interferometric technique for investigation of laser thermal retinal
TRANSCRIPT

Interferometric Technique For Investigation of LoserThermal Retinal Damage
Joel M. Krouss,* Carmen A. Puliafiro,* Wei Z. Lin,f and James G. Fujimoto^:
We describe a new technique for investigating laser-tissue interactions based on the use of an inter-ferometric laser exposure pattern. A Michelson interferometer is used to generate a sinusoidal fringeexposure pattern. The periodicity of the fringe pattern may be adjusted from macroscopic dimensionsto a scale of microns without the need for an imaging plane. Since fringe pattern periodicity is moreadjustable and directly measurable than laser spot size, this technique offers significant advantages forstudying the effects of thermal damage and diffusion in the irradiated tissue. In addition, the compari-son of tissue response with theoretical models is simplified since the sinusoidal fringe pattern is itselfan eigenfunction of the thermal diffusion equation. This technique is demonstrated for argon laserphotocoagulation in the rabbit retina. Exposures at durations comparable to the thermal relaxationtime produced spatially confined lesions, while those at much longer durations resulted in significantdiffusion of the thermal damage beyond the primary targeted regions. The role of thermal diffusion canthus be assessed directly from the ophthalmoscopic and histologic appearances of the lesions. Thistechnique can be employed to study thermal diffusion and other transport phenomena occurring inlaser-tissue interactions for a variety of laser sources and tissue targets. Invest Ophthalmol Vis Sci28:1290-1297,1987
Retinal photocoagulation, the first establishedtherapeutic laser procedure, is widely employed totreat such diseases as macular degeneration1 and dia-betic retinopathy.2 The procedure has undergone in-tensive investigation with regard to mechanisms andextents of tissue damage. It is generally recognizedthat therapeutically desirable retinal lesions resultfrom thermal effects in and around the irradiated re-gions.3 These effects include alteration of the geneticapparatus of cells, inactivation of enzymes, and de-naturation of proteins and nucleic acids, which leadto necrosis, hemostasis and coagulation.4 A determi-nation of the exposure conditions which producehighly localized rather than extended thermal dam-age is clinically relevant to the targeting of specifictissue sites. Sophisticated theoretical models havebeen developed to explain and predict laser-induced
From the * Laser Research Laboratory, Howe Laboratory ofOphthalmology, Massachusetts Eye and Ear Infirmary, and De-partment of Ophthalmology, Harvard Medical School, Boston,Massachusetts, the fZhongshan University, Guangzhou, People'sRepublic of China, and the ^Department of Electrical Engineeringand Computer Science and Research Laboratory of Electronics,Massachusetts Institute of Technology, Cambridge, Massachusetts.
Supported by Office of Naval Research Contract No. N-0014-86K-0117, and by the National Institutes of Health Contract No.1-R01-GM35459-01.
Submitted for publication: October 2, 1986.Reprint requests: Carmen A. Puliafito, MD, Massachusetts Eye
and Ear Infirmary, 243 Charles Street, Boston, MA 02114.
thermal damage in the retina,5"8 and these ultimatelyrely on laboratory measurements for verification orrefutation. It is thus essential from both clinical andtheoretical perspectives to have reliable experimentaltechniques with which to accurately assess thermaldamage.
In addition to laser wavelength and exposure dura-tion, spot size and beam profile have been identifiedas critical parameters affecting retinal tissue re-sponse.910 Until now, studies of laser damage andthermal diffusion in the retina have relied on the useof solid, circular spots to perform the exposures.""16
The correlation of tissue damage with exposure con-ditions is sometimes problematic, since these tech-niques rely on difficult and somewhat arbitrary mea-surements of laser spot size. In this paper we present anew interferometric exposure technique which allowshighly precise determination and adjustability of ex-posure parameters.
Materials and Methods
Theory
The use of a sinusoidally varying interference pat-tern for laser exposure provides a convenient andpowerful approach for the investigation of thermaldiffusion in laser-tissue interactions. In contrast tostandard exposure techniques, the periodicity of theinterference fringe pattern provides an important ex-posure parameter which can in general be more easily
1290
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933140/ on 04/08/2018

No. 8 INTERFEROMETRIC TECHNIQUE FOR STUDY OF RETINAL DAMAGE / Krauss er al. 1291
and accurately measured than laser spot size andbeam profile. In addition, the periodicity of the expo-sure pattern can be continuously varied from macro-scopic dimensions down to a scale comparable to thewavelength of the incident light. Finally, the use of asinusoidally varying exposure simplifies the theoreti-cal modeling of thermal diffusion since the sinusoid isan eigenfunction of the thermal diffusion equation.
