leadership and culture - the improvement...
TRANSCRIPT

Leadership and
Culture
Follow us on twitter @spsp_mh #spspmh5

Agenda 11.15 - 11.20 Introduction – David Hall 11.20 - 11.35 Quality Improvement, Leadership and Culture – Amar Shah and Kevin Cleary 11.35 - 11.50 Service users leadership role and the Patient Safety Climate Tool – Joyce Mouriki, MBE and Wendy McAuslan 11.50 - 12.00 Questions and Answers – All presenters 12.00 - 12.15 Workstream essentials 12.15 - 12.30 Whole group discussion
#spspmh5

Quality improvement
Leadership and culture
@ELFT_QI qi.eastlondon.nhs.uk
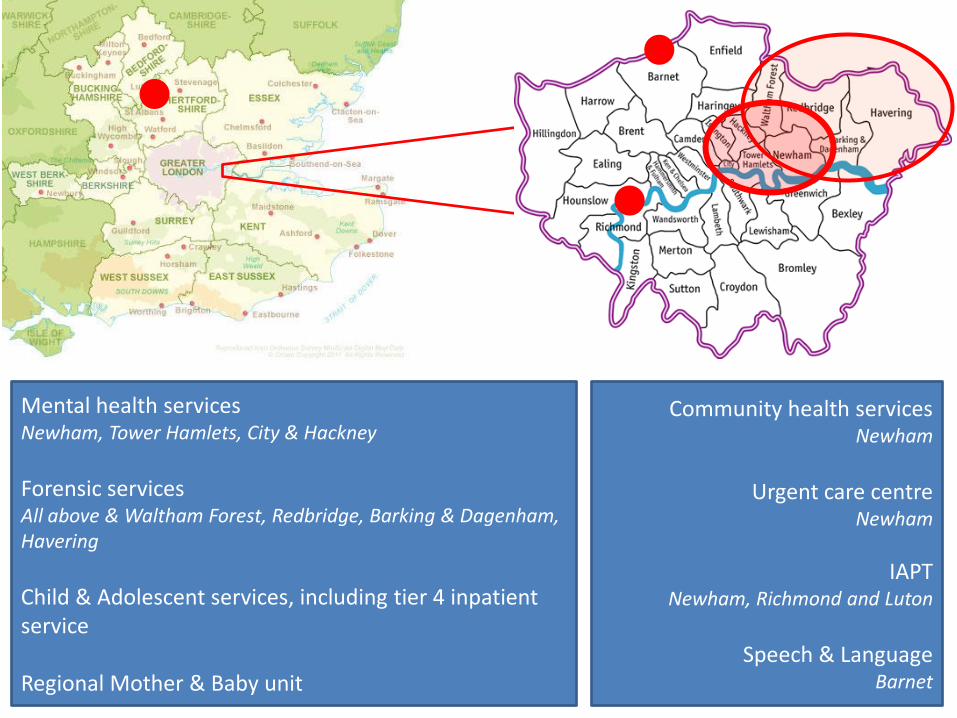
Mental health services Newham, Tower Hamlets, City & Hackney
Forensic services All above & Waltham Forest, Redbridge, Barking & Dagenham, Havering
Child & Adolescent services, including tier 4 inpatient service Regional Mother & Baby unit
Community health services Newham
Urgent care centre
Newham
IAPT Newham, Richmond and Luton
Speech & Language
Barnet

Challenges and
opportunities in East London
Cultural diversity
Social deprivation
Geographical diversity
Commissioning arrangements
Financial stability and
strong assurance systems

Our quality
improvement programme
Why?
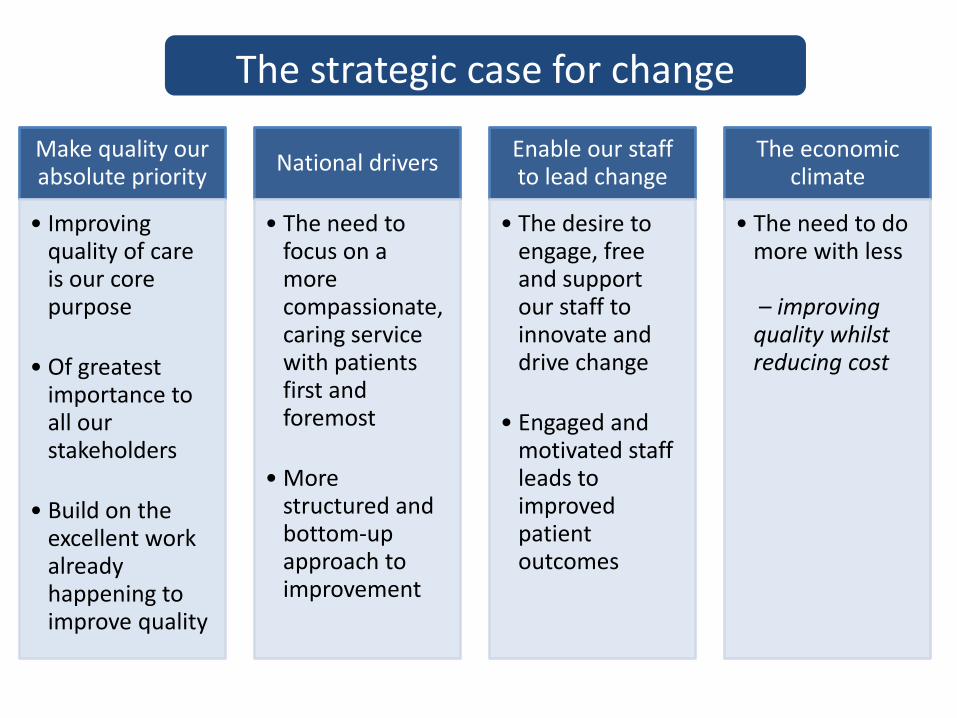
The strategic case for change
Make quality our absolute priority
• Improving quality of care is our core purpose
• Of greatest importance to all our stakeholders
• Build on the excellent work already happening to improve quality
National drivers
