inquadramento clinico e management del...
TRANSCRIPT
1/24/2015
1
Inquadramento clinico e management del NeuroLES
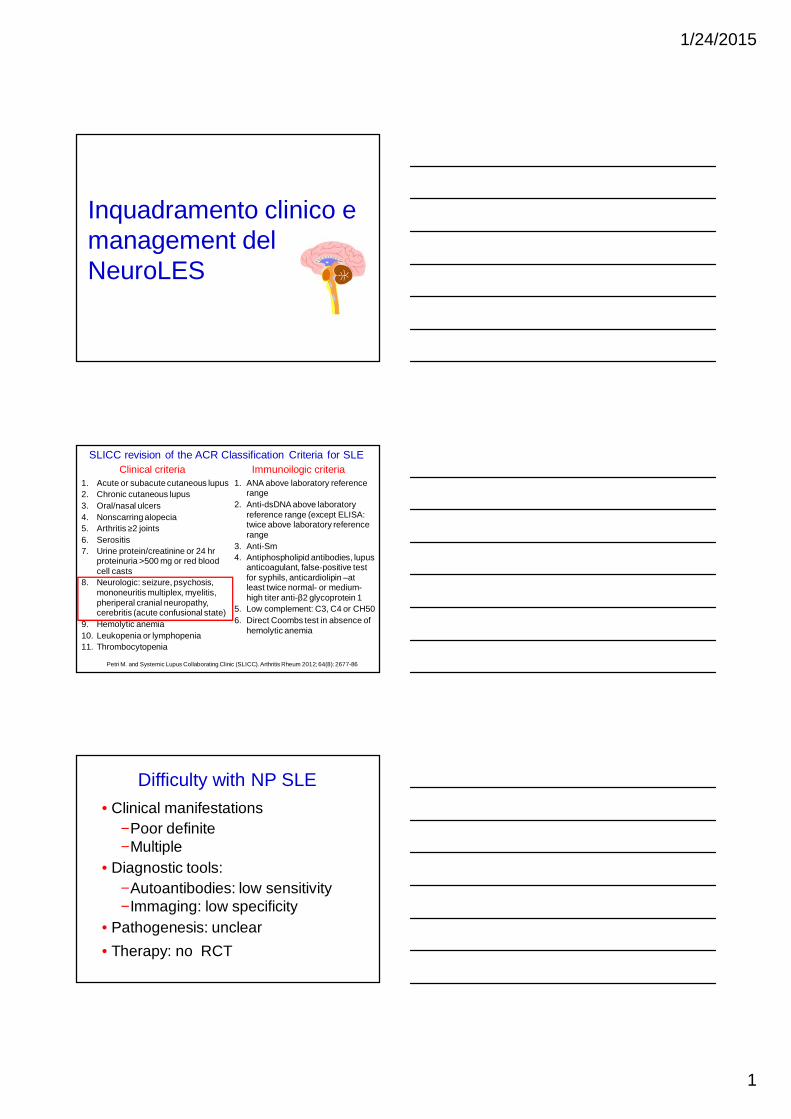
1. Acute or subacute cutaneous lupus2. Chronic cutaneous lupus3. Oral/nasal ulcers4. Nonscarring alopecia5. Arthritis ≥2 joints6. Serositis7. Urine protein/creatinine or 24 hr
proteinuria >500 mg or red blood cell casts
8. Neurologic: seizure, psychosis, mononeuritis multiplex, myelitis, pheriperal cranial neuropathy, cerebritis (acute confusional state)
9. Hemolytic anemia10. Leukopenia or lymphopenia11. Thrombocytopenia
SLICC revision of the ACR Classification Criteria for SLE
1. ANA above laboratory reference range
2. Anti-dsDNA above laboratory reference range (except ELISA: twice above laboratory reference range
3. Anti-Sm4. Antiphospholipid antibodies, lupus
anticoagulant, false-positive test for syphils, anticardiolipin –at least twice normal- or medium-high titer anti-β2 glycoprotein 1
5. Low complement: C3, C4 or CH506. Direct Coombs test in absence of
hemolytic anemia
Clinical criteria Immunoilogic criteria
Petri M. and Systemic Lupus Collaborating Clinic (SLICC). Arthritis Rheum 2012; 64(8): 2677-86
Difficulty with NP SLE
• Clinical manifestations−Poor definite−Multiple
• Diagnostic tools:−Autoantibodies: low sensitivity−Immaging: low specificity
• Pathogenesis: unclear
• Therapy: no RCT
1/24/2015
2
Major points which should be considered in a patient with neuropsychiatric SLE
• Accurate diagnosis
• Identification of the underling pathogenesis
• Management of NPSLE
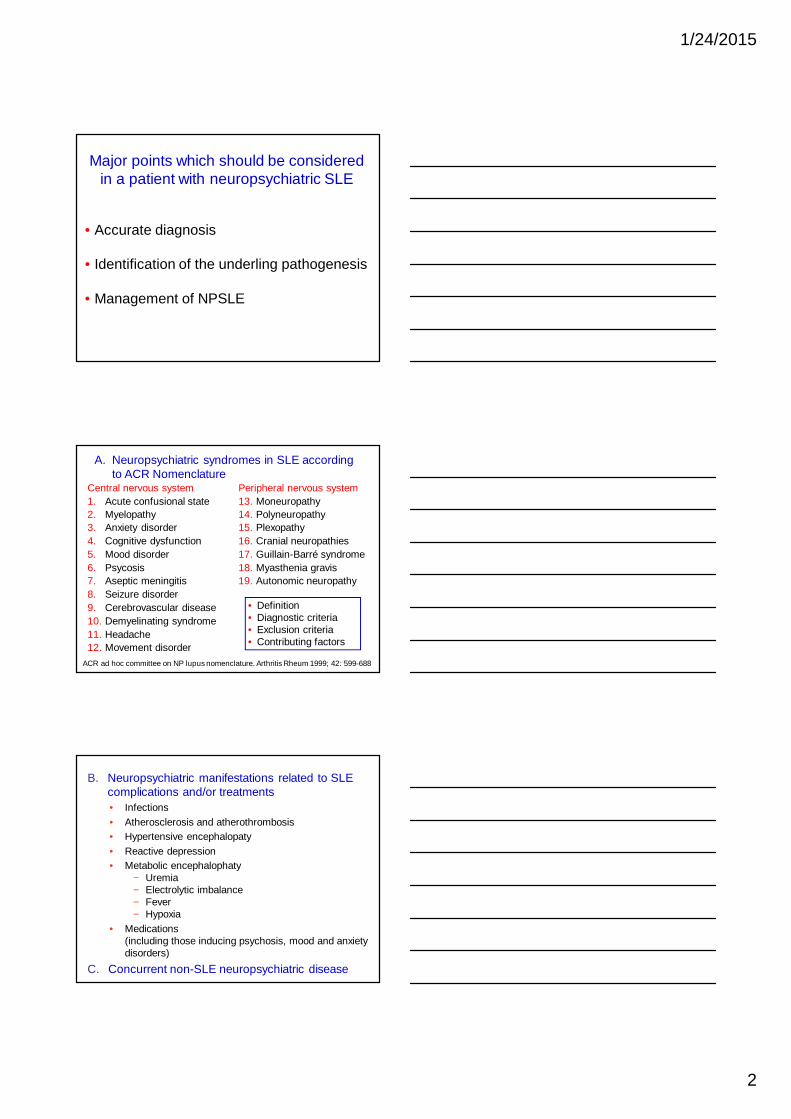
A. Neuropsychiatric syndromes in SLE according to ACR Nomenclature
