytic shellfish poisoning are less common but have a higher fatality rate than ciguatera. Mild gastrointestinal effects and a descending paralysis are characteristic of these types of poisoning. In severe poisoning, paralysis rapidly progresses to respiratory failure. Diagnosis of all types of marine poisoning is made from the circumstances of ingestion (type of fish and location) and the clinical effects. Because there are no antidotes, supportive care, including mechanical ventilation in patients with severe paralysis, is the mainstay of treatment.
Lancet Neurol 2005; 4: 219–28
Tropical Toxicology Unit, Menzies School of Health Research, Charles Darwin University, NT, and Department of Clinical Toxicology and Pharmacology, Newcastle Mater Misericordiae Hospital, NSW, Australia(G K Isbister MD); Prince of Wales Medical Research Institute and Prince of Wales Clinical School, University of New South Wales, and Institute of Neurological Sciences, Prince of Wales Hospital, Sydney, Australia (M C Kiernan FRACP)
In parts of the Pacific, the number of cases of marine poisoning exceeds 1200 per 100 000 people per year. 1,2
Fish and other marine animals are an important part of human diets in many parts of the world, including the Pacific and Caribbean, hence the high rates of marine poisoning in these regions. Many coastal communities rely entirely on fish for their protein intake. Although most of the burden of marine poisoning is in rural coastal communities, many people who live outside these communities, or travel to them, are presenting to their physicians with acute or ongoing effects after eating seafood. In this review, we focus on marine poisoning and various associated neurological syndromes that happen after ingestion of the common marine toxins. Specifically, the three major clinical syndromes that present with poisoning after the consumption of seafood—ciguatera, tetrodotoxin poisoning, and shellfish poisoning—will be covered. Ciguatera accounts for most cases of marine poisoning but is rarely fatal. By contrast with ciguatera, tetrodotoxin poisoning is less common but has a far higher fatality rate. Scombroid, which is not discussed, is another common marine poisoning, but differs from other types of marine poisoning because toxin is not accumulated (histamine accumulates during spoilage of the fish) and the effects are similar to an allergic reaction.3–6
Marine poisoningAn important distinction between envenoming and poisoning is pertinent to marine poisoning. Venomous animals have a specialised gland that produces venom, and the venom is applied or injected parenterally. Other marine animals accumulate toxic compounds from their environment and do not have specialised toxin- producing glands; consequently, these animals must be ingested to produce toxic effects.6 Marine poisons generally consist of heat and gastric-acid stable low- molecular-weight toxins.6 Many marine toxins have been identified and their structure and function is the subject of ongoing research (table 1).
Marine poisoning causes mostly gastrointestinal and neurological clinical effects, which differ from the typically painful and cardiovascular effects of marine envenoming. Many marine toxins affect voltage-gated Na+ channels in myelinated and unmyelinated nerves, and result in peripheral neurological effects, ranging from mild sensory polyneuropathies to life-threatening flaccid paralysis.
Impulse conductionIn peripheral-nerve myelinated axons, voltage-sensitive Na+ channels in the nodal axon are clustered at high densities (up to 1000/µm2) compared with the internodal
Correspondence to: Dr Geoffrey K Isbister,Department of Clinical Toxicology and Pharmacology, Newcastle Mater Misericordiae Hospital, Waratah, NSW 2298, Australia [email protected]
Marine toxin Toxin origin Food source Clinical syndrome and effects
Tetrodotoxin Thought to be bacterial Pufferfish (fugu), toadfish Tetrodotoxin (puffer fish or fugu) poisoning: mild gastrointestinal effects and a descending paralysis; rapid progression to respiratory failure when severe
Ciguatoxins: Pacific andCaribbean types
Dinoflagellate Gambierdiscus toxicus Reef fish Ciguatera: moderate to severe gastrointestinal effects (vomiting, diarrhoea, and abdominal cramps)and neurological effects (myalgia, paresthesiae, cold allodynia, and ataxia); rarely fatal
Saxitoxin and gonyautoxins Toxic marine microalgae: Alexandrium spp,Pyrodinium bahamense var compressum, and Gymnodinium catenatum
Bivalve shellfish (mussels, oysters, and clams)
Paralytic shellfish poisoning (similar to tetrodotoxin poisoning): descending paralysis; rapid progression to respiratory failure when severe
Brevetoxins Dinoflagellate Gymnodinium brevis Shellfish Neurotoxic shellfish poisoning, similar to ciguatera: gastrointestinal effects (abdominal pain, nausea,and diarrhoea) and neurological effects (paraesthesia, “temperature reversal”, myalgia, vertigo, and ataxia)
Domoic acid Nitzschia spp Shellfish Amnesic shellfish poisoning: gastrointestinal manifestations and unusual neurological features, includingheadache, confusion, loss of short-term memory, disordered eye movements, seizures, myoclonus, and coma
Palytoxin Zoanthid anemones Palythoa sp Crabs and fish Palytoxin poisoning: poorly characterised; reported to affect the neurological, autonomic, andgastrointestinal systems, and to cause myolysis

2 http://neurology.thelancet.com Vol 4 April
Table 1: Common marine toxins, their sources, and the associated clinical syndromes

Revie
s
http://neurology.thelancet.com Vol 4 April 2005 219
c
Na+ K+ s Na+ Ih
Extracellular
Na+K+f K+s
Node Internode K+
IntracellularNode
region (25/µm2).7 The high density of Na+ channels at the node reflects the need of saltatory conduction for a large inward current at the node (figure 1).8 When the nodal membrane is depolarised, an inward current forms, carried by Na+. The Na+ conductance is voltage sensitive and regenerative: it increases with depolarisation, and this in turn leads to depolarisation of the next node.9 This explosive process would result in depolarisation of the whole axon, except that channel inactivation causes the Na+ channels to close again.
Many toxins and drugs bind to the a. subunits of Na+
channels, and most bind to sites that are involved in activation and inactivation (domains I–IV of thea. subunits), except for tetrodotoxin and its derivatives,which occlude the outer pore of the Na+ channel.10
Neurotoxin binding sites are also the target of mutation in some Na+ channelopathies, with toxins capable of experimentally reproducing the abnormal channel kinetics documented for hereditary channelopathies.10
By contrast, local anaesthetics and antiepileptic drugs typically bind to the inner surface of the channel pore, producing resting and use-dependent block.11
Ciguatera poisoningThe commonest marine poisoning, ciguatera is endemic throughout subtropical and tropical regions of the Indo- Pacific and Caribbean.12–20 Ciguatera is rarely fatal and causes moderate neurological and gastrointestinal effects in most people. With the transportation of fish to distant locations, ciguatera is now also being reported in non-endemic regions.6
Ciguatera is caused by the ingestion of ciguatoxins that accumulate in certain tropical and subtropical finfish.13 The marine dinoflagellate Gambierdiscus toxicus produces gambiertoxins that are biotransformed into the more polar ciguatoxins. Herbivorous fish that feed on these organisms and carnivorous fish that eat the smaller herbivorous fish accumulate ciguatoxins and their metabolites. Ingestion of either type of fish can
Figure 2: Fish associated with ciguateraTop: Red bass (Lutjanus bohar) at a depth of 18 m in the Great Barrier Reef, Australia. Bottom: A giant moray eel (Gymnothorax javanicus) at a depth of 15 m, Pulau Redan, Malaysia.
