interpretation of medical literature statistics karen pieper, ms duke clinical research institute
TRANSCRIPT

Interpretation Interpretation of Medical Literature of Medical Literature StatisticsStatistics
Karen Pieper, MSKaren Pieper, MSDuke Clinical Research InstituteDuke Clinical Research Institute

www.mc.vanderbilt.edu/prevmed/ps
Website for Power and Sample Size program used in Website for Power and Sample Size program used in second classsecond class

To be an informed consumer of publishedTo be an informed consumer of publishedstatistical analyses, one should know:statistical analyses, one should know:
■ What needs to appear in a manuscriptWhat needs to appear in a manuscript
■ What to keep in mind when looking at data What to keep in mind when looking at data
■ The dangers of subgroup analysesThe dangers of subgroup analyses

Prior CABG Prior CABG No Prior CABG No Prior CABG No Enrolling MI No Enrolling MI
Enrolling MI Enrolling MI DM DM
No DMNo DM65 or Older 65 or Older
Under 65 Under 65 Female Female
Male Male OverallOverall
0.50.5 11 22
0.89 (0.79, 0.99) 0.89 (0.79, 0.99)
0.79 (0.69, 0.91)0.79 (0.69, 0.91)
1.10 (0.91, 1.34)1.10 (0.91, 1.34)
0.78 (0.66, 0.93)0.78 (0.66, 0.93)
0.98 (0.84, 1.13)0.98 (0.84, 1.13)
0.87 (0.76, 1.00)0.87 (0.76, 1.00)
0.96 (0.77, 1.19)0.96 (0.77, 1.19)
0.93 (0.80, 1.08)0.93 (0.80, 1.08)
0.85 (0.72, 1.00)0.85 (0.72, 1.00)
0.89 (0.79, 1.00)0.89 (0.79, 1.00)
0.90 (0.66, 1.24)0.90 (0.66, 1.24)
Death or MI at 30 DaysDeath or MI at 30 Days

PRISMPRISM
PRISM+PRISM+
PARAGON-APARAGON-A
PURSUITPURSUIT
PARAGON-BPARAGON-B
GP IIb/IIIa GP IIb/IIIa BetterBetter
Placebo/ Placebo/ Control Control BetterBetter
GUSTO-IVGUSTO-IV
AllAll
GP IIb/IIIa GP IIb/IIIa BetterBetter
Placebo/ Placebo/ Control Control BetterBetter
FemaleFemale MaleMale
0.50.5 11 22 0.50.5 11 22
OR and 95% CIOR and 95% CI OR and 95% CIOR and 95% CI

Sex IssueSex IssueOR (95% CI)OR (95% CI) P-value forP-value for
MalesMales FemalesFemales Heterogeneity Heterogeneity
All patientsAll patientsDeathDeath 0.83 (0.71-0.96)0.83 (0.71-0.96) 1.08 (0.89-1.33)1.08 (0.89-1.33) 0.0300.030Death or MIDeath or MI 0.81 (0.75-0.89)0.81 (0.75-0.89) 1.15 (1.01-1.30)1.15 (1.01-1.30) < 0.0001< 0.0001
Patients with missing data on baseline cardiac troponinPatients with missing data on baseline cardiac troponinDeathDeath 0.81 (0.67-0.98)0.81 (0.67-0.98) 1.20 (0.93-1.55)1.20 (0.93-1.55) 0.0110.011Death or MIDeath or MI 0.78 (0.70-0.86)0.78 (0.70-0.86) 1.18 (1.02-1.36)1.18 (1.02-1.36) < 0.0001< 0.0001
Patients with data on baseline cardiac troponinPatients with data on baseline cardiac troponinDeathDeath 0.85 (0.65-1.11)0.85 (0.65-1.11) 0.91 (0.66-1.27)0.91 (0.66-1.27) 0.830.83Death or MIDeath or MI 0.93 (0.78-1.11)0.93 (0.78-1.11) 1.07 (0.85-1.35)1.07 (0.85-1.35) 0.380.38
Patients with baseline cardiac troponin T or I < 0.1 Patients with baseline cardiac troponin T or I < 0.1 g/Lg/LDeathDeath 1.07 (0.67-1.71)1.07 (0.67-1.71) 1.20 (0.69-2.10)1.20 (0.69-2.10) 0.840.84Death or MIDeath or MI 1.10 (0.84-1.43)1.10 (0.84-1.43) 1.29 (0.91-1.83)1.29 (0.91-1.83) 0.650.65
Patients with baseline cardiac troponin T or I Patients with baseline cardiac troponin T or I 0.1 0.1 g/Lg/LDeathDeath 0.75 (0.54-1.04)0.75 (0.54-1.04) 0.80 (0.53-1.21)0.80 (0.53-1.21) 0.880.88Death or MIDeath or MI 0.82 (0.65-1.03)0.82 (0.65-1.03) 0.93 (0.68-1.28)0.93 (0.68-1.28) 0.480.48

