join the centerwatch community centerwatch · see parkinson’s clinical trials on page 5 » see...
TRANSCRIPT

Volume 22, Issue 40. © 2018 CenterWatch. All rights reserved.
Join the CenterWatch Community!
see Parkinson’s Clinical Trials on page 5 »
see Cancer Trials on page 4 »
Learn about best practicesto e�ectively manage andexecute clinical trials with the Research Practitioner.
» Earn ANCC contact hours» Maintain nursing certi�cation» Subscriptions at $197
DOWNLOAD A SAMPLE
Caution for NIH's single IRB policy for multi-site researchBy Sue Coons, MA
A tions had to comply with the National Institutes of Health’s (NIH’s) Final
NIH Policy on the Use of a Single Institutional Review Board for Multi-Site Researchpolicy established the expectation that a single institutional review board (sIRB) of record would be used in the ethical review of non-exempt human subjects research protocols funded by NIH that are carried out at more than one site in the United States.
It does not apply to career development, research training, or fellowship awards.
However, some institutions continue to be concerned about their ability to adhere to the policy and the cost of doing so. IRB executives say it is wise to be cautious. Some institutions could spend millions of dollars to upgrade their IRB infrastructure, while some IRBs already have many of the policy requirements in place. In addition, one IRB executive worries that past NIH actions
show that the agency could revise its policy
Emerging trends in clinical research: The need for changeBy John W. Mitchell, MS
T by emerging trends in the clinical trial research sector, consider insight from
a business author and a businessman/politi-cian. In his groundbreaking book, Good to Great: Why Some Companies Make the Leap…And Others Don’t,” Jim Collins wrote:
“Good is the enemy of great. And that is one of the key reasons why we have so little that becomes great. We don’t have great schools, principally because we have good schools. We don’t have great government, principally because we have good govern-ment.”
Secretary Donald Rumsfeld noted that one of the biggest threats to security was driven by factors that fell under the category of “we
don’t know what we don’t know.” In recent issues, Research Practitioner has
explored individual key emerging trends in clinical research, including patient centricity, eMobile advances, and precision medicine. As stand-alone trends, these innovations hold great promise and excitement.
But what insight is gained when all emerg-ing trends are considered in totality? What
clinical research? As Rumsfeld alluded, what might we not know that we don’t know? Are current advancements in clinical research, as Collins asserted, relevant enough to power (great) the sector beyond the status quo (good), given the rapidly evolving medical
ligence (AI), and the expectation of patients?
results on the use of electronic-sourced data, Hugo Stephenson, executive chairman of DrugDev and a physician investigator, observed: “I’m surprised and disappointed there hasn’t been much improvement in the entire clinical trial process, including the
© 2018 CenterWatch. Duplication or sharing of this publication is strictly prohibited. Volume 19, Number 3
Learning Objectives/Outcomes:1. Explain the need for change in clinical research.
2. List key drivers of transformation in clinical trials.
3. Describe examples of clinical trial research trends in action.
4. Discuss why the clinical trial sector will make the jump from trends to practice.
Learning Objectives/Outcomes:1. List the details that local IRBs may know about their
study populations as opposed to a single IRB.2. Describe NIH’s reasoning for going to a single IRB
policy for multi-site research.3. Discuss the impact of using a single IRB on a study’s
direct costs.4. Explain the concern about NIH’s history of choosing
the lowest-cost provider.
42 CE program information
43 Issues in research management
52 SMART IRB
55 CE post-test
May–June 2018
see Emerging trends on page 44
see Single IRB on page 49
o understand the opportunity o�ered
In a 2002 Department of Defense brie�ng,
do these opportunities say about the �eld of
reality of interconnectivity, arti�cial intel-
�ese seem to be fair questions. In a Feb-ruary 2017 CenterWatch article about survey
s of Jan. 25, 2018, research institu-
�is
Available in the CenterWatch Shop
Order Today!
Clinical Research Manual from EuromedCommunications translates regulations and bestpractices into real-world guidance.
Both new and experienced trial managers will �nd the information they need to set up and run every phase of a clinical research program.
practices into real-world guidance.
Both new and experienced trial managers will �nd the information they need to set up and run every phase of a clinical research program.
ClinicalResearchManual
Editors
David K LuscombePeter D Stonier
7th Edition
CLINICAL TRIAL RISKAND PERFORMANCE
MANAGEMENT SUMMITWEDNESDAY–THURSDAYNOVEMBER 14–15, 2018
PRINCETON, NJ
REG ISTE R NOW
A Metrics Champion Consortium/CenterWatch Event
October 8, 2018
Industry Briefs…2
Drug & Device Pipeline News…7Thirteen drugs and devices have entered a new trial phase this week.
Research Center Spotlight…8 Research center profiles.
CenterWatchWeekly
By Bill Myers
A Florida scientist is urging sponsors and care providers to do a better job of getting early-stage Parkinson’s
sufferers into clinical trials before they start treatment.
Robert A. Hauser, director of the Parkin-son’s & Movement Disorder Center at the University of South Florida and author of one of the most widely used patient diaries for Parkinson’s trials, says researchers need to recruit patients at the first sign of trouble — before they start taking meds so they have time to assess experimental therapies against placebos.
