interlaboratory comparison of serodiagnosis of lyme borreliosis using purified borrelia burgdorferi...
TRANSCRIPT
Serodiagn. Immunother. Infect. Disease 1993; 5: 245-250
tntertaboratory comparison of serodiagnosis of Lyme borret iosis using purified Borreh burgdorferi s./. cell surface components
I Nilssonl, J Buniki9, B Ekstrand-Hammarstr6m3, M Olssonl, M Sellin4, T Wadstr6m1, S Holm4, S Bergstr6m2
‘Department of Medical Microbiology, University of Lund, S-223 62, Lund; 2Department of Microbiology, University of Umea, S-901 87 Umea; 3Symbicom AB, S-901 24 Umed; 4Department of Bacteriology, University of Umea, S-901 87 UmeB, Sweden
Summary
For detection of antibodies to Borrelia burgdorferi s.l., the causative agent of Lyme borre- liosis, an enzyme immunoassay based on fractionated antigenic components (BF-EIA) pooled from two different Borrelia species, Borrelia burgdorferi B31, (type strain: ATCC 35210) and Borrelia afzelii strain ACAI isolated in Sweden, were used. To compare sensi- tivity and specificity, a standard enzyme immunoassay with a whole cell preparation of strain ACAI (WC-EIA) was included in the study. Three independent laboratories performed and evaluated the BF-EIA on the same sera, from patients with clinically diagnosed Lyme borreliosis and from individuals with no known exposure to Borrelia spirochaetes. In addition, serum samples obtained from patients with antibody titres against rheumatoid factor, or with specific and nonspecific antibodies to Treponema pallidurn, or positive and negative for C-reactive protein (CRP) were used to assess the specificity of the EIA tests. The test results showed a higher specificity in the BF-EIA and an equal or better sensitivity in comparison to the WC-EIA. Furthermore, results from the three laboratories correlated well. Our data suggest that the BF-EIA is a reliable and simple immunoassay for the detection of IgG antibodies to B. burgdorferi s.1.
Key words: Borrelia burgdorferi, serodiagnosis, enzyme immunoassay, outer surface components, interlaboratory comparison
Introduction
Lyme borreliosis is a multisystemic illness caused by the tick-transmitted spirochaete Borrelia burgdorferi complex’. The infection is characterized by a variety of manifestations and the infection may involve many organs but most commonly the skin, nervous system, joints, muscles and heart are affected2-s. The clinical diagnosis of this disorder is often difficult, since symptoms mimic other illnesses. With the dramatic increase in awareness of symptoms, prevalence and
Hwrivecl: 7X September I YY3 /lw~/ml: I Y October I YY3 (‘orre~p0nrlmc.e cult/ rqwint requests 10: S BerpstrGm, Department of Microbiology. University of IJmeA. S-Y01 X7 Umeri. Sweden (‘i IYY.3 Rutterworth-Heinem;mn Ltd 0XXX-07Xh/‘).3/~I~0245-0h
geographical distribution of the Lyme borreliosis spirochaetes, a new demand has been placed on clini- cal laboratories to diagnose the infection serologically. Conventional microbiological methods for isolation of spirochaetes from patients are time consuming, often fail and are not practicable for routine diagnostics. The most common diagnostic test at present is based on measurement of antibodies in serum and cerebrospinal fluid (CSF) with affinities to various antigens on the B. burgdorfrri spirochaete. The techniques frequently used are enzyme immunoassay (EIA)h. indirect immunofluorescent antibody test (IFA)’ and immunoblottingx~“. The two main problems encoun- tered with serological tests for Lyme borreliosis are the lack of standardization and lack of specificity. So far, no standardized test is available and a high degree of inter-laboratory variation is seen even when similar

246 Serodiagn. Immunother. Infect. Disease 1993; 5: No 4
serological assays are usedr”.rl. Crossreacting antibod- ies induced by other spirochaetal disease, rickettsial infections. human immunodeficiency virus infections, mumps. meningitis. bacterial endocarditis and mononucleosis have been reported to give false positive results in serological assays”,13. Fractionated whole cell preparations of B. burgdorferi xl. have been evaluated by several investigators, in order to improve serological assays’-‘. However, an EIA based on purified flagellin has shown to be more specific and sensitive than the EIA based on a whole-cell prepara- tionl5,lh.
