intrahepatic bile duct damage in children with kawasaki disease
TRANSCRIPT

7 5 0 Clinical and laboratory observations The Journal of Pediatrics May 1992
Intrahepatic bile duct damage in children with Kawasaki disease
Brigitte Bader-Meunier , MD, Michel le Hadchoue l , MD, Mon ique Fabre, MD, Marc Duval Arnoud, MD, and Jean Paul Dommergues , MD
From the Departement de P6diatrie and Unit6 de Recherche d'H~patologie P6diatrique INSERM U56, and the Laboratoire d'Anatomopathologie, H6pital de Bic~tre, Paris, France
Three children with Kawasaki disease had liver biopsies because of evidence of hepatic disease. Cholangitis or bile duct injury and proliferation were found. Similar d a m a g e to the hepatic ductular system may explain the hydrops of the gal lb ladder sometimes seen in this disease. (J PEDIATR 1992;120:750-2)
The association of Kawasaki syndrome with gallbladder hydrops 1 or hepatobiliary dysfunction has been reported, 2 but little is known about the pathologic changes in the liver. We describe three children with intrahepatic bile duct damage associated with Kawasaki disease.
M E T H O D S
Patients. Three children aged 3V2, 6, and 10 years, respectively, were admitted to the pediatric department of H6pital de Bic~tre because of suspected Kawasaki disease. They had had fever for more than 5 days, and had at least four of the following clinical features: (1) bilateral nonex- udative conjunctivitis, (2) polymorphous exanthem, (3) cervical lymphadenopathy, indurative edema, and desqua- mation of the hands and feet, (4) pharyngitis and straw- berry tongue, and (5) red, fissured lips.
All children were brought to our attention because of the association of Kawasaki disease and hepatobiliary dysfunc- tion. They were examined within 10 days of the onset of fe- ver; the erythrocyte sedimentation rate and initial leukocyte count were increased. Blood cultures were negative for bac- teria. An echocardiogram showed no coronary aneurysm. Two children received intravenous infusions of immune globulin (one a 2-day course, 1 gm/kg per day, and one a 3-day course, 400 mg/kg per day).
Hepatic function evaluation. The three children had ad- ditional liver function tests, abdominal ultrasonography, and serologic studies for hepatitis A and B, Epstein-Barr virus, cytomegalovirus, and mycoplasma; liver needle bi-
Submitted for publication April 11, 1991; accepted Dec. 12, 1991. Reprint requests: B. Bader-Meunier, MD, Service de P6diatrie" g6n6rale, H6pital de Bic&re, 78, Rue du G6n6ral Leclerc, 94270 Le Kremlin Bic~tre, France. 9/22/35570
opsy was performed aiter informed parental consent was obtained.
R E S U L T S
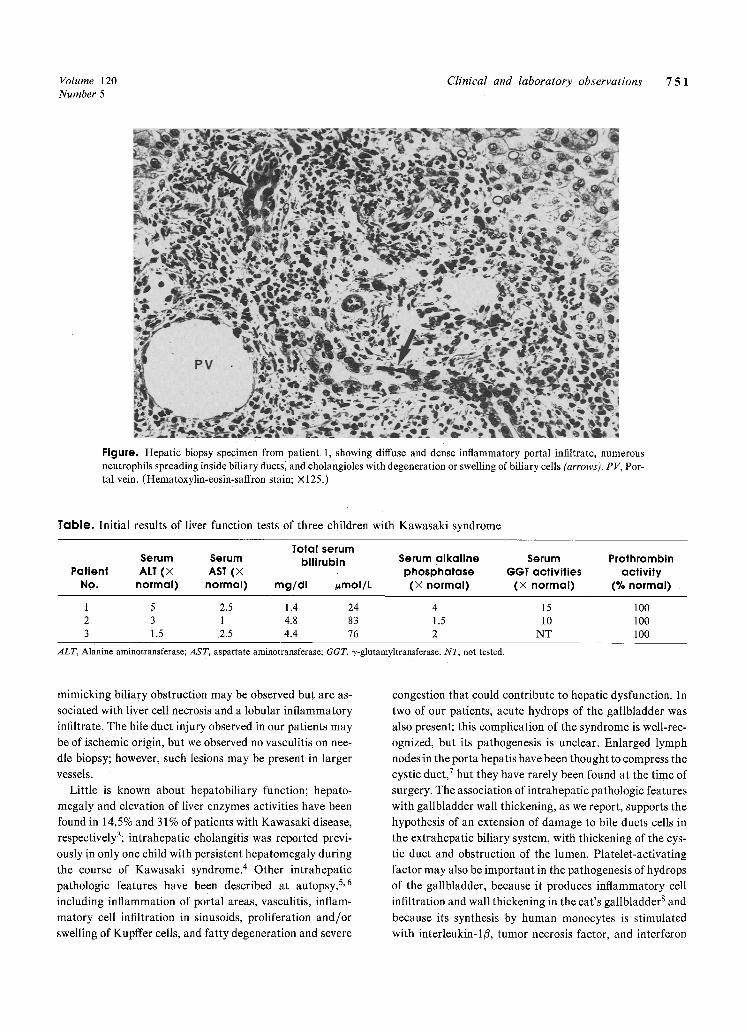
The three children were jaundiced, and physical exami- nation revealed an enlarged liver. Moderate conjugated hy- perbilirubinemia was present; serum aminotransferase ac- tivity and the total serum bilirubin level were moderately increased, and serum 3,-glutamyltransferase activity was markedly increased in patients 1 and 2 but was not tested in patient 3 (Table). Abdominal ultrasonography revealed homogeneous hepatomegaly and, in two patients, hydrops of the gallbladder with a thickened wall. Results of all se- rologic studies were negative. A liver biopsy specimen showed injury of the small bile ducts in all patients. In two patients, we observed features of cholangitis: the presence of an inflammatory infiltrate consisting primarily of poly- morphonuclear leukocytes and localized around and within the lumina of bile ducts, in association with slight ductular proliferation (Figure). In the third patient, bile duct el6ithelial cell injury and necrosis were more prominent than inflammatory infiltrate, but slight ductular proliferation was also observed; middle fibrosis was also present. There was no arterial lesion or lobular injury.
