intensity dependent repetitive transcranial magnetic stimulation modulation of blood oxygenation
TRANSCRIPT

Journal of Affective Disorders 136 (2012) 1243–1246
Contents lists available at SciVerse ScienceDirect
Journal of Affective Disorders
j ourna l homepage: www.e lsev ie r.com/ locate / j ad
Brief report
Intensity dependent repetitive transcranial magnetic stimulationmodulation of blood oxygenation
Richard H. Thomson a, Nigel C. Rogasch a, Jerome J. Maller a,Zafiris J. Daskalakis b, Paul B. Fitzgerald a,⁎a Monash Alfred Psychiatry Research Centre, The Alfred and Monash University School of Psychology and Psychiatry, Victoria, Australiab Centre for Addiction and Mental Health, University of Toronto, Toronto, Ontario, Canada
a r t i c l e i n f o
⁎ Corresponding author at: MAPrc, First Floor, OldAlfred, Commercial RdMelbourne, Victoria, 3004, Aust6552; fax: +61 3 9076 6588.
E-mail address: [email protected] (P.B.
0165-0327/$ – see front matter © 2011 Elsevier B.V.doi:10.1016/j.jad.2011.08.005
a b s t r a c t
Article history:Received 25 November 2010Received in revised form 11 July 2011Accepted 3 August 2011Available online 27 August 2011
Background: Repetitive transcranial magnetic stimulation (rTMS) is increasingly beinginvestigated in clinical settings for the treatment of neurological and psychiatric disorderssuch as dystonia, schizophrenia, and major depressive disorder (MDD). Using near infra-redspectroscopy (NIRS), very short trains of rTMS have previously been shown to modulatecortical blood oxygenation.Methods: In order to investigate the effect of longer, clinically relevant trains of 1 Hz rTMS onoxy-hemoglobin (HbO) at prefrontal cortex, the current study applied ten minute trains ofrTMS at both subthreshold and suprathreshold intensities.Results: A similar profile of oxygenation change was observed during the beginning 30–40 s ofthe trains, however for the remainder, subthreshold rTMS returned to baseline while thesuprathreshold TMS resulted in a long period of reduced oxygenation.Limitations: Small sample size.Conclusions: The differences observed may be a product of changes in HbO requirements byinhibitory/excitatory neural circuits, either by reduced HbO demand or by increased HbOconsumption, while sustained HbO reduction may be a consequence of a modulation of vaso-motor reactivity. This study has implications for understanding themechanisms involved in thephysiological changes evoked by rTMS and efficacious clinical application of rTMS in disorderssuch as MDD.
© 2011 Elsevier B.V. All rights reserved.
Keywords:Transcranial magnetic stimulationBlood oxygenationPrefrontal cortexMajor Depressive Disorder
1. Introduction
In both clinical and research applications, transcranialmagnetic stimulation (TMS) has become an important tool inthe fields of neurophysiology, neurology, and psychiatry(Fitzgerald et al., 2002). The application of repetitive stimu-lation (rTMS) has been shown to produce changes in brainactivity (Fitzgerald et al., 2006b) and it is increasingly beingapplied in therapeutic applications such as major depressivedisorder (Fitzgerald et al., 2006a; O'Reardon et al., 2007)
Baker Building, Theralia. Tel.: +61 3 9076
Fitzgerald).
All rights reserved.
although the mechanism of its effects is not fully understood.One line of research aimed at exploring the effects of rTMS onthe brain has examined changes in hemodynamic responsesresulting from rTMS. However, the focus of these studies haspredominately been on the effects of very short rTMS trainsthat are not as clinically relevant as longer trains of rTMS orthe cumulative effects of multiple trains that are frequentlyused in practice.
