management of rampant earies in children
TRANSCRIPT

Pediatnc Dentistry
Management of rampant earies in childrenCyntbia K, Y, Viu* /Stephen H, Y, Wei**
Because research has resulted in a better understanding of tht etiology of dental cariesas well as the introduction of rtew techniques and tnaterials in the practice of dentistry,approaches toward the management of rampant caries should be reevaluated. Thedevelopmetu of the acid-etching technique and the improvements in the physicalproperties and clmical performance of composite resins and glass-ionomer cementshave cotnpletely changed the concepts of prevention, conservative dentistry, and dentalesthetics. Several methods for the treatment of rampant caries are described andmanagement of two cases is documented. (Quintessence Int 1992;23:159-168.)
Introduction
Rampant caries has been described by Winter et al' asa lesion of acute onset involving many or all of theerupted teeth, rapidly destroying corona! tissue, oftenon surfaees normally immune to decay, and leading toearly involvement of the dental pulp. In a recentstudy, subjects with active, rampant dental caries weredefined as those who had five or more new carious sur-faces per year." It is perhaps one of the most difficultand challenging conditions confronting the dentalpractitioner from both a preventive and managementstandpoint.
The purpose of this article is to give an overview ofthe condition and outline a management programbased on current knowledge and techniques.
Clinical appearance
The pattern of rampant earies in the primary dentitionis usually related to the order of tooth eruption, with
Clinical Denial Surgeon, Department of Ctiildren's Dentistryand Orlhodoncics. Faculty of Dentistry, University of HongKong, Prince Philip Dental Hospital, 34 Hospital Road, Hong
Professor and Head, Department of Children's Dentistry and Or-thodonties. Dean, Faculty of Dentistry, University of Hong Kong,
the exception of the mandibular primary incisor. Themandibular incisors are probably more resistant tocaries because of their close proximity to the secretionsof the submandibular salivary glands as well as theeleansing action of the tongue during the process ofsuckling the bottle.
The initial lesion usually appears on the labial sur-face of the maxillary incisors, close to the gingivalmargins, as a whitish aiea of deealeifieation or pittingof the enamel surface shortly after eruption. Theselesions soon become pigmented to a light yellow andat the same time extend laterally to the approximalsurfaces and downward to the incisai edge. Less com-monly, the deealeifieation may present initially on thepalatal surfaces, or even at the incisai edge in someextreme cases,' At a more advanced stage, the cariousprocess will often extend around the eircumferenee ofthe tooth, leading to pathologic fracture of the crownon minimal trauma. Other teeth, namely the firstprimary molars, the second primary molars, and even-tually the canines, will gradually become involved.
Nursing bottle caries, also known by a number ofother names, such as bottle caries, baby bottle syn-drome, and baby bottle tooth decay, is a form of ram-pant dental earies in the primary dentition of infantsand children. In most cases, the problem is found in aninfant who frequently falls asleep with a baby bottlefilled with milk or sugar-eontaining substances,•*"' eg,vitamin C syrup, sweetened fruit juice, or even carbon-
Quintessence International Volume 23, Number 3/1992 159

Pédiatrie Dentistry
ated drinks. The condition can also be associatedwith breast-fed infants who have prolonged feedinghabits'*' or with children whose pacifiers arc frequentlydipped in honey, sugar, or syrup.'' The decrease insalivary flow rate during sleep, as well as the poolingof sweei fltjids around the teeth, results in a highlycariogenic environment.
Rampant caries may also occur in the permanentdentition of teenagers, because of their frequent in-take of cariogenic snacks and sweet drinks betweenmeals. Typical rampant caries in adolescents is charac-terized by buccal and lingual caries of premolars andmolars and proximal and iabial caries in the mandi-bular incisors. Johnsen et al'" have shown that childrenwith nursing caries who are receiving ongoing com-prehensive dental care are more susceptible to lesionsin approximal surfaces of primary molars than arechildren who are initially caries free. As a result, infantswith rampant caries are likely to develop the samecondition in the permanent teeth unless successfulpreventive measures have been implemented.
A specific form of rampant caries tiiay occur in chil-dren and adolescents who have a greatly reduced sali-vary flow as a result of radiotherapy for the treatmentof cancer of the head and neck region or as a result ofthe surgical retnoval of neoplasms in the oral cavity.
Etiology
The two major predisposing factors in rampant cariesare a specific microorganism atid diet.
