laparoscopic myomectomy
TRANSCRIPT

MAGDY ABDELRAHMAN MOHAMEDLECTURER OF OB/GYN
2015

Nomenclature Fibroid--------Fibroids
Myoma--------Myomata
Fibromyoma—Fibromyomata
Leiomyoma---Leiomyomata

Fibroids (leiomyomas) are benign smooth muscle cell tumors of the uterus.
Although they are extremely common, with an overall incidence of 40% to 60% by age 35 and 70% to 80% by age 50, the precise etiology of uterine fibroids remains unclear.

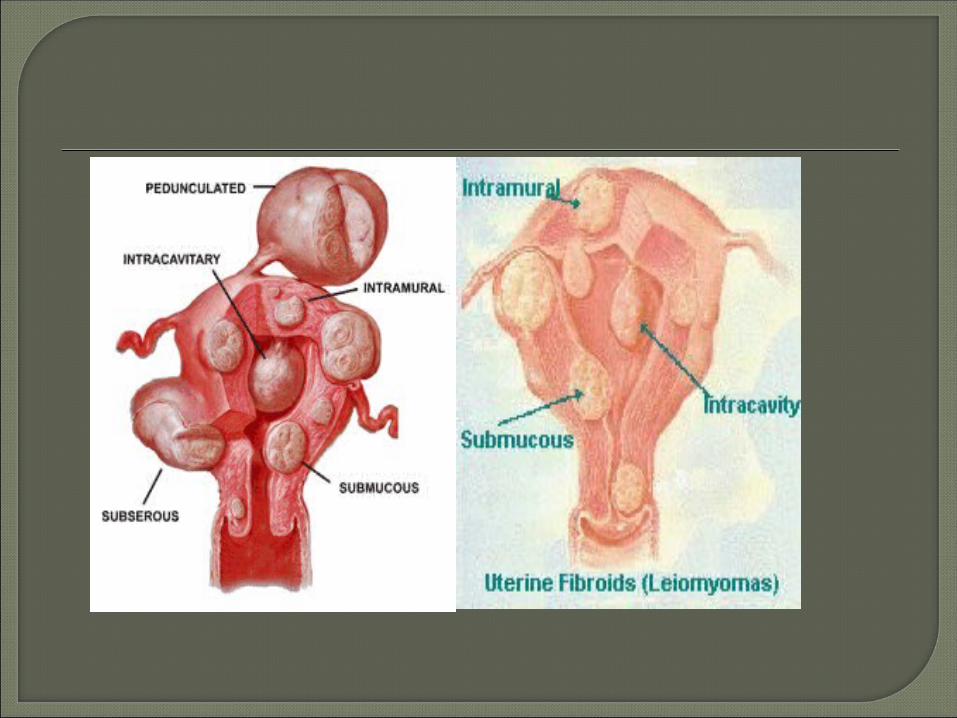
Described based on location in the uterus:• Intramural: develop from within uterine
wall, do not distort uterine cavity, <50% protruding into serosal surface.
• Submucosal: develop from myometrial cells just below endometrium, often protrude into and distort uterine cavity.

• Subserosal: originate from serosal surface of uterus, >50% protrudes out of serosal surface.
• Cervical: located in the cervix, rather than uterine corpus.




It was first described at 1979 by Semm, exclusively for subserous myoma.
From the beginning of 1990s, the technique was developed to include extraction of intramural myoma.

Should be particularly meticulous, there is no intraoperative palpation.• TAS , TVS.• Doppler assement.• MRI.• Diagnosic hysteroscopy, In selected cases.

Correction of anemia. GnRH analogues (controversial).
Size of myoma < 10 cm. Number ≤ 3.

Each myoma must be excised via its own hysterotomy.
Preventive occlusion of the uterine artery, using a clip, is prefered to decrease intra-operative Hge.

Dissection must take place along the cleavage plane.
Avoid iatrogenic lesions of the other pelvic organs.
Meticulous closure of myomectomy site.







Direct suprapubic extraction for small myoma.
Posterior colpotomy. Electric morcellation.
Broad ligament access to the uterine artery.
Posterior access to the uterine artery.

Dissection of the right broad ligament


Posterior access to perform occlusion of the uterine artery




Incidence: variable (5-40%) Factor increase the conversion rate:
• Size of the dominant myoma at ultrasonography.• Anterior location.• Intramural type. • Preoperative use of GnRH agonists.

There are several arguments suggesting that the laparoscopic approach reduces the risk of postoperative adhesions after myomectomy.

Only 2 randomized controlled trials compared myomectomy by laparotomy or laparoscopy.
There was no significant differences in the pregnancy and abortion rate.
Seracchioli et al 2000, Palomba et al 2007.

There is considerable debate concerning the strength of hysterotomy scars after laparoscopic myomectomy.
Particular care must be given to uterine closure.


Rate is higher than laparotomy & the time lapse before recurrence is shorter.
It is impossible to palpate the myometrium thoroughly, and small intramural nuclei which do not deform the uterine serosa can be overlooked.


Advantages:• 3-dimensional image.• Absence of tremor.• Superior instrument articulation.• Comfort for the surgeon.• Faster learning curve.


Laparoscopic myomectomy is a safe technique which has several advantages, including less postoperative pain, shorter recovery time and reduced post-myomectomy adhesion formation in comparison with the laparotomy.

However, it is a difficult operation, and the surgeon needs to be well experienced in laparoscopic surgery.