result in ciguatera.13 Many fish have been associated with ciguatera,6,21 including large tropical fish, such as moray eels (figure 2), although ingestion of only a few types of fish always causes poisoning. Human beings are the final link in the food-chain.22 Reef fish most commonly linked to human poisoning are listed in panel 1.23
Ciguatoxins are heat stable and some of the most potent known Na+ channel toxins in mammals. They activate voltage-sensitive Na+ channels at nanomolar and picomolar concentrations, by causing a hyperpolarising shift of the voltage dependence of channel activation, so
Figure 1: Saltatory conduction, with the action potential jumping from one node of Ranvier to the nextDifferent channels are distributed unevenly along the axonal membrane: Na+and K+
are in high concentrations at the node and K+fare almost exclusively paranodal. Ih
(permeable to both K+ and Na+) limits axonal hyperpolarisation, whereas the Na+/K+ pump reversesiconic fluxes that may be generated through activity.8
Panel 1: Pacific and Caribbean reef-fish species associated with ciguatera6,13
Lutjanids (red bass and snappers)Serranids (coral trout from the Great Barrier Reef, sea bass, and groupers)Epinephelids (cod, including flowery cod and spotted cod) Lethrinids (emperors and scavengers)Muraenids (moray eels*)Scombrids (mackerel, including Spanish mackerel, and tunas) Carangids (jacks and scads)Sphyraenids (barracuda)
*thought to be the most toxic ciguateric
Cour
tesy
of E
rik S
chlö
gl
y

Revie
2 http://neurology.thelancet.com Vol 4 April
Na+=Na channels; K+f=fast K channels; K+
s=slow K channels; Ih=inward rectifier channels.

http://neurology.thelancet.com Vol 4 April 2
Revie
the Na+ channels open at resting membrane potentials.13,24 Spontaneous firing of neurons then occurs as tetrodotoxin-sensitive Na+ channels are activated, which gives rise to the neurological signs and symptoms of ciguatera.
The two main classes of ciguatoxins are the Pacific ciguatoxins and Caribbean ciguatoxins. The difference between these toxins seems to account for the regional differences in the clinical effects of ciguatera.13 Pacific ciguatoxin-1 is ten times more toxic than the main Caribbean ciguatoxin, Caribbean ciguatoxin-1.21
Clinical effectsCiguatera is characterised by moderate to severe gastrointestinal symptoms (vomiting, diarrhoea, and abdominal cramps), neurological signs (myalgia, paraesthesia, “electric shock”-like shooting paraesthesia that has a similar presentation to L’hermitte’s phenomenon, cold allodynia, and ataxia), pruritus, and less commonly cardiovascular effects (panel 2).14–20,25,26
Both gastrointestinal and neurological effects after the consumption of fish is the hallmark of ciguatera, but the proportion of each type seems to be regionally dependent.16,17,28 Neurological effects predominate in the Indo-Pacific region whereas gastrointestinal ones predominate in the Caribbean.14–19 A further syndrome, characterised by hallucinations, incoordination, loss of equilibrium, depression, and nightmares, has been related to consumption of Indian Ocean fish.13
The onset of symptoms is highly variable and studies have shown a range from less than 1 h to 48 h. 12,16
Gastrointestinal effects occur first, commonly within 12 h and resolve over 24 h. Neurological features develop over 24 h, initially with paraesthesia and numbness of the lips and extremities.12,16 However, there may be substantial variation in the onset of symptoms between patients, even between people eating the same fish.16
In over 90% of patients, the neurological features are distal and perioral paraesthesia, cold allodynia, and numbness. Cold allodynia—dysaesthesia when touching cold water or objects—is almost pathognomic of ciguatera and is commonly incorrectly referred to as “temperature reversal”. These neurological symptoms are commonly associated with signs of a polyneuropathy.12 The polyneuropathy is mostly a sensory, length-dependent neuropathy involving large and small fibres, with prominent small-fibre dysfunction.12 In one study, 80% of patients had abnormal temperature sensation, over 50% had abnormal pin-prick and vibration sensation (glove and stocking distribution), and a third had diminished light touch sensation.12 Tendon areflexia occurred in 10% and cerebellar signs were rare.
Persistent effects of ciguatera poisoning have been reported,16,29 including subacute and chronic effects and sensitisation to the toxins. Whereas there is much anecdotal evidence for these clinical presentations, there
are no prospective studies with definite cases of ingestion.30 Reported chronic effects include fatigue, loss of energy, arthralgia (especially knees, ankles, shoulders, and elbows), myalgia, headache, and pruritus.16 Fluctuation of these symptoms has also been reported. It is important that other causes for these symptoms are considered. Depression and anxiety also have been associated with chronic ciguatera poisoning.31
An unusual feature, reported with repeated exposure to the toxins is sensitisation.16 People with previous exposure seem to have a more rapid onset of effects, although this has never been documented in rigorous studies. There have been rare reports that eating fish not typically associated with ciguatera, eating chicken, or drinking alcohol can sometimes provoke a recurrence.16
However, well-designed observational studies are needed.
Diagnosis and laboratory testingDiagnosis of ciguatera poisoning is clinical. Fish that contain ciguatoxins do not smell, taste, or look any different from other fish, and detection of ciguatoxins in reef fish is a problem.21 Methods exist for the identification of ciguatoxin in the flesh of fish, but in most cases of poisoning the fish has been eaten or lost.26,32 There is no laboratory method to confirm the ingestion of fish containing ciguatoxin, and simple qualitative testing systems are rarely reliable. Until a sensitive and specific test is available, the diagnosis must
Panel 2: Clinical effects of ciguatera
poisoning GastrointestinalDiarrhoeaAbdominal pain Vomiting Nausea
NeurologicalMyalgiaParaesthesiae (mouth, hands, feet) ArthralgiaCold allodynia (burning on contact with cold) HeadacheAtaxiaDizziness or vertigo
Other Asthenia Pruritus PerspirationMood disorders Bradycardia Eye painDental pain Dysuria Skin rash

Revie
2 http://neurology.thelancet.com Vol 4 April
be made from the history of ingestion and clinical effects. Whereas symptoms of cold allodynia are suggestive of ciguatera poisoning, differential diagnoses of neuropathy are needed, particularly for causes associated with the development of acute inflammatory demyelinating polyneuropathies, such as Guillain-Barré syndrome.