Microorganistn
Streptococcus muians is an important pathogen in thedevelopmetit of detital caries."'" Several clinicalstudies have shown that S mutons cannot be detectedin the mouths of normal, predentate infants.'•*''' Themicroorganisms are usually not detectable in themouths of infants until the later stage of incisor emer-gence.'^ The relative absence of S muians prior to thisstage of dental development indicates that the presenceof these microorganisms is associated with primaryinfection, and the main source of S mutans in primaryinfection is usuaily the mother.'' ""' Berkowitz et al''found a significant relationship between the salivaryS mutans level in the mother and the risk of infectionin the infant. In addition, the frequency of infantinfection is approximately tiine times greater whenmaternal salivary levels of S mutans exceed 10 colony-forming units (CFUs)/mL of saliva, than when maternalsalivary levels are less than 10' CFUs/mL. Similar
studies using bactcriocin testing of S muians frommother-infant pairs have suggested that S muluivi istransferred from mothers to infants.^""'
Plaque and saliva from children with nursing carieshave been found to contain unusually high levels ofS muttins."'^ Van Houte et al" demonstrated that Smuians constitutes about 60% of the cultivable flora ofdental plaque obtained from earious lesions, marginsof white-spot lesions, and clinically sound enamelsurfaces of preschool children with nursing caries. Inchildren with little or no caries, S mutans constitutesless than 1% of the flora." Milnes and Bowden'''showed that, besides S mutans, Veillonella is also foundin significantly higher amounts in plaque samplestaken from maxillary incisors than it is in samples fromthe mandibular incisors. Boue et ah^ found a similarbacterial distribution, consisting of high levels of 5mutans, Lactobacilhts. and Veillonella in black-pigmentedand unstained lesions in young children who developedrampant caries.
The eariogenicity of S mutans is probably related toits unique combination of properties, which include(/) colonization of the teeth (2) production of largeamounts of extracellular polysaccharide that enablevoluminous plaque formation, (3) production of largeamounts of acids, even at low pH, and (4¡ breakdownof salivary glycoprotein, which might be of greatimportance for the initial development oí cariouslesions.^' The correlation between 5 muuins levels anddental caries has been used to identify children whoare at "high risk" for caries attack. It is important thatsuch children be identified and given preventive treat-ment before they develop rampant decay. However,although S mutans and Lactobacilhts are strongly as-sociated with dental caries, several other factors caninteract to determine the risk of dental caries:
Number ofcariogenic microorganisms x virulence x time x diet
Protective mechanisms
Local protective mechanisms are anatomy fluoridesand other trace elements. General protectivejnechanisms are immune atid nonimmune factors insaliva and gingival crevicular fluid.-"
Diei
The carbohydrate component of the diet is associatedwith the formation of dental caries. The classicSwedish Vipeholm study demonstrated that cariogenicpotential is closely related to the texture ot ilie carbo-hydrate and the frequency of consumption of sticky
160 Quintessence International Volume 23, Number 3/1995
Pédiatrie Dentistry
sugars, rather than to the amount of sugar eaten.-'The carbohydrate provides the plaque bacteria withthe substrate for acid production and for tlie synthesisof exttacelhilar polysaccharides. Low-molecular-weight carbohydrates (eg, sugar), which readily diffuseinto plaque and are metabolized by plaque bacteria,are more cariogenic than are complex carbohydrates{eg, starch).
Sucrose, in particular, has been considered to be themost cariogenic sugar in the hnman diet, because (1) itis a small, uncharged molecule that easily diffuses intothe dental plaques, (2) it Is highly soluble and acts as asubstrate both for the production of e.^itracellularpolysaceharides and for acid production, ¡3) it favorsthe estabhshmeni of S muians on teeth, and a highsucrose intake gives rise to voluminous amount ofplaque formation, and ¡4) it does not contain substancesthat can inhibit plaque bacteria or form a protectivecoating on the enamel surface of teeth in children whoare introduced to sweet foods early in their infancy.^^Several clinieal studies have shown thai the cause ofnursing caries is prolonged botile feeding with sweeifluids, particularly during nap times.""'
There is some controversy as to whether bovine andhreast milk are cariogenic. Bovine milk contains highconcentrations of calcium and phosphorus, whichcould contribute to the reminerahzation of enamel.Breast milk contains a higher content of lactose thanbovine milk, and therefore possesses a greater cario-genic potential. Hackett et al,'' however, concludedthat, although it is possible for breast and bovine milkto cause dental caries, the prevalence is low and is as-sociated with frequent and prolonged breast or bottlefeeding, during the day and night, until the child is 2or more years old.
Parents frequently provide their children with freshlysqueezed or commercially prepared fruit juices becauseof the belief that they contain large quantities of vita-min C. The parents are, however, unaware of the highsugar content of fruit juices, their acidic pH. whichcan range from 3 to 4, and their erosive effect ondental enamel."'^ Erosion is particularly harmful in theprimary dentition, because the layer of dental enameland dentin is much thinner than in the permanentdentition.
