kaiser permanente for individuals and families · welcome to your kaiser permanente for individuals...
TRANSCRIPT

Healthy togetherCare and coverage that fits your life
2018 Enrollment | Washingtonkp.org/wa/if
Kaiser Permanente for Individuals and Families

Welcome to care that fits your life
Your doctor, your choiceChoose your doctor based on what’s important to you. Go to kp.org/wa/provider-directory for details about education, specialties, languages spoken, and more. You can also change doctors at any time.
*These features are available when you get care at Kaiser Permanente facilities.
Right care, right timeGet the care you need when you need it with routine, specialty, urgent, and emergency care. If you’re ever unsure where to go, call us for 24/7 care advice by phone at 1-800-297-6877.
Many services under one roofDo more in less time. In most of our facilities, you can see your doctor, get a lab test, and pick up prescriptions — all in a single trip.
More care optionsHow you get care is up to you. Choose a phone appointment, email your doctor’s office with routine questions, or come see us in person.*
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
1 IF0001383-51-17 KPWA 2018
The right choice for your healthWelcome to your Kaiser Permanente for Individuals and Families enrollment guide. This guide will help you select the right health plan for your needs.
Important deadline for open enrollmentThe open enrollment period for 2018 coverage runs from November 1, 2017, through January 15, 2018. You can change or apply for coverage through Kaiser Permanente, or we can help you apply through Washington Healthplanfinder.
For coverage that starts on January 1, 2018, we must receive your Application for Health Coverage no later than December 15, 2017.
Enrolling during a special enrollment period
Are you getting married, having a baby, or losing your health coverage? You may also enroll or change your coverage throughout the year if you have a triggering event (or qualifying life event).
See the Enrolling During a Special Enrollment Period guide for a list of triggering events and instructions. Visit kp.org/wa/if-sep or call 1-800-358-8815
(TTY 711) to request a copy.
Visit kp.org/wa/if to compare plans, see if you qualify for federal financial assistance, calculate your rate, or apply online.
Simple steps to applyUse this guide to help you find a plan that works for you. Then, apply online or fill out a paper application.
Choose your health plan ................ 3
Find your rate ................................... 10
Learn about dental and vision coverage ......................... 19
Find a facility near you ................... 21

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
2 IF0001383-51-17 KPWA 2018
*These features are available when you get care at Kaiser Permanente facilities.
Choose how you connect to care
Online
Stay on top of your care at kp.org/wa. Once you’re registered, you can view your medical record, refill most prescriptions, schedule routine appointments, and more. Email your doctor’s office anytime with nonurgent questions.* You’ll usually get a response within 2 business days.
PhoneYou may be able to save a trip to the doctor’s office by having a phone appointment instead. We also offer care guidance and advice by phone 24/7 at 800-297-6877.
In personMost of our locations have many services under one roof, so you can see your doctor, get lab services or X-rays, and pick up a prescription — all in the same trip.
Online wellness tools
Visit kp.org/wa/health-wellness for wellness information, health calculators, fitness videos, podcasts, and recipes from world-class chefs.
Discounts for members
Enjoy discounts on products and services that can help you stay healthy — like gym memberships, massage therapy, and more. Explore your options at kp.org/wa/member-perks.
Your care, your wayGet care where, when, and how you want it. With more options to choose from, it’s easier to stay on top of your health.

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
3 IF0001383-51-17 KPWA 2018
Choose your health plan Understanding health plansWe offer a variety of plans to fit your needs and budget. All of them offer the same quality care, but the way they split the costs is different. Learn more below.
Deductible plans
Gold, Silver, Bronze, CatastrophicWith a deductible plan, your monthly rate is lower, but you’ll have to reach a deductible. This means you’ll pay the full charges for most covered services until you reach a set amount known as your deductible. Then you’ll start paying less — just a copay or coinsurance. Depending on your plan, some services, like office visits or prescriptions, may be available at a copay or coinsurance before you meet your deductible.
HSA-qualified deductible plans
Silver, BronzeHSA-qualified deductible plans are deductible plans with a special feature. With this plan, you can set up a health savings account (HSA) to pay for health costs like copays, coinsurance, and deductible payments. And you won’t pay federal taxes on the money in this account.
You can use your HSA anytime to pay for care, including some services that may not be covered by your plan, such as eyeglasses, adult dental care, or chiropractic services.* And if you have money left in your HSA at the end of the year, it will roll over for you to use the next year.
* For a complete list of services you can use your HSA to pay for, see Publication 502, Medical and Dental Expenses, at irs.gov.
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
4 IF0001383-51-17 KPWA 20184
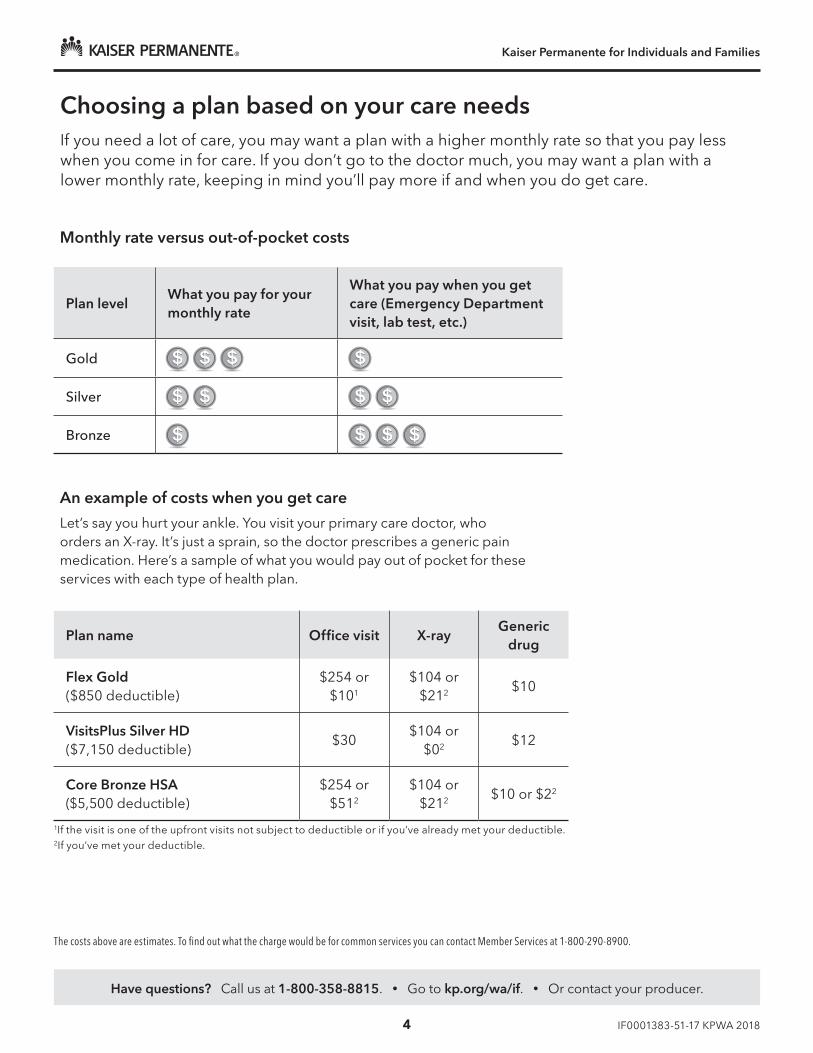
Choosing a plan based on your care needsIf you need a lot of care, you may want a plan with a higher monthly rate so that you pay less when you come in for care. If you don’t go to the doctor much, you may want a plan with a lower monthly rate, keeping in mind you’ll pay more if and when you do get care.
An example of costs when you get care
Let’s say you hurt your ankle. You visit your primary care doctor, who orders an X-ray. It’s just a sprain, so the doctor prescribes a generic pain medication. Here’s a sample of what you would pay out of pocket for these services with each type of health plan.
Monthly rate versus out-of-pocket costs
Plan levelWhat you pay for your monthly rate
What you pay when you get care (Emergency Department visit, lab test, etc.)
Gold
Silver
Bronze
Plan name Office visit X-rayGeneric
drug
Flex Gold ($850 deductible)
$254 or $101
$104 or $212 $10
VisitsPlus Silver HD ($7,150 deductible)
$30$104 or
$02 $12
Core Bronze HSA ($5,500 deductible)
$254 or $512
$104 or $212 $10 or $22
1If the visit is one of the upfront visits not subject to deductible or if you’ve already met your deductible.2If you’ve met your deductible.
The costs above are estimates. To find out what the charge would be for common services you can contact Member Services at 1-800-290-8900.

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
5 IF0001383-51-17 KPWA 2018
Flex Gold
Plan type Deductible
Features
Annual medical deductible(individual/family) $850/$1,700
Annual out-of-pocket maximum (individual/family) $5,000/$10,000
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge
Outpatient services (per visit or procedure)
Primary care office visit Deductible does not apply to first 5 office visits,* additional visits $10 after deductible
Specialty care office visit Deductible does not apply to first 5 office visits,* additional visits $30 after deductible
Most X-rays 20% after deductible
Most lab tests 20% after deductible
MRI, CT, PET 20% after deductible
Outpatient surgery 20% after deductible
Mental health visit Deductible does not apply to first 5 office visits,* additional visits $10 after deductible
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care
20% after deductible
Maternity
Routine prenatal care visits, first postpartum visit No charge
Delivery and inpatient well-baby care 20% after deductible
Emergency and urgent care
Emergency Department visit 20% after deductible
Urgent care visit Deductible does not apply to first 5 office visits,* additional visits $10 after deductible
Prescription drugs (up to a 30-day supply)
Tier 1: Preferred generic $10
Tier 2: Preferred brand $35
Tier 3: Non-preferred generic and brand 40% after deductible
Tier 4: Specialty 40% after deductible
Whole health
Healthy services: 10 chiropractic visits and 12 acupuncture visits
Deductible does not apply to first 5 office visits,* additional visits $10 after deductible
Here’s a quick look at how to use the chart
Annual deductibleYou need to pay this amount before your plan starts helping you pay for most covered services. Under this sample plan, you’d pay the full charges for covered services until you reach $850 for yourself or $1,700 for your family. Then you’d start paying copays or coinsurance.
KP Offered through Kaiser Permanente
M Offered through the Marketplace, Washington Healthplanfinder
Preventive care at no chargeMost preventive care services — including routine physical exams and mammograms — are covered at no charge. Plus, they’re not subject to the deductible.
Annual out-of-pocket maximumThis is the most you’ll pay for care during the calendar year before your plan starts paying 100% for most covered services. In this example, you’d never pay more than $5,000 for yourself and no more than $10,000 for your family for your copays, coinsurance, and deductible in a calendar year.
Covered before you reach the deductibleWith some services, you’ll only pay a copay or coinsurance, regardless of whether you’ve reached your deductible. Under this plan, the first 5 primary care visits are covered at a $10 copay — even before you meet your deductible. With our Flex plans, you get a set number of office visits covered before you reach the deductible.
CoinsuranceAfter reaching your deductible, this is a percentage of the charges that you may pay for covered services. Here, you’d pay 20% of the cost per day for your inpatient hospital care after you reach your deductible. Your plan would pay the rest for the remainder of the calendar year.
CopayThis is the set amount you pay for covered services, usually after you reach your deductible. In this example, you’d just pay a $10 copay for an urgent care visit if it’s one of the first 5 visits of the year; otherwise, you pay $10 after deductible.
KP M
Understanding the plans: benefit highlightsThe charts on the next few pages show you a sample of each plan’s benefits. Review the diagram below to help you understand how to read those charts.
*Upfront visits not subject to deductible are combined for all visits. Each service does not have its own set of upfront visits.

