look inside crps
DESCRIPTION
"Look Inside" pages from CRPS: Current Diagnosis and TherapyTRANSCRIPT

CRPS: CuRRent DiagnoSiS anD theRaPy
Peter R. WilsonMichael Stanton-Hicks
R. Norman HardenEditors
Progress in Pain Research and ManagementV O L U M E 32
®
32IASP
PRESS
CR
PS: C
uR
Ren
t Dia
gn
oSiS a
nD t
heR
aP
y
WilsonStanton-Hicks
Harden
IASP brings together scientists, clinicians, health care providers, and policy makers to stimulate and support the study of pain and to translate that knowledge
into improved pain relief worldwide. IASP Press publishes timely, high-quality, and reasonably priced books relating to pain research and treatment.
®
International Association for the Study of Pain111 Queen Anne Avenue N., Suite 501
Seattle, WA 98109-4955 USAwww.iasp-pain.org
Mechanisms and Management
of Pain for the Physical TherapistKathleen A. Sluka, Editor
July 2009
Current Topics in Pain: 12th World Congress on Pain
José Castro-Lopes, EditorJune 2009
Functional Pain Syndromes:
Presentation and PathophysiologyEmeran A. Mayer and M. Catherine Bushnell, Editors
April 2009
For detailed information on these and other IASP Press publications, visit the IASP website at www.iasp-pain.org/Books

Mission Statement of IASP Press®
The International Association for the Study of Pain (IASP) is a nonprofit, inter-disciplinary organization devoted to understanding the mechanisms of pain andimproving the care of patients with pain through research, education, and communi-cation. The organization includes scientists and health care professionals dedicatedto these goals. The IASP sponsors scientific meetings and publishes newsletters, tech-nical bulletins, the journal Pain, and books.
The goal of IASP Press is to provide the IASP membership with timely, high-quality, attractive, low-cost publications relevant to the problem of pain. These publi-cations are also intended to appeal to a wider audience of scientists and cliniciansinterested in the problem of pain.

Progress in Pain Research and ManagementVolume 32
CRPS: Current Diagnosisand Therapy
Editors
Peter R. Wilson, MB, BS, PhD
Division of Pain Medicine, Mayo Clinic College of Medicine,Rochester, Minnesota, USA
IASP PRESS® • SEATTLE
Michael Stanton-Hicks, MB, BS, Dr med,FRCA, ABPM, FIPP
Department of Pain Management, Division of Anesthesiology,Cleveland Clinic Foundation; Lerner College of Medicine,Case Western Reserve University, Cleveland, Ohio, USA
R. Norman Harden, MD
Department of Physical Medicine and Rehabilitation,Northwestern University Medical School; Rehabilitation
Institute of Chicago, Chicago, Illinois, USA
© 2005 IASP Press®
International Association for the Study of Pain®
10
All rights reserved. No part of this publication may be reproduced, stored in a retrievalsystem, or transmitted, in any form or by any means, electronic, mechanical, photocopy-ing, recording, or otherwise, without the prior written permission of the publisher.
Timely topics in pain research and treatment have been selected for publication, but theinformation provided and opinions expressed have not involved any verification of thefindings, conclusions, and opinions by IASP®. Thus, opinions expressed in CRPS:Current Diagnosis and Therapy do not necessarily reflect those of IASP or of theOfficers and Councillors.
No responsibility is assumed by IASP for any injury and/or damage to persons orproperty as a matter of product liability, negligence, or from any use of any methods,products, instruction, or ideas contained in the material herein. Because of the rapidadvances in the medical sciences, the publisher recommends that there should beindependent verification of diagnoses and drug dosages.