The critical time to enroll patients is during their so-called Golden Year — that is, as soon as they’re diagnosed with “mild
classic motor features until they truly require symptomatic therapy,” Hauser said.
This gives both researchers and patients the best shot at coming up with a treatment that may stave off symptoms and prevent disease progression, he tells CenterWatch.
Hauser says his clinic is part of at least four early-stage Parkinson’s trials, two privately sponsored and two funded by a combination of grants from private founda-tions and the National Institutes of Health. There are about 20 participants in total in those studies but Hauser says he’s lost count of the number of patients who came to see him long after their symptoms started and it was too late to enroll them.
“My experience is a lot of patients come
Timing is Key in Parkinson’s Clinical Trials
By James Miessler
A new study questions the use of progression-free survival as a sur-rogate endpoint in cancer clinical
trials after finding it overlooks quality of life issues.
Progression-free survival (PFS) has be-come a frequent outcome used to evaluate new cancer drug efficacy.
But Canadian researchers failed to find a substantial link between PFS and health-related quality of life (HRQoL) in cancer trials, casting doubt on its role as a surrogate endpoint.
Lead investigators Sean Alexander Ken-nedy, Bruno Kovic and Xuejing Jin analyzed the results of 38 randomized oncology trials to try to pin down the connection between
patients’ length of survival and quality of life.
They evaluated trials that focused on in-travenous, oral, intraperitoneal or intrapleu-ral chemotherapy or biological treatments and reported progression-free survival or health-related quality of life.
Their findings, published in JAMA Internal Medicine, suggest PFS benefits are unrelated to improved quality-of-life scores reported by patients — and don’t always translate into an overall survival (OS) benefit, an objective endpoint representing the dura-tion of survival that’s viewed as the most important cancer trial outcome.
The report says there are only two possi-ble reasons to use progression-free survival
Cancer Trials: Is Progression-Free Survival Enough?

© 2018 CenterWatch. Duplication or sharing of this publication is strictly prohibited. CWW2240
WCG | CWWeekly (ISSN 1528-5731)
Lisa Stein Editorial DirectorBill Myers Clinical Trials SpecialistRenee Breau Production
CenterWatch Main and Editorial Offices10 Winthrop Square, Fifth Floor, Boston, MA [email protected] / [email protected]
© 2018 CenterWatch. All rights reserved. No part of this publication may be distributed or reproduced in any form or by any means without the express written consent of the publisher. Permission requests can be obtained via fax at (617) 948-5101 or emailed to [email protected]. Advertising packages and reprints are available. Email [email protected] or call (617) 948-5100.
continues on next page »
WCG | CWWeekly October 8, 2018 2 of 8
Industry Briefs
FDA Guidance: Start with Kids in Atopic Dermatitis TrialsSponsors of atopic dermatitis drugs for children don’t have to wait to test a drug’s safety or efficacy on adults before beginning pediatric trials, the FDA says.
The new guidance, released last week, reverses longstanding FDA recommenda-tions that drugs trying to treat a disease by affecting the entire body start with adult trials.
Atopic dermatitis is the dry, itchy rash caused by eczema that affects nearly 18 million Americans, most of them children. It often clusters with asthma and hay fever.
The agency says its U-turn was prompted by recommendations from a 2015 meeting of its Dermatologic and Ophthalmic Drug Advisory Committee.
The FDA acknowledges that “some major safety questions” may be left open before trials can begin.
But it says it’s “not generally necessary to have an extensive safety database in adults before initiating pediatric studies” as long as the disease isn’t potentially fatal to pediatric populations and there’s a risk doctors may be prescribing therapies off-label before trials wrap up.
Trials will have to consider a drug’s effect on children of all ages, including toddlers and infants, the guidance adds.
Sponsors may have to start with older children first if specific data from an older subpopulation can help inform the study, if there’s an “age-related technical issue” or if there is some reason to worry about a drug’s safety in younger children.
Read the final guidance here: www.fdanews.com/10-02-18-AtopicDermatitis.pdf.
Re-Trials for Pediatrics Pay OffThe FDA’s pediatric exclusivity rules allowed drugmakers to reap a 680 percent return on their investments, a new analysis finds.
The Best Pharmaceuticals for Children Act of 2002 offered drugmakers six months of market exclusivity in return for running drugs already approved for adults through clinical trials again to test their safety and efficacy for children.
Congress passed the measure because it was concerned that doctors were pre-scribing adult meds to kids off-label and the pharmaceutical industry argued that limited exclusivity provided proper incentive to invest in fresh trials.
The incentive has proved lucratice, ac-cording to the analysis published in JAMA Internal Medicine.
Study author Michael S. Sinha and his colleagues at Boston’s Brigham and Women’s Hospital examined 54 drugs given exclusivity between 2007 and 2012.
They estimate pharma companies spent an average of $36.4 million to re-test their drugs in clinical trials and the median net return was $176 million—a ratio of about 680 percent.
“Meaningful knowledge of pediatric uses of pharmaceuticals has come from the pediatric exclusivity program, but at a high cost” in hefty drug prices passed along to consumers, Sinha said, noting that “other approaches … such as direct funding” for pediatric trials “may be more economically efficient.”
