jejunal perforation in a football player
TRANSCRIPT
64 Injury: the British Journal of Accident Surgery (1993) Vol. 24/No. I
Jejunal perforation in a football player
N. Williams, M. Striven and I’. R. F. Bell Department of Surgery, Leicester Royal Infirmary, Leicester, UK
Introduction
Soccer is a contact sport, usually by direct one-to-one confrontation. That the sport is associated with injuries is not surprising; the predominant ones are musculoskeletal, the knee being the commonest site (Nicholas et al., 1988). When abdominal injury occurs, the kidneys, liver and spleen are most frequently involved (Bergquist et al., 1982), but injuries to the gastrointestinal tract are extremely rare. We report a case ofejejunal perforation sustained during a game of soccer.
Case report
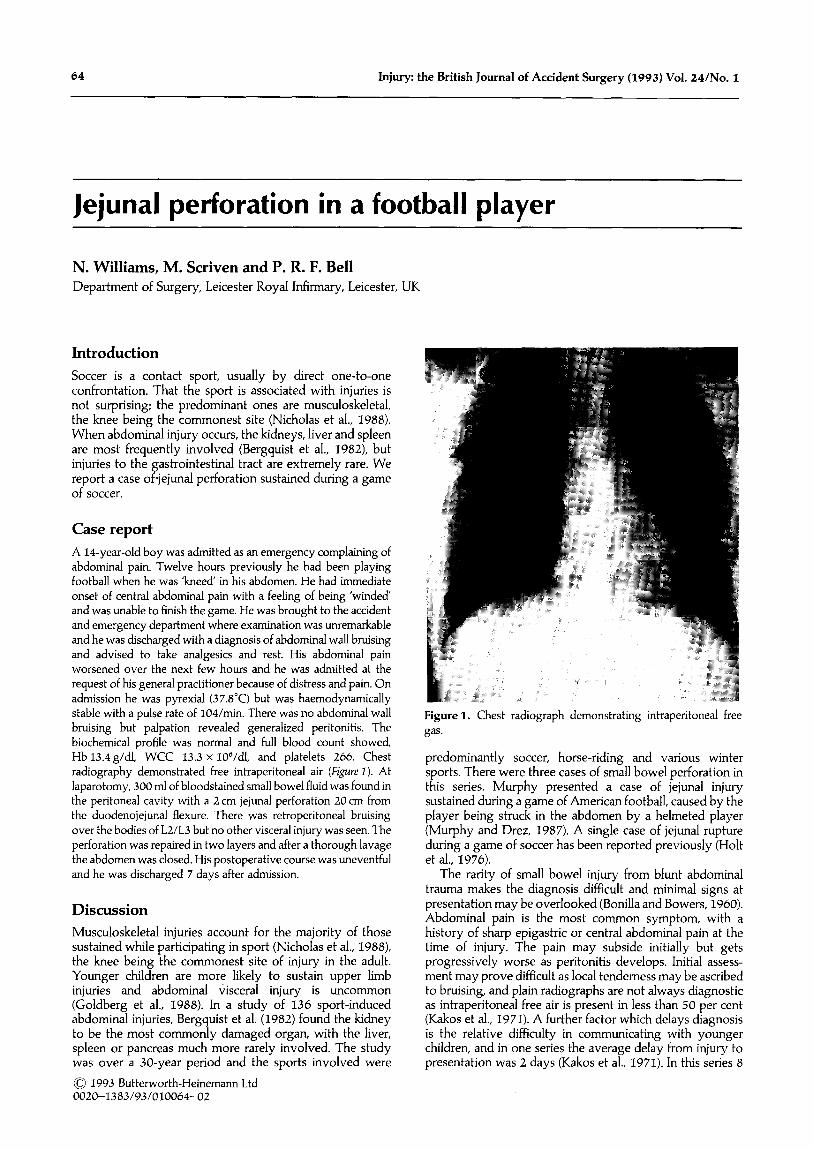
A 14-year-old boy was admitted as an emergency complaining of abdominal pain. Twelve hours previously he had been playing football when he was ‘kneed in his abdomen. He had immediate onset of central abdominal pain with a feeling of being ‘winded and was unable to finish the game. He was brought to the accident and emergency department where examination was unremarkable and he was discharged with a diagnosis of abdominal wall bruising and advised to take analgesics and rest. His abdominal pain worsened over the next few hours and he was admitted at the request of his general practitioner because of distress and pain. On admission he was pyrexial (37.8”C) but was haemodynamically stable with a pulse rate of 104/min. There was no abdominal wall bruising but palpation revealed generalized peritonitis. The biochemical profile was normal and full blood count showed, Hb 13.4 g/dl, WCC 13.3 x 106/dl, and platelets 266. Chest radiography demonstrated free intraperitoneal air (Figure I). At laparotomy, 300 ml of bloodstained small bowel fluid was found in the peritoneal cavity with a 2 cm jejunal perforation 20 cm from the duodenojejunal flexure. There was retroperitoneal bruising over the bodies of L2/L3 but no other visceral injury was seen. The perforation was repaired in two layers and after a thorough lavage the abdomen was closed. His postoperative course was uneventful
and he was discharged 7 days after admission.
Discussion
Musculoskeletal injuries account for the majority of those sustained while participating in sport (Nicholas et al., 1988), the knee being the commonest site of injury in the adult. Younger children are more likely to sustain upper limb injuries and abdominal visceral injury is uncommon (Goldberg et al., 1988). In a study of 136 sport-induced abdominal injuries, Bergquist et al. (1982) found the kidney to be the most commonly damaged organ, with the liver, spleen or pancreas much more rarely involved. The study was over a 30-year period and the sports involved were