• The need to focus on a more compassionate, caring service with patients first and foremost
• More structured and bottom-up approach to improvement
Enable our staff to lead change
• The desire to engage, free and support our staff to innovate and drive change
• Engaged and motivated staff leads to improved patient outcomes
The economic climate
• The need to do more with less – improving quality whilst reducing cost
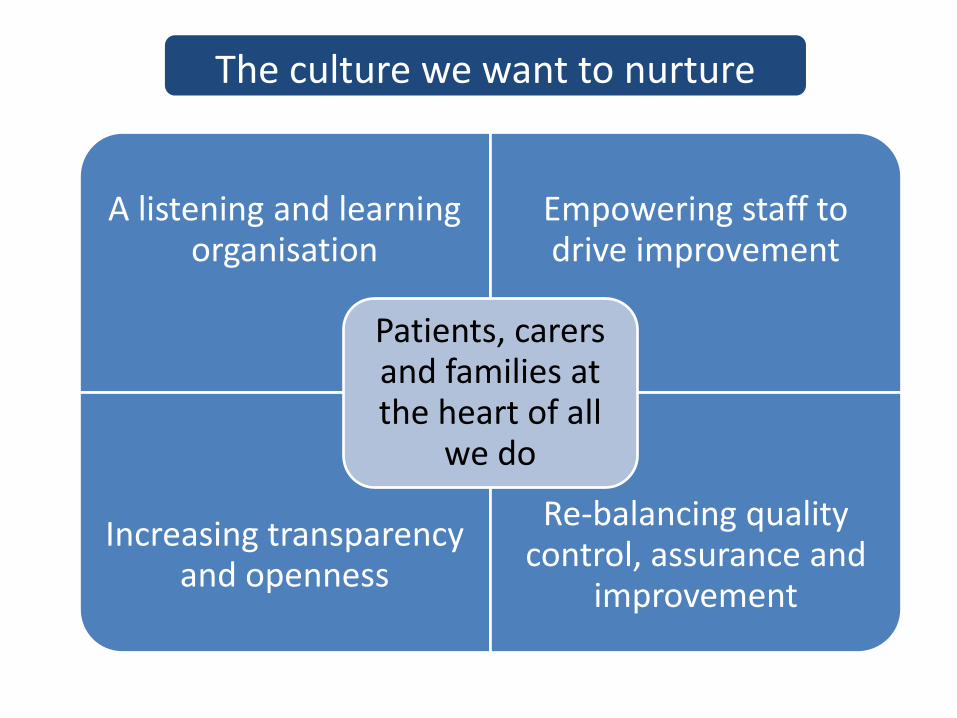
The culture we want to nurture
A listening and learning organisation
Empowering staff to drive improvement
Increasing transparency and openness
Re-balancing quality control, assurance and
improvement
Patients, carers and families at the heart of all
we do

Our quality
improvement programme
How?
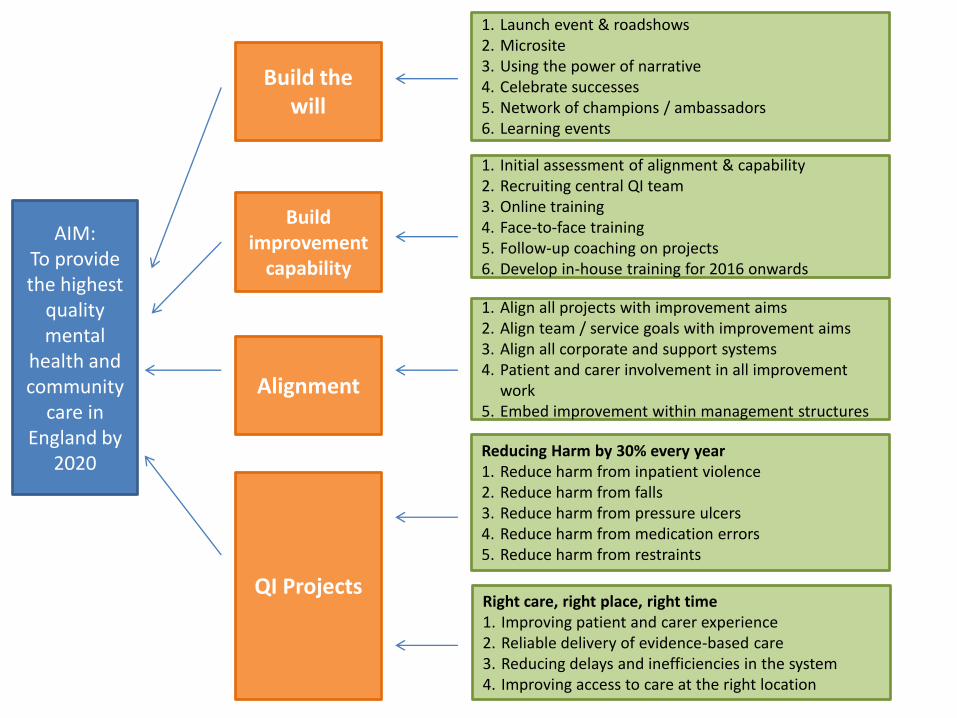
AIM: To provide the highest
quality mental
health and community
care in England by
2020
Build the will
Build improvement
capability
Alignment
QI Projects
1. Launch event & roadshows 2. Microsite 3. Using the power of narrative 4. Celebrate successes 5. Network of champions / ambassadors 6. Learning events
1. Initial assessment of alignment & capability 2. Recruiting central QI team 3. Online training 4. Face-to-face training 5. Follow-up coaching on projects 6. Develop in-house training for 2016 onwards
1. Align all projects with improvement aims 2. Align team / service goals with improvement aims 3. Align all corporate and support systems 4. Patient and carer involvement in all improvement
work 5. Embed improvement within management structures
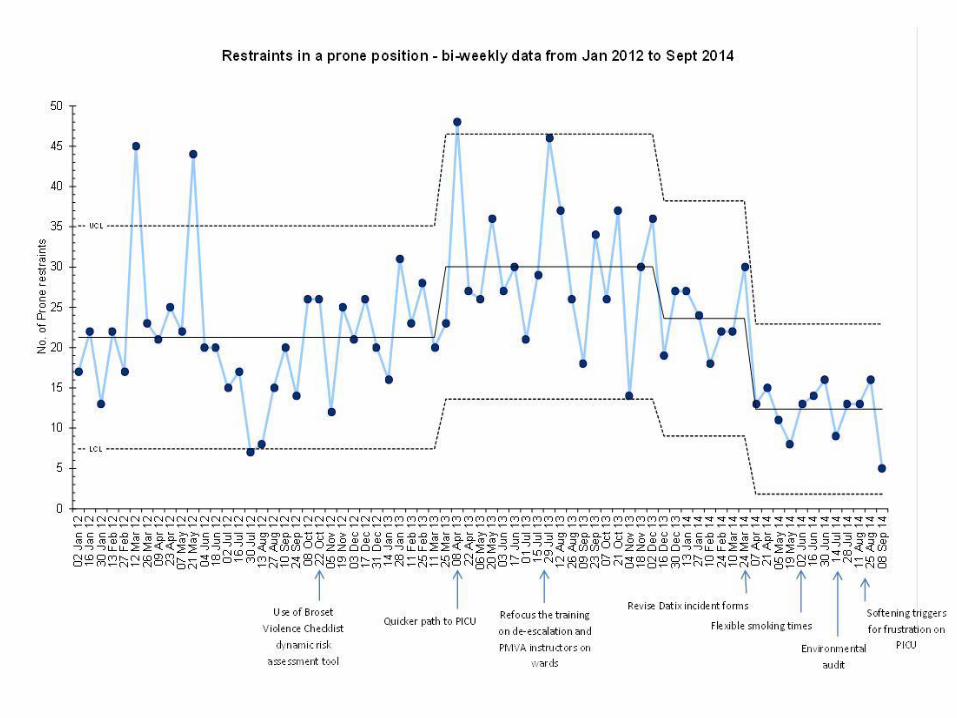