When two mutually coherent laser beams of inten-sity Io are directed onto a target, they will interfere toproduce a sinusoidally varying interference fringepattern of the form:
sin (1)
where k = 2TT/A (A = the periodicity of the fringepattern). The periodicity of the interference pattern isdetermined by the optical path difference betweenthe phase fronts of the two laser beams, and can bevaried from macroscopic dimensions to those com-parable to the laser wavelength by adjusting the twoincident laser beams.
It should be stressed that the use of two coherentlyinterfering beams to produce a sinusoidally varyingexposure pattern differs appreciably from other ex-posure techniques such as projecting an image orproducing a Moire pattern. These techniques con-struct the desired exposure at a specific image planeand thus require careful focusing onto the retina orthe exposure pattern will be degraded. In contrast, theinterference exposure pattern generates a sinusoidallyvarying exposure at all planes where the beams over-lap without the need for an image plane. Thus, as-suming that scattering is small, variations in focusingon the retina will produce only a scale change in theexposure without defocusing the fringes.
In order to simulate the conditions in the retina asaccurately as possible, models of thermal diffusion inthe retina have taken into account several factors.These include considerations of the exact locus of theoptical absorption and thermal deposition during theexposure, as well as the role of thermal diffusion be-tween retinal layers and in the transverse direction. Inaddition, the damage characteristic of the retina isitself nonlinear. While these theories can be used tomodel a wide variety of exposure conditions, the so-lutions to the associated differential equations aregenerally quite complex. The use of interference ex-posure patterns can provide a significant simplifica-tion of exposure conditions which facilitates the anal-ysis and the correlation between those conditions andthe resulting tissue response.
In order to illustrate these points, we consider asimple model for thermal diffusion. While this ap-proach does not include many of the processes whichoccur in retinal photocoagulation, it nevertheless
provides qualitatively correct predictions and dem-onstrates the potential applicability of the interfer-ence exposure technique to a wide variety of studies.
The transport of heat17 is governed by the thermaldiffusion equation:
at(2)
where Cis the heat capacity, K'\s the thermal conduc-tivity, and J is the source term representing the depo-sition of the heat via laser absorption. We begin byconsidering the diffusion associated with a tempera-ture change produced by an exposure which is sinu-soidally varying as in equation (1). For simplicitythermal diffusion between the retinal layers is ne-glected, and only the thermal transport transverse tothe fringes is considered. The diffusion then reducesto a single spatial dimension. If it is assumed that thetissue is initially heated in a sinusoidally varying tem-perature distribution, it is possible to examine theeffect of diffusion as a function of time. The solutionof the thermal diffusion equation for a sinusoidallyvarying initial condition is:
8T(x, t) ~8T(l+ e~KkM sin he) (3)
where K = K/C is the thermal diffusivity. As shown,the effect of thermal diffusion is to produce a homog-enization of the sinusoidally varying temperaturechange. That change relaxes exponentially with atime constant:
1 A2
( 4 )
where r is termed the thermal relaxation time, and isa measure of the time required for thermal diffusionto produce a smearing out of the initial sinusoidaltemperature distribution. It should be noted that rdepends on the periodicity of the exposure patternand increases as the square of A.