Advanced Cancer Trials SetThe FDA has greenlighted clinical trials for a Chinese biotech hoping to treat non-Hodg-kin’s lymphoma, ovarian cancer and other advanced cancers.
Innovent Biologics is planning several trials on IBI-188, an anti-CD47 monoclonal antibody, which works by boosting patients’ immune systems and setting up markers on cancer cells for targeted treatments that spare surrounding healthy tissue.
There are about 14 ongoing clinical trials on these types of meds. But Innovent is the first Chinese company given the nod to test such a treatment.
In January, the FDA gave Innovent the go-ahead for clinical trials of Sintilimab, an anti-PD-1 antibody that also targets cancer.
Personalized Pain Trial Scores Big on Patient Satisfaction Scale Patients gave thumbs up to a clinical trial that provided a menu of a la carte treat-ment options even though it didn’t make a dramatic difference in managing their pain.
In what’s believe to be the largest trial of its kind, a team at the University of Califor-nia, Davis, enrolled 215 people in a single-patient multi-crossover trial to test pain management.
Often called n-of-1 trials, the single-patient, multi-crossover approach allows participants to switch between two or more therapies during the trial and allows re-searchers to gauge the effect of treatments on each individual.
Researchers randomly assigned 108 of the pain patients to personalized mini-trials in which they were given eight different treatment options, ranging from opioids to acupuncture, to try for between four to 12 weeks.
© 2018 CenterWatch. Duplication or sharing of this publication is strictly prohibited. CWW2240
continues on next page »
WCG | CWWeekly October 8, 2018 3 of 8
Industry Briefs
Participants were also given access to an open-source mobile app called Trialist, which sent reminders about beginning each treatment, daily questionnaires rating their pain, and warnings about possible side ef-fects of their selected treatments.
The remaining 107 volunteers continued using their same pre-trial treatment.
Researchers measured patients’ pain management as well as their level of satis-faction with their treatment.
Patients in the n-of-1 trials group reported slight but statistically insignificant improvement in pain symptoms but still raved about their experience. For instance, 88 percent said Trialist was “extremely or very helpful” in keeping track of their pain.
The team reported its findings in JAMA Internal Medicine, which carried a separate editorial praising the trial for its “ambition.”
ACRES: Accreditation of Trial SitesA nonprofit group has begun evaluating standards for first-of-its kind voluntary ac-creditation of clinical research sites as part of a new effort to enhance quality and speed development of new medical products worldwide.
The Alliance for Clinical Research Excellence and Safety (ACRES) is currently performing its first evaluation at research facilities owned by ActivMed, a company in Massachusetts that’s completed 720 clinical trials since it was founded in 1994.
ACRES officials believe accrediting site performance and research quality can “dramatically” shrink both the costs and time spent on clinical trials.
As part of its effort, the company is working on technology dubbed “Dynamic Accreditation” to provide real-time feedback to sites, sponsors, CROs, regulators and patients about site performance.
“The idea of site accreditation is an impor-tant one. We are sure that both our site and ACRES will learn more as we move through the beta-testing of the standards,” said Terry Stubbs, ActivMed president and CEO.
Once the pilot program wraps up, ACRES will commission an independent study to assess its impact.
Highlights include:
Succinct overview of the clinical investigational processCRO/vendor management guidelinesKey elements from ISO 14155
Guidance on risk-based monitoring and technology implementationImportant medical device development steps
�
��
�
�
�
� VISIT STORE.CENTERWATCH.COMTO ORDER store.centerwatch.com CONTACT SALES [email protected] (617) 948-5100
Medical Device GuidanceSOP for Good Clinical Practice by Sponsors of Medical Device Clinical Trials is the industry’s only medical device SOP available that re� ects best practices while addressing FDA Guidance documents and current device regulations to minimize your organization’s regulatory exposure and comply with industry standards.
© 2018 CenterWatch. Duplication or sharing of this publication is strictly prohibited. CWW2240
WCG | CWWeekly October 8, 2018 4 of 8
Features
According to current evidence, progression-free survival is too unpredictable and
inconsistent to serve as a viable surrogate for overall survival.
—Study published in JAMA Internal Medicine
as an endpoint in oncology — the belief that it’s a valid surrogate marker for overall survival and the assumption that patients who live longer without disease progres-sion — even without longer survival — will experience a higher quality of life.
But according to current evidence, progression-free survival is too unpredict-able and inconsistent to serve as a viable surrogate for overall survival.
“[PFS’] association with improved [health-related quality of life] is far from self-evident,” the study says, “because HRQoL is likely to be impaired by adverse events resulting from the treatments responsible for prolonged” progression-free survival.
Oncological experts have questioned whether it’s appropriate to use PFS to evalu-ate treatments given the uncertainties, the investigators say.
They note that progression-free survival is a frequent surrogate because shorter and
smaller trials can be used to measure it, making it more convenient.
It’s also a popular measure in FDA drug approvals.At least a dozen drugs approved by the agency over a five-year period used PFS as a primary endpoint.