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Core Basics Plus
Core Bronze HSA
Bronze
Flex Bronze
Plan type Deductible HSA-qualified Deductible Deductible
Features
Annual medical deductible(individual/family) $7,350/$14,700 $5,500/$11,000 $7,150/$14,300 $7,000/$14,000
Annual out-of-pocket maximum (individual/family) $7,350/$14,700 $6,550/$13,100 $7,150/$14,300 $7,150/$14,300
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge No charge No charge No charge
Outpatient services (per visit or procedure)
Primary care office visitDeductible does not apply to first
3 office visits,* additional visits no charge after deductible
20% after deductible No charge after deductible First 3 office visits $40,* additional visits 20% after deductible
Specialty care office visit No charge after deductible 20% after deductible No charge after deductible 20% after deductible
Most X-rays No charge after deductible 20% after deductible No charge after deductible 20% after deductible
Most lab tests No charge after deductible 20% after deductible No charge after deductible 20% after deductible
MRI, CT, PET No charge after deductible 20% after deductible No charge after deductible 20% after deductible
Outpatient surgery No charge after deductible 20% after deductible No charge after deductible 20% after deductible
Mental health visitDeductible does not apply to first
3 office visits,* additional visits no charge after deductible
20% after deductible No charge after deductibleFirst 3 office visits no charge,*
additional visits 20% after deductible
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care No charge after deductible 20% after deductible No charge after deductible 20% after deductible
Maternity
Routine prenatal care visits, first postpartum visit No charge No charge No charge No charge
Delivery and inpatient well-baby care No charge after deductible 20% after deductible No charge after deductible 20% after deductible
Emergency and urgent care
Emergency Department visit No charge after deductible 20% after deductible No charge after deductible 20% after deductible
Urgent care visitDeductible does not apply to first
3 office visits,* additional visits no charge after deductible
20% after deductible No charge after deductible First 3 office visits $40,* additional visits 20% after deductible
Prescription drugs (up to a 30-day supply)
Tier 1: Preferred generic No charge after deductible 20% after deductible No charge after deductible $25
Tier 2: Preferred brand No charge after deductible 40% after deductible No charge after deductible 40% after deductible
Tier 3: Non-preferred generic and brand No charge after deductible 50% after deductible No charge after deductible 50% after deductible
Tier 4: Specialty No charge after deductible 50% after deductible No charge after deductible 50% after deductible
Whole health
Healthy services: 10 chiropractic visits and 12 acupuncture visits
Deductible does not apply to first 3 office visits,* additional visits no
charge after deductible20% after deductible No charge after deductible First 3 visits $40,* additional visits
20% after deductible
This plan summary is intended to highlight only some of the most frequently asked-about benefits and their copays, coinsurance, and deductibles. Please refer to the Coverage Agreement for more details on your plan or for specific limitations and exclusions. To request a copy of the Coverage Agreement , please call us at 1-800-290-8900 or contact your producer. For services subject to the deductible, you’ll have to pay health care expenses out of pocket until you meet your deductible. Most deductibles, copays, and coinsurance contribute to the out-of-pocket maximum.
KP Offered through Kaiser Permanente
M Offered through the Marketplace, Washington Healthplanfinder
Financial assistance options with lower copays, coinsurance, and deductibles are available for certain plans, and for Native Alaskans and American Indians on Washington Healthplanfinder.
M KP M KP M KP M
*Upfront visits not subject to deductible are combined for all visits. Each service does not have its own set of upfront visits.
All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.

Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Core Silver HSA
VisitsPlus Silver HD
Flex Silver
Flex Gold
Plan type HSA-qualified Deductible Deductible Deductible
Features
Annual medical deductible(individual/family) $3,000/$6,000 $7,150/$14,300 $1,750/$3,500 $850/$1,700
Annual out-of-pocket maximum (individual/family) $5,750/$11,500 $7,150/$14,300 $6,850/$13,700 $5,000/$10,000
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge No charge No charge No charge
Outpatient services (per visit or procedure)
Primary care office visit 10% after deductible $30 Deductible does not apply to first 4 office visits,* additional visits $20
after deductible
Deductible does not apply to first 5 office visits,* additional visits $10
after deductible
Specialty care office visit 10% after deductible $55 Deductible does not apply to first 4 office visits,* additional visits $45
after deductible
Deductible does not apply to first 5 office visits,* additional visits $30
after deductible
Most X-rays 10% after deductible No charge after deductible 30% after deductible 20% after deductible
Most lab tests 10% after deductible No charge after deductible 30% after deductible 20% after deductible
MRI, CT, PET 10% after deductible No charge after deductible 30% after deductible 20% after deductible
Outpatient surgery 10% after deductible No charge after deductible 30% after deductible 20% after deductible
Mental health visit 10% after deductible $30 Deductible does not apply to first 4 office visits,* additional visits $20
after deductible
Deductible does not apply to first 5 office visits,* additional visits $10
after deductible
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care 10% after deductible No charge after deductible 30% after deductible 20% after deductible
Maternity
Routine prenatal care visits, first postpartum visit No charge No charge No charge No charge
Delivery and inpatient well-baby care 10% after deductible No charge after deductible 30% after deductible 20% after deductible
Emergency and urgent care
Emergency Department visit 10% after deductible No charge after deductible 30% after deductible 20% after deductible
Urgent care visit 10% after deductible $30Deductible does not apply to first 4 office visits,* additional visits $20
after deductible
Deductible does not apply to first 5 office visits,* additional visits $10
after deductible
Prescription drugs (up to a 30-day supply)
Tier 1: Preferred generic 10% after deductible $12 $10 $10
Tier 2: Preferred brand 30% after deductible $55 40% after deductible $35
Tier 3: Non-preferred generic and brand 50% after deductible 50% after deductible 50% after deductible 40% after deductible
Tier 4: Specialty 50% after deductible 50% after deductible 50% after deductible 40% after deductible
Whole health
Healthy services: 10 in-network chiropractic visits and 12 acupuncture visits 10% after deductible $30
Deductible does not apply to first 4 office visits,* additional visits $20
after deductible
Deductible does not apply to first 5 office visits,* additional visits $10
after deductible
This plan summary is intended to highlight only some of the most frequently asked-about benefits and their copays, coinsurance, and deductibles. Please refer to the Coverage Agreement for more details on your plan or for specific limitations and exclusions. To request a copy of the Coverage Agreement , please call us at 1-800-290-8900 or contact your producer. For services subject to the deductible, you’ll have to pay health care expenses out of pocket until you meet your deductible. Most deductibles, copays, and coinsurance contribute to the out-of-pocket maximum.
KP Offered through Kaiser Permanente
M Offered through the Marketplace, Washington Healthplanfinder
Financial assistance options with lower copays, coinsurance, and deductibles are available for certain plans, and for Native Alaskans and American Indians on Washington Healthplanfinder.
MKP M KP M
*Upfront visits not subject to deductible are combined for all visits. Each service does not have its own set of upfront visits.
All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
M Offered through the Marketplace, Washington Healthplanfinder
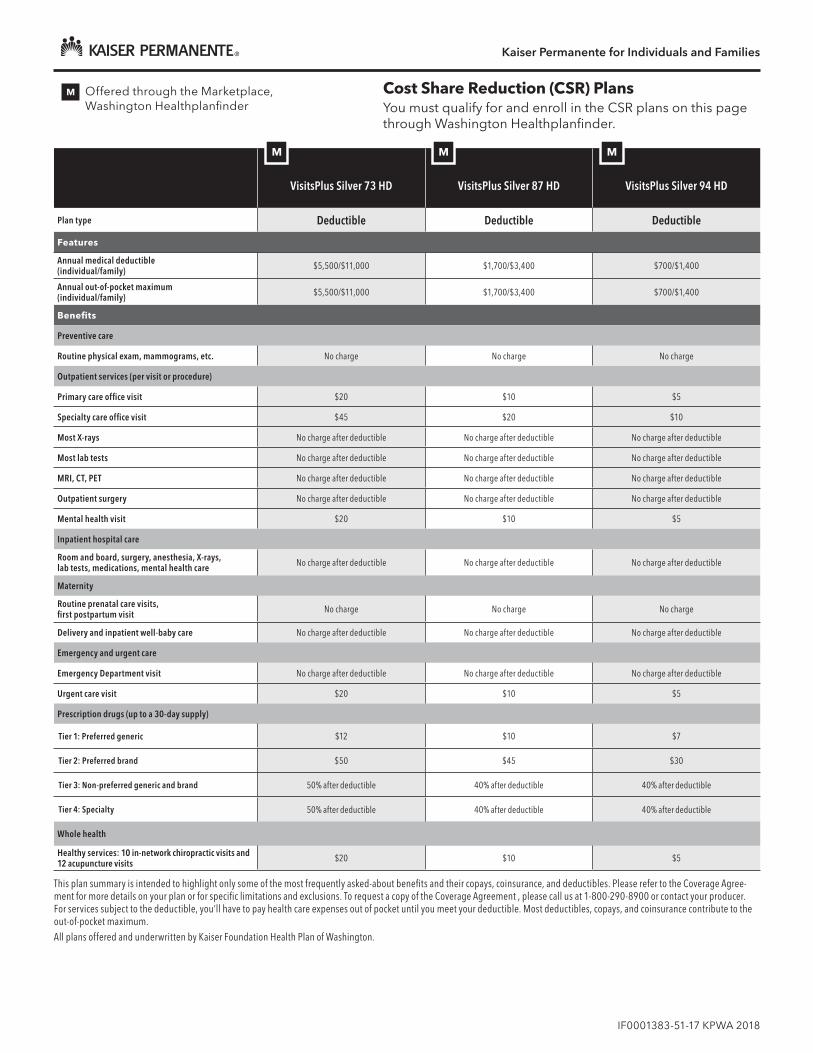
Cost Share Reduction (CSR) Plans You must qualify for and enroll in the CSR plans on this page through Washington Healthplanfinder.
VisitsPlus Silver 73 HD
VisitsPlus Silver 87 HD
VisitsPlus Silver 94 HD
Plan type Deductible Deductible Deductible
Features
Annual medical deductible(individual/family) $5,500/$11,000 $1,700/$3,400 $700/$1,400
Annual out-of-pocket maximum (individual/family) $5,500/$11,000 $1,700/$3,400 $700/$1,400
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge No charge No charge
Outpatient services (per visit or procedure)
Primary care office visit $20 $10 $5
Specialty care office visit $45 $20 $10
Most X-rays No charge after deductible No charge after deductible No charge after deductible
Most lab tests No charge after deductible No charge after deductible No charge after deductible
MRI, CT, PET No charge after deductible No charge after deductible No charge after deductible
Outpatient surgery No charge after deductible No charge after deductible No charge after deductible
Mental health visit $20 $10 $5
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care No charge after deductible No charge after deductible No charge after deductible
Maternity
Routine prenatal care visits, first postpartum visit No charge No charge No charge
Delivery and inpatient well-baby care No charge after deductible No charge after deductible No charge after deductible
Emergency and urgent care
Emergency Department visit No charge after deductible No charge after deductible No charge after deductible
Urgent care visit $20 $10 $5
Prescription drugs (up to a 30-day supply)
Tier 1: Preferred generic $12 $10 $7
Tier 2: Preferred brand $50 $45 $30
Tier 3: Non-preferred generic and brand 50% after deductible 40% after deductible 40% after deductible
Tier 4: Specialty 50% after deductible 40% after deductible 40% after deductible
Whole health
Healthy services: 10 in-network chiropractic visits and 12 acupuncture visits $20 $10 $5
MM M
This plan summary is intended to highlight only some of the most frequently asked-about benefits and their copays, coinsurance, and deductibles. Please refer to the Coverage Agree-ment for more details on your plan or for specific limitations and exclusions. To request a copy of the Coverage Agreement , please call us at 1-800-290-8900 or contact your producer. For services subject to the deductible, you’ll have to pay health care expenses out of pocket until you meet your deductible. Most deductibles, copays, and coinsurance contribute to the out-of-pocket maximum. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.

Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Flex Silver 73
Flex Silver 87
Flex Silver 94
Plan type Deductible Deductible Deductible
Features
Annual medical deductible(individual/family) $1,500/$3,000 $400/$800 $50/$100
Annual out-of-pocket maximum (individual/family) $5,700/$11,400 $2,350/$4,700 $2,350/$4,700
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge No charge No charge
Outpatient services (per visit or procedure)
Primary care office visit Deductible does not apply to first 4 office visits,* additional visits $20 after deductible
Deductible does not apply to first 4 office visits,* additional visits $10 after deductible
Deductible does not apply to first 4 office visits,* additional visits no charge after deductible
Specialty care office visit Deductible does not apply to first 4 office visits,* additional visits $45 after deductible
Deductible does not apply to first 4 office visits,* additional visits $30 after deductible
Deductible does not apply to first 4 office visits,* additional visits $5 after deductible
Most X-rays 30% after deductible 10% after deductible 5% after deductible
Most lab tests 30% after deductible 10% after deductible 5% after deductible
MRI, CT, PET 30% after deductible 10% after deductible 5% after deductible
Outpatient surgery 30% after deductible 10% after deductible 5% after deductible
Mental health visit Deductible does not apply to first 4 office visits,* additional visits $20 after deductible
Deductible does not apply to first 4 office visits,* additional visits $10 after deductible
Deductible does not apply to first 4 office visits,* additional visits no charge after deductible
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care 30% after deductible 10% after deductible 5% after deductible
Maternity
Routine prenatal care visits, first postpartum visit No charge No charge No charge
Delivery and inpatient well-baby care 30% after deductible 10% after deductible 5% after deductible
Emergency and urgent care
Emergency Department visit 30% after deductible 10% after deductible 5% after deductible
Urgent care visit Deductible does not apply to first 4 office visits,* additional visits $20 after deductible
Deductible does not apply to first 4 office visits,* additional visits $10 after deductible
Deductible does not apply to first 4 office visits,* additional visits no charge after deductible
Prescription drugs (up to a 30-day supply)
Tier 1: Preferred generic $10 $10 $7
Tier 2: Preferred brand 40% after deductible 30% after deductible 10% after deductible
Tier 3: Non-preferred generic and brand 50% after deductible 40% after deductible 40% after deductible
Tier 4: Specialty 50% after deductible 40% after deductible 40% after deductible
Whole health
Healthy services: 10 chiropractic visits and 12 acupuncture visits
Deductible does not apply to first 4 office visits,* additional visits $20 after deductible
Deductible does not apply to first 4 office visits,* additional visits $10 after deductible
Deductible does not apply to first 4 office visits,* additional visits no charge after deductible
M Offered through the Marketplace, Washington Healthplanfinder
Cost Share Reduction (CSR) Plans You must qualify for and enroll in the CSR plans on this page through Washington Healthplanfinder.
M M M
This plan summary is intended to highlight only some of the most frequently asked-about benefits and their copays, coinsurance, and deductibles. Please refer to the Coverage Agree-ment for more details on your plan or for specific limitations and exclusions. To request a copy of the Coverage Agreement , please call us at 1-800-290-8900 or contact your producer. For services subject to the deductible, you’ll have to pay health care expenses out of pocket until you meet your deductible. Most deductibles, copays, and coinsurance contribute to the out-of-pocket maximum. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.
*Upfront visits not subject to deductible are combined for all visits. Each service does not have its own set of upfront visits.