Published by:
IASP PressInternational Association for the Study of Pain
, Suite Seattle, WA 9810 - USA
: 206- --
www. .org
Printed in the United States of America
Library of Congress Cataloging-in-Publication Data
CRPS : current diagnosis and therapy / editors, Peter R. Wilson, Michael Stanton-Hicks, R. Norman Harden. p. ; cm. -- (Progress in pain research and management ; v. 32) Includes bibliographical references and index. ISBN 0-931092-55-8 (alk. paper) 1. Reflex sympathetic dystrophy. [DNLM: 1. Complex Regional Pain Syndromes--diagnosis. 2. Complex Regional Pain Syndromes--therapy. WL 544 C954 2004] I. Title: Complex Regional Pain Syndrome. II. Wilson, Peter R., 1941- III. Stanton-Hicks, Michael d’A. IV. Harden, R. Norman, 1954- V. Series. RC422.R43C77 2004 616'.0472--dc22
2004062439

List of Contributing Authors viiPreface ix
Part I Overview of Taxonomy of Syndromes and Diseases
Section Editor: Peter R. Wilson
1. IntroductionJohn D. Loeser 3
2. Taxonomy and Complex Regional Pain SyndromeHarold Merskey 9
3. Retrospection, Science and Epidemiology of CRPSPeter R. Wilson and Nikolai Bogduk 19
Part II Taxonomy and Diagnosis: Clinical Experience
Section Editor: Peter R. Wilson
4. Diagnostic Criteria: The Statistical Derivation of the FourCriterion FactorsR. Norman Harden and Stephen P. Bruehl 45
5. Factor I: Sensory Changes—Pathophysiology and MeasurementAnne Louise Oaklander and Frank Birklein 59
6. Factor II: Vasomotor Changes—Pathophysiology and MeasurementGunnar Wasner and Ralf Baron 81
7. Factor III: Sudomotor Changes and Edema—Pathophysiologyand MeasurementPaola Sandroni and Peter R. Wilson 107
8. Factor IV: Movement Disorders and Dystrophy—Pathophysiologyand MeasurementJacobus J. Van Hilten, Helmut Blumberg, and Robert J. Schwartzman 119
9. Laboratory Tests for Complex Regional Pain SyndromeOliver Rommel, Heinz-Joachim Häbler, and Matthias Schürmann 139
Part III Management of CRPS
Section Editor: R. Norman Harden
10. The Rationale for Integrated Functional RestorationR. Norman Harden 163
11. Physical and Occupational TherapiesJan H.B. Geertzen and R. Norman Harden 173
12. Evidence-Based Pharmacotherapy for CRPS and Related ConditionsAnne Louise Oaklander 181
Contents
v

vi CONTENTS
13. Psychological InterventionsStephen P. Bruehl 201
14. Traditional Interventional TherapiesAllen W. Burton, Timothy R. Lubenow, and P. Prithvi Raj 217
15. Implanted TherapiesTimothy R. Lubenow, Asokumar Buvanendran,and Michael Stanton-Hicks 235
16. Miscellaneous and Experimental TherapiesMichael Stanton-Hicks, Richard L. Rauck, Mark Hendrickson,and Gabor Racz 255
17. Management of Pediatric Patients with CRPSRobert T. Wilder and Gunnar Olsson 275
Part IV Epilogue
Section Editor: Peter R. Wilson
18. Future PerspectivesWilfrid Jänig 293
Index 309
Contributing Authors
vii
Ralf Baron, Dr med Department of Neurological Pain Research and Therapy,Neurological Clinic, University of Schleswig-Holstein, Kiel, Germany
Frank Birklein, MD, PhD Department of Neurology, University of Mainz,Mainz, Germany
Helmut Blumberg, MD Department of Neurosurgery, University of Freiburg,Freiburg, Germany
Nikolai Bogduk, MD, PhD Department of Neurology, University of Newcastle,and Newcastle Bone and Joint Institute, Royal Newcastle Hospital, Newcastle,New South Wales, Australia
Stephen P. Bruehl, PhD Department of Anesthesiology, Vanderbilt UniversityMedical Center, Nashville, Tennessee, USA
Allen W. Burton, MD Department of Anesthesiology, M.D. Anderson CancerCenter, University of Texas, Houston, Texas, USA
Asokumar Buvanendran, MD Section of Pain Medicine, Departmentof Anesthesiology, Rush University Medical Center, Chicago, Illinois, USA
Jan H.B. Geertzen, MD, PhD Center for Rehabilitation, University of Groningen,Groningen, The Netherlands
Heinz-Joachim Häbler, MD Bonn-Rhein-Sieg University of Applied Sciences,Rheinbach, Germany
R. Norman Harden, MD Department of Physical Medicine and Rehabilitation,Northwestern University Medical School, and Rehabilitation Institute ofChicago, Chicago, Illinois, USA
Mark Hendrickson, MD Department of Orthopaedic Surgery, Cleveland ClinicFoundation, Cleveland, Ohio, USA
Wilfrid Jänig, Dr med Department of Physiology, Christian-AlbrechtsUniversity, Kiel, Germany
John D. Loeser, MD Departments of Neurological Surgery and Anesthesia,University of Washington, Seattle, Washington, USA
Timothy R. Lubenow, MD Section of Pain Medicine, Departmentof Anesthesiology, Rush University Medical Center, Chicago, Illinois, USA
Harold Merskey, DM, FRCPC, FRCPsych Professor Emeritus of Psychiatry,University of Western Ontario, London, Ontario, Canada
Anne Louise Oaklander, MD, PhD Nerve Injury Unit, Departmentsof Anesthesiology, Neurology, and Neuropathology, MassachusettsGeneral Hospital, Harvard Medical School, Boston, Massachusetts, USA

xiv CONTRIBUTING AUTHORSviii CONTRIBUTING AUTHORS
Gunnar L. Olsson, MD, PhD Department of Pediatric Anesthesiology, AstridLindgren Children’s Hospital, Stockholm, Sweden; Karolinska Institute,Stockholm, Sweden
Gabor Racz, MD Pain Services, Department of Anesthesiology, Texas TechUniversity Health Sciences, Lubbock, Texas, USA