Its use as a surrogate outcome has also been popular in clinical trials due to limita-tions associated with overall survival that include higher costs, larger sample sizes, longer follow-up and confounding effects that come from crossover designs and post-progression therapies.
Researchers say their findings indicate clinical trials must be “adequately powered” for overall survival and/or designed for strict and accurate quality of life measurements to meet the needs of cancer patients.
Cancer Trialscontinued from page 1
By John W Mitchell
Frustration about clinical trial start-up costs is not unlike Sisyphus’ dilemma. A host of long-standing expense and
inefficiency realities continues to create such uphill headwinds for the clinical trial sector. According to some sources, such problems even threaten the viability of the sector. Sites complain they incur more over-head costs driven by regulatory documen-tation, antiquated data collection and the demands of precision medicine to name a few — all without increased compensation from sponsors and CROs. A recent study supports this concern. Researchers at the Tufts Center for the Study of Drug Devel-opment found that the study start-up phase of five to six months for clinical trials has remained unchanged for the past decade. The study also concluded that CROs mak-ing investments in technology are getting trials done faster. None of this bodes well for smaller, independent players.
“Sites are doing more work for [fewer] patients. We used to enroll about eight pa-
tients per study 10 years ago, and today the number is less than three,” says Jeff King-sley, CEO at IACT Health. His company operates 13 locations in Georgia and a few outside the state in a network of about 100 clinical specialists. “The protocols are lon-ger, and there are more procedures per pa-tient per day. So, you’re doing loads more work, but you’re only paid when you put patients in trials. The averages speak for themselves — you put fewer patients in tri-als today.”
According to Kingsley, the only way to continue this financial model is to partici-pate in three times as many concurrent tri-als. However, he says it’s far more efficient from an overhead standpoint to have one trial that places eight patients, rather than three trials that place eight patients.
Also, at a time when technology is con-quering inefficiencies in other industries, technology is compounding problems in the clinical trial sector. In each of the three studies he cites above, it’s likely that three different electronic health records, tablets
and wearables are used by the different sponsors. When each sponsor uses their own networks and devices for patient-re-ported outcomes, it adds to site workload and time.
“We have no ability to standardize tech-nology,” Kingsley says “We have to do so many trials with so many sponsors, and they have their own decision-making… Our industry suffers from adoptive pho-bia (standardization between sponsors and sites).”
As an example, he cites the advantages of sites adopting electronic platforms such as eSource. Using such a platform could save billions compared to the aggregate cost of monitors flying to sites to review source documents. Clinically, an electronic plat-form also prevents errors such as entering a blood pressure incorrectly or performing a patient procedure out of order from the test protocol.
“We’re trying to convince the industry it’s a huge benefit, but the sites can’t afford
Start-up Costs Can Be an Uphill Slog in Need of Change
© 2018 CenterWatch. Duplication or sharing of this publication is strictly prohibited.
Status Quo is Not a Viable Option: A Host of Challenges Strain Clinical Trial Site Viability
September 2018 A CenterWatch Publication Volume 25, Issue 09
see Site Viability on page 7
By John W Mitchell
C linical trial site finances are a problem that keeps getting bigger. While there’s agreement improvements are on the
horizon — and at least one sponsor is work-ing to shake things up — there’s also a lot of frustration about the slow pace of reinven-tion. A host of longstanding challenges are intensifying. These issues range from slug-
gish payments, contract viability, preferred site status, interconnectivity and something less tangible — a lack of consideration in the relationship.
Payments, which have traditionally ar-rived quarterly, are often now even later. And sites are hiring extra staff to chase down payments— and medical doctors to keep up with the regulatory requirements, says Karri Venn, president of research at LMC Mann
Research, which operates 19 trial and prima-ry care sites in Canada.
According to recent data, 80 percent of sites prefer monthly payments — with 59 percent in-dicating that quarterly payments have a nega-tive impact on trials. Given a choice, they said they’d choose studies that reimburse monthly.
“We learned very quickly that we had to have a floating line-of-credit...[or] we would
see Start-up Costs on page 6
By John W Mitchell
rustration about clinical trial start-up costs is not unlike Sisyphus’ dilemma. A host of long-standing expense and
inefficiency realities continues to create such uphill headwinds for the clinical trial sector. According to some sources, such problems even threaten the viability of the sector. Sites complain they incur more over-head costs driven by regulatory documen-tation, antiquated data collection and the demands of precision medicine to name a few — all without increased compensation from sponsors and CROs. A recent study supports this concern. Researchers at the Tufts Center for the Study of Drug Devel-opment found that the study start-up phase of five to six months for clinical trials has remained unchanged for the past decade. The study also concluded that CROs mak-The study also concluded that CROs mak-The study also concluded that CROs making investments in technology are getting trials done faster. None of this bodes well for smaller, independent players.
“Sites are doing more work for [fewer] patients. We used to enroll about eight pa-
tients per study 10 years ago, and today the number is less than three,” says Jeff King-sley, CEO at IACT Health. His company operates 13 locations in Georgia and a few outside the state in a network of about 100 clinical specialists. “The protocols are lon-ger, and there are more procedures per pa-tient per day. So, you’re doing loads more work, but you’re only paid when you put patients in trials. The averages speak for themselves — you put fewer patients in tri-als today.”