Neurophysiological investigationsPacific ciguatoxin-1 causes tetrodotoxin-sensitive Na+
channels to open near their resting membrane potential, and tetrodotoxin-resistant Na+ channels to recover quickly from inactivation,33 with these effects resistant to lengthy washout.34 Neurophysiological study of experimental animals has found slowing of mixed and motor conduction velocities.35 In patients poisoned with Pacific ciguatoxin-1, neurophysiology may be normal.36
Although severe poisoning might slow sensory conduction, this is associated with increase of the refractory period, indicative of impaired recovery of Na+ channels from their inactivated state.37
ManagementNo effective antidote for ciguatera is available and treatment is supportive, including appropriate rehydration, observation, and symptomatic relief. Rare cardiovascular complications, such as symptomatic bradycardia and severe hypotension, may require treatment.12
Although intravenous mannitol was an accepted treatment for ciguatera and some animal studies have shown that it reverses the in-vitro effects of ciguatoxins,24 a double-blind, randomised, controlled trial found no difference between mannitol and normal saline.12 Hyperosmolar mannitol infusions were initially suggested for treatment after an uncontrolled study of 24 patients,38 and were later supported by case series, non-randomised studies, and a randomised, but not double-blind study.39–42 In 50 patients with ciguatera who were randomised to either mannitol or normal saline, symptomatic improvement was reported in 24 (96%) patients treated with mannitol, which was not significantly different from the 23 (92%) patients who improved with normal saline (only 3 [12%] and 6 [24%] of each group, respectively, were asymptomatic at24 h).12 Treatment satisfaction and requirement for additional treatment were the same in both groups. Infusion site pain occurred in 21 (84%) mannitol- treated patients but only 9 (36%) normal saline-treated patients. Because it is unlikely that normal saline is an effective treatment, the study suggests that most patients improve without treatment. Studies of ciguatoxin-intoxicated animals showed that mannitol did not reverse the effects of ciguatoxin, supporting the results of clinical study.43,44 According to these outcomes, mannitol can no longer be recommended for the treatment of ciguatera.12
Many drugs have been used to treat the chronic symptoms associated with ciguatera and seem to be effective.27,45–49 Small uncontrolled series and case reports suggest amitriptyline is effective. Symptomatic improvement in patients taking amitriptyline is thought to be through Na+ channel modulation.27,48,49 Tocainide was reported to be effective in three patients45 and gabapentin seemed to be beneficial in two patients with ongoing symptoms.46 Other drugs have had variable success.31 It is difficult to make treatment recommendations because there have been no controlled trials of these treatments.
Prevention of ciguatera is important in endemic regions.47 Health recommendations to eat more fish must include caution about ciguatera in some fish species (panel 1).23
Puffer fish (tetrodotoxin) poisoningPuffer fish poisoning results from the ingestion of fish containing tetrodotoxin and is the commonest lethal marine poisoning. Tetrodotoxin poisoning mainly occurs in southeast Asia, most commonly in Japan where fugu (puffer fish fillet) is a delicacy.50–53 In the early part of the 20th century, 100 deaths per year from ingestion of fugu were reported in Japan;52 the rate of deaths has decreased substantially with improved legislation of fugu preparation and marketing. However, tetrodotoxin poisoning is the major cause of fatal food poisoning in Japan, owing to the unlicensed cooks and unskilled preparation of the fish.52
Tetrodotoxin occurs in bony fish in the order Tetraodontiformes, mainly from the family Tetraodontidae, which includes puffer fish and toadfish (figure 3).52 The concentration of tetrodotoxin varies in different parts of the fish, with the highest concentrations in the liver, then ovary, intestines, and skin. Some fresh-water puffer fish species also cause tetrodotoxin poisoning.54 Tetrodotoxin has also been found in xanthid crabs, horse-shoe crabs (including their eggs),55–57 some other fish species, and in certain newt,
Figure 3: A common toadfish (Tetractenos hamiltoni) at a depth of 3 m, near Sydney, Australia
Cour
tesy
of E
rik S
chlö
gl

http://neurology.thelancet.com Vol 4 April 2
Revie
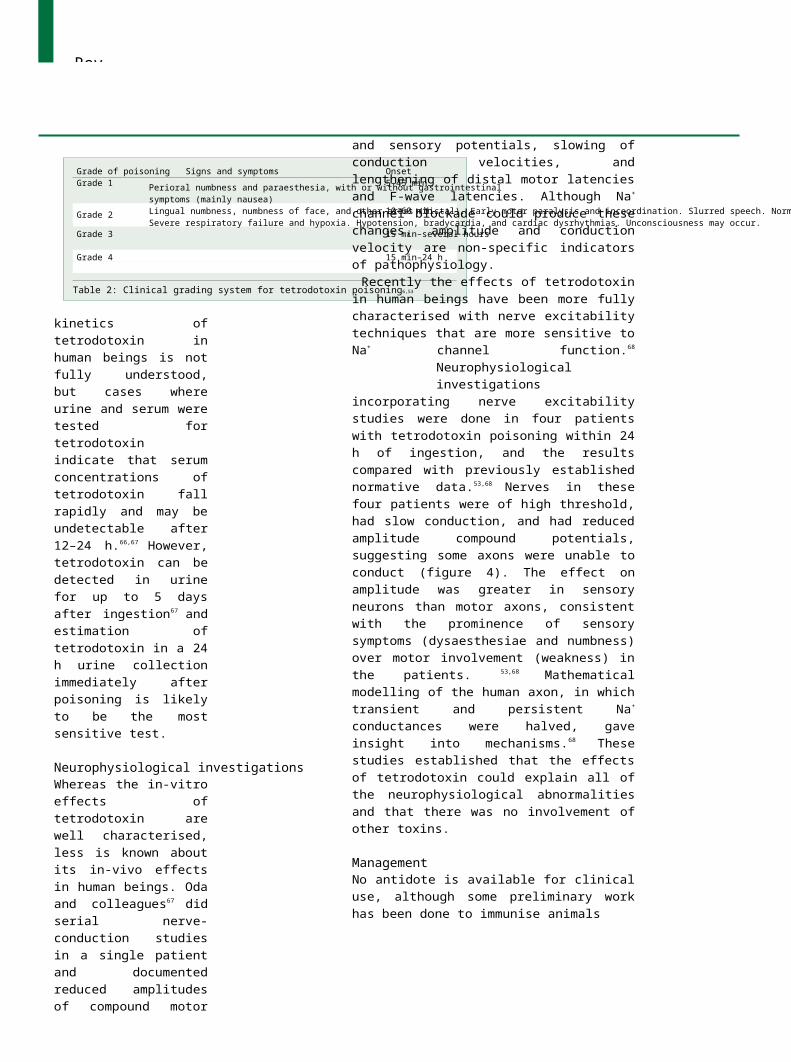
Grade of poisoning Signs and symptomsGrade 1
Grade 2
Grade 4
Perioral numbness and paraesthesia, with or without gastrointestinalsymptoms (mainly nausea)Lingual numbness, numbness of face, and other areas (distal). Early motor paralysis and incoordination. Slurred speech. Normal reflexes. Generalised flaccid paralysis, respiratory failure, aphonia, and fixed or dilated pupils. Patient is conscious.Severe respiratory failure and hypoxia. Hypotension, bradycardia, and cardiac dysrhythmias. Unconsciousness may occur.
Onset5–45 min
10–60 min
Grade 3 15 min–several hours
15 min–24 h
Table 2: Clinical grading system for tetrodotoxin poisoning6,53
frog, and worm species. The bite of the blue-ringed octopus can cause tetrodotoxin envenoming.52
Tetrodotoxin is a water soluble heterocyclic guanidine that blocks Na+ conductance over the single nanomolar range by binding extracellularly at receptor-site 1 of Na+ channels to occlude the outer pore and thereby prevent access of monovalent cations to the pore.58,59 Low threshold currents through tetrodotoxin-sensitive Na+ channels contribute to action potential generation and control of peripheral nerve excitability.60 Blockade of these voltage-sensitive Na+
channels at the nodes of Ranvier affects both action potential generation and impulse conduction and leads to conduction failure in severe cases.61 Tetrodotoxin thus has effects both on action potential generation and impulse conduction.
