jason rand pa-c, pt · jason rand pa-c, pt boston sports and shoulder center boston celtics medical...
TRANSCRIPT
Jason Rand PA-C, PT Boston Sports and Shoulder Center
Boston Celtics Medical Team
New England Baptist Hospital – Sports Medicine Service
Corticosteroid An Aqueous Suspension a practically white,
odorless, crystalline powder
Suppress inflammation by decreasing collagenase and prostaglandin formation
But also…. Catabolic promoter that block glucose
uptake in tissues, and decrease new protein synthesis
Indications Arthritis flair
Synovitis
Adhesive capsulitis
Tendonopathy/tendonitis (NWB Tendon)
Crystal-Induced Arthritis
Rheumatoid arthritis
Corticosteroid
“I heard you can only have….”
Depends on diagnosis
End stage oa vs. Tendonitis
“Will the arthritis worsen”
Intra-articular cortisone injections do not lead to the progression of osteoarthritis 1
1) Raynauld JP, Buckland-Wright C Ward R et al. Safety and efficacy of long-term
intraarticular steroid injections in oa of the knee: a randomized , double-blinded
placebo-controled trial Arthritis Rhum. 2003;2005 13(1):37-46
Single injections of the 4 most commonly injected
corticosteroids do not appear to have significant
chondrotoxic properties when studied in a bioreactor
perfusion model over the average residence time of
each medication post injection.
- A0SSM 2010 Podium Presentation
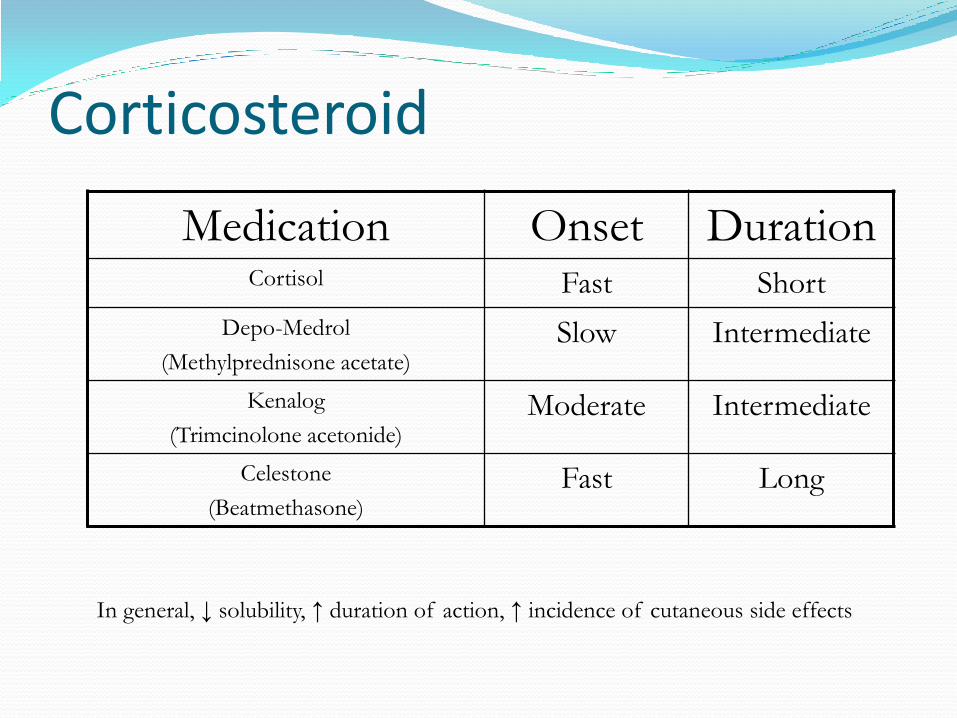
Corticosteroid
Medication Onset Duration Cortisol Fast Short
Depo-Medrol
(Methylprednisone acetate) Slow Intermediate
Kenalog
(Trimcinolone acetonide) Moderate Intermediate
Celestone
(Beatmethasone) Fast Long
In general, ↓ solubility, ↑ duration of action, ↑ incidence of cutaneous side effects
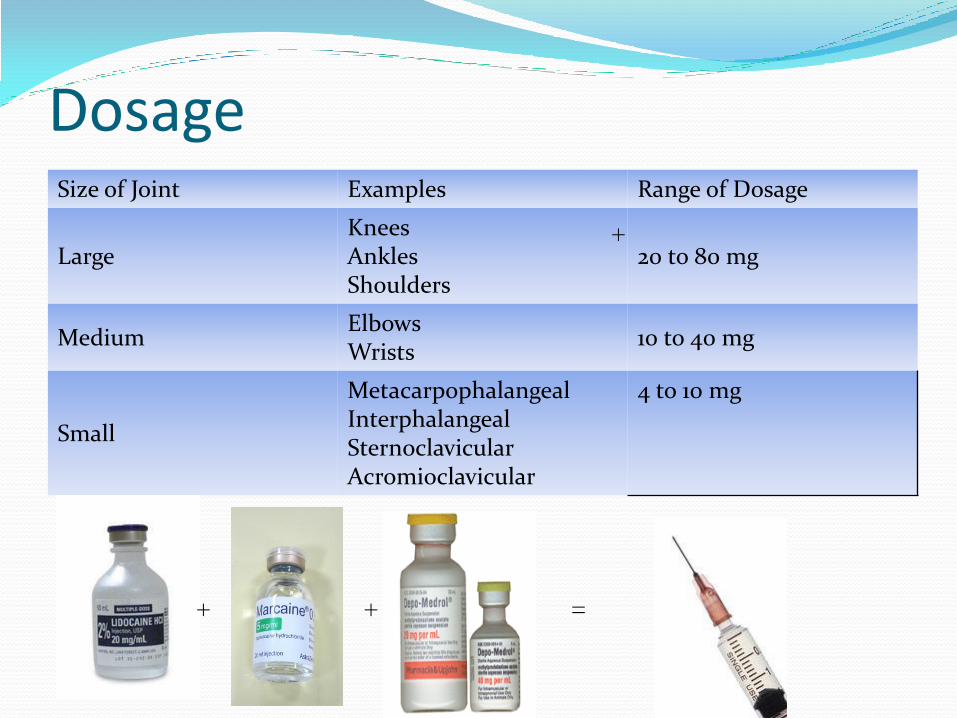
Dosage Size of Joint Examples Range of Dosage
Large Knees Ankles Shoulders
20 to 80 mg
Medium Elbows Wrists
10 to 40 mg
Small
Metacarpophalangeal Interphalangeal Sternoclavicular Acromioclavicular
4 to 10 mg
+ +
+
=
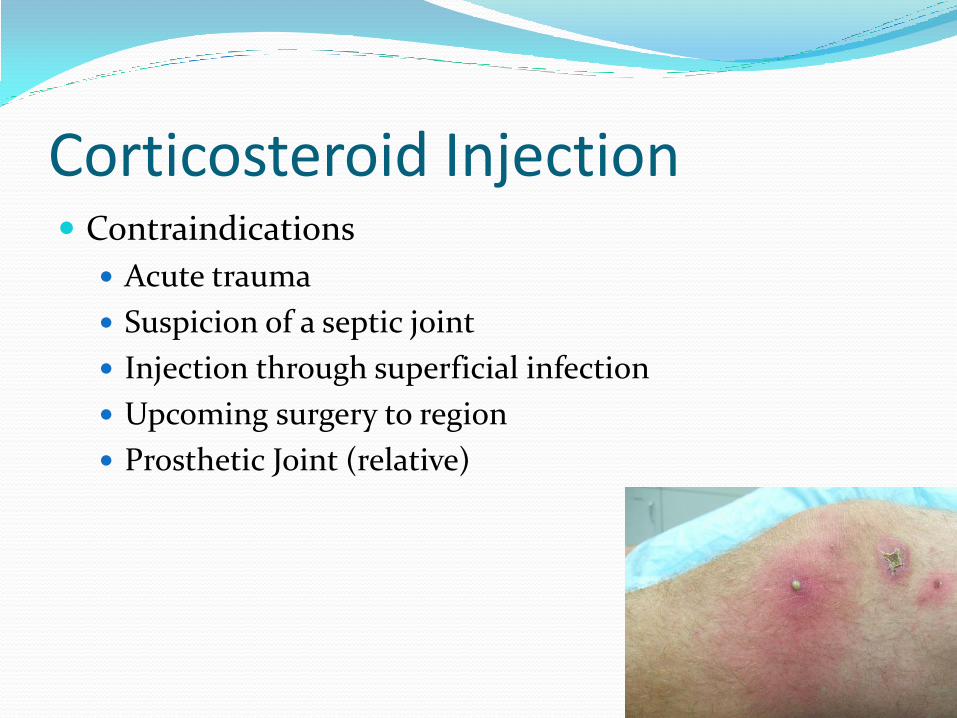
Corticosteroid Injection Contraindications
Acute trauma
Suspicion of a septic joint
Injection through superficial infection
Upcoming surgery to region
Prosthetic Joint (relative)
Corticosteroid Injection Adverse reactions
Hypothalamic-pituitary adrenal (HPA) axis suppression.
Transient hyperglycemia
Sodium Retention
Joint infection rare ( 1 in 13,000)1 ( 1 in 15,000)2 (<1 in 78,000)3
Local Effects: Lipodystrophy
Loss of skin pigmentation
Tendon rupture
Post – Injection Flair 2-10%
1: Charalambous CP, Tryfonidis M, Sadiq S et al. Septic arthritis following intra-
articular steriod injection of the knee: a survey of current practice
regarding antiseptic technique used during intra-articular steroid injection
of the knee Clin Rheumatol. 2003 Dec;22(6):386-390. 2: Essentials of Musculoskeletal Care 3
3. Courtney P, Doherty M. Joint aspiration and injection and synovial fluid analysis. Bet
practice and reaserch in clinical rheumatology 23 (2009) 161-192.