0 1993 Butter-worth-Heinemann Ltd 0020-1383/93/010064-02
Figure 1. Chest radiograph demonstrating intraperitoneal free gas.
predominantly soccer, horse-riding and various winter sports. There were three cases of small bowel perforation in this series. Murphy presented a case of jejunal injury sustained during a game of American football, caused by the player being struck in the abdomen by a helmeted player (Murphy and Drez, 1987). A single case of jejunal rupture
during a game of soccer has been reported previously (Holt et al., 1976).
The rarity of small bowel injury from blunt abdominal trauma makes the diagnosis difficult and minimal signs at presentation may be overlooked (Bonilla and Bowers, 1960). Abdominal pain is the most common symptom, with a history of sharp epigastric or central abdominal pain at the time of injury. The pain may subside initially but gets progressively worse as peritonitis develops. Initial assess- ment may prove difficult as local tenderness may be ascribed to bruising, and plain radiographs are not always diagnostic as intraperitoneal free air is present in less than 50 per cent (Kakos et al., 1971). A further factor which delays diagnosis is the relative difficulty in communicating with younger children, and in one series the average delay from injury to presentation was 2 days (Kakos et al., 1971). In this series 8

Case reports 65
of 26 children had mesenteric haematomas alone. No specific figure is given for those with bowel perforation (Kakos et al., 1971).
The mechanism of injury is usually by direct compression of the bowel against the vertebral body (Williams and Sargeant, 1963) and the Japarotomy findings of retroperi- toneal bruising as in our case would seem to confirm this.
Clearly, the key to successful management of these patients is early diagnosis and prompt laparotomy. The rarity of small bowel injury in these situations makes it easy to overlook and the clinician should have a high index of suspicion in these cases.
Goldberg B. et al. (1988) Injuries in youth football. Paediafrics 81,
255. Holt R. W., Wolf G. T. and France P. E. (1976) Rupture of the
jejunum secondary to blunt trauma in a football player. South. Med. J. 60, 281.
Kakos G. S., Grossfield J. L. and Morse T. S. (1971) Small bowel injuries in children after blunt trauma. Ann. Surg. 174, 238.
Murphy C. P. and Drez D. (1987) Jejunal rupture in a football player. Am. ]. Sports Med. 15, 184.