Clinical effectsThe major clinical effects of tetrodotoxin poisoning develop rapidly and severity seems to depend on the amount ingested. Early symptoms are sensory, including perioral and distal limb numbness and paraesthesia. In cases of mild poisoning, only sensory features develop and are associated with minor gastrointestinal effects such as nausea and vomiting. Patients with moderately severe poisoning develop distal muscle weakness, weakness of the bulbar and facial muscles, and later, ataxia and incoordination with normal reflexes. Dizziness is reported in moderately severe poisoning, and may be accompanied by a sensation of floating,53 possibly reflecting loss of proprioceptive input. Severe poisoning causes generalised flaccid paralysis, respiratory failure, aphonia, and fixed, dilated pupils. However, patients are conscious and there are many reports of patients later recalling the events that occurred when they were unable to respond.62,63 Severe and life-threatening tetrodotoxin poisoning is characterised by cardiovascular effects (bradycardia, hypotension, and dysrhythmias), respiratory failure, and coma. Table 2 gives a simple clinical grading system for patients with tetrodotoxin poisoning. Severe tetrodotoxin poisoning has been used as an explanation for voodoo rituals that create zombies in Haiti, but recent work has not confirmed this.64
Patients with severe poisoning rapidly progress to flaccid paralysis. Symptoms develop well within 1 h when poisoning is severe and fatal.65 In moderately severe cases, symptoms occur within 90 min. Most moderate to severe cases resolve after 5 days,53,62,63 but resolution may take longer in severe poisoning. In minor cases the duration may be only a few hours.
Diagnosis and laboratory testingThe diagnosis of tetrodotoxin poisoning is clinical. Analysis of uneaten fish or patients’ urine or serum for tetrodotoxin confirms diagnosis. High performance liquid chromatography allows simple quantification of tetrodotoxin in urine and serum.66 The pharmaco-
kinetics of tetrodotoxin in human beings is not fully understood, but cases where urine and serum were tested for tetrodotoxin indicate that serum concentrations of tetrodotoxin fall rapidly and may be undetectable after 12–24 h.66,67 However, tetrodotoxin can be detected in urine for up to 5 days after ingestion67
and estimation of tetrodotoxin in a 24 h urine collection immediately after poisoning is likely to be the most sensitive test.
Neurophysiological investigationsWhereas the in-vitro effects of tetrodotoxin are well characterised, less is known about its in-vivo effects in human beings. Oda and colleagues67 did serial nerve- conduction studies in a single patient and documented reduced amplitudes of compound motor and sensory potentials, slowing of conduction velocities, and lengthening of distal motor latencies and F-wave latencies. Although Na+ channel blockade could produce these changes, amplitude and conduction velocity are non-specific indicators of pathophysiology.
Recently the effects of tetrodotoxin in human beings have been more fully characterised with nerve excitability techniques that are more sensitive to Na+
channel function.68
Neurophysiological investigations incorporating nerve excitability studies were done in four patients with tetrodotoxin poisoning within 24 h of ingestion, and the results compared with previously established normative data.53,68 Nerves in these four patients were of high threshold, had slow conduction, and had reduced amplitude compound potentials, suggesting some axons were unable to conduct (figure 4). The effect on amplitude was greater in sensory neurons than motor axons, consistent with the prominence of sensory symptoms (dysaesthesiae and numbness) over motor involvement (weakness) in the patients. 53,68 Mathematical modelling of the human axon, in which transient and persistent Na+
conductances were halved, gave insight into mechanisms.68 These studies established that the effects of tetrodotoxin could explain all of the neurophysiological abnormalities and that there was no involvement of other toxins.
ManagementNo antidote is available for clinical use, although some preliminary work has been done to immunise animals

Revie
2 http://neurology.thelancet.com Vol 4 April
A15
p=0·000005 B p=0·0003
8Puffer fish ingestion
104
Control
5
0 0
C10
p=0·055 D75
p=0·0008
505
25
0 0
E p=0·0003 F p=0·06
8 4
4 3
0 2
Figure 4: Neurophysiological assessment of four adults within 24 h of puffer fish ingestionMotor (A, C, E) and sensory (B, D, F) nerve conduction studies of the median nerve were done with surface electrodes. Mean (± standard error) results are shown, together with the significance of an unpaired two-tailed t test. The stimulus current needed to generate compound motor and sensory action potentials was significantly higher in patients than controls (A, B), suggesting an overall reduction in axonal membrane excitability.Compound potentials were smaller in amplitude (C, D) and of prolonged latency, measured to peak (E, F). These parameters are dependent on Na+ channel function and suggest reduction both in the number of conducting axons and in the conduction velocity of those axons still available for impulse transmission. In total, these findings indicate a reduction in Na+ conductances in the nerves of affected patients, consistent with direct blockade of axonal Na+ channels by tetrodoxin. Reproduced with permission from the Australian Medical Association.53
in Japan and China.69,70 The mainstay of treatment is careful observation and serial neurological assessment to monitor progression of the clinical effects so that respiratory failure or cardiac effects are appropriately treated. Admission to an intensive care unit is necessary in moderate to severe cases to prevent complications from coma, respiratory failure, and cardiovascular effects.51–53 All but the mildest cases should be admitted for observation until the peak of effects has passed. In patients not already severely poisoned, life-threatening effects are highly unlikely after 24 h.51,53 Complications are unlikely with good supportive care and early diagnosis.
In patients with severe poisoning, atropine can be used to treat bradycardia.51 Respiratory support may be needed for a period of 24–72 h.53,62 Patients are typically fully conscious and may become extremely distressed by their inability to respond.62 Sedation is important while the patient is paralysed, and staff must be sensitive when commenting on the patient’s state.
Case reports have suggested the use of neostigmine in the treatment of tetrodotoxin poisoning.62,71 However, there have been no controlled trials to confirm the efficacy of neostigmine and in other reports it had no
effect.63 This lack of response is further supported by animal studies that failed to show any effect of tetrodotoxin at the neuromuscular junction.72
Prevention of tetrodotoxin poisoning is important and must centre on increased public education about poisonous fish that should not be ingested. In Japan greater prevention has been achieved after the introduction of legislation related to the preparation and marketing of fugu.52 However, in most coastal communities, despite knowledge of the risks, seafood is still eaten because it is a major food source.73
Shellfish poisoningShellfish contamination is a medical and economic problem affecting fisheries mainly in temperate regions. Although viral and bacterial infections resulting from shellfish ingestion are more common, toxin-mediated shellfish poisoning can cause severe and life-threatening neurological effects. Toxic shellfish poisoning makes up about 1·1% of food-borne illness, or 7·4% of marine intoxications in the USA.6
Four major toxic syndromes result from shellfish ingestion and three of these are mostly neurological in nature.2,6 The other type of shellfish poisoning is diarrhoetic and is not discussed in this review. Paralytic shellfish poisoning causes paralysis that is similar to tetrodotoxin poisoning, and is caused by saxitoxin, gonyautoxins, and their derivatives. Neuroexcitatory effects occur with neurotoxic shellfish poisoning, which is caused by brevetoxins. Amnesic or encephalopathic shellfish poisoning causes severe gastroenteritis, associated with confusion, memory loss, headaches, and coma, and is due to domoic acid.