According to Kingsley, the only way to continue this financial model is to partici-pate in three times as many concurrent tri-als. However, he says it’s far more efficient from an overhead standpoint to have one trial that places eight patients, rather than three trials that place eight patients.
Also, at a time when technology is con-quering inefficiencies in other industries, technology is compounding problems in the clinical trial sector. In each of the three studies he cites above, it’s likely that three different electronic health records, tablets
and wearables are used by the different sponsors. When each sponsor uses their own networks and devices for patient-re-ported outcomes, it adds to site workload and time.
“We have no ability to standardize tech-nology,” Kingsley says “We have to do so many trials with so many sponsors, and they have their own decision-making… Our industry suffers from adoptive pho-bia (standardization between sponsors and sites).”
As an example, he cites the advantages of sites adopting electronic platforms such as eSource. Using such a platform could save billions compared to the aggregate cost of monitors flying to sites to review source documents. Clinically, an electronic plat-form also prevents errors such as entering a blood pressure incorrectly or performing a patient procedure out of order from the test protocol.
“We’re trying to convince the industry it’s a huge benefit, but the sites can’t afford
Start-up Costs Can Be an Uphill Slog in Need of Change
Status Quo is Not a Viable Option: A Host of Challenges Strain Clinical Trial Site ViabilityBy John W Mitchell
linical trial site finances are a problem
gish payments, contract viability, preferred site status, interconnectivity and something less tangible — a lack of consideration in the
Research, which operates 19 trial and prima-ry care sites in Canada.
According to recent data, 80 percent of sites
see Start-up Costs on page 6
In this issue3-4 In Review
Regulatory Update
5 Action Items
Part 4: How to Identify Candidate Fraudulence Early in The Recruitment Cycle By Angela Roberts
Top Considerations for Using Digital Health Devices in Clinical Trials By Vicki Gashwiler
Risk-based Quality Management: The New Normal By Brion Regan
10-11 Pipeline NewsFDA Actions
The CenterWatch MonthlyISSN 1556-3367
Editorial Director Lisa SteinProduction Renee Breau
© 2018 CenterWatch, LLC. All rights reserved. No part of this publication may be distributed or reproduced in any form or by any means without the express written consent of the publisher. Permission requests can be obtained via fax at (617) 948-5101 or emailed at [email protected]. Single-user annual subscriptions start at $399.
For inquiries on multi-reader and corporate subscription rates and article reprints:Tel: (617) 948-5100Email: [email protected]
For inquiries regarding your subscription:CenterWatch Customer ServiceTel: (866) 219-3440, Fax: (617) 948-5101Email: [email protected]
For inquiries regarding advertising:Advertising Sales RepresentativeTel: (617) 948-5100, Email: [email protected]
Send address changes to: CenterWatch Customer Service10 Winthrop Square, Fifth Floor, Boston, MA 02110CenterWatch Main and Editorial Offices:Tel: (617) 948-5100 Fax: (617) 948-5101Email: [email protected]
The CenterWatch Monthly September 2018 3
InReview
FDA Signs Off on Treatment for Rare, Adrenal Gland Tumors
The FDA has approved the injectable drug Azedra for rare cancers of the adre-nal glands — the first ever non-surgical therapy OK’d for these tumors.
Azedra (iobenguane I131) is a radiother-apy drug that attacks tumors with a high, specifically targeted dose. It’s designed to treat adults and children (12 and older) with inoperable locally advanced or metas-tic cancers called phenochromocytoma and paraganglioma.
Pheochromocytoma forms inside and paraganglioma grows outside the adrenal gland(s).
Both tumor types release hormones that can cause symptoms including high blood pressure, rapid heartbeat and anxiety.
University of Pennsylvania research-ers gave 68 patients in a trial at least one therapeutic dose of Azedra. The results: 25 percent who received at least one dose and 32 percent of those who received two doses saw their blood pressure drop enough to cut their hypertension meds in half.
“This is a true breakthrough. Until to-day, there were no anti-tumor therapies available for patients with these tumors who were not candidates for surgery,” said principal investigator Daniel Pryma, an associate professor of Radiology and Ra-diation Oncology.
“This therapy not only controls the tu-mors but also the debilitating symptoms caused by their excess hormone produc-tion, meaning it provides dual benefit to patients,” added Pryma, also chief of Penn’s Nuclear Medicine and Clinical Mo-lecular Imaging.
Reported side effects include low white blood cell and platelet counts, fatigue and anemia.
The FDA gave Azedra an Orphan Drug designation, Fast Track status and Break-
through Therapy designation in the U.S. Its license is held by Progenics Pharmaceuticals.
Japan Greenlights Parkinson’s TrialIn the first trial of its kind, Kyoto University
scientists have won approval from Japanese regulators to test adult stem cells as a possible treatment for Parkinson’s disease.
Induced pluriopotent stem cells (iPS) are derived from skin or blood cells and induced back into an embryonic-like plu-ripotent state that can divide into more stem cells or become any type of cell in the body, leading to a potentially unlimited source of any type of human cell needed for therapeutic purposes. They’re consid-ered promising for regenerative research because they can become different hu-man cells and, also, avoid controversy sur-rounding stem cells from human embryos.