Reducing Harm by 30% every year 1. Reduce harm from inpatient violence 2. Reduce harm from falls 3. Reduce harm from pressure ulcers 4. Reduce harm from medication errors 5. Reduce harm from restraints
Right care, right place, right time 1. Improving patient and carer experience 2. Reliable delivery of evidence-based care 3. Reducing delays and inefficiencies in the system 4. Improving access to care at the right location

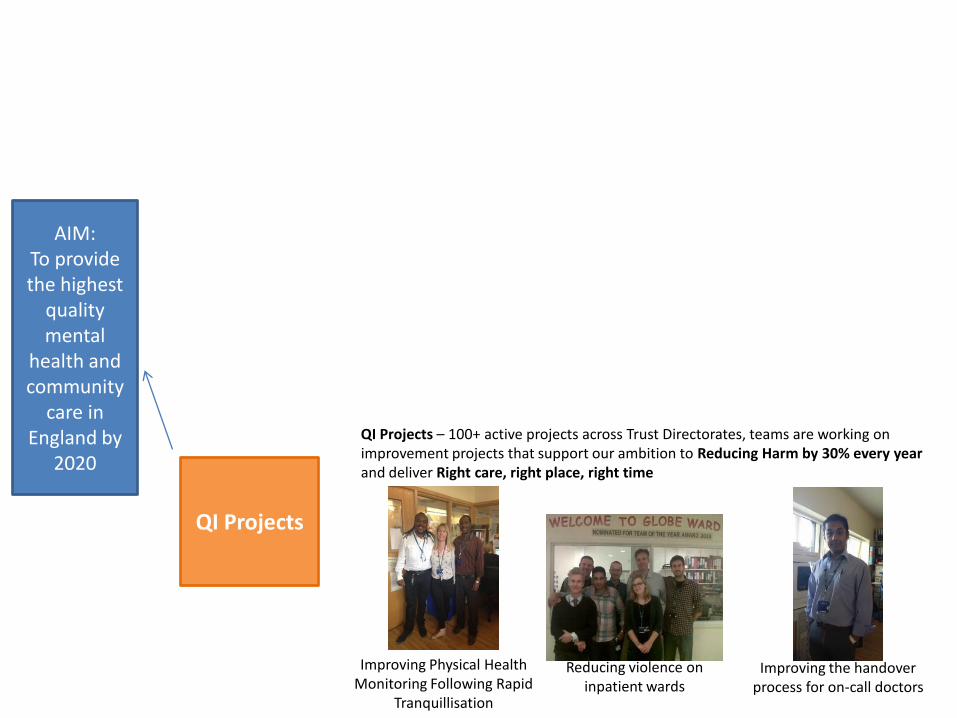
AIM: To provide the highest
quality mental
health and community
care in England by
2020
Build the will
QI microsite the online hub for the programme qi.eastlondon.nhs.uk
Staff and service user newsletter reaches 4000 people every month
QI launch event and roadshows attended by over 1000 staff, service users and carers
Bespoke QI learning events for staff, service users, commissioners, governors
AIM: To provide the highest
quality mental
health and community
care in England by
2020 Build improvement
capability
Face to face improvement training - hundreds of staff, services users, Governors to be trained over the next few years
Support for improvement work from
the Trust’s QI team
IHI Open School available to all
Strategic partnership with IHI
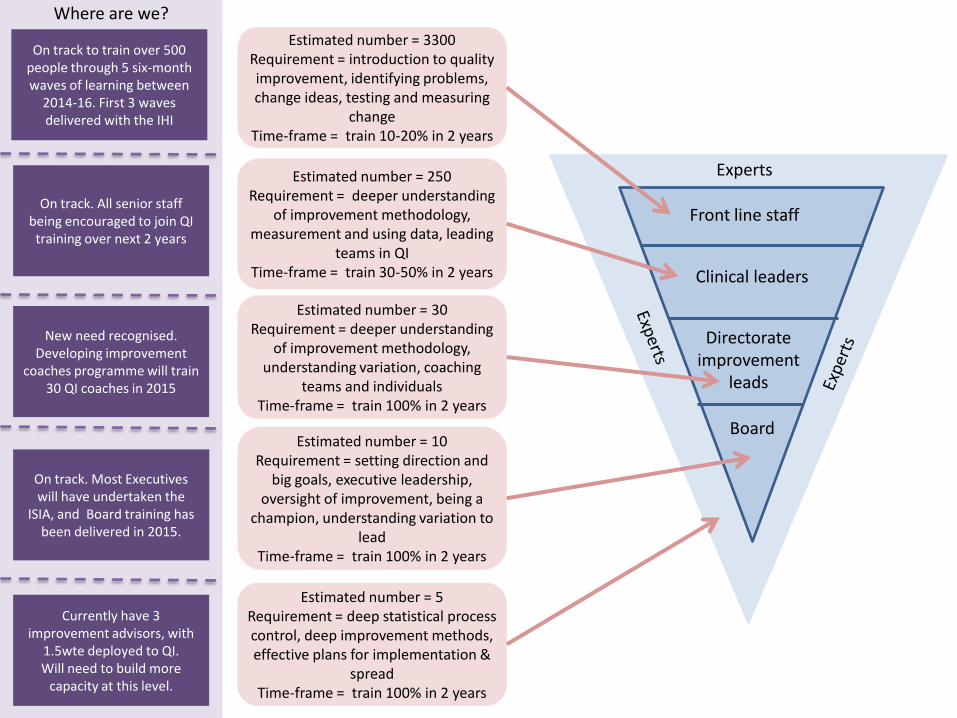
Experts
Front line staff
Clinical leaders
Directorate improvement
leads
Board
Estimated number = 3300 Requirement = introduction to quality improvement, identifying problems, change ideas, testing and measuring
change Time-frame = train 10-20% in 2 years