Serum aminotransferase, alkaline phosphatase, and 3,-glutamyltransferase activities began to decrease shortly after immune globulin therapy in two children, and sponta- neously in the third; liver size and liver function were nor- mal 1 month later.
D I S C U S S I O N
Our three patients had intrahepatic cholangitis and intrahepatic bile duct epithelium necrosis in association with Kawasaki disease. There was no lobular injury, in contrast with acute viral hepatitis, in which portal changes
Volume 120 Clinical and laboratory observations 75 1 Number 5
Figure. Hepatic biopsy specimen from patient 1, showing diffuse and dense inflammatory portal infiltrate, numerous neutrophils spreading inside biliary ductsl and cholangioles with degeneration or swelling of biliary cells (arrows). PV, Por- tal vein. (Hematoxylin-eosin-saffron stain; x125.)
Table. Initial results of liver function tests of three children with Kawasaki syndrome
Total serum Serum Serum bilirubin Serum alkaline Serum Prothrombin
Patient ALT (X AST (X phosphatase GGT activities activity No. normal) normal) mg/dl #mol/L (X normal) (X normal) (% normal)
1 5 2.5 1.4 24 4 15 100 2 3 1 4.8 83 1.5 10 100 3 1.5 2.5 4.4 76 2 NT 100
ALT, Alanine aminotransferase; AST, aspartate aminotransferase; GGT, 3,-glutamyltransferase. NT, not tested.
mimicking biliary obstruction may be observed but are as- sociated with liver cell necrosis and a lobular inflammatory infiltrate. The bile duct injury observed in our patients may be of ischemic origin, but we observed no vasculitis on nee- dle biopsy; however, such lesions may be present in larger vessels.
Little is known about hepatobiliary function; hepato- megaly and elevation of liver enzymes activities have been found in 14.5% and 31% of patients with Kawasaki disease, respectively3; intrahepatic cholangitis was reported previ- ously in only one child with persistent hepatomegaly during the course of Kawasaki syndrome. 4 Other intrahepatic pathologic features have been described at autopsy, 5,6 including inflammation of portal areas, vasculitis, inflam- matory cell infiltration in sinusoids, proliferation and/or swelling of Kupffer cells, and fatty degeneration and severe
congestion that could contribute to hepatic dysfunction. In two of our patients, acute hydrops of the gallbladder was also present; this complication of the syndrome is Well-rec- ognized, but its pathogenesis is unclear. Enlarged lymph nodes in the porta hepatis have been thought to compress the cystic duct, 7 but they have rarely been found at the time of surgery. The association of intrahepatic pathologic features with gallbladder wall thickening, as we report, supports the hypothesis of an extension of damage to bile ducts cells in the extrahepatic biliary system, with thickening of the cys- tic duct and obstruction of the lumen. Platelet-activating factor may also be important in the pathogenesis of hydrops of the gallbladder, because it produces inflammatory cell infiltration and wall thickening in the cat's gallbladder 8 and because its synthesis by human monocytes is stimulated with interleukin-1/3, tumor necrosis factor, and interferon

7 5 2 Clinical and laboratory observations The Journal of Pediatrics May 1992
gamma, 9 levels of which increase during the course of Ka- wasaki syndrome. 1~ 11
Immune globulin has been proved effective in the treat- ment of Kawasaki disease. 12 The use of immune globulin might have contributed to the regression of the hepatobil- iary abnormalities in two of our patients, but liver enzyme activities spontaneously returned to normal values in the third child.
