laboratory diagnosis of allergy - tmlpath.com.au · laboratory diagnosis of allergy ... an...
TRANSCRIPT
INSIDE THIS ISSUE:> Laboratory Diagnosis of Allergy
> Faecal Calprotectin: A Biomarker of Bowel Inflammation
> Blood Tests in Investigation of Coeliac Disease
ISSUE 2, 2017
If you would prefer to receive the newsletter electronically, please email [email protected]
Laboratory Diagnosis of AllergyDr David Heyworth-Smith
Allergic disorders are increasingly prominent in Australia and globally. This reflects both a true increase in the burden of allergic disease, especially that of childhood food allergy in the last 2 decades, and also increased awareness of allergy amongst health care and community members. Correspondingly, advances in allergy diagnosis and management have occurred over this period.
The management of allergic disorders requires accurate diagnosis of the offending triggers or allergens provoking the condition.
Tasmanian Medical laboratories provides tests for allergy diagnosis including In vitro Specific IgE (RAST) detection, and specific IgE for native and recombinant component allergens. Our methodology utilises world leading technology including Phadia ImmunoCAP and ISAC systems.
The detection of specific IgE is integral to the assessment and management of allergic disorders including those of:
• Allergic rhino conjunctivitis• Atopic eczema• Asthma• Food allergy• Stinging insect allergy• Certain drug allergies• Certain occupational allergies
>>> CONTINUED OVERLEAF
FEATURE ARTICLE
ALLERGEN-SPECIFIC IGE
An allergen-specific IgE test is used to measure the amount of IgE antibody in the serum that is specific to a particular allergen. In clinical practice, 0.35 kU/L has commonly been used as a cut-off for allergen-specific IgE to separate positive from negative results. Measurement of low levels of IgE (between 0.10 and 0.50 kU/L) have recently been shown to be important in some patients for particular allergens and Tasmanian Medical Laboratories now reports these results down to a concentration of 0.10kU/L. These are most relevant for some drug and venom allergens. Specific IgE results of <0.10 kU/L on the Phadia ImmunoCAP platform indicate low probability of clinical allergy to a specific allergen, whereas high antibody levels to an allergen show good correlation with clinical allergy to a specific allergen. Significance may also be affected by total IgE levels, which is a useful additional test to assist with interpretation. Very elevated levels of total IgE (e.g. > 5000 kU/L) may lead to low level false positive specific IgE results.
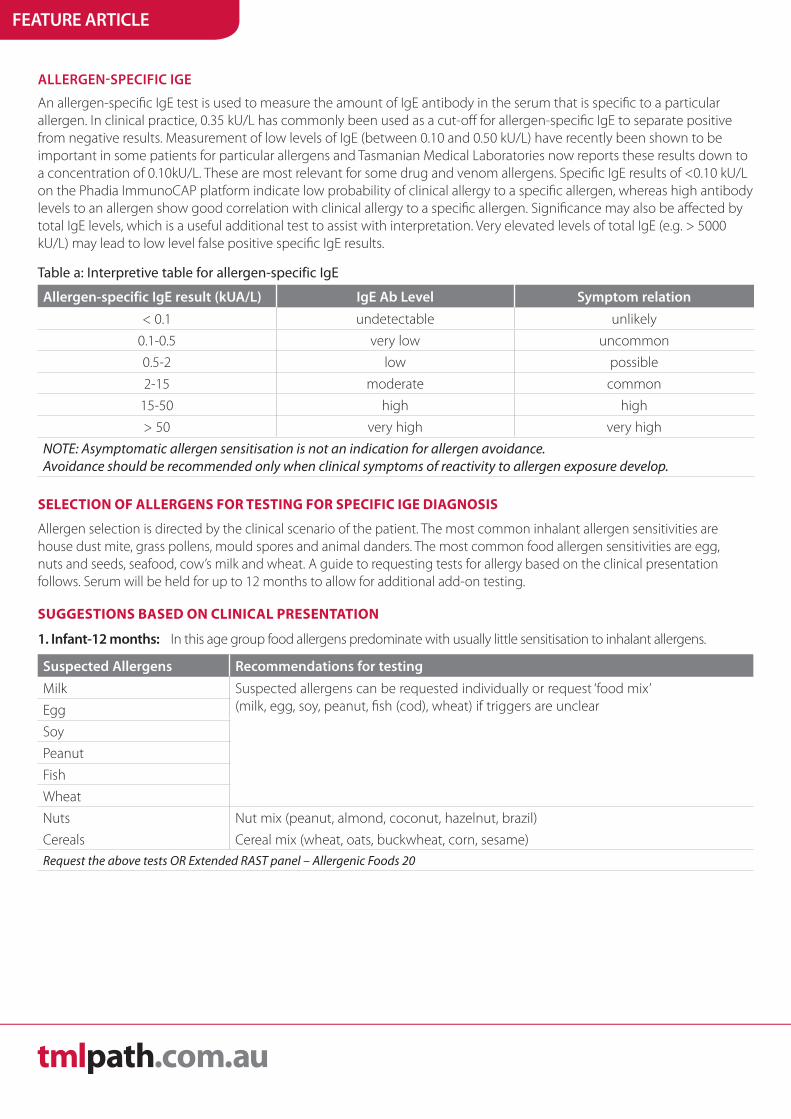
Table a: Interpretive table for allergen-specific IgE
Allergen-specific IgE result (kUA/L) IgE Ab Level Symptom relation
< 0.1 undetectable unlikely
0.1-0.5 very low uncommon
0.5-2 low possible
2-15 moderate common
15-50 high high
> 50 very high very high
NOTE: Asymptomatic allergen sensitisation is not an indication for allergen avoidance.Avoidance should be recommended only when clinical symptoms of reactivity to allergen exposure develop.