P. Prithvi Raj, MD Department of Anesthesiology and Pain Medicine,Texas Tech University Health Sciences Center School of Medicine,and World Institute of Pain, Lubbock, Texas, USA
Richard L. Rauck, MD Piedmont Pain Consultants, Winston-Salem, NorthCarolina, USA
Oliver Rommel, Dr med Departments of Neurology and Pain Therapy,Rommel Clinic, Bad Wildbad, Germany
Paola Sandroni, MD Department of Neurology, Mayo Clinic Collegeof Medicine, Rochester, Minnesota, USA
Matthias Schürmann, Dr med Department of Accident and RehabilitationSurgery, Hof Clinic, Hof, Germany
Robert J. Schwartzman, MD Department of Neurology, Drexel UniversityCollege of Medicine, Philadelphia, USA
Michael Stanton-Hicks, MB:BS, Dr med, FRCA, ABPM, FIPP Departmentof Pain Management, Cleveland Clinic Foundation; Lerner Collegeof Medicine, Case Western Reserve University, Cleveland, Ohio, USA
J.J. van Hilten, MD Department of Neurology, Leiden University MedicalCenter, Leiden, The Netherlands
Gunnar Wasner, Dr med Department of Neurological Pain Research andTherapy, Neurological Clinic, University of Schleswig-Holstein,Kiel, Germany
Robert T. Wilder, MD, PhD Mayo Clinic and Mayo Eugenio Litta Children’sHospital, Rochester, Minnesota, USA
Peter R. Wilson, MB:BS, PhD Division of Pain Medicine, Mayo ClinicCollege of Medicine, Rochester, Minnesota, USA
ix
Preface
Complex regional pain syndrome (CRPS) has been extensively studiedand discussed since the publication of Reflex Sympathetic Dystrophy: AReappraisal (W. Jänig and M. Stanton-Hicks [Eds]; Seattle: IASP Press,1996). This volume presents the results of changes brought about by thediagnostic reclassification and redefinition of CRPS based on clinical andbasic research. CRPS can now regarded as a systemic condition involvingthe entire neuraxis with manifestation of all the inflammatory changes de-scribed centrally and in the periphery. Unfortunately, CRPS cannot yet bereduced to a single mechanism involving only one system. It is a syndromethat represents a spectrum of changes involving nervous, endocrine, vascu-lar, and musculoskeletal systems. The proportion of each involvement deter-mines those criteria that make up the definition of CRPS types I and II.
Changes to the diagnostic criteria of CRPS suggested in this volumehave resulted from prospective multicenter epidemiological studies that haveidentified four clinically and statistically distinct subgroups or factors withinthe existing IASP criteria. Each factor consists of subjective symptoms and/or objective signs. They comprise: (1) hyperalgesia and hyperesthesia,(2) temperature asymmetry and color changes, (3) edema and sweating, and(4) motor dysfunction and trophic changes.
The stimulus to review what has been 10 years’ progress in our under-standing of CRPS comes from these observations and changing clinical andresearch views. Treatment decisions now can be based on an improvedunderstanding of the pathophysiology, rather than on consensus (althoughconsensus is still important, in the absence of evidence-based outcome data).Most of the contributors to this volume deliberated at a consensus confer-ence over two days to decide what changes should be made, if any, to theexisting IASP diagnostic criteria. Sensitivity has been improved, and theissues of specificity have been clarified so that the new criteria can berecommended to the Committee on Taxonomy of the IASP. Also, the secondcharge for this group was to provide a critical analysis of non-interventionaland interventional methods that are currently employed for the treatment ofCRPS. Given the time constraints and number of aspects to cover, a remark-able level of understanding and cooperation formed the basis for the con-tents of the four parts that comprise this text. This book is designed as areference, not only for clinicians, pain specialists, and others in the healthcare industry, but also for anyone seeking information that is current andrelevant on the day of its publication.

x PREFACE
This book is divided into four parts. Part I—Overview of Taxonomy ofSyndromes and Diseases lays the foundation historically and in context withscientific and epidemiological facts that were not previously known.
Part II—Taxonomy and Diagnosis: Clinical Experience provides thebackground data for making a proposal to the Committee on Taxonomy ofthe IASP. There are minor structural changes to the existing taxonomy thatwill, as described above, improve its specificity.
Part III addresses the management of CRPS, as far as possible on thebasis of evidence-based practice. It describes the different modalities thatare currently used to manage a “syndrome” that awaits a defining mecha-nism.
Part IV—Epilogue, is an overview by the doyen of CRPS basic re-search, Wilfrid Jänig, who is indefatigable in his efforts to understand therelationship of the autonomic nervous system to disease states. His persua-sive educational skills have mentored innumerable clinicians and scientists,many of whom have contributed to this volume. This chapter provides aroadmap for further studies that will lead to a full understanding of CRPS.