Central nervous system1. Acute confusional state2. Myelopathy3. Anxiety disorder4. Cognitive dysfunction5. Mood disorder6. Psycosis7. Aseptic meningitis8. Seizure disorder9. Cerebrovascular disease10. Demyelinating syndrome11. Headache12. Movement disorder
Peripheral nervous system13. Moneuropathy14. Polyneuropathy15. Plexopathy16. Cranial neuropathies17. Guillain-Barré syndrome18. Myasthenia gravis19. Autonomic neuropathy
ACR ad hoc committee on NP lupus nomenclature. Arthritis Rheum 1999; 42: 599-688
• Definition• Diagnostic criteria• Exclusion criteria• Contributing factors
B. Neuropsychiatric manifestations related to SLE complications and/or treatments• Infections• Atherosclerosis and atherothrombosis• Hypertensive encephalopaty• Reactive depression• Metabolic encephalophaty
− Uremia− Electrolytic imbalance− Fever− Hypoxia
• Medications(including those inducing psychosis, mood and anxiety disorders)
C. Concurrent non-SLE neuropsychiatric disease
1/24/2015
3
Marcello Govoni, Stefano Bombardieri, Alessandra Bortoluzzi, Luisa Caniatti, Cinzia Casu, Fabrizio Conti, Salvatore De Vita, Andrea Doria, Ilaria Farina, Gianfranco Ferraccioli, Elisa Gremese, Elisa Mansutti, Marta Mosca, Melissa Padovan, Matteo Piga, Angela Tincani, Maria Rosaria Tola, Paola Tomietto, Marco Taglietti, Francesco Trotta, Guido Valesini, Margherita Zen and Alessandro Mathieu on behalf of the Italian Society of Rheumatology
Rheumatology 2012;51:157168
Frequency of individual NP events in 469 SLE patients with NP manifestations
Govoni M, et al. Rheumatology 2012;51:157168
30.5%
1. Exclusion and association factors reported in the ACR nomenclature and case definitions for NPSLE were referred to as non-SLE factors
2. Time at onset: events occurring before (>6 months) the onset of SLE were considered to be not attributable to SLE