Cortisone – Skin Blanching
Increased risk in African American Population
Dec. Risk by attempting to avoid peri-dermal
injection

Cortisone – Fat Atrophy
Corticosteroid Injection Post- injection education
Avoid heavy activity for next 48 hours
Site of injection may be sore
Ice, NSAIDS, Tylenol
Benefits may take hours or days
May get worse before it gets better
Cortisone and Physical Therapy Match made in heaven
Adhesive Capsulitis/ Arthrofibrosis
RC inpingment
Osteoarthritis
Precautions
Post injection pain: Hold or modify PT


Steroid Contamination! New England Compounding Center (Framingham, MA)
323 Cases of fungal meningitis
5 Peripheral infections
24 Deaths

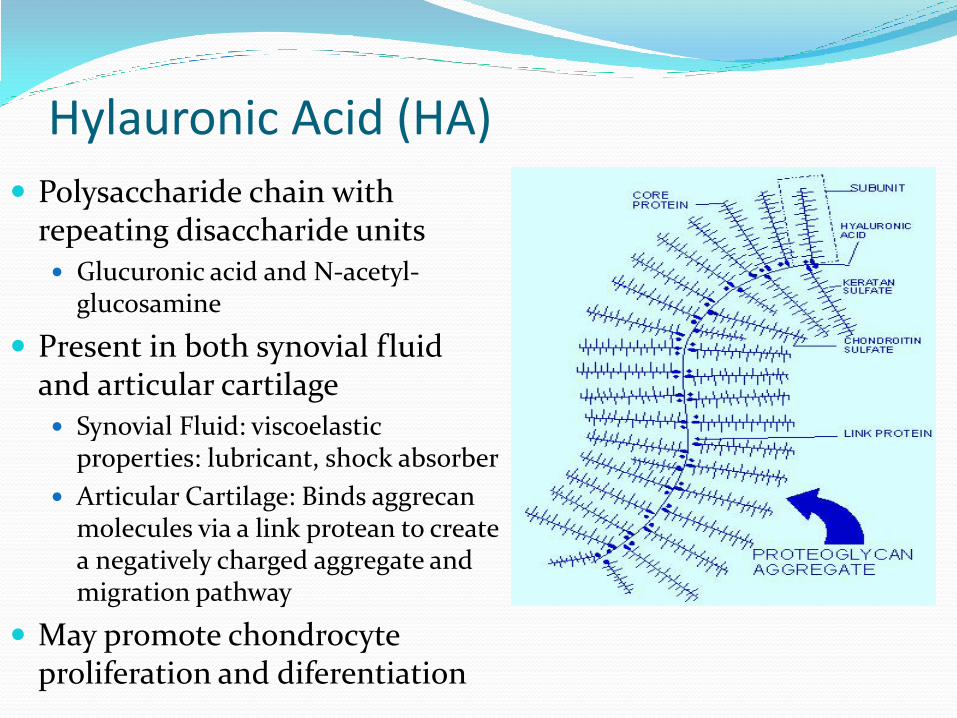
Hylauronic Acid (HA)
Polysaccharide chain with repeating disaccharide units Glucuronic acid and N-acetyl-
glucosamine
Present in both synovial fluid and articular cartilage Synovial Fluid: viscoelastic
properties: lubricant, shock absorber
Articular Cartilage: Binds aggrecan molecules via a link protean to create a negatively charged aggregate and migration pathway
May promote chondrocyte proliferation and diferentiation
Hylauronic Acid (HA) Endrogenous HA
Produced by Synovioum (Type B synoviocytes, Fibroblasts)
In the arthritic joint:
Reduction in HA concentration and molecular weight by 33 – 50%.
Inflammatory effusion, molecular fragmentation, abnormal synoviocyte production
Mechanism of Action: Unknown, thought to exert anti-inflammatory, analgesic and
possibly chondroprotective effects on the joint synovium and cartilage.