Grading of the evidence used to justify treatment modalities is a deliber-ately simplified version of the basic methodology used by the CochraneCollaboration. The highest level of evidence (level 1) is from systematicreview or meta-analysis of properly designed controlled randomized trials,while level 2 reflects evidence from one or more such trials. The next level(level 3) is from cohort studies, nonrandomized trials, or open-label trials.The lowest level (level 4) is from individual patient data (case reports).
There is little, if any, reliance placed on “clinical experience” or “usualpractice.” This volume was not intended to apply meta-analytic techniquesto all available published data, but to filter the information for generalapplicability.
The editors acknowledge the timeliness, cooperation, and insights of allthe authors, and their patience with the process. The production of thisvolume would not have been possible without their support and the addi-tional invaluable technical assistance and guidance from Elizabeth Endres ofthe IASP Press.
The editors wish to gratefully acknowledge the support that was pro-vided in the form of an unrestricted educational grant by the MedtronicCorporation toward the publication of this book.
PETER WILSON, MB, BS, PHDMICHAEL STANTON-HICKS, MB, BS, DR MED, FRCA, ABPM, FIPPR. NORMAN HARDEN, MD
19
3
CRPS: Current Diagnosis and Therapy, Progress inPain Research and Management, Vol. 32, edited byPeter Wilson, Michael Stanton-Hicks, and R. NormanHarden, IASP Press, Seattle, © 2005.
Retrospection, Scienceand Epidemiology of CRPS
Peter R. Wilsona and Nikolai Bogdukb
aDivision of Pain Medicine, Mayo Clinic College of Medicine, Rochester,Minnesota, USA; bDepartment of Neurology, University of Newcastle,
and Newcastle Bone and Joint Institute, Royal Newcastle Hospital,Newcastle, New South Wales, Australia
Widespread pain following injury has long been an enigma in medicine,particularly when, to the patient and physician alike, its extent seems dispro-portionate to the nature of the precipitating injury. When such pain is ac-companied by what appear to be features mediated by the sympathetic ner-vous system, such as swelling, discoloration, and temperature changes, itappears to constitute a distinctive syndrome. This type of pain has beenrecorded for hundreds of years under numerous descriptors, as documentedin a masterly doctoral thesis (Veldman 1995). Veldman suggests that thefirst description may have been by Ambrose Paré in 1598. Nonetheless,three linguistically distinct variants began to be described in the American,French, and German literature. These schools were founded on the observa-tions of Mitchell et al. (1864), Charcot (1890), and Sudeck (1900). There areat least 79 descriptors in the English literature, 32 in the French, and 49 inthe German (Veldman 1995).
The term reflex sympathetic dystrophy (RSD) appears to have been coinedby Evans in 1947. It became more widely accepted after the publication ofBonica’s Textbook of Pain in 1953. RSD became the term eventually adoptedby the Index Medicus and Medline for a painful syndrome with widespreaddistribution of pain associated with so-called sympathetic features.
Causalgia is a term with different clinical and pathophysiological con-notations. It has been used to describe the burning nature of the pain syn-drome that commonly occurs after peripheral nerve injuries. It was adoptedto describe a particular subtype of RSD in which the precipitating injury

45
4
CRPS: Current Diagnosis and Therapy, Progress inPain Research and Management, Vol. 32, edited byPeter Wilson, Michael Stanton-Hicks, and R. NormanHarden, IASP Press, Seattle, © 2005.
Diagnostic Criteria: The StatisticalDerivation of the Four Criterion Factors
R. Norman Hardena and Stephen P. Bruehlb
aDepartment of Physical Medicine and Rehabilitation, Northwestern UniversityMedical School, and Rehabilitation Institute of Chicago, Chicago, Illinois, USA;
bDepartment of Anesthesiology, Vanderbilt University School of Medicine,Nashville, Tennessee, USA
Complex regional pain syndrome has been known by many names, suchas algodystrophy mineures, mimocausalgia, sympathalgia, post-traumaticspreading neuralgia, and most commonly reflex sympathetic dystrophy andcausalgia. It has historically been diagnosed using a variety of nonstandard-ized, idiosyncratic, or incompatible diagnostic systems (e.g., Bonica 1953;Kozin et al. 1981; Blumberg 1991; Gibbons and Wilson 1992). ClaudeBernard first mentioned a syndrome characterized by the association of painand the sympathetic nervous system. Lucid descriptions of “causalgia” byone of Bernard’s students, Silas Weir-Mitchell (1829–1914), came out ofthe American Civil War.
The name “reflex sympathetic dystrophy” (RSD) is attributed to Evans(1946), but this terminology is problematic. If there is a “reflex” involved inCRPS, it is complicated, multisynaptic, and not fully characterized. The“sympathetic” or autonomic changes may be epiphenomena and may not becausative or perpetuating, and true “dystrophy” occurs in only about 10% ofcases. After much discussion in the literature and at scientific meetings, thename was ultimately changed to complex regional pain syndrome (CRPS) ata consensus workshop in Orlando, Florida in 1993 (Merskey and Bogduk1994; Stanton-Hicks et al. 1995; Jänig and Stanton-Hicks 1996). This namefor the syndrome was meant to be descriptive and general, and was notintended to imply any etiopathology (including any direct role for the sym-pathetic nervous system).