3. The occurrence of a minor NP event, as defined by Ainiala et al (A&R 2001), scored against the attribution to SLE
4. The presence of other information [e.g. neuroimaging, cerebrospinal fluid (CSF) analysis, response to treatment] scored in favor of the attribution to SLE
The attribution of each NP event to SLE was based on four items suggested by the SLICC group (Hanly, et al A&R 2007):
Score: 0 = unrelated; 1 = low; 2 = moderate; 3 = high probability to be disease-related
Major points which should be considered in a patient with neuropsychiatric SLE
• Accurate diagnosis
• Identification of the underling pathogenesis
• Management of NPSLE
1/24/2015
4
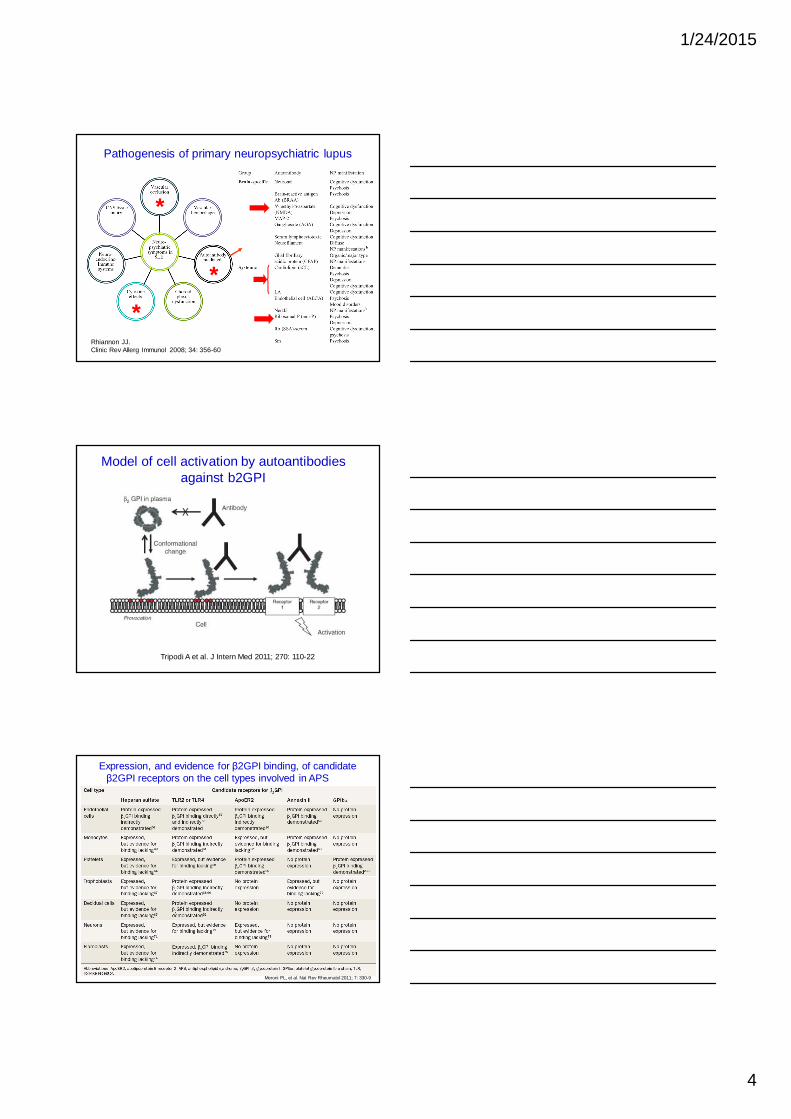
Pathogenesis of primary neuropsychiatric lupus
Rhiannon JJ. Clinic Rev Allerg Immunol 2008; 34: 356-60
*
*
*
Model of cell activation by autoantibodies against b2GPI
Tripodi A et al. J Intern Med 2011; 270: 110-22
Expression, and evidence for β2GPI binding, of candidate β2GPI receptors on the cell types involved in APS
Meroni PL, et al. Nat Rev Rheumatol 2011; 7: 330-9
1/24/2015
5
13
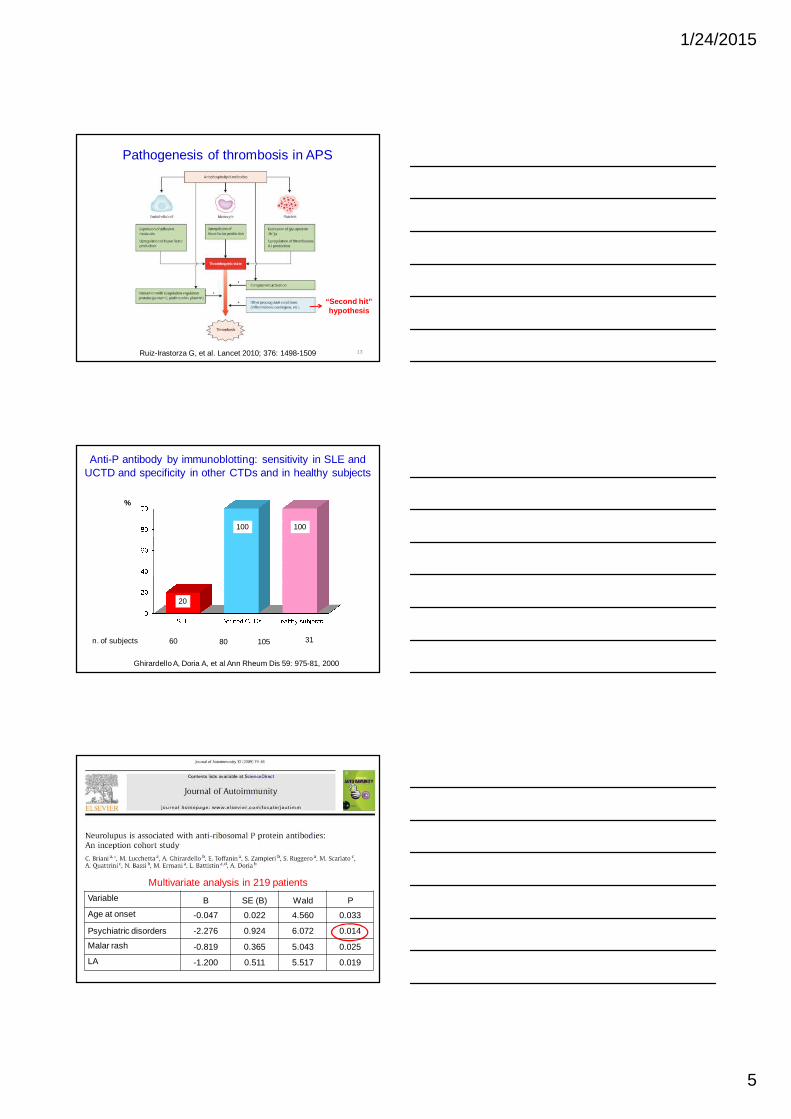
Pathogenesis of thrombosis in APS
Ruiz-Irastorza G, et al. Lancet 2010; 376: 1498-1509
“Second hit” hypothesis
20
100
Anti-P antibody by immunoblotting: sensitivity in SLE and UCTD and specificity in other CTDs and in healthy subjects
n. of subjects 60 80 105 31
Ghirardello A, Doria A, et al Ann Rheum Dis 59: 975-81, 2000
100
%
Variable B SE (B) Wald P
Age at onset -0.047 0.022 4.560 0.033
Psychiatric disorders -2.276 0.924 6.072 0.014
Malar rash -0.819 0.365 5.043 0.025
LA -1.200 0.511 5.517 0.019
Multivariate analysis in 219 patients
1/24/2015
6
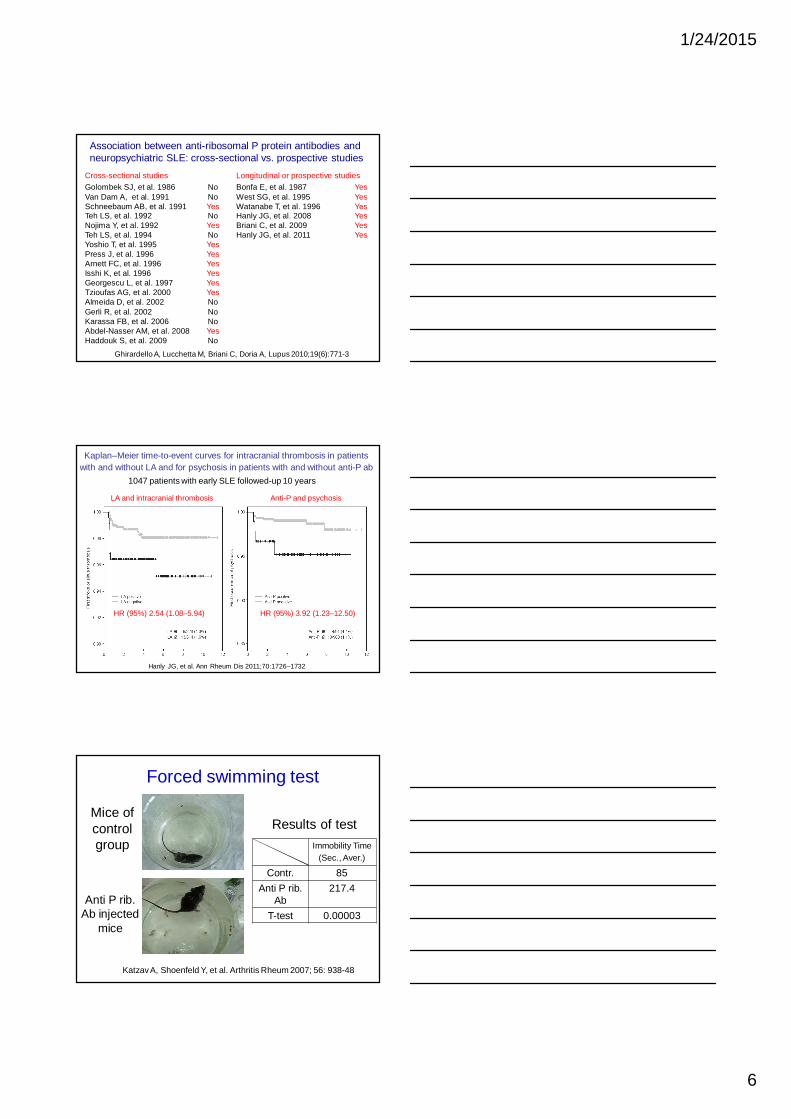