SELECTION OF ALLERGENS FOR TESTING FOR SPECIFIC IGE DIAGNOSIS
Allergen selection is directed by the clinical scenario of the patient. The most common inhalant allergen sensitivities are house dust mite, grass pollens, mould spores and animal danders. The most common food allergen sensitivities are egg, nuts and seeds, seafood, cow’s milk and wheat. A guide to requesting tests for allergy based on the clinical presentation follows. Serum will be held for up to 12 months to allow for additional add-on testing.
SUGGESTIONS BASED ON CLINICAL PRESENTATION
1. Infant-12 months: In this age group food allergens predominate with usually little sensitisation to inhalant allergens.
Suspected Allergens Recommendations for testing
Milk Suspected allergens can be requested individually or request ‘food mix’(milk, egg, soy, peanut, fish (cod), wheat) if triggers are unclearEgg
Soy
Peanut
Fish
Wheat
Nuts Nut mix (peanut, almond, coconut, hazelnut, brazil)
Cereals Cereal mix (wheat, oats, buckwheat, corn, sesame) Request the above tests OR Extended RAST panel – Allergenic Foods 20
FEATURE ARTICLE
>>> CONTINUED OVERLEAF
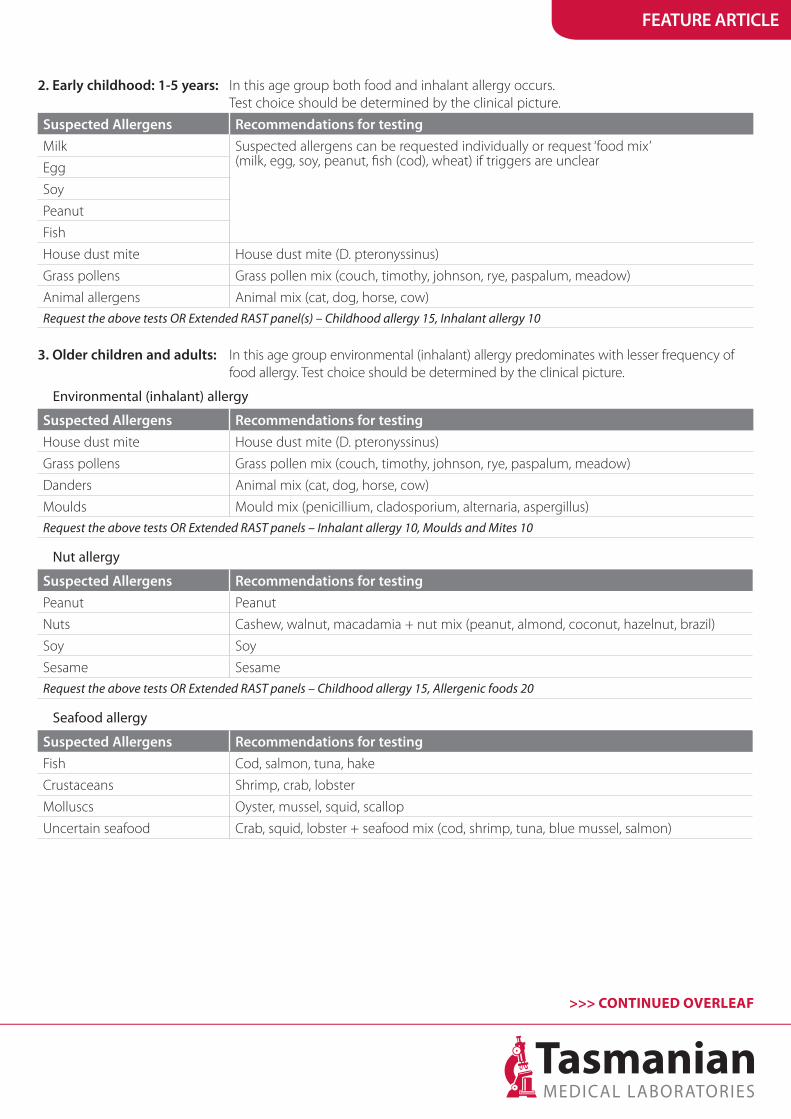
2. Early childhood: 1-5 years: In this age group both food and inhalant allergy occurs. Test choice should be determined by the clinical picture.