Prevalence
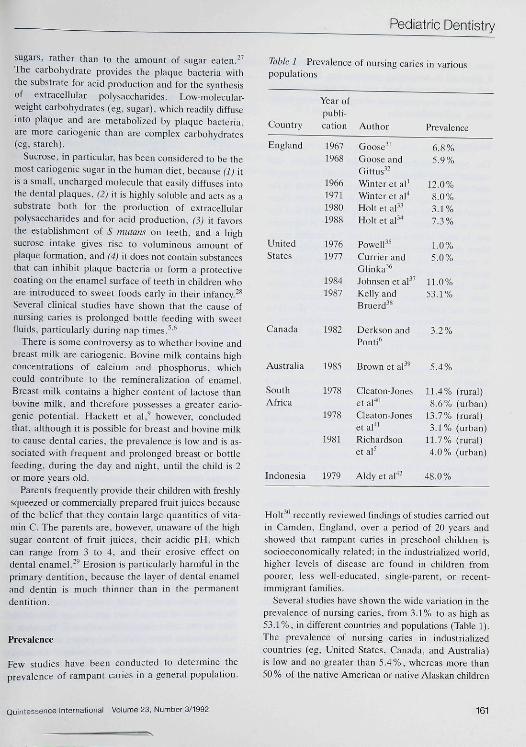
Few studies have been conducted to determine theprevalence of rampant caries in a general population.
Table I Prevalence of nursing caries in variotispopulations
Country
England
UnitedSlates
Year ofpubli-cation
19671968
1966197119801988
19761977
Author
Goose''Goose andGittus"Wnter et al'Winteretal''Holt et al"Holt et al'''
Powell^^Currier and
Prevalence
6.8%5.9%
12.0%8.0%3.1%7.3%
1.0%5.0%
1984 Johnsen et a P 11.0%1987 Kelly and 53.1%
Bruerd^^
Canada 1982 Derkson andPonti*
3.2%
Australia 1985 Brown et aP
SouthAfrica
Indonesia
1978
1978
1981
1979
Cleaton-Joneset al*Cleaton-Joneset al*"Richardsonetal^
Aldy et al"'-
11.4%8.6%
13.7%3.1%
11.7%4.0%
48.0%
(ruTal)(urban)(rural)(urhan)(rural)(urban)
Hoir' ' recently reviewed findings of studies carried outin Camden, England, over a period of 20 years andshowed that rampant caries in preschool children issocioeconomically related; in the industrialized world,higher levéis of disease are found in children frompoorer, less well-educated, single-parent, or recent-immigrant families.
Several studies have shown the wide variation in theprevalence of nursing caries, from 3.1% to as high as53.1%, in different countries and populations (Table 1).The prevalence of nursing caries in industrializedcountries (eg. United States, Canada, and Australia)is low and no greater than 5.47o, whereas more than50% of the native American or native Alaskan children
Quintessence International Voiume 23, Number 3/1992 161
Pédiatrie Dentistry
have tiursing caries, A high prevalence of nursing cariesis observed in developing countries (eg. South Africaand various parts of Asia) and is probably related tothe increase in consumption of sugar containing foods,drinks, and confectionary,
li-eatment
The type of treatment instituted for patients withrampant caries depends on the patient's and parents'motivation toward dental treatment, the extent of thedecay, and the age and cooperation of the child. Thesefactors shouid be assessed during the child's first fewvisits to the dentist. Restorative dentistry is expensiveand. by itself, is not a complete cure for rampant caries.Many practitioners have gone to considerable effortsto restore all the teeth in subjects with high-cariesactivity only to find new lesions within a very shorttime. Initial treatment, ineluding provisional restora-tions, diet assessment, oral hygiene instruction, andhome and professional fluoride treatments, should beperformed before any comprehensive restorative treat-ment commences. The initial therapy will help thedentist to determine the ultimate success or failure ofthe case.
Caries stabilization and provisional restorationsshould be placed in symptom-free teeth with establisheddentinal caries to minimize the risk of pulpal exposurein the future and to improve function. However, inpatients presenting with acute and severe signs andsymptoms of gross caries, pain, abscess, sinus, or facialswelling, immediate treatment is indicated, Formoeresolpulpotomy may be performed if the pulp is still vital,but pulpeetomy followed by obturation with formalizedzinc oxide-eugenol cement is indicated if the pulp isnonvital.