Cross-sectional studiesGolombek SJ, et al. 1986 NoVan Dam A, et al. 1991 NoSchneebaum AB, et al. 1991 YesTeh LS, et al. 1992 NoNojima Y, et al. 1992 YesTeh LS, et al. 1994 NoYoshio T, et al. 1995 YesPress J, et al. 1996 YesArnett FC, et al. 1996 YesIsshi K, et al. 1996 YesGeorgescu L, et al. 1997 YesTzioufas AG, et al. 2000 YesAlmeida D, et al. 2002 NoGerli R, et al. 2002 NoKarassa FB, et al. 2006 NoAbdel-Nasser AM, et al. 2008 YesHaddouk S, et al. 2009 No
Longitudinal or prospective studiesBonfa E, et al. 1987 YesWest SG, et al. 1995 YesWatanabe T, et al. 1996 YesHanly JG, et al. 2008 YesBriani C, et al. 2009 YesHanly JG, et al. 2011 Yes
Association between anti-ribosomal P protein antibodies and neuropsychiatric SLE: cross-sectional vs. prospective studies
Ghirardello A, Lucchetta M, Briani C, Doria A, Lupus 2010;19(6):771-3
Kaplan–Meier time-to-event curves for intracranial thrombosis in patients with and without LA and for psychosis in patients with and without anti-P ab
Hanly JG, et al. Ann Rheum Dis 2011;70:1726–1732
LA and intracranial thrombosis Anti-P and psychosis
HR (95%) 3.92 (1.23–12.50)HR (95%) 2.54 (1.08–5.94)
1047 patients with early SLE followed-up 10 years
Forced swimming test
Immobility Time (Sec., Aver.)
85Contr.
217.4Anti P rib. Ab
0.00003T-test
Results of testMice of control group
Anti P rib. Ab injected
mice
Katzav A, Shoenfeld Y, et al. Arthritis Rheum 2007; 56: 938-48
1/24/2015
7
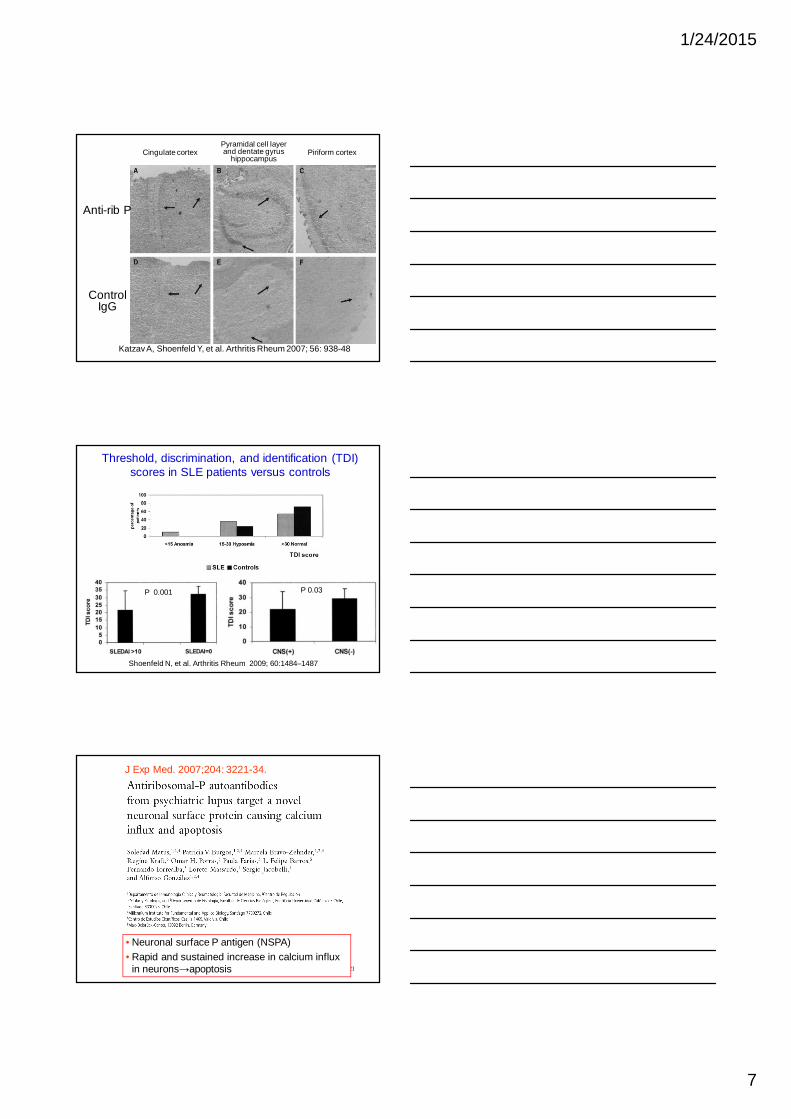
19Katzav A, Shoenfeld Y, et al. Arthritis Rheum 2007; 56: 938-48
Cingulate cortexPyramidal cell layer and dentate gyrus
hippocampusPiriform cortex
Anti-rib P
Control IgG
Threshold, discrimination, and identification (TDI) scores in SLE patients versus controls
Shoenfeld N, et al. Arthritis Rheum 2009; 60:1484–1487
P 0.001 P 0.03
21
J Exp Med. 2007;204: 3221-34.