Near infra-red spectroscopy (NIRS) is a technique formeasuring blood oxygenation (HbO) that combines a hightemporal resolution with a high signal to noise ratio, andtherefore meets the requirements for monitoring the corticalresponse to TMS (Gratton et al., 1997). Previous researchwhich has used NIRS to study the effects of single TMS pulses,for example (Mochizuki et al., 2006; Thomson et al., 2011b),

1244 R.H. Thomson et al. / Journal of Affective Disorders 136 (2012) 1243–1246
paired TMS pulses (Thomson et al., 2011a) and rTMS(Aoyama et al., 2009; Kozel et al., 2009), have quiteconsistently demonstrated that higher intensity TMS resultsin a drop in HbO, both at primary motor cortex (M1) and atprefrontal cortex (PFC), while subthreshold single pulse TMSresults in a more recognizable increase in HbO that wouldbe expected to be seen during normal brain activation. TMS atsuprathreshold intensities is speculated to result in ‘unnatural’brain activation, producing a non-standard hemodynamicresponse, i.e. a drop in HbO (Mochizuki et al., 2006; Thomsonet al., 2011a,b). In clinical practice, long trains of suprathresholdTMS are routinely used in treating a variety of disorders.Research by Loo et al. (2003) using single photon emissioncomputed tomography (SPECT) demonstrated differentialeffects of rTMS frequency upon regional cerebral blood flow(rCBF),with low frequency (1 Hz) rTMS resulting in lower rCBFduring stimulation.While there are limitations upon the lengthof the interval over which rCBF can be assessed using SPECT, byemploying NIRS it becomes possible to investigate relativechanges in blood oxygenation directly, and for the entireduration of a long train.
Therefore, the aim of the current studywas to compare theeffects of long (10 min) trains of both subthreshold andsuprathreshold repetitive low frequency TMS on changes inHbO at a clinically relevant cortical brain region, in this casethe PFC. It was hypothesized that suprathreshold TMS wouldresult in continuously decreased HbO similar to that observedin previous single pulse and repetitive TMS studies (Aoyamaet al., 2009; Kozel et al., 2009;Mochizuki et al., 2006; Thomsonet al., 2011a,b).
2. Method
2.1. Subjects
Data was collected for 6 right handed subjects (3 females,age 26±4). The experimental procedures conformed tothe declaration of Helsinki and were approved by The AlfredHospital Ethics Committee. All participants gave writteninformed consent.
2.2. EMG and TMS
Electromyographic (EMG) activity was recorded fromAg/AgCl surface electrodes placed over the first dorsal inter-osseus (FDI) muscle in a belly-tendonmontage. The signal wasamplified (1000×), filtered (20–2000 Hz), and sampled at5 kHz. TMS was applied using a figure-of-8 coil over the lefthemisphere at a 45° angle from the midline by a MagVentureR30 (MagVenture, Copenhagen, Denmark). Resting motorthreshold (rMT) was defined as the minimal TMS intensityneeded to evoke anMEP in right FDI larger than 50 μV in threeof five consecutive trials (Carroll et al., 2001).
During the experiment, the TMS was applied over thePFC, between F3 and AF3 in the 10–20 system, just posteriorto the hairline where the NIRS probe was located. The probeemitters were located medially and the photodetector waslocated laterally. (Fitzgerald et al., 2009; Thomson et al.,2011a,b). Participants were tested on two counterbalancedsessions at least 24 h apart with TMS delivered at either 80%or 120% of rMT. Each session consisted of two 10 minute
blocks of 1 Hz TMS with a 20 minute rest interval betweenblocks. This length of time was chosen since several studieshave indicated that this is sufficient for changes in neuralexcitability evoked by rTMS to return to baseline levels (Chenet al., 1997; Romero et al., 2002).
2.3. NIRS
An Oximeter Model 96108 (OxiTS; ISS Inc, Champaign,Illinois, USA) was used to collect DC, AC, and phase data foreach wavelength (687 nm and 830 nm) sampled at 50 Hzusing a single channel. The Differential Pathlength Factor(DPF) and change in absorption were calculated from the ACand phase (Fantini et al., 1999) and changes in HbOwere thencalculated with the extinction coefficients corresponding tothe selected wavelengths (Toronov et al., 2001). Quantifyingthese changes assumes a homogenous scattering medium, anassumption that may be nullified by the non-homogenouslayering of head tissues, hence they are expressed in arbitraryunits (a.u) (Toronov et al., 2001). The signal was smoothedusing a zero phase shift moving average filter (length of 2 s)and linearly detrended to remove drift (Matsuda and Hiraki,2006). The mean blood oxygenation (HbO) was measuredover the duration of the rTMS and split into five blocks of2 minute intervals. These values were analyzed by repeatedmeasures ANOVA with block (T1-5) and intensity (80%,120%) as factors. Post hoc multiple comparisons werecorrected by Tukey's HSD. In order to visualize the longterm changes in HbO, the signal was smoothed using amoving average filter with a length of 20 s.