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Find your rateUse the monthly rate charts on the following pages, or apply on kp.org/wa/if to have your rate calculated automatically. Along with your monthly rate, consider what you’ll need to pay when you get care. See page 4 for more information.
What determines your rate?
Your rate is based on the following:• The plan you select • Where you live, based on your county• Your age on your start date (effective date)• If you use tobacco• If you add an optional dental rider for adult/
family members or pediatric only for family members 18 and younger
• If you qualify for federal financial assistance. Visit kp.org/wa/if or call us at 1-800-358-8815 to see if you may qualify for federal financial assistance.
Interested in a family plan?Find the rate for each family member, based on his or her age on the start date.• You• Your spouse/domestic partner• All adult children 21 through 25• Your 3 oldest children under 21
If you have more than 3 children under 21, you only have to pay for the 3 oldest. The other children under 21 will be covered at no charge.
The rates in the monthly rate charts apply to the counties below. Please check that your county is listed below.
Our service area
BentonColumbiaFranklinIslandKing
KitsapKittitasLewisMasonPierce
San JuanSkagitSnohomishSpokaneThurston
Walla WallaWhatcomWhitmanYakima

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Age on 2018 effective date
Core Basics Plus Core Bronze HSA Bronze Flex Bronze Core Silver HSA
VisitsPlus Silver HDVisitsPlus Silver 73 HDVisitsPlus Silver 87 HDVisitsPlus Silver 94 HD
Flex SilverFlex Silver 73Flex Silver 87Flex Silver 94
Flex Gold
0–14 134.57 163.34 158.19 162.48 193.04 243.39 241.68 243.09 15 146.53 177.86 172.25 176.92 210.20 265.03 263.16 264.70 16 151.10 183.41 177.63 182.44 216.76 273.30 271.37 272.96 17 155.68 188.96 183.00 187.96 223.32 281.57 279.59 281.22 18 160.60 194.94 188.79 193.91 230.38 290.48 288.43 290.12 19 165.53 200.91 194.58 199.86 237.45 299.39 297.28 299.01 20 170.63 207.11 200.58 206.02 244.77 308.62 306.44 308.23 21 175.91 213.51 206.78 212.39 252.34 318.16 315.92 317.76 22 175.91 213.51 206.78 212.39 252.34 318.16 315.92 317.76 23 175.91 213.51 206.78 212.39 252.34 318.16 315.92 317.76 24 175.91 213.51 206.78 212.39 252.34 318.16 315.92 317.76 25 176.61 214.37 207.61 213.24 253.35 319.43 317.18 319.03 26 180.13 218.64 211.75 217.48 258.39 325.80 323.50 325.39 27 184.35 223.76 216.71 222.58 264.45 333.43 331.08 333.02 28 191.21 232.09 224.77 230.86 274.29 345.84 343.40 345.41 29 196.84 238.92 231.39 237.66 282.37 356.02 353.51 355.58 30 199.65 242.34 234.70 241.06 286.40 361.11 358.57 360.66 31 203.87 247.46 239.66 246.16 292.46 368.75 366.15 368.29 32 208.10 252.58 244.62 251.25 298.52 376.38 373.73 375.91 33 210.74 255.79 247.73 254.44 302.30 381.16 378.47 380.68 34 213.55 259.20 251.03 257.84 306.34 386.25 383.52 385.76 35 214.96 260.91 252.69 259.54 308.36 388.79 386.05 388.31 36 216.36 262.62 254.34 261.24 310.37 391.34 388.58 390.85 37 217.77 264.33 256.00 262.94 312.39 393.88 391.11 393.39 38 219.18 266.04 257.65 264.63 314.41 396.43 393.63 395.93 39 221.99 269.45 260.96 268.03 318.45 401.52 398.69 401.02 40 224.81 272.87 264.27 271.43 322.49 406.61 403.74 406.10 41 229.03 277.99 269.23 276.53 328.54 414.24 411.32 413.73 42 233.08 282.90 273.99 281.41 334.35 421.56 418.59 421.04 43 238.70 289.74 280.60 288.21 342.42 431.74 428.70 431.20 44 245.74 298.28 288.88 296.70 352.52 444.47 441.34 443.91 45 254.01 308.31 298.59 306.69 364.38 459.42 456.19 458.85 46 263.86 320.27 310.17 318.58 378.51 477.24 473.88 476.64 47 274.94 333.72 323.20 331.96 394.40 497.28 493.78 496.66 48 287.61 349.09 338.09 347.25 412.57 520.19 516.53 519.54 49 300.10 364.25 352.77 362.33 430.49 542.78 538.96 542.10 50 314.17 381.33 369.31 379.32 450.67 568.23 564.23 567.52 51 328.06 398.20 385.65 396.10 470.61 593.37 589.19 592.63 52 343.37 416.78 403.64 414.58 492.56 621.05 616.67 620.27 53 358.85 435.56 421.84 433.27 514.77 649.05 644.47 648.24 54 375.56 455.85 441.48 453.45 538.74 679.27 674.48 678.42 55 392.27 476.13 461.13 473.62 562.71 709.50 704.50 708.61 56 410.39 498.12 482.43 495.50 588.70 742.27 737.04 741.34 57 428.68 520.33 503.93 517.59 614.95 775.36 769.89 774.39 58 448.21 544.03 526.88 541.16 642.96 810.67 804.96 809.66 59 457.88 555.77 538.26 552.84 656.83 828.17 822.33 827.14 60 477.41 579.47 561.21 576.42 684.84 863.49 857.40 862.41 61 494.30 599.97 581.06 596.81 709.07 894.03 887.73 892.91 62 505.38 613.42 594.09 610.19 724.97 914.07 907.63 912.93 63 519.27 630.29 610.42 626.97 744.90 939.21 932.59 938.03
64+ 527.72 640.53 620.34 637.16 757.01 954.48 947.75 953.28
Rates are effective January 1, 2018, through December 31, 2018. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.
2018 Monthly rates Please note: These rates do not include the federal financial assistance you may be eligible to receive through Washington Healthplanfinder.
Tobacco Non-User Rates
King county
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Age on 2018 effective date
Core Basics Plus Core Bronze HSA Bronze Flex Bronze Core Silver HSA
VisitsPlus Silver HDVisitsPlus Silver 73 HDVisitsPlus Silver 87 HDVisitsPlus Silver 94 HD
Flex SilverFlex Silver 73Flex Silver 87Flex Silver 94
Flex Gold
0–14 134.57 163.34 158.19 162.48 193.04 243.39 241.68 243.09 15 146.53 177.86 172.25 176.92 210.20 265.03 263.16 264.70 16 151.10 183.41 177.63 182.44 216.76 273.30 271.37 272.96 17 155.68 188.96 183.00 187.96 223.32 281.57 279.59 281.22 18 160.60 194.94 188.79 193.91 230.38 290.48 288.43 290.12 19 165.53 200.91 194.58 199.86 237.45 299.39 297.28 299.01 20 170.63 207.11 200.58 206.02 244.77 308.62 306.44 308.23 21 211.09 256.21 248.14 254.86 302.80 381.79 379.10 381.32 22 211.09 256.21 248.14 254.86 302.80 381.79 379.10 381.32 23 211.09 256.21 248.14 254.86 302.80 381.79 379.10 381.32 24 211.09 256.21 248.14 254.86 302.80 381.79 379.10 381.32 25 211.93 257.24 249.13 255.88 304.02 383.32 380.62 382.84 26 216.15 262.36 254.10 260.98 310.07 390.96 388.20 390.47 27 221.22 268.51 260.05 267.10 317.34 400.12 397.30 399.62 28 229.45 278.50 269.73 277.04 329.15 415.01 412.08 414.49 29 236.21 286.70 277.67 285.19 338.84 427.23 424.21 426.69 30 239.58 290.80 281.64 289.27 343.68 433.33 430.28 432.79 31 244.65 296.95 287.59 295.39 350.95 442.50 439.38 441.94 32 249.72 303.10 293.55 301.50 358.22 451.66 448.48 451.10 33 252.88 306.94 297.27 305.33 362.76 457.39 454.16 456.82 34 256.26 311.04 301.24 309.41 367.61 463.50 460.23 462.92 35 257.95 313.09 303.23 311.44 370.03 466.55 463.26 465.97 36 259.64 315.14 305.21 313.48 372.45 469.60 466.29 469.02 37 261.33 317.19 307.20 315.52 374.87 472.66 469.33 472.07 38 263.01 319.24 309.18 317.56 377.29 475.71 472.36 475.12 39 266.39 323.34 313.15 321.64 382.14 481.82 478.43 481.22 40 269.77 327.44 317.12 325.72 386.98 487.93 484.49 487.32 41 274.84 333.59 323.08 331.83 394.25 497.09 493.59 496.47 42 279.69 339.48 328.79 337.70 401.22 505.88 502.31 505.24 43 286.44 347.68 336.73 345.85 410.91 518.09 514.44 517.44 44 294.89 357.93 346.65 356.05 423.02 533.36 529.60 532.70 45 304.81 369.97 358.31 368.02 437.25 551.31 547.42 550.62 46 316.63 384.32 372.21 382.30 454.21 572.69 568.65 571.97 47 329.93 400.46 387.84 398.35 473.28 596.74 592.54 596.00 48 345.13 418.91 405.71 416.70 495.09 624.23 619.83 623.45 49 360.11 437.10 423.33 434.80 516.59 651.34 646.75 650.52 50 377.00 457.60 443.18 455.19 540.81 681.88 677.07 681.03 51 393.68 477.84 462.78 475.32 564.73 712.04 707.02 711.15 52 412.04 500.13 484.37 497.50 591.08 745.26 740.01 744.33 53 430.62 522.68 506.21 519.92 617.72 778.86 773.37 777.88 54 450.67 547.02 529.78 544.14 646.49 815.13 809.38 814.11 55 470.72 571.36 553.35 568.35 675.25 851.40 845.40 850.33 56 492.47 597.75 578.91 594.60 706.44 890.72 884.44 889.61 57 514.42 624.39 604.72 621.11 737.94 930.43 923.87 929.26 58 537.85 652.83 632.26 649.40 771.55 972.81 965.95 971.59 59 549.46 666.93 645.91 663.41 788.20 993.81 986.80 992.56 60 572.89 695.37 673.45 691.70 821.81 1,036.18 1,028.88 1,034.89 61 593.15 719.96 697.27 716.17 850.88 1,072.84 1,065.27 1,071.50 62 606.45 736.10 712.91 732.23 869.96 1,096.89 1,089.16 1,095.52 63 623.13 756.34 732.51 752.36 893.88 1,127.05 1,119.11 1,125.64
64+ 633.26 768.63 744.42 764.58 908.40 1,145.37 1,137.30 1,143.95
Rates are effective January 1, 2018, through December 31, 2018. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.
2018 Monthly rates Please note: These rates do not include the federal financial assistance you may be eligible to receive through Washington Healthplanfinder.
Tobacco User Rates
King county
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Age on 2018 effective date
Core Basics Plus Core Bronze HSA Bronze Flex Bronze Core Silver HSA
VisitsPlus Silver HDVisitsPlus Silver 73 HDVisitsPlus Silver 87 HDVisitsPlus Silver 94 HD
Flex SilverFlex Silver 73Flex Silver 87Flex Silver 94
Flex Gold
