journal of bodywork & movement therapies · 2018-01-13 · neurodynamics is commonly utilized...
TRANSCRIPT

lable at ScienceDirect
Journal of Bodywork & Movement Therapies xxx (2017) 1e9
Contents lists avai
Journal of Bodywork & Movement Therapies
journal homepage: www.elsevier .com/jbmt
Pilot Study
Integration of a neurodynamic approach into the treatment ofdysarthria for patients with idiopathic Parkinson's disease: A pilotstudy
Barbara Ateras a, *, Harry von Piekartz b
a Faculty of Health and Medicine, Danube University Krems, Austriab Faculty of Business, Management and Social Science, University of Applied Science, Osnabrueck, Germany
a r t i c l e i n f o
Article history:Received 7 August 2017Received in revised form24 November 2017Accepted 4 December 2017
* Corresponding author. Heilpaedagogisches ZentOberurnen, Switzerland.
E-mail address: [email protected] (B. Ateras
https://doi.org/10.1016/j.jbmt.2017.12.0041360-8592/© 2017 Elsevier Ltd. All rights reserved.
Please cite this article in press as: Ateras, Bpatients with idiopathic Parkinson's diseasj.jbmt.2017.12.004
a b s t r a c t
Purpose: Differences between standard dysarthria treatment and the same treatment with the inte-gration of neurodynamic techniques tailored to the severity of dysarthria in patients with Parkinson'sdisease were examined.Method: In total, 10 subjects with idiopathic Parkinson's disease and rigidehypokinetic dysarthria wereenrolled in this quasi-randomized, controlled, single-blind, preepost study. In each of 12 therapy ses-sions the control group (n ¼ 5) received standard dysarthria treatment (usual care), while the inter-vention group (n ¼ 5) received the same treatment with the addition of integrated neurodynamictreatment (special care).Results: There was no significant difference between the two groups for either the pre-test (p ¼ 0.739) orthe post-test (p ¼ 0.156) results. However, significant differences between the pre-test and post-testresults within each group (intervention group p ¼ 0.001; control group p ¼ 0.003) were found.Conclusions: The significant differences in the preepost comparison within the groups may indicate ahigh probability of a positive effect of standard dysarthria treatment on the severity of dysarthria. Inbetween-group comparisons, the study results indicated no evidence of a significant difference betweenstandard dysarthria treatment with or without neurodynamics. Due to the small sample size, theeffectiveness of the integration of neurodynamics into speech therapy cannot be definitively concludedfor now. In order to be able to have generalized applicability, future studies with larger numbers ofparticipants are required.
© 2017 Elsevier Ltd. All rights reserved.
1. Introduction
Neurodynamics is commonly utilized in the physiotherapeuticdomain for diagnosis and treatment of neuromusculoskeletal dys-functions and pain (Butler, 2006; Shacklock, 2008). The basis forneurodynamics is the premise that there is a reciprocal relationshipand influence between the biomechanics and the physiology of thenervous system, which in turn have an impact on musculoskeletalfunctions (Shacklock, 2008). The term ‘biomechanics of the nervoussystem’ refers to the natural disposition of the nervous system tomove itself. This ability is necessary to withstand the mechanicalforces generated by everyday physiological movements (Butler,
rum, Arenaweg 6, CH-8868,
).
., von Piekartz, H., Integratioe: A pilot study, Journal of
1995; Nee and Butler, 2006; Shacklock, 2008). The nervous sys-tem must be able to carry out three mechanical functions suc-cessfully in order to fulfill normal movement: it needs to becompressible, able to slide relative to its surrounding structures,and be able to resist tension. All threemechanical functions interactinterdependently, triggered by a complex sequence of events,including, for example, the movement of joints and movementsthat increase 2 points of the nervous system. Likewise, the me-chanical functions of the nervous system are activated by move-ments of the mechanical interface, such as adjacent structures ofthe nervous system (e.g. muscles, ligaments, bones, blood vessels).As mentioned above, these mechanisms of the nervous system aredirectly interdependent with its physiology (Coppieters and Butler,2008). Accordingly, pathomechanical changes of peripheral neuraltissue, which may be due to, for example, a neurological disorder,result in pathophysiological responses, which in turn have an
n of a neurodynamic approach into the treatment of dysarthria forBodywork & Movement Therapies (2017), https://doi.org/10.1016/

B. Ateras, H. von Piekartz / Journal of Bodywork & Movement Therapies xxx (2017) 1e92
impact on the appropriate target tissue (Rolf, 2006). Correspond-ingly, it is assumed that recovery of the nerve leads to animprovement in the neurophysiological processes (Butler, 2006).This relation and mutual interaction of the mechanics and physi-ology (or the pathomechanics and pathophysiology) of the nervoussystem are used both therapeutically and diagnostically in theconcept of neurodynamics. Thus, mechanical treatment of thenervous system, such as in a trophic disorder of peripheral nerveconnective tissue, can be used to improve its physiology (Shacklock,2008). Just as in physiotherapy, neuromusculoskeletal dysfunctionsare treated in speech therapy, such as dysarthria, dysphagia,dysphonia, and facial paresis. From a clinical perspective, it can beassumed that it is possible to integrate neurodynamic treatmenttechniques effectively into speech therapy. Subjectively, clearchanges are observable within a short time with the use of neu-rodynamic techniques in speech therapy treatment of dysarthria,dysphagia, dysphonia, and facial paresis. To assess the viability ofthis new approach in speech and language therapy, a small testinggroup was used to perform a pilot study of the integration ofneurodynamic techniques in dysarthria treatment for patients withidiopathic Parkinson's disease. Given the small sample size in thisinitial study, generalizations of the study results are limited. On theother hand, it is possible to adjust the sample size in a possiblysubsequent large-scale study by estimating the variance in thispilot study.
At the time of the pilot study, two Meta-studies from theCochrane Library (Herd et al., 2012a, 2012b) indicate that there arealtogether nine randomized controlled trials available on speechtherapies for patients with Parkinson's disease and dysarthria. Inone Meta study Herd et al. (2012a) compared the efficacy of speechand language therapy (SLT) versus placebo or no intervention forspeech and voice problems in patients with Parkinson's disease(Johnson and Pring, 1990; Ramig et al., 2001; Robertson andThomson, 1984). In the other Meta-study (Herd et al., 2012b) theycompared the efficacy and effectiveness of novel SLT techniquesversus a standard SLT approach to treat Parkinsonian speechproblems (Scott and Caird, 1983; Ramig et al., 1995; Lowit et al.,2010; Halpern et al., 2007; Constantinescu et al., 2011; Healy,2002). In two of these nine studies, no statistical data analysiswas carried out (Healy, 2002; Scott and Caird,1983). Only one studyshowed no significant results to refute the null hypothesis (Lowitet al., 2010), whereas the remaining studies achieved significantimprovements in at least a portion of their outcomes. All studieshad rather small sample sizes (total sample size ranged from 10 to45). Four of the nine studies (Constantinescu et al., 2011; Halpernet al., 2007; Ramig et al., 2001, 1995) investigated the Lee Silver-man Voice Treatment (LSVT). The guidelines of the GermanNeurological Society note that there is an extensive body of dataindicating significant improvements in dysarthric disorders withthe use of LSVT speech therapy exercises (Diener, 2012). However,there are no studies on the effectiveness of neurodynamics inspeech therapy.
The orthopedic literature contains a number of scientific studiescovering all areas of neurodynamics, some of which have a largesample size. Quality criteria for neurodynamic tests, such as thestraight leg raise (SLR), the slump test, the upper limb neuro-dynamic test (ULNT), and nerve palpationwere identified in variousstudies (Capra et al., 2011; Carla et al., 2010; Majlesi et al., 2008;Rabin et al., 2007; Vanti et al., 2011; Walsh and Hall, 2009). Like-wise, there are studies on the effectiveness of neural mobilizationto treat orthopedic conditions such as carpal tunnel syndrome anda herniated disc (De-la-Llave-Rincon et al., 2012; Heebner andRoddey, 2008; Nee et al., 2013; Oskay et al., 2010; Villafa~ne et al.,2011). A number of studies have scientifically investigated the in-fluence of neurodynamic techniques on the biomechanics and
Please cite this article in press as: Ateras, B., von Piekartz, H., Integratiopatients with idiopathic Parkinson's disease: A pilot study, Journal ofj.jbmt.2017.12.004
physiology of the nervous system (Beneciuk et al., 2009; Breig,1960, 1978; Brown et al., 2011), as well as the effects of sensitizedneurodynamic components on individual neurodynamic tests ormuscle activity (Boyd et al., 2009; Lohkamp and Small, 2011; Neeet al., 2010). Thus, there are several studies providing evidence ofthe effectiveness of neurodynamics for diagnosis and treatment inorthopedics.