• Neuronal surface P antigen (NSPA)• Rapid and sustained increase in calcium influx
in neurons→apoptosis
1/24/2015
8
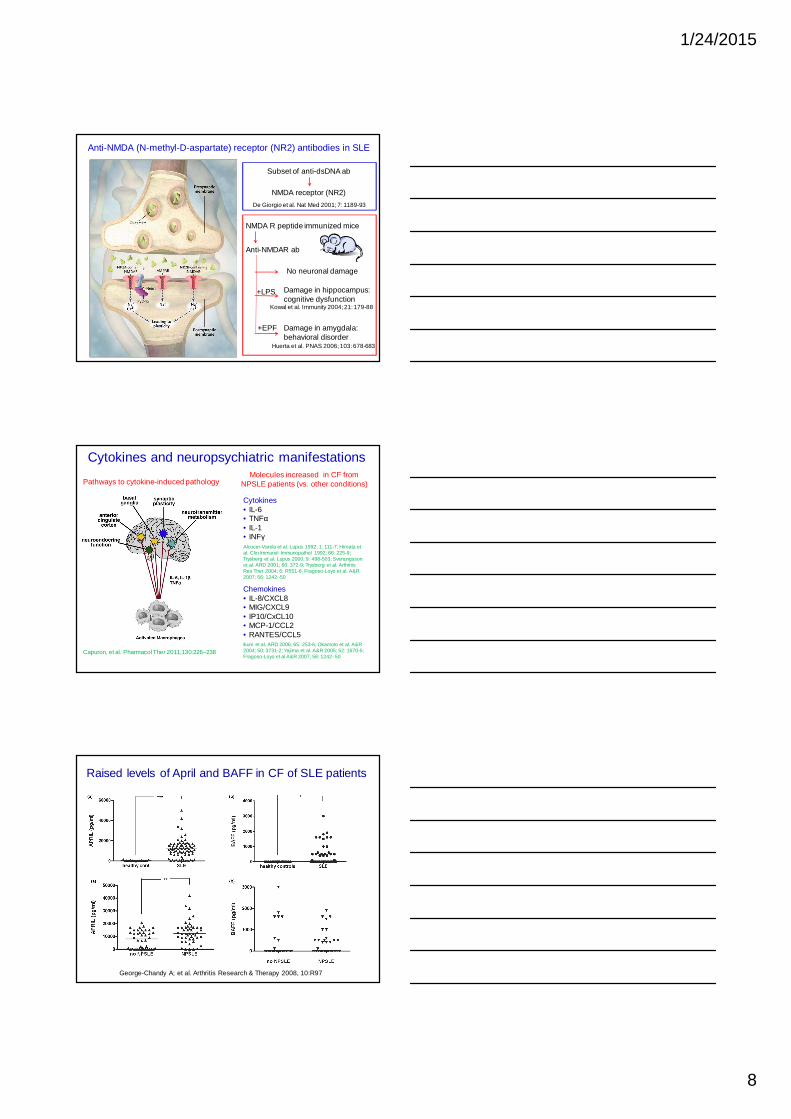
Anti-NMDA (N-methyl-D-aspartate) receptor (NR2) antibodies in SLE
Subset of anti-dsDNA ab
NMDA receptor (NR2)
De Giorgio et al. Nat Med 2001; 7: 1189-93
NMDA R peptide immunized mice
Anti-NMDAR ab
No neuronal damage
Damage in hippocampus: cognitive dysfunction
+LPS
Damage in amygdala: behavioral disorder
+EPF
Kowal et al. Immunity 2004; 21: 179-88
Huerta et al. PNAS 2006; 103: 678-683
Cytokines and neuropsychiatric manifestations
Pathways to cytokine-induced pathology
Capuron, et al. Pharmacol Ther 2011;130:226–238
Molecules increased in CF from NPSLE patients (vs. other conditions)
Cytokines• IL-6• TNFα• IL-1• INFγAlcocer-Varela et al. Lupus 1992; 1: 111-7; Hiroata etal. Clin Immunol Immunopathol 1992; 66: 225-9; Trysberg et al. Lupus 2000; 9: 498-503; Svenungssonet al. ARD 2001; 60: 372-9; Trysberg et al. ArthritisRes Ther 2004; 6: R551-6; Fragoso-Loyo et al. A&R2007; 56: 1242–50
Chemokines• IL-8/CXCL8• MIG/CXCL9• IP10/CxCL10• MCP-1/CCL2• RANTES/CCL5Ikuni et al. ARD 2006; 65: 253-6; Okamoto et al. A&R2004; 50: 3731-2; Yajima et al. A&R 2005; 52: 1670-5; Fragoso-Loyo et al A&R 2007; 56: 1242–50
George-Chandy A; et al. Arthritis Research & Therapy 2008, 10:R97