Estimated number = 250 Requirement = deeper understanding
of improvement methodology, measurement and using data, leading
teams in QI Time-frame = train 30-50% in 2 years
Estimated number = 30 Requirement = deeper understanding
of improvement methodology, understanding variation, coaching
teams and individuals Time-frame = train 100% in 2 years
Estimated number = 10 Requirement = setting direction and
big goals, executive leadership, oversight of improvement, being a
champion, understanding variation to lead
Time-frame = train 100% in 2 years
Estimated number = 5 Requirement = deep statistical process control, deep improvement methods, effective plans for implementation &
spread Time-frame = train 100% in 2 years
Where are we?
On track to train over 500 people through 5 six-month waves of learning between
2014-16. First 3 waves delivered with the IHI
On track. All senior staff being encouraged to join QI training over next 2 years
New need recognised. Developing improvement
coaches programme will train 30 QI coaches in 2015
On track. Most Executives will have undertaken the
ISIA, and Board training has been delivered in 2015.
Currently have 3 improvement advisors, with
1.5wte deployed to QI. Will need to build more
capacity at this level.

AIM: To provide the highest
quality mental
health and community
care in England by
2020
A process is in place for teams to submit project ideas to the QI team, who will help with planning, structure and measurement, and ensure projects are aligned with our high-level aims.