Paralytic shellfish poisoningAlthough less common than ciguatera, paralytic shellfish poisoning is the commonest form of shellfish poisoning.74 Deaths continue to occur, with an average mortality rate of about 6% worldwide, although this is higher in developing countries.6 The effects of paralytic shellfish poisoning are almost indistinguishable from tetrodotoxin poisoning, consistent with the similarities of the toxins.6,74,75
Paralytic shellfish poisoning occurs most commonly after the ingestion of bivalve shellfish (mussels, oysters, and clams) containing toxin. The toxins are produced by toxic marine microalgae dinoflagellates, including Alexandrium spp, Pyrodinium bahamense var compressum, and Gymnodinium catenatum.6,74 These dinoflagellates are commonly, but not always, associated with “red tides” (sea discoloration).6 Bivalves ingest the toxic microalgae or dinoflagellates by filter feeding, which concentrates the toxins.74 Species of predator crabs (mainly Xanthidae) that eat shellfish contain paralytic shellfish poisoning toxins and there are reports of human fatalities after ingestion of xanthid crab.57,76 Paralytic-shellfish-poisoning toxins have been identified
Late
ncy
(ms)
Ampl
itude
(mV)
Thre
shol
d (m
A)
Late
ncy (
ms)
Ampl
itude
(µV)
Thre
shol
d (m
A)

Revie
http://neurology.thelancet.com Vol 4 April 2
in three species of cyanobacteria (blue-green algae),77
but no human poisoning has been reported.The main paralytic shellfish toxin, saxitoxin, is
similar to tetrodotoxin but far more potent.61 Saxitoxin and its derivatives, including gonyautoxins, are water soluble, heat stable, tetrahydropurine compounds that are among the most potent neurotoxins known.6,74 These neurotoxins block tetrodotoxin-sensitive Na+ channels, preventing entry of Na+ into cells, which disrupts nerve conduction and results in motor and sensory nerve abnormalities.61,78
Clinical effectsThe median time between ingestion and onset of clinical effects is 1 h (30 min to 3 h)6,74 with rapid development of paralysis and respiratory failure in severe cases. The rate of progression is correlated with poisoning severity,6,74,79 similar to tetrodotoxin poisoning.53 The first effect is typically paraesthesia, with tingling and numbness, of the tongue and lips that spreads to the face, neck, fingers, and toes. The patient may also describe a feeling of dizziness or “floating”, owing to distortion of sensation and proprioception.6
The next symptoms to develop are generalised paraesthesia, arm and leg weakness, and ataxia. Headache, nausea, and vomiting also occur in the initial part of the poisoning, and hypersalivation and diaphoresis may occur. Patients are conscious and alert throughout the poisoning. In patients with mild to moderate poisoning, the effects resolve over 2–3 days, but in more severe cases weakness may persist for a week.6,74 In most fatalities, death occurs rapidly, typically within 12 h.
Diagnosis and laboratory testingTesting for paralytic shellfish toxins is done with a mouse bioassay or immunoassay,80,81 which can be supplemented by analytic techniques, including high performance liquid chromatography57 and more recently liquid mass spectrometry.82 In the mouse bioassay one mouse unit (MU) is defined as the amount of toxin that kills a 20 g mouse in 15 min by intraperitoneal injection and is equivalent to 0·18 µg of saxitoxin.83
Neurophysiological investigationsLimited neurophysiological data are available from patients after paralytic shellfish poisoning. Serial nerve conduction studies in a single patient with paralytic shellfish poisoning found prolonged distal latencies, reduced conduction velocities, and a moderate reduction in sensory and motor amplitudes in peripheral-nerve studies.84 F-wave latencies were prolonged in two of nine patients, associated with increased dispersion, with subsequent return to normal over 2–4 weeks.85 Somatosensory evoked responses were normal in latency, arguing against any substantial proximal (particularly spinal) conduction abnormalities or involvement of large myelinated afferents induced by
saxitoxin. Milder involvement of small myelinated or unmyelinated fibres may happen.
ManagementThe treatment of paralytic shellfish poisoning is supportive, similar to that for tetrodotoxin poisoning. Patients are closely observed in the early stages of poisoning, so that progressing paralysis and respiratory failure can be recognised and treated effectively. Antibodies to saxitoxin have been developed and tested in animal models but are currently not available for human treatment.6 Prevention of paralytic shellfish poisoning is important and monitoring programmes are in place in parts of the world.6
Neurotoxic shellfish poisoningThe distribution of neurotoxic shellfish poisoning is more restricted than for paralytic shellfish poisoning; human poisoning has been reported only from the west coast of Florida,6 North Carolina,86 and New Zealand.87 It is clinically similar to ciguatera, with neuroexcitation rather than a flaccid paralysis. Filter-feeding shellfish cause neurotoxic shellfish poisoning; these shellfish contain brevetoxins produced by the marine dinoflagellate Gymnodinium brevis.
Brevetoxins are lipid-soluble polyether toxins88 that enhance Na+ entry into cells via voltage-sensitive Na+
channels and bind at site 5, similar to ciguatoxins. These toxins have a neuroexcitatory effect because Na+
entry causes nerve-cell depolarisation and spontaneous firing. Toxicity occurs in the nanomolar to picomolar concentration range in animal models by oral and parenteral routes.88
Neurotoxic shellfish poisoning is characterised by a combination of gastrointestinal effects (abdominal pain, nausea, and diarrhoea) and neurological effects (paraesthesia, “temperature reversal”, myalgia, vertigo, and ataxia), similar to ciguatera. Other reported effects include rectal-burning pain, headache, bradycardia, and mydriasis. The clinical effects are commonly mild and treatment is symptomatic and supportive.
Amnesic or encephalopathic shellfish poisoning Amnesic or encephalopathic shellfish poisoning differs from most other neurotoxic marine poisoning because the main effect is to the CNS. It is a toxic encephalopathy that is characterised by severe memory loss and confusion. Ingestion of mussels contaminated with domoic acid causes amnesic shellfish poisoning. Although mass deaths of marine mammals and sea birds have been attributed to fish containing domoic acid,89 there has been only one human outbreak of amnesic shellfish poisoning, in Canada in 1987.90
Domoic acid is a heat stable, water soluble, neuroexcitatory amino acid that acts like the neurotransmitter glutamic acid. The microscopic algae genus Nitzschia produces domoic acid. This

Revie
2 http://neurology.thelancet.com Vol 4 April
neuroexcitatory toxin seems to overstimulate cells but not destroy them. In an outbreak in Canada, the source of domoic acid was found to be N pungens, which was in extensive blooms in the region at the time. Domoic acid has been found in other places including the Pacific coast of Mexico, where it has caused massive poisoning of sea birds and mammals,91 and the coasts of Washington and Oregon in razor clams and Dungeness crabs.92
In the outbreak in Canada, 107 patients were reported to have an acute illness after ingestion of mussels contaminated with domoic acid.90,93 The patients presented with gastrointestinal symptoms (median onset 5·5 h), including vomiting, abdominal cramps, and diarrhoea. Patients developed unusual neurological features after 48 h, including headache, confusion,disorientation, loss of short-term memory, disordered eye movements, mutism, seizures, myoclonus, and coma.90 Other features included haemodynamic instability, cardiac arrhythmias, and profuse respiratory secretions.93 Young patients were most likely to have diarrhoea, and memory loss was most common in old patients and males. Four patients died; all of these were over 70 years of age and had focal neural necrosis and loss of the amygdala and hippocampus.93 14 severely affected patients had ongoing neurological abnormalities, including an anterograde amnestic syndrome with relative preservation of other cognitive functions.93
The diagnosis of amnesic shellfish poisoning is likely to be difficult, because there has been only one reported outbreak. However, amnesic shellfish poisoning is a possibility if there is a combination of gastrointestinal and neurological features, particularly memory loss and confusion, after the ingestion of shellfish. A CT scan may be normal, but an electroencephalogram may show generalised, slow-wave activity. A mouse bioassay and high performance liquid chromatography can be used to test for the presence of domoic acid in mussels.90
Treatment is supportive, and symptomatic and neurological dysfunction should be monitored carefully. Although animals have been protected from the effects of domoic acid when they are given kynurenic acid before domoic acid, further studies are needed.94
Other neurotoxic marine poisoningClupeotoxism is an enigmatic marine poisoning reported from the Caribbean and Indo-Pacific region that results from the ingestion of plankton-eating fish, such as herring and sardines.6,73,95 The effects of clupeotoxism are more severe than for other marine poisoning and the fatality rate is high.95 Gastrointestinal symptoms include nausea, vomiting, abdominal cramping, and diarrhoea associated with an unusual sharp metallic taste. Neurological effects include dilated pupils, paraesthesia, muscle cramps, paralysis, and coma.6 The cause and pathophysiology of clupeotoxism is unclear but findings from a fatality in Madagascar suggest palytoxin may be the cause.95 Treatment is supportive and severe poisoning is commonly fatal.