N Engl J Med 2001;344:1888-94N Engl J Med 2001;344:1888-94
Do Do TTirofiban irofiban AAnd nd RReoPro eoPro GGive Similar ive Similar EEfficacy Outcomes fficacy Outcomes TTrialrial
Primary HypothesisPrimary HypothesisTirofiban will have comparable efficacy to Tirofiban will have comparable efficacy to
abciximab in reducing the incidence of adverse abciximab in reducing the incidence of adverse cardiac ischemic events during the first 30 days cardiac ischemic events during the first 30 days
after intracoronary stent placement.after intracoronary stent placement.

Statistical ConsiderationsStatistical Considerations
Sample size provides 88% power to declare Sample size provides 88% power to declare tirofiban noninferior to abciximab, based tirofiban noninferior to abciximab, based on the relative efficacy of abciximab to on the relative efficacy of abciximab to placebo in EPISTENT.*placebo in EPISTENT.*
**The upper bound of the one-sided 95% C.I. The upper bound of the one-sided 95% C.I. for the odds ratio (tirofiban relative to for the odds ratio (tirofiban relative to abciximab) must be below 1.47.abciximab) must be below 1.47.
N Engl J Med 2001;344:1888-94N Engl J Med 2001;344:1888-94

Primary EndpointPrimary Endpoint
30-day composite of:30-day composite of:
■ DeathDeath
■ Myocardial infarctionMyocardial infarction■ CK-MB > 3x ULN in two samplesCK-MB > 3x ULN in two samples■ New Q wavesNew Q waves
■ Urgent TVRUrgent TVR■ PCI or CABGPCI or CABG
N Engl J Med 2001;344:1888-94N Engl J Med 2001;344:1888-94

Primary EndpointPrimary Endpoint
N Engl J Med 2001;344:1888-94N Engl J Med 2001;344:1888-94
30-day Death, MI, Urgent TVR30-day Death, MI, Urgent TVR
Upper bound Upper bound of 95% C.I. of 95% C.I. = 1.51= 1.51
Noninferiority Noninferiority boundaryboundary
R.R. = 1.26R.R. = 1.26
AbciximabAbciximabBetterBetter
TirofibanTirofibanBetterBetter
p = 0.038p = 0.038
7.6%7.6%
6.0%6.0%
0%0%
2%2%
4%4%
6%6%
8%8%
10%10%
R.R. = 1.26R.R. = 1.26
TirofibanTirofiban AbciximabAbciximab30-
da
y D
eath
, MI,
Urg
en
t T
VR
(%
)3
0-d
ay
Dea
th, M
I, U
rge
nt
TV
R (
%)

Primary Endpoint AnalysisPrimary Endpoint Analysis
N Engl J Med 2001;344:1888-94N Engl J Med 2001;344:1888-94
7.6%
0.5%
6.9%7.2%
0.8%
6.0%
0.4%
5.4%5.7%
0.7%
0%
2%
4%
6%
8%
Composite Death MI Death/MI UrgentTVR
Ev
en
t R
ate
Tirofiban Abciximab7.6%
0.5%
6.9%7.2%
0.8%
6.0%
0.4%
5.4%5.7%
0.7%
0%
2%
4%
6%
8%
Composite Death MI Death/MI UrgentTVR
Ev
en
t R
ate
Tirofiban Abciximab
p = 0.038 p = 0.04 p = 0.04p = 0.66 p = 0.49