3. Results
On average, blood oxygenation during TMS followed asimilar profile over the first 30–40 s of the train (Fig. 1A).However, the two signals then differed markedly, with thesuprathreshold TMS resulting in a continual drop in HbObefore reaching an approximate plateau after 2 min (Fig. 1B).The subthreshold TMS demonstrated a period of slightlyelevated HbO at around the 4–5 minute mark before return-ing to baseline levels. At the cessation of the suprathresholdTMS, HbO rapidly returned to baseline levels. When compar-ing mean HbO across time, there was a significant main effectof intensity (F=7.3, pb0.05), with HbO significantly lowerduring the 120% rMT TMS compared to 80%, and there was asignificant interaction between block and intensity (F=3.0,pb0.05). Post-hoc tests revealed that this was due to sig-nificant differences between the two intensities at each timeinterval (pb0.05), except for the first 2 min (p=0.7).
4. Discussion
The current study found that 10 minute trains of 1 HzrTMS delivered at 120% of rMT resulted in decreased HbOlevels compared with 80% rMT during the period ofstimulation. HbO levels returned rapidly to baseline followingthe end of the stimulation train. To our knowledge, this is thefirst time that the changes in HbO evoked by these clinicallyrelevant trains, in terms of length and intensity, have beensystematically investigated.
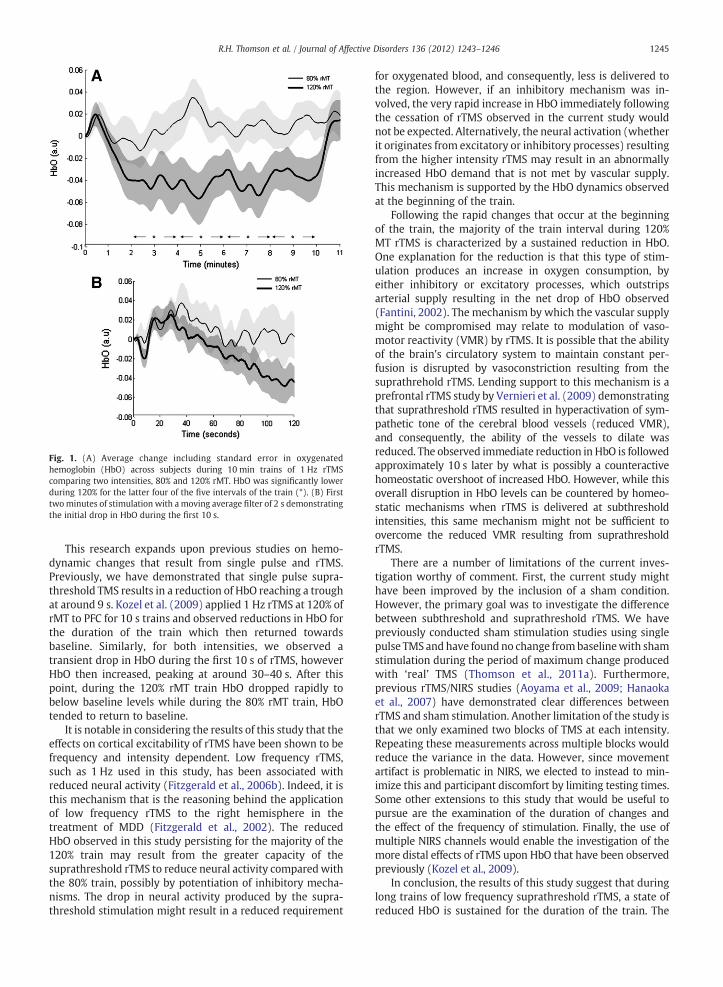
Fig. 1. (A) Average change including standard error in oxygenatedhemoglobin (HbO) across subjects during 10 min trains of 1 Hz rTMScomparing two intensities, 80% and 120% rMT. HbO was significantly lowerduring 120% for the latter four of the five intervals of the train (*). (B) Firsttwominutes of stimulation with a moving average filter of 2 s demonstratingthe initial drop in HbO during the first 10 s.