0–14 150.04 182.12 176.38 181.16 215.24 271.38 269.47 271.04 15 163.38 198.31 192.06 197.26 234.37 295.51 293.42 295.14 16 168.48 204.50 198.05 203.42 241.68 304.73 302.58 304.35 17 173.58 210.69 204.05 209.58 249.00 313.95 311.74 313.56 18 179.07 217.35 210.50 216.21 256.88 323.89 321.60 323.48 19 184.56 224.02 216.96 222.84 264.76 333.82 331.47 333.40 20 190.25 230.92 223.65 229.71 272.92 344.11 341.68 343.68 21 196.13 238.07 230.56 236.81 281.36 354.75 352.25 354.31 22 196.13 238.07 230.56 236.81 281.36 354.75 352.25 354.31 23 196.13 238.07 230.56 236.81 281.36 354.75 352.25 354.31 24 196.13 238.07 230.56 236.81 281.36 354.75 352.25 354.31 25 196.92 239.02 231.49 237.76 282.48 356.17 353.66 355.72 26 200.84 243.78 236.10 242.50 288.11 363.26 360.70 362.81 27 205.55 249.49 241.63 248.18 294.86 371.78 369.16 371.31 28 213.20 258.78 250.62 257.41 305.83 385.61 382.89 385.13 29 219.47 266.40 258.00 264.99 314.84 396.96 394.17 396.47 30 222.61 270.20 261.69 268.78 319.34 402.64 399.80 402.14 31 227.32 275.92 267.22 274.46 326.09 411.15 408.26 410.64 32 232.03 281.63 272.76 280.15 332.84 419.67 416.71 419.14 33 234.97 285.20 276.21 283.70 337.06 424.99 421.99 424.46 34 238.11 289.01 279.90 287.49 341.57 430.67 427.63 430.13 35 239.68 290.92 281.75 289.38 343.82 433.50 430.45 432.96 36 241.25 292.82 283.59 291.28 346.07 436.34 433.27 435.80 37 242.82 294.73 285.44 293.17 348.32 439.18 436.08 438.63 38 244.38 296.63 287.28 295.07 350.57 442.02 438.90 441.46 39 247.52 300.44 290.97 298.86 355.07 447.69 444.54 447.13 40 250.66 304.25 294.66 302.65 359.57 453.37 450.17 452.80 41 255.37 309.96 300.19 308.33 366.33 461.88 458.63 461.31 42 259.88 315.44 305.50 313.78 372.80 470.04 466.73 469.45 43 266.16 323.06 312.87 321.35 381.80 481.39 478.00 480.79 44 274.00 332.58 322.10 330.83 393.05 495.58 492.09 494.96 45 283.22 343.77 332.93 341.96 406.28 512.26 508.65 511.62 46 294.20 357.10 345.84 355.22 422.03 532.12 528.37 531.46 47 306.56 372.10 360.37 370.14 439.76 554.47 550.56 553.78 48 320.68 389.24 376.97 387.19 460.02 580.01 575.93 579.29 49 334.61 406.14 393.34 404.00 479.99 605.20 600.94 604.44 50 350.30 425.19 411.79 422.95 502.50 633.58 629.12 632.79 51 365.79 443.99 430.00 441.65 524.73 661.61 656.94 660.78 52 382.86 464.70 450.06 462.26 549.21 692.47 687.59 691.60 53 400.12 485.65 470.35 483.10 573.97 723.69 718.59 722.78 54 418.75 508.27 492.25 505.59 600.70 757.39 752.05 756.44 55 437.38 530.89 514.16 528.09 627.42 791.09 785.51 790.10 56 457.58 555.41 537.90 552.48 656.40 827.63 821.79 826.59 57 477.98 580.17 561.88 577.11 685.66 864.52 858.43 863.44 58 499.75 606.59 587.48 603.40 716.90 903.90 897.53 902.77 59 510.54 619.69 600.16 616.42 732.37 923.41 916.90 922.26 60 532.31 646.11 625.75 642.71 763.60 962.79 956.00 961.58 61 551.14 668.96 647.88 665.44 790.61 996.84 989.82 995.60 62 563.50 683.96 662.41 680.36 808.34 1,019.19 1,012.01 1,017.92 63 578.99 702.77 680.62 699.07 830.56 1,047.22 1,039.84 1,045.91
64+ 588.39 714.20 691.68 710.43 844.07 1,064.25 1,056.74 1,062.92
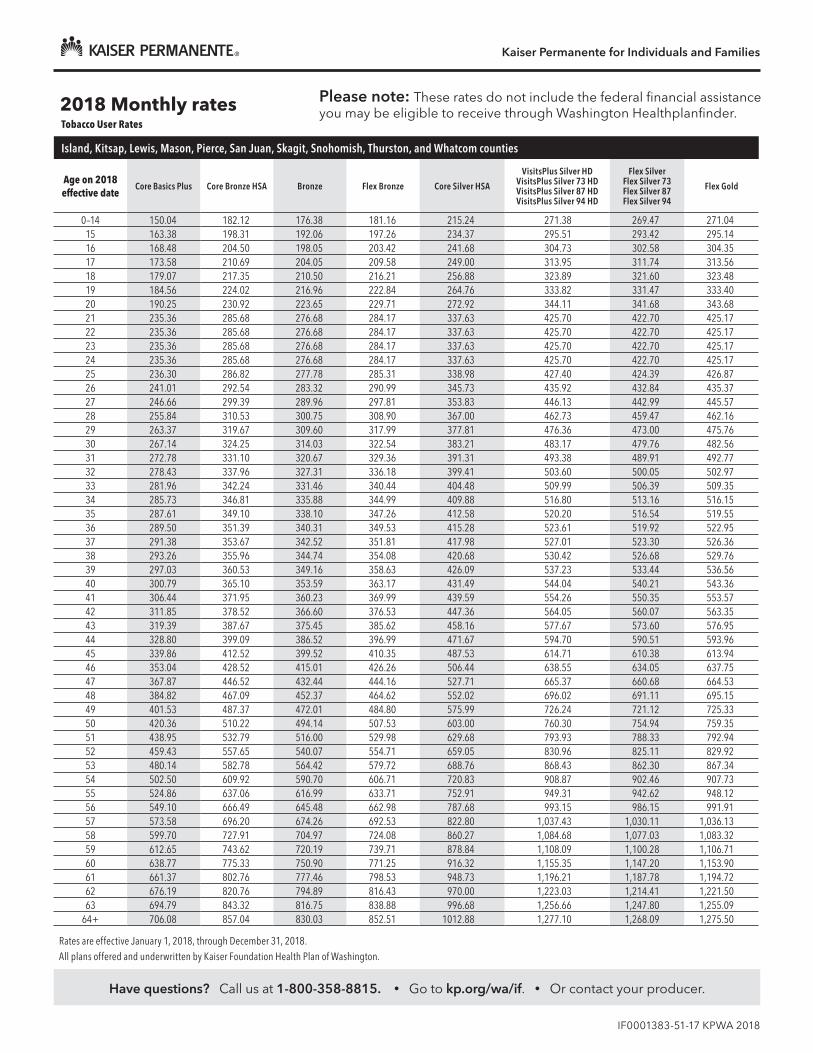
2018 Monthly rates Please note: These rates do not include the federal financial assistance you may be eligible to receive through Washington Healthplanfinder.
Tobacco Non-User Rates
Island, Kitsap, Lewis, Mason, Pierce, San Juan, Skagit, Snohomish, Thurston, and Whatcom counties
Rates are effective January 1, 2018, through December 31, 2018. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Age on 2018 effective date
Core Basics Plus Core Bronze HSA Bronze Flex Bronze Core Silver HSA
VisitsPlus Silver HDVisitsPlus Silver 73 HDVisitsPlus Silver 87 HDVisitsPlus Silver 94 HD
Flex SilverFlex Silver 73Flex Silver 87Flex Silver 94
Flex Gold
0–14 150.04 182.12 176.38 181.16 215.24 271.38 269.47 271.04 15 163.38 198.31 192.06 197.26 234.37 295.51 293.42 295.14 16 168.48 204.50 198.05 203.42 241.68 304.73 302.58 304.35 17 173.58 210.69 204.05 209.58 249.00 313.95 311.74 313.56 18 179.07 217.35 210.50 216.21 256.88 323.89 321.60 323.48 19 184.56 224.02 216.96 222.84 264.76 333.82 331.47 333.40 20 190.25 230.92 223.65 229.71 272.92 344.11 341.68 343.68 21 235.36 285.68 276.68 284.17 337.63 425.70 422.70 425.17 22 235.36 285.68 276.68 284.17 337.63 425.70 422.70 425.17 23 235.36 285.68 276.68 284.17 337.63 425.70 422.70 425.17 24 235.36 285.68 276.68 284.17 337.63 425.70 422.70 425.17 25 236.30 286.82 277.78 285.31 338.98 427.40 424.39 426.87 26 241.01 292.54 283.32 290.99 345.73 435.92 432.84 435.37 27 246.66 299.39 289.96 297.81 353.83 446.13 442.99 445.57 28 255.84 310.53 300.75 308.90 367.00 462.73 459.47 462.16 29 263.37 319.67 309.60 317.99 377.81 476.36 473.00 475.76 30 267.14 324.25 314.03 322.54 383.21 483.17 479.76 482.56 31 272.78 331.10 320.67 329.36 391.31 493.38 489.91 492.77 32 278.43 337.96 327.31 336.18 399.41 503.60 500.05 502.97 33 281.96 342.24 331.46 340.44 404.48 509.99 506.39 509.35 34 285.73 346.81 335.88 344.99 409.88 516.80 513.16 516.15 35 287.61 349.10 338.10 347.26 412.58 520.20 516.54 519.55 36 289.50 351.39 340.31 349.53 415.28 523.61 519.92 522.95 37 291.38 353.67 342.52 351.81 417.98 527.01 523.30 526.36 38 293.26 355.96 344.74 354.08 420.68 530.42 526.68 529.76 39 297.03 360.53 349.16 358.63 426.09 537.23 533.44 536.56 40 300.79 365.10 353.59 363.17 431.49 544.04 540.21 543.36 41 306.44 371.95 360.23 369.99 439.59 554.26 550.35 553.57 42 311.85 378.52 366.60 376.53 447.36 564.05 560.07 563.35 43 319.39 387.67 375.45 385.62 458.16 577.67 573.60 576.95 44 328.80 399.09 386.52 396.99 471.67 594.70 590.51 593.96 45 339.86 412.52 399.52 410.35 487.53 614.71 610.38 613.94 46 353.04 428.52 415.01 426.26 506.44 638.55 634.05 637.75 47 367.87 446.52 432.44 444.16 527.71 665.37 660.68 664.53 48 384.82 467.09 452.37 464.62 552.02 696.02 691.11 695.15 49 401.53 487.37 472.01 484.80 575.99 726.24 721.12 725.33 50 420.36 510.22 494.14 507.53 603.00 760.30 754.94 759.35 51 438.95 532.79 516.00 529.98 629.68 793.93 788.33 792.94 52 459.43 557.65 540.07 554.71 659.05 830.96 825.11 829.92 53 480.14 582.78 564.42 579.72 688.76 868.43 862.30 867.34 54 502.50 609.92 590.70 606.71 720.83 908.87 902.46 907.73 55 524.86 637.06 616.99 633.71 752.91 949.31 942.62 948.12 56 549.10 666.49 645.48 662.98 787.68 993.15 986.15 991.91 57 573.58 696.20 674.26 692.53 822.80 1,037.43 1,030.11 1,036.13 58 599.70 727.91 704.97 724.08 860.27 1,084.68 1,077.03 1,083.32 59 612.65 743.62 720.19 739.71 878.84 1,108.09 1,100.28 1,106.71 60 638.77 775.33 750.90 771.25 916.32 1,155.35 1,147.20 1,153.90 61 661.37 802.76 777.46 798.53 948.73 1,196.21 1,187.78 1,194.72 62 676.19 820.76 794.89 816.43 970.00 1,223.03 1,214.41 1,221.50 63 694.79 843.32 816.75 838.88 996.68 1,256.66 1,247.80 1,255.09
64+ 706.08 857.04 830.03 852.51 1012.88 1,277.10 1,268.09 1,275.50
2018 Monthly rates Please note: These rates do not include the federal financial assistance you may be eligible to receive through Washington Healthplanfinder.
Tobacco User Rates
Island, Kitsap, Lewis, Mason, Pierce, San Juan, Skagit, Snohomish, Thurston, and Whatcom counties
Rates are effective January 1, 2018, through December 31, 2018. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Age on 2018 effective date
Core Basics Plus Core Bronze HSA Bronze Flex Bronze Core Silver HSA
VisitsPlus Silver HDVisitsPlus Silver 73 HDVisitsPlus Silver 87 HDVisitsPlus Silver 94 HD
Flex SilverFlex Silver 73Flex Silver 87Flex Silver 94
Flex Gold
0–14 143.99 174.77 169.26 173.85 206.55 260.43 258.59 260.10 15 156.79 190.31 184.31 189.30 224.91 283.58 281.58 283.22 16 161.68 196.25 190.06 195.21 231.93 292.43 290.37 292.07 17 166.57 202.19 195.81 201.12 238.95 301.28 299.16 300.91 18 171.84 208.58 202.01 207.48 246.51 310.81 308.62 310.43 19 177.11 214.98 208.20 213.85 254.07 320.35 318.09 319.95 20 182.57 221.60 214.62 220.44 261.90 330.22 327.89 329.81 21 188.22 228.46 221.26 227.25 270.00 340.43 338.03 340.01 22 188.22 228.46 221.26 227.25 270.00 340.43 338.03 340.01 23 188.22 228.46 221.26 227.25 270.00 340.43 338.03 340.01 24 188.22 228.46 221.26 227.25 270.00 340.43 338.03 340.01 25 188.97 229.37 222.14 228.16 271.08 341.79 339.38 341.37 26 192.74 233.94 226.57 232.71 276.48 348.60 346.14 348.17 27 197.25 239.42 231.88 238.16 282.96 356.77 354.26 356.33 28 204.59 248.33 240.51 247.03 293.49 370.05 367.44 369.59 29 210.62 255.64 247.59 254.30 302.13 380.94 378.26 380.47 30 213.63 259.30 251.13 257.93 306.45 386.39 383.67 385.91 31 218.15 264.78 256.44 263.39 312.93 394.56 391.78 394.07 32 222.66 270.27 261.75 268.84 319.41 402.73 399.89 402.23 33 225.49 273.69 265.07 272.25 323.46 407.84 404.96 407.33 34 228.50 277.35 268.61 275.89 327.78 413.28 410.37 412.77 35 230.00 279.18 270.38 277.70 329.94 416.01 413.07 415.49 36 231.51 281.00 272.15 279.52 332.10 418.73 415.78 418.21 37 233.02 282.83 273.92 281.34 334.26 421.45 418.48 420.93 38 234.52 284.66 275.69 283.16 336.42 424.18 421.19 423.65 39 237.53 288.31 279.23 286.79 340.74 429.62 426.60 429.09 40 240.54 291.97 282.77 290.43 345.06 435.07 432.00 434.53 41 245.06 297.45 288.08 295.89 351.54 443.24 440.12 442.69 42 249.39 302.71 293.17 301.11 357.75 451.07 447.89 450.51 43 255.41 310.02 300.25 308.38 366.39 461.97 458.71 461.39 44 262.94 319.16 309.10 317.47 377.19 475.58 472.23 474.99 45 271.79 329.89 319.50 328.16 389.88 491.58 488.12 490.97 46 282.33 342.69 331.89 340.88 405.00 510.65 507.05 510.01 47 294.19 357.08 345.83 355.20 422.01 532.09 528.34 531.43 48 307.74 373.53 361.76 371.56 441.45 556.61 552.68 555.91 49 321.10 389.75 377.47 387.70 460.62 580.78 576.68 580.05 50 336.16 408.03 395.17 405.88 482.22 608.01 603.72 607.25 51 351.03 426.07 412.65 423.83 503.55 634.90 630.43 634.11 52 367.40 445.95 431.90 443.60 527.04 664.52 659.84 663.69 53 383.97 466.05 451.37 463.60 550.80 694.48 689.58 693.61 54 401.85 487.76 472.39 485.19 576.45 726.82 721.70 725.91 55 419.73 509.46 493.41 506.78 602.10 759.16 753.81 758.21 56 439.12 532.99 516.19 530.18 629.91 794.23 788.63 793.23 57 458.69 556.75 539.21 553.82 657.99 829.63 823.78 828.59 58 479.58 582.11 563.77 579.04 687.96 867.42 861.31 866.34 59 489.93 594.68 575.93 591.54 702.81 886.14 879.90 885.04 60 510.83 620.03 600.49 616.77 732.78 923.93 917.42 922.78 61 528.90 641.97 621.73 638.58 758.70 956.61 949.87 955.42 62 540.75 656.36 635.67 652.90 775.71 978.06 971.17 976.84 63 555.62 674.41 653.15 670.85 797.04 1,004.95 997.87 1,003.70
64+ 564.66 685.37 663.77 681.75 810.00 1,021.29 1,014.09 1,020.02
Rates are effective January 1, 2018, through December 31, 2018. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.
2018 Monthly rates Please note: These rates do not include the federal financial assistance you may be eligible to receive through Washington Healthplanfinder.
Tobacco Non-User Rates
Spokane county