Researchers plan to transplant iPS cells into the brains of Parkinson’s patients in the hope they will help repair or replace damaged nerve cells. This is the first trial of its kind to use iPS cells.
Scientists say they’re cautiously optimis-tic after testing the process in monkeys, who showed improvement and didn’t de-velop brain tumors — a much-feared po-tential side effect.
FDA: Focus on Hardest to Treat in Cohort Cancer Trials
The FDA says sponsors considering adaptive studies for early phase cancer treatments should focus on patients with no other options.
The agency notes that so-called expan-sion cohort trials — which start out rela-tively small but expand if a potential treat-ment shows promise--can be a way to get a treatment to market more quickly.
Regulatory Update
see Regulatory Update on page 4
problems even threaten the viability of the
Start-up Costs Can Be an Uphill Slog in Need of Change
SUBSCRIBE TODAY! store.centerwatch.com [email protected] (617) 948-5100
By John W Mitchell
Frustration about clinical trial start-up costs is not unlike Sisyphus’ dilemma. A host of long-standing expense and
inefficiency realities continues to create such uphill headwinds for the clinical trial sector. According to some sources, such problems even threaten the viability of the
Start-up Costs Can Be an Uphill Slog in Need of ChangeBy John W Mitchell
Finefficiency realities continues to create such uphill headwinds for the clinical trial sector. According to some sources, such problems even threaten the viability of the
Start-up Costs Can Be an Uphill Slog in Need of Change
Unique content, critical analysis & expert market research
Subscribe to the industry’s leading global news source.
Download a sample issue!www.centerwatch.com/promotions
» In-depth analytical reports on key trends o� ering insights for your strategies and practices
» Key regulatory updates to keep organizations informed of the latest FDA initiatives, changes and requirements
» Subscriptions start at $399

© 2018 CenterWatch. Duplication or sharing of this publication is strictly prohibited. CWW2240
WCG | CWWeekly October 8, 2018 5 of 8
Features
“You have sort of a window during which there are enough symptoms for us to be sure that the person has this disease but
it’s not so far gone that we’re not likely to see any improvement.”
—Sofija Jovic, business transformation advisor, MedAvante-Prophase
to us and say, ‘I’m really here because my symptoms are bothering me.’ Boy, if only this patient had come a year ago,” Hauser says.
He notes that patients, care providers and especially sponsors can play a critical role in early trial recruiting.
Parkinson’s develops subtly — a tremor here, slight difficulty moving there, says Sofija Jovic, business transformation advisor at MedAvante-Prophase. Typically, patients have about six months to a year after displaying very early signs before requiring systemic therapies to address underlying symptoms.
Parkinson’s disease, and most other neuro-degenerative disorders, can hide for a long time because human brains are adaptable. That’s good news for stroke pa-tients because the brain will dig new neural pathways. But it’s bad news for Parkinson’s sufferers because it generally means that by the time symptoms present their brain has literally run out of room to adapt.
“You have sort of a window during which there are enough symptoms for us to be sure that the person has this disease but it’s
not so far gone that we’re not likely to see any improvement,” Jovic says.
As it stands, less than 3 percent of Par-kinson’s patients enroll in clinical trials, Jovic says. Patients are a lot like the frog in the boiling water — they don’t realize there’s trouble until it’s already too late, she adds.
Recent discoveries that Parkinson’s appears to be related to the buildup of misfolded alpha-synuclein proteins — and that those protein clusters may respond to treatments — has given researchers renewed hope that they’re on a path to-
ward effective treatments and even cures, Hauser says.
But he stresses that won’t happen with-out enough patients to recruit for clinical trials at the earliest, pre-med stages of the disease.
He admits that the subtlety of early-stage Parkinson’s creates “a Catch-22” of sorts. “How do we get this message to patients who don’t know there’s this message to be received?” he says.
The answer, he tells CenterWatch: Spon-sors have to do a better job of getting the word out to doctors that they shouldn’t rush to prescribe systemic meds prematurely — and should instead refer patients to early clinical trials.
Jovic agrees that sponsors have to do a better job establishing relationships with care providers. But she says they also need to develop technology that enables virtual trials because neuro-degenerative disorders don’t lend themselves to site visits.
“You have a patient who’s been up half the night, and you’re going to ask his care-giver to drive him two hours to a site for four hours of tests?” Jovic says. “That’s just not realistic.”
Parkinson’s Clinical Trialscontinued from page 1
#1 EVENT FOR QUALITY, COMPLIANCE AND INSPECTIONAL READINESS PROFESSIONALS
FDA INSPECTIONS SUMMIT
OCT. 23–25, 2018
BETHESDA, MDPRESENTS THE
13TH ANNUAL
REGISTER
The FDA will always do inspections, and the regulated community is still making mistakes. Warning letters, 483 citations, and hits to your reputation can cost you time, energy and money! You can’t afford to be caught off guard. So mark your calendar and book reservations early for the must-attend conference of the regulatory year.
Celebrating
Years of Pioneering, Together.
