intestinal perforation as the initial presentation of wegener’s granulomatosis
TRANSCRIPT
LETTER TO THE EDITOR
Intestinal perforation as the initial presentationof Wegener’s granulomatosis
Hakan Bulus • Erdem Kocak • Alper Yavuz •
Muzaffer Akkoca • Ali coskun • Seyfettin Koklu
Received: 3 March 2012 / Accepted: 23 August 2012
� Springer-Verlag 2012
To the Editor
Wegener’s granulomatosis is a necrotizing vasculitis of
unknown etiology characterized mainly by inflammation of
the small- and medium-sized arteries and veins that affect
any viscera [1]. Gastrointestinal involvement is rather
uncommon and is presented with mild-to-severe life-
threatening complications. We report a female patient with
WG who presented with massive intestinal perforation as
the initial presentation.
A 47-year-old female patient was admitted to our hos-
pital with the complaints of abdominal pain, nausea, and
vomiting. On physical examination, blood tension was
100/60 mmHg; pulse rate, 115/min; and the temperature,
39 �C. Abdominal examination revealed diffuse rebound
tenderness and diminished bowel sounds. Her detailed
history revealed that she had been admitted to another
hospital because of recurrent sinusitis two weeks ago. She
had been treated with antibiotics and nasal decongestants.
Initial laboratory findings were as follows: serum hemo-
globin, 8.1 g/dl; white cell count, 21,000/mm3; and platelet
count, 125,000/mm3; erythrocyte sedimentation rate,
68 mm/h; and positive anti-neutrophil cytoplasmic anti-
body (c-ANCA). Her liver and renal functional tests were
normal. Chest X-ray showed multiple round opacities in
the right lung, and the plain abdominal radiograph revealed
subdiaphragmatic free air. Contrast-enhanced computer-
ized tomography scan showed small bowel thickening with
intra-abdominal free air and fluid. The patient was operated
in the emergent condition with these findings. During
surgery, multiple ischemic, necrotic, and perforated areas
in the jejunal and ileal regions were detected. After intra-
abdominal irrigation, massive small intestinal resection and
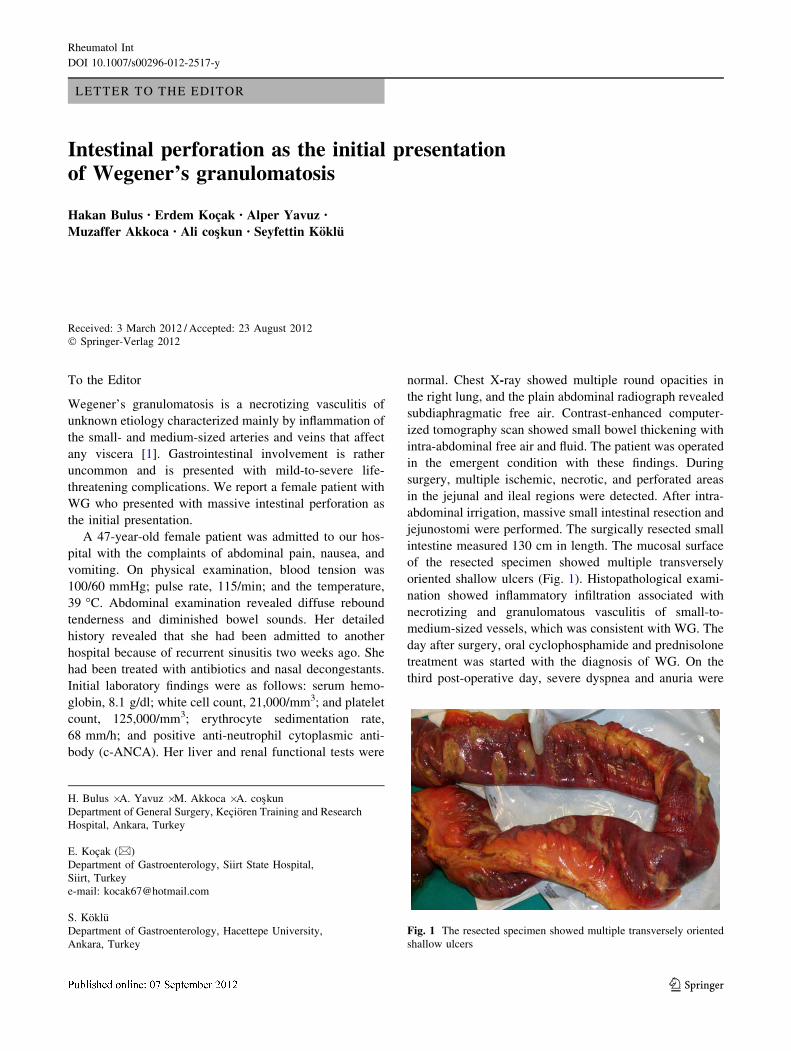
jejunostomi were performed. The surgically resected small
intestine measured 130 cm in length. The mucosal surface
of the resected specimen showed multiple transversely
oriented shallow ulcers (Fig. 1). Histopathological exami-
nation showed inflammatory infiltration associated with
necrotizing and granulomatous vasculitis of small-to-
medium-sized vessels, which was consistent with WG. The
day after surgery, oral cyclophosphamide and prednisolone
treatment was started with the diagnosis of WG. On the
third post-operative day, severe dyspnea and anuria were
H. Bulus � A. Yavuz � M. Akkoca � A. coskun
Department of General Surgery, Kecioren Training and Research
Hospital, Ankara, Turkey
E. Kocak (&)