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Age on 2018 effective date
Core Basics Plus Core Bronze HSA Bronze Flex Bronze Core Silver HSA
VisitsPlus Silver HDVisitsPlus Silver 73 HDVisitsPlus Silver 87 HDVisitsPlus Silver 94 HD
Flex SilverFlex Silver 73Flex Silver 87Flex Silver 94
Flex Gold
0–14 143.99 174.77 169.26 173.85 206.55 260.43 258.59 260.10 15 156.79 190.31 184.31 189.30 224.91 283.58 281.58 283.22 16 161.68 196.25 190.06 195.21 231.93 292.43 290.37 292.07 17 166.57 202.19 195.81 201.12 238.95 301.28 299.16 300.91 18 171.84 208.58 202.01 207.48 246.51 310.81 308.62 310.43 19 177.11 214.98 208.20 213.85 254.07 320.35 318.09 319.95 20 182.57 221.60 214.62 220.44 261.90 330.22 327.89 329.81 21 225.86 274.15 265.51 272.71 324.00 408.52 405.64 408.01 22 225.86 274.15 265.51 272.71 324.00 408.52 405.64 408.01 23 225.86 274.15 265.51 272.71 324.00 408.52 405.64 408.01 24 225.86 274.15 265.51 272.71 324.00 408.52 405.64 408.01 25 226.77 275.25 266.57 273.80 325.30 410.15 407.26 409.64 26 231.28 280.73 271.88 279.25 331.78 418.32 415.37 417.80 27 236.70 287.31 278.25 285.80 339.55 428.13 425.11 427.59 28 245.51 298.00 288.61 296.43 352.19 444.06 440.93 443.50 29 252.74 306.77 297.11 305.16 362.56 457.13 453.91 456.56 30 256.35 311.16 301.35 309.52 367.74 463.67 460.40 463.09 31 261.78 317.74 307.73 316.07 375.52 473.47 470.13 472.88 32 267.20 324.32 314.10 322.61 383.29 483.28 479.87 482.67 33 270.58 328.43 318.08 326.70 388.15 489.40 485.95 488.79 34 274.20 332.82 322.33 331.06 393.34 495.94 492.44 495.32 35 276.00 335.01 324.45 333.25 395.93 499.21 495.69 498.58 36 277.81 337.20 326.58 335.43 398.52 502.48 498.94 501.85 37 279.62 339.40 328.70 337.61 401.11 505.75 502.18 505.11 38 281.43 341.59 330.82 339.79 403.71 509.01 505.43 508.38 39 285.04 345.98 335.07 344.15 408.89 515.55 511.92 514.90 40 288.65 350.36 339.32 348.52 414.07 522.09 518.41 521.43 41 294.07 356.94 345.69 355.06 421.85 531.89 528.14 531.23 42 299.27 363.25 351.80 361.33 429.30 541.29 537.47 540.61 43 306.50 372.02 360.30 370.06 439.67 554.36 550.45 553.67 44 315.53 382.99 370.92 380.97 452.63 570.70 566.68 569.99 45 326.15 395.87 383.40 393.79 467.86 589.90 585.74 589.16 46 338.79 411.22 398.26 409.06 486.00 612.78 608.46 612.01 47 353.02 428.50 414.99 426.24 506.41 638.51 634.01 637.72 48 369.29 448.23 434.11 445.87 529.74 667.93 663.22 667.09 49 385.32 467.70 452.96 465.24 552.75 696.93 692.02 696.06 50 403.39 489.63 474.20 487.05 578.67 729.61 724.47 728.70 51 421.23 511.29 495.18 508.60 604.26 761.89 756.52 760.93 52 440.88 535.14 518.27 532.32 632.45 797.43 791.81 796.43 53 460.76 559.26 541.64 556.32 660.96 833.38 827.50 832.33 54 482.22 585.31 566.86 582.23 691.74 872.19 866.04 871.10 55 503.67 611.35 592.09 608.13 722.52 911.00 904.57 909.86 56 526.94 639.59 619.43 636.22 755.89 953.07 946.35 951.88 57 550.43 668.10 647.05 664.58 789.59 995.56 988.54 994.31 58 575.50 698.53 676.52 694.85 825.55 1,040.90 1,033.57 1,039.60 59 587.92 713.61 691.12 709.85 843.38 1,063.37 1,055.88 1,062.04 60 612.99 744.04 720.59 740.12 879.34 1,108.72 1,100.90 1,107.33 61 634.68 770.36 746.08 766.30 910.44 1,147.94 1,139.84 1,146.50 62 648.90 787.63 762.81 783.48 930.86 1,173.67 1,165.40 1,172.20 63 666.75 809.29 783.78 805.03 956.45 1,205.95 1,197.44 1,204.44
64+ 677.58 822.45 796.53 818.12 972.00 1,225.55 1,216.91 1,224.02
Rates are effective January 1, 2018, through December 31, 2018. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.
2018 Monthly rates Please note: These rates do not include the federal financial assistance you may be eligible to receive through Washington Healthplanfinder.
Tobacco User Rates
Spokane county

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Age on 2018 effective date
Core Basics Plus Core Bronze HSA Bronze Flex Bronze Core Silver HSA
VisitsPlus Silver HDVisitsPlus Silver 73 HDVisitsPlus Silver 87 HDVisitsPlus Silver 94 HD
Flex SilverFlex Silver 73Flex Silver 87Flex Silver 94
Flex Gold
0–14 148.70 180.49 174.80 179.54 213.31 268.95 267.05 268.61 15 161.92 196.53 190.34 195.50 232.27 292.86 290.79 292.49 16 166.97 202.66 196.28 201.60 239.52 302.00 299.87 301.62 17 172.02 208.80 202.22 207.70 246.77 311.14 308.94 310.75 18 177.47 215.40 208.62 214.27 254.57 320.98 318.72 320.58 19 182.91 222.01 215.01 220.84 262.38 330.82 328.49 330.41 20 188.54 228.85 221.64 227.65 270.47 341.02 338.62 340.59 21 194.38 235.93 228.50 234.69 278.83 351.57 349.09 351.13 22 194.38 235.93 228.50 234.69 278.83 351.57 349.09 351.13 23 194.38 235.93 228.50 234.69 278.83 351.57 349.09 351.13 24 194.38 235.93 228.50 234.69 278.83 351.57 349.09 351.13 25 195.15 236.87 229.41 235.63 279.95 352.97 350.49 352.53 26 199.04 241.59 233.98 240.32 285.52 360.00 357.47 359.55 27 203.71 247.26 239.46 245.95 292.22 368.44 365.85 367.98 28 211.29 256.46 248.37 255.11 303.09 382.15 379.46 381.68 29 217.51 264.01 255.69 262.62 312.01 393.40 390.63 392.91 30 220.62 267.78 259.34 266.37 316.48 399.03 396.22 398.53 31 225.28 273.44 264.83 272.00 323.17 407.47 404.59 406.96 32 229.95 279.11 270.31 277.64 329.86 415.90 412.97 415.38 33 232.86 282.64 273.74 281.16 334.04 421.18 418.21 420.65 34 235.97 286.42 277.39 284.91 338.50 426.80 423.79 426.27 35 237.53 288.31 279.22 286.79 340.73 429.62 426.59 429.08 36 239.08 290.19 281.05 288.67 342.96 432.43 429.38 431.89 37 240.64 292.08 282.88 290.54 345.19 435.24 432.17 434.70 38 242.19 293.97 284.71 292.42 347.43 438.05 434.96 437.50 39 245.30 297.74 288.36 296.18 351.89 443.68 440.55 443.12 40 248.41 301.52 292.02 299.93 356.35 449.30 446.14 448.74 41 253.08 307.18 297.50 305.56 363.04 457.74 454.51 457.17 42 257.55 312.61 302.76 310.96 369.45 465.83 462.54 465.24 43 263.77 320.16 310.07 318.47 378.38 477.08 473.71 476.48 44 271.54 329.60 319.21 327.86 389.53 491.14 487.68 490.53 45 280.68 340.68 329.95 338.89 402.63 507.66 504.08 507.03 46 291.56 353.90 342.74 352.03 418.25 527.35 523.63 526.69 47 303.81 368.76 357.14 366.82 435.82 549.50 545.63 548.81 48 317.80 385.75 373.59 383.71 455.89 574.81 570.76 574.09 49 331.61 402.50 389.81 400.38 475.69 599.77 595.55 599.02 50 347.16 421.37 408.09 419.15 498.00 627.90 623.47 627.11 51 362.51 440.01 426.14 437.69 520.02 655.67 651.05 654.85 52 379.42 460.54 446.02 458.11 544.28 686.26 681.42 685.40 53 396.53 481.30 466.13 478.76 568.82 717.20 712.14 716.30 54 414.99 503.71 487.84 501.06 595.31 750.60 745.30 749.66 55 433.46 526.13 509.54 523.35 621.80 783.99 778.47 783.01 56 453.48 550.43 533.08 547.53 650.52 820.21 814.42 819.18 57 473.69 574.96 556.84 571.93 679.52 856.77 850.73 855.70 58 495.27 601.15 582.21 597.98 710.47 895.79 889.48 894.67 59 505.96 614.13 594.77 610.89 725.80 915.13 908.68 913.99 60 527.54 640.32 620.14 636.94 756.75 954.15 947.43 952.96 61 546.20 662.97 642.07 659.47 783.52 987.90 980.94 986.67 62 558.44 677.83 656.47 674.26 801.09 1,010.05 1,002.93 1,008.79 63 573.80 696.47 674.52 692.80 823.11 1,037.83 1,030.51 1,036.53
64+ 583.13 707.79 685.49 704.06 836.49 1,054.70 1,047.27 1,053.38
Rates are effective January 1, 2018, through December 31, 2018. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.
2018 Monthly rates Please note: These rates do not include the federal financial assistance you may be eligible to receive through Washington Healthplanfinder.
Tobacco Non-User Rates
Benton, Columbia, Franklin, Kittitas, Walla Walla, Whitman, and Yakima counties