The aim of this study was to evaluate an enzyme immunoassay, based on fractionated antigenic subunits prepared from two different Borrelia species of differ- ent geographical origin. Recent studies of B. burgdor- feri s.1. strains B31 and ACAI have taxonomically identified them in two different Borrelia species, Borrelia burgdorferi sensu strict0 and Borrelia afzelii, respectively17Jx. The antigen preparation consisted of 11 proteins including the previously defined OspA and the OspB proteins 14J). The 41 kDa protein (flagellin) was not detectable after fractionation.
We also determined the specificity and sensitivity of the BF-EIA in comparison to the WC-EIA and assessed inter-laboratory variation of the BF-EIA when the same serum samples were tested in three independent laboratories.
Materials and methods
Patient sera
The following serum samples were tested: sera from patients with Lyme borreliosis at stage II or III (n = 19) kindly obtained from Drs L Dotevall (Department of Infectious Diseases, University of Gothenburg, Sweden) and L Magnarelli (Connecticut Agricultural Experimental Station, New Haven, CT. USA); sera from patients with clinically verified neuroborreliosis (n = 16); sera from patients with various neurological disorders other than neuroborreliosis (n = 10) kindly obtained from Dr B Ryberg (Department of Neurology, University Hospital of Lund): sera from patients with high titres of rheumatoid factor (n = 20) and from patients with specific (positive in the TPHA- test, Cellognost-Syphilis H, Behringwerke AG. Germany), (n = 10) and non-specific (only positive in the Wasserman test), (n = 10) antibodies to Treponema pallidurn, selectively obtained from the Section of Clinical Immunology, University Hospital of Lund and the Department of Bacteriology, University Hospital of Northern Sweden.
Additional sera were collected from patients tested for C-reactive protein (CRP-test. positive n = 40. negative n = 99) obtained from the Department of Bacteriology, University Hospital of Northern Sweden. Finally, set-a from 89 healthy blood donors from Northern Sweden, with no known exposure to B. burgdor#?ri. were used to calculate the cut-off level.
All serum samples were aliquoted and stored frozen until mailed to the various laboratories for testing.
Participating laboratories
The following three laboratories participated in the study: Department of Medical Microbiology, University of Lund (lab A), where both BF-EIA and WC-EIA were performed: Department of Clinical Microbiology, University Hospital of Umeb (lab B); and Symbicom AB, Umea (lab C) where only BF-EIA was performed.
Borrelia strains and culture conditions
The B. burgdorferi strain B31 (ATCC 35210) and the B. afzelii strain ACAI, isolated from the skin of a patient with acrodermatitis chronica atrophicans in Sweden. were used for antigen preparation. The spirochaetes were grown in Barbour-Stoenner-Kelly medium II (BSK II)” at 34” C for five days in 5% CO? : 95% atmospheric air to a cell density of 108 ml-‘. The BSK II medium was supplemented with 5% bovine serum albumin (BSA) fraction V (Boehringer Mannheim, Germany).
Antigen preparation and polyacrylamide gel electrophoresis (SDS-PAGE)
A pooled antigen fraction, the B-fraction, was prepared from the two B. burgdorferi strains B31 and ACAI as previously described’“J”. The fractionation procedure was based on a detergent precipitation with octyl-P-D-glucopyranoside (Calbicochem Novabio- them, San Diego, CA, USA). The protein profiles of the whole cell preparations and the B-fractions of both strains B31 and ACAI were analysed by SDS-PAGE (12% separating gel) using the system of Laemmli”. The gels were stained with Coomassie brilliant blue R- 250 (Sigma Chemical Co.. St Louis, MO, USA). Molecular weight standards (Pharmacia, Uppsala. Sweden) included proteins ranging from 21.5 to 92.5 kDa in size.