Six Synthetic HA injections approved for use.
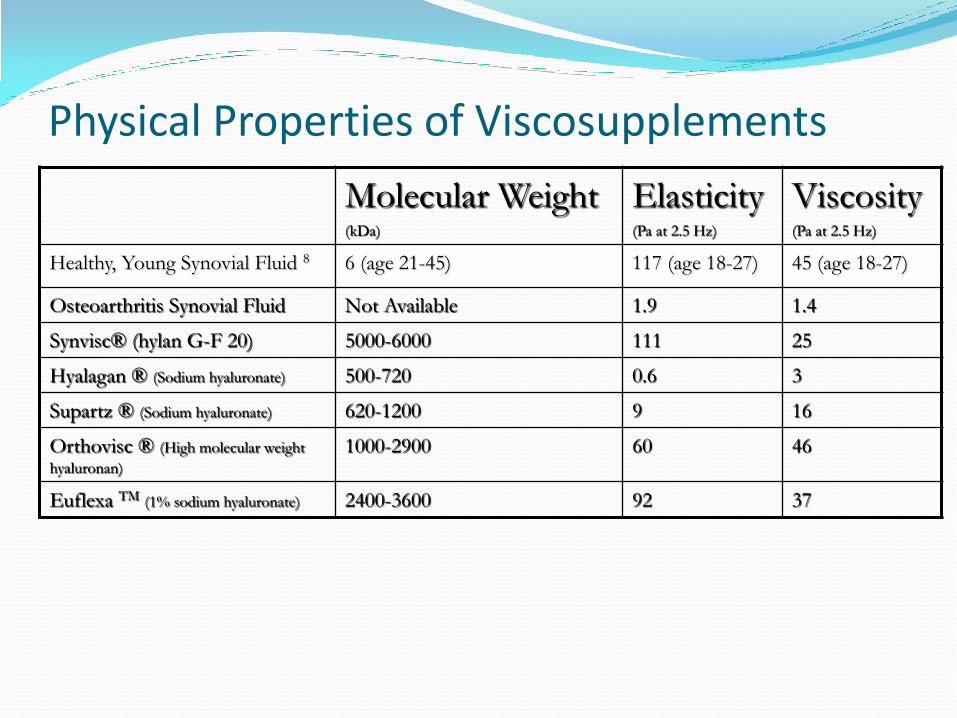
Physical Properties of Viscosupplements
Molecular Weight (kDa)
Elasticity (Pa at 2.5 Hz)
Viscosity (Pa at 2.5 Hz)
Healthy, Young Synovial Fluid 8 6 (age 21-45) 117 (age 18-27) 45 (age 18-27)
Osteoarthritis Synovial Fluid Not Available 1.9 1.4
Synvisc® (hylan G-F 20) 5000-6000 111 25
Hyalagan ® (Sodium hyaluronate) 500-720 0.6 3
Supartz ® (Sodium hyaluronate) 620-1200 9 16
Orthovisc ® (High molecular weight
hyaluronan)
1000-2900 60 46
Euflexa TM (1% sodium hyaluronate) 2400-3600 92 37
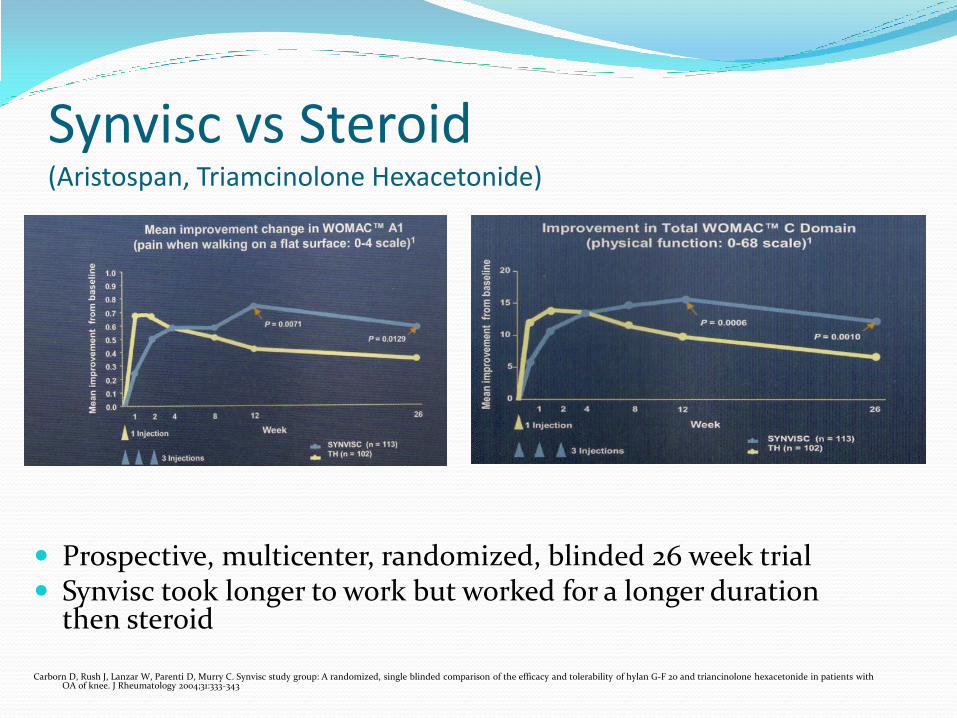
Synvisc vs Steroid
(Aristospan, Triamcinolone Hexacetonide)
Prospective, multicenter, randomized, blinded 26 week trial Synvisc took longer to work but worked for a longer duration
then steroid Carborn D, Rush J, Lanzar W, Parenti D, Murry C. Synvisc study group: A randomized, single blinded comparison of the efficacy and tolerability of hylan G-F 20 and triancinolone hexacetonide in patients with
OA of knee. J Rheumatology 2004;31:333-343
Viscosupplementation Indications:
Patient with Osteoarthritis who has failed or is unable to participate in basic conservative treatment
Only approved for the knee joint (US)
Precautions With Physical Therapy
Avoid repetitive “high level activity” for first 24 – 48 hours
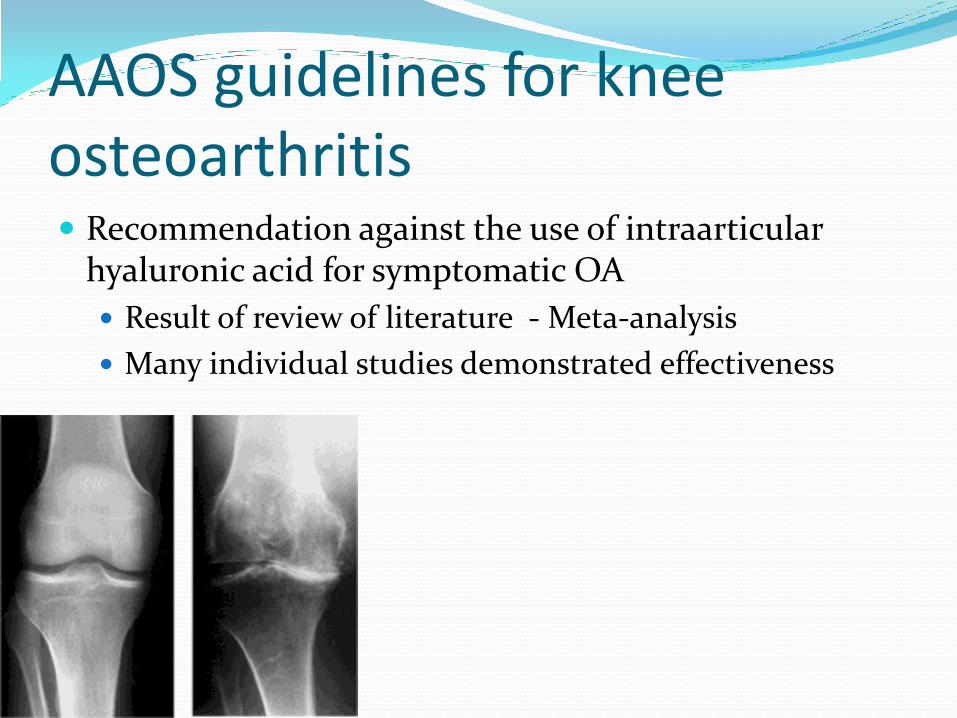
AAOS guidelines for knee osteoarthritis Recommendation against the use of intraarticular
hyaluronic acid for symptomatic OA
Result of review of literature - Meta-analysis
Many individual studies demonstrated effectiveness

