learning about safe systems dr. maureen baker cbe dm frcgp clinical director for patient safety nhs...
TRANSCRIPT
Learning about Safe Systems
Dr. Maureen Baker CBE DM FRCGPClinical Director for Patient Safety
NHS Connecting for Health
Overview
• The NPfIT• Development of patient safety movement• Safe systems in a safety critical industry• Safety management systems• NHS CFH Clinical Safety Management System• The Clinician/System Interface
The National Programme for IT in the NHS in England
• Established 2002• Has a number of central features and programmes
(National Spine; Choose and Book; GP2GP; National Care Record Service; Picture Archive and Communications Service; Electronic Transfer of Prescriptions)
• Local Service Providers• Estimated cost £12.4 Billion over 10 years (contracts,
training and implementation)• Being delivered by NHS Connecting for Health
What for?
NHS Modernisation?
OR
To support better safer care?
Healthcare – a Safety Critical Industry
• Studies based on retrospective analysis of medical records
• Harvard study 1991 (Lucien Leape) – adverse event rate in ‘hospitalisations’ of 3.7% of which two thirds were ‘errors’
• Australian study 1995 (Ross Wilson) – adverse event rate 16.6%
• British study 2001 (Charles Vincent) – adverse event rate of 10.8%
To Err is Human (Institute of Medicine 1999)
As many as 98,000 people die each year in USA from medical errors that occur in hospitals. That is more than die in RTAs or from breast cancer or AIDS. Medical error is fifth leading cause of death in USA
An Organisation with a Memory (CMO, 2000)
The NHS is doomed to make the same mistakes over and over again as we have no way of learning from when things go wrong
Human Error (Reason, 1990)
Humans are fallible and errors are inevitable
Systems approach takes holistic view of causes of failure
Cannot change the human condition but can change conditions in which people work and minimise opportunities for error
Learning from when disasters happen in safety critical industries
Complex set of interactions
No single causal factor
Combination of local conditions, human behaviours, social factors, organisational weaknesses
When things go wrong in healthcare
Complex set of interactions
No single causal factor
Combination of local conditions, human behaviours, social factors, organisational weaknesses
The Contribution of Health IT
Positive• Supporting clinicians in delivering better safer
care
Negative• BUT CAN INTRODUCE NEW HAZARDS
THAT WEREN’T THERE BEFORE !
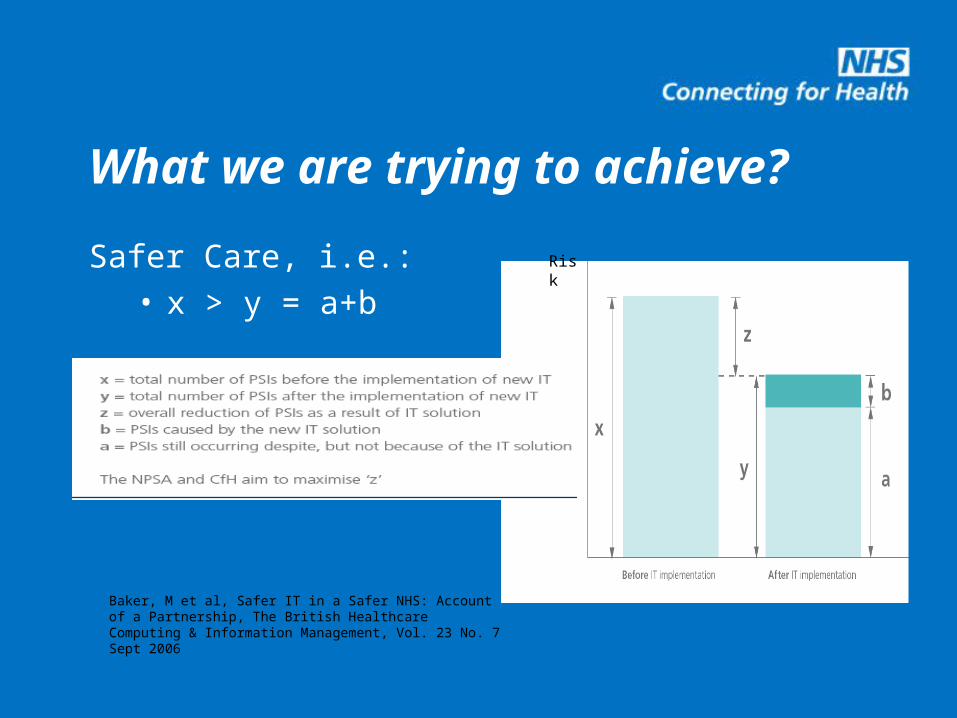
Safer Care, i.e.:• x > y = a+b
What we are trying to achieve?