It isn’t in our nature to seek the limelight or to sing our own praises.
But when you turn 50, well, that’s something pretty special. We don’t want
to celebrate alone though, because we know the real power comes from
pioneering together. To all of those who share our passion for protecting
people and are inspired by science and medical discovery, a heart felt thank
you for joining us on our first 50 years of pioneering together!
www.wcgirb.com/50
WIRB50_CenterwatchWeekly_Ad.indd 1 5/1/18 1:49 PM
© 2018 CenterWatch. Duplication or sharing of this publication is strictly prohibited. CWW2240
WCG | CWWeekly October 8, 2018 7 of 8
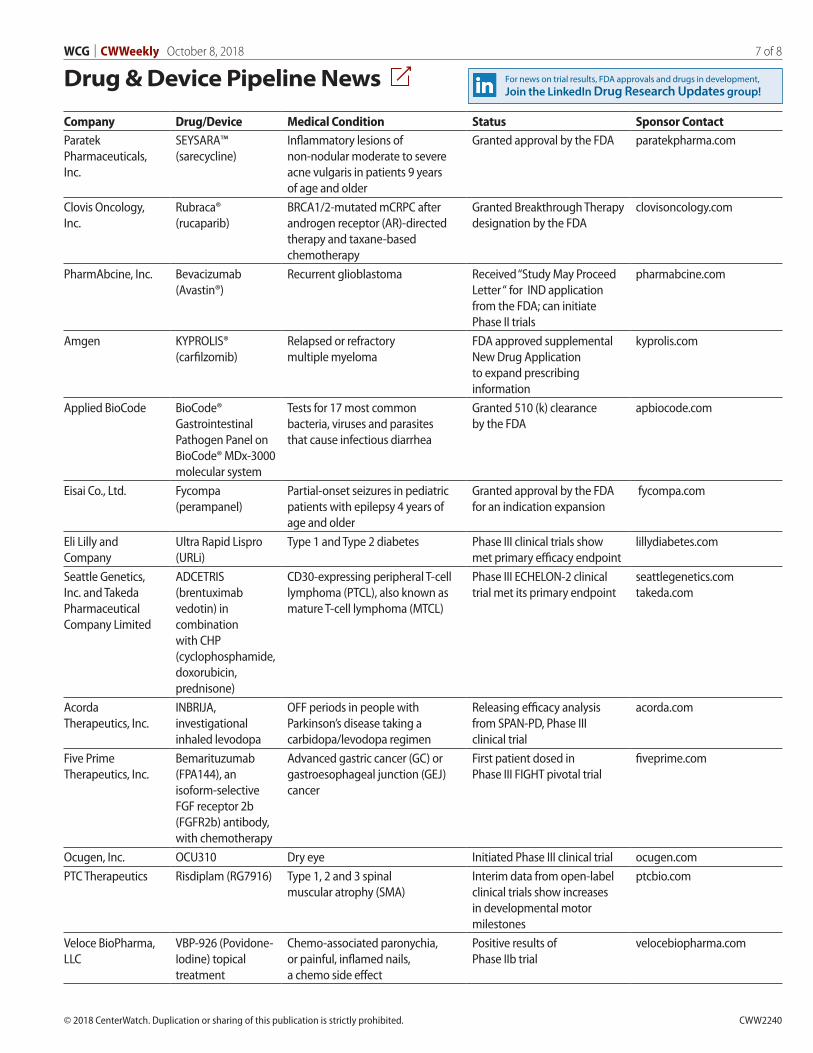
Drug & Device Pipeline News
Company Drug/Device Medical Condition Status Sponsor ContactParatek Pharmaceuticals, Inc.
SEYSARA™ (sarecycline)
Inflammatory lesions of non-nodular moderate to severe acne vulgaris in patients 9 years of age and older
Granted approval by the FDA paratekpharma.com
Clovis Oncology, Inc.
Rubraca® (rucaparib)
BRCA1/2-mutated mCRPC after androgen receptor (AR)-directed therapy and taxane-based chemotherapy
Granted Breakthrough Therapy designation by the FDA
clovisoncology.com
PharmAbcine, Inc. Bevacizumab (Avastin®)
Recurrent glioblastoma Received “Study May Proceed Letter “ for IND application from the FDA; can initiate Phase II trials
pharmabcine.com
Amgen KYPROLIS® (carfilzomib)
Relapsed or refractory multiple myeloma
FDA approved supplemental New Drug Application to expand prescribing information
kyprolis.com
Applied BioCode BioCode® Gastrointestinal Pathogen Panel on BioCode® MDx-3000 molecular system
Tests for 17 most common bacteria, viruses and parasites that cause infectious diarrhea
Granted 510 (k) clearance by the FDA
apbiocode.com
Eisai Co., Ltd. Fycompa (perampanel)
Partial-onset seizures in pediatric patients with epilepsy 4 years of age and older
Granted approval by the FDA for an indication expansion
fycompa.com
Eli Lilly and Company
Ultra Rapid Lispro (URLi)
Type 1 and Type 2 diabetes Phase III clinical trials show met primary efficacy endpoint
lillydiabetes.com
Seattle Genetics, Inc. and Takeda Pharmaceutical Company Limited
ADCETRIS (brentuximab vedotin) in combination with CHP (cyclophosphamide, doxorubicin, prednisone)
CD30-expressing peripheral T-cell lymphoma (PTCL), also known as mature T-cell lymphoma (MTCL)
Phase III ECHELON-2 clinical trial met its primary endpoint
seattlegenetics.comtakeda.com
Acorda Therapeutics, Inc.