Platelet-Rich Plasma Autologus blood fraction rich in platelets
Injected to region of poor or delayed heeling
Theory: Platelets are first to arrive at site of tissue injury, release growth factors that are critical to the heeling
process
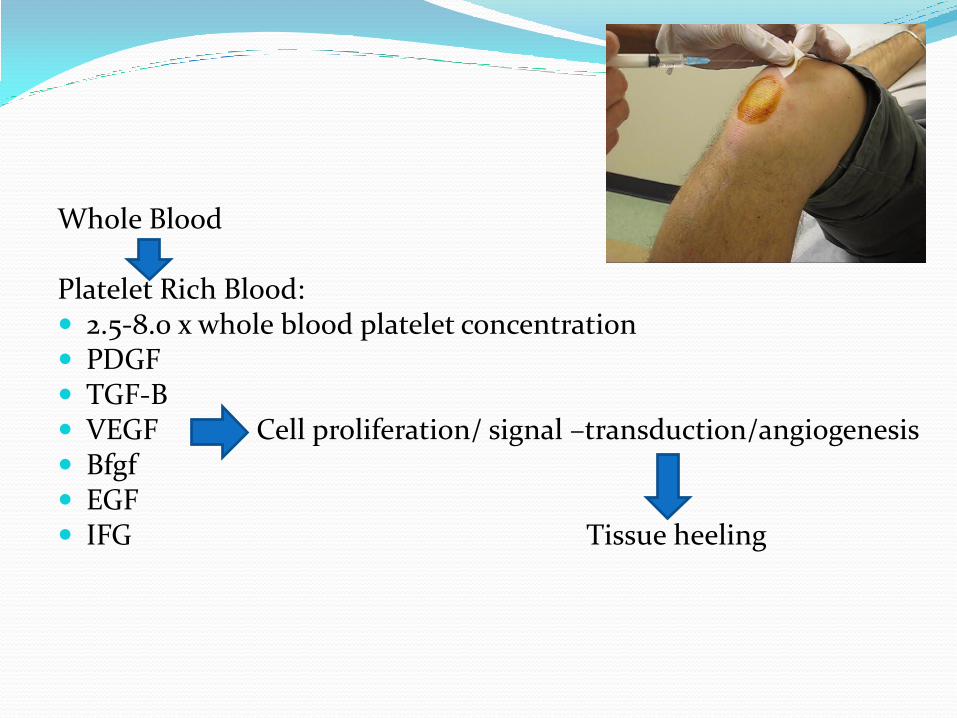
Whole Blood Platelet Rich Blood: 2.5-8.0 x whole blood platelet concentration PDGF TGF-B VEGF Cell proliferation/ signal –transduction/angiogenesis Bfgf EGF IFG Tissue heeling
Numerous
Systems
Achilles Tendinopathy One year follow up of PRP for chronic Achilles
Tendonapathy: Double blinded Placebo-controlled trial (de Jonge et al, 2011):
No statistical difference at one year follow up Recover platelet seperation system
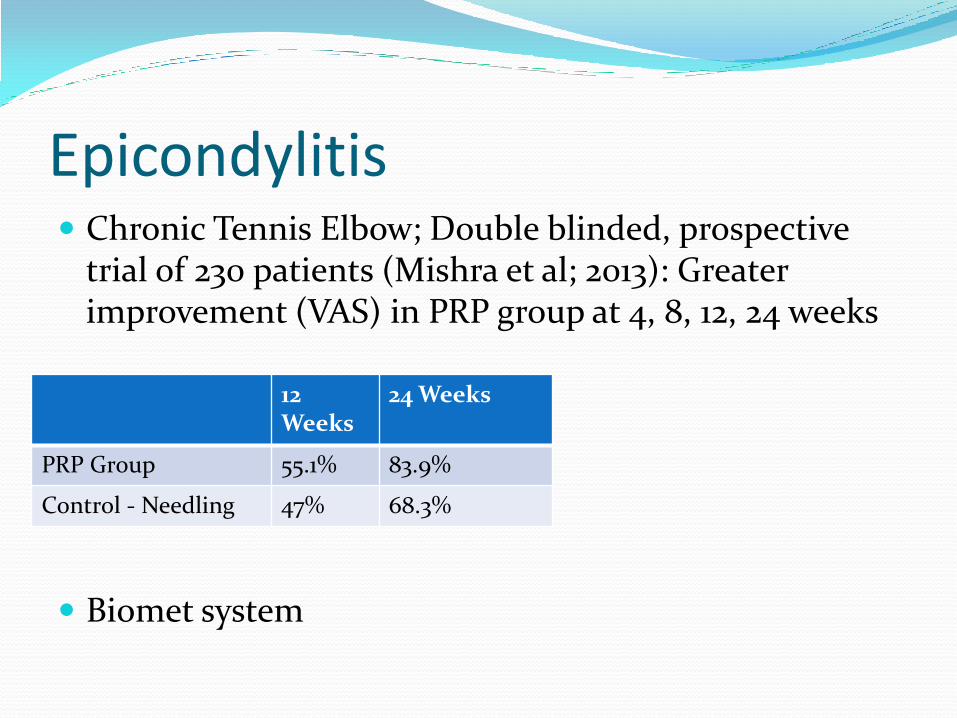
Epicondylitis Chronic Tennis Elbow; Double blinded, prospective
trial of 230 patients (Mishra et al; 2013): Greater improvement (VAS) in PRP group at 4, 8, 12, 24 weeks
Biomet system
12 Weeks
24 Weeks
PRP Group 55.1% 83.9%
Control - Needling 47% 68.3%
Osteoarthritis
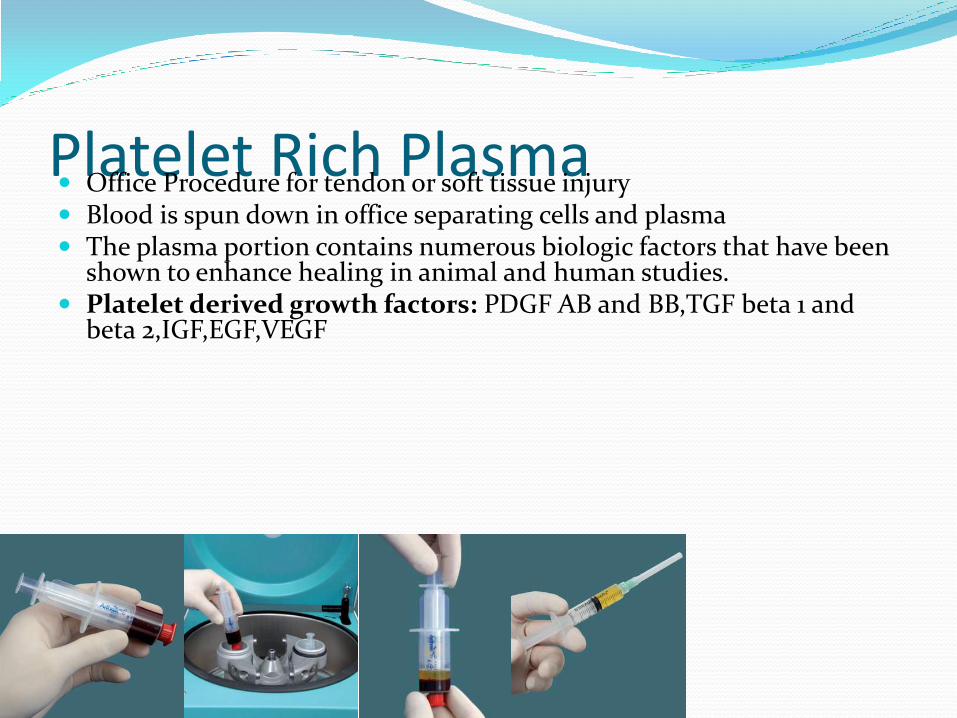