Nicholas J. A., Rosenthal P. and Gleim G. W. (1988) A historical perspective of injuries in professional football.]AMA 260,939.
Williams R. D. and Sargent F. T. (1963) The mechanism of intestinal injury in trauma. J. Trauma 31, 288.
References Paper accepted 7 April 1992.
Bergquist D., Hedelin H., Karlsson G. et al. (1982) Abdominal injuries from sporting activities. Br. J. Sporfs Med. 16, 76.
Bonilla K. B. and Bowers W. F. (1960) Traumatic rupture of the proximal jejunum. Am. 1. Surg. 100, 731.
Requests for reprinfs should be addressed fo: Mr N. Williams, Department of Surgery, Leicester Royal Infirmary, Leicester LEl
5WW, UK.
Gastric rupture from blunt trauma: two unusual presentations
J. D. Knottenbeltl, S. Van As’ and S. Volschenk’ ‘Trauma Unit and 3urgical Intensive Care Unit, Groote Schuur Hospital, Cape Town, South Africa
Introduction
Blunt gastric rupture is rare; Brunsting and Morton (1987) could find only 67 cases in the English literature since 1930. Mortality and morbidity in the reviewed cases were high (47 per cent). We present two survivors of this unusual condition, each of whom had interesting features.
Case reports
Close 1 A 24.year-old man was knocked down by a car and was brought into the trauma unit resuscitation area with a depressed level of consciousness and fracture of the right femur. On examination blood pressure was 120150 mmHg, pulse 112/min and haemoglo- bin level 12.5 g/d]. He was noted to have abrasions to the left frontotemporal region, with no CSF leak and the Glasgow Coma Score was initially assessed at 10/15, rising to 15/15 within 10 min of arrival. Chest examination was normal with no fractured ribs clinically. The abdomen was soft and undistended, with no rebound, tenderness or guarding. The right femur was clinically fractured in the midshaft, but there was no neurovascular deficit.
The patient was initially intubated to protect the airway because of the depressed level of consciousness and I litre of crystalloid given via peripheral line. Arterial blood gas analysis (ABG) (pH, 7.27; Pco,, 4.74 kPa; PO,, 31.6 kPa; Std bicarb, 17.0; Base excess, - 8.8) revealed a moderately severe metabolic acidosis with normal respiratory parameters. Serum urea and electrolytes were within normal limits. Urine obtained at catheter- ization showed the presence of microscopic haematuria but was
<<“I 1993 Butterworth-Heinemann Ltd 0020-1383/93/010065-02
otherwise normal. A nasogastric tube was inserted and 30 ml of normal-looking stomach contents returned. Radiography con- firmed a normal cervical spine and chest, and revealed a minor pelvic fracture (pubic rami), apart from the obvious fracture of the femur. The ABG was repeated 30 min later, showing a persistent acidosis in spite of the patient being warm, well-perfused and passing adequate urine (pH, 7.27; Pco,, 4.71 kPa; PO,, 32.8 kPa; Std bicarb, 16.9; Base excess, 9.1).
A careful, complete clinical examination was repeated, the patient now being fully awake. Although the abdomen was found to be completely pain free, soft and undistended, a diagnostic peritoneal lavage was performed. On insertion of the catheter there was an immediate backflow of stomach content, acid to litmus paper, suggesting rupture of the stomach. At lapatotomy there was a 15 cm laceration of the greater curvature of the stomach extending into the greater omentum. A small laceration on the inferior surface of the left lobe of the liver required no treatment. No other intra-abdominal injuries were found and after repair of the stomach and irrigation of the abdominal cavity the abdomen was closed. The patient made an uneventful postopera- tive recovery.
Case 2 A 31.year-old man was involved in a motor vehicle accident as a passenger on his way home from a party at which he had consumed large amounts of food and drink. He was taken to a provincial hospital accident department where he was found to be hypotensive (BP 90160mmHg) with a clinically obvious acute painful abdomen. The initial chest radiograph (Figure I) showed a fluid level in the pericardial sac consistent with traumatic haemo-