54 R.N. HARDEN AND S.P. BRUEHL
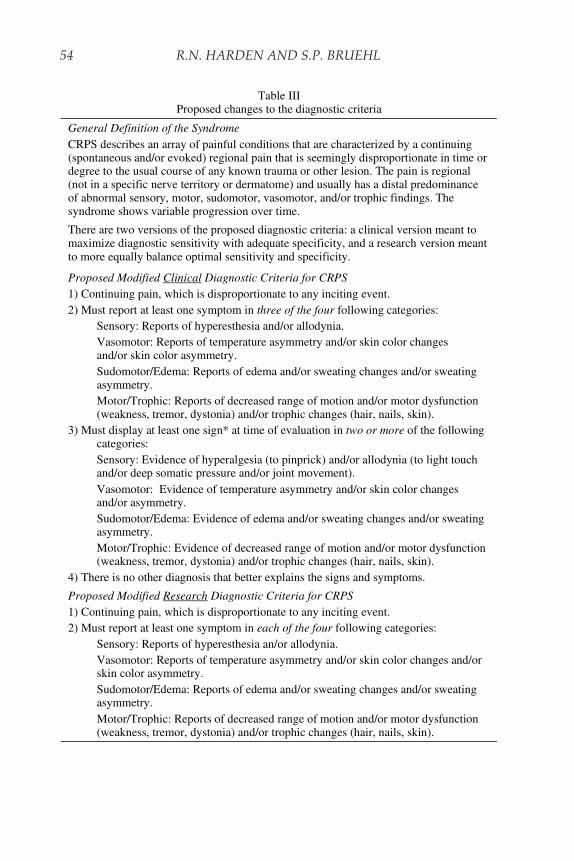
Table III Proposed changes to the diagnostic criteria
General Definition of the Syndrome CRPS describes an array of painful conditions that are characterized by a continuing (spontaneous and/or evoked) regional pain that is seemingly disproportionate in time or degree to the usual course of any known trauma or other lesion. The pain is regional (not in a specific nerve territory or dermatome) and usually has a distal predominance of abnormal sensory, motor, sudomotor, vasomotor, and/or trophic findings. The syndrome shows variable progression over time.
There are two versions of the proposed diagnostic criteria: a clinical version meant to maximize diagnostic sensitivity with adequate specificity, and a research version meant to more equally balance optimal sensitivity and specificity.
Proposed Modified Clinical Diagnostic Criteria for CRPS 1) Continuing pain, which is disproportionate to any inciting event. 2) Must report at least one symptom in three of the four following categories: Sensory: Reports of hyperesthesia and/or allodynia. Vasomotor: Reports of temperature asymmetry and/or skin color changes
and/or skin color asymmetry. Sudomotor/Edema: Reports of edema and/or sweating changes and/or sweating
asymmetry. Motor/Trophic: Reports of decreased range of motion and/or motor dysfunction
(weakness, tremor, dystonia) and/or trophic changes (hair, nails, skin). 3) Must display at least one sign* at time of evaluation in two or more of the following
categories: Sensory: Evidence of hyperalgesia (to pinprick) and/or allodynia (to light touch
and/or deep somatic pressure and/or joint movement). Vasomotor: Evidence of temperature asymmetry and/or skin color changes
and/or asymmetry. Sudomotor/Edema: Evidence of edema and/or sweating changes and/or sweating
asymmetry. Motor/Trophic: Evidence of decreased range of motion and/or motor dysfunction
(weakness, tremor, dystonia) and/or trophic changes (hair, nails, skin). 4) There is no other diagnosis that better explains the signs and symptoms.
Proposed Modified Research Diagnostic Criteria for CRPS 1) Continuing pain, which is disproportionate to any inciting event. 2) Must report at least one symptom in each of the four following categories: Sensory: Reports of hyperesthesia an/or allodynia. Vasomotor: Reports of temperature asymmetry and/or skin color changes and/or
skin color asymmetry. Sudomotor/Edema: Reports of edema and/or sweating changes and/or sweating
asymmetry. Motor/Trophic: Reports of decreased range of motion and/or motor dysfunction
(weakness, tremor, dystonia) and/or trophic changes (hair, nails, skin).
FOUR DIAGNOSTIC CRITERION FACTORS 55
be valuable for future work to address how these specific patterns may relateto the patient subtypes identified.
In summary, while these results are preliminary, they are consistent withlimited previous empirical work that argues against three sequential stagesof CRPS (Veldman et al. 1993; Bickerstaff and Kanis 1994; Zyluk 1998).Future application of similar analytic techniques to the problem of CRPSmay allow identification of distinct CRPS subgroups that have potentialutility in targeting treatment more effectively.