Platelet Rich Plasma Office Procedure for tendon or soft tissue injury Blood is spun down in office separating cells and plasma The plasma portion contains numerous biologic factors that have been
shown to enhance healing in animal and human studies. Platelet derived growth factors: PDGF AB and BB,TGF beta 1 and
beta 2,IGF,EGF,VEGF
Prolotherapy Injection of non-phamacological irritant solution
(Dextrose)
Theory: Decreasing pain and repairing tissue by reinitiating the inflammatory process
Mechanism of Action: Unknown
May involve multiple treatment sessions each costing 200-1000$
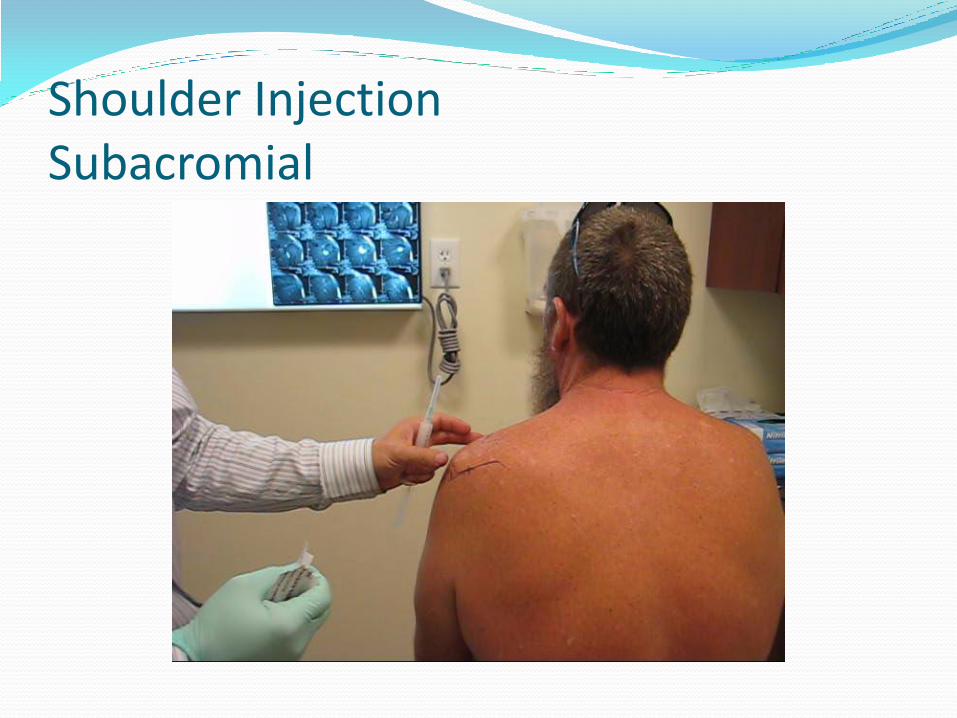
Shoulder Injection Subacromial
Shoulder Injection Subacromial Common injection issues
Encounter bone
Redirect needle in a downward fashion, around prominent acromian or superiorly if the humerous is the obstruction.
Post-injection care
Pain may worsen 24-48 hours after injection
Post-injection examination (diagnostic portion)
TLC Physical Therapy or hold off a few days
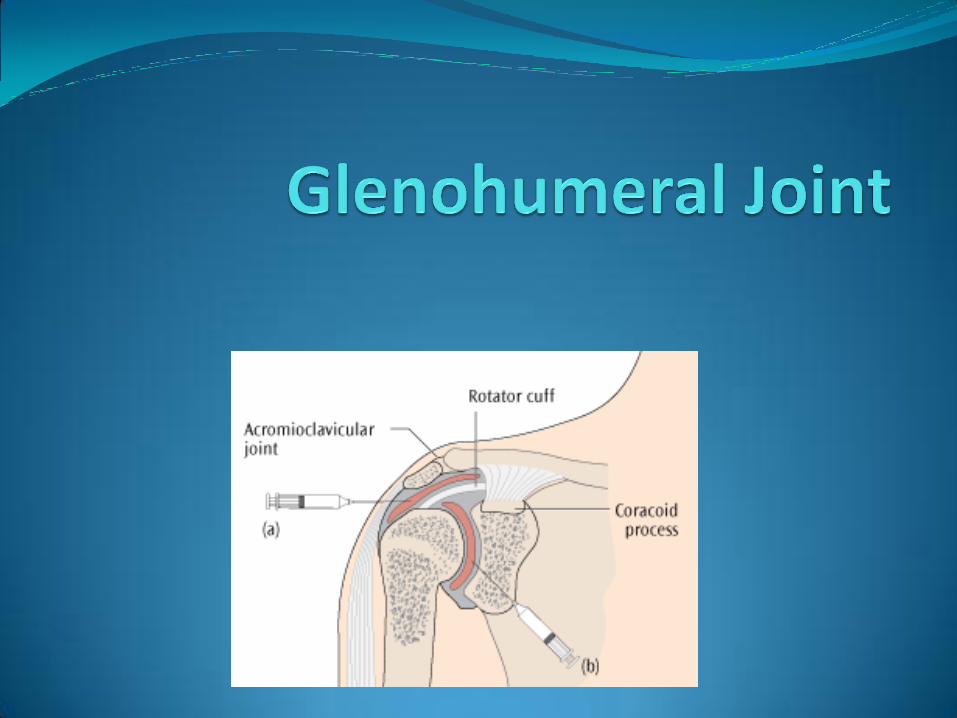
Shoulder Injection Glenohumeral Indications
Adhesive capsulitis
Osteoarthritis
Aspiration to rule out infection
Risks
Infection
Cartilage Injury
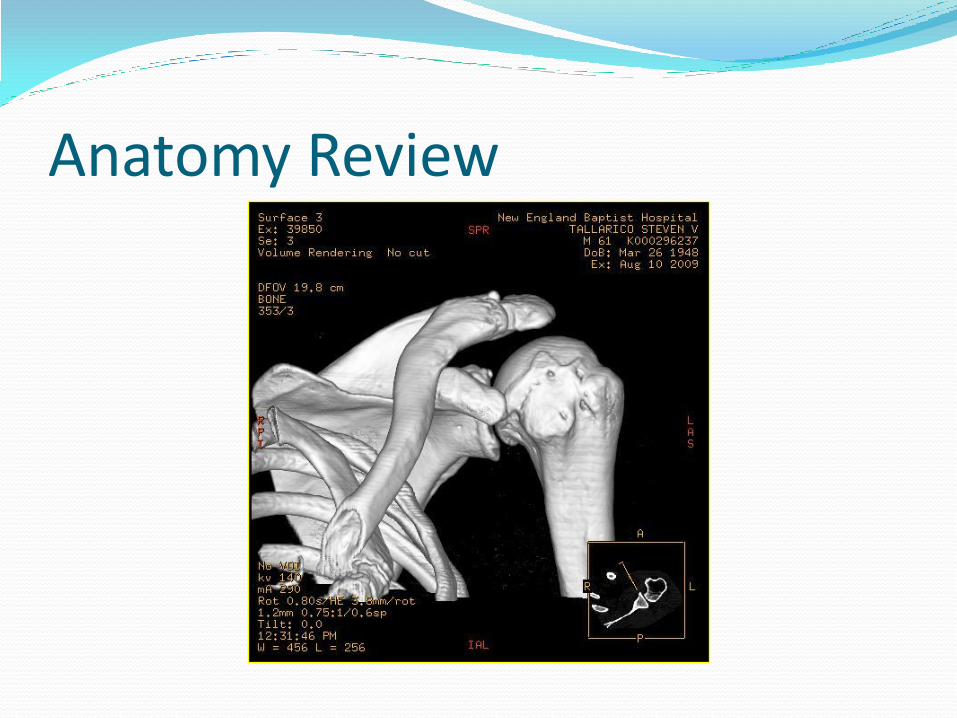
Anatomy Review