Department of Gastroenterology, Siirt State Hospital,
Siirt, Turkey
e-mail: [email protected]
S. Koklu
Department of Gastroenterology, Hacettepe University,
Ankara, Turkey
Fig. 1 The resected specimen showed multiple transversely oriented
shallow ulcers
123
Rheumatol Int
DOI 10.1007/s00296-012-2517-y

developed and the patient was died due to multiorgan
failure.
Essentially, all patients with WG present with upper
airway or pulmonary involvement, and the majority have
both. Because of its variable presentation, there is often a
delay in the diagnosis. It can rapidly lead to death in people
with multiple affected organs, who do not get appropriate
treatment. During the course of WG, intestinal involvement
is uncommon and usually detected in autopsy studies [2].
Reviewing the literature, only few cases have been reported
with intestinal perforation associated with WG [3–5]. The
ileal perforation is seen more commonly in men, usually
manifest in age between age 26 to 56, and occur within the
first year of the disease [6].
The present case had been admitted to another hospital
two weeks before intestinal perforation. At that time, the
clinicians did not suspected WG, and treatment was
delayed. It has been suggested that severe intestinal
involvement improved after treatment with immunosup-
pressive drugs in patients with WG [7]. In this case, it can
be speculated that early treatment with immunosuppressive
drugs may be prevented severe intestinal perforation.
In conclusion, WG should be suspected in patients with
chronic, unexplained respiratory symptoms and signs. Also
the clinicians should be considered WG in the differential
diagnosis of intestinal perforation.
References
1. Storesund B, Gran JT, Koldingsnes W (1998) Severe intestinal
involvement in Wegener’s granulomatosis: report of two cases and
review of the literature. Br J Rheumatol 37:387–390
2. Walton EW (1958) Giant-cell granuloma of the respiratory tract
(Wegener’s granulomatosis). Br Med J 2:265–270
3. Akca T, Colak T, Caðlykulekci M, Ocal K, Aydyn S (2005)
Intestinal perforation in Wegener’s granulomatosis: a case report.
Ulus Travma Derg 11:348–351
4. Storesund B, Gran JT, Koldingsnes W (1998) Severe intestinal
involvement in Wegener’s granulomatosis: report of two cases and
review of two cases and review of the literature. Br J Rheumatol
37:387–390
5. Demling RH, Salvatierra O, Belzer FO (1975) Intestinal necrosis
and perforation after renal transplantation. Arch Surg 110:251–253
6. Yildirim AC, Kocak E, Yildiz P, Yildiz M, Karakayali AS,
Kaptanoglu B, Koklu S (2010) Multiple intestinal perforation in a
patient with Wegener’s granulomatosis: a case report and review
of the literature. Gastroenterol Clin Biol 34:712–715
7. Haworth SJ, Pusey CD (1984) Severe intestinal involvement in
Wegener’s granulomatosis. Gut 25:1296–1300
Rheumatol Int
123