Enzyme inzmunoassays
BF-EZA: Flat-bottomed microtitre plates (Maxi Sorp. Nunc, Roskilde, Denmark) were coated with 50 yl welll’ of the antigen preparation at a protein concen- tration of 12 ug ml-’ diluted in 10 mM phosphate buffered saline (PBS), pH 7.2 overnight at room temperature in a humid chamber. Wells were washed with the same buffer and 100 ul of patient and reference sera diluted 1 : 500 in PBS containing 1% milk powder was added in each well and incubated for 1 h at 37” C. All serum samples were analysed in duplicate and each plate contained the same positive and negative controls (supplied by Symbicom AB). After washing. 100 ul of alkaline-phosphatase conjugated anti-human ‘gG antibodies (Dakopatts A/S. Copenhagen. Denmark). diluted I : 500 in PBS containing 1% milk powder was
Nilsson et al.: Serodiagnosis of Lyme borreliosis using B. burgdorferi cell surface components 247
added and incubated for 1 h at 37” C. The plates were washed and 100 1-11 of substrate, 1 mg ml-’ of p-nitro- phenyl phosphate (Sigma) in diethanolamine buffer pH 9.8 with OS mM MgCl, was added to each well. After 30 min incubation at 37” C in the dark the enzymatic reaction was stopped by the addition of 50 pl 1 M NaOH to each well and the optical density (OD) was measured at 405 nm in a microplate photometer (Multiskan Plus, Labsystems, Stockholm, Sweden).
WC-EIA: The assay is commercially available and was performed according to the recommendations of the manufacturer (SBL, 10.5 21, Stockholm, Sweden). Briefly. flat-bottomed microtitre plates were coated overnight at 22” C with 100 pl well-’ (protein concen- tration 5 ug ml-‘) of the whole-cell antigen (strain ACAI). After three washings in PBS pH 7.2 with 0.05% Tween 20 (PBS-T), 100 ~1 of patient and refer- ence sera (supplied by the SBL) diluted 1 : 1000 in PBS-T were added and incubated for 1 h at 22” C. All patient sera as well as positive and negative reference sera were tested in duplicate. The plates were washed three times in PBS-T and incubated for 3 h at 22” C with 100 pl well-’ of alkaline-phosphatase conjugated anti-human IgG antibodies (Orion Diagnostica, Espoo, Finland) diluted I : 300 in PBS-T. After washing the well three times, 100 ul of substrate, 1 mg ml-’ of p- nitrophenyl phosphatase (Sigma) in diethanolamine buffer pH 9.8 with 0.5 mM MgClz was added to each well. After incubating for 25 min at 37” C or when the positive control. after deducting the background value, was equal to 1.0, the OD was measured at 405 nm in a microplate photometer (Multiskan Plus). Interpretation guidelines provided by the manufac- turer were followed.
Results
Fractionated antigens
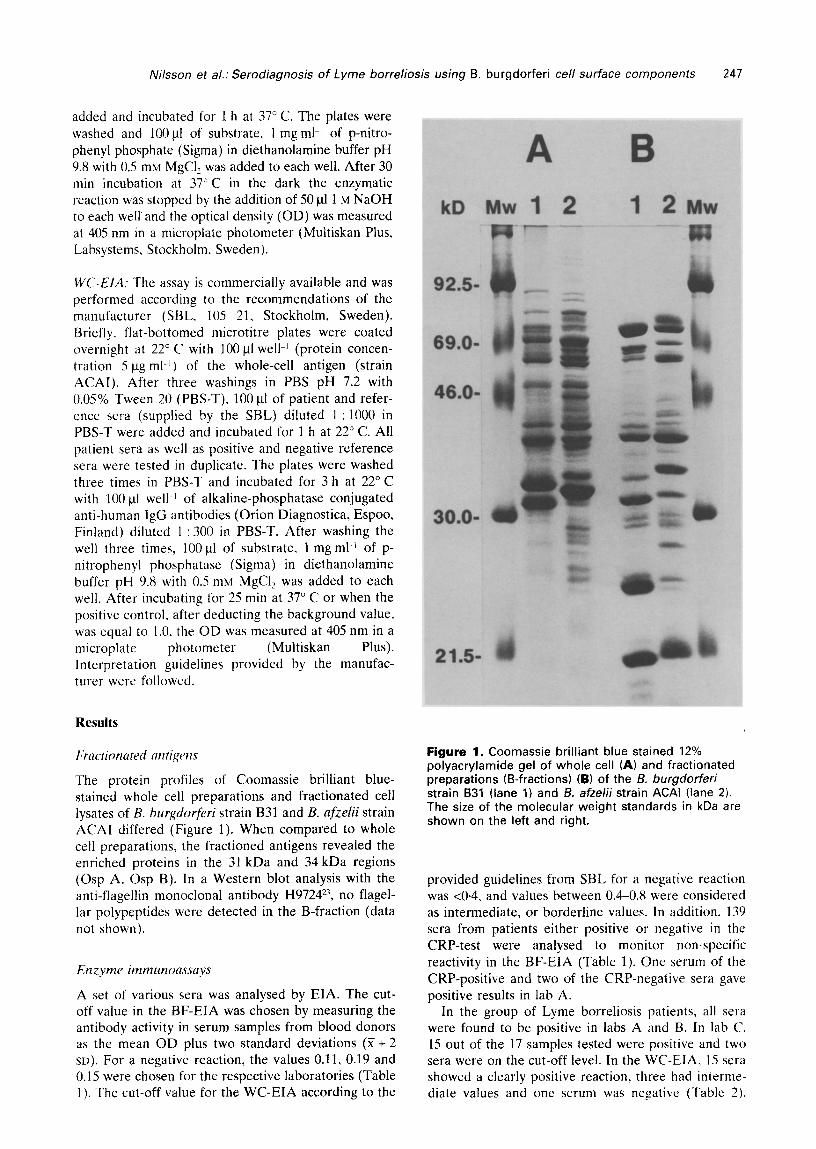
