maintaining function, stability and ... - teacher training · isacowitz, rael. pilates second...
TRANSCRIPT
Maintaining function, stability and well-being in clients with
facioscapulohumeral muscular dystrophy (FSHD)
Laura-May Baldwin 10th December 2016 Wimbledon, The Pilates clinic - 2016
2
Abstract
Pilates is a well-stablished and long-standing exercise program renowned for it’s holistic
benefits.
Joseph Pilates addressed not only physical strength and mobility but also believed that
through striving for physical excellence we achieve general well-being.
The focus is not just on the physical, but also the ability to be in total control of the body
and it’s movements through a true mind-body connection.
With this in mind it is easy to see why Pilates is so complimentary for individuals where
movement is part of their career for example the dance community and professional
athletes. It is also incredibly successful in aiding recovery in injuries and assisting those with
physical imbalance and disability.
This case report covers a comprehensive programme utilising the BASI block system to assist
those with FSHD, with particular attention to scapular stabilisation and long term
maintenance of muscular balance.
3
Contents
Abstract………………………………………………………………………..…………………………..P2
Contents…………………………………………………………………..……………………………….P3
Anatomical description/focus………………………………………………..………………… P4-5
Introduction…………………………………………………………………….……………………… P6
Case study……………………………………………………………………………..………………….P7-8
Programme……………………………………………………………………..……..………………..P9-12
Conclusion………………………………………………………………………….….…………..……P13
Bibliography…………………………………………………………………………….......………..P14
4
Anatomical focus
This case report discusses the use of Pilates to stabilise the use of the scapula.
The scapula has no direct bony attachment; instead it relies on muscular attachment to the
axial skeleton. It lies posterior to the thorax roughly from T2-T8.
The muscles enable a large degree of mobility which in turn allows for shoulder/arm
mobility.
The primary muscles of scapula stabilisation are as follows:-
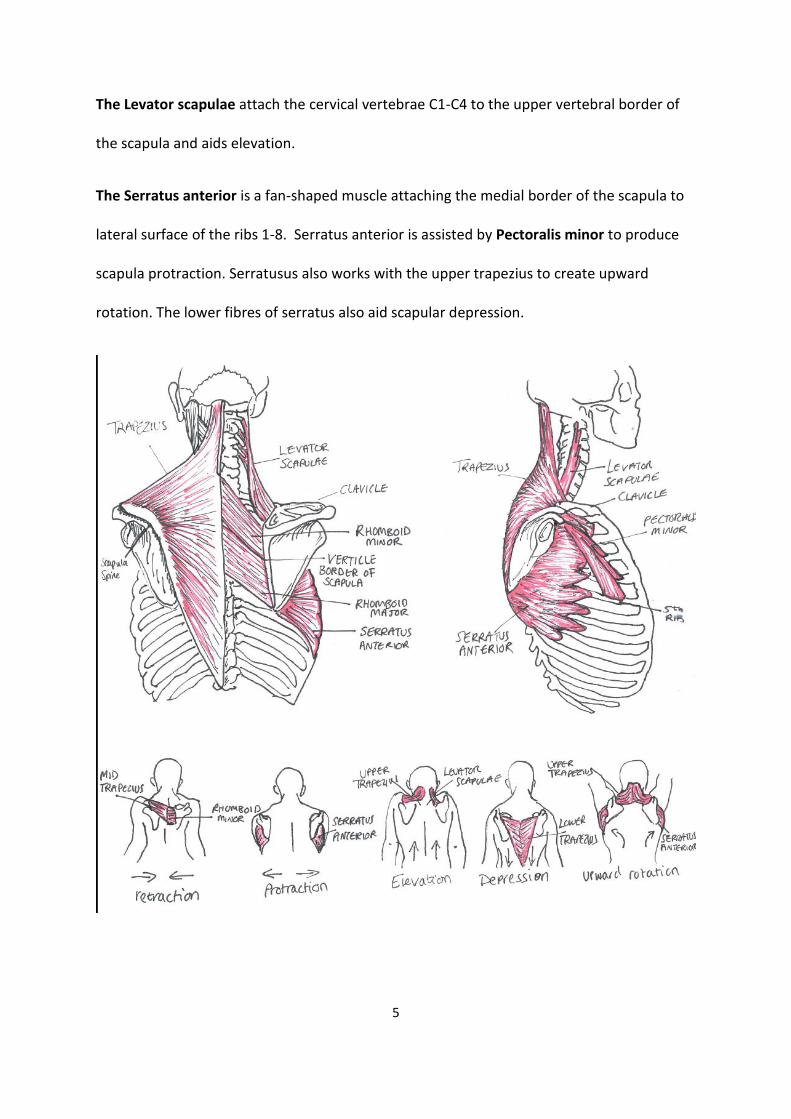
The Trapezius is a large triangular-shaped muscle divided into upper, mid and lower
sections as the fibres of this muscle run in different directions, thus these differing sections
are responsible for different scapulothoracic movements.