Subgroup AnalysisSubgroup Analysis
DiabetesDiabetes
No DiabetesNo Diabetes
Age < 65Age < 65
Age Age 65 65
MaleMale
FemaleFemale
11Tirofiban Tirofiban BetterBetter
TirofibanTirofiban AbciximabAbciximab%% %% RRRR CICI
6.36.3 5.45.4 1.161.16 0.72, 1.900.72, 1.90
7.97.9 6.26.2 1.291.29 1.01, 1.641.01, 1.64
6.66.6 4.64.6 1.451.45 1.05, 2.011.05, 2.01
8.88.8 7.87.8 1.131.13 0.82, 1.500.82, 1.50
7.27.2 6.56.5 1.101.10 0.86, 1.430.86, 1.43
8.78.7 4.74.7 1.861.86 1.19, 2.891.19, 2.89
N Engl J Med 2001;344:1888-94N Engl J Med 2001;344:1888-94
Abciximab Abciximab BetterBetter

Subgroup AnalysisSubgroup AnalysisPre-procedure Pre-procedure ClopidogrelClopidogrel
YesYes
NoNo
ACSACS
Non-ACSNon-ACS
U.S.U.S.
Ex-U.S.Ex-U.S.
TirofibanTirofiban AbciximabAbciximab%% %% RRRR CICI
7.27.2 5.85.8 1.241.24 1.00, 1.581.00, 1.58
12.512.5 8.38.3 1.501.50 0.73, 2.680.73, 2.68
9.39.3 6.36.3 1.491.49 1.15, 1.941.15, 1.94
4.54.5 5.65.6 0.820.82 0.54, 1.240.54, 1.24
7.77.7 6.76.7 1.141.14 0.91, 1.450.91, 1.45
6.96.9 2.92.9 2.422.42 1.27, 4.641.27, 4.64
N Engl J Med 2001;344:1888-94N Engl J Med 2001;344:1888-94
11Tirofiban Tirofiban BetterBetter
Abciximab Abciximab BetterBetter

30-Day Conclusions30-Day Conclusions
■ Abciximab was superior to tirofiban in Abciximab was superior to tirofiban in reducing the incidence of the composite reducing the incidence of the composite endpoint of death/MI/urgent target vessel endpoint of death/MI/urgent target vessel revascularization at 30 days after revascularization at 30 days after intracoronary stent placement.intracoronary stent placement.
■ There were no differences in rates of TIMI There were no differences in rates of TIMI major bleeding, but significant differences in major bleeding, but significant differences in minor bleeding and thrombocytopenia were minor bleeding and thrombocytopenia were observed and favored tirofiban.observed and favored tirofiban.
N Engl J Med 2001;344:1888-94N Engl J Med 2001;344:1888-94

95% CI: 0.90,1.2295% CI: 0.90,1.2295% CI: 1.05,1.5295% CI: 1.05,1.52
Composite Endpoint (Death/MI/TVR)Composite Endpoint (Death/MI/TVR)
7.6%
14.4%
6.0%
13.8%
0%
5%
10%
15%
30-Day 6-Month
Tirofiban (N = 2398) Abciximab (N = 2411)
7.6%
14.4%
6.0%
13.8%
0%
5%
10%
15%
30-Day 6-Month
Tirofiban (N = 2398) Abciximab (N = 2411)
p = 0.038 p = 0.509

95% CI: 0.96,1.4495% CI: 0.96,1.4495% CI: 1.01,1.5895% CI: 1.01,1.58
Death/MIDeath/MI
7.2%8.7%
5.7%7.4%
0%
5%
10%
15%
30-Day 6-Month
Tirofiban (N = 2398) Abciximab (N = 2411)
7.2%8.7%
5.7%7.4%
0%
5%
10%
15%
30-Day 6-Month
Tirofiban (N = 2398) Abciximab (N = 2411)
p = 0.04 p = NS

95% CI: 0.76,1.1495% CI: 0.76,1.1495% CI: 0.65,2.4495% CI: 0.65,2.44
Target Vessel RevascularizationTarget Vessel Revascularization
0.8%
7.5%
0.7%
8.0%
0%
5%
10%
15%
30-Day 6-Month
Tirofiban (N = 2398) Abciximab (N = 2411)
0.8%
7.5%
0.7%
8.0%
0%
5%
10%
15%
30-Day 6-Month
Tirofiban (N = 2398) Abciximab (N = 2411)
p = NS
p = NS
Urgent TVRUrgent TVR