The Budapest consensus group considered these data too preliminary tojustify codifying these subtypes in formal diagnostic criteria. However, theconsensus group did discuss the old CRPS subtypes described at the Or-lando conference and in the IASP criteria (Merskey and Bogduk 1994).There was general agreement that there are problems with making a distinc-tion between CRPS type I (without distinct major nerve damage, most likethe old RSD) versus type II (with major nerve damage, most like the oldcausalgia; see Table I).
Specifically, the definition is rather vague as to what characterizes “ma-jor” nerve damage and how this should be objectively defined. The problemof distinguishing CRPS types I and II is complicated clinically by the factthat the definitive tests of nerve damage, such as EMG, are consideredunnecessarily painful for patients, and even cruel. Moreover, this diagnosticdistinction does not currently influence the specific therapeutic approachemployed. Despite these limitations, the distinction between these two exist-ing CRPS subtypes was retained by the Budapest group, with eventual re-evaluation of this issue planned as more data become available regarding itsclinical importance. Another subtype of CRPS was added by the consensusgroup out of concern that lowering the sensitivity would leave some previously
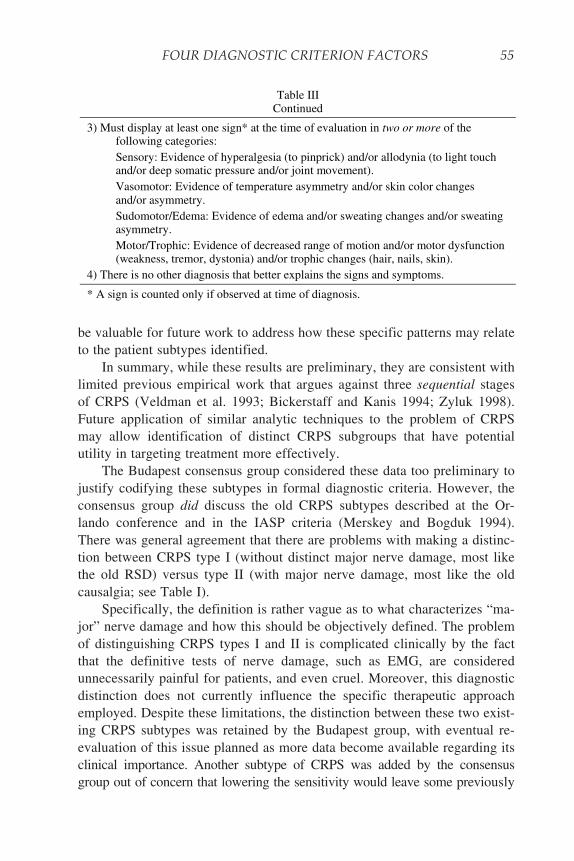
Table III Continued
3) Must display at least one sign* at the time of evaluation in two or more of the following categories:
Sensory: Evidence of hyperalgesia (to pinprick) and/or allodynia (to light touch and/or deep somatic pressure and/or joint movement).
Vasomotor: Evidence of temperature asymmetry and/or skin color changes and/or asymmetry.
Sudomotor/Edema: Evidence of edema and/or sweating changes and/or sweating asymmetry.
Motor/Trophic: Evidence of decreased range of motion and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic changes (hair, nails, skin).
4) There is no other diagnosis that better explains the signs and symptoms.
* A sign is counted only if observed at time of diagnosis.

INTEGRATED FUNCTIONAL RESTORATION 165
that objective functional features and biometric data could be measuredlongitudinally, that they were sensitive enough to demonstrate change overtime (in response to a functional restoration-based interdisciplinary pro-gram), and that they were correlated with change in subjective outcomes(decreased pain). These early studies provided the primary rationale for areliance on functional measures as the foundation of judging success in thetreatment of CRPS. Baker et al. (1998) later demonstrated more conclu-sively the utility of quasi-quantitative and psychometric measures in predict-ing functional outcome in an open-label sample of musculoskeletal pain. Invarious uncontrolled studies, CRPS patients benefited from specific physio-therapeutic modalities such as stress loading and isometric techniques (Carlsonand Watson 1988). Oerlemans et al. (1999a,b) conducted a prospective
ReactivationContrast BathsDesensitization
Exposure Therapy
FlexibilityEdema Control
Isometric StrengtheningCorrection of Postural Abnormalities
Diagnosis and Treatment of Secondary Myofascial Pain
ROM (gentle)Stress Loading
Isotonic StrengtheningGeneral Aerobic Conditioning
Postural Normalization & Balanced Use
ErgonomicsMovement TherapiesNormalization of Use
Vocational/Functional Rehabilitation
Fig. 1. A sample, step-wise, functional restoration algorithm. From the outset, in appropri-ate cases, the patient should have access to injections, oral medications, and psycho-therapy. If the patient fails to progress, at any step or in any regard, the clinical team shouldconsider more or different interventions, stronger medications, or more intensive psycho-therapies. ROM (gentle) denotes gentle exercises to improve range of motion.