Suspected Allergens Recommendations for testing
Milk Suspected allergens can be requested individually or request ‘food mix’(milk, egg, soy, peanut, fish (cod), wheat) if triggers are unclear Egg
Soy
Peanut
Fish
House dust mite House dust mite (D. pteronyssinus)
Grass pollens Grass pollen mix (couch, timothy, johnson, rye, paspalum, meadow)
Animal allergens Animal mix (cat, dog, horse, cow)Request the above tests OR Extended RAST panel(s) – Childhood allergy 15, Inhalant allergy 10
3. Older children and adults: In this age group environmental (inhalant) allergy predominates with lesser frequency of food allergy. Test choice should be determined by the clinical picture.
Environmental (inhalant) allergy
Suspected Allergens Recommendations for testing
House dust mite House dust mite (D. pteronyssinus)
Grass pollens Grass pollen mix (couch, timothy, johnson, rye, paspalum, meadow)
Danders Animal mix (cat, dog, horse, cow)
Moulds Mould mix (penicillium, cladosporium, alternaria, aspergillus)Request the above tests OR Extended RAST panels – Inhalant allergy 10, Moulds and Mites 10
Nut allergy
Suspected Allergens Recommendations for testing
Peanut Peanut
Nuts Cashew, walnut, macadamia + nut mix (peanut, almond, coconut, hazelnut, brazil)
Soy Soy
Sesame SesameRequest the above tests OR Extended RAST panels – Childhood allergy 15, Allergenic foods 20
Seafood allergy
Suspected Allergens Recommendations for testing
Fish Cod, salmon, tuna, hake
Crustaceans Shrimp, crab, lobster
Molluscs Oyster, mussel, squid, scallop
Uncertain seafood Crab, squid, lobster + seafood mix (cod, shrimp, tuna, blue mussel, salmon)
FEATURE ARTICLE
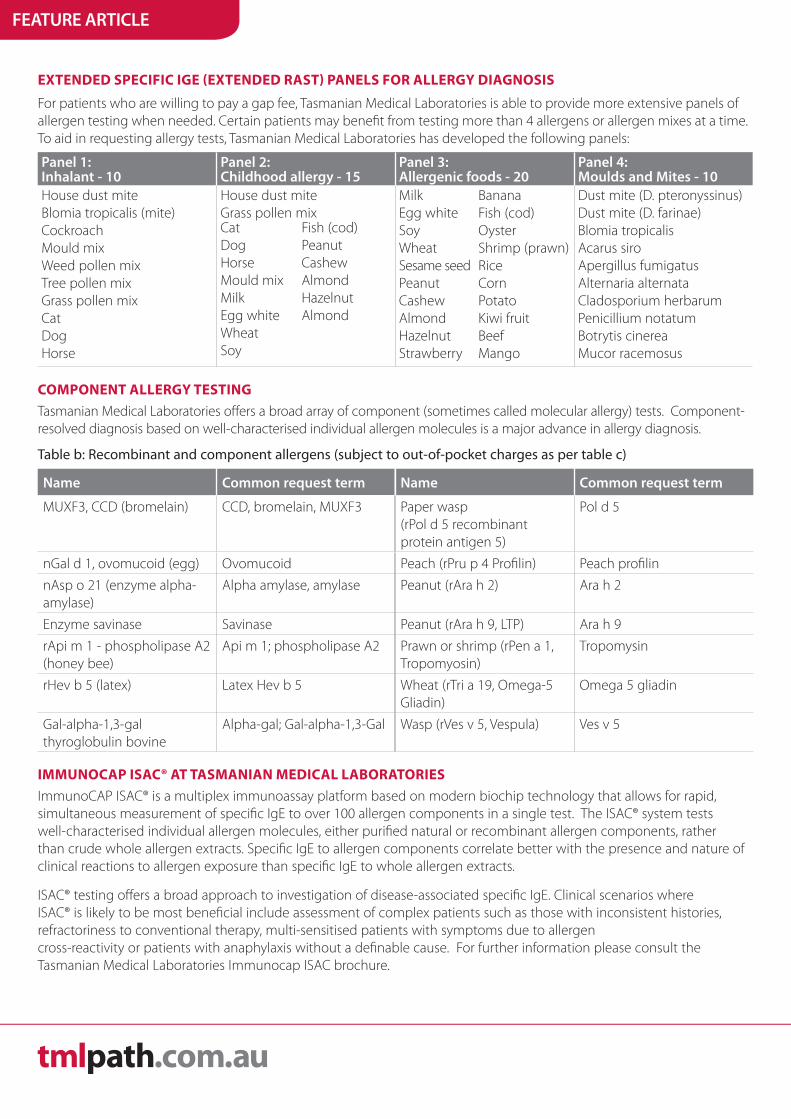
EXTENDED SPECIFIC IGE (EXTENDED RAST) PANELS FOR ALLERGY DIAGNOSIS
For patients who are willing to pay a gap fee, Tasmanian Medical Laboratories is able to provide more extensive panels of allergen testing when needed. Certain patients may benefit from testing more than 4 allergens or allergen mixes at a time. To aid in requesting allergy tests, Tasmanian Medical Laboratories has developed the following panels:
Panel 1: Inhalant - 10
Panel 2: Childhood allergy - 15
Panel 3: Allergenic foods - 20
Panel 4: Moulds and Mites - 10
House dust miteBlomia tropicalis (mite)CockroachMould mixWeed pollen mixTree pollen mixGrass pollen mixCatDogHorse
House dust mite Grass pollen mix
Milk Egg white Soy Wheat Sesame seed Peanut Cashew Almond Hazelnut Strawberry
Banana Fish (cod) Oyster Shrimp (prawn) Rice Corn Potato Kiwi fruit Beef Mango
Dust mite (D. pteronyssinus) Dust mite (D. farinae) Blomia tropicalis Acarus siro Apergillus fumigatus Alternaria alternata Cladosporium herbarum Penicillium notatum Botrytis cinerea Mucor racemosus
CatDogHorseMould mixMilkEgg whiteWheatSoy
Fish (cod)PeanutCashewAlmondHazelnutAlmond
COMPONENT ALLERGY TESTING