Raised levels of April and BAFF in CF of SLE patients
1/24/2015
9
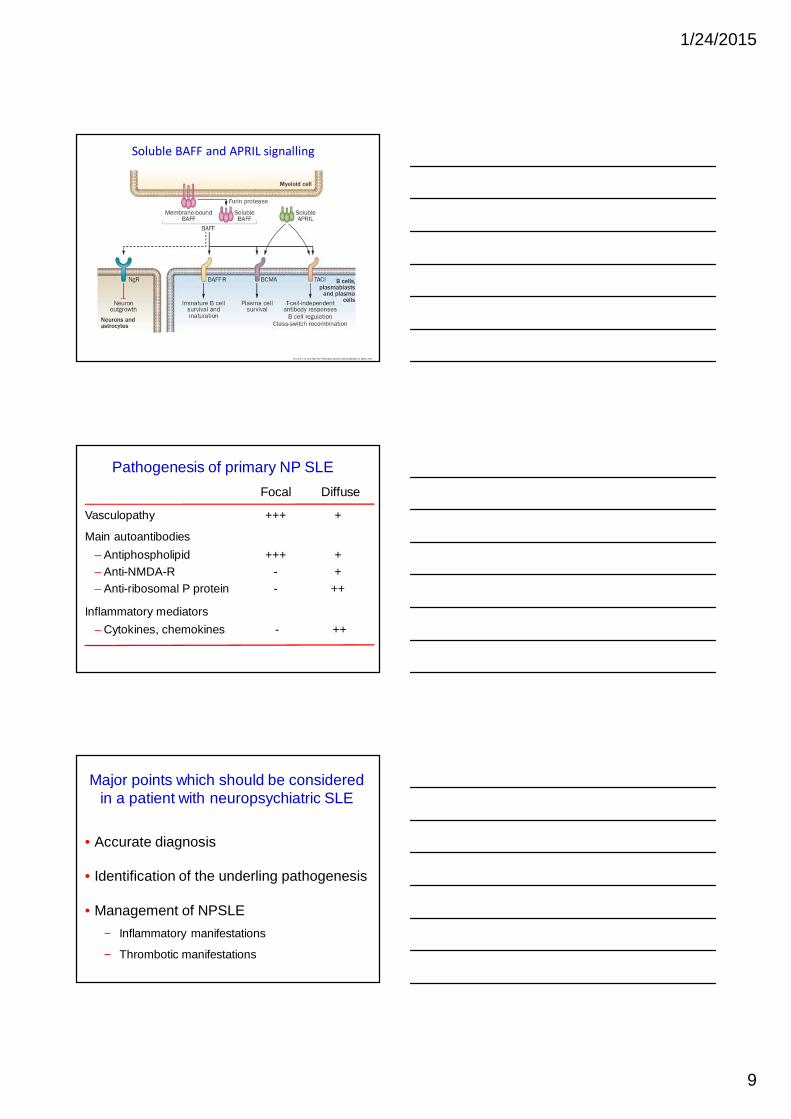
Vincent, F. B. et al. Nat. Rev. Rheumatol. advance online publication 11 March 2014
Soluble BAFF and APRIL signalling
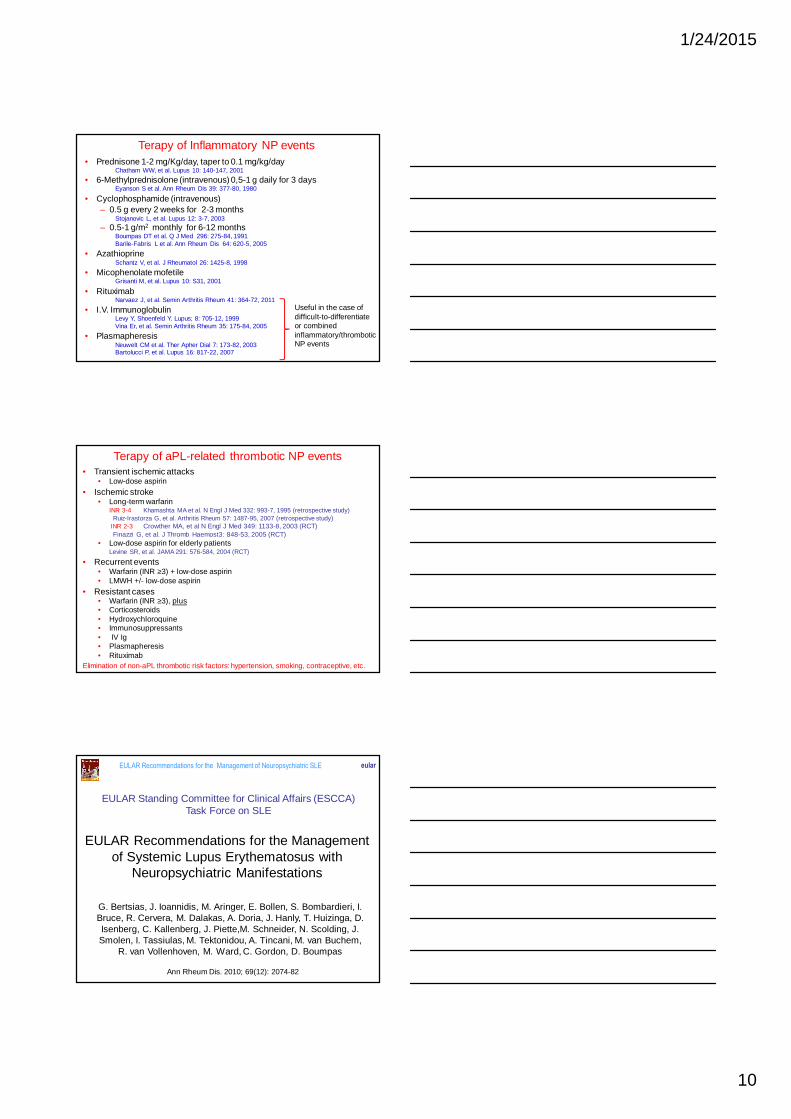
Pathogenesis of primary NP SLE
Vasculopathy +++ +
Main autoantibodies
– Antiphospholipid +++ +– Anti-NMDA-R - +– Anti-ribosomal P protein - ++
Inflammatory mediators
– Cytokines, chemokines - ++
Focal Diffuse
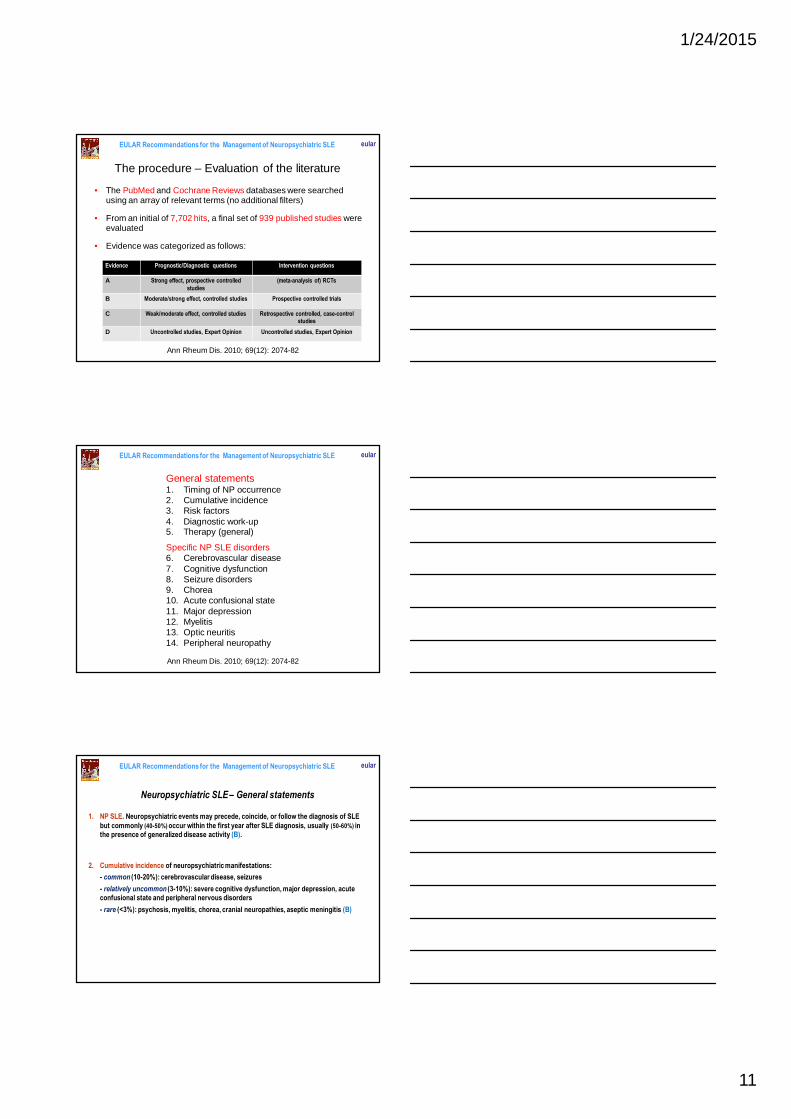
Major points which should be considered in a patient with neuropsychiatric SLE
• Accurate diagnosis
• Identification of the underling pathogenesis
• Management of NPSLE
− Inflammatory manifestations
− Thrombotic manifestations
1/24/2015
10
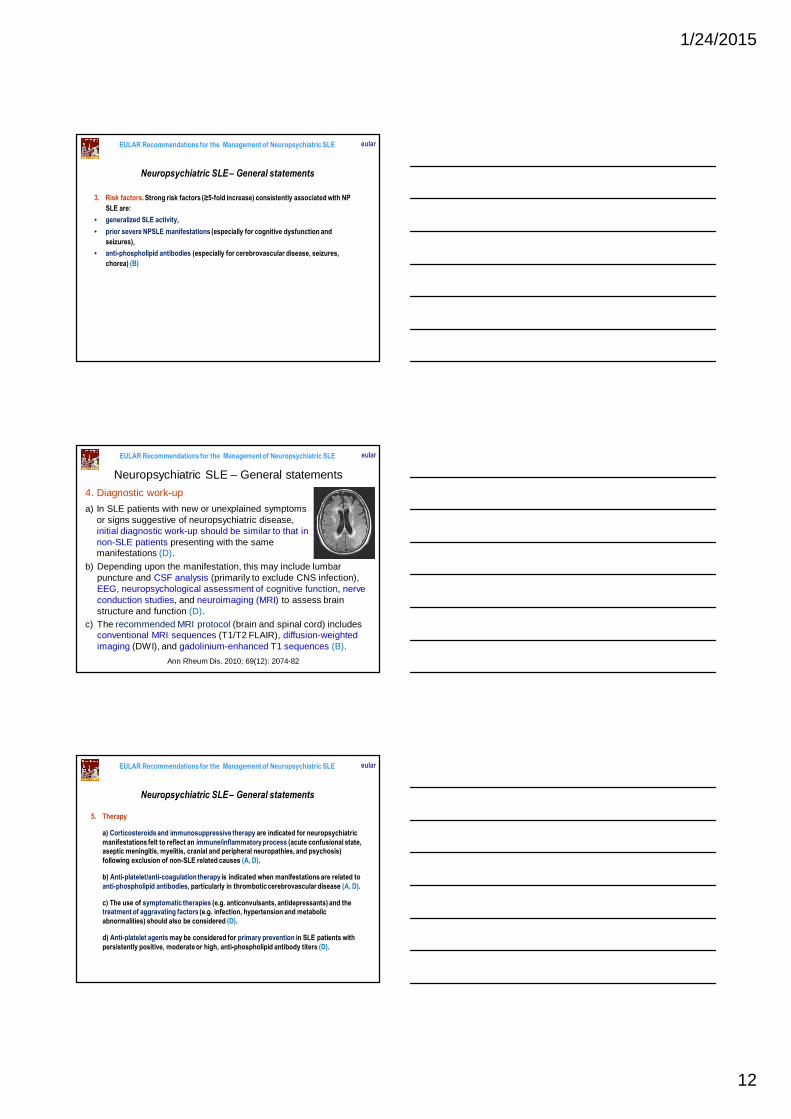
Terapy of Inflammatory NP events• Prednisone 1-2 mg/Kg/day, taper to 0.1 mg/kg/day
Chatham WW, et al. Lupus 10: 140-147, 2001
• 6-Methylprednisolone (intravenous) 0,5-1 g daily for 3 daysEyanson S et al. Ann Rheum Dis 39: 377-80, 1980
• Cyclophosphamide (intravenous) – 0.5 g every 2 weeks for 2-3 months
Stojanovic L, et al. Lupus 12: 3-7, 2003
– 0.5-1 g/m2 monthly for 6-12 monthsBoumpas DT et al. Q J Med 296: 275-84, 1991 Barile-Fabris L et al. Ann Rheum Dis 64: 620-5, 2005