Fewer scientific studies exist on neurodynamics in theneurology literature. Altered muscle activity and sensitivity in theupper extremities are the primary topics in published studies onneurology in the context of treatment with ULNT (Castilho et al.,2012; Cha et al., 2012; Godoi et al., 2010; Wolny et al., 2010). Onlyone neurological study has been conducted on mobilization of thecervical spine (Villafa~ne et al., 2012). Currently, no published clin-ical studies exist on neurodynamic diagnosis and treatment of thetorso or lower limbs of patients with central nervous system le-sions. In the studies conducted so far, stroke was by far the mostcommon underlying neurological disorder of the patients. Only onestudy references a patient with Alzheimer's disease being diag-nosed and treated (Villafa~ne et al., 2012) and one case study ispublished on the treatment of dysfunction and pain effected by aperipheral neurogenic cause in the temporomandibular region(Geerse and Piekartz von, 2015). There are no studies about otherneurological or neurodegenerative diseases in relation to neuro-dynamics. In addition, the sample sizes in the existing studies arelow (ranging from n ¼ 1 to n ¼ 32). Based on this summary ofevidence-based neurodynamics in neurology, there is a need forclinical trials of neurodynamic diagnosis and treatment in patientswith neurological disorders.
Because there are no studies on the use of neurodynamics in thefield of speech therapy up to now and there has only been a smallnumber of studies on the treatment of dysarthria in Parkinson'sdisease or on the use of neurodynamics in the field of neurology, apilot study on the integration of neurodynamic techniques in thetreatment of dysarthria in patients with Parkinson's disease wascarried out. The aim of the study was to identify any differences inthe severity of dysarthria between a group of patients with Par-kinson's disease given standard dysarthria treatment alone andanother group given the same treatment with the integration ofneurodynamic techniques. In addition, a first insight into theviability of the integration of neurodynamics into speech therapyshould be provided.
The rationale for the integration of neurodynamics into stan-dard treatment is, that it may directly affect the peripheral nervoussystem, resulting in improved efficiency of the region treated. Aftera short neural mobilization, the clinician observes an obviousimprovement in speech motor skills, e.g. a clearer speaking voice.With the improved speech skills, the subsequent speech therapyexercises can be carried out in a more intensive and more effectivemanner. Therefore, a speech therapy treatment with the integra-tion of neurodynamic techniques may lead to better results thanthe same treatment without neurodynamics.
2. Method
2.1. Study design
The total sample of 10 patients with Parkinson's disease wasquasi-randomized into an intervention group (IG) and a controlgroup (CG). The CG received standard dysarthria treatment (usualcare) alone, while the IG received the same standard dysarthriatreatment with integrated neurodynamic therapy (special care).The additional inclusion of a control group that received no treat-ment was not possible for operational reasons. Based on thepreepost study design, a standardized dysarthria diagnostic test,
n of a neurodynamic approach into the treatment of dysarthria forBodywork & Movement Therapies (2017), https://doi.org/10.1016/

B. Ateras, H. von Piekartz / Journal of Bodywork & Movement Therapies xxx (2017) 1e9 3
named Bogenhausener-Dysarthrie-Skalen (BoDyS) (Ziegler et al.,2015), was completed immediately before and immediately afterthe full therapeutic intervention (consisting of 12 therapy sessionsin total). The test evaluation was carried out in a blinded manner.
The entire study was conducted in Germany in two inpatientrehabilitation clinics for patients with Parkinson's disease, and alsoincluded one outpatient with Parkinson's disease, from a privatespeech-therapy practice. The in-patient subjects visited the reha-bilitation clinics exclusively because of their Parkinson's disease.Their duration of stay corresponded to the requirements of thehealth insurance companies.
Because the patients from the inpatient rehabilitation clinicscame from the entire Federal Republic of Germany, there is a highexternal validity. The diagnosis and treatment of participating pa-tients took place from July 6 to August 13, 2012.
2.2. Participants
Patients with a diagnosis of idiopathic Parkinson's disease withmild to moderate rigidehypokinetic dysarthria were included inthe study. Exclusion criteria were the presence of additionalneurological diseases or presence of existing dementia. In total, 10subjects (three women, seven men) with a mean age of 68.7 years(SD ± 7.8 years) participated in the pilot study. Five subjects (onewoman and four men) with a mean age of 65.0 years (SD ± 6. 11years) were assigned to the intervention group and five subjects(two women and three men) with a mean age of 72.2 years(SD ± 7.2 years) were assigned to the control group. The meanduration of illness, based on the time of diagnosis of Parkinson'sdisease, was 8.2 and 7.8 years in the intervention and controlgroups, respectively. The previous outpatient speech therapyreceived by the patients was counted in numbers of therapy ses-sions received to baseline: 4 and 4.8 therapy sessions for theintervention and control groups, respectively. Prior to treatment,the severity of cognitive deficits was assessed by the Mini-MentalStatus Examination (MMSE) (Folstein et al., 2000), which gives amaximum score of 30. A score greater than or equal to 24 indicatesnormal cognition. Mean scores were 28 and 28.4 for the interven-tion and control groups, respectively (Table 1).
2.3. Procedure
The study period corresponded to the ethics criteria of theDeclaration of Helsinki (World Medical Association, 2013). All pa-tients were informed both, verbally and in writing, about the pur-pose, the procedure and the type of the research intervention, aswell as about their voluntary participation prior to their signing aconsent form.
To assess differences in the severity of dysarthria in patientswith Parkinson's disease between the standard dysarthria treat-ment with and without the integration of neurodynamic
Table 1Gender distribution, mean age, duration of disease, outcome of the MMSE, durationof treatment, frequency of therapy of the IG and CG.
Interventiongroup (n ¼ 5)
Controlgroup (n ¼ 5)
Female/male 20%/80% 40%/60%Age in years 65 (±6.11) 72.7 (±7.2)Duration of disease in years 8.2 7.8Outpatient speech therapy
sessions (TS)4 4.8
Median MMSE score 28 28.4Duration of treatment in days 11 11.4TS/day 1.15 1.07
Please cite this article in press as: Ateras, B., von Piekartz, H., Integratiopatients with idiopathic Parkinson's disease: A pilot study, Journal ofj.jbmt.2017.12.004
techniques, a quasi-randomized, controlled, single-blind studywith preepost comparison was performed. The IG received stan-dard dysarthria treatment with the integration of neurodynamictechniques, while the CG received the same standard dysarthriatreatment without additional stimulation. All patients received 12therapy sessions that lasted 45 min. Sessions were spread out overa period of 7e14 days (further details see below). During thetherapy session the IG received about 10e15 min neurodynamictreatment. The treatment for both groups was conducted in indi-vidual sessions by a speech & language therapist with 20 years ofprofessional clinical experience, including over five years experi-ence with neurodynamic techniques and who has worked as aninstructor for neurodynamics in speech therapy. In all locations ofthe study the allocation of the patients to the respective groups wascarried out in a quasi-randomized manner using a deterministicallocation, which was alternating assignment of the patients, i.e.the first registered patient was assigned to the intervention group,the second to the control group, the third to the intervention group,etc. (Trampisch and Windeler, 2000). Regular randomization of asmall sample size leads to the risk of an inhomogeneous group size.This would bias the study results. The use of quasi-randomizationenabled homogeneous distribution of the patients, with n ¼ 5 forboth groups.