Tasmanian Medical Laboratories offers a broad array of component (sometimes called molecular allergy) tests. Component-resolved diagnosis based on well-characterised individual allergen molecules is a major advance in allergy diagnosis.
Table b: Recombinant and component allergens (subject to out-of-pocket charges as per table c)
Name Common request term Name Common request term
MUXF3, CCD (bromelain) CCD, bromelain, MUXF3 Paper wasp (rPol d 5 recombinant protein antigen 5)
Pol d 5
nGal d 1, ovomucoid (egg) Ovomucoid Peach (rPru p 4 Profilin) Peach profilin
nAsp o 21 (enzyme alpha-amylase)
Alpha amylase, amylase Peanut (rAra h 2) Ara h 2
Enzyme savinase Savinase Peanut (rAra h 9, LTP) Ara h 9
rApi m 1 - phospholipase A2 (honey bee)
Api m 1; phospholipase A2 Prawn or shrimp (rPen a 1, Tropomyosin)
Tropomysin
rHev b 5 (latex) Latex Hev b 5 Wheat (rTri a 19, Omega-5 Gliadin)
Omega 5 gliadin
Gal-alpha-1,3-gal thyroglobulin bovine
Alpha-gal; Gal-alpha-1,3-Gal Wasp (rVes v 5, Vespula) Ves v 5
IMMUNOCAP ISAC® AT TASMANIAN MEDICAL LABORATORIES
ImmunoCAP ISAC® is a multiplex immunoassay platform based on modern biochip technology that allows for rapid, simultaneous measurement of specific IgE to over 100 allergen components in a single test. The ISAC® system tests well-characterised individual allergen molecules, either purified natural or recombinant allergen components, rather than crude whole allergen extracts. Specific IgE to allergen components correlate better with the presence and nature of clinical reactions to allergen exposure than specific IgE to whole allergen extracts.
ISAC® testing offers a broad approach to investigation of disease-associated specific IgE. Clinical scenarios where ISAC® is likely to be most beneficial include assessment of complex patients such as those with inconsistent histories, refractoriness to conventional therapy, multi-sensitised patients with symptoms due to allergen cross-reactivity or patients with anaphylaxis without a definable cause. For further information please consult the Tasmanian Medical Laboratories Immunocap ISAC brochure.
HOW TO ORDER
Specific IgE: Request 'Specific IgE (RAST)' on a Tasmanian Medical Laboratories request form, followed by the individual allergens or mixes required for testing. In the case of the lab receiving unspecified requests for Specific IgE, allergen testing will be based on the patient’s age and any clinical information supplied. In this scenario, the standard number of allergens/mixes tested is three. A measurement of total IgE is useful in the interpretation of the significance of specific IgE and may be requested at the same time.
Extended Specific IgE (Extended RAST): Write the name of the panel from the table above e.g. ‘Extended RAST panel 1’ or ‘Extended sIgE panel 1’ in the ‘Tests Requested’ area of your Tasmanian Medical Laboratories request form.