Alignment
Quality improvement programme-project support structures
AIM: To provide the highest
quality mental
health and community
care in England by
2020
QI Projects
QI Projects – 100+ active projects across Trust Directorates, teams are working on improvement projects that support our ambition to Reducing Harm by 30% every year and deliver Right care, right place, right time
Improving Physical Health Monitoring Following Rapid
Tranquillisation
Reducing violence on inpatient wards
Improving the handover process for on-call doctors
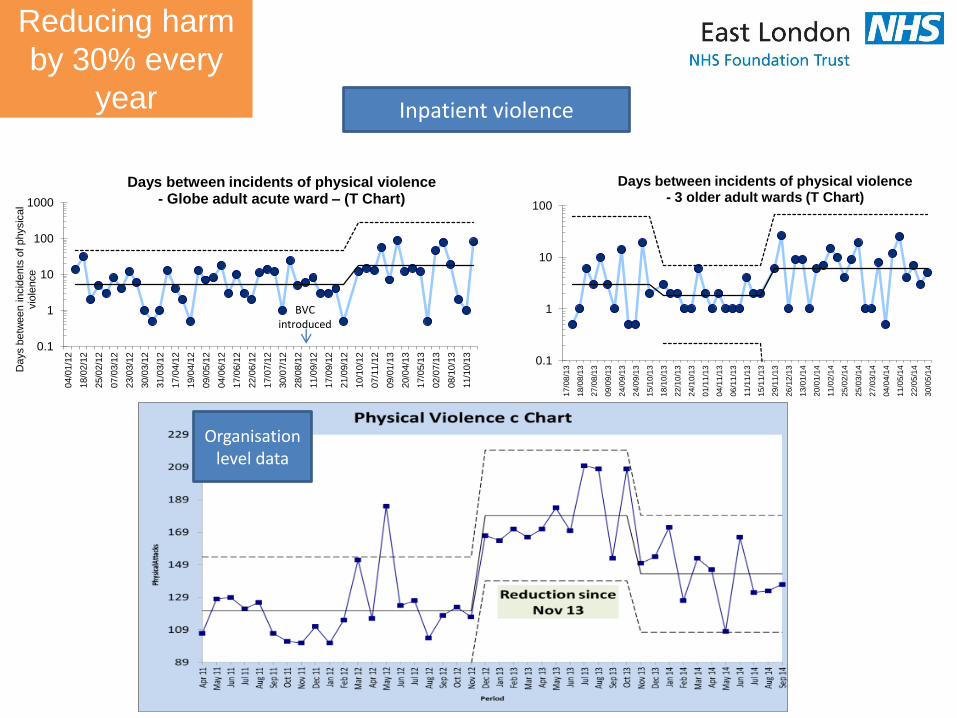
Reducing harm
by 30% every
year
0.1
1
10
100
1000
04/0
1/1
2
18/0
2/1
2
25/0
2/1
2
07/0
3/1
2
23/0
3/1
2
30/0
3/1
2
31/0
3/1
2
17/0
4/1
2
19/0
4/1
2
09/0
5/1
2
04/0
6/1
2
17/0
6/1
2
22/0
6/1
2
17/0
7/1
2
30/0
7/1
2
28/0
8/1
2
11/0
9/1
2
17/0
9/1
2
21/0
9/1
2
10/1
0/1
2
07/1
1/1
2
09/0
1/1
3
20/0
4/1
3
17/0
5/1
3
02/0
7/1
3
08/1
0/1
3
11/1
0/1
3
Days b
etw
een in
cid
ents
of physic
al
vio
lence
Days between incidents of physical violence - Globe adult acute ward – (T Chart)
BVC introduced
0.1
1
10
100
17
/08
/13
18
/08
/13
27
/08
/13
09
/09
/13
24
/09
/13
24
/09
/13
15
/10
/13
18
/10
/13
22
/10
/13
24
/10
/13
01
/11
/13
04
/11
/13
06
/11
/13
11
/11
/13
15
/11
/13
29
/11
/13
26
/12
/13
13
/01
/14
20
/01
/14
11
/02
/14
25
/02
/14
25
/03
/14
27
/03
/14
04
/04
/14
11
/05
/14
22
/05
/14
30
/05
/14
Days between incidents of physical violence - 3 older adult wards (T Chart)
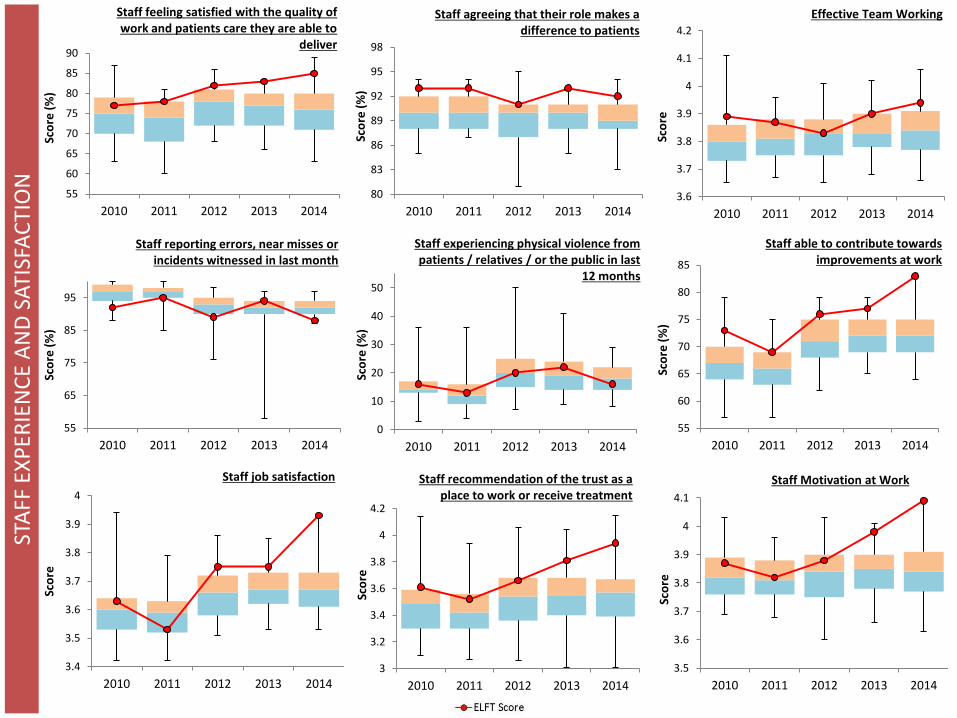
Inpatient violence
Organisation level data
STA
FF E
XP
ERIE
NC
E A
ND
SAT
ISFA
CTI
ON
55
60
65
70
75
80
85
90
2010 2011 2012 2013 2014
Sco
re (
%)
Staff feeling satisfied with the quality of work and patients care they are able to