It originates in the occipital bone of the skull, attaching to the clavicular and scapula spinal
processes.
The upper trapezius is responsible for elevation and upward rotation of the scapula.
The mid trapezius is responsible for retraction of the scapula.
The mid and lower trapezius is responsible for depression of the scapula.
The Rhomboids (major and minor) are deep to the trapezius with diagonal running fibres
attaching the mid spinal process to the vertebral border of the scapula.
The rhomboids are responsible for retraction of the scapula and downward rotation and to
some degree scapula elevation.
5
The Levator scapulae attach the cervical vertebrae C1-C4 to the upper vertebral border of
the scapula and aids elevation.
The Serratus anterior is a fan-shaped muscle attaching the medial border of the scapula to
lateral surface of the ribs 1-8. Serratus anterior is assisted by Pectoralis minor to produce
scapula protraction. Serratusus also works with the upper trapezius to create upward
rotation. The lower fibres of serratus also aid scapular depression.
6
Introduction
Facioscapulohumeral muscular dystrophy (FSHD) is a genetic, neuromuscular disease. It is
marked by slowly progressing skeletal muscle weakness and death of muscle cells and
tissues.
FSHD primarily affects the back muscles that stabilise the scapula; the upper arm muscle
and shoulder girdle and often affecting the pelvic girdle and leg muscles as the disease
progresses. Muscle fatigue and pain is widely reported in patients with this condition.
Muscle groups tend to deteriorate asymmetrically with one side being affected more than
the other.
There is little research surrounding the effects of Pilates or any exercise on FSHD as it is
difficult to create a controlled test. This is because as a rare genetic disease it manifests in
different ways and people’s experiences differ.
However with a condition that is so unique to the individual, it seems appropriate to utilise
the BASI block system. Creating a programme for a client with FSHD where, alongside
focused muscle strengthening, balance is always addressed, which is a key concern for all
people especially those with FSHD.
7
Case study
Laura is a 32 year old woman with excellent fitness. She partakes in daily exercise including
running, high intensity bodyweight interval training and Pilates.
She has two children aged 5 and 7, born naturally with no medical intervention.
Laura was diagnosed with late onset FSHD in November 2014. Attributed to this condition is
a reduced strength and stabilisation of the left shoulder. Winging of the left scapula is visible
and this is exacerbated by certain exercises.
Laura has had multiple incidences of severe shoulder and neck pain due to over-active
upper trapezius compensating for weaker lower/mid trapezius muscles and surrounding
stabilising muscles.
For this she has been seen regularly by a specialist (MD) physiotherapist and her osteopath
but reports improvement in her left shoulder stability since committing more time to
Pilates.
She experiences some left hip pain that may be associated with FSHD or poor biomechanics
during running.
On examination Laura has good posture but has a tendency to allow her shoulders to round
forward. She has hammer toes and is conscious of correcting her ankle alignment.
After examination and discussion the objectives for the client are to:
Continue to improve shoulder stabilisation
Improve muscular balance between left and right side back and shoulder muscles.

8
Improve muscular balance between hip flexors and adductors
Feel positive about the future!