Component Allergy Testing: Please request individual component allergens by name for specific IgE testing. For example, 'specific IgE for Ara h2' or 'RAST for Ara h2'.
ISAC Testing: Please request 'ISAC' on your Tasmanian Medical Laboratories request form. When possible, please provide brief clinical notes to assist with the interpretation of the ISAC results.
TURNAROUND TIME
RAST, Extended RAST and Component Testing: RAST testing is performed daily (Mon - Fri). Results are normally available within 72 hours from the time of collection.
ISAC Testing: Approximately 4 weeks.
COST FOR ALLERGY TESTING
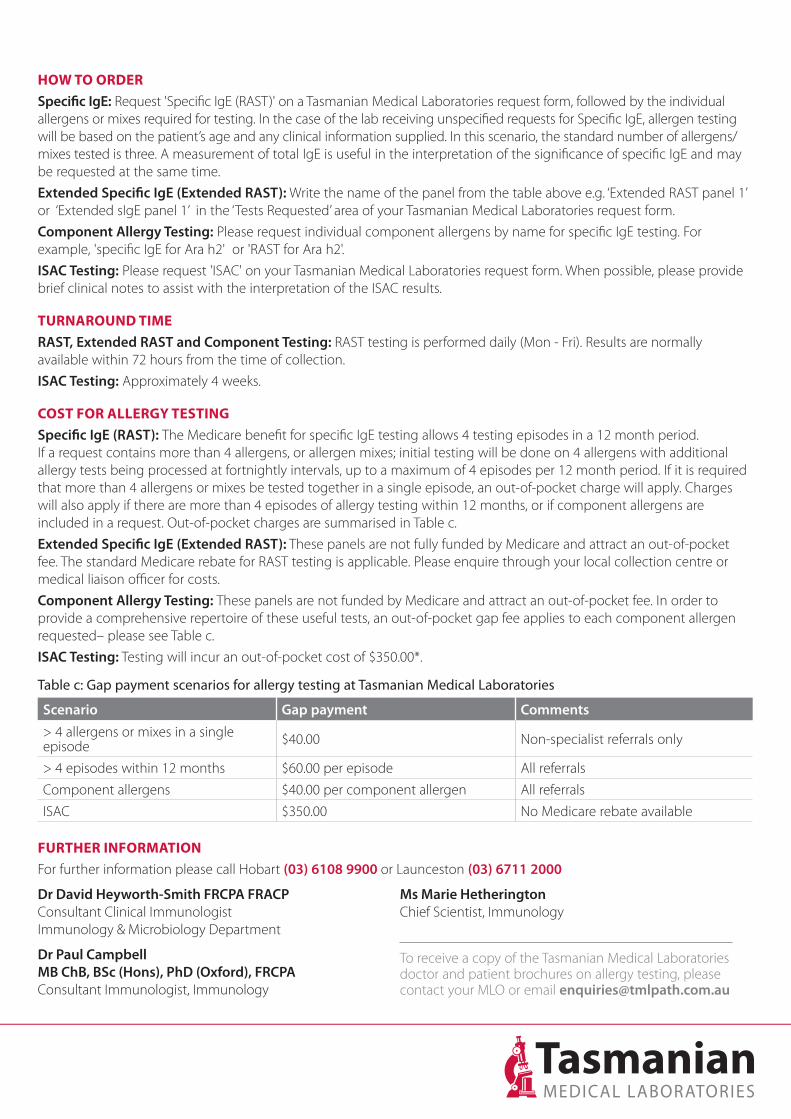
Specific IgE (RAST): The Medicare benefit for specific IgE testing allows 4 testing episodes in a 12 month period. If a request contains more than 4 allergens, or allergen mixes; initial testing will be done on 4 allergens with additional allergy tests being processed at fortnightly intervals, up to a maximum of 4 episodes per 12 month period. If it is required that more than 4 allergens or mixes be tested together in a single episode, an out-of-pocket charge will apply. Charges will also apply if there are more than 4 episodes of allergy testing within 12 months, or if component allergens are included in a request. Out-of-pocket charges are summarised in Table c.
Extended Specific IgE (Extended RAST): These panels are not fully funded by Medicare and attract an out-of-pocket fee. The standard Medicare rebate for RAST testing is applicable. Please enquire through your local collection centre or medical liaison officer for costs.
Component Allergy Testing: These panels are not funded by Medicare and attract an out-of-pocket fee. In order to provide a comprehensive repertoire of these useful tests, an out-of-pocket gap fee applies to each component allergen requested– please see Table c.
ISAC Testing: Testing will incur an out-of-pocket cost of $350.00*.