• AzathioprineSchantz V, et al. J Rheumatol 26: 1425-8, 1998
• Micophenolate mofetileGrisanti M, et al. Lupus 10: S31, 2001
• RituximabNarvaez J, et al. Semin Arthritis Rheum 41: 364-72, 2011
• I.V. ImmunoglobulinLevy Y, Shoenfeld Y. Lupus; 8: 705-12, 1999Vina Er, et al. Semin Arthritis Rheum 35: 175-84, 2005
• PlasmapheresisNeuwelt CM et al. Ther Apher Dial 7: 173-82, 2003Bartolucci P, et al. Lupus 16: 817-22, 2007
Useful in the case of difficult-to-differentiate or combined inflammatory/thrombotic NP events
Terapy of aPL-related thrombotic NP events• Transient ischemic attacks
• Low-dose aspirin
• Ischemic stroke• Long-term warfarin
INR 3-4 Khamashta MA et al. N Engl J Med 332: 993-7, 1995 (retrospective study)Ruiz-Irastorza G, et al. Arthritis Rheum 57: 1487-95, 2007 (retrospective study)
INR 2-3 Crowther MA, et al N Engl J Med 349: 1133-8, 2003 (RCT)Finazzi G, et al. J Thromb Haemost3: 848-53, 2005 (RCT)
• Low-dose aspirin for elderly patientsLevine SR, et al. JAMA 291: 576-584, 2004 (RCT)
• Recurrent events• Warfarin (INR ≥3) + low-dose aspirin • LMWH +/- low-dose aspirin
• Resistant cases• Warfarin (INR ≥3), plus• Corticosteroids• Hydroxychloroquine • Immunosuppressants• IV Ig• Plasmapheresis• Rituximab
Elimination of non-aPL thrombotic risk factors: hypertension, smoking, contraceptive, etc.