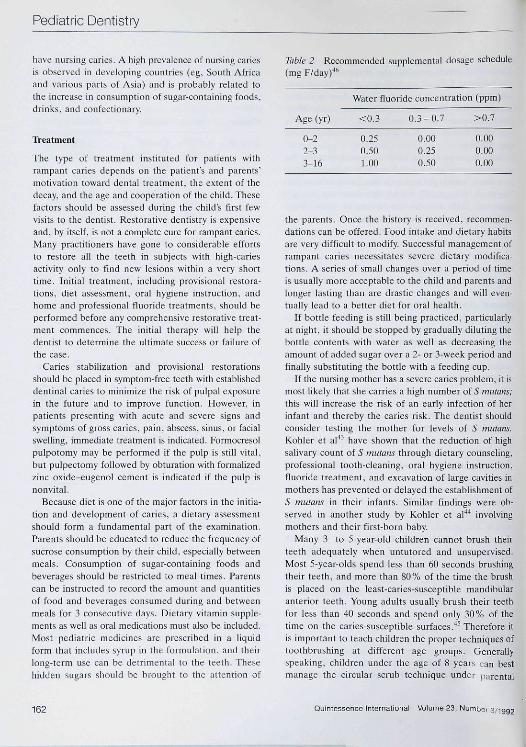
Because diet is one of the major factors in the initia-tion and development of caries, a dietary assessmentshould form a fundamental part of the examination.Parents should be educated to reduce the frequency ofsucrose consumption by their child, especially betweenmeals. Consumption of sugar-containing foods andbeverages should be restricted to meal times. Parentscan be instructed to record the amount and quantitiesof food and beverages consumed during and betweenmeais for 3 consecutive days. Dietary vitamin supple-ments as well as oral medications must also be included.Most pédiatrie medicines are prescribed in a liquidform that includes syrup in the formulation, and theirlong-term use can be detrimental to the teeth. Thesehidden sugars should be brought to the attention of
Table 2 Recommended supplemental dosage schedule{mg F/day)-""
Age (yr)
0-22-33-16
Water fluoride coticentration (ppm)
<0,3
0,250-5«I.Ofl
0,3-0.7
0,000.250-50
>0,7
0.000,000,00
the parents, Onee the history is received, recommen-dations can be offered. Food intake and dietary habitsare very difficult to modify. Sueeessful management oframpant caries neeessitates severe dietary modifica-tions, A series of small changes over a period of timeis usually more acceptable to the child and parents andlonger lasting than are drastic changes and will even-tually lead to a better diet for oral health.
If bottle feeding is still being practiced, particularlyat night, it should be stopped by gradually diluting thebottle contents with water as well as decreasing theamount of added sugar over a 2- or 3-week period andfinally substituting the bottle with a feeding eup.
If the tiursing mother has a severe caries problem, it ismost likely that she carries a high number of 5 mutans;this will increase the risk of an early infection of herinfant and thereby the caries risk- The dentist shouldconsider testing the mother for levels of S mutatis.Köhler et al''' have shown that the reduction of highsalivary count of S mutans through dietary counsehng,professional tooth-cleaning, oral hygiene instruction,fluoride treatment, and excavation of large cavities inmothers has prevented or delayed the establishment of5 mutans in their infants. Similar findings were ob-served in another study by Köhler et al'*'' involvingmothers and their first-bom baby.
Many 3- to 5-year-old children cannot brush theirteeth adequately when untutored and unsupervised.Most 5-year-olds spend less than 60 seconds brushingtheir teeth, and more than 80% of the time the brushis piaced on the least-caries-susceptible mandibularanterior teeth. Young adults usually brush their teethfor less than 40 seconds and spend only 30% of thetime on the caries-susceptible surfaces,"*^ Therefore itis important to teach children the proper techniques oftoothbrushing at different age groups. Generallyspeaking, children under the age of 8 years <;an bestmanage the circular scrub technique under narental
162 Quintessence International Volume 23, t^umber 3/1992

Pédiatrie Dentistry
Table 3 Fluoride treatment for children with rampant caries (0.3 to Ü.7 ppm water tluoride level)'"'
0-2 yr 2-3 yr 3-13yr >13Yr
Dietary fluoridesupplement
Operator-appliedtopical tluoride
Self-appliedtopical fluoride
Fluoridedentifrice
Not indicated
APF topical solutionor gel, 1.23% F,applied four times ayear
Not indicated
Brush withF-COntainingdentifrice
O.25tngFdaily
APF topical solutionorgel.l.23%F,applied four times ayear
Not indicated
Brush withF-eontainingdentifrice
0.5mgFdaily
APF topical solutionor gel, 1.23% F,applied four times ayear
Self-application ofgel-tray daily forapproximately 4weeks; thereaftercontinue with adaily fluoride rinse(0.05% NaF)
Brush withF-eontainingdentifrice
Not indicated
APF topical solutionorgel,].23%Fapplied four timesayear
Self-application ofgel-tray daily forapproximately4weeks; thereaftercontinue with adaily fluoride rinse(0.05 % NaF)
Brush withF-containingdentifrice
supervision, whereas, after the age of 11 to 12 years, asulcular brushing technique, eg, the Bass technique,can be taught. The use of disclosing tablets is a usefulaid to demonstrate to children the presence and distri-bution of dental plaque on the teeth. Interdentalcleaning should be introduced to adolescents with ayoung permanent dentition to remove interdentalplaque that is inaccessible with normal toothbrushing.