Table c: Gap payment scenarios for allergy testing at Tasmanian Medical Laboratories
Scenario Gap payment Comments
> 4 allergens or mixes in a single episode $40.00 Non-specialist referrals only
> 4 episodes within 12 months $60.00 per episode All referrals
Component allergens $40.00 per component allergen All referrals
ISAC $350.00 No Medicare rebate available
FURTHER INFORMATION
For further information please call Hobart (03) 6108 9900 or Launceston (03) 6711 2000
Dr David Heyworth-Smith FRCPA FRACP Consultant Clinical Immunologist Immunology & Microbiology Department
Dr Paul Campbell MB ChB, BSc (Hons), PhD (Oxford), FRCPAConsultant Immunologist, Immunology
Ms Marie HetheringtonChief Scientist, Immunology
To receive a copy of the Tasmanian Medical Laboratories doctor and patient brochures on allergy testing, please contact your MLO or email [email protected]
TML UPDATES
Calprotectin is a cytoplasmic protein released by activated neutrophils. Its biological function is to sequester calcium and zinc ions, and deny them to pathogens. Calprotectin released by mucosal or luminal neutrophils may be measured in faecal specimens as an index of bowel inflammation. As such, testing is useful in the assessment of patients with suspected or known inflammatory bowel diseases.
WHEN TO ORDER
Calprotectin levels correlate with the degree of bowel inflammation and it is stable for at least 3 days at room temperature. This test permits non-invasive, inexpensive and rapid assessment of bowel inflammation. An endoscopy may be required to help determine the cause of inflammation, signs, and symptoms.
A faecal specimen is required because measurement of serum calprotectin does not correlate with mucosal inflammation. Normal levels of faecal calprotectin do not exclude the
possibility of colorectal carcinoma and coeliac disease. The validity of measurement can be negatively affected by faecal heterogeneity and therapy using Aspirin, NSAIDs and PPIs.
TESTING AT TASMANIAN MEDICAL LABORATORIES
A faecal specimen is required; samples can remain stable for up to 72 hours. To order the test, request faecal or stool calprotectin level on a standard Tasmanian Medical Laboratories request form. This is a self-collect for patients; please ensure patients understand the procedure required. Our collection centres can provide faeces collection kits for your patient or clinic. Results are usually available within 3-4 working days. There is currently no Medicare rebate for this test and as such, Tasmanian Medical Laboratories will charge an out-of-pocket fee of $75*.
For more information regarding faecal calprotectin or to receive a copy of the doctor and patient brochures please contact your MLO or email [email protected]
Faecal Calprotectin: A Biomarker of Bowel Inflammation
The diagnosis of suspected coeliac disease (CD) involves serological testing for antibodies, and upper intestinal endoscopy with histological examination of a small bowel biopsy for confirmation in most cases. Endoscopy with biopsy findings confirms serological results and may exclude other causes of gastrointestinal pathology. CD is associated with the MHC alleles HLA-DQ2 and HLA-DQ8 and coeliac genotyping is also useful in certain circumstances.
ANTIBODY MEASUREMENT IN INVESTIGATION
Serological investigation of CD involves the detection of antibodies to gliadin (deamidated gliadin protein or DPG) and auto-antibodies to the antigen tissue transglutaminase. Thus, relevant assays are measurement of anti-gliadin antibodies and anti-tissue transglutaminase antibodies. In CD, measurement of antibodies of IgA isotype provides optimal sensitivity and specificity (in contrast to most autoimmune disorders in which the antibodies tested for are of IgM or IgG isotype). IgG antigliadin testing is useful in infants and in patients with IgA deficiency. Antibody measurement is useful both diagnostically and also to monitor compliance with a gluten-free diet.
GENOTYPING
As a negative HLA-DQ2/ DQ8 status means CD is unlikely, coeliac genotype assessment may be useful when there are
equivocal serological or biopsy results, or when a patient is on a gluten-free diet and does not wish to undergo a gluten challenge. However, a positive HLA-DQ2/DQ8 status is not diagnostic as these are permissive genetic factors only and approximately 25-30% of the Australian population are HLA-DQ2/DQ8 positive, whereas only 1-2% of the population have CD.
TESTING AT TASMANIAN MEDICAL LABORATORIES
Please request ‘coeliac serology’ on a standard Tasmanian Medical Laboratories request form. This generates a result for anti-tissue transglutaminase IgA antibodies and anti-gliadin IgG antibodies. Results are usually available within 3 working days. This test is bulk-billed subject to Medicare guidelines and criteria.
To request assessment of HLA DQ2/DQ8 status please request ‘coeliac genotype’. Results are usually available within 1 week. This test may be requested as a bulk-billed test, subject to Medicare guidelines and criteria.
For more information regarding laboratory investigation of coeliac disease or to receive a copy of the doctor and patient brochures please contact your MLO or email [email protected]
*Prices, where displayed, are correct at time of printing and subject to change without notice.