For all participating patients the BoDyS (Ziegler et al., 2015) wasused. This is a standardized dysarthria assessment to determine thefrequency and the severity of the different clinical features ofdysarthria. Unlike other instruments, the BoDyS exclusively as-sesses speech motor functions. In a total population sample of 167patients with different etiologies of dysarthria, the overall score ofthe BoDyS achieved excellent reliability (Cronbach's a ¼ 0.99)(Ziegler et al., 2015). Pearson's product-moment correlation coef-ficient was used to analyze the objective scoring. Verified on thebasis of two independent listeners and a sample size of n ¼ 71patients, it also resulted in a high objective score (r ¼ 0.95). Thecontent validity of the BoDyS is high because the test criteria relateto speech motor functions, the scales are neurophonetically justi-fied, and the features to be examined correspond to the mostimportant symptoms of dysarthria described in the literature.Moreover, there is numerous empirical evidence for the constructvalidity of the BoDyS (Ziegler et al., 2015). The BoDyS is divided intothree stages, each of which contains measures to examine speechmotor skills in four categories: interview questions, repetitive tasksat sentence-level, text-level reading, and narrating storylinesprompted by wordless picture stories. In total, 12 (3 stages x 4categories) speech samples are collected (Ziegler and Vogel, 2010).The evaluation of the BoDyS is carried out in two parts, with twoevaluation sheets for each. In the first part, the auditive assessmentof the 12 speech samples takes place on the basis of nine scales(breathing, voice pitch, voice quality, voice stability, articulation,resonance, speech tempo, oral fluency, and modulation). Majorcharacteristic features (e.g. increased inspiratory frequency is oneof the main features subordinated to the breathing scale) are sub-ordinated to each of these scales. After each speech sample themajor observed features of each scale are marked on the evaluationsheet. For the treatment decisions the most frequently observedmajor features are selected. Accordingly, this first evaluation sheetis a qualitative analysis, which gives information about the majorfeatures of the individual's dysarthric speech and thus enables thetherapist to draw specific conclusions for treatment planning. Thequalitative analysis was only relevant for the treatment planning;however, the qualitative results of the pre- and post-testing werenot included in the statistical evaluation. The second part of theevaluation provides data for statistical analysis and quantifies theseverity of the speech disorder. It is carried out after the assessmentand is based on audio/video recording during the assessment. In a
n of a neurodynamic approach into the treatment of dysarthria forBodywork & Movement Therapies (2017), https://doi.org/10.1016/

B. Ateras, H. von Piekartz / Journal of Bodywork & Movement Therapies xxx (2017) 1e94
predetermined sequence, the examiner watches and listens to oneof the 12 speech samples at a time (Nicola et al., 2004). With the aidof a table (columns: speech samples; lines: nine scales) and adefined scoring system (0 points ¼ most severe disorder, 1point ¼ severe disorder, 2 points ¼ moderate disorder, 3points ¼ mild disorder, 4 points ¼ no disorder), the examinerevaluates the severity of the disorder in the current speech samplewithin the nine scales described above. With the scores assigned toeach speech sample, a profile in the form of a line diagram can beconstructed based on a predetermined coordinate system. Acrossthe nine scales in all 12 speech samples of the BoDyS, a maximumof 432 points (12 speech samples x 9 scales x the maximum of 4points) can be achieved. For the statistical evaluation the total scoreof each test within the intervention group and the study group iscalculated. These four sums (pre- and post-test of both groups) arethe basis for the statistical analysis (further details see below).
In the current study, the BoDySwas used for all subjects as a pre-test 1 day before the start of the therapy sequence, and as a post-test 1 day after completion of the therapy sequence. While theassessments were conducted by the same personwho also directedthe treatments, the requirements for test performancewere exactlyspecified (Nicola et al., 2004) to ensure a high degree of proceduralobjectivity. Given these safeguards, this test set-up whereby boththe test as well as the treatment is carried out by the same personshould not undermine the test results. The test evaluation wasconducted by an independent speech therapist with 30 years ofprofessional clinical experience. After intensive training in testevaluation with the BoDyS, the evaluator received, in quasi-randomized sequence, the video recording of the test survey tobe analyzed. Therefore, the speech therapist had no informationabout the group affiliation of the respective subjects or aboutwhether the examination concerned a pre- or post-test. The pa-tients themselves were also unaware of whether they belonged tothe intervention or to the control group. All participating patientswere treated by the same therapist, who was aware of the patientgroups, since the therapist had to arrange the appropriate treat-ment plan. Because the patients had different lengths of stay in therehabilitation centers, the therapy frequency of the 12 therapysessions (45 min each) could not be carried out within a consistenttime-frame. Therefore, to detect any possible resulting distortion, acorrelation was computed between the time-frame of the therapyfrequency and the diagnostic results. No follow-up has been carriedout.
The following flow chart (Fig. 1), according to the guidelines ofthe CONSORT statement (Schulz et al., 2011), illustrates theincluded and excluded subjects during the research process.
2.4. Therapy content
The therapy content was derived from the first evaluation of theBoDyS. The standard dysarthria treatment involved speech therapyexercises targeting functional areas of the speech musculoskeletalsystem that had previously been diagnosed as core deficit areas(breathing, resonance, phonation, articulation, prosody) in therespective patient. The standard dysarthria treatment is based onthe German version of the therapeutic approach pioneered byRobertson and Thomson (2000) and supplemented with exercisesof speech training (Fiukowski, 2010) and functional voice therapy(Brügge and Mohs, 2014). For the purpose of treating speechbreathing disorders, exercises were included in order to establish acorrect posture and costo-abdominal breathing patterns, toimprove breath control, to increase loudness, to achieve appro-priate breath phrasing during speech and to regulate the intraoralair pressure. An increased vocal intensity and projection of thevoice as well as extended ranges of vocal pitch and loudness have
Please cite this article in press as: Ateras, B., von Piekartz, H., Integratiopatients with idiopathic Parkinson's disease: A pilot study, Journal ofj.jbmt.2017.12.004
been treated in the field of phonatory disturbances. The manage-ment of articulatory disorders involves exercises for the lips, tongueand jaw. Accordingly, the therapy techniques were designed toimprove the strength, endurance and rate of these articulatorsacross a variety of speech production tasks: repetition of words,phrases and sentences, minimal pairs, tongue twisters as well asreading and spontaneous speech. In case velopharyngeal insuffi-ciency was detected, an articulation therapy programwas also usedto provide adequate intraoral pressure for the production of plosiveand fricative consonants. The prosody therapy included exercises toimprove stress patterns and intonational contours in differentspeech situations and with various emotional expressions. Theadditional neurodynamic treatment in the IG includedmobilizationand palpation of peripheral nerves. Palpation and mobilization ofthe peripheral nerves are painless manual techniques, which maybe used as physical examination but also as treatment techniques.Superficial peripheral nerves may be palpated by gentle lateralpulling of the nerve with the fingertip (like plucking a guitar string)(Butler, 2006). The purpose of mobilization of the nervous systemsupports normal functional movement of peripheral neural tissues,like gliding and stretching without discomfort, and treatment ofnon-neural structures surrounding the nervous system, like joints,muscles or even scar tissue (Coppieters and Butler, 2008). Detailedpalpation and mobilization techniques have been described byButler (1995, 2006), Maitland (2004), and specifically for cranialnerves by Piekartz von (2007).
The following cranial nerves supply the muscles involved inspeech: trigeminal nerve (V), facial nerve (VII), glossophar-ynfpleasegeal nerve (IX), vagus nerve (X), accessory nerve (XI), andhypoglossal nerve (XII) (Wendler et al., 2005; Ziegler, 2006; Zieglerand Vogel, 2010). In addition, motor innervation of the respiratorymuscles is effected through the phrenic nerve, the intercostalnerves IeXI, and branches from the cervical and the brachial plexus(Larsen and Ziegenfub, 2012; Schulte et al., 2007; Ziegler, 2006;Ziegler and Vogel, 2010). As part of the clinical reasoning process,the particular choice of which nerves were treated was derivedfrom the outcome of the first evaluation sheet of the BoDyS. Theneurodynamic techniques described below were integrated intothe standard dysarthria treatment. To improve respiration, thoracicmobilizationwas performed (Butler, 2006; Jeangros, 2011; Piekartzvon, 2011) to mobilize the intercostal nerves. Likewise, palpationand mobilization of the cervical plexus, brachial plexus, andaccessory nerve (Butler, 1995, 2006; Shacklock, 2008) wereimplemented for the treatment of speech-related breathing.Palpation and mobilization of the vagus nerve (Maitland, 2004;Piekartz, 2015) were the neurodynamic treatment techniquesused to improve vocal function. Similarly, in patients with articu-lation disorders, palpation techniques alonewere used for the facialnerve (Fig. 2), whereas mobilization and palpation techniques wereused for the trigeminal (Fig. 3), hypoglossal, and glossopharyngealnerves (Butler, 2006; Piekartz von, 2007). The neurodynamic ma-neuvers within the context of dysarthria treatment are summarizedin Table 2.