Risk
Baker, M et al, Safer IT in a Safer NHS: Account of a Partnership, The British Healthcare Computing & Information Management, Vol. 23 No. 7 Sept 2006
Learning from failure
“The NHS is not unique: other sectors have experience of learning from failures which is of relevance to the NHS”
Sir Liam Donaldson in ‘Organisation with a Memory’
Safety Critical Industries with Safety Approach
Aviation
Railways
Oil and Gas
Construction
Nuclear
Military
NHS CFH Clinical Safety Management System
• Based on principles of IEC 61508• Light touch, yet robust• Three key pieces of documentation• Practical and pragmatic – in place for over 4
years• Supplemented by established Safety Incident
Management Process
NHS CFH CSMS Deliverables
• Hazard assessment• Safety case• Safety closure report• Clinical Authority to Release (CATR) (Includes ‘caveats’)
Safety
Closure
Report
Patient
Safety
AssessmentClinical
Systems
Safety Case
Safety
Closure
Report
Safety
Closure
Report
Patient
Safety
Assessment
Patient
Safety
AssessmentClinical
Systems
Safety Case
Clinical
Systems
Safety Case
Safety Incident Management System
• Incidents related to Health IT reported and logged
• Assessed and managed by Clinical Safety Group (clinicians and safety engineers)
• Aim to ‘make safe’ (remove potential for harm) with 24 hours
• Around 430 incidents reported since 2005• 97% made safe within 24 hours

NHS IT – What can go wrong?
• Patient identification (wrong notes, wrong results, wrong procedure)
• Data migration (re-start discontinued drugs, incorrect preservation of meaning)
• Data mapping (mapped to non-identical preparation, eg long-acting or slow release)
• Data corruption (over-writing of info on NHS Spine)
The Role of Clinicians in Safety Management
• Awareness – not just IT, not just records, but systems that can have positive or negative impact on patient care
• Risk management and safe implementation – engage in assessing what could go wrong and what can be done to prevent things going wrong
• Data quality is a patient safety issue• Remain ‘thinking clinicians’ – IT is a tool, YOU are the
clinician
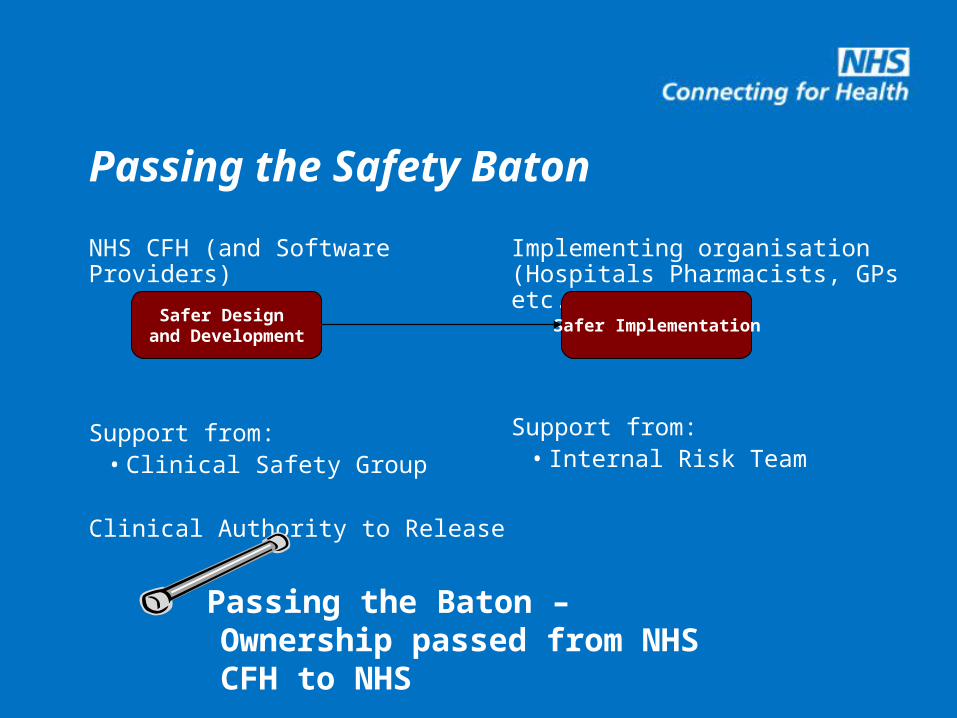
Passing the Safety Baton
NHS CFH (and Software Providers)
Support from:• Clinical Safety Group
Clinical Authority to Release
Implementing organisation (Hospitals Pharmacists, GPs etc.)
Support from:• Internal Risk Team
Safer Design and Development
Safer Implementation
Passing the Baton – Ownership passed from NHS CFH to NHS
National Programme for IT in NHS
“ The National Programme is not just an IT programme, but a patient safety and clinical governance programme”
Gordon Hextall, Chief Operating Officer
NHS CFH
Conclusion
• Healthcare is a safety critical industry• IT systems don’t deliver care, but are used by
clinicians in the delivery of care• Good safety practice requires proactive work –
systems as safe as design and forethought will allow
• Understanding of benefit and risks of IT by clinicians is essential for safe care