The role of thermal diffusion in retinal damage isshown schematically in Figure 1. For exposure timeswhich are short compared to the thermal relaxationtime, the thermal diffusion away from the initiallytargeted areas will be minimal and the lesion willresemble the exposure pattern (in this case, the verti-cal lines of the fringe pattern). In contrast, as theexposure time is increased above T, thermal diffusioncan be seen directly in the structure of the lesion andis manifest as a fusing together of the fringe lines.Laser intensity, exposure duration, and fringe period-icity may be systematically varied to study thermaldiffusion and measure the thermal relaxation times.The role of thermal diffusion for given exposure pa-rameters may thus be assessed directly from the ap-pearance of the lesion.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933140/ on 04/08/2018
1292 INVESTIGATIVE OPHTHALMOLOGY & VISUAL SCIENCE / Augusr 1987 Vol. 28
Lesion with negligible^ transverse diffusion
Damage
No Damage
Dominantdiffusion
logT
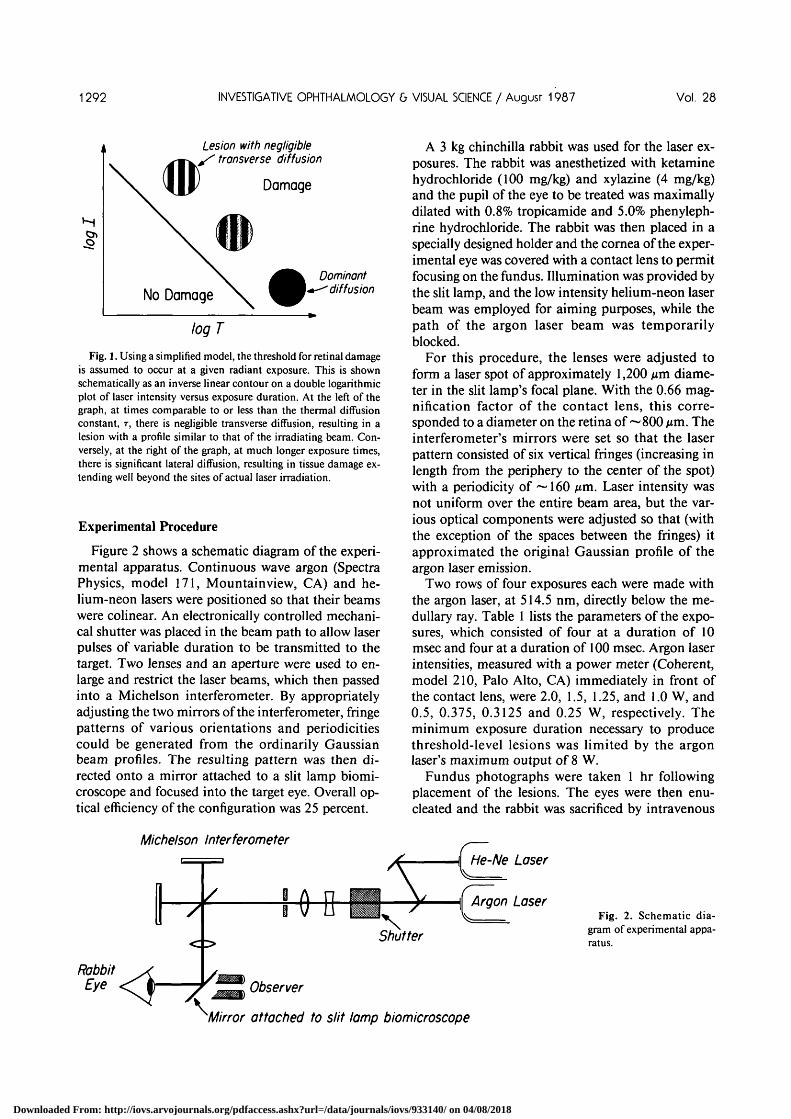
Fig. 1. Using a simplified model, the threshold for retinal damageis assumed to occur at a given radiant exposure. This is shownschematically as an inverse linear contour on a double logarithmicplot of laser intensity versus exposure duration. At the left of thegraph, at times comparable to or less than the thermal diffusionconstant, T, there is negligible transverse diffusion, resulting in alesion with a profile similar to that of the irradiating beam. Con-versely, at the right of the graph, at much longer exposure times,there is significant lateral diffusion, resulting in tissue damage ex-tending well beyond the sites of actual laser irradiation.
Experimental Procedure
Figure 2 shows a schematic diagram of the experi-mental apparatus. Continuous wave argon (SpectraPhysics, model 171, Mountainview, CA) and he-lium-neon lasers were positioned so that their beamswere colinear. An electronically controlled mechani-cal shutter was placed in the beam path to allow laserpulses of variable duration to be transmitted to thetarget. Two lenses and an aperture were used to en-large and restrict the laser beams, which then passedinto a Michelson interferometer. By appropriatelyadjusting the two mirrors of the interferometer, fringepatterns of various orientations and periodicitiescould be generated from the ordinarily Gaussianbeam profiles. The resulting pattern was then di-rected onto a mirror attached to a slit lamp biomi-croscope and focused into the target eye. Overall op-tical efficiency of the configuration was 25 percent.
Michelson Interferometer
A 3 kg chinchilla rabbit was used for the laser ex-posures. The rabbit was anesthetized with ketaminehydrochloride (100 mg/kg) and xylazine (4 mg/kg)and the pupil of the eye to be treated was maximallydilated with 0.8% tropicamide and 5.0% phenyleph-rine hydrochloride. The rabbit was then placed in aspecially designed holder and the cornea of the exper-imental eye was covered with a contact lens to permitfocusing on the fundus. Illumination was provided bythe slit lamp, and the low intensity helium-neon laserbeam was employed for aiming purposes, while thepath of the argon laser beam was temporarilyblocked.
For this procedure, the lenses were adjusted toform a laser spot of approximately 1,200 nm diame-ter in the slit lamp's focal plane. With the 0.66 mag-nification factor of the contact lens, this corre-sponded to a diameter on the retina of ~800 nm. Theinterferometer's mirrors were set so that the laserpattern consisted of six vertical fringes (increasing inlength from the periphery to the center of the spot)with a periodicity of ~ 160 nm. Laser intensity wasnot uniform over the entire beam area, but the var-ious optical components were adjusted so that (withthe exception of the spaces between the fringes) itapproximated the original Gaussian profile of theargon laser emission.