2.5. Statistical analysis
All statistical analyses were performed with SPSS software(version 20.0; IBM SPSS, Armonk, NY, USA). To compare pre- andpost-testing within the overall sample and between the inter-vention and control groups, the t-test for paired samples wasused, with a 95% confidence interval. Owing to the small samplesize, the KolmogoroveSmirnov test was used to quantify thenormal distribution, and according to the results of this test(n ¼ 10; most extreme differences absolute: 0.202; asymptoticsignificance: p ¼ 0.200) the theoretical assumption of a normal
n of a neurodynamic approach into the treatment of dysarthria forBodywork & Movement Therapies (2017), https://doi.org/10.1016/
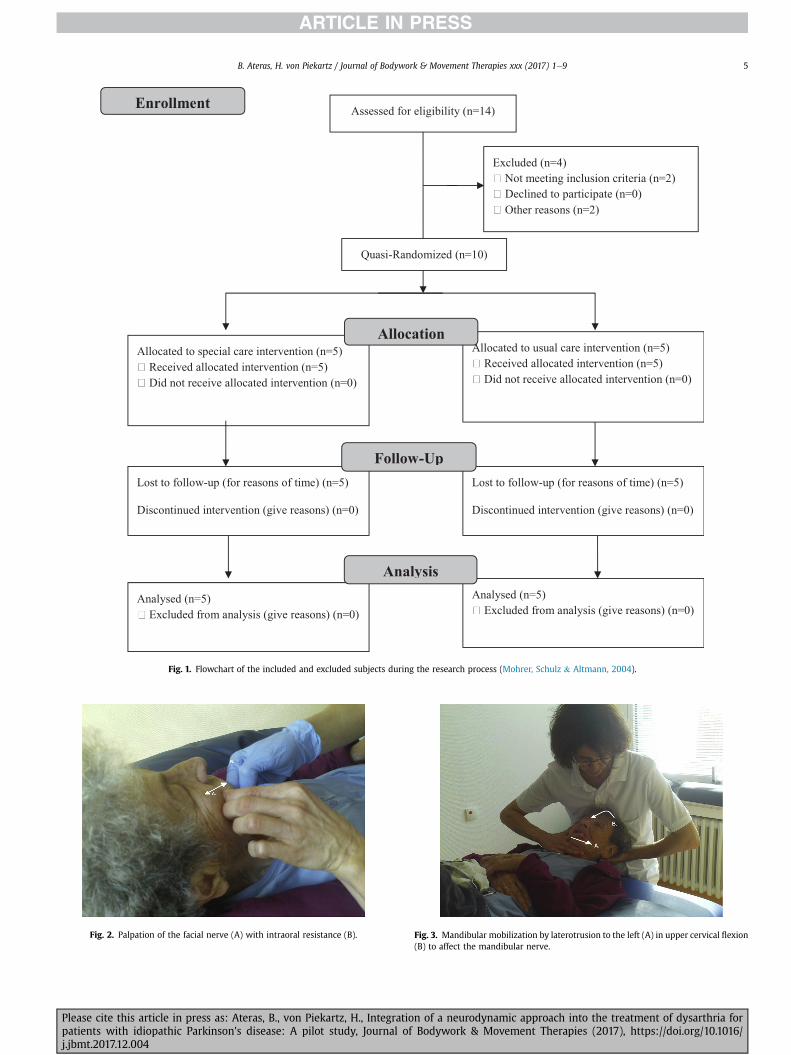
Fig. 1. Flowchart of the included and excluded subjects during the research process (Mohrer, Schulz & Altmann, 2004).
Fig. 2. Palpation of the facial nerve (A) with intraoral resistance (B). Fig. 3. Mandibular mobilization by laterotrusion to the left (A) in upper cervical flexion(B) to affect the mandibular nerve.
B. Ateras, H. von Piekartz / Journal of Bodywork & Movement Therapies xxx (2017) 1e9 5
Please cite this article in press as: Ateras, B., von Piekartz, H., Integration of a neurodynamic approach into the treatment of dysarthria forpatients with idiopathic Parkinson's disease: A pilot study, Journal of Bodywork & Movement Therapies (2017), https://doi.org/10.1016/j.jbmt.2017.12.004
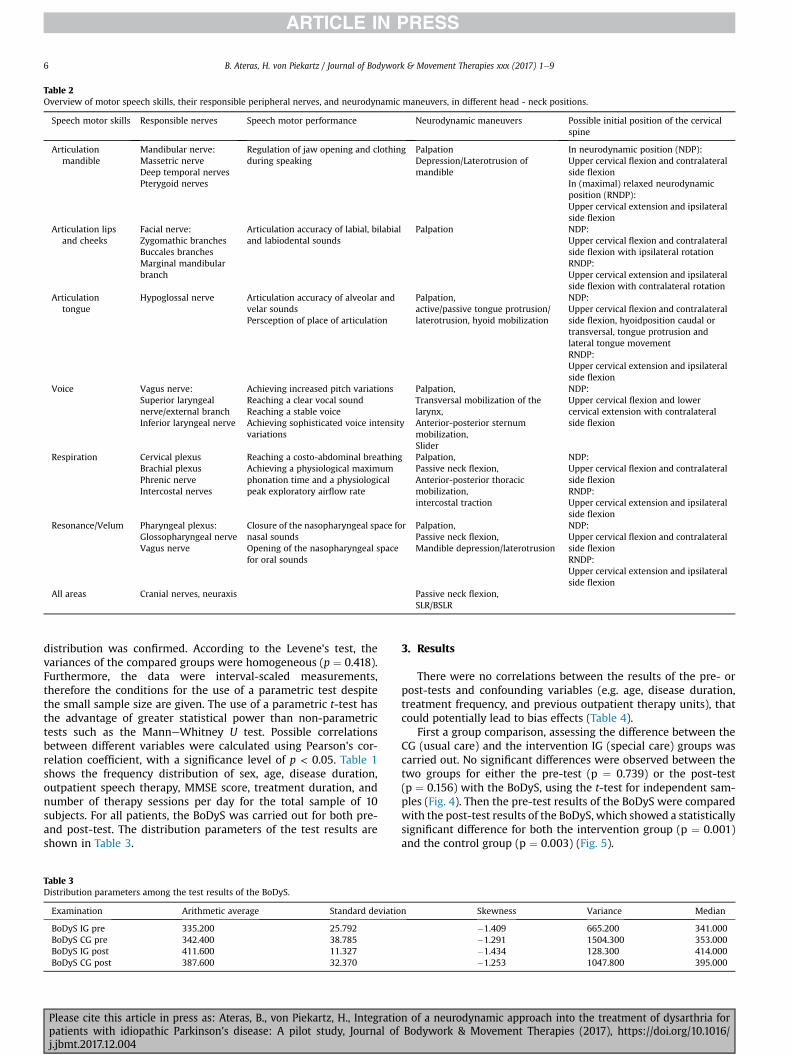
Table 2Overview of motor speech skills, their responsible peripheral nerves, and neurodynamic maneuvers, in different head - neck positions.