255
16
CRPS: Current Diagnosis and Therapy, Progress inPain Research and Management, Vol. 32, edited byPeter Wilson, Michael Stanton-Hicks, and R. NormanHarden, IASP Press, Seattle, © 2005.
Miscellaneous and ExperimentalTherapies
Michael Stanton-Hicks,a Richard L. Rauck,c
Mark Hendrickson,b and Gabor Raczd
Departments of aPain Management and bOrthopedic Surgery, Cleveland ClinicFoundation, Cleveland, Ohio, USA; cPiedmont Pain Consultants, Winston-Salem, North Carolina, USA; dPain Services, Department of Anesthesiology,
Texas Tech University Health Sciences, Lubbock, Texas, USA
PRINCIPLES AND GOALS
Failure to understand the fundamental underlying mechanisms of CRPShas spawned a variety of symptom-directed treatments. Some of these treat-ments are of proven efficacy, as determined either by their longstanding useor through rigorous testing and prospective controlled studies in relatedapplications such as neuropathic pain. With a better understanding of patho-logical processes, researchers are pursuing a number of pharmacological andinterventional approaches. While at least many characteristics of CRPS-Isuggest a neuropathic process, CRPS-II is unquestionably a form of neuro-pathic pain that lends itself to treatment by neuro-augmentation.
Frequently, a patient with CRPS is referred for evaluation and manage-ment when the pain pattern progresses rather than resolves and varioussymptoms emerge that suggest involvement of the somatosensory, sympa-thetic, and somatomotor systems. Diagnosis must be based upon currentdiagnostic criteria and the time course of the pain syndrome. The static anddynamic levels of pain and functional loss will serve as reference thresholdsfor clinical improvement. As in other complex problems, interdisciplinarymanagement is the approach most likely to yield optimal clinical and func-tional outcomes. The primary goal is to significantly alleviate or extinguishpain and to stabilize, then improve, functional deficits. Placing functionalimprovement before pain control often results in significant pain aggravation.
256 M. STANTON-HICKS ET AL.
Rehabilitation entails a graded therapy program with goal-specific measuresfor functional improvement without causing a resurgence of pain. The sta-bility of the reduction in pain and improvement in function must be moni-tored.
The long-established empirical association between CRPS and dysfunc-tion of the sympathetic nervous system has suggested both the α1 and α2
adrenoceptors as targets for pharmacological modulation. The N-methyl-D-aspartate (NMDA) receptor, a common site for neuropathic pain research,has been singled out as a recent clinical experimental target. Similarly, someof the deep-seated pain reported by CRPS patients, and thought by some tobe related to osseous changes, has resulted in empiric treatment with somesuccess by bisphosphonates, an established therapy for some osteoscleroticconditions (see Chapter 12).
TRANSCUTANEOUS ELECTRICAL NERVE STIMULATION
Transcutaneous electrical nerve stimulation (TENS) therapy may be usefulas an adjunct to the pharmacological management of CRPS and may be ahelpful treatment for mononeuropathic pain in some cases of CRPS-II. Themost useful application for TENS therapy in CRPS is for symptomatic man-agement of the frequently associated myofascial syndrome. In CRPS-II, TENSmay provide sufficient analgesia to allow compliance with physical therapy.In our experience it is also useful in predicting the success of peripheralnerve stimulation. In the original description by Wall and Sweet (1967),TENS can achieve analgesia by stimulating Aβ fibers. It is most effective intreating mononeuropathies, as shown by level 3 clinical evidence (Andersonet al. 1976; Thorsteinsson et al. 1977; Eriksson et al. 1979; Long et al. 1979;Johnson et al. 1991a,b).
In our experience, it is important to perform a trial of adequate length, atleast 3–4 weeks, to determine whether TENS is a suitable modality, particu-larly when attempting to manage symptoms of myofascial dysfunction. It isimportant that the pain is not aggravated, that the patient becomes familiarwith the system, and that suitable electrode placement is achieved. Initially,TENS should be used for 1 hour three times per day, but frequency andduration of application may be extended with experience. Most patients willselect a range between 40 and 70 Hz (Thorsteinsson et al. 1977; Johnson etal. 1991a). Although tolerance is seen less frequently with TENS than withpharmacological agents, Eriksson et al. (1979) reported that 55% of patientsreceived adequate pain relief at 2 months, dropping to 41% at 12 months.

302 W. JÄNIG
to correct this mismatch can reverse the changes. Moseley’s and relatedstudies (Schwoebel et al. 2001; McCabe et al. 2003b,c) are opening newways to investigate the mechanisms underlying the sensory, motor, and au-tonomic changes in CRPS-I patients.