Two rows of four exposures each were made withthe argon laser, at 514.5 nm, directly below the me-dullary ray. Table 1 lists the parameters of the expo-sures, which consisted of four at a duration of 10msec and four at a duration of 100 msec. Argon laserintensities, measured with a power meter (Coherent,model 210, Palo Alto, CA) immediately in front ofthe contact lens, were 2.0, 1.5, 1.25, and 1.0 W, and0.5, 0.375, 0.3125 and 0.25 W, respectively. Theminimum exposure duration necessary to producethreshold-level lesions was limited by the argonlaser's maximum output of 8 W.
Fundus photographs were taken 1 hr followingplacement of the lesions. The eyes were then enu-cleated and the rabbit was sacrificed by intravenous
RabbitEye
Fig. 2. Schematic dia-gram of experimental appa-ratus.
Mirror attached to slit lamp biomicroscope
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933140/ on 04/08/2018
No. 8 INTERFEROMETRIC TECHNIQUE FOR STUDY OF RETINAL DAMAGE / Krouss er ol. 1293
injection of pentobarbitol. The treated eye was imme-diately fixed in a 2% glutaraldehyde, 4% paraformal-dehyde, 0.1 M sodium cacodylate buffer solution. Inpreparation for light microscopy, the retina was em-bedded in JB-4 glycol methacrylate, cut at 2 to 3 jum,and stained with hematoxylin and eosin. All animalprocedures were done in accordance with the ARVOResolution on the Use of Animals in Research.
Results
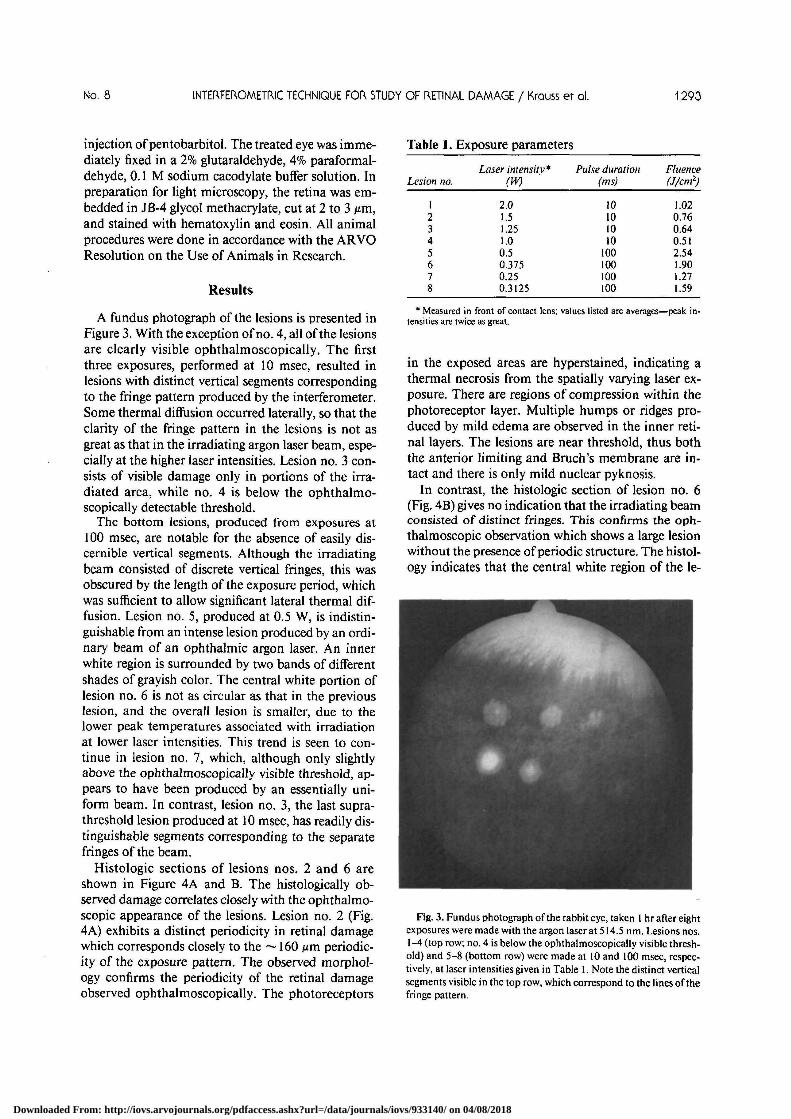
A fundus photograph of the lesions is presented inFigure 3. With the exception of no. 4, all of the lesionsare clearly visible ophthalmoscopically. The firstthree exposures, performed at 10 msec, resulted inlesions with distinct vertical segments correspondingto the fringe pattern produced by the interferometer.Some thermal diffusion occurred laterally, so that theclarity of the fringe pattern in the lesions is not asgreat as that in the irradiating argon laser beam, espe-cially at the higher laser intensities. Lesion no. 3 con-sists of visible damage only in portions of the irra-diated area, while no. 4 is below the ophthalmo-scopically detectable threshold.