1245R.H. Thomson et al. / Journal of Affective Disorders 136 (2012) 1243–1246
This research expands upon previous studies on hemo-dynamic changes that result from single pulse and rTMS.Previously, we have demonstrated that single pulse supra-threshold TMS results in a reduction of HbO reaching a troughat around 9 s. Kozel et al. (2009) applied 1 Hz rTMS at 120% ofrMT to PFC for 10 s trains and observed reductions in HbO forthe duration of the train which then returned towardsbaseline. Similarly, for both intensities, we observed atransient drop in HbO during the first 10 s of rTMS, howeverHbO then increased, peaking at around 30–40 s. After thispoint, during the 120% rMT train HbO dropped rapidly tobelow baseline levels while during the 80% rMT train, HbOtended to return to baseline.
It is notable in considering the results of this study that theeffects on cortical excitability of rTMS have been shown to befrequency and intensity dependent. Low frequency rTMS,such as 1 Hz used in this study, has been associated withreduced neural activity (Fitzgerald et al., 2006b). Indeed, it isthis mechanism that is the reasoning behind the applicationof low frequency rTMS to the right hemisphere in thetreatment of MDD (Fitzgerald et al., 2002). The reducedHbO observed in this study persisting for the majority of the120% train may result from the greater capacity of thesuprathreshold rTMS to reduce neural activity comparedwiththe 80% train, possibly by potentiation of inhibitory mecha-nisms. The drop in neural activity produced by the supra-threshold stimulation might result in a reduced requirement
for oxygenated blood, and consequently, less is delivered tothe region. However, if an inhibitory mechanism was in-volved, the very rapid increase in HbO immediately followingthe cessation of rTMS observed in the current study wouldnot be expected. Alternatively, the neural activation (whetherit originates from excitatory or inhibitory processes) resultingfrom the higher intensity rTMS may result in an abnormallyincreased HbO demand that is not met by vascular supply.This mechanism is supported by the HbO dynamics observedat the beginning of the train.
Following the rapid changes that occur at the beginningof the train, the majority of the train interval during 120%MT rTMS is characterized by a sustained reduction in HbO.One explanation for the reduction is that this type of stim-ulation produces an increase in oxygen consumption, byeither inhibitory or excitatory processes, which outstripsarterial supply resulting in the net drop of HbO observed(Fantini, 2002). The mechanism by which the vascular supplymight be compromised may relate to modulation of vaso-motor reactivity (VMR) by rTMS. It is possible that the abilityof the brain's circulatory system to maintain constant per-fusion is disrupted by vasoconstriction resulting from thesuprathrehold rTMS. Lending support to this mechanism is aprefrontal rTMS study by Vernieri et al. (2009) demonstratingthat suprathreshold rTMS resulted in hyperactivation of sym-pathetic tone of the cerebral blood vessels (reduced VMR),and consequently, the ability of the vessels to dilate wasreduced. The observed immediate reduction in HbO is followedapproximately 10 s later by what is possibly a counteractivehomeostatic overshoot of increased HbO. However, while thisoverall disruption in HbO levels can be countered by homeo-static mechanisms when rTMS is delivered at subthresholdintensities, this same mechanism might not be sufficient toovercome the reduced VMR resulting from suprathresholdrTMS.