The protein profiles of Coomassie brilliant blue- stained whole cell preparations and fractionated cell lysates of B. burgdorferi strain B31 and B. afzelii strain ACAI differed (Figure 1). When compared to whole cell preparations, the fractioned antigens revealed the enriched proteins in the 31 kDa and 34 kDa regions (Osp A, Osp B). In a Western blot analysis with the anti-flagellin monoclonal antibody H9724*‘, no flagel- lar polypeptides were detected in the B-fraction (data not shown).
Enzyme irnrnunoassnys
A set of various sera was analysed by EIA. The cut- off value in the BF-EIA was chosen by measuring the antibody activity in serum samples from blood donors as the mean OD plus two standard deviations (X + 2 SD). For a negative reaction, the values 0.11, 0.19 and 0.15 were chosen for the respective laboratories (Table 1). The cut-off value for the WC-EIA according to the
Figure 1. Coomassie brilliant blue stained 12% polyacrylamide gel of whole cell (A) and fractionated preparations (B-fractions) (6) of the f3. burgdorferi strain 831 (lane 1) and B. afzelii strain ACAI (lane 2). The size of the molecular weight standards in kDa are shown on the left and right.
provided guidelines from SBL for a negative reaction was ~0.4, and values between 0.4-0.8 were considered as intermediate, or borderline values. In addition. 139 sera from patients either positive or negative in the CRP-test were analysed to monitor non-specific reactivity in the BF-EIA (Table 1). One serum of the CRP-positive and two of the CRP-negative sera gave positive results in lab A.
In the group of Lyme borreliosis patients, all sera were found to be positive in labs A and B. In lab C. 15 out of the 17 samples tested were positive and two sera were on the cut-off level. In the WC-EIA, 15 sera showed a clearly positive reaction, three had interme- diate values and one serum was negative (Table 2).
248 Serodiagn. Immunother. Infect. Disease 1993; 5: No 4
Table 1. BF-EIA- the distribution of antibody activity in the group of blood donors and serum samples from patients in the CRP-tested group
Blood Age donors (years)
n 89
Lab A 0.11 I3 0.19 C 0.15
(Z + 2 SD).
CRP CRP CRP CRP w Pas nw w 5-15 15-65 15-65 265
19 40 40 40
0.068 0.18 0.13 0.35 0.070 0.19 0.14 0.17 0.010 0.072 0.08 0.096
Table 2. Comparable study of the BF-EIA and the WC-EIA carried out at three different laboratories on the same serum samples
No. of sera No. positive tested
Lab Lab Lab Whole A B C cell
Lyme borreliosis 19 19 19 17” 18b Neurological sera 26
Neuroborreliosis 16 7 8 8 9” Other disorders 10 0 0 1 0
Rheumatoid factor positive sera 20 0 2 0 Id Wasserman positive sera 10 0 0 0 6” TPHA positive sera 10 0 0 0 0
a17 samples tested. b3 intermediate values. c2 intermediate values. dl intermediate value. e4 intermediate values.