Palytoxin, originally found in the zoanthid anemones Palythoa sp, is among the most potent of toxins.6,96
Palytoxin is a pore forming toxin that has multiple actions. This toxin causes contraction of smooth and skeletal muscle and H+ influx into cells, which increases intracellular Ca+ in cardiac myocytes and haemolysis.96
Poisoning has happened after the ingestion of crabs and fish that contain palytoxin. Severe muscle and lower back pain were reported in a recent series of 11 patients from Japan. Recovery of the patients took over a month and serum creatine kinase concentrations were high (700–23 800 IU/L).97
Poisoning has also been reported from ingestion of sharks and marine turtles. An unusual mass poisoning was reported in Madagascar after the ingestion of a single bull shark (Carcharhinus leucas).98 188 patients were hospitalised with almost exclusively neurological effects, the most prominent being severe ataxia; gastrointestinal effects were rare. Some patients developed coma quickly, which was associated with a high mortality (30% overall). Two toxins other than ciguatoxins were identified from the shark.98
ConclusionDescription of the common neurotoxic marine poisonings is important for increased awareness of these syndromes. However, prevention of potentially life- threatening poisoning is key and clearly, people should exercise caution—discretion rather than valour— whenever confronted with a plate of exotic shellfish or large tropical fish. Travellers should consult appropriate medical travel-information services for region and season specific information.Authors’ contributionsGKI did the research review and MCK reviewed the neurophysiological and clinical neurological sections of the paper. Both authors contributed to all drafts.
Conflicts of interestWe have no conflicts of interest.
Role of the funding sourceNo funding source was involved in the preparation of this review or in the decision to submit it for publication.
Search strategy and selection criteria
MEDLINE 1966 to October 2004 and EMBASE 1980 to October 2004 were searched for: “marine poisoning”, “nerve conduction studies”, “neurotoxicity”, “ciguatera”, “tetrodotoxin poisoning”, and “shellfish poisoning”. Further articles were included from reference lists, review articles, and major textbook chapters on marine toxinology. Abstracts and reports from meetings were also included. The final reference list was generated based on originality and relevance to the topics covered in the review.
Revie
http://neurology.thelancet.com Vol 4 April 2
References1 Brusle J. Ciguatera fish poisoning—a review: sanitary
and economic aspects. INSERM: Paris, 1992.2 White J, Warrell D, Eddleston M, Currie BJ, Whyte IM, Isbister
GK. Clinical toxicology—where are we now? J Toxicol Clin Toxicol 2003; 41: 263–76.
3 Smart DR. Scombroid poisoning: a report of seven cases involving the Western Australian salmon, Arripis truttaceus. Med J Aust 1992; 157: 748–51.
4 Morrow JD, Margolies GR, Rowland J, Roberts LJ. Evidence that histamine is the causative toxin of scombroid-fish poisoning.N Engl J Med 1991; 324: 716–20.
5 Hall M. Something fishy: six patients with an unusual cause of food poisoning! Emerg Med 2003; 15: 293–95.
6 Meier J, White J. Handbook of clinical toxicology of animal venoms and poisons 1st edn. Boca Raton: CRC Press, 1995.
7 Waxman SG, Ritchie JM. Molecular dissection of the myelinated axon. Ann Neurol 1993; 33: 121–36.
8 Burke D, Kiernan MC, Bostock H. Excitability of human axons.Clin Neurophysiol 2001; 112: 1575–85.
9 Hille B. Ionic channels of excitable membranes. Sunderland, Massachussets: Sinauer Associates Inc, 1992.
10 Ogata N, Ohishi Y. Molecular diversity of structure and function of the voltage-gated Na+ channels. Jpn J Pharmacol 2002; 88: 365–77.
11 Porreca F, Lai J, Bian D, et al. A comparison of the potential role of the tetrodotoxin-insensitive sodium channels, PN3/SNS and NaN/SNS2, in rat models of chronic pain. Proc Natl Acad Sci USA 1999; 96: 7640–44.
12 Schnorf H, Taurarii M, Cundy T. Ciguatera fish poisoning:a double-blind randomized trial of mannitol therapy. Neurology2002; 58: 873–80.
13 Lewis RJ. The changing face of ciguatera. Toxicon 2001; 39: 97–106.14 Bagnis R, Kuberski T, Laugier S. Clinical observations on
3009 cases of ciguatera (fish poisoning) in the South Pacific.Am J Trop Med Hyg 1979; 28: 1067–73.
15 Bagnis R, Legrand AM. Clinical features of 12 890 cases of ciguatera (fish poisoning) in French Polynesia. In: Gopalakrishnakone P,Tan CK, eds. Progress in venom and toxin research 1st edn. Singapore: National University of Singapore and International Society of Toxinology, Asia Pacific Section, 1987: 372–77.
16 Gillespie NC, Lewis RJ, Pearn JH, et al. Ciguatera in Australia: occurrence, clinical features, pathophysiology, and management. Med J Aust 1986; 145: 584–90.
17 Johnson R, Jong EC. Ciguatera: Caribbean and Indo-Pacific Fish Poisoning. West J Med 1983; 138: 872–74.
18 Narayan Y. Fish poisoning in Fiji. Fiji Med 1980; 8: 567–74.19 Lawrence DN, Enriquez MB, Lumish RM. Ciguatera fish
poisoning in Miami. JAMA 1980; 244: 254–58.20 Morris JG, Lewin P, Smith WC, Blake PA, Schneider R.
Ciguatera fish poisoning: epidemiology of the disease on St Thomas, US Virgin Islands. Am J Trop Med Hyg 1982; 31: 574–78.