These case reports suggest that intrahepatic bile duct damage should be added to the list of complications of Ka- wasaki disease.
R E F E R E N C E S
1. Magilavy DB, Speert DP, Silver TM, et al. Mucocutaneous lymphnode syndrome: report of two cases complicated by gall- bladder hydrops and diagnosed by ultrasound. Pediatrics 1978;61:699-702.
2. Melish M, Hicks RV, Reddy V. Kawasaki syndrome: an up- date. Hosp Pract 1982;17:99-106.
3. Burns JC, Mason WH, Glode MP, et al. Clinical and epide- miologic characteristics of patients referred for evaluation of possible Kawasaki disease. J PEDIATR 1991;118:680-6.
4. Edwards KM, Glick AD, Grenne HL. Intrahepatic cholangi-
tis associated with mucocutaneous lymph node syndrome. J Pediatr Gastroenterol Nutr 1985;4:140-2.
5. Amano S, Hazama F, Kubagawa H, et al. General pathology of Kawasaki disease. Acta Pathol Jpn 1980;30:681-94.
6. Ohshio G, Furukawa F, Fujiwara H, et al. Hepatomegaly and splenomegaly in Kawasaki disease. Pediatr Pathol 1985;4:257- 64.
7. Mofenson HC, Greensher J, Molavi M. Gallbladder hydrops: complication of Kawasaki disease. NY State J Med 1980; 80:249-51.
8. Kaminski DL, Andrus CH, German D, et al. The role of pros- tanoids in the production of acute acalculous cholecystis by platelet-activating factor. Ann Surg 1990;212:455-61.
9. Valone FH, Epstein LB. Biphasic platelet-activating factor synthesis by human monocytes stimulated with IL-I/~, tumor necrosis factor, or IFN-3,. J Immunol 1988;141:3945-50.
10. Rowley AH, Shulman ST, Preble OT, et al. Serum interferon concentrations and retroviral serology in Kawasaki syndrome. Pediatr Infect Dis J 1988;7:663-6.
11. Leung DY, Geha RS, Newburger JW, et al. Two monokines, interleukin-1/3 and tumor necrosis factor, render cultured vas- cular endothelial cells susceptible to lysis by antibodies circu- lating during Kawasaki syndrome. J Exp Med 1986;164:1958- 72.
12. Newburger JW, Takahashi M, Burns JC, et al. The treatment of Kawasaki syndrome with intravenous gamma globulin. N Engl J Med 1986;315:341-7.
Successful use of a metal detector in locating coins ingested by children
Simon P, Ros, MD, a n d Frank C e t t a , MD
From the Department of Pediatrics, Loyola University Medical Center, Maywood, Illinois
The purpose of this study was to examine the accuracy of a metal detector in locating coins ingested by children. The metal detector correctly identified the presence or absence of coins in 43 patients (93%), as confirmed by radiologic studies. (J PEDIATR 4992;120:752-3)
Coins are frequently ingested by children. Litovitz et al., 1 in their summary of data from 70 poison control centers, reported 5185 cases of coin ingestion by children in 1989. Although radiologic examination of all children after coin ingestion has been advocated, a recent survey in Salt Lake City, Utah, indicated that 77% of practicing pediatricians do not routinely obtain roentgenograms of symptom-free
Submitted for publication May 15, 1991; accepted Oct. 4, 1991. Reprint requests: Simon P. Ros, MD, Department of Pediatrics, Loyola University Medical Center, 2160 South First ~Ave., May- wood, IL 60153. 9/22/34168
patients. 2 Furthermore, only 1696 patients (32%) reported by Litovitz et al. were examined in a health care facility, thus indicating poor compliance~nationwide with the rec- ommendation of radiographic examination of children af- ter a coin ingestion.
We investigated an alternative approach to the evalua- tion of coin ingestions in symptom-free children--the use of a metal detector. We previously described the high accuracy of this device in locating coins in a model simulating inges- tion3; the accuracy of the metal detector in identifying the presence or absence of coins in ou~:model was 100%. The purpose of this study was to validate our findings in the clinical setting of children coming to an emergency depart- ment after a coin ingestion.