deliver
80
83
86
89
92
95
98
2010 2011 2012 2013 2014
Sco
re (
%)
Staff agreeing that their role makes a difference to patients
3.6
3.7
3.8
3.9
4
4.1
4.2
2010 2011 2012 2013 2014
Sco
re
Effective Team Working
55
65
75
85
95
2010 2011 2012 2013 2014
Sco
re (
%)
Staff reporting errors, near misses or incidents witnessed in last month
0
10
20
30
40
50
2010 2011 2012 2013 2014
Sco
re (
%)
Staff experiencing physical violence from patients / relatives / or the public in last
12 months
55
60
65
70
75
80
85
2010 2011 2012 2013 2014
Sco
re (
%)
Staff able to contribute towards improvements at work
3.4
3.5
3.6
3.7
3.8
3.9
4
2010 2011 2012 2013 2014
Sco
re
Staff job satisfaction
3
3.2
3.4
3.6
3.8
4
4.2
2010 2011 2012 2013 2014
Sco
re
Staff recommendation of the trust as a place to work or receive treatment
3.5
3.6
3.7
3.8
3.9
4
4.1
2010 2011 2012 2013 2014
Sco
re
Staff Motivation at Work
Leading cultural
transformation through QI
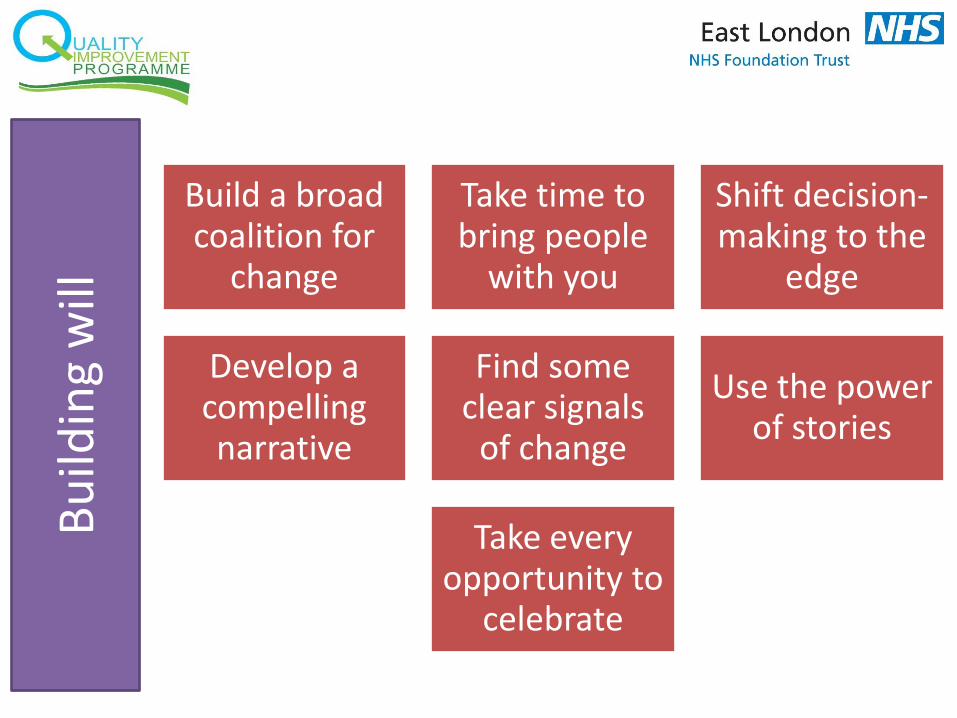
Bu
ildin
g w
ill
Build a broad coalition for
change
Take time to bring people
with you
Shift decision-making to the
edge
Develop a compelling narrative
Find some clear signals
of change
Use the power of stories
Take every opportunity to
celebrate
Bu
ildin
g ca
pab
ility
&
cap
acit
y
Be prepared to invest
Train all levels and across disciplines
Realign existing
resources
Stop lower value work
Alig
nm
ent
& in
tegr
atio
n
Start at the top Create a support
structure
Build a learning system
Ensure patients and carers are
integral
Ensure the context is ripe
Line of sight from team to system goals

QI Team
QI Resources
Project Sponsor
QI Forums

Think big. Start small. Move fast.