9
Programme
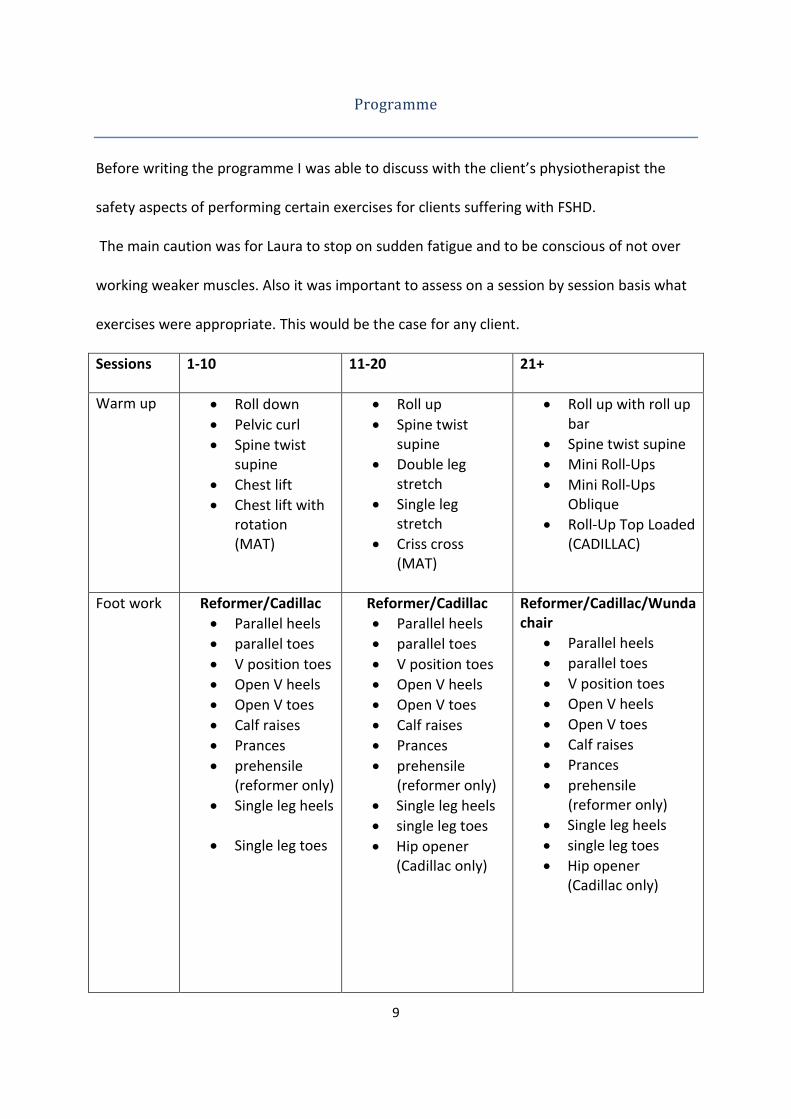
Before writing the programme I was able to discuss with the client’s physiotherapist the
safety aspects of performing certain exercises for clients suffering with FSHD.
The main caution was for Laura to stop on sudden fatigue and to be conscious of not over
working weaker muscles. Also it was important to assess on a session by session basis what
exercises were appropriate. This would be the case for any client.
Sessions 1-10 11-20 21+
Warm up Roll down
Pelvic curl
Spine twist supine
Chest lift
Chest lift with rotation (MAT)
Roll up
Spine twist supine
Double leg stretch
Single leg stretch
Criss cross (MAT)
Roll up with roll up bar
Spine twist supine
Mini Roll-Ups
Mini Roll-Ups Oblique
Roll-Up Top Loaded (CADILLAC)
Foot work Reformer/Cadillac
Parallel heels
parallel toes
V position toes
Open V heels
Open V toes
Calf raises
Prances
prehensile (reformer only)
Single leg heels
Single leg toes
Reformer/Cadillac
Parallel heels
parallel toes
V position toes
Open V heels
Open V toes
Calf raises
Prances
prehensile (reformer only)
Single leg heels
single leg toes
Hip opener (Cadillac only)
Reformer/Cadillac/Wunda chair
Parallel heels
parallel toes
V position toes
Open V heels
Open V toes
Calf raises
Prances
prehensile (reformer only)
Single leg heels
single leg toes
Hip opener (Cadillac only)
10
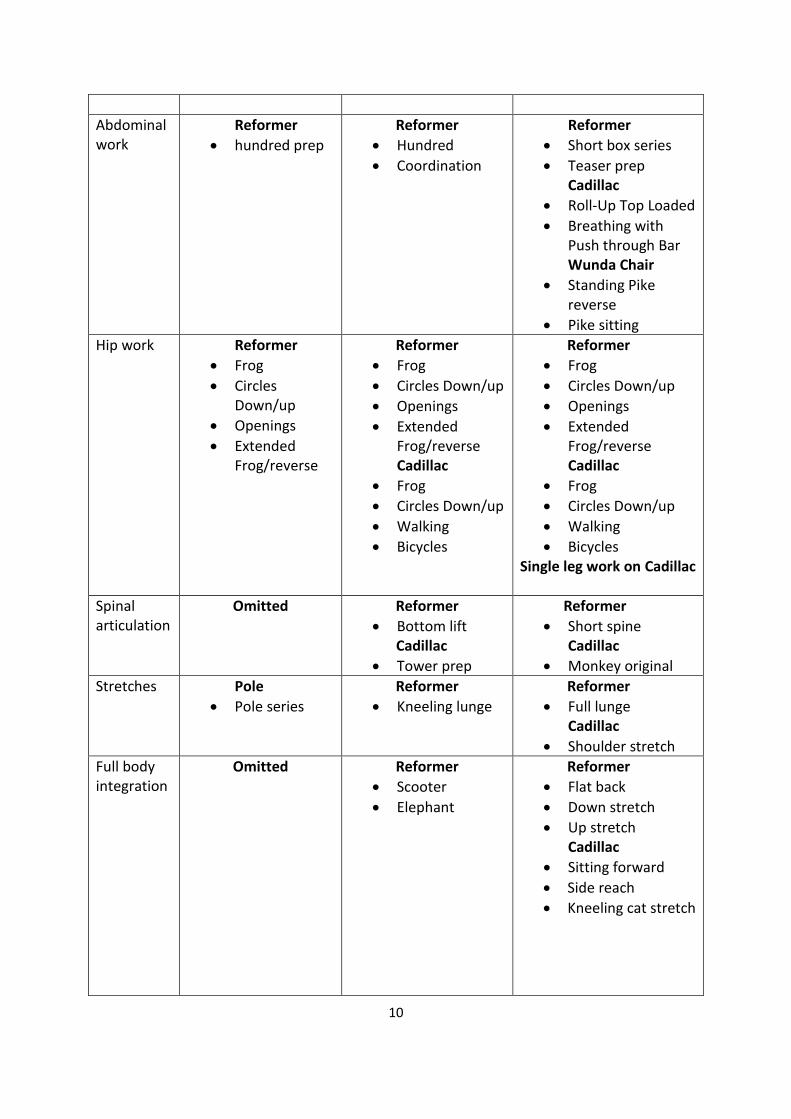
Abdominal work
Reformer
hundred prep
Reformer
Hundred
Coordination
Reformer
Short box series
Teaser prep Cadillac
Roll-Up Top Loaded
Breathing with Push through Bar Wunda Chair
Standing Pike reverse
Pike sitting
Hip work Reformer
Frog
Circles Down/up
Openings
Extended Frog/reverse
Reformer
Frog
Circles Down/up
Openings
Extended Frog/reverse Cadillac
Frog
Circles Down/up