Both systemic and topical fluoride treatments areuseful for preventing dental caries; the choice dependson the level of fluoride in the drinking water and thestage of development of the dentition. The Council onDental Therapeutics of the American Dental Associa-tion'^ has recommended a dosage schedule for fluoridesupplementation of children at various ages accordingto the level of fluoride in the drinking water (Table 2).Children with a primary dentition will benefit fromboth fluoride tablets and the use of a small amount offluoride toothpaste. The child should be encouragedto chew or suck the tablet, preferably at bedtime.This provides a topical effect on dental enamel of theerupted teeth followed by a systemic effeet on develop-ing enamel after swallowing. Dietary fluoride supple-ments should be given, flrst, to those in whom preser-
vation of a caries-free dentition is particularly impor-tant, eg, those with elefts and hypodontia and themedically compromised, and, second, to those whoare especially prone to caries, eg, those with the firstsign of caries in the primary dentition by the age of 5years.""' Parents are instructed to use only a smallpea-sized amount of dentifrice for their young ehildand to remind their children to rinse and expectoratethoroughly after toothbrushing to avoid excessive in-gestion of fluoride from toothpaste. Periodic topicalfluoride therapy with an acidulated phosphate fluoride(APF) gel or fluoride varnish is useful in children withrampant caries to prevent further tooth destruction.The value of systemie therapy decreases with age, asthe permanent teeth are calcined and erupt, so fluoridetablets are not prescribed for older children and adoles-cents. However, fluoride toothpastes, fluoride mouth-rinses, and professionally apphed topical fluoride areof significant value. Tables 3 and 4 summarize themethods of fluoride treatment and other methodsused for the prevention of rampant caries in differentage groups.
Once rampant caries is under control, comprehensiverestorative treatment can be carried out. Restorative
Quiniessence International Voiume 23, Number 3/1992 163
Pediatnc Dentistry
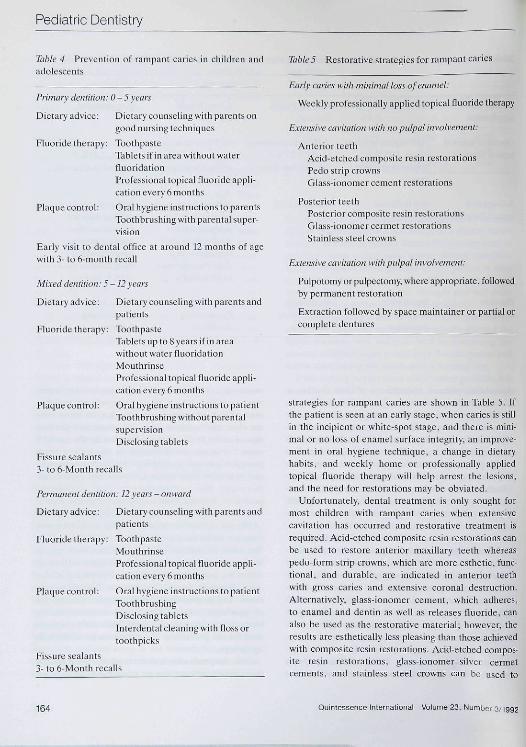
Table 4 Prevention of rampant caries in children andadolescents
Primary dentition: 0-5years
Dietary adviee: Dietary eoutiseling with parents ongood nursing techniques
Fluotide therapy: ToothpasteTablets if in area without waterfluoridationProfessional topical fluoride appli-cation every 6 months
Plaque control: Oral hygiene instructions to parentsToothbrushing witb parental super-vision
Early visit to dental office at around 12 tnonths of agewith 3- to 6-motith recall
Mixed detitition: 5-12 years
Dietary advice: Dietary counseling with parents andpatients
Fluoride therapy: TootbpasteTablets up to 8 years if in areawitbout water fluoridationMouthrinseProfessional topical fluoride appli-cation every 6 months
Plaque control: Oral hygiene i nstructions to patientToothbrushing without parentalsupervisionDisclosing tablets
Fissure sealants3-to 6-Month reealls
Pertnanent dentition: 12 years - onward
Dietary advice: Dietarycounselingwith parents andpatients
Fluoride therapy: ToothpasteMouthrinseProfessional topical fluoride appli-cation every 6 months
Plaque control: Oral hygiene instructions to patientToothbrushingDisclosing tabletsInterdental cleaning with floss ortoothpicks
Fissure sealants3- to 6-Month recalls
Table 5 Restorative strategies for ratnpant earies
Eariy caries with minimal loss of enamel:
Weekly professionally applied topical fluoride therapy
Extensive cavitation with no puipai involvement:
Anterior teethAcid-etched composite resin restorationsPedo strip crownsGlass-ionomer cement restorations
Posterior teethPosterior composite resin restorationsGlass-ionomer cermet restorationsStainless steel crowns
Extensive cavitation with pulpal involvement:
Pulpotomy or pulpectomy, where appropriate, followedby permanent restoration
Extraction followed by space maintainer or partial orcomplete dentures
strategies for rampant caries are shown in Table 5, Ifthe patient is seen at an early stage, when caries is stillin the incipient or white-spot stage, and there is mini-mal or no loss of enamel surface integrity, an improve-ment in oral hygiene technique, a change in dietaryhabits, and weekly home or professionally appliedtopieal fluoride therapy will help arrest the lesions,and the need for restorations may be obviated,
Utifortunateiy, dental treatment is only sought formost children with rampant caries when extensiveeavitation has occurred and restorative treatment isrequired. Acid-etched composite resin restorations canbe used to restore anterior maxillary teeth whereaspedo-form strip crowns, which are more esthetic, func-tional, and durable, are indicated in anterior teethwith gross caries and extensive coronal destruction.Alternatively, glass-ionomer cement, which adheres,to enamel and dentin as well as releases fluoride, canalso be used as the restorative material; however, theresults are esthetieally less pleasing than those achievedwith eotnposite resin restorations. Acid-etched compos-ite resin restorations, glass-ionomer-silver cermeteements, and .stainless steel crowns can he used to
164 Quintessence International Volume 23, Number 3/1992

Pédiatrie Dentistry
Fig 1 Intraoral photograph of a 4-year-old child with ram-pant caries.
Fig 2 Immediately postoperative photograph of the samepatient.
Fig 3 A maxillary occlusal view showing the distribution ofcaries in the teeth.
Fig 4 The carious teeth have been restored with stainlesssteel crowns and acid-etched anterior and postericr com-posite resin restorations.
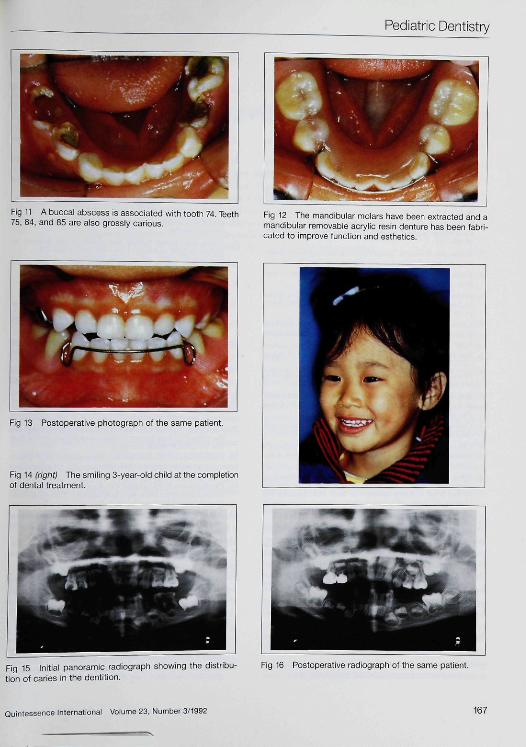
restore the posterior teeth. Depending on the extentof the lesions, pulpotomies. pulpectomies, or extractionmay be indicated. Where extractions of teeth havebeen carried out, a prosthesis should be provided forspace maintenance, function, and esthetics. Manage-ment of ratnpant caries in two children is shown inFigs 1 to 16.
Summary
Rampant caries is a distressing clinical condition con-fronting the child, parents, and dentist. With the ad-vances in knowledge about the etiology and patho-genesis of dental caries, rampant caries can now beprevented. Successful managenient of rampant cariesdepends on a coordinated team approach among the
pediatrician, pédiatrie dentist, parents, and child. Thepediatrician should educate the parents about goodnursing and dietary habits and the importance of goodoral hygiene to their child's teeth and should encourageparents to bring their child to the dental office beforehe or she is 12 months of age for a screening examina-tion and counseling, because pediatricians are oftenthe first medical personnel to see the newborn baby.
Pédiatrie dentists, who are more experienced in theimplementation of preventive and restorative dentistryto infants and young children, should play a vital role inthe management of rampant caries in children. However,interest and cooperation from the parents and childrenare equally important. Consequently, educational effortsshould be emphasized and reinforced, especially inareas where the prevalence of rampant caries is high.