Speech motor skills Responsible nerves Speech motor performance Neurodynamic maneuvers Possible initial position of the cervicalspine
Articulationmandible
Mandibular nerve:Massetric nerveDeep temporal nervesPterygoid nerves
Regulation of jaw opening and clothingduring speaking
PalpationDepression/Laterotrusion ofmandible
In neurodynamic position (NDP):Upper cervical flexion and contralateralside flexionIn (maximal) relaxed neurodynamicposition (RNDP):Upper cervical extension and ipsilateralside flexion
Articulation lipsand cheeks
Facial nerve:Zygomathic branchesBuccales branchesMarginal mandibularbranch
Articulation accuracy of labial, bilabialand labiodental sounds
Palpation NDP:Upper cervical flexion and contralateralside flexion with ipsilateral rotationRNDP:Upper cervical extension and ipsilateralside flexion with contralateral rotation
Articulationtongue
Hypoglossal nerve Articulation accuracy of alveolar andvelar soundsPersception of place of articulation
Palpation,active/passive tongue protrusion/laterotrusion, hyoid mobilization
NDP:Upper cervical flexion and contralateralside flexion, hyoidposition caudal ortransversal, tongue protrusion andlateral tongue movementRNDP:Upper cervical extension and ipsilateralside flexion
Voice Vagus nerve:Superior laryngealnerve/external branchInferior laryngeal nerve
Achieving increased pitch variationsReaching a clear vocal soundReaching a stable voiceAchieving sophisticated voice intensityvariations
Palpation,Transversal mobilization of thelarynx,Anterior-posterior sternummobilization,Slider
NDP:Upper cervical flexion and lowercervical extension with contralateralside flexion
Respiration Cervical plexusBrachial plexusPhrenic nerveIntercostal nerves
Reaching a costo-abdominal breathingAchieving a physiological maximumphonation time and a physiologicalpeak exploratory airflow rate
Palpation,Passive neck flexion,Anterior-posterior thoracicmobilization,intercostal traction
NDP:Upper cervical flexion and contralateralside flexionRNDP:Upper cervical extension and ipsilateralside flexion
Resonance/Velum Pharyngeal plexus:Glossopharyngeal nerveVagus nerve
Closure of the nasopharyngeal space fornasal soundsOpening of the nasopharyngeal spacefor oral sounds
Palpation,Passive neck flexion,Mandible depression/laterotrusion
NDP:Upper cervical flexion and contralateralside flexionRNDP:Upper cervical extension and ipsilateralside flexion
All areas Cranial nerves, neuraxis Passive neck flexion,SLR/BSLR
B. Ateras, H. von Piekartz / Journal of Bodywork & Movement Therapies xxx (2017) 1e96
distribution was confirmed. According to the Levene's test, thevariances of the compared groups were homogeneous (p ¼ 0.418).Furthermore, the data were interval-scaled measurements,therefore the conditions for the use of a parametric test despitethe small sample size are given. The use of a parametric t-test hasthe advantage of greater statistical power than non-parametrictests such as the ManneWhitney U test. Possible correlationsbetween different variables were calculated using Pearson's cor-relation coefficient, with a significance level of p < 0.05. Table 1shows the frequency distribution of sex, age, disease duration,outpatient speech therapy, MMSE score, treatment duration, andnumber of therapy sessions per day for the total sample of 10subjects. For all patients, the BoDyS was carried out for both pre-and post-test. The distribution parameters of the test results areshown in Table 3.
Table 3Distribution parameters among the test results of the BoDyS.
Examination Arithmetic average Standard deviatio
BoDyS IG pre 335.200 25.792BoDyS CG pre 342.400 38.785BoDyS IG post 411.600 11.327BoDyS CG post 387.600 32.370
Please cite this article in press as: Ateras, B., von Piekartz, H., Integratiopatients with idiopathic Parkinson's disease: A pilot study, Journal ofj.jbmt.2017.12.004
3. Results
There were no correlations between the results of the pre- orpost-tests and confounding variables (e.g. age, disease duration,treatment frequency, and previous outpatient therapy units), thatcould potentially lead to bias effects (Table 4).
First a group comparison, assessing the difference between theCG (usual care) and the intervention IG (special care) groups wascarried out. No significant differences were observed between thetwo groups for either the pre-test (p ¼ 0.739) or the post-test(p ¼ 0.156) with the BoDyS, using the t-test for independent sam-ples (Fig. 4). Then the pre-test results of the BoDyS were comparedwith the post-test results of the BoDyS, which showed a statisticallysignificant difference for both the intervention group (p ¼ 0.001)and the control group (p ¼ 0.003) (Fig. 5).
n Skewness Variance Median
�1.409 665.200 341.000�1.291 1504.300 353.000�1.434 128.300 414.000�1.253 1047.800 395.000
n of a neurodynamic approach into the treatment of dysarthria forBodywork & Movement Therapies (2017), https://doi.org/10.1016/
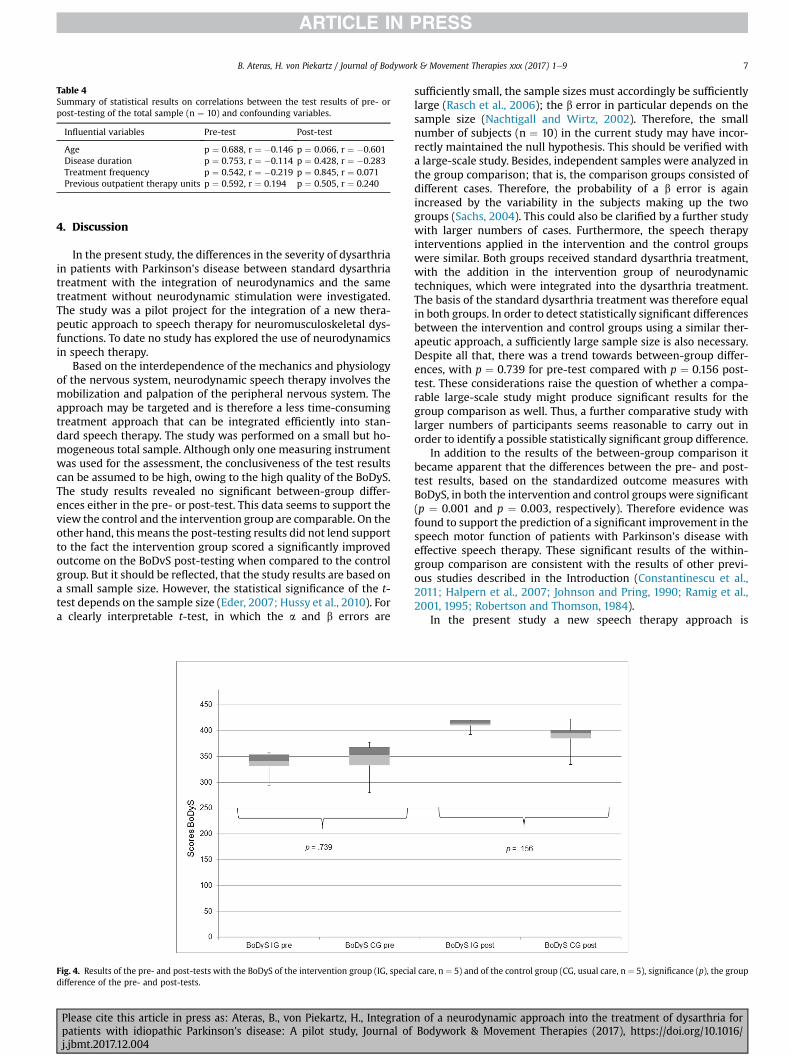
Table 4Summary of statistical results on correlations between the test results of pre- orpost-testing of the total sample (n ¼ 10) and confounding variables.
Influential variables Pre-test Post-test
Age p ¼ 0.688, r ¼ �0.146 p ¼ 0.066, r ¼ �0.601Disease duration p ¼ 0.753, r ¼ �0.114 p ¼ 0.428, r ¼ �0.283Treatment frequency p ¼ 0.542, r ¼ �0.219 p ¼ 0.845, r ¼ 0.071Previous outpatient therapy units p ¼ 0.592, r ¼ 0.194 p ¼ 0.505, r ¼ 0.240
B. Ateras, H. von Piekartz / Journal of Bodywork & Movement Therapies xxx (2017) 1e9 7
4. Discussion
In the present study, the differences in the severity of dysarthriain patients with Parkinson's disease between standard dysarthriatreatment with the integration of neurodynamics and the sametreatment without neurodynamic stimulation were investigated.The study was a pilot project for the integration of a new thera-peutic approach to speech therapy for neuromusculoskeletal dys-functions. To date no study has explored the use of neurodynamicsin speech therapy.
Based on the interdependence of the mechanics and physiologyof the nervous system, neurodynamic speech therapy involves themobilization and palpation of the peripheral nervous system. Theapproach may be targeted and is therefore a less time-consumingtreatment approach that can be integrated efficiently into stan-dard speech therapy. The study was performed on a small but ho-mogeneous total sample. Although only one measuring instrumentwas used for the assessment, the conclusiveness of the test resultscan be assumed to be high, owing to the high quality of the BoDyS.The study results revealed no significant between-group differ-ences either in the pre- or post-test. This data seems to support theview the control and the intervention group are comparable. On theother hand, this means the post-testing results did not lend supportto the fact the intervention group scored a significantly improvedoutcome on the BoDvS post-testing when compared to the controlgroup. But it should be reflected, that the study results are based ona small sample size. However, the statistical significance of the t-test depends on the sample size (Eder, 2007; Hussy et al., 2010). Fora clearly interpretable t-test, in which the a and b errors are
Fig. 4. Results of the pre- and post-tests with the BoDyS of the intervention group (IG, speciadifference of the pre- and post-tests.