The neurological group included 16 sera from patients Both assays showed equally low sensitivity in with clinically diagnosed neuroborreliosis and, as diagnosing neuroborreliosis. Prior antibiotic treatment controls, 10 sera from patients with neurological disor- may be one explanation, alternatively, antibody ders other than neuroborreliosis. In the group of production may be restricted to the site of active neuroborreliosis patients, eight sera were positive in disease. Cases of neuroborreliosis have been recorded the BF-EIA in two laboratories (labs B and C) and in which the CSF (cerebrospinal fluid) was positive but seven sera were positive in one laboratory (lab A). In the serum was negativelh. Antibody may be produced the WC-EIA, seven sera were positive and two had but remain sequestered in immune complexes with intermediate values. In the group of neurological circulating antigen and thus not be detectable by controls, one serum showed antibody activity in lab C commonly used assay methods”. For a serological (Table 2). For further investigation of possible false diagnosis of neuroborreliosis, demonstration of local positive reactions to B. burgdorferi proteins, 20 sera antibody production is required. This can be performed with rheumatoid factor were tested. In this group, two by measuring the CSF ratio of total IgG/IgM and sera showed antibody activity in the BF-EIA in lab B albumin in CSF and serum. The neurological sera were and one serum showed activity in the WC-EIA (Table included for two reasons: firstly, to monitor the sensi- 2). Among the Wasserman positive patients, six sera tivity in sera from patients with neuroborreliosis in the gave positive or intermediate values in the WC-EIA, BF-EIA and secondly, to analyse the crossreactivity in but no reactivity was observed in the BF-EIA. The sera from patients with neurological disorders other TPHA positive sera showed no antibody activity in any than neuroborreliosis. Both EIA assays showed good of the EIAs (Table 2). specificity, but low sensitivity.
Discussion
To optimize serological testing for Lyme borreliosis, we evaluated an EIA based on fractionated antigenic components (11 different proteins, including OspA, OspB) from two different Borrelia species, B. hurgdor- feri sense strict0 and B. nfielii. Whole cell preparations or supernatants of crude fractions have been devel- oped for serological diagnosis of Lyme borreliosis. Such EIA methods have shown good sensitivity but are less satisfactory in specificity”‘J’. Some studies have focused on using antigenic preparations of purified flagellin to increase the sensitivity and specificity of the serological tests :. ’ Ih. In comparison to the assays based on a whole cell preparation, these methods have shown improvements. One potential problem with the use of flagella protein, however, is that flagella of other Borrelia species and treponemes share epitopes common to the flagella of B. brugdorferi s.I.?~~~~. No crossreactvity to treponemal antigen was observed in the BF-EIA as opposed to the WC-EIA. This is most likely due to the fact that the B-fraction lacks the 41 kDa protein (flagellin). Therefore, use of this B- fraction to detect 1gG antibodies will reduce the number of false-positive reactions associated with immune response to T. pallidurn or other treponemes. The average cut-off values for the BF-EIA were usually lower than those for the WC-EIA, which probably depends on the reduced amounts of irrele- vant proteins coated on the solid phase. Serum samples from patients analysed in the CRP-test were chosen to represent an arbitrarily selected patient group for monitoring non-specific reactivity in the BF-EIA. Forty of these individuals had positive CRP-test indicating an on-going inflammatory process and 99 individuals had a negative CRP-test. Compared to the blood donors, the age distribution among these patients was of a wider range (5-65 years). The use of sera from the CRP-group showed that crossreactivity in the BF-EIA was negligible.