Shoulder Injection Glenohumeral Structures to avoid
Axillary Nerve
Articular cartillage
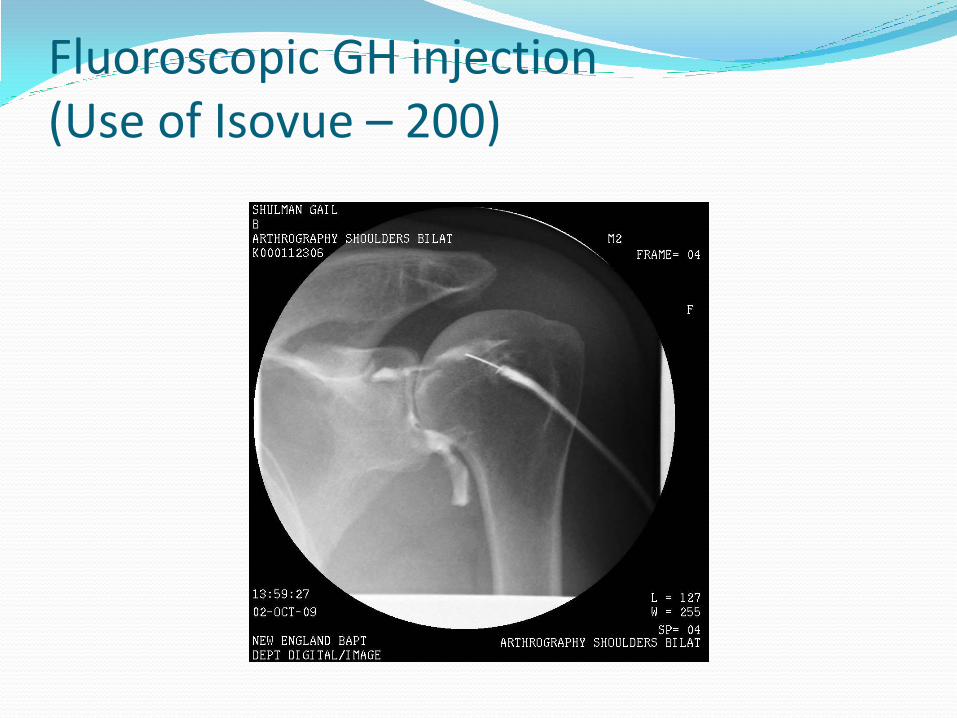
Fluoroscopic GH injection (Use of Isovue – 200)