21 Lehane L, Lewis RJ. Ciguatera: recent advances but the risk remains. Int J Food Microbiol 2000; 61: 91–125.
22 Lewis RJ, Holmes MJ. Origin and transfer of toxins involved in ciguatera. Comp Biochem Physiol C 1993; 106: 615–28.
23 Connell JE, Colquhoun D. Risk of ciguatera fish poisoning: impact on recommendations to eat more fish. Asia Pac J Clin Nutr 2003; 12 (suppl): S67.
24 Mattei C, Molgo J, Marquais M, Vernoux J, Benoit E. Hyperosmolar D-mannitol reverses the increased membrane excitability and the nodal swelling caused by Caribbean ciguatoxin- 1 in single frog myelinated axons. Brain Res 1999; 847: 50–58.
25 Pearn J, Harvey P, De Ambrosis W, Lewis R, McKay R. Ciguatera and pregnancy. Med J Aust 1982; 1: 57–58.
26 Lucas RE, Lewis RJ, Taylor JM. Pacific ciguatoxin-1 associated with a large common-source outbreak of ciguatera in east Arnhem Land, Australia. Nat Toxins 1997; 5: 136–40.
27 Lange WR, Snyder FR, Fudala PJ. Travel and ciguatera fish poisoning. Arch Intern Med 1992; 152: 2049–53.
28 Lewis RJ, Chaloupka MY, Gillespie NC, Holmes MJ. An analysis
of the human response to ciguatera in Australia. Proc 6th Int Coral Reef Symp, Aust, 1988; 3: 67–71.

Revie
2 http://neurology.thelancet.com Vol 4 April
29 Goonetilleke A, Harris JB. Envenomation and consumption of poisonous seafood. J Neurol Neurosurg Psychiatry 2002; 73: 103–09.
30 Isbister GK. Data collection in clinical toxinology: debunking myths and developing diagnostic algorithms. J Toxicol Clin Toxicol 2002; 40: 231–37.
31 Berlin RM, King SL, Blythe DG. Symptomatic improvement of chronic fatigue with fluoxetine in ciguatera fish poisoning. Med J Aust 1992; 157: 567.
32 Fenner PJ, Lewis RJ, Williamson JA, Williams ML. A Queensland family with ciguatera after eating coral trout. Med J Aust 1997; 166: 473–75.
33 Strachan LC, Lewis RJ, Nicholson GM. Differential actions of pacific ciguatoxin-1 on sodium channel subtypes in mammalian sensory neurons. J Pharmacol Exp Ther 1999; 288: 379–88.
34 Lewis RJ, Hoy AW. Comparative action of three major ciguatoxins on guinea-pig atria and ilea. Toxicon 1993; 31: 437–46.
35 Cameron J, Flowers AE, Capra MF. Effects of ciguatoxin on nerve excitability in rats (part I). J Neurol Sci 1991; 101: 87–92.
36 Butera R, Prockop LD, Buonocore M, Locatelli C, Gandini C, Manzo L. Mild ciguatera poisoning: case reports with neurophysiological evaluations. Muscle Nerve 2000; 23: 1598–603.
37 Cameron J, Flowers AE, Capra MF. Electrophysiological studies on ciguatera poisoning in man (part II). J Neurol Sci 1991; 101: 93–97.
38 Palafox NA, Jain LG, Pinano AZ, Gulick TM, Williams RK, Schatz IJ. Successful treatment of ciguatera fish poisoning with intravenous mannitol. JAMA 1988; 259: 2740–42.
39 Pearn JH, Lewis RJ, Ruff T, et al. Ciguatera and mannitol: experience with a new treatment regimen. Med J Aust 1989; 151: 77–80.
40 Stewart MP. Ciguatera fish poisoning: treatment with intravenous mannitol. Trop Doct 1991; 21: 54–55.
41 Blythe DG, De Sylva DP, Fleming LE, Ayyar RA, Baden DG, Shrank K. Clinical experience with iv: mannitol in the treatment of ciguatera. Bull Soc Pathol Exot 1992; 85: 425–26.
42 Bagnis R, Spiegel A, Boutin JP, et al. Evaluation of the efficacy of mannitol in the treatment of ciguatera in French Polynesia.Med Trop (Mars) 1992; 52: 67–73.
43 Purcell CE, Capra MF,
Cameron J. Action of mannitol in ciguatoxin-intoxicated rats. Toxicon 1999; 37: 67–76.
44 Lewis RJ, Hoy AW, Sellin M. Ciguatera and mannitol: in vivo and in vitro assessment in mice. Toxicon 1993; 31:1039–50.
45 Lange WR, Kreider SD, Hattwick M, Hobbs J. Potential benefit of tocainide in the treatment of ciguatera: report of three cases.Am J Med 1988; 84: 1087–88.
46 Perez CM, Vasquez PA, Perret CF. Treatment of ciguatera poisoning with gabapentin. N Engl J Med 2001; 344: 692–93.
47 Pottier I, Vernoux JP, Lewis RJ. Ciguatera fish poisoning in the Caribbean islands and Western Atlantic.Rev Environ Contam Toxicol 2001; 168: 99–141.
48 Davis RT, Villar LA. Symptomatic improvement with amitriptyline in ciguatera fish poisoning. N Engl J Med 1986; 315: 65.
49 Calvert GM, Hryhorczuk DO, Leikin JB. Treatment of ciguatera fish poisoning with amitriptyline and nifedipine.J Toxicol Clin Toxicol 1987; 25: 423–28.
50 Kanchanapongkul J. Puffer fish poisoning: clinical features and management experience in 25 cases.J Med Assoc Thai 2001; 84: 385–89.
51 How C-K, Chern C-H, Huang Y-C, Wang L-M, Lee C-H. Tetrodotoxin poisoning. Am J Emerg Med 2003; 21: 51–54.
52 Kaku N, Meier J. Clinical toxicology of fugu poisoning. In: Meier J, White J, eds. Handbook of clinical toxicology of animal venoms and poisons 1st edn. Boca Raton: CRC Press, 1995: 75–83.
53 Isbister GK, Son J, Wang F, et al. Puffer fish poisoning: a potentially life-threatening condition. Med J Aust 2002; 177: 650–53.
54 Mahmud Y, Arakawa O, Noguchi T. An epidemic survey on freshwater puffer poisoning in Bangladesh. J Nat Toxins 2000; 9: 319–26.
55 Kanchanapongkul J, Kungsuwan A, Tantisiriwan V, Punthawangkun C, Krittayapoositpot P. An outbreak of horseshoe crab poisoning in Chon Buri, Thailand: clinical, toxicologic and therapeutic considerations.Southeast Asian J Trop Med Public Health 1996; 27: 806–09.

Revie
http://neurology.thelancet.com Vol 4 April 2
56 Tsai YH, Hwang DF, Chai TJ, Jeng SS. Occurrence of tetrodotoxin and paralytic shellfish poison in the Taiwanese crab Lophozozymus pictor. Toxicon 1995; 33: 1669–73.
57 Llewellyn LE, Dodd MJ, Robertson A, Ericson G, de Koning C, Negri AP. Post-mortem analysis of samples from a human victim of a fatal poisoning caused by the xanthid crab, Zosimus aeneus. Toxicon 2002; 40: 1463–69.
58 Hille B. The receptor for tetrodotoxin and saxitoxin: a structural hypothesis. Biophys J 1975; 15: 615–19.
59 Cestele S, Catterall WA. Molecular mechanisms of neurotoxin action on voltage-gated sodium channels. Biochimie 2000; 82: 883–92.