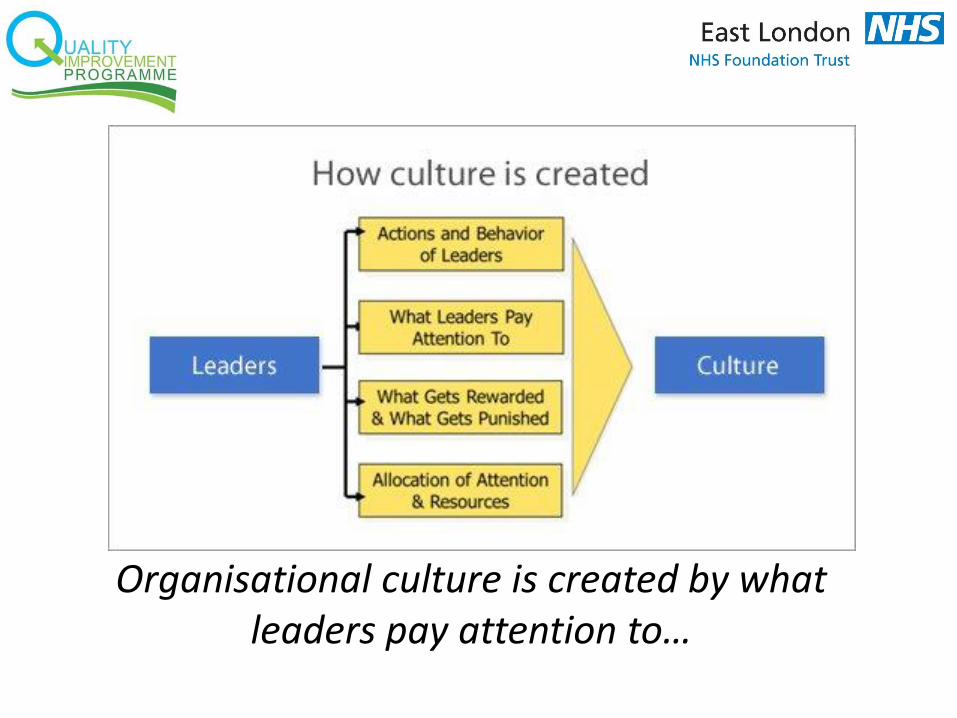
Organisational culture is created by what leaders pay attention to…

web qi.eastlondon.nhs.uk email [email protected] @ELFT_QI
Service User Leadership and
Culture
Joyce Mouriki, VOX’s chairperson
Wendy McAuslan, VOX’s Development Coordinator
Leaders don’t create followers..
they create more leaders
Tom Peters
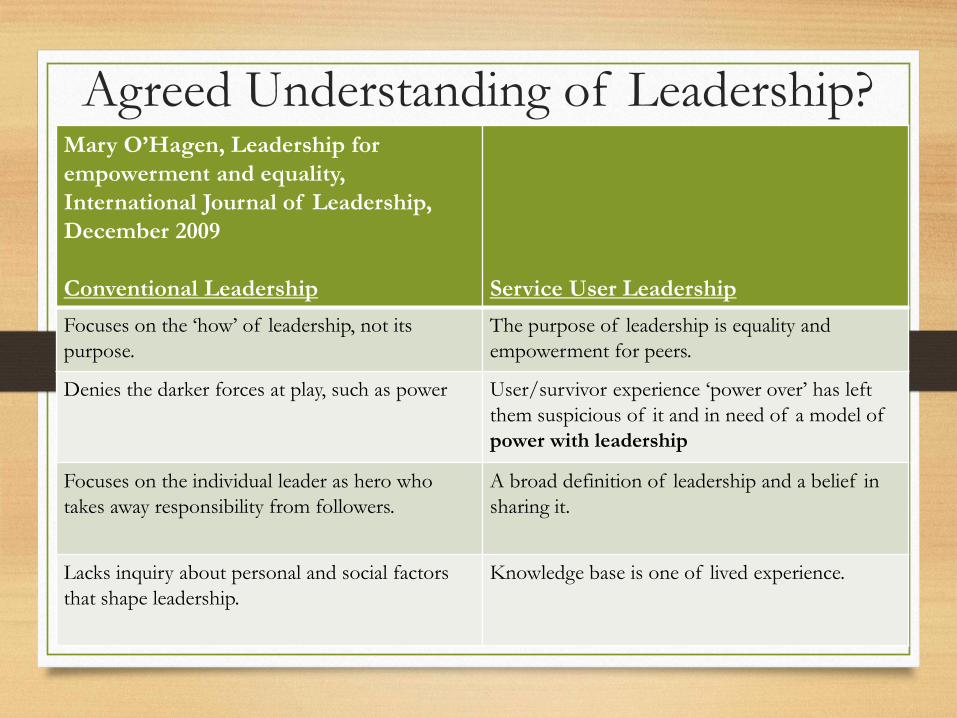
Agreed Understanding of Leadership?