Blood Tests in Investigation of Coeliac Disease
247 Wellington St | Launceston | Tasmania | 7250
34 Argyle St | Hobart | Tasmania | 7000
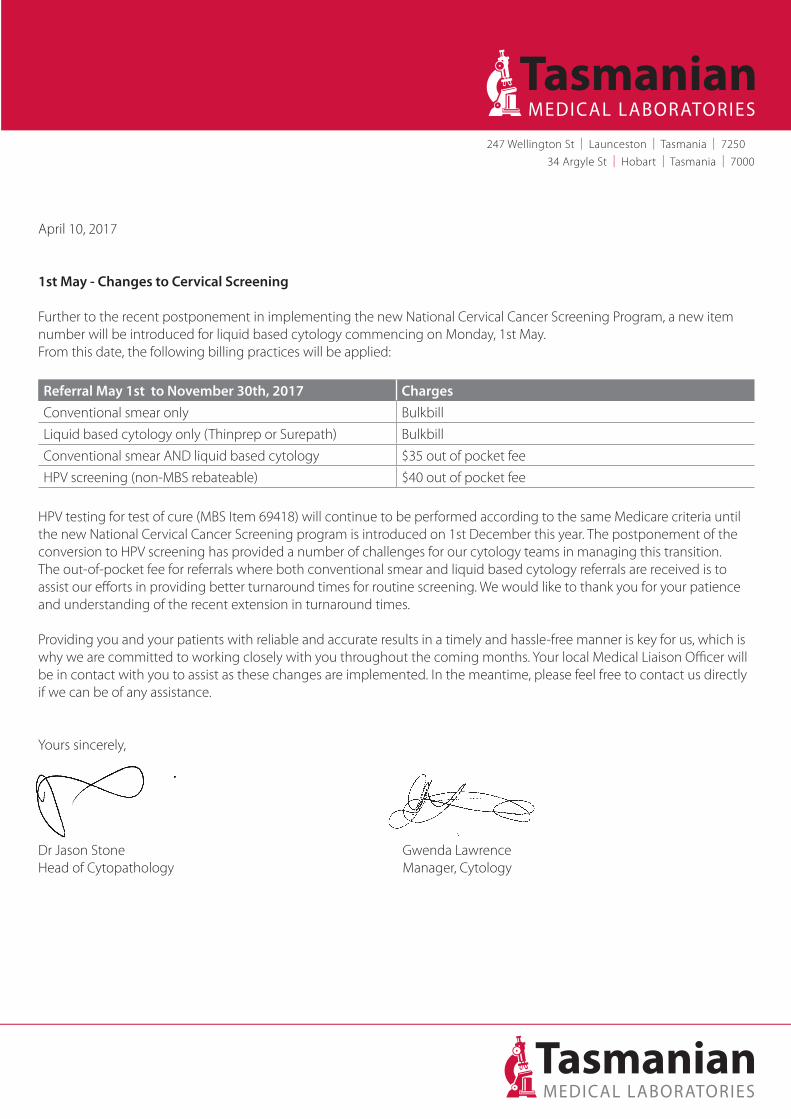
April 10, 2017
1st May - Changes to Cervical Screening
Further to the recent postponement in implementing the new National Cervical Cancer Screening Program, a new item number will be introduced for liquid based cytology commencing on Monday, 1st May. From this date, the following billing practices will be applied:
Referral May 1st to November 30th, 2017 Charges
Conventional smear only Bulkbill
Liquid based cytology only (Thinprep or Surepath) Bulkbill
Conventional smear AND liquid based cytology $35 out of pocket fee
HPV screening (non-MBS rebateable) $40 out of pocket fee
HPV testing for test of cure (MBS Item 69418) will continue to be performed according to the same Medicare criteria until the new National Cervical Cancer Screening program is introduced on 1st December this year. The postponement of the conversion to HPV screening has provided a number of challenges for our cytology teams in managing this transition. The out-of-pocket fee for referrals where both conventional smear and liquid based cytology referrals are received is to assist our efforts in providing better turnaround times for routine screening. We would like to thank you for your patience and understanding of the recent extension in turnaround times.
Providing you and your patients with reliable and accurate results in a timely and hassle-free manner is key for us, which is why we are committed to working closely with you throughout the coming months. Your local Medical Liaison Officer will be in contact with you to assist as these changes are implemented. In the meantime, please feel free to contact us directly if we can be of any assistance.