The bottom lesions, produced from exposures at100 msec, are notable for the absence of easily dis-cernible vertical segments. Although the irradiatingbeam consisted of discrete vertical fringes, this wasobscured by the length of the exposure period, whichwas sufficient to allow significant lateral thermal dif-fusion. Lesion no. 5, produced at 0.5 W, is indistin-guishable from an intense lesion produced by an ordi-nary beam of an ophthalmic argon laser. An innerwhite region is surrounded by two bands of differentshades of grayish color. The central white portion oflesion no. 6 is not as circular as that in the previouslesion, and the overall lesion is smaller, due to thelower peak temperatures associated with irradiationat lower laser intensities. This trend is seen to con-tinue in lesion no. 7, which, although only slightlyabove the ophthalmoscopically visible threshold, ap-pears to have been produced by an essentially uni-form beam. In contrast, lesion no. 3, the last supra-threshold lesion produced at 10 msec, has readily dis-tinguishable segments corresponding to the separatefringes of the beam.
Histologic sections of lesions nos. 2 and 6 areshown in Figure 4A and B. The histologically ob-served damage correlates closely with the ophthalmo-scopic appearance of the lesions. Lesion no. 2 (Fig.4A) exhibits a distinct periodicity in retinal damagewhich corresponds closely to the ~ 160 Mm periodic-ity of the exposure pattern. The observed morphol-ogy confirms the periodicity of the retinal damageobserved ophthalmoscopically. The photoreceptors
Table 1. Exposure parameters
Lesion no.
123456f;
S:
Laser intensity*(W)
2.01.51.251.00.50.3750.250.3125
Pulse duration(ms)
10101010
100100100100
Fluence(J/cm*)
1.020.760.640.512.541.901.271.59
' Measured in front of contact lens; values listed are averages—peak in-tensities are twice as great.
in the exposed areas are hyperstained, indicating athermal necrosis from the spatially varying laser ex-posure. There are regions of compression within thephotoreceptor layer. Multiple humps or ridges pro-duced by mild edema are observed in the inner reti-nal layers. The lesions are near threshold, thus boththe anterior limiting and Bruch's membrane are in-tact and there is only mild nuclear pyknosis.
In contrast, the histologic section of lesion no. 6(Fig. 4B) gives no indication that the irradiating beamconsisted of distinct fringes. This confirms the oph-thalmoscopic observation which shows a large lesionwithout the presence of periodic structure. The histol-ogy indicates that the central white region of the le-
Fig. 3. Fundus photograph of the rabbit eye, taken 1 hr after eightexposures were made with the argon laser at 514.5 nm. Lesions nos.1 -4 (top row; no. 4 is below the ophthalmoscopically visible thresh-old) and 5-8 (bottom row) were made at 10 and 100 msec, respec-tively, at laser intensities given in Table 1. Note the distinct verticalsegments visible in the top row, which correspond to the lines of thefringe pattern.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933140/ on 04/08/2018

1294 INVESTIGATIVE OPHTHALMOLOGY & VISUAL 5CIENCE / August 1987 Vol. 28
100
Fig. 4. Histologic sections of lesions 2 (A) and 6 (B). For a 10 msec, near-threshold laser exposure, retinal damage is highly localized on thesites of the irradiation (arrows in A). Conversely, for a 100 msec, near-threshold exposure, thermal diffusion causes delocalized retinal damage(B). There is a clear correlation between the extent and type of histologic damage and the ophthalmoscopic appearance of the respectivelesions. Sections were stained with hematoxylin and eosin (original magnification XI72).
sion corresponds to severe damage in the neural ret-ina. A large ~300 ^m central lesion is observed fromthe widespread thermal diffusion of the heat asso-ciated with the long exposure time. The integrity ofthe ganglion and nerve fiber layer is lost. The innernuclear layer is widely dispersed, while the outer layeris alternately elevated and depressed. There is severecondensation within the photoreceptor layer. RPEcells are condensed centrally, while Bruch's mem-brane remains intact.
Discussion
Fringe patterns from low intensity helium-neonlasers have been used with some success to predictpotential visual acuity in patients undergoing treat-ment for cataracts,18 amblyopia,19 corneal opacifica-tion20 and macular degeneration.21 This is done byprojecting the fringe pattern onto the retina and de-termining the smallest fringe periodicity which theindividual is able to resolve. Helium-neon laser inter-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933140/ on 04/08/2018

No. 8 INTERFEROMETRIC TECHNIQUE FOR STUDY OF RETINAL DAMAGE / Krouss er ol. 1295
ferometers for these and other applications are avail-able commercially. To our knowledge, however, ourtechnique represents the first reported use of interfer-ometry for examining direct laser effects on theretina.