Nilsson et al.: Serodiagnosis of Lyme borreliosis using B. burgdorferi cell surface components 249
Many laboratories both in Europe and the US perform Lyme borreliosis serology, but assay proce- dures have so far not been satistfactorily standardized. Antigens, reagents, incubation times and type of analy- sis can vary. This lack of standardization may affect test results and furthermore, the interpretation of the results can vary considerably among laboratories. This study demonstrated almost no inter-laboratory variability between the three participating laboratories when using the BF-EIA (Table 2). A similar result was recently obtained by Lane et al.‘” using two different indirect immunotluorescent assays, although significant serologic crossreactivity was demonstrated with B. hurgdorferi. Borrelia hermsii and Borrelia coriacea using the conventional indirect immunofluorescence assay. Variations in the antigenic and genetic profile of different Borrelin species in the Lyme borreliosis group have been reported’. The use of a single Borrelia isolate for antigenic preparation might therefore not be acceptable over a wide geographic area. The special design of this antigen, containing protein fractions from two Borrelia species of different geographic origin, might offer important improvements in the serodiagnosis of Lyme borreliosis. The next generation of antigen preparations will probably also contain proteins from the third species, Borrefia garinii. While serology will continue to be a useful adjunct to the clinical evaluation for establishing a diagnosis of Lyme borreliosis, further studies on standardization of antigen preparations and interpretation of test results are needed.
Acknowledgements
We greatly acknowledge Drs E Asbrink, A Hovmark (SGdersjukhuset, Stockholm, Sweden) and L Magnarelli (Connecticut Agricultural Experimental Station, New Haven, CT. USA). We thank Christin Wallberg for her technical assistance. This work was supported by grants from the Swedish Medical Research Council (Dnr 07922), the Swedish Research Council for Engineering Sciences (Dnr 90-513) and by Symbicom AB (Lime% Sweden).
References
1 Steere AC, Grodzicki RL. Kornblatt AN, Craft JE, Barbour AB, Burgdorfer W. Schmid GP, Johnson E, Malawista SE. The spirochetal etiology of Lyme disease. !li Engl .I Med 1983; 308: 73340
2 Steere AC, Malawista SE, Hardin JA, Ruddy S, Askenase W, Andiman WA. Erythema chronicum migrans and Lyme arthritis: the enlarging clinical spectrum. Ann Itzt Med 1977; 86: 685-98
3 Asbrink E, Hovmark A, Hederstedt B. The spirochetal etiology of acrodermatitis chronica atrophicans Hcrxheimer. Ach Derm Venereal 1984; 66: 479-84
3 Pachner AR. Stecrc AC. The triad of neurologic manifestations of Lyme disease: meningitis, cranial neuritis and radiculoneuritis. Neurology 1985; 35: 47-53
5 Malawista SE, Stcere AC. Lyme disease: infectious in origin. rheumatic in expression. Arf\, Intern Med 1986; 31: 147-hfl
6
7
8
9
10
II
12
13
14
15
16
17
18
19
20
21
22
23
24
Craft J, Grodzicki R. Steere AC. Antibody response in Lyme disease: evaluation of diagnostic tests. J Itzfect Dis 1984; 149: 789-95 Russell H. Sampson JS, Schmid GP. Wilkinson HW. Plikaytis B. Enzyme-linked immunosorbent assay and indirect immunofluorescence assay for Lyme disease. J Infect Dis 1984; 146: 789-95 Zijller L, Burkard S, Schafer H. Validity of Western immunoblot band patterns in the serodiagnosis of Lyme borreliosis. J Clin Microhiol 1991; 29: 174-82 Rose C, Fawcett P, Singsen B. Dubbs S, Doughty R. Use of Western blot and enzyme-linked immunosorhent assays to assist in the diagnosis of Lyme disease. Pediatrics 1991; 29: 174-82 Hedberg CW. Osterholm TM, MacDonald. White KE. An interlaboratory study of antibody lo Borrelia burgdorferi. J Infect Dis 1987: 155: 1325-7 Schwartz BS, Goldstein MD, Ribeiro JMC. Schultze TL, Shahied SI. Antibody testing in Lyme disease: a comparison of results in four laboratories. .I Am Mud Ass 1989; 262: 