INBRIJA, investigational inhaled levodopa
OFF periods in people with Parkinson’s disease taking a carbidopa/levodopa regimen
Releasing efficacy analysis from SPAN-PD, Phase III clinical trial
acorda.com
Five Prime Therapeutics, Inc.
Bemarituzumab (FPA144), an isoform-selective FGF receptor 2b (FGFR2b) antibody, with chemotherapy
Advanced gastric cancer (GC) or gastroesophageal junction (GEJ) cancer
First patient dosed in Phase III FIGHT pivotal trial
fiveprime.com
Ocugen, Inc. OCU310 Dry eye Initiated Phase III clinical trial ocugen.comPTC Therapeutics Risdiplam (RG7916) Type 1, 2 and 3 spinal
muscular atrophy (SMA)Interim data from open-label clinical trials show increases in developmental motor milestones
ptcbio.com
Veloce BioPharma, LLC
VBP-926 (Povidone-Iodine) topical treatment
Chemo-associated paronychia, or painful, inflamed nails, a chemo side effect
Positive results of Phase IIb trial
velocebiopharma.com
For news on trial results, FDA approvals and drugs in development, Join the LinkedIn Drug Research Updates group!
© 2018 CenterWatch. Duplication or sharing of this publication is strictly prohibited. CWW2240
WCG | CWWeekly October 8, 2018 8 of 8
Research Center Spotlight
Research Center Spotlight is a monthly selection of clinical research centers who have Research Center Profile pages posted on CenterWatch.com. Included in their annual subscriptions, company profiles are randomly selected to appear in this section, providing added exposure for their expertise and services in conducting and managing clinical studies.
To learn more about becoming a Research Center Profile page subscriber, contact Sales at (617) 948-5100 or [email protected].
Homestead, FL (786) 339-8454 [email protected]
Clinical Research of Homestead is a privately owned and operated clinical research site. It conducts multi-specialty trials for the phar-maceutical industry focusing in Phases II, III, and IV — and supports pharma companies and CROs in introducing new and approved FDA meds.
Ft. Lauderdale, FL (954) 355-5563 [email protected]
Broward Health, providing service for more than 80 years, is a nationally recognized system that offers world-class healthcare to all. It is one of the 10 largest public healthcare systems in the nation. It has cardiovas-cular, adult and pediatric cancer and pediatric sickle cell research teams.
Fargo, ND (701) [email protected]
Bagan Strinden Vision is a private fast- growing ophthalmology practice with staff to conduct trials on a full- time basis. Its mission: to treat patients with compassion using the latest technology and most improved treatments and procedures.
Arlington Heights, IL(847) [email protected]
AMITA Health is a nine-hospital health system with an extensive physician provider network of more than 3,000 physicians. Three AMITA Health hospitals have been ranked among the Best Hospitals in the Chicago metropolitan area by U.S News and World Report.
Austin, TX (512) 421-3851 [email protected]
Established in 1995, Austin Heart’s clinical research program is dedicated to providing the most innovative and progressive care to patients, while also contributing to the science of medicine through the conduct of clinical trials.
Kalamazoo, MI (269) 337-4264 [email protected]
The Center for Clinical Research was created in 2015 within an academic medical center at Western Michigan University Homer Stryker M.D. School of Medicine. The Center brings experienced investigators, coordinators and other support staff to the conduct of clinical trials across multiple therapeutic areas.
San Diego, CA (858) 836-8350 [email protected]
For more than 40 years, Sharp HealthCare has provided excellence in mental health treatment. Since 1994, Sharp Mesa Vista Hospital’s Clinical Research Center has conducted more than 200 clinical trials of investigational psychiatric medications.
Salt Lake City, UT(801) 269-8200 [email protected]
At any given time, the Salt Lake City research center concurrently runs 50-80 clinical studies in Human Abuse Potential (HAP), addiction, pain, psychiatry, neurology, pediatric and infectious disease services. The clinic has been conducting clinical research for more than 13 years.
Jasper, AL (205) 387-7555 (option #3)[email protected]
Jasper Summit Research, LLC, is a thriving multi-therapeutic dedicated research site proficient in Phase II, III, & IV clinical trials with many adult participants, under direct supervision of Jan H. Westerman, MD.
Raleigh, NC (919) 346-6945 [email protected]
Founded in 2012, Oculus Research is a clinical research company that specializes in ophthalmic research and is focused on the well-being of its patients. It conducts research studies that include all ages.
Jasper Summit Research, LLC
Oculus Research, Inc.
AMITA Health
Austin Heart Research
Bagan Strinden Vision Research
Western Michigan University Clinical Research of Homestead
PRA Health Sciences
Broward Health Medical Center Sharp Mesa Vista Hospital Clinical Research Center