95% CI: 0.67,1.2195% CI: 0.67,1.2195% CI: 0.72,1.9095% CI: 0.72,1.90
Diabetics: Composite Endpoint Diabetics: Composite Endpoint (Death/MI/TVR)(Death/MI/TVR)
6.3%
15.2%
5.4%
16.7%
0%
5%
10%
15%
30-Day 6-Month
Tirofiban (N = 2398) Abciximab (N = 2411)
6.3%
15.2%
5.4%
16.7%
0%
5%
10%
15%
30-Day 6-Month
Tirofiban (N = 2398) Abciximab (N = 2411)
p = NS p = NS

Subgroups: EPISTENT Diabetes PaperSubgroups: EPISTENT Diabetes Paper
6-month Event Rates for Study Group6-month Event Rates for Study Group
Stent/PlaceboStent/Placebo Stent/AbciximabStent/Abciximab pp
Death, MI, TVRDeath, MI, TVR DiabeticsDiabetics 43 (25.2)43 (25.2) 21 (13.0)21 (13.0) 0.0050.005NondiabeticsNondiabetics 104 (16.5)104 (16.5) 81 (13.0)81 (13.0) 0.0620.062
Death or MIDeath or MIDiabeticsDiabetics 22 (12.7)22 (12.7) 10 (6.2)10 (6.2) 0.041 0.041 NondiabeticsNondiabetics 70 (11.0)70 (11.0) 34 (5.4)34 (5.4) < 0.001< 0.001
MIMIDiabeticsDiabetics 19 (11.0)19 (11.0) 10 (6.2)10 (6.2) 0.11 0.11 NondiabeticsNondiabetics 64 (10.1)64 (10.1) 31 (4.9)31 (4.9) < 0.001< 0.001
DeathDeathDiabeticsDiabetics 3 (1.7)3 (1.7) 1 (0.6)1 (0.6) 0.350.35NondiabeticsNondiabetics 7 (1.1)7 (1.1) 3 (0.5)3 (0.5) 0.210.21Diabetics (1 yr)Diabetics (1 yr) 8 (4.8)8 (4.8) 2 (0.9)2 (0.9) 0.080.08

Post-randomization Post-randomization SubgroupsSubgroups

Issues Specific to theIssues Specific to the“Post-randomization” Component“Post-randomization” Component
Example:Example:
■ A clinical trial evaluated the treatment A clinical trial evaluated the treatment effect of a new drug (A) versus placebo effect of a new drug (A) versus placebo (P) in ACS patients. The primary (P) in ACS patients. The primary endpoint of the trial was 30-day death endpoint of the trial was 30-day death or MI. Of special interest was the or MI. Of special interest was the effectiveness of the new drug in effectiveness of the new drug in patients who had received a PCI patients who had received a PCI versus those who had not. versus those who had not.

Sample Patient 1Sample Patient 1
RandomizationRandomization
PCIPCIPCIPCI
Death or MIDeath or MIDeath or MIDeath or MI
30-day 30-day AssessmentAssessment
30-day 30-day AssessmentAssessment

Sample Patient 2Sample Patient 2
RandomizationRandomization
Death or MIDeath or MIDeath or MIDeath or MI
30-day 30-day AssessmentAssessment
30-day 30-day AssessmentAssessment

Incidence of 1Incidence of 1 Endpoint Endpoint Odds RatioOdds RatioEptifibatideEptifibatide PlaceboPlacebo PP (95% CI)(95% CI)
PCI < 72 hoursPCI < 72 hours (N = 606)(N = 606) (N = 622)(N = 622)
96 hours96 hours 57 (9.4)57 (9.4) 95 (15.3)95 (15.3) 0.0020.002 0.576 (0.406, 0.817)0.576 (0.406, 0.817)
7 days7 days 62 (10.2)62 (10.2) 100 (16.1)100 (16.1) 0.0030.003 0.595 (0.424, 0.835)0.595 (0.424, 0.835)
30 days30 days 70 (11.6)70 (11.6) 104 (16.7)104 (16.7) 0.0100.010 0.650 (0.469, 0.901)0.650 (0.469, 0.901)
No PCI < 72 hrsNo PCI < 72 hrs (N = 4116)(N = 4116) (N = 4117)(N = 4117)
96 hours96 hours 302 (7.3)302 (7.3) 334 (8.1)334 (8.1) 0.1880.188 0.897 (0.763, 1.055)0.897 (0.763, 1.055)
7 days7 days 415 (10.1)415 (10.1) 452 (11.0)452 (11.0) 0.1850.185 0.909 (0.790, 1.047)0.909 (0.790, 1.047)
30 days30 days 602 (14.6)602 (14.6) 641 (15.6)641 (15.6) 0.2320.232 0.929 (0.823, 1.048)0.929 (0.823, 1.048)
PCI = percutaneous coronary intervention; CI = confidence intervalPCI = percutaneous coronary intervention; CI = confidence interval
Improper SubgroupsImproper Subgroups