Glenohumeral Injection (fluroscopic assist)

Glenohumeral Injection (fluroscopic assist)

Glenohumeral Injection (fluroscopic assist)

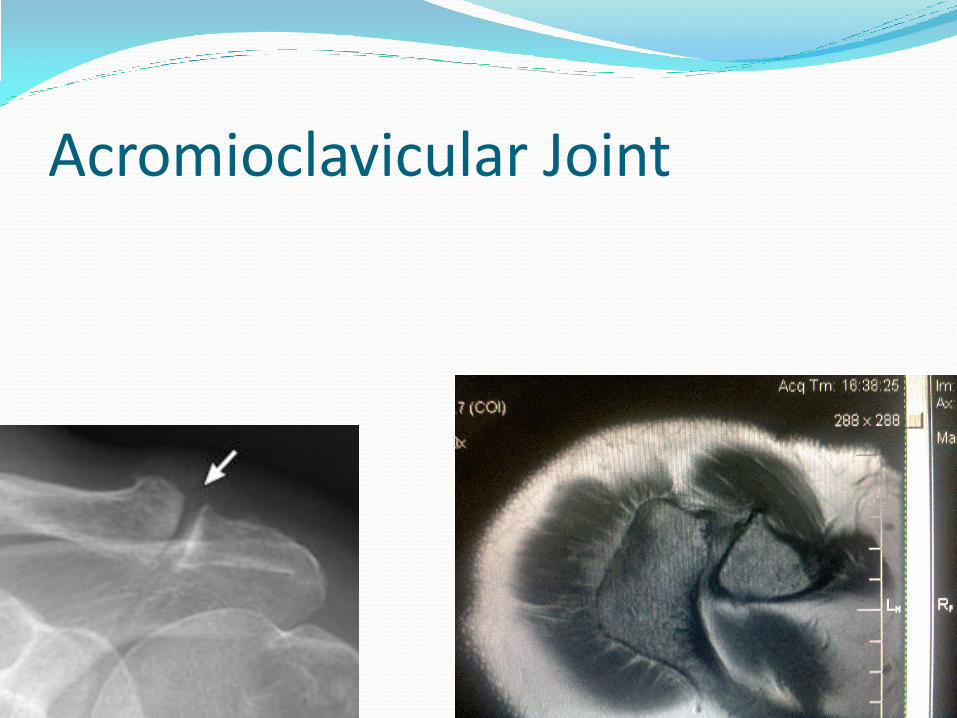
Acromioclavicular Joint

Acromioclavicular Joint

Common Injections Elbow joint – OA/RA
Olecranon Bursitis
Medial and Lateral Epicondyles
Aspiration: Fracture, gout
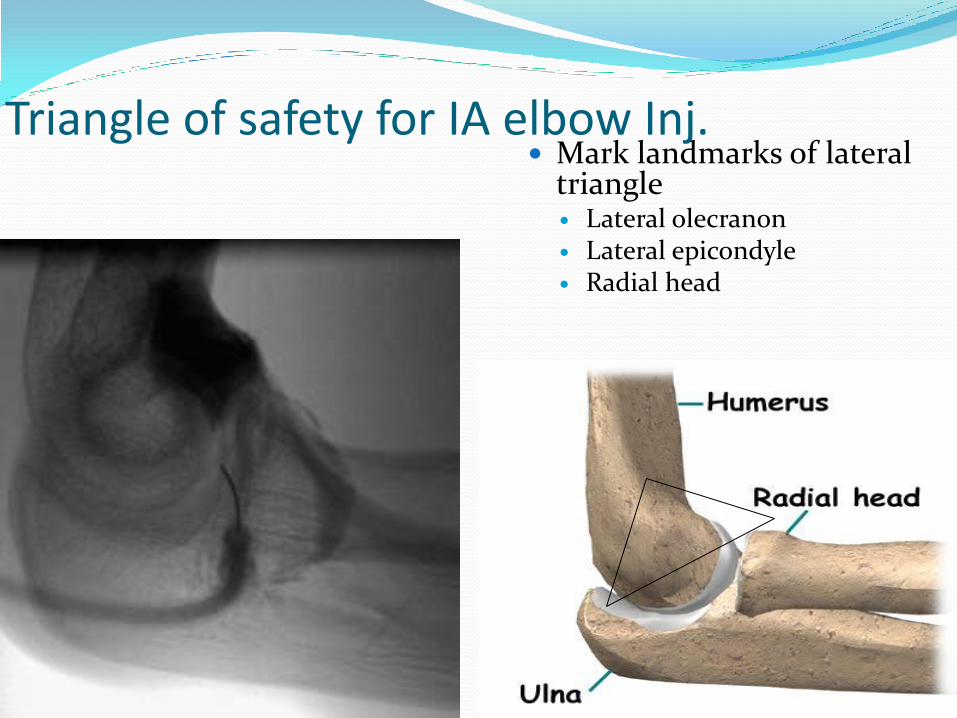
Triangle of safety for IA elbow Inj. Mark landmarks of lateral
triangle Lateral olecranon Lateral epicondyle Radial head
Medial and Lateral Epicondylitis
Injection for epicondylitis (opathy) Used in conjunction with Physical Therapy
Procedure as well as an injection
Mobilize needle within tendon during injection
Ouch! Pain prescription ?

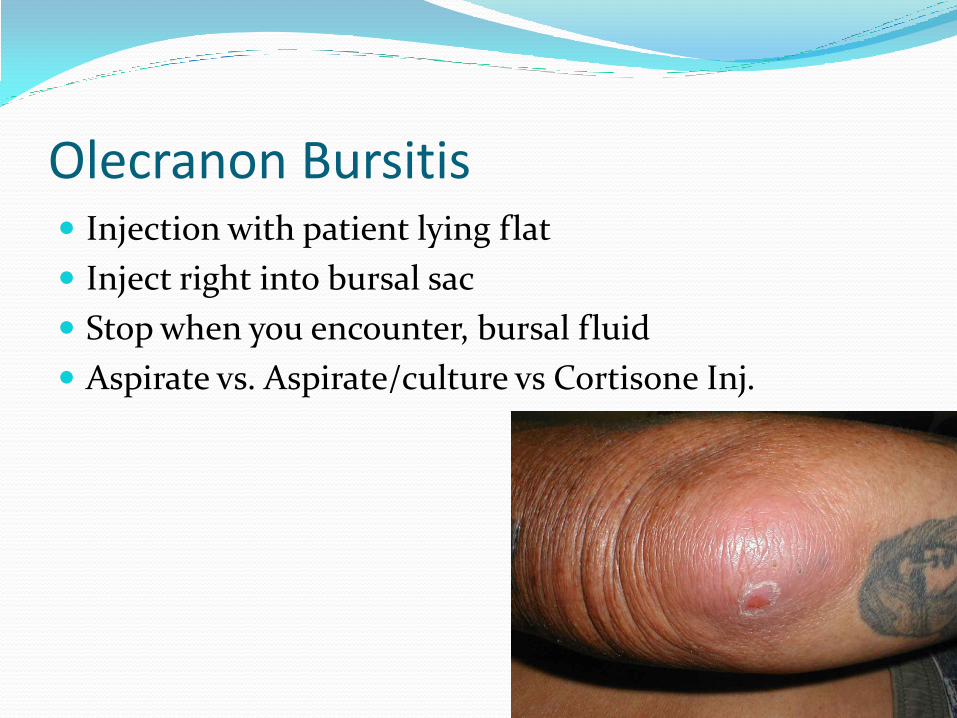
Olecranon Bursitis Injection with patient lying flat
Inject right into bursal sac
Stop when you encounter, bursal fluid
Aspirate vs. Aspirate/culture vs Cortisone Inj.


Ankle Joint Injection Indications for Injection
Diagnostic Suspected septic arthritis
Evaluation of joint effusion
Identification of intra-articular fracture
Identification of crystal arthropathy
Therapeutic Relief of pain by aspirating effusion or
blood
Injection of medications (eg, corticosteroids, anesthetics)
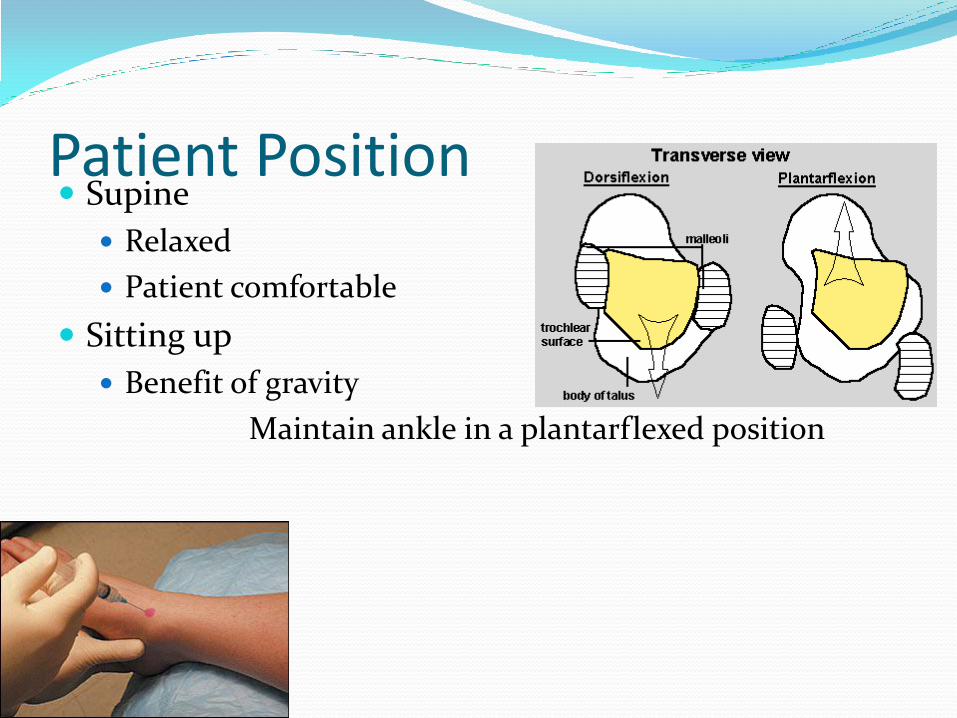
Patient Position Supine
Relaxed
Patient comfortable
Sitting up
Benefit of gravity
Maintain ankle in a plantarflexed position
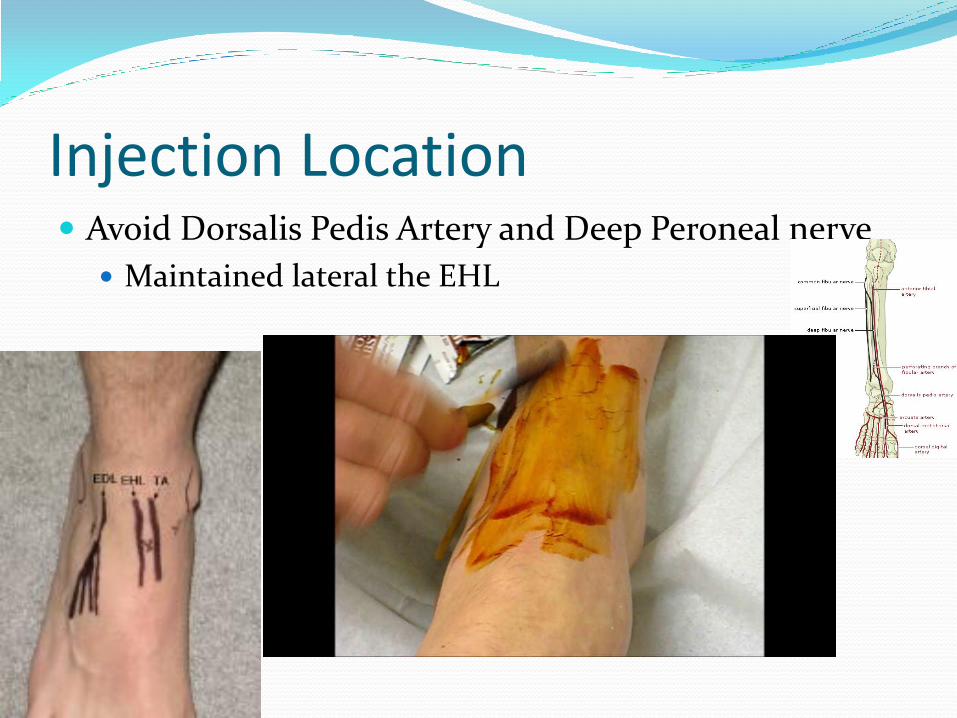
Injection Location Avoid Dorsalis Pedis Artery and Deep Peroneal nerve
Maintained lateral the EHL
Hip Injection
Indications
OA
RA
Labral Tear
Anterior Technique
Patient supine with hip slightly flexed and IR
Femoral artery is palpated
Point of entry: 2 cm inferior to the inguinal ligament
Hip Injection Best done under fluoroscopy
Hard to confirm placement
Most get fluid back to confirm placement
Shown to be very challenging as in office procedure 1
Anterior approach was successful in only 60% of injections,
The needle pierced or contacted the femoral nerve in 27% of anterior injections and was within 5 mm of the femoral nerve in 60% of anterior attempts
Leopold SS, Battista V, Oliverio JA. Safety and efficacy if intraaticular hip injection using
anatomical landmarks. Arthritis Rheum 2001; 44: 2449-50.