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
Age on 2018 effective date
Core Basics Plus Core Bronze HSA Bronze Flex Bronze Core Silver HSA
VisitsPlus Silver HDVisitsPlus Silver 73 HDVisitsPlus Silver 87 HDVisitsPlus Silver 94 HD
Flex SilverFlex Silver 73Flex Silver 87Flex Silver 94
Flex Gold
0–14 148.70 180.49 174.80 179.54 213.31 268.95 267.05 268.61 15 161.92 196.53 190.34 195.50 232.27 292.86 290.79 292.49 16 166.97 202.66 196.28 201.60 239.52 302.00 299.87 301.62 17 172.02 208.80 202.22 207.70 246.77 311.14 308.94 310.75 18 177.47 215.40 208.62 214.27 254.57 320.98 318.72 320.58 19 182.91 222.01 215.01 220.84 262.38 330.82 328.49 330.41 20 188.54 228.85 221.64 227.65 270.47 341.02 338.62 340.59 21 233.25 283.12 274.19 281.63 334.60 421.88 418.91 421.35 22 233.25 283.12 274.19 281.63 334.60 421.88 418.91 421.35 23 233.25 283.12 274.19 281.63 334.60 421.88 418.91 421.35 24 233.25 283.12 274.19 281.63 334.60 421.88 418.91 421.35 25 234.18 284.25 275.29 282.75 335.94 423.57 420.58 423.04 26 238.85 289.91 280.78 288.38 342.63 432.01 428.96 431.47 27 244.45 296.71 287.36 295.14 350.66 442.13 439.01 441.58 28 253.54 307.75 298.05 306.13 363.71 458.58 455.35 458.01 29 261.01 316.81 306.82 315.14 374.42 472.08 468.76 471.49 30 264.74 321.34 311.21 319.64 379.77 478.83 475.46 478.24 31 270.34 328.13 317.79 326.40 387.80 488.96 485.51 488.35 32 275.94 334.93 324.37 333.16 395.83 499.08 495.57 498.46 33 279.43 339.17 328.48 337.39 400.85 505.41 501.85 504.78 34 283.17 343.70 332.87 341.89 406.20 512.16 508.55 511.52 35 285.03 345.97 335.07 344.15 408.88 515.54 511.90 514.89 36 286.90 348.23 337.26 346.40 411.56 518.91 515.26 518.26 37 288.76 350.50 339.45 348.65 414.23 522.29 518.61 521.64 38 290.63 352.76 341.65 350.91 416.91 525.66 521.96 525.01 39 294.36 357.29 346.03 355.41 422.26 532.41 528.66 531.75 40 298.09 361.82 350.42 359.92 427.62 539.16 535.36 538.49 41 303.69 368.62 357.00 366.68 435.65 549.29 545.42 548.60 42 309.06 375.13 363.31 373.15 443.34 558.99 555.05 558.29 43 316.52 384.19 372.08 382.17 454.05 572.49 568.46 571.78 44 325.85 395.51 383.05 393.43 467.44 589.37 585.21 588.63 45 336.81 408.82 395.94 406.67 483.16 609.20 604.90 608.43 46 349.88 424.68 411.29 422.44 501.90 632.82 628.36 632.03 47 364.57 442.51 428.57 440.18 522.98 659.40 654.75 658.57 48 381.37 462.90 448.31 460.46 547.07 689.77 684.91 688.91 49 397.93 483.00 467.78 480.45 570.83 719.73 714.65 718.83 50 416.59 505.65 489.71 502.98 597.59 753.48 748.17 752.54 51 435.01 528.01 511.37 525.23 624.03 786.81 781.26 785.82 52 455.31 552.64 535.23 549.73 653.14 823.51 817.71 822.48 53 475.83 577.56 559.36 574.52 682.58 860.64 854.57 859.56 54 497.99 604.45 585.41 601.27 714.37 900.72 894.37 899.59 55 520.15 631.35 611.45 628.02 746.16 940.79 934.16 939.62 56 544.17 660.51 639.70 657.03 780.62 984.25 977.31 983.02 57 568.43 689.96 668.21 686.32 815.42 1,028.12 1,020.88 1,026.84 58 594.32 721.38 698.65 717.58 852.56 1,074.95 1,067.37 1,073.61 59 607.15 736.95 713.73 733.07 870.96 1,098.16 1,090.41 1,096.78 60 633.04 768.38 744.16 764.33 908.10 1,144.98 1,136.91 1,143.55 61 655.44 795.56 770.49 791.37 940.22 1,185.48 1,177.13 1,184.00 62 670.13 813.39 787.76 809.11 961.30 1,212.06 1,203.52 1,210.55 63 688.56 835.76 809.42 831.36 987.74 1,245.39 1,236.61 1,243.83
64+ 699.75 849.35 822.57 844.88 1,003.80 1,265.64 1,256.72 1,264.05
Rates are effective January 1, 2018, through December 31, 2018. All plans offered and underwritten by Kaiser Foundation Health Plan of Washington.
2018 Monthly rates Please note: These rates do not include the federal financial assistance you may be eligible to receive through Washington Healthplanfinder.
Tobacco User Rates
Benton, Columbia, Franklin, Kittitas, Walla Walla, Whitman, and Yakima counties