Please cite this article in press as: Ateras, B., von Piekartz, H., Integratiopatients with idiopathic Parkinson's disease: A pilot study, Journal ofj.jbmt.2017.12.004
sufficiently small, the sample sizes must accordingly be sufficientlylarge (Rasch et al., 2006); the b error in particular depends on thesample size (Nachtigall and Wirtz, 2002). Therefore, the smallnumber of subjects (n ¼ 10) in the current study may have incor-rectly maintained the null hypothesis. This should be verified witha large-scale study. Besides, independent samples were analyzed inthe group comparison; that is, the comparison groups consisted ofdifferent cases. Therefore, the probability of a b error is againincreased by the variability in the subjects making up the twogroups (Sachs, 2004). This could also be clarified by a further studywith larger numbers of cases. Furthermore, the speech therapyinterventions applied in the intervention and the control groupswere similar. Both groups received standard dysarthria treatment,with the addition in the intervention group of neurodynamictechniques, which were integrated into the dysarthria treatment.The basis of the standard dysarthria treatment was therefore equalin both groups. In order to detect statistically significant differencesbetween the intervention and control groups using a similar ther-apeutic approach, a sufficiently large sample size is also necessary.Despite all that, there was a trend towards between-group differ-ences, with p ¼ 0.739 for pre-test compared with p ¼ 0.156 post-test. These considerations raise the question of whether a compa-rable large-scale study might produce significant results for thegroup comparison as well. Thus, a further comparative study withlarger numbers of participants seems reasonable to carry out inorder to identify a possible statistically significant group difference.
In addition to the results of the between-group comparison itbecame apparent that the differences between the pre- and post-test results, based on the standardized outcome measures withBoDyS, in both the intervention and control groups were significant(p ¼ 0.001 and p ¼ 0.003, respectively). Therefore evidence wasfound to support the prediction of a significant improvement in thespeech motor function of patients with Parkinson's disease witheffective speech therapy. These significant results of the within-group comparison are consistent with the results of other previ-ous studies described in the Introduction (Constantinescu et al.,2011; Halpern et al., 2007; Johnson and Pring, 1990; Ramig et al.,2001, 1995; Robertson and Thomson, 1984).
In the present study a new speech therapy approach is
l care, n ¼ 5) and of the control group (CG, usual care, n ¼ 5), significance (p), the group
n of a neurodynamic approach into the treatment of dysarthria forBodywork & Movement Therapies (2017), https://doi.org/10.1016/
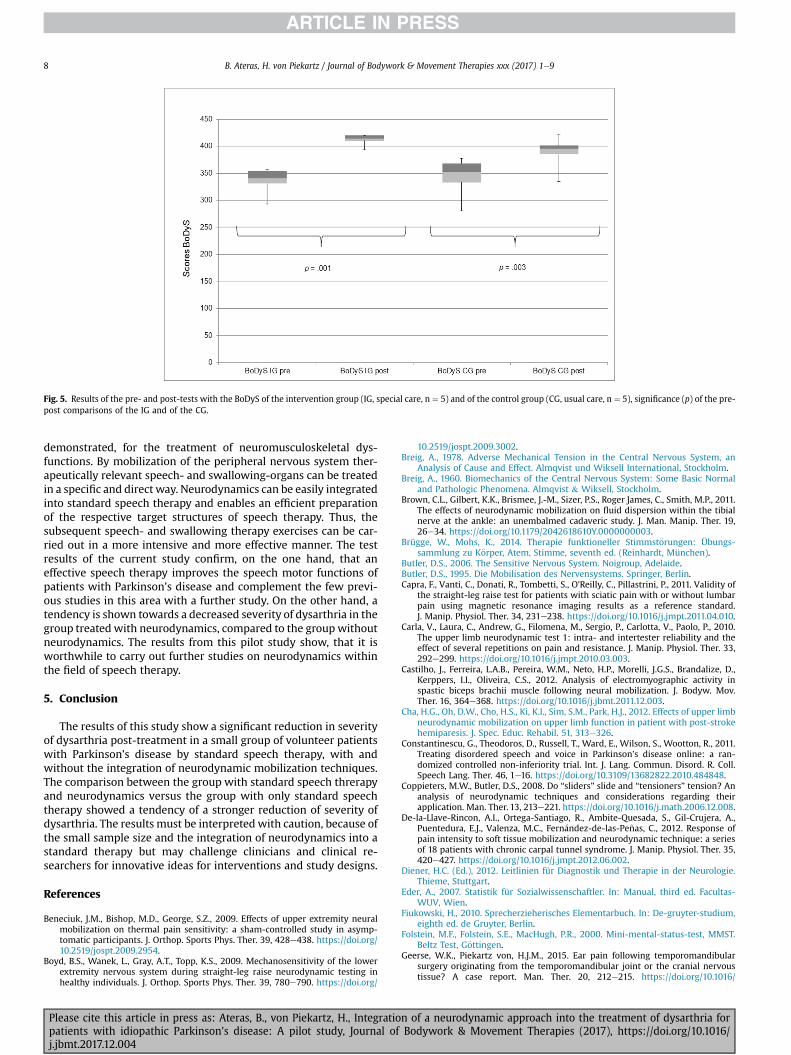
Fig. 5. Results of the pre- and post-tests with the BoDyS of the intervention group (IG, special care, n ¼ 5) and of the control group (CG, usual care, n ¼ 5), significance (p) of the pre-post comparisons of the IG and of the CG.
B. Ateras, H. von Piekartz / Journal of Bodywork & Movement Therapies xxx (2017) 1e98
demonstrated, for the treatment of neuromusculoskeletal dys-functions. By mobilization of the peripheral nervous system ther-apeutically relevant speech- and swallowing-organs can be treatedin a specific and direct way. Neurodynamics can be easily integratedinto standard speech therapy and enables an efficient preparationof the respective target structures of speech therapy. Thus, thesubsequent speech- and swallowing therapy exercises can be car-ried out in a more intensive and more effective manner. The testresults of the current study confirm, on the one hand, that aneffective speech therapy improves the speech motor functions ofpatients with Parkinson's disease and complement the few previ-ous studies in this area with a further study. On the other hand, atendency is shown towards a decreased severity of dysarthria in thegroup treated with neurodynamics, compared to the group withoutneurodynamics. The results from this pilot study show, that it isworthwhile to carry out further studies on neurodynamics withinthe field of speech therapy.
5. Conclusion
The results of this study show a significant reduction in severityof dysarthria post-treatment in a small group of volunteer patientswith Parkinson's disease by standard speech therapy, with andwithout the integration of neurodynamic mobilization techniques.The comparison between the group with standard speech threrapyand neurodynamics versus the group with only standard speechtherapy showed a tendency of a stronger reduction of severity ofdysarthria. The results must be interpreted with caution, because ofthe small sample size and the integration of neurodynamics into astandard therapy but may challenge clinicians and clinical re-searchers for innovative ideas for interventions and study designs.
References
Beneciuk, J.M., Bishop, M.D., George, S.Z., 2009. Effects of upper extremity neuralmobilization on thermal pain sensitivity: a sham-controlled study in asymp-tomatic participants. J. Orthop. Sports Phys. Ther. 39, 428e438. https://doi.org/10.2519/jospt.2009.2954.
Boyd, B.S., Wanek, L., Gray, A.T., Topp, K.S., 2009. Mechanosensitivity of the lowerextremity nervous system during straight-leg raise neurodynamic testing inhealthy individuals. J. Orthop. Sports Phys. Ther. 39, 780e790. https://doi.org/
Please cite this article in press as: Ateras, B., von Piekartz, H., Integratiopatients with idiopathic Parkinson's disease: A pilot study, Journal ofj.jbmt.2017.12.004
10.2519/jospt.2009.3002.Breig, A., 1978. Adverse Mechanical Tension in the Central Nervous System, an
Analysis of Cause and Effect. Almqvist und Wiksell International, Stockholm.Breig, A., 1960. Biomechanics of the Central Nervous System: Some Basic Normal
and Pathologic Phenomena. Almqvist & Wiksell, Stockholm.Brown, C.L., Gilbert, K.K., Brismee, J.-M., Sizer, P.S., Roger James, C., Smith, M.P., 2011.