Walking
Bicycles
Reformer
Frog
Circles Down/up
Openings
Extended Frog/reverse Cadillac
Frog
Circles Down/up
Walking
Bicycles Single leg work on Cadillac
Spinal articulation
Omitted
Reformer
Bottom lift Cadillac
Tower prep
Reformer
Short spine Cadillac
Monkey original
Stretches Pole
Pole series
Reformer
Kneeling lunge
Reformer
Full lunge Cadillac
Shoulder stretch
Full body integration
Omitted Reformer
Scooter
Elephant
Reformer
Flat back
Down stretch
Up stretch Cadillac
Sitting forward
Side reach
Kneeling cat stretch
11
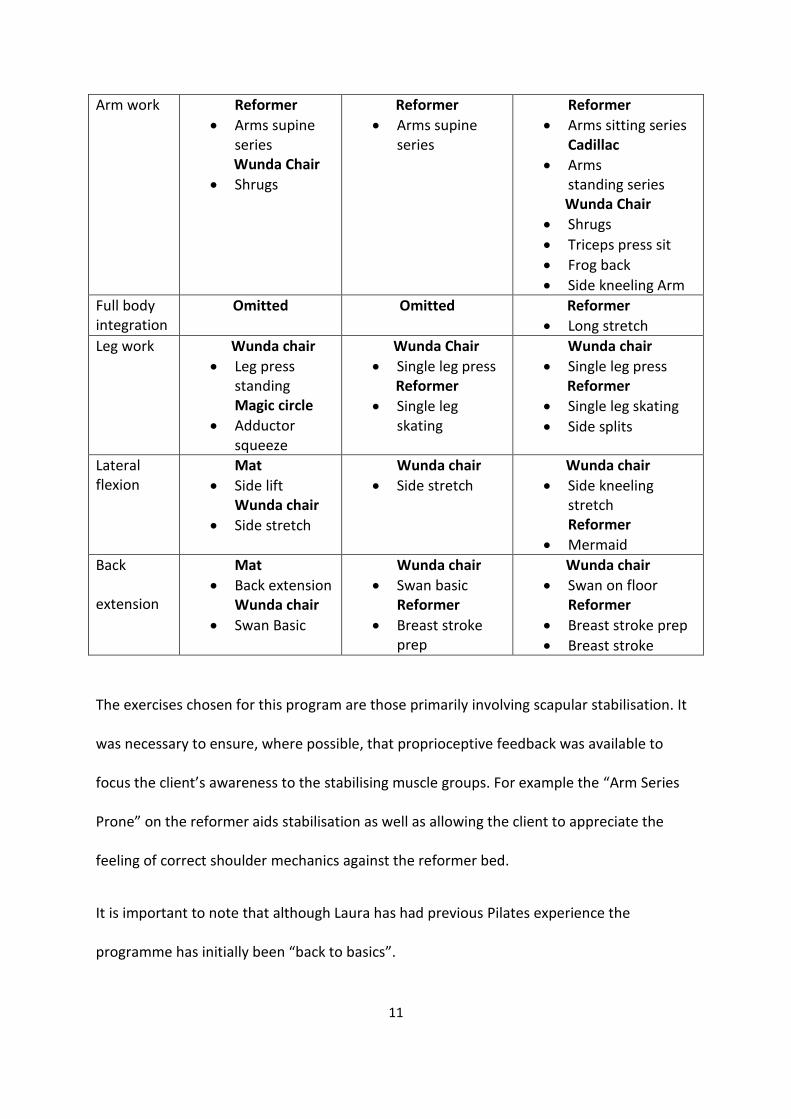
Arm work Reformer
Arms supine series
Wunda Chair
Shrugs
Reformer
Arms supine series
Reformer
Arms sitting series Cadillac
Arms standing series Wunda Chair
Shrugs
Triceps press sit
Frog back
Side kneeling Arm
Full body integration
Omitted Omitted Reformer
Long stretch
Leg work Wunda chair
Leg press standing Magic circle
Adductor squeeze
Wunda Chair
Single leg press Reformer
Single leg skating
Wunda chair
Single leg press Reformer
Single leg skating
Side splits
Lateral flexion
Mat
Side lift Wunda chair
Side stretch
Wunda chair
Side stretch
Wunda chair
Side kneeling stretch
Reformer
Mermaid
Back
extension
Mat
Back extension Wunda chair
Swan Basic
Wunda chair
Swan basic Reformer
Breast stroke prep
Wunda chair
Swan on floor Reformer
Breast stroke prep
Breast stroke
The exercises chosen for this program are those primarily involving scapular stabilisation. It
was necessary to ensure, where possible, that proprioceptive feedback was available to
focus the client’s awareness to the stabilising muscle groups. For example the “Arm Series
Prone” on the reformer aids stabilisation as well as allowing the client to appreciate the
feeling of correct shoulder mechanics against the reformer bed.