Mary O’Hagen, Leadership for
empowerment and equality,
International Journal of Leadership,
December 2009
Conventional Leadership
Service User Leadership
Focuses on the ‘how’ of leadership, not its
purpose.
The purpose of leadership is equality and
empowerment for peers.
Denies the darker forces at play, such as power
User/survivor experience ‘power over’ has left
them suspicious of it and in need of a model of
power with leadership
Focuses on the individual leader as hero who
takes away responsibility from followers.
A broad definition of leadership and a belief in
sharing it.
Lacks inquiry about personal and social factors
that shape leadership.
Knowledge base is one of lived experience.
Important Elements in Service
User Leadership
Personal development through the experience of mental
distress.
Empathy for other service users/patients.
Ability to encourage others to use their strengths and
resources.
Ability to relate to diverse groups of service users/patients.
Ability to be non-judgemental
VOX Leadership Program
An asset based community
development approach
• recruits and trains a number of “community leaders”
• focuses on key populations who experience structural
and mental health inequalities
• creates peer leaders who are best placed to challenge
stigma and discrimination
• peer leaders can provide specific training sessions to
diverse groups and organisations using a community
conversations approach
General population approach-Developing
leadership in order to;
• Support patients to have a greater awareness of their situation so that they can make informed decisions and choices; e.g. encourage using advocacy
• Support patients to have more control over the direction of their lives; e.g. support the development of advance statements
• Understand the patients perspective e.g. develop tools which tap into their views (patient safety climate tool)
• and challenge stigma, injustice and social exclusion (in conjunction with practitioners and members of the wider community)
Ultimate Aim Shared
Leadership?
• Shared purpose and collective goals
• Social support - recognition of everyones’ contributions and accomplishments.
• Voice – the degree of input.
Carson et al. (2007)]
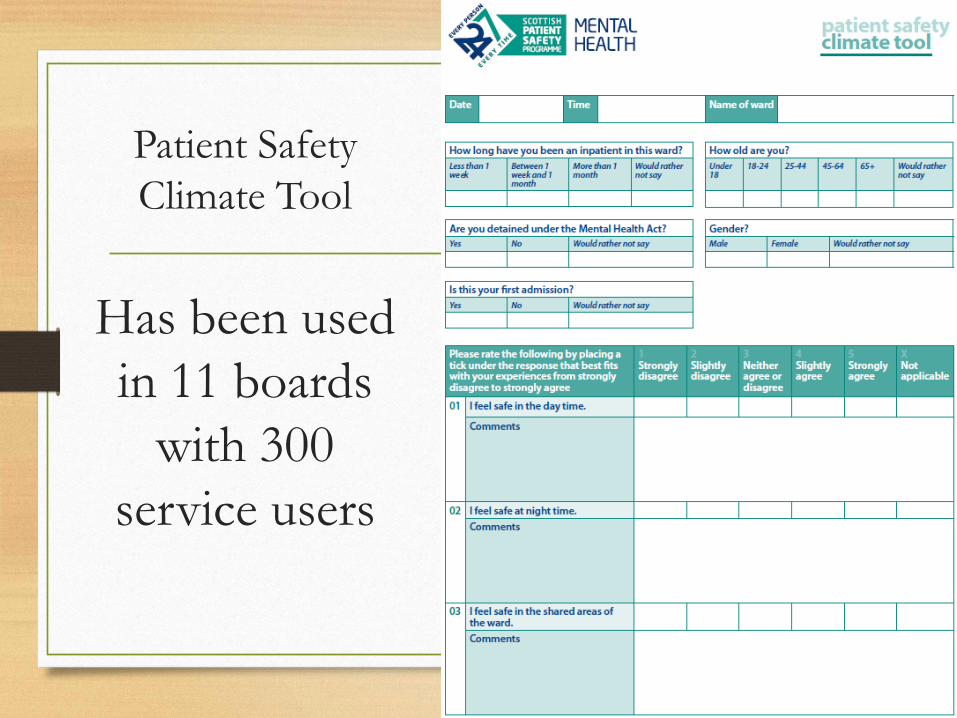
Patient Safety
Climate Tool
Has been used
in 11 boards
with 300
service users
Service user leadership myth or
reality?
• Methods to demonstrate better outcomes – example
community conversations
• Shared learning – events co facilitated by service user
leads- better shared understanding
• Tools designed by service users for service users –
implemented jointly for maximum benefit
• And continuous improvement
Who can help? - to find out more
about VOX contact Wendy
www.voxscotland.org.uk
Wendy McAuslan
0141 572 1663
Questions and Answers
David Hall
Amar Shah
Kevin Cleary
Joyce Mouriki, MBE
Wendy McAuslan
#spspmh5
Leadership and Culture Essentials
• Patient Safety Climate Tool
• Staff Climate Tool
• Leadership walkrounds/ safety conversations
• Learning from adverse events
#spspmh5
Workstream essentials – questions/issues
• Are they correct?
• If not, what should they be?
• What are we already doing?
• What change packages, bundles, interventions should be developed and tested to deliver them?

Lunch – available outside Strathallan Foyer and opposite Stuart Lounge
Storyboard viewing – Strathallan Drop in data surgery - Glenallan