Quintessence International Volume 23, Number 3/1992 165

Pédiatrie Dentistry
Fig 5 A mandibular occlusal view showing the distribution Fig 6 The carious teeth have been restored with stainlessof caries in the teeth. steei crowns and acid-etched anterior composite resin res-
torations.
Fig 7 Initial panoramic radiograph showing the distribu- Fig 8 Immediately postoperative radiograph of the sametion of caries In the dentition. patient
Fig 9 initial intraorai photograph of a 3-year-old child withcarious invoivement of the maxiiiary molars.
Fig 10 The carious moiars have been restored with stain-less steel crowns and acid-etched posterior compositeresin restorations.
166 Quintessence Internationai Volume 23, Number 3/1992
Pédiatrie Dentistry
Fig 11 A buccal abscess is associated with tooth 74. Teeth Fig 12 The mandibular molars have been extracted and a75, 84, and 85 are also grossly carious. mandibular removable acrylic resin denture has been fabri-
cated to improve functicn and esthetics.
Fig 13 Postoperative photograph of the same patient
Fig 14 (right) The smiling 3-vear-old child at the completionof dental treatment.
Fig 15 Initial panoramic radiograph showing the distribu-tion of caries in the dentition.
Fig 16 Postoperative radiograph of the same patient.
Quintessence International Volume 23, Number 3/1992 167

Pédiatrie Dentistry
References
1. Winter GB. Hamilloii MC, James PMC; Role of the tomforlcras an acliologii;al factor in rampanl caries of (lie deciduousdentition. Ardi D/.v Cliitd l%6;417:21)7-212.
2. Tinanoff N. Klock 13, Camosei DA. et al: Microbiologie ef-fects of SnF, und NaF moulhrinses in subjecls with high cariesactivily: results after one year. J Dem Res t9«3;62:yO7-9tl.
3. Pills AT: Some observation in Ihc occurrence of caries in veryyoung children. Br DcniJ l')27;48:197-214.
4. Winter GB. Rule DC, Mailer GP. cc al: The prevalence ofdental caries in preschool children aged I lo 4 years. Br DemJ 1971:130:271-277.
5. Richardson BD, Cleaton.Jones PE, Mclnnes PM. et al: Infamfeeding praelieeí and nursing bottle caries. / Dem ChiUI I'iSl ;48.423-129.
6. Derkson GD, Ponli P: Nursing bottle syndrome: prevalenceand etiology in a non-fluoridated city. J Ciiii Dtm Ajisoc 1982;43:3S9-393.'
7. Marino RV. Bomze K. Scholl TO. et al: Nursing bottle caries,characteristics of children at risk. Clin Peiliulr iy89:2S:t29-131.
8. Kotlow LA: Breast feeding. A cause of ttental caries in chil-dren. J Dem Child 1977:44:192-iy3.
9. Hacketl AF, Rugg-Gunn AJ. Murray JJ. et al: Can breastfeeding cause dental earies? Hum Niiir AppI Nuir 1984;38(1):23-28.
10. Johnsen DC, Gerstenmaier JH, DiSantis TA, et al: Suscepti-bility of nursing-caries children to future approximal molardecay. PeJiaIr Dem 1986;16S-17Ü.
11. Van Houte J: Baeterial speeificity in the etiology of dentalearies. Im Dem J 198n;3O:3O5-32ñ.
12. Hamada S, Slade HD: Biology, immunology and cariogenicityof SirepiacocciLi mmims. Mk'Oh Rev 1980;44:331-384.
t3. Berkowitz RJ, Jordan HV, White G: The early establishmentof Sireplococciis mulam in the month of infants. Arch OralBiol 1975 ;20:171-174.
14. Carlsson J. Grahnen H, Jonsson G: Lactobacilli and strepto-coeci in the mouth of children. Cark-s Re.i 1975:9:333-339.
15. Catalanotto FA, Shklair IC, Keene HJ: Prevalenee and loeali-îation of Siiepiocacciis mmam; in infants and children. / AmDem Assoc 1975:91:606-609.
16. Stiles HM. Meyers R. Brunelle JA. et al: Occurrence ofSireplacoccus imttans and Slreplococcus sangiiis in the oral esv-ity and feces of young children, in Stiles HM, Loesche WJ,O'Brien TC (eds): Mkrvbiat Aspeçti of Dumat Caries, vol 1.Washmgton, DC, Information Retrieval Ltd, 197fi. pp 187-199.
17. Berkowitz RJ: Slrepwcoccus miilans and dental caries in in-fants. Competid Comin Edui Dem I985;6:463^66.
18. Berkowit; RJ, Turner J, Green P: Primary oral infectionof infants with Sireploeoecus mulans. Arch Orat Biolt980;25:221-224.