The effects of neurodynamic mobilization on fluid dispersion within the tibialnerve at the ankle: an unembalmed cadaveric study. J. Man. Manip. Ther. 19,26e34. https://doi.org/10.1179/2042618610Y.0000000003.
Brügge, W., Mohs, K., 2014. Therapie funktioneller Stimmst€orungen: Übungs-sammlung zu K€orper, Atem, Stimme, seventh ed. (Reinhardt, München).
Butler, D.S., 2006. The Sensitive Nervous System. Noigroup, Adelaide.Butler, D.S., 1995. Die Mobilisation des Nervensystems. Springer, Berlin.Capra, F., Vanti, C., Donati, R., Tombetti, S., O'Reilly, C., Pillastrini, P., 2011. Validity of
the straight-leg raise test for patients with sciatic pain with or without lumbarpain using magnetic resonance imaging results as a reference standard.J. Manip. Physiol. Ther. 34, 231e238. https://doi.org/10.1016/j.jmpt.2011.04.010.
Carla, V., Laura, C., Andrew, G., Filomena, M., Sergio, P., Carlotta, V., Paolo, P., 2010.The upper limb neurodynamic test 1: intra- and intertester reliability and theeffect of several repetitions on pain and resistance. J. Manip. Physiol. Ther. 33,292e299. https://doi.org/10.1016/j.jmpt.2010.03.003.
Castilho, J., Ferreira, L.A.B., Pereira, W.M., Neto, H.P., Morelli, J.G.S., Brandalize, D.,Kerppers, I.I., Oliveira, C.S., 2012. Analysis of electromyographic activity inspastic biceps brachii muscle following neural mobilization. J. Bodyw. Mov.Ther. 16, 364e368. https://doi.org/10.1016/j.jbmt.2011.12.003.
Cha, H.G., Oh, D.W., Cho, H.S., Ki, K.I., Sim, S.M., Park, H.J., 2012. Effects of upper limbneurodynamic mobilization on upper limb function in patient with post-strokehemiparesis. J. Spec. Educ. Rehabil. 51, 313e326.
Constantinescu, G., Theodoros, D., Russell, T., Ward, E., Wilson, S., Wootton, R., 2011.Treating disordered speech and voice in Parkinson's disease online: a ran-domized controlled non-inferiority trial. Int. J. Lang. Commun. Disord. R. Coll.Speech Lang. Ther. 46, 1e16. https://doi.org/10.3109/13682822.2010.484848.
Coppieters, M.W., Butler, D.S., 2008. Do “sliders” slide and “tensioners” tension? Ananalysis of neurodynamic techniques and considerations regarding theirapplication. Man. Ther. 13, 213e221. https://doi.org/10.1016/j.math.2006.12.008.
De-la-Llave-Rincon, A.I., Ortega-Santiago, R., Ambite-Quesada, S., Gil-Crujera, A.,Puentedura, E.J., Valenza, M.C., Fern�andez-de-las-Pe~nas, C., 2012. Response ofpain intensity to soft tissue mobilization and neurodynamic technique: a seriesof 18 patients with chronic carpal tunnel syndrome. J. Manip. Physiol. Ther. 35,420e427. https://doi.org/10.1016/j.jmpt.2012.06.002.
Diener, H.C. (Ed.), 2012. Leitlinien für Diagnostik und Therapie in der Neurologie.Thieme, Stuttgart.
Eder, A., 2007. Statistik für Sozialwissenschaftler. In: Manual, third ed. Facultas-WUV, Wien.
Fiukowski, H., 2010. Sprecherzieherisches Elementarbuch. In: De-gruyter-studium,eighth ed. de Gruyter, Berlin.
Folstein, M.F., Folstein, S.E., MacHugh, P.R., 2000. Mini-mental-status-test, MMST.Beltz Test, G€ottingen.
Geerse, W.K., Piekartz von, H.J.M., 2015. Ear pain following temporomandibularsurgery originating from the temporomandibular joint or the cranial nervoustissue? A case report. Man. Ther. 20, 212e215. https://doi.org/10.1016/
n of a neurodynamic approach into the treatment of dysarthria forBodywork & Movement Therapies (2017), https://doi.org/10.1016/
B. Ateras, H. von Piekartz / Journal of Bodywork & Movement Therapies xxx (2017) 1e9 9
j.math.2014.05.006.Godoi, J., Kerppers, I.I., Rossi, L.P., Correa, F.I., Costa, R.V., Correa, J.C.F., Oliveira, C.S.,
2010. Electromyographic analysis of biceps brachii muscle following neuralmobilization in patients with stroke. Electromyogr. Clin. Neurophysiol. 50,55e60.
Halpern, A., Spielman, J., Ramig, L., Cable, J., Panzer, I., Sharpley, A., 2007. The effectsof loudness and noise on speech intelligibility in Parkinson's disease. Mov.Disord. 22, 105. https://doi.org/10.1002/mds.21535.
Healy, V., 2002. A Comparison of the Efficacy of Two Methods of Rate Control in theSpeech of People with Parkinson’s Disease. Internal report. Manchester RoyalInfirmary.
Heebner, M.L., Roddey, T.S., 2008. The effects of neural mobilization in addition tostandard care in persons with carpal tunnel syndrome from a communityhospital. J. Hand Ther. Off. J. Am. Soc. Hand Ther. 21, 229e240. https://doi.org/10.1197/j.jht.2007.12.001.
Herd, C.P., Tomlinson, C.L., Deane, K.H., Brady, M.C., Smith, C.H., Sackley, C.M.,Clarke, C.E., 2012a. Speech and language therapy versus placebo or no inter-vention for speech problems in Parkinson's disease. Cochrane Database Syst.Rev. https://doi.org/10.1002/14651858.CD002812.pub2.
Herd, C.P., Tomlinson, C.L., Deane, K.H.O., Brady, M.C., Smith, C.H., Sackley, C.,Clarke, C.E., 2012b. Speech and Language Therapy versus Placebo or No Inter-vention for Speech Problems in Parkinson's Disease (Review). https://doi.org/10.1002/14651858.CD002812.
Hussy, W., Schreier, M., Echterhoff, G., 2010. Forschungsmethoden in Psychologieund Sozialwissenschaften. Springer, Berlin.
Jeangros, P., 2011. T 4-Syndrom. In: Westerhuis, W. (Ed.), Klinische Muster in DerManuellen Therapie. Thieme, Stuttgart, pp. 353e381.
Johnson, J.A., Pring, T.R., 1990. Speech therapy and Parkinson's disease: a review andfurther data. Int. J. Lang. Commun. Disord. 25, 183e194. https://doi.org/10.3109/13682829009011973.
Larsen, R., Ziegenfuß, T., 2012. Beatmung. In: Indikationen, Techniken, Krank-heitsbilder, fifth ed. Springer, Berlin.
Lohkamp, M., Small, K., 2011. Normal response to upper limb neurodynamic test 1and 2A. Man. Ther. 16, 125e130. https://doi.org/10.1016/j.math.2010.07.008.
Lowit, A., Dobinson, C., Timmins, C., Howell, P., Kr€oger, B., 2010. The effectiveness oftraditional methods and altered auditory feedback in improving speech rateand intelligibility in speakers with Parkinson's disease. Int. J. Speech Lang.Pathol. 12, 426e436. https://doi.org/10.3109/17549507.2010.497559.
Maitland, G.D., 2004. In: Manipulation der peripheren Gelenke, third ed. Springer,Berlin.
Majlesi, J., Togay, H., Unalan, H., Toprak, S., 2008. The sensitivity and specificity ofthe Slump and the Straight Leg Raising tests in patients with lumbar discherniation. J. Clin. Rheumatol. Pract. Rep. Rheum. Musculoskelet. Dis. 14, 87e91.https://doi.org/10.1097/RHU.0b013e31816b2f99.
Moher, D., Schulz, K., Altman, D., 2004. Das CONSORT Statement: ÜberarbeiteteEmpfehlungen zur Qualit€atsverbesserung von Reports randomisierter Studienim Parallel-Design. Dtsch. Med. Wochenschr. 129, T16eT20.
Nachtigall, C., Wirtz, M.A., 2002. Statistische Methoden für Psychologen. In:Juventa-paperback, second ed. Juventa Verlag, Weinheim.