34314 Brucebauer HR, Preac-Mursic V, Fuchs R. Wilske B. Cross reactive proteins of Borrelia burgdo+~ri. Ew J Infect Dis 1992; 3: 224-32 Raoult D. Hechemy KE, Baranton B. Cross-reaction with Borrelia burgdorferi antigen of sera from patients with human immunodeficiency virus infection, syphilis. and leptospirosis. J Clin Microbiol 1989: 27: 7152-5 Coleman IL. Benach IL. Isolation of antigenic components from the Lyme disease spirochete: their role in early diagnosis. J lnfecr Dis 1987: 155: 756-65 Hansen K, Hindersen P, Pedersen NS. Measurements of antibodies to Borrelia burgdorferi flagellum improves serodiagnosis in Lyme disease. J C/in Microbial 1988: 26: 33846 Hansen K. Pi1 K. Lebech AM. Improved immunoglobulin M serodiagnosis in Lyme borreliosis by using a y-capture enzyme-linked immunosorbent assay with biotinylated Borrelia burgdorferi flagella. J Clirl Microbial 1991; 29: 1477-80 Baranton G, Postic D. Girons 1. Boerlin P. Piffaretti J-C, Assous M, Grimont PAD. Delineation of Borrelia burgdorferi senstl srricto, Borrelia garinii sp. nov. and group VS461 associated with Lyme borreliosis. Int J Syst Bacterial 1992: 42: 378-83 Canica MM, Nato F. du Merle L. Mazie JC, Baranton G, Postic D. Monoclonal antibodies for identification of Borrelia afzelii sp. nov. Associated with late cutaneous manifestations of Lyme borreliosis. Stand J l,z,fec.r Dis 1993; 25: 441-8 Magnarelli LA, Andersson JF, Barbour AG. Enzyme- linked immunosorbent assays for Lyme disease: reactivity of subunits of Borrelia burgdorferi. .I In fecr Dis 1989; 159: 43-9 Bergstriim S. SjGstedt A. Dotevall L. Ekstrand- HammarstrGm B. Wallberg C, Skogman G and Barbour AG. Diagnosis of Lyme borreliosis by an cnzymc immunoassay detecting immunoglobulin G reactive to purified Borrelia burgdorferi cell components. Ew J Clin Microbial Infect Dis 1991; 10: 422-7 Barbour AC. Isolation and cultivation of Lyme disease spirochaetes. Y&e J Biol Med 1984; 57: 521-S Laemmli UK. Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Namrc 1970: 227: 680-S Barbour AC. Hayes SF, Heiland RA. Schrumpf ME, Tessier SL. A Borrelia-specific monoclonal antibody binds to a tlagellar epitope. Infecf Inmrrn 1986: 52: 54Y-54 Coleman JL, Benach JL. Identification and characterization of an endoflagellar antigen of Borrelitr brrrgdorferi. J Clin imw[ 1989: 84: 321-30
250 Serodiagn. Immunother. Infect. Disease 1993; 5: No 4
25 Blanc0 DR. Champion CI, Miller JN, Lovett MA. Antigenic and structural characterization of Treponemn pallidurn (Nichols strains) endoflagella. Infect Imrnun 1988; 56: 168-75
26 Baig S, Olsson T, Link H. Predominance of Borrelia burgdorferi specific B cells in cerebrospinal fluid in neuroborreliosis. Lancet 1989; 334: 71-4
27 Coyle PK, Schuster SE, Belman AL, Krupp LB, Golightly MG. Cerebrospinal fluid immune complexis in patients exposed to Borrelia hurgdorferi: detection of
Borrelia-specific and non-specific complexis. Ann Neural 1990; 28: 739-44
28 Lane RS, Lenette ET, Madigan JE. Interlaboratory and intralaboratory comparisons of indirect immunofluorescence assays for serodiagnosis of Lyme disease. .I Clin Microbial 1990; 28: 1774-9
29 Marconi RT, Garon CF. Phylogenetic analysis of the genus Borrelia: a comparison of north American and european isolates of Borrelia burgdorferi. Am J Bacterial 1992; 174: 2414
REPRINTS We offer a reprints service in respect of all articles in this journal.
Companies: an article featuring your product or a new application provides its readers with an independent authoritative comment.
Reprints can be used by you to inform and educate your customers and staff about scientific or technical advances in subjects relevant to your
business. They are a cost-effective, ethical way of promoting your company and its products.
For a quotation on your reprint requirements, please contact:
The Reprints Department, Butter-worth-Heinemann Ltd., Linacre House, Jordan Hill, Oxford, OX2 8DI? Tel: +44 (01865 310366. Fax: +44 (01865 314519