Retinal heating results from absorption of incidentradiation by one or more of its three principal chro-mophores. These include melanin (located in the re-tinal pigment epithelium, with little variation in ab-sorption across the visible portion of the spectrum),hemoglobin (in blood vessels, with highest absorptionfor yellow light), and xanthophyll (in the inner andouter plexiform. layers of the macula, with highestabsorption for blue light). Argon laser green (514.5nm) radiation is absorbed primarily by randomly dis-tributed melanin granules in the pigment epithelium,the monocellular layer which in the chinchilla rabbitis about 10 nm thick.8 Of argon laser intensity enter-ing the cornea, only 18.5 percent is dissipated in theocular media, while 51.5 percent is absorbed by thepigment epithelium.22 The physiological basis for ret-inal photocoagulation is the destruction of the pho-toreceptors by thermal action spreading from ab-sorption (in the case of the argon laser) by the pig-ment epithelial melanin granules.23
As laser treatments require increased precision, it isimportant to have a thorough understanding of theeffects of various lasers on their intended targets. Ofprimary concern is the evaluation of current and po-tential clinical procedures and the testing of modelsfor laser-tissue interactions. In addition, there is also aneed to establish safety levels for inadvertent expo-sure to lasers in industry, the military and the labora-tory.
The use of the interferometric fringe exposure pro-vides a direct ophthalmoscopic and histologic indica-tor for the role of thermal diffusion in the localizationof lesions. Experimental results are in qualitativeagreement with our simplified model. According toequation (4), using a fringe pattern periodicity of 160Mm and a K of 1.3 X 10"3 cm2/s (the value for liquidwater), T for the retina is approximately 5 msec. Therelatively large spot sizes used here made the resultsmore readily discernible, but prevented us fromachieving sufficiently high fluences at 5 msec. Even at10 msec, however, it was apparent both ophthalmo-scopically and histologically that the tissue had beenirradiated by a beam with discrete vertical segments.
Ophthalmoscopic observations indicate a definiteperiodicity in the top row of lesions (Fig. 3), demon-strating that only minimal thermal diffusion oc-curred for the 10 msec exposures. Because of thethreshold nature of retinal damage, the histologicallyobserved retinal morphology does not exactly reflectgradual variations in damage corresponding to the
sinusoidal exposure pattern. Rather, the retinal dam-age is present in areas where the induced temperaturechange exceeds the damage threshold. It should bestressed, however, that the histologically observeddamage exhibits a distinct ~ 160 nm periodicity thatcorresponds to the laser exposure and thus confirmsthe ophthalmoscopic observation of distinct verticaldamage stripes. It is interesting to note that the peri-odicity of the damage is less than the thickness of theretina itself, indicating that retinal damage may behighly localized in the transverse direction by appro-priate choice of exposure parameters.
As expected, results from irradiation at 100 msecbelied the fringe pattern of the argon laser beam. Ex-posure at some 20 times the thermal diffusion con-stant allowed sufficient time for heat to spread be-tween the fringe-like areas that were actually irra-diated. As intensity was lowered, overall thermaldamage was less severe and approached thresholdlevels, yet always with damage covering essentiallythe entire circular area. The critical determinant ofthermal diffusion is exposure duration, not intensity.These are the results predicted in Figure 1. For bothexposure times, tissue damage was qualitatively simi-lar to that observed for more conventional exposuremethods.24-25
Although the argon laser26 is the source most oftenused for retinal photocoagulation, for some patholo-gies and under certain conditions within the eye it isdesirable to use other lasers, sometimes to selectivelytarget specific areas or layers of the retina. The kryp-ton laser,27 with emission at 568 and 647 nm, is fre-quently used for photocoagulation, and as newsources, such as metal vapor and dye lasers, becomeavailable, they may be tested to determine if theyprovide a particular advantage for clinical use. Over-all retinal absorption varies considerably for the visi-ble and near infrared wavelengths,28 and there isstrong interest in customizing photocoagulation tospecific retinal conditions.2930 The interferometricexposure technique should facilitate the evaluationof, and distinction among, the thermal effects of dif-ferent laser sources. It should be noted, however, thatphotocoagulation with the fringe pattern itself wouldprobably not offer any improvement over existingtherapeutic techniques. Rather, it is an investigativeand diagnostic technique with which to more pre-cisely study fundamental laser interactions with theretina. Our results graphically demonstrate charac-teristics of thermal diffusion in the retina that may behelpful in further refining existing clinical methods.