There are a number of limitations of the current inves-tigation worthy of comment. First, the current study mighthave been improved by the inclusion of a sham condition.However, the primary goal was to investigate the differencebetween subthreshold and suprathreshold rTMS. We havepreviously conducted sham stimulation studies using singlepulse TMS and have found no change frombaselinewith shamstimulation during the period of maximum change producedwith ‘real’ TMS (Thomson et al., 2011a). Furthermore,previous rTMS/NIRS studies (Aoyama et al., 2009; Hanaokaet al., 2007) have demonstrated clear differences betweenrTMS and sham stimulation. Another limitation of the study isthat we only examined two blocks of TMS at each intensity.Repeating these measurements across multiple blocks wouldreduce the variance in the data. However, since movementartifact is problematic in NIRS, we elected to instead to min-imize this and participant discomfort by limiting testing times.Some other extensions to this study that would be useful topursue are the examination of the duration of changes andthe effect of the frequency of stimulation. Finally, the use ofmultiple NIRS channels would enable the investigation of themore distal effects of rTMS upon HbO that have been observedpreviously (Kozel et al., 2009).
In conclusion, the results of this study suggest that duringlong trains of low frequency suprathreshold rTMS, a state ofreduced HbO is sustained for the duration of the train. The

1246 R.H. Thomson et al. / Journal of Affective Disorders 136 (2012) 1243–1246
mechanism involved is unclear, however it may possiblybe described as the result of two mechanisms. Early HbOdynamicsmay be a product of changes in HbO requirements byinhibitory/excitatory neural circuits, either by reduced HbOdemand or by increased HbO consumption, while sustainedHbO reduction may be a consequence of a modulation of VMR.
Role of funding sourceFunding for this study was provided by an Australian Research Council
grant (PBF), a National Health and Medical Research Council (NHMRC)Practitioner Fellowship (PBF) and by a National Alliance for Research onSchizophrenia and Depression (NARSAD) Independent Investigator award(ZJD); these bodies had no further role in study design; in the collection,analysis and interpretation of data; in the writing of the report; or in thedecision to submit the paper for publication.
Conflict of interestPBF has received equipment for research from MagVenture A/S and
Brainsway Ltd.
AcknowledgmentsThis work was funded by an Australian Research Council (ARC) grant
(PBF), a National Health andMedical Research Council (NHMRC) PractitionerFellowship (PBF) and by a National Alliance for Research on Schizophreniaand Depression (NARSAD) Independent Investigator award (ZJD). Theauthors gratefully acknowledge the assistance of all persons and volunteerswhose participation was essential in the successful completion of the study.
References
Aoyama, Y., Hanaoka, N., Kameyama,M., Suda, M., Sato, T., Song,M., Fukuda, M.,Mikuni, M., 2009. Stimulus intensity dependence of cerebral blood volumechanges in left frontal lobe by low-frequency rTMS to right frontal lobe: anear-infrared spectroscopy study. Neurosci. Res. 63, 47–51.
Carroll, T.J., Riek, S., Carson, R.G., 2001. Reliability of the input-output propertiesof the cortico-spinal pathway obtained from transcranial magnetic andelectrical stimulation. J. Neurosci. Methods 112, 193–202.
Chen, R., Classen, J., Gerloff, C., Celnik, P., Wassermann, E.M., Hallett, M., Cohen,L.G., 1997. Depression of motor cortex excitability by low-frequencytranscranial magnetic stimulation. Neurology 48, 1398–1403.
Fantini, S., 2002. A haemodynamic model for the physiological interpretationof in vivo measurements of the concentration and oxygen saturation ofhaemoglobin. Phys. Med. Biol. 47, N249–N257.
Fantini, S., Hueber, D., Franceschini,M.A.,Gratton, E., Rosenfeld,W., Stubblefield,P.G., Maulik, D., Stankovic, M.R., 1999. Non-invasive optical monitoring ofthe newborn piglet brain using continuous-wave and frequency-domainspectroscopy. Phys. Med. Biol. 44, 1543–1563.
Fitzgerald, P.B., Brown, T.L., Daskalakis, Z.J., 2002. The application of transcranialmagnetic stimulation in psychiatry and neurosciences research. ActaPsychiatr. Scand. 105, 324–340.
Fitzgerald, P.B., Benitez, J., de Castella, A., Daskalakis, Z.J., Brown, T.L.,Kulkarni, J., 2006a. A randomized, controlled trial of sequential bilateralrepetitive transcranial magnetic stimulation for treatment-resistantdepression. Am. J. Psychiatry 163, 88–94.