60 Baker MD, Bostock H. Low-threshold, persistent sodium current in rat large dorsal root ganglion neurons in culture. J Neurophysiol 1997; 77: 1503–13.
61 Kao CY. Tetrodotoxin, saxitoxin and their significance in the study of excitation phenomena. Pharmacol Rev 1966; 18: 997–1049.
62 Torda TA, Sinclair E, Ulyatt DB. Puffer fish (tetrodotoxin) poisoning: clinical record and suggested management. Med J Aust 1973; 1: 599–602.
63 Tibballs J. Severe tetrodotoxic fish poisoning.Anaesth Intensive Care 1988; 16: 215–17.
64 Littlewood R, Douyon C. Clinical findings in three cases of zombification. Lancet 1997; 350: 1094–96.
65 Kan SK, Chan MK, David P. Nine fatal cases of puffer fish poisoning in Sabah, Malaysia. Med J Malaysia 1987; 42: 199–200.
66 O’Leary MA, Schneider JJ, Isbister GK. Use of high performance liquid chromatography to measure tetrodotoxin in serum and urine of poisoned patients. Toxicon 2004; 44: 549–53.
67 Oda K, Araki K, Totoki T, Shibasaki H. Nerve conduction study of human tetrodotoxication. Neurology 1989; 39: 743–45.
68 Kiernan MC, Isbister GK, Lin CY, Burke D, Bostock H. Acute tetrodotoxin induced neurotoxicity following ingestion of puffer fish. Ann Neurol 2005; (in press).
69 Fukiya S, Matsumura K. Active and passive immunization for tetrodotoxin in mice. Toxicon 1992; 30: 1631–34.
70 Xu QH, Wei CH, Huang K, Rong KT. Toxin-neutralizing effect and activity-quality relationship for mice tetrodotoxin-specific polyclonal antibodies. Toxicology 2005; 206: 439–48.
71 Sorokin M. Puffer fish poisoning. Med J Aust 1973;1: 957.72 Southcott RV. Australian venomous and poisonous fishes.
Clin Toxicol 1977; 10: 291–325.73 Ribes GC, Ramarokoto S, Rabearintsoa S, et al. Seafood poisoning
in Madagascar: current state of knowledge and results of a retrospective study of the inhabitants of coastal villages. Sante 1999; 9: 235–41.
74 Lehane L. Paralytic shellfish poisoning: a potential public health problem. Med J Aust 2001; 175: 29–31.
75 Gessner BD, Middaugh JP. Paralytic shellfish poisoning in Alaska: a 20-year retrospective analysis. Am J Epidemiol 1995; 141: 766–70.
76 Llewellyn LE. Human fatalities in Vanuatu after eating a crab (Daira perlata). Med J Aust 2001; 175: 343–44.
77 Lagos N, Onodera H, Zagatto PA, Andrinolo D, Azevedo SMFQ, Oshima Y. The first evidence of paralytic shellfish toxins in the freshwater cyanobacterium Cylindrospermopsis raciborskii, isolated from Brazil. Toxicon 1999; 37: 1359–73.
78 Ritchie JM, Rogart RB. The binding of saxitoxin and tetrodotoxin to excitable tissue. Rev Physiol Biochem Pharmacol 1977; 79: 1–50.
79 Rodrigue DC, Etzel RA, Hall S, et al. Lethal paralytic shellfish poisoning in Guatemala. Am J Trop Med Hyg 1990; 42: 267–71.
80 Usleber E, Dietrich R, Burk C, Schneider E, Martlbauer E. Immunoassay methods for paralytic shellfish poisoning toxins. J AOAC Int 2001; 84:1649–56.
81 Usleber E, Donald M, Straka M, Martlbauer E. Comparison of enzyme immunoassay and mouse bioassay for determining paralytic shellfish poisoning toxins in shellfish. Food Addit Contam 1997; 14: 193–98.
82 Bire R, Krys S, Fremy JM, Dragacci S. Improved solid-phase extraction procedure in the analysis of paralytic shellfish poisoning toxins by liquid chromatography with fluorescence detection.J Agric Food Chem 2003; 51: 6386–90.
83 Schantz EJ. Historical perspective on paralytic shellfish poisoning. In: Ragelis EP, ed. Seafood toxins. Washington DC: American Chemical Society, 1984: 99–111.
84 Long RR, Sargent JC, Hammer K. Paralytic shellfish poisoning: a case report and serial electrophysiologic observations. Neurology 1990; 40: 1310–12.
85 De Carvalho M, Jacinto J, Ramos N, De Oliveira V, Pinho e Melo T, de Sá J. Paralytic shellfish poisoning: clinical and electrophysiological observations. J Neurol 1998; 245: 551–54.
86 Morris PD, Campbell DS, Taylor TJ, Freeman JI. Clinical and epidemiological features of neurotoxic shellfish poisoning in North Carolina. Am J Public Health 1991; 81: 471–74.
87 Ishida H, Muramatsu N, Nukaya H, Kosuge T, Tsuji K. Study on neurotoxic shellfish poisoning involving the oyster, Crassostrea gigas, in New Zealand. Toxicon 1996; 34: 1050–53.
88 Baden DG. Brevetoxins: unique polyether dinoflagellate toxins.FASEB J 1989; 3: 1807–17.
89 Vale P, Sampayo MAM. Domoic acid in Portuguese shellfish and fish. Toxicon 2001; 39: 893–904.
90 Perl TM, Bedard L, Kosatsky T, Hockin JC, Todd EC, Remis RS. An outbreak of toxic encephalopathy caused by eating mussels contaminated with domoic acid. N Engl J Med 1990; 322: 1775–80.
91 Sierra-Beltran AP, Cruz A, Nunez E, Del Villar LM, Cerecero J, Ochoa JL. An overview of the marine food poisoning in Mexico. Toxicon 1998; 36: 1493–502.
92 Wekell JC, Gauglitz EJ Jr, Barnett HJ, Hatfield CL, Simons D, Ayres D. Occurrence of domoic acid in Washington state razor clams (Siliqua patula) during 1991–1993. Nat toxins 1994;2: 197–205.
93 Teitelbaum JS, Zatorre RJ, Carpenter S, et al. Neurologic sequelae of domoic acid intoxication due to the ingestion of contaminated mussels. N Engl J Med 1990; 322: 1781–87.
94 Glavin GB, Pinsky C, Bose R. Mussel poisoning and excitatory amino acid receptors. Trends Pharmacol Sci 1989; 10: 15–16.
95 Onuma Y, Satake M, Ukena T, et al. Identification of putative palytoxin as the cause of clupeotoxism. Toxicon 1999; 37: 55–65.
96 Frelin C, Van Renterghem C. Palytoxin: recent electrophysiological and pharmacological evidence for several mechanisms of action. Gen Pharmacol 1995; 26: 33–37.
97 Taniyama S, Mahmud Y, Terada M, Takatani T, Arakawa O, Noguchi T. Occurrence of a food poisoning incident by palytoxin from a serranid Epinephelus sp in Japan. J Nat Toxins 2002;11: 277–82.
98 Boisier P, Ranaivoson G, Rasolofonirina N, et al. Fatal mass poisoning in Madagascar following ingestion of a shark (Carcharhinus leucas): clinical and epidemiological aspects and isolation of toxins. Toxicon 1995; 33: 1359–64.