Sample Patient 3Sample Patient 3
RandomizationRandomization
MIMIMIMI
PCIPCIPCIPCI
30-day 30-day AssessmentAssessment
30-day 30-day AssessmentAssessment

EptifibatideEptifibatide PlaceboPlacebo Absolute Absolute Time IntervalTime Interval (N = 606)(N = 606) (N = 622)(N = 622) ReductionReduction P-valueP-value
Before PTCABefore PTCA Death/MI Death/MI 1.7%1.7% 5.5%5.5% 3.8%3.8% < 0.001< 0.001
96 hours96 hours Death/MI* Death/MI* 8.1%8.1% 10.9%10.9% 2.9%2.9% 0.0900.090
7 days7 days Death/MI* Death/MI* 8.9%8.9% 11.7%11.7% 2.8%2.8% 0.1050.105
30 days30 days Death/MI* Death/MI* 10.2%10.2% 12.4%12.4% 2.2%2.2% 0.2350.235
*Composite only includes myocardial infarctions (MI) occurring after the *Composite only includes myocardial infarctions (MI) occurring after the percutaneous percutaneous

SUPPORTSUPPORT
JAMA 1996; 276:889-897JAMA 1996; 276:889-897
Study of effectiveness of Right Heart Catheterization (RHC) in the initial care of
critically ill patients.
•Issues:
•Timing of RHC relative to hospital arrival
•Timing of RHC relative to death
•Need to survive long enough to get a RHC – patients who die early will be in the no RHC group.
•Bias in who is chosen for a RHC
Study of effectiveness of Right Heart Catheterization (RHC) in the initial care of
critically ill patients.
•Issues:
•Timing of RHC relative to hospital arrival
•Timing of RHC relative to death
•Need to survive long enough to get a RHC – patients who die early will be in the no RHC group.
•Bias in who is chosen for a RHC
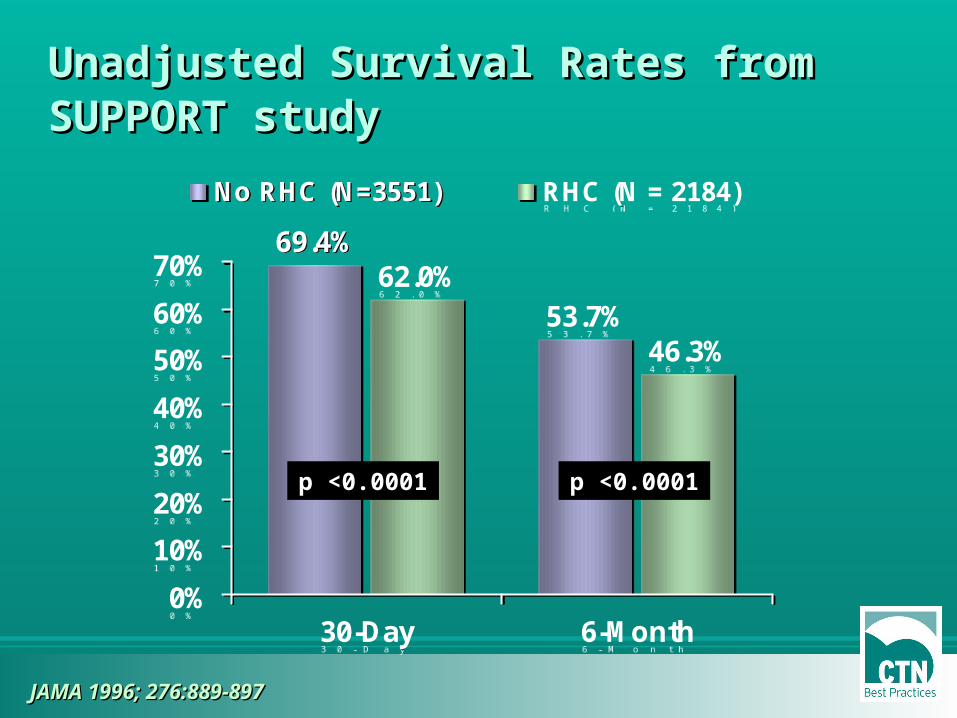
Unadjusted Survival Rates from SUPPORT Unadjusted Survival Rates from SUPPORT studystudy
69.4%
53.7%62.0%
46.3%
0%
10%
20%
30%
40%
50%
60%
70%
30-Day 6-Month
No RHC (N=3551) RHC (N = 2184)
69.4%
53.7%62.0%
46.3%
0%
10%
20%
30%
40%
50%
60%
70%
30-Day 6-Month
No RHC (N=3551) RHC (N = 2184)
p <0.0001 p <0.0001
JAMA 1996; 276:889-897JAMA 1996; 276:889-897