Fitzgerald, P.B., Fountain, S., Daskalakis, Z.J., 2006b. A comprehensive reviewof the effects of rTMS on motor cortical excitability and inhibition. Clin.Neurophysiol. 117, 2584–2596.
Fitzgerald, P.B., Maller, J.J., Hoy, K.E., Thomson, R.H., 2009. Exploring theoptimal site for the localization of dorsolateral prefrontal cortex in brainstimulation experiments. Brain Stimul. 2, 234–237.
Gratton, E., Fantini, S., Franceschini, M.A., Gratton, G., Fabiani, M., 1997.Measurements of scattering and absorption changes inmuscle and brain.Philos. Trans. R. Soc. Lond. B Biol. Sci. 352, 727–735.
Hanaoka, N., Aoyama, Y., Kameyama, M., Fukuda, M., Mikuni, M., 2007.Deactivation and activation of left frontal lobe during and after low-frequency repetitive transcranial magnetic stimulation over right prefron-tal cortex: a near-infrared spectroscopy study. Neurosci. Lett. 414, 99–104.
Kozel, F.A., Tian, F., Dhamne, S., Croarkin, P.E.,McClintock, S.M., Elliott, A.,Mapes,K.S., Husain, M.M., Liu, H., 2009. Using simultaneous repetitive TranscranialMagnetic Stimulation/functional Near Infrared Spectroscopy (rTMS/fNIRS)to measure brain activation and connectivity. Neuroimage 47, 1177–1184.
Loo, C.K., Sachdev, P.S., Haindl, W., Wen, W., Mitchell, P.B., Croker, V.M.,Malhi, G.S., 2003. High (15 Hz) and low (1 Hz) frequency transcranialmagnetic stimulation have different acute effects on regional cerebralblood flow in depressed patients. Psychol. Med. 33, 997–1006.
Matsuda, G., Hiraki, K., 2006. Sustained decrease in oxygenated hemoglobinduring video games in the dorsal prefrontal cortex: a NIRS study ofchildren. Neuroimage 29, 706–711.
Mochizuki, H., Ugawa, Y., Terao, Y., Sakai, K.L., 2006. Cortical hemoglobin-concentration changes under the coil induced by single-pulse TMS inhumans: a simultaneous recordingwith near-infrared spectroscopy. Exp.Brain Res. 169, 302–310.
O'Reardon, J.P., Solvason, H.B., Janicak, P.G., Sampson, S., Isenberg, K.E., Nahas,Z., McDonald, W.M., Avery, D., Fitzgerald, P.B., Loo, C., Demitrack, M.A.,George, M.S., Sackeim, H.A., 2007. Efficacy and safety of transcranialmagnetic stimulation in the acute treatment of major depression: amultisite randomized controlled trial. Biol. Psychiatry 62, 1208–1216.
Romero, J.R., Anschel, D., Sparing, R., Gangitano, M., Pascual-Leone, A., 2002.Subthreshold low frequency repetitive transcranial magnetic stimulationselectively decreases facilitation in the motor cortex. Clin. Neurophysiol.113, 101–107.
Thomson, R.H., Daskalakis, Z.J., Fitzgerald, P.B., 2011a. A near infra-redspectroscopy study of the effects of pre-frontal single and paired pulsetranscranial magnetic stimulation. Clin. Neurophysiol. 122, 378–382.
Thomson, R.H., Maller, J.J., Daskalakis, Z.J., Fitzgerald, P.B., 2011b. Bloodoxygenation changes resulting from suprathreshold transcranial magneticstimulation. Brain Stimul. 4, 165–168.
Toronov, V., Webb, A., Choi, J.H., Wolf, M., Michalos, A., Gratton, E., Hueber, D.,2001. Investigation of human brain hemodynamics by simultaneousnear-infrared spectroscopy and functional magnetic resonance imaging.Med. Phys. 28, 521–527.
Vernieri, F., Maggio, P., Tibuzzi, F., Filippi, M.M., Pasqualetti, P., Melgari, J.M.,Altamura, C., Palazzo, P., Di Giorgio, M., Rossini, P.M., 2009. High frequencyrepetitive transcranial magnetic stimulation decreases cerebral vasomotorreactivity. Clin. Neurophysiol. 120, 1188–1194.