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
19 IF0001383-51-17 KPWA 2018
A reason to smile
Oral health is an important part of your overall health. When you select a Kaiser Permanente medical plan, you can choose to add this vital dental coverage — for yourself, for your children, or for your entire family.
These Delta Dental plans give you the freedom to see any dentist, and you receive better benefits when you see a Delta Dental participating dentist.
Choosing a dentist
You may choose a dentist from two networks: Delta Dental PPO or Delta Dental Premier. To find a participating, in-network dentist in your area, visit deltadentalwa.com and use the Find a Dentist tool.
Delta Dental network dentists provide treatments at discounted rates and file all claims paperwork for you. Delta Dental will pay its portion and you’re only responsible for your stated deductibles, coinsurance, and any amounts in excess of the plan maximums.
If you choose a non-participating (out-of-network) dentist, you are responsible for having the dentist complete your claim forms and for ensuring the claims are submitted to Delta Dental. Claim payments to out-of-network dentists are based
on actual charges or Delta Dental’s maximum allowable fees for non-participating dentists, whichever is less. You’re then responsible for any balance remaining after Delta Dental pays.
For questions or to locate a participating provider, please visit deltadentalwa.com or call Delta Dental at 1-800-554-1907.
Choosing a plan
We work with Delta Dental of Washington to offer you dental coverage when paired with one of our 2018 medical plans.
A federal mandate requires dental coverage for anyone 18 and younger. You can buy this coverage separately or with a family dental plan.
Adult/family planThe optional adult/family plan includes dental coverage for everyone covered on the medical plan.
• This plan is available for adults or families who purchase their medical plan directly from Kaiser Permanente.
• Adults or families who purchase their medical plan through Washington Healthplanfinder can also purchase their family dental there.
Learn about dental and vision coveragePediatric-only planThe pediatric-only plan includes dental coverage for those 18 and younger only.
• This plan is available if you purchase your medical plan directly from Kaiser Permanente.
• If you purchase your medical plan through Washington Healthplanfinder you will be required to purchase pediatric dental for those 18 and younger through Washington Healthplanfinder.
Vision essentials
We offer comprehensive eye care services to help keep your world in focus. Plus, when you’re a Kaiser Foundation Health Plan of Washington member, your eye health information becomes part of your overall medical record, giving your care team a complete picture of your health.1
All of our medical plans have adult vision exams included subject to applicable cost shares. All plans include medically necessary eye exams, pediatric vision exams for members 18 and younger, as well as glasses or contact lenses for children at no cost.2 For more information, including our eye care locations, visit wa-eyecare.kaiserpermanente.org.
1This is available when you get care at Kaiser Permanente facilities.2Vision hardware must be prescribed and purchased at a Kaiser Permanente Eye Care location or contracted provider.
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
20 IF0001383-51-17 KPWA 2018
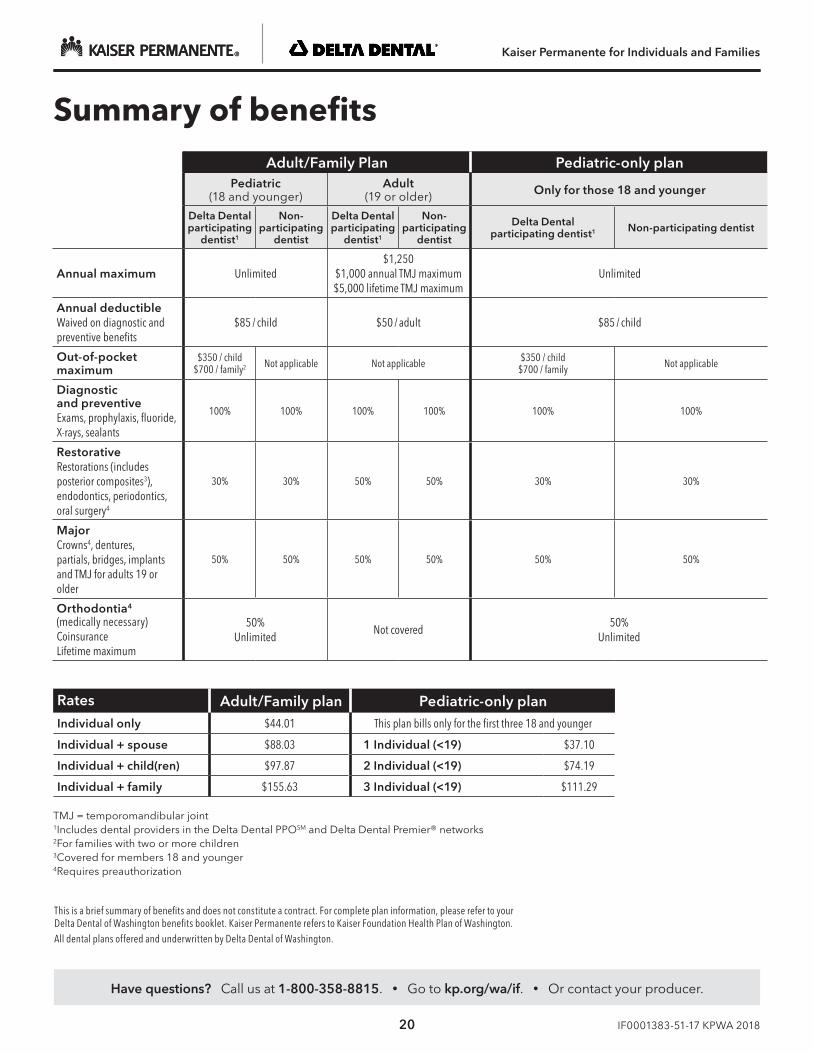
This is a brief summary of benefits and does not constitute a contract. For complete plan information, please refer to your Delta Dental of Washington benefits booklet. Kaiser Permanente refers to Kaiser Foundation Health Plan of Washington.All dental plans offered and underwritten by Delta Dental of Washington.
TMJ = temporomandibular joint1Includes dental providers in the Delta Dental PPOSM and Delta Dental Premier® networks 2For families with two or more children3Covered for members 18 and younger4Requires preauthorization
Summary of benefitsAdult/Family Plan Pediatric-only plan
Pediatric (18 and younger)
Adult (19 or older) Only for those 18 and younger
Delta Dental participating
dentist1
Non-participating
dentist
Delta Dental participating
dentist1
Non-participating
dentist
Delta Dental participating dentist1 Non-participating dentist
Annual maximum Unlimited$1,250
$1,000 annual TMJ maximum$5,000 lifetime TMJ maximum
Unlimited
Annual deductibleWaived on diagnostic and preventive benefits
$85 / child $50 / adult $85 / child
Out-of-pocketmaximum
$350 / child$700 / family2 Not applicable Not applicable $350 / child
$700 / family Not applicable
Diagnostic and preventiveExams, prophylaxis, fluoride, X-rays, sealants
100% 100% 100% 100% 100% 100%
RestorativeRestorations (includes posterior composites3), endodontics, periodontics, oral surgery4
30% 30% 50% 50% 30% 30%
MajorCrowns4, dentures, partials, bridges, implants and TMJ for adults 19 or older
50% 50% 50% 50% 50% 50%
Orthodontia4
(medically necessary)CoinsuranceLifetime maximum
50%Unlimited
Not covered50%
Unlimited
Rates Adult/Family plan Pediatric-only planIndividual only $44.01 This plan bills only for the first three 18 and younger
Individual + spouse $88.03 1 Individual (<19) $37.10
Individual + child(ren) $97.87 2 Individual (<19) $74.19
Individual + family $155.63 3 Individual (<19) $111.29
Kaiser Permanente for Individuals and Families
21 IF0001383-51-17 KPWA 2018
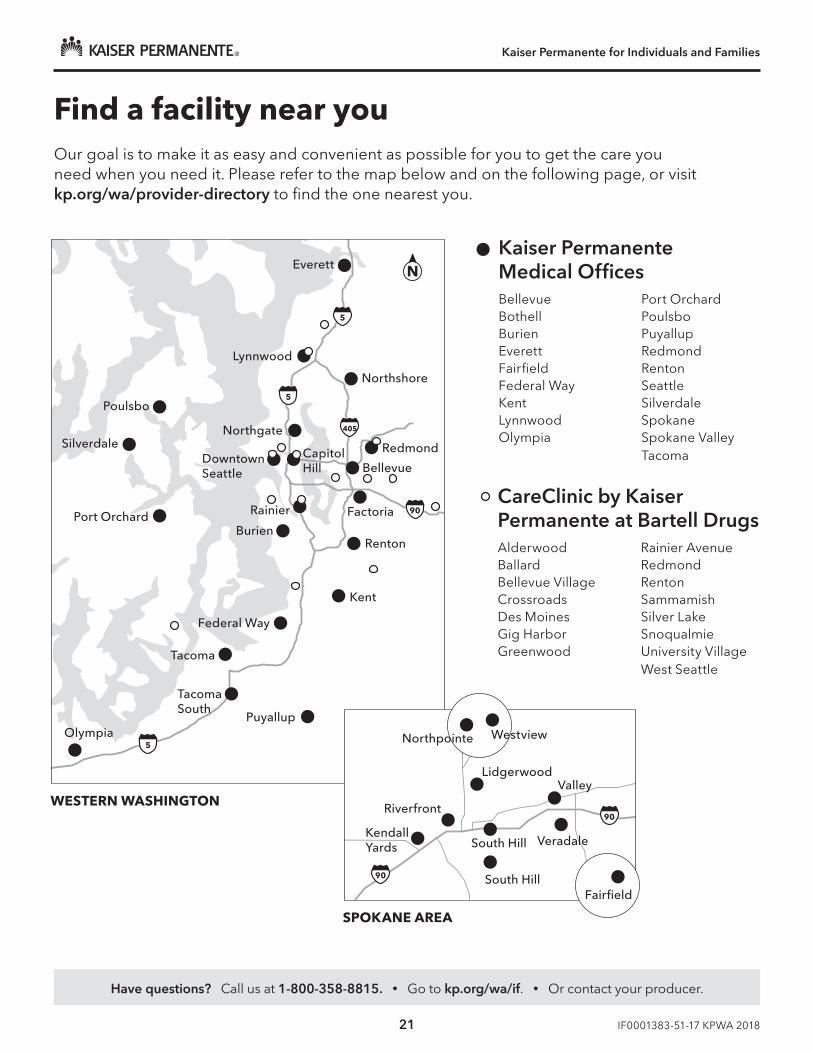
Find a facility near youOur goal is to make it as easy and convenient as possible for you to get the care you need when you need it. Please refer to the map below and on the following page, or visit kp.org/wa/provider-directory to find the one nearest you.
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente Medical OfficesBellevueBothellBurienEverettFairfieldFederal WayKentLynnwoodOlympia
Port OrchardPoulsboPuyallupRedmondRentonSeattleSilverdaleSpokaneSpokane ValleyTacoma
CareClinic by Kaiser Permanente at Bartell DrugsAlderwoodBallardBellevue VillageCrossroadsDes MoinesGig HarborGreenwood
Rainier AvenueRedmondRentonSammamishSilver LakeSnoqualmieUniversity VillageWest Seattle
©2017 Kaiser Foundation Health Plan of Washington
Seattle and Spokane Close UpLorem ipsum dolor sit amet, bibendum vel a, sodales accumsan potenti lobortis.
Bellevue
FactoriaRainier
Renton
RedmondCapitolHill
Northgate
Northshore
Silverdale
Everett
Lynnwood
Kent
Federal Way
Burien
Puyallup
DowntownSeattle
Olympia
Port Orchard
Poulsbo
Tacoma
TacomaSouth
N
90
405
5
5
5
WESTERN WASHINGTON
SPOKANE AREA
Riverfront
KendallYards
South Hill
South Hill Veradale
90
90
Northpointe Westview
Fairfield
ValleyLidgerwood
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
22 IF0001383-51-17 KPWA 2018
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
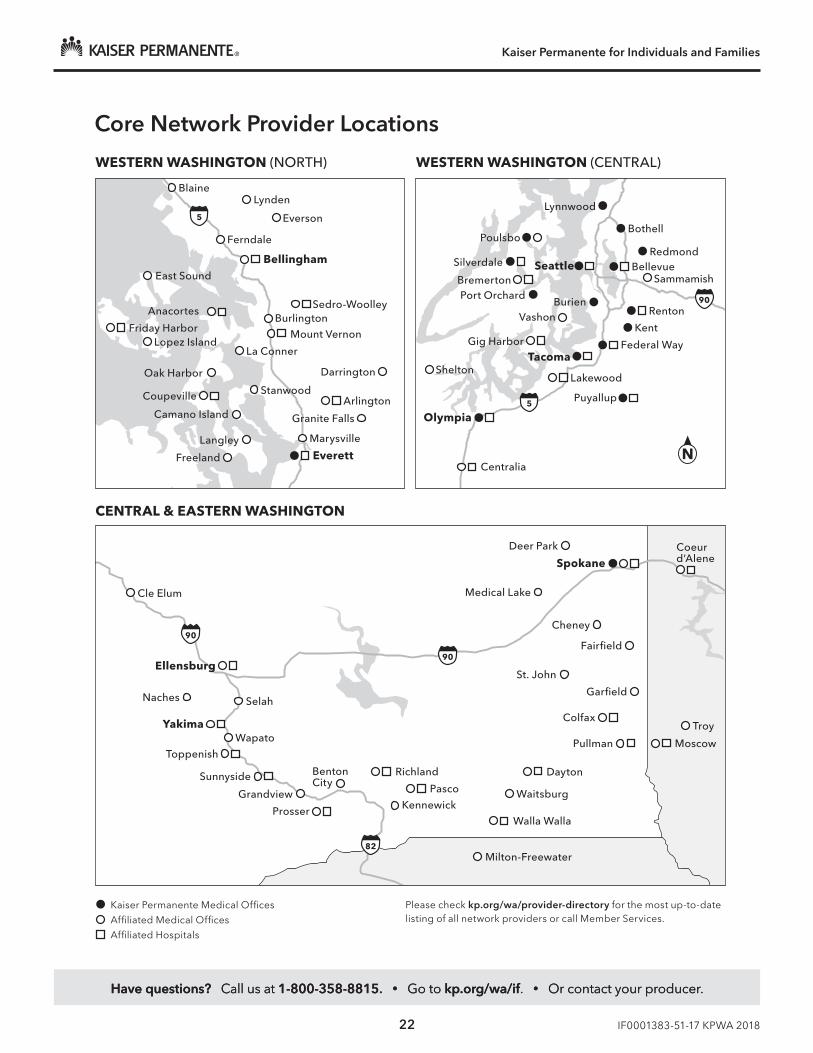
Core Network Provider Locations
Kaiser Permanente Medical Offices
Affiliated Medical Offices
Affiliated Hospitals
WESTERN WASHINGTON (NORTH) WESTERN WASHINGTON (CENTRAL)
Everett
Marysville
Darrington
Langley
Camano Island
Coupeville
Freeland
Granite Falls
ArlingtonStanwood
La Conner
Lakewood
Puyallup
Bellevue
Tacoma
Renton
Redmond
Sammamish
Bothell
Lynnwood
Poulsbo
Silverdale
Port OrchardBremerton
Seattle
Federal Way
Olympia
Centralia
Kent
BurienVashon
Shelton
Gig HarborMount Vernon
Sedro-Woolley
Oak Harbor
CENTRAL & EASTERN WASHINGTON
Milton-Freewater
Walla Walla
Dayton
Cle Elum
Deer Park
SpokaneCoeurd’Alene
Fairfield
Troy
MoscowPullman
Colfax
Garfield
St. John
Medical Lake
Cheney
Ellensburg
Naches
YakimaWapato
Toppenish
Grandview
Prosser
BentonCity
Richland
Pasco
Kennewick
Sunnyside
Selah
Waitsburg
Burlington
Ferndale
BlaineLynden
Everson
Bellingham
N
Anacortes
Friday Harbor
East Sound
Lopez Island
Please check kp.org/wa/provider-directory for the most up-to-date listing of all network providers or call Member Services.
90
90
90
5
5
82
©2017 Kaiser Foundation Health Plan of Washington
Option 1 Black
Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
23 IF0001383-51-17 KPWA 2018
Important disclosure information
Kaiser Foundation Health Plan of Washington | Kaiser Foundation Health Plan of Washington Options, Inc.
Understanding your health plan RCW.48.43.510 and WAC 284-43-5130
Your health plan is designed to help you live your healthiest life. To achieve that, it’s important that you understand your plan’s benefits, coverage, and policies. Upon request, Kaiser Foundation Health Plan of Washington or Kaiser Foundation Health Plan of Washington Options, Inc. (collectively referred to as “Kaiser Permanente” within this document) will provide you with the following information:
• A list of covered benefits, including prescription drug benefits, if any; exclusions, reductions, and limitations to covered benefits, and any definition of medical necessity on which they may be based.
• Information on how members may be involved in decisions about benefits.
• A list of coverage policies for pharmacy benefits, including how drugs are added or removed from the drug formulary.
• Information on policies for protecting the confidentiality of health information.
• Information on premiums and enrollee cost-sharing requirements.
• A summary explanation of the complaints and appeals processes.
• Point-of-service plan availability and how the plan operates.
• A copy of the plan’s current drug formulary for prescription drug coverage.
• A list of participating primary care and specialty care providers, including network arrangements that restrict access to providers within the plan network.
• A list of all available disclosure items, in addition to the above, as required by law.
How we protect your personal informationYour health is our number one priority, and part of caring for you is keeping your personal information safe. Our policies and procedures are designed to protect your personal information in written, verbal, and electronic forms. Specifically:
• We’ll protect your right to access, review, amend, and receive copies of your medical records.
• We’ll protect the confidentiality of your health care information by instituting physical, technical, and administrative controls throughout the organization to protect the use and disclosure of oral, hard copy, and electronic personal health information. We train our employees on these policies and procedures. Employees who violate our confidentiality and security policies are subject to disciplinary action.
• We use and share your personal information to provide treatment, receive and provide payment for health care services, and conduct health care operations.
• We won’t release patient-identifiable health information to third parties without your written permission or authorization except as permitted or required by law.
• We may use health information to support utilization review, quality assessment and measurement, billing, claims management, audits, accreditation, and other health care operations.
• We won’t release detailed utilization information to employers when it might identify individual patients unless permitted or required by law.
For information regarding our privacy practices, you can view our Notice of Privacy Practices at kp.org/wa or call Member Services at 1-888-901-4636. If you are speech- or hearing-impaired, please call the TTY WA Relay at 1-800-833-6388 or 711.
Understanding your plan coverage
Treatment coverageYour treatment and service coverage is determined by your specific health plan. If you ever have any concerns or questions regarding your coverage, contact Member Services for assistance.
For a particular treatment or service to be covered, it must be:

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
24 IF0001383-51-17 KPWA 2018
• Provided or arranged by a Kaiser Foundation Health Plan of Washington or Kaiser Foundation Health Plan of Washington Options, Inc. health care provider (depending on your plan), except for emergency care and urgent care outside of the Kaiser Permanente service area. Kaiser Foundation Health Plan of Washington Options, Inc. members may self-refer to care from any licensed health care provider in the U.S. at a lower benefit level.
• Covered by the Kaiser Foundation Health Plan of Washington or Kaiser Foundation Health Plan of Washington Options, Inc. plan in which you are enrolled. To ask about coverage for a specific treatment or service, contact Member Services.
Utilization reviewsAt Kaiser Permanente, we provide or authorize your medical care based on what is appropriate and necessary for the condition being treated or diagnosed. We do not use financial incentives to encourage our providers to withhold care from members. Our doctors are free to make their own decisions. However, some treatments and services require a utilization review (or coverage review) by the plan.
A utilization review determines whether a treatment or service is covered under the terms of your coverage agreement. It does not determine whether a provider may render services or whether you may choose to purchase a medical service on your own. Utilization reviews may occur at different times relative to the services you receive. It may occur before you receive the services, at the same time you receive services, or after you receive services.
During a utilization review, we will:
• Evaluate whether a specific health care service, procedure, or setting is necessary, appropriate, effective, and efficient for the condition in question; or
• Monitor the use of a specific health care service, procedure, or setting.
Some treatments and services are subject to utilization reviews based on criteria developed by Kaiser Permanente or another organization. In some cases, a service for which we have conducted a utilization review may not be deemed medically necessary, as defined in the plan’s clinical review criteria.
If you believe you need a specific type of care, talk to your health care provider. He or she will discuss it with you and recommend the most appropriate care. For more information about utilization reviews, or
for a written explanation of our criteria for a specific service, contact Member Services.
A pre-service review (or preauthorization) is a specific type of utilization review that occurs prior to your receiving services. Some care requires a referral from your personal physician but does not require preauthorization. However, certain services do require pre-service review to be covered. In addition, the service must be covered by your health plan for you to receive the coverage benefit.
Usually, your provider will arrange for pre-service review when necessary. If a treatment or service is not authorized, you’ll receive a written explanation of the reason for the denial, your right to appeal the decision, and the appeal process.
Kaiser Permanente will not deny coverage retroactively for preauthorized services that have already been provided to the member. Exceptions are if there has been an intentional misrepresentation of a material fact by the patient, member, or provider of services; if coverage was obtained based on inaccurate, false, or misleading information on the enrollment application; or if premiums have not been paid.
Grievances and appeals processesIf you ever have a concern, request, complaint, or compliment, we encourage you to let us know. Kaiser Permanente offers grievance, coverage decision (including exceptions), and appeals processes. Generally, grievances are complaints regarding the quality of care you receive, or the quality of service we provide, including problems getting appointments and disrespectful or rude behavior of staff.
Coverage decisions are decisions about what your plan will and won’t cover. These types of decisions could include an exception for a prescription drug that isn’t on our list of covered drugs or a request for a drug at a lower out-of-pocket cost.
An appeal is a formal way of asking us to review and change a coverage decision we’ve made. You have the right to appeal any coverage decision. The type of appeal, and timeframe for resolution, depends on what is being denied. We’ll tell you how to appeal in the letter we send you explaining our denial decision. We quickly review appeals involving urgently needed care and act as fast as necessary, given the clinical urgency of the condition. Reviews that are clinically urgent will take no longer than 72 hours.

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
KAISER PERMANENTE NONDISCRIMINATION NOTICEKaiser Foundation Health Plan of Washington and Kaiser Foundation Health Plan of Washington Options, Inc. (“Kaiser Permanente”) comply with applicable Federal civil rights laws and do not discriminate on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity. Kaiser Permanente does not exclude people or treat them differently because of race, color, national origin, age, disability, sex, sexual orientation, or gender identity.
Kaiser Permanente: Provides free aids and services to people with disabilities to communicate effectively with us, such as:• Qualified sign language interpreters• Written information in other formats (large print, audio, accessible electronic formats, other formats)
Provides free language services to people whose primary language is not English, such as:• Qualified interpreters• Information written in other languages
If you need these services, contact Kaiser Permanente Member Services.
If you believe that Kaiser Permanente has failed to provide these services or discriminated in another way on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity, you can file a grievance by phone, mail, fax, or email. If you need help filing a grievance, a Kaiser Permanente Member Services Representative is available to help you. Language assistance is provided free of charge. The Kaiser Permanente Civil Rights Coordinator will be notified of all grievances related to discrimination on the basis of race, color, national origin, age, disability, sex, sexual orientation, or gender identity.
Phone: 206-630-4636 Toll-free: 1-888-901-4636 TTY Washington Relay Service: 1-800-833-6388 or 711 TTY Idaho Relay Service: 1-800-377-3529 or 711 Fax: 206-901-6205 or toll-free 1-888-874-1765 Address: Kaiser Foundation Health Plan of Washington Civil Rights Coordinator, Quality GNE-D1E-07 P.O. Box 9812 Renton, WA 98057-9054 Email: [email protected]
You can also file a civil rights complaint with the U.S. Department of Health and Human Services, Office for Civil Rights electronically through the Office for Civil Rights Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at: U.S. Department of Health and Human Services 200 Independence Avenue SW., Room 509F HHH Building Washington, DC 20201 1-800-368-1019, 800-537-7697 (TDD) Complaint forms are available at http://www.hhs.gov/ocr/office/file/index.html
For Medicare Advantage Plans Only: Kaiser Permanente is an HMO plan with a Medicare contract. Enrollment in Kaiser Permanente depends on contract renewal.
Kaiser Permanente Nondiscrimination Notice and Language Access Services
© 2017 Kaiser Foundation Health Plan of Washington H5050_XB0001444_55_17 accepted 2017-XB-6_ACA_Notice_Taglines

Kaiser Permanente for Individuals and Families
IF0001383-51-17 KPWA 2018
LANGUAGE ACCESS SERVICES
English: ATTENTION: If you speak English, language assistance services, free of charge, are available to you. Call 1-888-901-4636 (TTY: 1-800-833-6388 or 711).
Español (Spanish): ATENCIÓN: si habla español, tiene a su disposición servicios gratuitos de asistencia lingüística. Llame al 1-888-901-4636 (TTY: 1-800-833-6388 / 711).
中文 (Chinese):注意:如果您使用繁體中文,您可以免費獲得語言援助服務。請致電 1-888-901-4636 (TTY: 1-800-833-6388 / 711)。
Tiếng Việt (Vietnamese): CHÚ Ý: Nếu bạn nói Tiếng Việt, có các dịch vụ hỗ trợ ngôn ngữ miễn phí dành cho bạn. Gọi số 1-888-901-4636 (TTY: 1-800-833-6388 / 711).
한국어(Korean): 주의: 한국어를 사용하시는 경우, 언어 지원 서비스를 무료로 이용하실 수 있습니다. 1-888-901-4636 (TTY: 1-800-833-6388 / 711) 번으로 전화해 주십시오.
Русский (Russian): ВНИМАНИЕ: Если вы говорите на русском языке, то вам доступны бесплатные услуги перевода. Звоните 1-888-901-4636 (телетайп: 1-800-833-6388 / 711).
Filipino (Tagalog): PAUNAWA: Kung nagsasalita ka ng Tagalog, maaari kang gumamit ng mga serbisyo ng tulong sa wika nang walang bayad. Tumawag sa 1-888-901-4636 (TTY: 1-800-833-6388 / 711).
Українська (Ukrainian): УВАГА! Якщо ви розмовляєте українською мовою, ви можете звернутися до безкоштовної служби мовної підтримки. Телефонуйте за номером 1-888-901-4636 (телетайп: 1-800-833-6388 / 711).
ភាសាខ្មែរ (Khmer)៖ របយ័ត�៖ េេបើសិន�អ�កនិ�យ��ខ្�រ, េស�ជំនួខយផ�ក�� េ�យមិនគិត�ល គឺ�ច�នសំ�ប់បំេរ�អ�ក។ ចូរទូរស័ព� 1-888-901-4636 (TTY: 1-800-833-6388 / 711)។
日本語 (Japanese): 注意事項:日本語を話される場合、無料の言語支援をご利用いただけます。 1-888-901-4636 (TTY: 1-800-833-6388 / 711) まで、お電話にてご連絡ください。
አማርኛ (Amharic)፥ ማስታወሻ: የሚናገሩት ቋንቋ ኣማርኛ ከሆነ የትርጉም እርዳታ ድርጅቶች፣ በነጻ ሊያግዝዎት ተዘጋጀተዋል፡ ወደ ሚከተለው ቁጥር ይደውሉ 1-888-901-4636 (መስማት ለተሳናቸው: 1-800-833-6388 / 711).
Oromiffa (Oromo): XIYYEEFFANNAA: Afaan dubbattu Oroomiffa, tajaajila gargaarsa afaanii, kanfaltiidhaan ala, ni argama. Bilbilaa 1-888-901-4636 (TTY: 1-800-833-6388 / 711).
العربية (Arabic): لديكم حق الحصول على مساعدة ومعلومات فيملحوظة: إذا كنت تتحدث اذكر اللغة، فإن خدمات المساعدة اللغوية
تتوافر لك بالمجان. اتصل برقم 1-888-901-4636 (رقم هاتف الصم والبكم: 1-800-833-6388 / 711).
ਪੰਜਾਬੀ (Punjabi): ਧਿਆਨ ਧਿਓ: ਜੇ ਤੁਸੀਂ ਪੰਜਾਬੀ ਬੋਲਿੇ ਹੋ, ਤਾਂ ਭਾਸਾ ਧਿੱਚ ਸਹਾਇਤਾ ਸੇਿਾ ਤੁਹਾਡੇ ਲਈ ਮੁਫਤ ਉਪਲਬਿ ਹੈ। 1-888-901-4636 (TTY: 1-800-833-6388 / 711) ‘ਤੇ ਕਾਲ ਕਰੋ।
Deutsch (German): ACHTUNG: Wenn Sie Deutsch sprechen, stehen Ihnen kostenlos sprachliche Hilfsdienstleistungen zur Verfügung. Rufnummer: 1-888-901-4636 (TTY: 1-800-833-6388 / 711).
ພາສາລາວ (Lao): ໂປດຊາບ: ຖາ້ວ່າ ທ່ານເວົາ້ພາສາລາວ, ການບໍ ລກິານຊ່ວຍເຫຼອືດາ້ນພາສາ, ໂດຍບ່ໍເສຽັຄ່າ, ແມ່ນມພີອ້ມໃຫທ່້ານ. ໂທຣ 1-888-901-4636 (TTY: 1-800-833-6388 / 711).
Srpsko-hrvatski (Serbo-Croatian): OBAVJEŠTENJE: Ako govorite srpsko-hrvatski, usluge jezičke pomoći dostupne su vam besplatno. Nazovite 1-888-901-4636 (TTY- Telefon za osobe sa oštećenim govorom ili sluhom: 1-800-833-6388 / 711).
Français (French): ATTENTION : Si vous parlez français, des services d’aide linguistique vous sont proposés gratuitement. Appelez le 1-888-901-4636 (ATS: 1-800-833-6388 / 711).
Română (Romanian): ATENȚIE: Dacă vorbiți limba română, vă stau la dispoziție servicii de asistență lingvistică, gratuit. Sunați la 1-888-901-4636 (TTY: 1-800-833-6388 / 711).
Adamawa (Fulfulde): MAANDO: To a waawi Adamawa, e woodi ballooji-ma to ekkitaaki wolde caahu. Noddu 1-888-901-4636 (TTY: 1-800-833-6388 / 711).
فارسی (Farsi): توجه: اگر به زبان فارسی گفتگو می کنيد، تسهيالت زبانی بصورت رايگان برای شما فراهم می باشد. با
1-888-901-4636 (TTY: 1-800-833-6388 / 711) تماس بگيريد.
XB0001444-55-17

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
27 IF0001383-51-17 KPWA 2018
Notes

Have questions? Call us at 1-800-358-8815. • Go to kp.org/wa/if. • Or contact your producer.
Kaiser Permanente for Individuals and Families
28 IF0001383-51-17 KPWA 2018
Notes

Care is just a click awayDigital tools designed to make your life easier
New member?Visit kp.org/wa/getstarted to learn more. It’s easy to register at kp.org/wa, choose your doctor, transfer your prescriptions, and schedule your first routine appointment.* And if you need help, just give us a call.
Already a member?Manage your care online anytime at kp.org/wa. If you haven’t already, go to kp.org/wa/register so you can start emailing your doctor’s office* with nonurgent questions, schedule routine appointments,* order most prescription refills, and more.
*These features are available when you get care at Kaiser Permanente facilities.

The right choice for a healthier youHaving a good health plan is important. So is getting quality care. With Kaiser Permanente, you get both.
Please recycle. IF0001381-50-17
Kaiser Foundation Health Plan of Washington 601 Union St., Suite 3100
Seattle, WA 98101
©2017 Kaiser Foundation Health Plan of Washington
facebook.com/kaiserpermanentewashington
youtube.com/kaiserpermanenteorg
@kpwashington
Stay connected to good health
Want to learn more?Visit kp.org/wa or call us at 1-800-358-8815. (For TTY, call 711.)