Retinal photocoagulation is not without its risks.Threshold levels for a given amount of tissue damagedecrease along with exposure duration, and it hasbeen suggested31 that procedures requiring less watt-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933140/ on 04/08/2018

1296 INVESTIGATIVE OPHTHALMOLOGY 6 VISUAL SCIENCE / Augusr 1987 Vol. 28
age are at lower risk for complications. Clinical pho-tocoagulation is typically performed at exposure du-rations of at least 100 msec.32 In view of our findings,it would appear that some procedures might be moreeffectively performed with shorter times. In particu-lar, treatment in the macular region and near bloodvessels might be more accurately performed at timeson the order of 1-10 msec, since tissue damage wouldbe limited to the immediately targeted regions. Expo-sures with too short times would be inadvisable, how-ever, since they run the risk of causing acoustic shockwave damage and hemorrhage.
While we have demonstrated the interferometrictechnique in the context of retinal photocoagulation,the majority of other biomedical laser applicationsalso rely on thermal effects.4 This approach couldeasily be adapted to other tissues. Anderson and Par-rish33 have proposed an intriguing method of lasersurgery, "selective photothermolysis," in which se-lective damage is determined not by precise aiming ofthe laser beam but by the unique absorption proper-ties of the intended target. If the target has an absorp-tion coefficient at least twice as great as that of thesurrounding tissue at a given wavelength, preferentialabsorption will result in localized thermal damage ifirradiation is performed at a duration similar to orless than the thermal diffusion constant. Shortness ofthe exposures is determined largely by the size of thetarget. Anderson and Parrish used this method to se-lectively damage blood vessels (3 X 10~7 s, 577 nm)and melanocytes (2 X 10"8 s, 351 nm), although se-lective photothermolysis is, in principal, applicableeven at the subcellular level. Selective photothermol-ysis depends on the selective absorption properties ofspecific target chromophores for suitably brief pulses,while the interferometric exposure technique directlydemonstrates thermal diffusion by employing selec-tive irradiation with the fringe pattern. By appropri-ately adjusting the fringe pattern periodicity, the in-terferometric technique could be used to determinethermal damage and absorption characteristics of awide range of potential targets of biomedical interest.
In principle, the interferometric technique can alsobe used to study other processes in laser-tissue inter-actions. The only factor limiting its applicability isthe necessity of maintaining the coherence of thelaser beams in order for the fringe pattern to be prop-erly constructed. Procedures that involve significantscattering in turbid media would thus be difficult tostudy in this manner. However, one process thatshould be suitable for this method is excimer lasertissue ablation. This phenomenon has been consid-ered in the eye principally for corneal surgery.34 Rela-tive contributions of thermal and photochemicalmechanisms to the ablation process are currently
being debated, and are of considerable relevance tothe procedure's application to any potential tissuetarget. Histologic examination of tissue sections fol-lowing irradiation with appropriately adjusted inter-ferometric fringe patterns could be instrumental inelucidating the fundamental nature of this procedure.
Key words: fringe pattern, interferometer, laser, photoco-agulation, retina, thermal diffusion
Acknowledgments
We wish to thank Bob Schoenlein and Joan Palumbo,and Drs. R. Rox Anderson, Erich Ippen and ReginaldBiragruber, for their assistance and advice on this study.
References1. Macular Photocoagulation Study Group: Argon laser photo-
coagulation for senile macular degeneration: Results of a ran-domized clinical trial. Arch Ophthalmol 100:912, 1982.
2. The Diabetic Retinopathy Study Research Group: Photocoag-ulation treatment of proliferative diabetic retinopathy: Thesecond report of diabetic retinopathy study findings. Ophthal-mology 85:82, 1978.
3. Mellerio J: The thermal nature of retinal laser photocoagula-tion. Exp Eye Res 5:242, 1966.
4. Hillenkamp F: Interaction between laser radiation and biologi-cal systems. In Lasers in Biology and Medicine, Hillenkamp F,Pratesi R, and Sacchi CA, editors. New York, Plenum, 1980 p.37.
5. Clarke AM, Geeraets WJ, and Ham WT: An equilibriumthermal model for retinal injury from optical sources. AppliedOptics 8:1951, 1969.
6. Mainster MA, White TJ, Tips JH, and Wilson PW: Spectraldependence of retinal damage produced by intense lightsources. J Opt Soc Am 60:848, 1970.
7. Roulier A: Calculation of the thermal effect generated in theretina by photocoagulation. Graefes Arch Clin Exp Ophthal-mol 181:281, 1971.
8. Birngruber R, Hillenkamp F, and Gabel VP: Theoretical in-vestigations of laser thermal retinal injury. Health Physics48:781, 1985.
9. Welch AJ and Polhamus GD: Measurement and prediction ofthermal injury in the retina of the rhesus monkey. IEEE TransBiomed Eng BME-31:633, 1984.