FUTURE RESEARCH DIRECTIONS
CRPS patients exhibit changes that occur in systems processing nox-ious, tactile, and thermal information, in sympathetic systems innervatingblood vessels, sweat glands, and possibly other targets, and in the somatomotorsystem, indicating that the central representations of these systems are al-tered. The way these central changes are triggered by a peripheral trauma,which is often minor compared to the dramatic expression of the clinicalphenomena, remains an enigma. Furthermore, how these central changesrelate to the peripheral inflammatory and immunological changes is unclear.Finally, we cannot explain why pain and the other changes associated withthe sympathetic nervous system (including swelling), the motor system, andthe somatosensory system may disappear, in CRPS patients with sympa-thetically maintained pain (SMP), after sympathetic blockade (e.g., with alocal anesthetic or with guanethidine). Hypotheses must be formulated aboutthe underlying mechanisms of clinical changes that can be measured quanti-tatively. These hypotheses should be tested by using a multidisciplinaryapproach combining clinical experimentation, human models, and varioustypes of animal models (in vivo and in vitro). This type of integrative re-search is a necessity if we are to unravel the mechanisms that operate inCRPS and if we are to find the organizing pathophysiological principles thatorchestrate the different changes. It is essential that basic research in animalmodels and in humans and clinical studies of CRPS should be closely aligned(Fig. 3). Such an approach is imperative if we are to achieve a mechanism-based diagnostic classification of CRPS and ultimately develop a mecha-nism-based therapeutic strategy.
New research should focus on the following areas (Baron et al. 2002b;Jänig and Baron 2004):
Draft a consensus definition of CRPS with standardized diagnosticcriteria. Neurologists, anesthesiologists, and others agree about the minimalclinical criteria (signs and symptoms) that define CRPS (Stanton-Hicks et al.1995; Bruehl et al. 1999; Baron and Jänig 2004). However, without a uni-versally accepted definition and diagnostic criteria and a further validationand extension of the present clinical criteria, it is difficult to accuratelyidentify CRPS patients, select patients for clinical trials, validate experimental

FUTURE PERSPECTIVES 303
human and animal model systems for research, and formulate testable hy-potheses. A symposium to specifically define the clinical and diagnosticcriteria, based on what is known, should be a high priority for the field.Once determined, these consensus criteria should be disseminated to themedical, research, and advocacy communities, in particular to those groupsinvolved in epidemiological studies, in the design of appropriate models forsymptoms in CRPS, in research on underlying mechanisms, and in the de-sign of CRPS therapies to be tested in prospective clinical trials.
Perform epidemiological studies using well-defined diagnostic criteria.Epidemiological studies are urgently needed to identify the characteristics ofpatients at high risk for developing CRPS, to better define the relationshipbetween certain clinical signs and disease onset, progression, and distribu-tion on the body, and to determine the incidence of patients with CRPS.
HYPOTHESES
HUMAN PATIENTClinical observations
Experimental observationson patients
Reduced animalmodels in vivo
& in vitro
Behavioral animalmodels
Fig. 3. Hierarchy of human and animal models and clinical investigations in experimentalresearch on the role of the sympathetic nervous system in pain. This hierarchy consists ofdifferent levels that interact reciprocally. The scientific questions to be asked are formu-lated on the basis of clinical observations. The human models and the behavioral animalmodels mostly focus on one component (e.g., SMP, autonomic abnormalities, motorabnormalities, or edema in CRPS type I or II). On the basis of the experimental behavioralanimal models and the experimental human models the questions are formulated fortesting in the more reduced animal models. These reduced animal models focus on onecomponent (e.g., sympathetic-afferent coupling in the periphery or in the dorsal rootganglion). The results obtained using the behavioral models must be interpreted in light ofthe clinical observations; the results obtained using the reduced animal models in vivomust be interpreted in light of behavioral animal models and of the human experimentalmodels; and the results obtained in the reduced animal models in vitro must be interpretedin light of the animal models in vivo. Research performed on the various animal modelsshapes the clinical research performed on patients with SMP. This interactive researchstrategy applies to most experimental research that aims to elucidate the pathophysiologi-cal processes underlying diseases.

CRPS: CuRRent DiagnoSiS anD theRaPy
Peter R. WilsonMichael Stanton-Hicks
R. Norman HardenEditors
Progress in Pain Research and ManagementV O L U M E 32
®
32IASP
PRESS
CR
PS: C
uR
Ren
t Dia
gn
oSiS a
nD t
heR
aP
y
WilsonStanton-Hicks
Harden
IASP brings together scientists, clinicians, health care providers, and policy makers to stimulate and support the study of pain and to translate that knowledge
into improved pain relief worldwide. IASP Press publishes timely, high-quality, and reasonably priced books relating to pain research and treatment.
®
International Association for the Study of Pain111 Queen Anne Avenue N., Suite 501
Seattle, WA 98109-4955 USAwww.iasp-pain.org
Mechanisms and Management
of Pain for the Physical TherapistKathleen A. Sluka, Editor
July 2009
Current Topics in Pain: 12th World Congress on Pain
José Castro-Lopes, EditorJune 2009
Functional Pain Syndromes:
Presentation and PathophysiologyEmeran A. Mayer and M. Catherine Bushnell, Editors
April 2009
For detailed information on these and other IASP Press publications, visit the IASP website at www.iasp-pain.org/Books