SUPPORT study – AdjustmentsSUPPORT study – Adjustments
JAMA 1996; 276:889-897JAMA 1996; 276:889-897
• Only included RHC that occurred within the first 24 hrs. This cut down on the problem of survivor bias.
• Calculated the “propensity” to receive a RHC and adjusted for both baseline differences and this propensity score.
• Only included RHC that occurred within the first 24 hrs. This cut down on the problem of survivor bias.
• Calculated the “propensity” to receive a RHC and adjusted for both baseline differences and this propensity score.

SUPPORT study – Adjusted resultsSUPPORT study – Adjusted results
JAMA 1996; 276:889-897JAMA 1996; 276:889-897
Hazard Ratio: 1.21 (1.09, 1.25), (p<0.001)Hazard Ratio: 1.21 (1.09, 1.25), (p<0.001)

EMBARGOED FOR RELEASE Tuesday, November 9, 2004 CONTACT:
NHLBI Communications Office (301) 496-4236Email: [email protected]
AHA Scientific Sessions News Media Center: (504) 670-6500. (8 a.m. to 8 p.m. EST, Sun., Nov 7, through Tues., Nov 9, and 8 a.m. to 6 p.m. EST, Weds. Nov 10.)
No Increase in Deaths or Hospitalizations for Heart Failure Patients Who Have a Pulmonary Artery Catheter
EMBARGOED FOR RELEASE Tuesday, November 9, 2004 CONTACT:
NHLBI Communications Office (301) 496-4236Email: [email protected]
AHA Scientific Sessions News Media Center: (504) 670-6500. (8 a.m. to 8 p.m. EST, Sun., Nov 7, through Tues., Nov 9, and 8 a.m. to 6 p.m. EST, Weds. Nov 10.)
No Increase in Deaths or Hospitalizations for Heart Failure Patients Who Have a Pulmonary Artery Catheter
SafeguardsSafeguards
■ Remember that the primary hypothesis is the Remember that the primary hypothesis is the only one the study was designed to answeronly one the study was designed to answer
■ Nonsignificant results may indicate that there Nonsignificant results may indicate that there were too few patients studied to detect a small were too few patients studied to detect a small meaningful difference.meaningful difference.
■ Subgroup results should be confirmed in Subgroup results should be confirmed in subsequent studies before acceptance.subsequent studies before acceptance.

Baseline TableBaseline Table
■ The baseline table is needed to show where The baseline table is needed to show where the differences in baseline characteristics the differences in baseline characteristics exist, especially when the sample size is small exist, especially when the sample size is small or the groups being compared are not or the groups being compared are not randomized.randomized.
■ If baseline characteristics are not equally If baseline characteristics are not equally distributed, be sure that there is at least one distributed, be sure that there is at least one analysis of the endpoint(s) adjusted for the analysis of the endpoint(s) adjusted for the other factors associated with the endpoint(s).other factors associated with the endpoint(s).