Trochanteric Bursitis
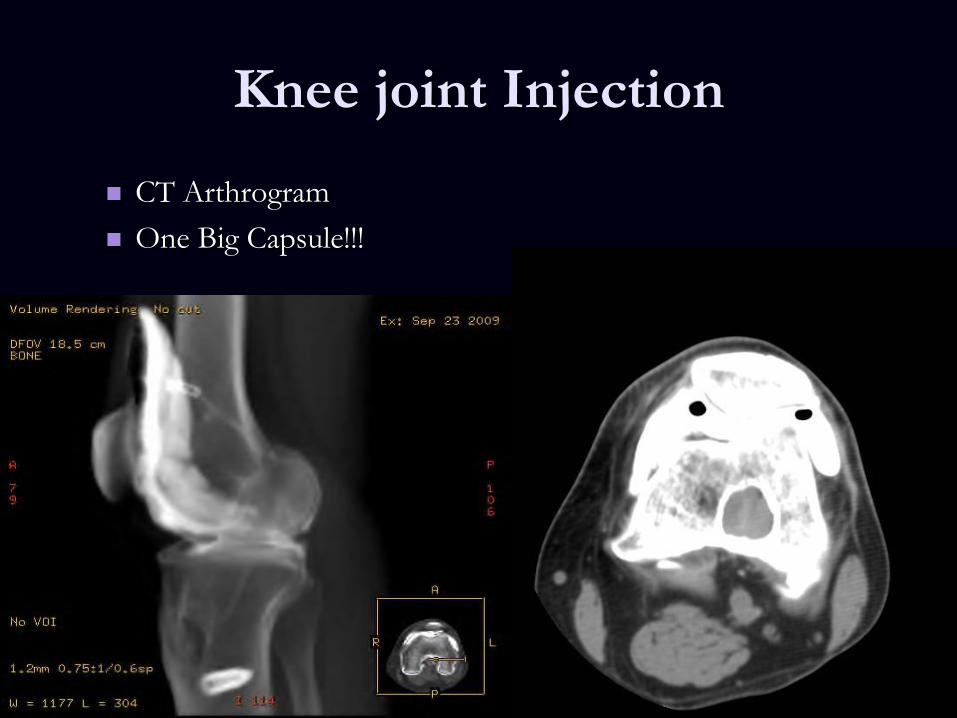
Knee joint Injection
CT Arthrogram
One Big Capsule!!!
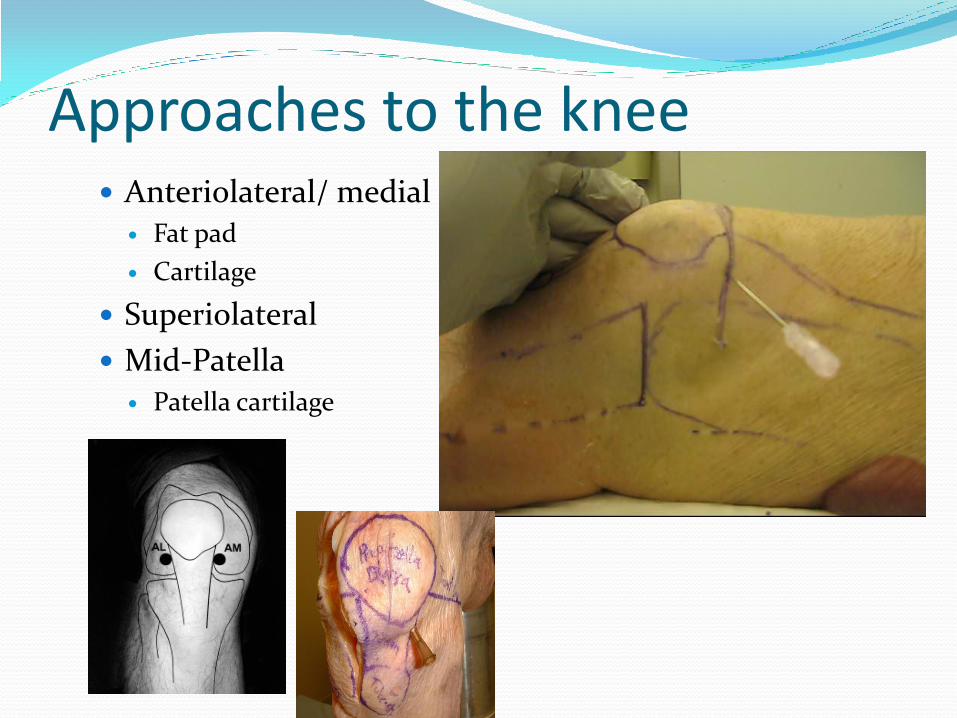
Approaches to the knee Anteriolateral/ medial
Fat pad
Cartilage
Superiolateral
Mid-Patella Patella cartilage



Thank You! Jason Rand PA-C, PT [email protected]
Jason Rand PA-C, PT
Boston Sports and Shoulder Center
Boston Celtics Medical Team
New England Baptist Hospital – Sports Medicine
Service