Yours sincerely,
Dr Jason Stone Gwenda LawrenceHead of Cytopathology Manager, Cytology
TML UPDATES
CLINICAL DATA
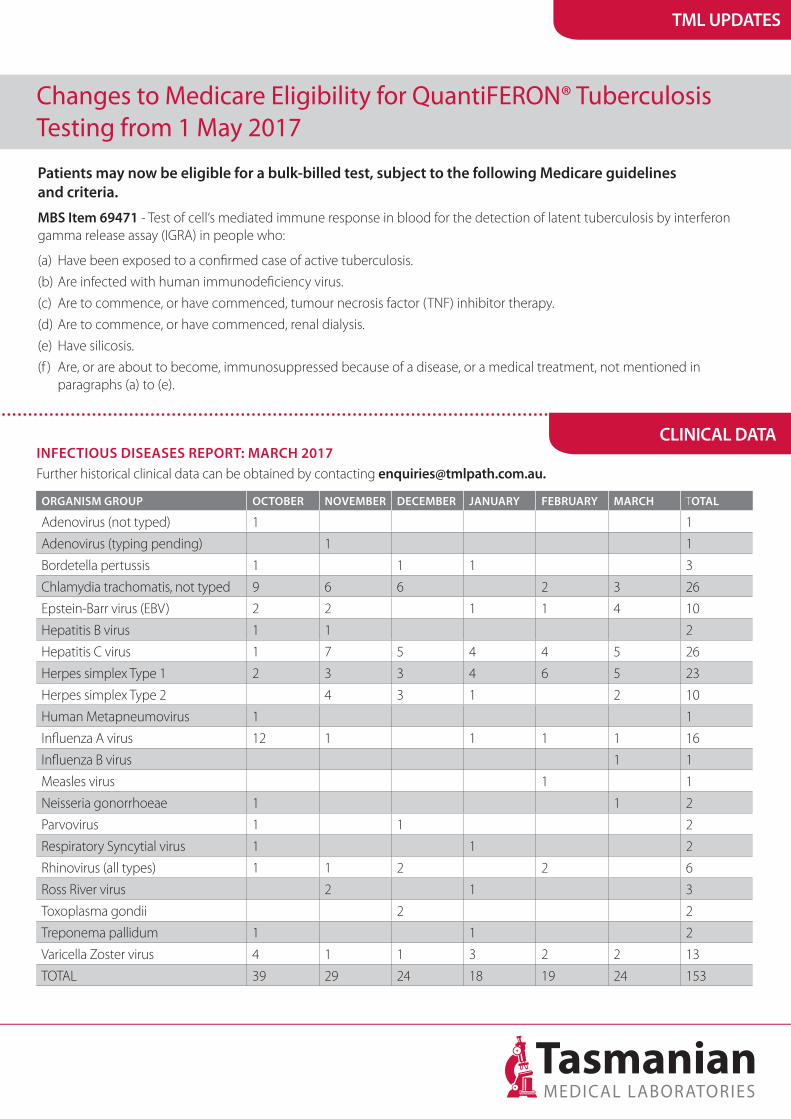
Further historical clinical data can be obtained by contacting [email protected] DISEASES REPORT: MARCH 2017
ORGANISM GROUP OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH TOTAL
Adenovirus (not typed) 1 1
Adenovirus (typing pending) 1 1
Bordetella pertussis 1 1 1 3
Chlamydia trachomatis, not typed 9 6 6 2 3 26
Epstein-Barr virus (EBV) 2 2 1 1 4 10
Hepatitis B virus 1 1 2
Hepatitis C virus 1 7 5 4 4 5 26
Herpes simplex Type 1 2 3 3 4 6 5 23
Herpes simplex Type 2 4 3 1 2 10
Human Metapneumovirus 1 1
Influenza A virus 12 1 1 1 1 16
Influenza B virus 1 1
Measles virus 1 1
Neisseria gonorrhoeae 1 1 2
Parvovirus 1 1 2
Respiratory Syncytial virus 1 1 2
Rhinovirus (all types) 1 1 2 2 6
Ross River virus 2 1 3
Toxoplasma gondii 2 2
Treponema pallidum 1 1 2
Varicella Zoster virus 4 1 1 3 2 2 13
TOTAL 39 29 24 18 19 24 153
Changes to Medicare Eligibility for QuantiFERON® Tuberculosis Testing from 1 May 2017
Patients may now be eligible for a bulk-billed test, subject to the following Medicare guidelines and criteria.
MBS Item 69471 - Test of cell‘s mediated immune response in blood for the detection of latent tuberculosis by interferon gamma release assay (IGRA) in people who:
(a) Have been exposed to a confirmed case of active tuberculosis.
(b) Are infected with human immunodeficiency virus.
(c) Are to commence, or have commenced, tumour necrosis factor (TNF) inhibitor therapy.
(d) Are to commence, or have commenced, renal dialysis.
(e) Have silicosis.
(f ) Are, or are about to become, immunosuppressed because of a disease, or a medical treatment, not mentioned in paragraphs (a) to (e).