Example—ESPRIT DiabetesExample—ESPRIT DiabetesBaseline Characteristics for Diabetics and NondiabeticsBaseline Characteristics for Diabetics and Nondiabetics
Diabetics (%)Diabetics (%) Nondiabetics (%)Nondiabetics (%)VariableVariable N = 466N = 466 N = 1595N = 1595 P-valueP-value
Age, yrsAge, yrs 62.0 (55.0, 70.0)62.0 (55.0, 70.0) 62.0 (54.0, 71.0)62.0 (54.0, 71.0) 0.6680.668
Weight, kgWeight, kg 89.0 (77.0, 102.0)89.0 (77.0, 102.0) 83.5 (73.2, 94.5)83.5 (73.2, 94.5) < 0.001< 0.001
Women Women 175 (37.6)175 (37.6) 386 (24.2)386 (24.2) 0.0010.001
Previous MIPrevious MI 142 (30.5)142 (30.5) 509 (31.9)509 (31.9) 0.5560.556
Previous PCIPrevious PCI 125 (26.8)125 (26.8) 357 (22.4)357 (22.4) 0.0460.046
Previous CABGPrevious CABG 55 (11.8)55 (11.8) 156 (9.8)156 (9.8) 0.2050.205
HypertensionHypertension 334 (71.7)334 (71.7) 877 (55.0)877 (55.0) 0.0010.001
HypercholesterolemiaHypercholesterolemia 294 (63.1)294 (63.1) 905 (56.8)905 (56.8) 0.0150.015
PVDPVD 51 (10.9)51 (10.9) 86 (5.4)86 (5.4) 0.0010.001
Previous strokePrevious stroke 29 (6.2)29 (6.2) 60 (3.8)60 (3.8) 0.0210.021
Current smokerCurrent smoker 89 (19.3)89 (19.3) 389 (24.6)389 (24.6) 0.0120.012

Be Careful of Axes Sizes!Be Careful of Axes Sizes!Compare this…Compare this…
Event Rates for Death
0
0.01
0.02
0.03
0 100 200 300
Days
Eve
nt
Rat
e
Diabetic
Non-diabetic
p = 0.167
Event Rates for Death
0
0.01
0.02
0.03
0 100 200 300
Days
Eve
nt
Rat
e
Diabetic
Non-diabetic
p = 0.167

To this…To this…(It’s the same data!)(It’s the same data!)
Event Rates for Death
0
0.2
0.4
0.6
0.8
1
0 100 200 300
Days
Eve
nt
Rat
e
Diabetic
Non-diabetic
p = 0.167
Event Rates for Death
0
0.2
0.4
0.6
0.8
1
0 100 200 300
Days
Eve
nt
Rat
e
Diabetic
Non-diabetic
p = 0.167

Other PrecautionsOther Precautions
■ Check the Ns—do things add up? You’d Check the Ns—do things add up? You’d be surprised how many times they don’t!be surprised how many times they don’t!
■ Watch for missing data. Does it appear Watch for missing data. Does it appear that the sample size has dropped for that the sample size has dropped for some variables? What has been done some variables? What has been done about missing data? How will that about missing data? How will that influence the results?influence the results?

Other PrecautionsOther Precautions
■ Can you account for every patient in how the Can you account for every patient in how the sample for this study was drawn from the sample for this study was drawn from the original study population?original study population?
■ Are confidence intervals or error bars Are confidence intervals or error bars included for estimates?included for estimates?

References:References:
■ Bailar JC III, Mosteller F. Guidelines for statistical Bailar JC III, Mosteller F. Guidelines for statistical reporting in articles for medical journals, Ann Intern reporting in articles for medical journals, Ann Intern Med, 108:266-273, 1988.Med, 108:266-273, 1988.
■ DerSimonian R, Charette LJ, McPeek B, Mosteller F. DerSimonian R, Charette LJ, McPeek B, Mosteller F. Reporting on methods in clinical trials. In Reporting on methods in clinical trials. In Medical Medical Uses of Statistics, Uses of Statistics, 2nd ed, Bailar JC III et al (ed), 2nd ed, Bailar JC III et al (ed), Boston, NEJM, 1992, pp333-348.Boston, NEJM, 1992, pp333-348.
■ Gardner MJ, Machin D, Campbell MJ. Use of check Gardner MJ, Machin D, Campbell MJ. Use of check lists in assessing the statistical content of medical lists in assessing the statistical content of medical studies. In studies. In Statistics with ConfidenceStatistics with Confidence, Gardner MJ, et , Gardner MJ, et al (eds), London, British Medical Journal, 1989, pp101-al (eds), London, British Medical Journal, 1989, pp101-108.108.