It is important to note that although Laura has had previous Pilates experience the
programme has initially been “back to basics”.
12
Readdressing foundation level work enables the instructor to ensure technique is precise
and therefore the client gets the full benefits of a comprehensive programme as well
ensuring that they are safe to progress to more challenging exercises.
The programme has also been complimentary to Laura’s hobby of running, with many
exercises working to balance hip adductors/abductors and hip flexors/extensors. The aim of
the these exercises would be to alleviate the left hip pain she has experienced.
13
Conclusion
The client progressed through the programme well and improvements in stabilisation have
become apparent specifically in purposeful activation of the serratus anterior which has
significantly reduced scapula winging on the left-hand side.
As FSHD is a slow progressing condition and deterioration is difficult to monitor, one can
only speculate on maintenance but it is my belief that if the client continues to build on her
mind body connection that functional movement will be longer lasting.
Most importantly Laura has expressed her enjoyment of her self-development through
Pilates. She reports to feeling stronger and that she is happy to be doing something to
counteract FSHD. This has given her a sense of control over her condition and a belief in her
body!
14
Bibliography
Books
Isacowitz, Rael. Pilates second edition, 2014
Isacowitz, Rael and Clippnger Karen. Pilates Anatomy, 2011
Pilates, H Joseph. Return to life, 1945
Kapt and Elson. The Anatomy colouring in book 3rd edition 2002
Isacowitz, Rael. Study Guide Comprehensive Course, Body Arts & Science
International 200-2014
Website
“About FSHD” , fshsociety.org