Nee, R.J., Butler, D., 2006. Management of peripheral neuropathic pain: integratingneurobiology, neurodynamics, and clinical evidence. Phys. Ther. Sport 7, 36e49.https://doi.org/10.1016/j.ptsp.2005.10.002.
Nee, R.J., Vicenzino, B., Jull, G.A., Cleland, J.A., Coppieters, M.W., 2013. Baselinecharacteristics of patients with nerve-related neck and arm pain predict thelikely response to neural tissue management. J. Orthop. Sports Phys. Ther. 43,379e391. https://doi.org/10.2519/jospt.2013.4490.
Nee, R.J., Yang, C.-H., Liang, C.-C., Tseng, G.-F., Coppieters, M.W., 2010. Impact oforder of movement on nerve strain and longitudinal excursion:A biomechanicalstudy with implications for neurodynamic test sequencing. Man. Ther. 15,376e381. https://doi.org/10.1016/j.math.2010.03.001.
Nicola, F., Ziegler, W., Vogel, M., 2004. Die Bogenhausener Dysarthrieskalne(BODYS): Ein Instrument für die Klinische Dysarthriediagnostik. Forum Log-op€adie 18, 14e22.
Oskay, D., Meriç, A., Kirdi, N., Firat, T., Ayhan, Ç., Leblebicio�glu, G., 2010. Neuro-dynamic mobilization in the conservative treatment of cubital tunnel syn-drome: long-term follow-up of 7 cases. J. Manip. Physiol. Ther. 33, 156e163.https://doi.org/10.1016/j.jmpt.2009.12.001.
Piekartz von, H. (Ed.), 2007. Craniofacial Pain: Guidelines for a Neuro-orthopaedicApproach. Butterworth-Heinemann, Edinburgh.
Piekartz, H.J.M. von, 2015. Kiefer, Gesichts- und Zervikalregion: neuro-muskuloskeletales Assessment und Behandlungsstrategien, 2., überarbeite underweiterte Auflage. ed, physiofachbuch. Georg Thieme Verlag, Stuttgart NewYork.
Piekartz von, H.J.M., 2011. Dysregulationen des autonomen Nervensystems. In:
Please cite this article in press as: Ateras, B., von Piekartz, H., Integratiopatients with idiopathic Parkinson's disease: A pilot study, Journal ofj.jbmt.2017.12.004
Westerhuis, P., Wienser, R. (Eds.), Klinische Muster in Der Manuellen Therapie.IMTA-kurshandbuch Level 2a Und B. Thieme, Stuttgart, pp. 221e237.
Rabin, A., Gerszten, P.C., Karausky, P., Bunker, C.H., Potter, D.M., Welch, W.C., 2007.The sensitivity of the seated straight-leg raise test compared with the supinestraight-leg raise test in patients presenting with magnetic resonance imagingevidence of lumbar nerve root compression. Arch. Phys. Med. Rehabil. 88,840e843. https://doi.org/10.1016/j.apmr.2007.04.016.
Ramig, L.O., Countryman, S., Thompson, L.L., Horii, Y., 1995. Comparison of twoforms of intensive speech treatment for Parkinson disease. J. Speech Lang. Hear.Res. 38, 1232. https://doi.org/10.1044/jshr.3806.1232.
Ramig, L.O., Sapir, S., Fox, C., Countryman, S., 2001. Changes in vocal loudnessfollowing intensive voice treatment (LSVT®) in individuals with Parkinson'sdisease: a comparison with untreated patients and normal age-matched con-trols. Mov. Disord. 16, 79e83. https://doi.org/10.1002/1531-8257(200101)16,1<79::AID-MDS1013>3.0.CO;2-H.
Rasch, B., Friese, M., Hofmann, W., Naumann, E., 2006. Quantitative methoden. In:Springer-lehrbuch, second ed. Springer, Berlin.
Robertson, S.J., Thomson, F., 2000. In: Therapie mit Dysarthrikern, second ed. Urban& Fischer, München.
Robertson, S.J., Thomson, F., 1984. Speech therapy in Parkinson's disease: a study ofthe efficacy ad long term effects of intensive treatment. Br. J. Disord. Commun.19, 213e224.
Rolf, G., 2006. Schmerzpuzzle - Verlust der Beweglichkeit, Ausweichbewegungenund Selbstmanagement. manuelletherapie 10, 211e224. https://doi.org/10.1055/s-2006-927244.
Sachs, L., 2004. In: Angewandte Statistik: Anwendung Statistischer Methoden,eleventh ed. Springer, Berlin.
Schulte, E., Schumacher, U., Schünke, M., Voll, M., Wesker, K., 2007. AllgemeineAnatomie und Bewegungssystem. In: 182 Tabellen, second ed. Thieme, Stuttgart[u.a.].
Schulz, K.F., Altman, D.G., Moher, D., 2011. CONSORT 2010: aktualisierte Leitlinie fürBerichte randomisierter Studien im Parallelgruppen-Design. DMW - Dtsch.Med. Wochenschr 136, e20ee23. https://doi.org/10.1055/s-0031-1272980.
Scott, S., Caird, F.I., 1983. Speech therapy for Parkinson's disease. J. Neurol. Neuro-surg. Psychiatry 46, 140e144.
Shacklock, M.O., 2008. Angewandte Neurodynamik. In: NeuromuskuloskeletaleStrukturen verstehen und behandeln, first ed. Elsevier Urban & Fischer,München.
Trampisch, H.J., Windeler, J. (Eds.), 2000. Medizinische Statistik, second ed.Springer, Berlin.
Vanti, C., Bonfiglioli, R., Calabrese, M., Marinelli, F., Guccione, A., Violante, F.S.,Pillastrini, P., 2011. Upper limb neurodynamic test 1 and symptoms reproduc-tion in carpal tunnel syndrome. A validity study. Man. Ther. 16, 258e263.https://doi.org/10.1016/j.math.2010.11.003.
Villafa~ne, J.H., Fernandez-de-las-Pe~nas, C., Pillastrini, P., 2012. Botulinum toxin typeA combined with cervical spine manual therapy for masseteric hypertrophy in apatient with Alzheimer-type dementia: a case report. J. Chiropr. Med. 11,280e285. https://doi.org/10.1016/j.jcm.2012.10.004.
Villafa~ne, J.H., Silva, G.B., Fernandez-Carnero, J., 2011. Short-term effects of neuro-dynamic mobilization in 15 patients with secondary thumb carpometacarpalosteoarthritis. J. Manip. Physiol. Ther. 34, 449e456. https://doi.org/10.1016/j.jmpt.2011.05.016.
Walsh, J., Hall, T., 2009. Reliability, validity and diagnostic accuracy of palpation ofthe sciatic, tibial and common peroneal nerves in the examination of low backrelated leg pain. Man. Ther. 14, 623e629. https://doi.org/10.1016/j.math.2008.12.007.
Wendler, J., Seidner, W., Eysholdt, U., Appel, H., 2005. In: Lehrbuch der Phoniatrieund P€adaudiologie, fourth ed. Thieme, Stuttgart.
Wolny, T., Saulicz, E., Gnat, R., Kokosz, M., 2010. Butler's neuromobilizations com-bined with proprioceptive neuromuscular facilitation are effective in reducingof upper limb sensory in late-stage stroke subjects: a three-group randomizedtrial. Clin. Rehabil. 24, 810e821. https://doi.org/10.1177/0269215510367561.
World Medical Association, 2013. Declaration of Helsinki - Ethical principles formedical research involving human subjects. http://www.wma.net/en/30publications/10policies/b3/index.html.
Ziegler, W., 2006. Sprechapraxie und Dysarthrie. In: Br€otz, D., Karnath, H.-O. (Eds.),Kognitive Neurologie. Thieme, Stuttgart, pp. 72e83.
Ziegler, W., Sch€olderle, T., Staiger, A., Vogel, M., 2015. Die Bogenhausener Dysar-thrieskalen (BoDyS): Ein standardisierter Test für die Dysarthriediagnostik beiErwachsenen. Sprache $ Stimme $ Geh€or 39, 171e175. https://doi.org/10.1055/s-0041-102792.
Ziegler, W., Vogel, M., 2010. Dysarthrie. In: Verstehen - Untersuchen - Behandeln,first ed. Thieme, Stuttgart.
n of a neurodynamic approach into the treatment of dysarthria forBodywork & Movement Therapies (2017), https://doi.org/10.1016/