10. Welch AJ, Priebe LA, Forster LD, Gilbert R, Lee C, and DrakeP: Experimental validation of thermal retinal models of dam-age from laser radiation. USAF School Aerospace Medicine,Contract F33615-76-C-0605, Final Rep, 1978.
11. L'Esperance FA and Kelly GR: The threshold of the retina todamage by argon laser radiation. Arch Ophthalmol 81:583,1969.
12. Bresnick GH, Frisch GD, Powell JO, Landers MB, Hoist GC,and Dallas AG: Ocular effects of argon laser radiation I. Reti-nal damage threshold studies. Invest Ophthalmol 9:901, 1970.
13. Beatrice ES and Frisch GD: Retinal laser damage thresholds asa function of image diameter. Arch Environ Health 27:322,1973.
14. Cain CP and Welsh AJ: Measured and predicted laser inducedtemperature rise in the rabbit fundus. Invest Ophthalmol13:60, 1974.
15. Priebe LA, Cain CP, and Welsh AJ: Temperature rise requiredfor production of minimal lesions in the Macaca mulatto ret-ina. Am J Ophthalmol 79:405, 1975.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933140/ on 04/08/2018

No. 8 INTERFEROMETRIC TECHNIQUE FOR STUDY OF RETINAL DAMAGE / Krouss er ol. 1297
16. Birngruber R, Gabel VP, and Hillenkamp F: Experimentalstudies of laser thermal retinal injury. Health Physics 44:519,1983.
17. Lightfoot EN, Bird R, and Stewart W: Transport Phenomena.New York, John Wiley and Sons, 1960.
18. Green DG: Testing the vision of cataract patients by means oflaser-generated interference fringes. Science 168:1240, 1970.
19. Selenow A, Ciuffreda KJ, Mozlin R, and Rumpf D: Prognosticvalue of laser interferometric visual acuity in amblyopia ther-apy. Invest Ophthalmol Vis Sci 27:273, 1986.
20. Gstalder RJ and Green DG: Laser interferometry in cornealopacification. Arch Ophthalmol 87:269, 1972.
21. Bloom TD, Fishman GA, and Traubert BS: Laser interfero-metric visual acuity in senile macular degeneration. ArchOphthalmol 101:925, 1983.
22. Lachenmayr B, Birngruber R, and Gabel VP: The wavelengthdependence of light absorption in the fundus of the eye, partic-ularly regarding argon-, krypton- and neodymium-laser emis-sion. Doc Ophthal Proc Series 36:3, 1984.
23. Wolbarsht ML and Landers MB: Some considerations forchoosing the wavelength appropriate for laser photocoagula-tion of the retina. In Laser Treatment and Photocoagulation ofthe Eye. Proceedings of the International Symposium, Birn-gruber R and Gabel VP, editors. The Hague, Junk, 1984, p. 11.
24. Marshall J and Mellerio J: Histology of the formation of retinallaser lesions. Exp Eye Res 6:4, 1967.
25. Powell JO, Bresnick GH, YanoffM, Frisch GD, and Chester
JE: Ocular effects of argon laser radiation. II. Histopathologyof chorioretinal lesions. Am J Ophthalmol 71:1267, 1971.
26. L'Esperance FA: An ophthalmic argon laser photocoagulationsystem: Design, construction, and laboratory investigations.Trans Am Ophthalmol Soc 66:827, 1968.
27. L'Esperance FA: Clinical photocoagulation with the kryptonlaser. Arch Ophthalmol 87:693, 1972.
28. Geeraets WJ and Berry ER: Ocular spectral characteristics asrelated to hazards from lasers and other light sources. Am JOphthalmol 66:15, 1968.
29. Wieder M, Pomerantzeff O, and Schneider J: Retinal vesselphotocoagulation: A quantitative comparison of argon andkrypton laser effects. Invest Ophthalmol Vis Sci 20:418, 1981.
30. Trempe CL, Mainster MA, Pomerantzeff O, Avila MP, JalkhAE, Weiter JJ, McMeel JW, and Schepens CL: Macular pho-tocoagulation. Optimal wavelength selection. Ophthalmology89:721, 1982.
31. Goldberg MF and Herbst RW: Acute complications of argonlaser photocoagulation, epipapillary and peripapillary neovas-cularization. Arch Ophthalmol 89:311, 1973.
32. Sigelman J: Retina Diseases: Pathogenesis, Laser Therapy, andSurgery. Boston, Little, Brown, 1984, p. 67.
33. Anderson RR and Parrish JA: Selective photothermolysis:Precise microsurgery by selective absorption of pulsed radia-tion. Science 200:524, 1983.
34. Krauss JM, Puliafito CA, and Steinert RF: Laser interactionswith the cornea. Surv Ophthalmol 31:37, 1986.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933140/ on 04/08/2018