19. Berkowitz RJ. Turner J. Green P: Maternal salivary levels ofSirepl'Koceiis mulam and primary oral infection of infants.Arch Oral Biot 1981,26:147-149.
20. Berkowitz KS. Jordan HV: Similarity of baeterioeins of Sirep-loeoecus mulans from mother and infant. Arch Oral Biol
21. Masuda N, Shimamato T, Sobue S, et al: Transmission ofSircptococciis mulans in some selected families. ./ Dem Re\1980;59:463 (abstr No. 7S4).
22. Van Houte J, Gibbs G. Butera C: Oral llora of children with"nursin" botilc caries." J Dent Rc.i 1982:61:382-385.
23. Berkowitz RJ. Turner J, Hughes C: Microbial characteriilicsof the human denial caries associated with prolonged botllefeeding. Arch Orat Biol I984;29:949-951.
24. Milnes AR, Bowden GHW: The niicroflora associated withdeveloping lesions of nursing caries. Caries Re.i 1985:19:289-297.
25. Boue D, Armau E, Tiraby G: A bacteriological study oframpant caries in children. J Dem ties 1987;66:23-28.
26. Krasse B: Specific microorganisms <ind dental earies in chil-dren. Pedialrician 1989; Ifi: 156-16(1.
27. Gustaffson BE, Ouensel CE, Lanke LS, et al: The Vipeholmdental caries study./I cm Odomot Semid 1954; I h 232-264.
28. Krasse B: Carles Rist(—A Praclicat Guide for Asscssmem andComrol. Chicago, Quintessence Publ Co. 1985, p 24.
29. Smith AJ, Shaw C: Baby fruit juices and tooth erosion. B:Draiy 1987;162:65-67.
30. Holt RD: Caries in preschool children: British trends. ] Dem1990; 18:296-299.
31. Goose DH: Infant feeding and caries of the incisors: anepidemiological approach. Curies Res 1967:1 :lñ7-l73.
32. Goose DH. Gittus E: Infant feeding methods and dentalcaries. Piibtk Heatlh 1968,82:72-76.
33. Holt RD, Joels D, Winter GB: Caries in preschool children.TheCamden study. Br Dem J 1982:153:107-109.
34. Holt RD, Joels D, Bulman J, et al: A third study of earies inpresehool aged children in Camden. BrDe/i / / 1988;i65:S7-91.
35. Powell D: Milk. Is it related to rampant caries of the earlyprimary dentition? / Calif Dem Assoc 1976;4:58-63.
36. Currier GF. Glinka MP: The prevalence of nursing bottlecaries or baby bottle syndrome in an inner city fluoridatedeommunity. Va Dem J 1977:54:9-19.
37. Johnsen DC. Schultz OW. Schubot DB: Caries patterns inHead Start children in a fluoridated community. / PublicHeatlh Dem 1984;44:61-66.
38. Kelly M, Bruerd B; The prevalence of baby bottle toothdecay among two native Ameriean populations. / PublieHealth Dem 1987;47:94-97.
39. Brown CR. Crawford JJ. Mclver FT. et al: Effeet of milk andfluoridated milk on bacterial enamel déminéralisation. / Den!Re.i l977;5(i:210 (abstr No. 632).
40. Cleaton-Joncs P, Richardson BD, Mclnnes PM, et al: Dentalcaries in South African white children aged 1-5 years. Com-muniiy Dem Oral Epidemiol 1978;6:78-S1.
41. Cleaton.Jones P. Richardson BD, Rantsho JM: Dental cariesin rural and urban black. preb;chool children. Cotnmunily DemOral Epidemiol 1978:6:135-138.
42. Aldy D. Siregar Z, Siregar H, ct al: A comparative study ofcaries formation in breast fed and bottle fed children. Paediair¡•¡dones 1979; 19:308-312.
43. Köhler B, Andreen I, Jonsson B. et al: Effect of caries pre-ventive measures on Streptococcus mutans and lactobacilli inselected mothers. Scand J Dem Res 19R2;90:102-108.
44. Köhler B. Bratthall D. Krasse B: Preventive measures inmothers influenec the establishment of the baeterium Strepto-coccus mutans in their infants. Arch Orat Biot 1983-,23:225-231.
45. Rugg-Gunn AJ, MacGregor IDM: A survey of toothbrushingbehaviour in children and young adults. J Pcriodom Res t978;13:382-389.
46. National Foundation of Dentistry for the Handicapped: Aguide to the use of fluoride for the prevention of dental carieswith alternative recommendations for patients with hand-icaps. JAm Dem Assoc 1986; 113:515.522.531,535.
47. Rugg-Gunn AJ; Fluorides in the prevention of earies in thepreschool children. J Detil 1990:18:304-307. g
168 Quintessence International Volume 23, Number 3/1992