EULAR Recommendations for the Management of Systemic Lupus Erythematosus with
Neuropsychiatric Manifestations
EULAR Standing Committee for Clinical Affairs (ESCCA)Task Force on SLE
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
G. Bertsias, J. Ioannidis, M. Aringer, E. Bollen, S. Bombardieri, I. Bruce, R. Cervera, M. Dalakas, A. Doria, J. Hanly, T. Huizinga, D. Isenberg, C. Kallenberg, J. Piette,M. Schneider, N. Scolding, J. Smolen, I. Tassiulas, M. Tektonidou, A. Tincani, M. van Buchem,
R. van Vollenhoven, M. Ward, C. Gordon, D. Boumpas
Ann Rheum Dis. 2010; 69(12): 2074-82
1/24/2015
11
The procedure – Evaluation of the literature
• The PubMed and Cochrane Reviews databases were searched using an array of relevant terms (no additional filters)
• From an initial of 7,702 hits, a final set of 939 published studies were evaluated
• Evidence was categorized as follows:
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Evidence Prognostic/Diagnostic questions Intervention questions
A Strong effect, prospective controlled
studies
(meta-analysis of) RCTs
B Moderate/strong effect, controlled studies Prospective controlled trials
C Weak/moderate effect, controlled studies Retrospective controlled, case-control studies
D Uncontrolled studies, Expert Opinion Uncontrolled studies, Expert Opinion
Ann Rheum Dis. 2010; 69(12): 2074-82
General statements1. Timing of NP occurrence2. Cumulative incidence3. Risk factors4. Diagnostic work-up5. Therapy (general)
Specific NP SLE disorders6. Cerebrovascular disease7. Cognitive dysfunction8. Seizure disorders9. Chorea10. Acute confusional state11. Major depression12. Myelitis13. Optic neuritis14. Peripheral neuropathy
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Ann Rheum Dis. 2010; 69(12): 2074-82
Neuropsychiatric SLE – General statements
1. NP SLE. Neuropsychiatric events may precede, coincide, or follow the diagnosis of SLE
but commonly (40-50%) occur within the first year after SLE diagnosis, usually (50-60%) in the presence of generalized disease activity (B).
2. Cumulative incidence of neuropsychiatric manifestations:
- common (10-20%): cerebrovascular disease, seizures
- relatively uncommon (3-10%): severe cognitive dysfunction, major depression, acute confusional state and peripheral nervous disorders
- rare (<3%): psychosis, myelitis, chorea, cranial neuropathies, aseptic meningitis (B)
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
1/24/2015
12
3. Risk factors. Strong risk factors (≥5-fold increase) consistently associated with NP
SLE are:
• generalized SLE activity,
• prior severe NPSLE manifestations (especially for cognitive dysfunction and
seizures),
• anti-phospholipid antibodies (especially for cerebrovascular disease, seizures,
chorea) (B)
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – General statements
4. Diagnostic work-up
a) In SLE patients with new or unexplained symptoms or signs suggestive of neuropsychiatric disease, initial diagnostic work-up should be similar to that in non-SLE patients presenting with the same manifestations (D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – General statements
b) Depending upon the manifestation, this may include lumbar puncture and CSF analysis (primarily to exclude CNS infection), EEG, neuropsychological assessment of cognitive function, nerve conduction studies, and neuroimaging (MRI) to assess brain structure and function (D).
c) The recommended MRI protocol (brain and spinal cord) includes conventional MRI sequences (T1/T2 FLAIR), diffusion-weighted imaging (DWI), and gadolinium-enhanced T1 sequences (B).
Ann Rheum Dis. 2010; 69(12): 2074-82
5. Therapy
a) Corticosteroids and immunosuppressive therapy are indicated for neuropsychiatric
manifestations felt to reflect an immune/inflammatory process (acute confusional state, aseptic meningitis, myelitis, cranial and peripheral neuropathies, and psychosis)
following exclusion of non-SLE related causes (A, D).
b) Anti-platelet/anti-coagulation therapy is indicated when manifestations are related to
anti-phospholipid antibodies, particularly in thrombotic cerebrovascular disease (A, D).
c) The use of symptomatic therapies (e.g. anticonvulsants, antidepressants) and the treatment of aggravating factors (e.g. infection, hypertension and metabolic
abnormalities) should also be considered (D).
d) Anti-platelet agents may be considered for primary prevention in SLE patients with
persistently positive, moderate or high, anti-phospholipid antibody titers (D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – General statements
1/24/2015
13
5. Therapy (general)
Common (10-30%)• Cerebrovascular disease• SeizuresRelatively uncommon (3-10%)• Severe cognitive dysfunction• Major depression• Acute confusional state• Peripheral nervous system
disordersRare (<3%)• Psycosis• Myelitis• Chorea• Cranial neuropathies• Aseptic meningitis
Corticosteroids and/or immunosuppressants
Antiplatelet/anticoagulation therapy
Symptomatic treatment
+ Corticosteroids and/or immunosuppressants in presence of generalized disease activity+ Antiplatelet/anticoagulation therapy in patients with aPL
EULAR Recommendations for the Management of Neuropsychiatric SLE
Ann Rheum Dis. 2010; 69(12): 2074-82
6. Cerebrovascular disease.
a) Atherosclerotic/thrombotic/embolic cerebrovascular disease
is common, hemorrhagic stroke is rare, and stroke caused by
vasculitis is very rare in SLE patients; accordingly,
immunosuppressive therapy is rarely indicated (B, D).
b) Long-term anticoagulation should be strongly considered in
patients with stroke fulfilling the classification criteria for
antiphospholipid syndrome for secondary prevention of
recurrent stroke which commonly (30-40%) occurs (D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – Cerebrovascular disease
7. Cognitive dysfunction
a) Mild or moderate cognitive dysfunction is common in SLE
but severe cognitive impairment resulting in functional
compromise is relatively uncommon and should be confirmed
by neuropsychological tests in collaboration with a clinical
neuropsychologist where available (B, D).
b) Management of both SLE- and non-SLE-associated factors
as well as psycho-educational support may prevent further
deterioration of cognitive dysfunction; progressive cognitive
decline develops only in a minority of patients (D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – Cognitive dysfunction
1/24/2015
14
8. Seizure disorder
a) Single seizures are common and have been related to disease
activity. Chance of recurrence is comparable to that in the general
population (B).
b) The diagnostic work-up aims to exclude structural brain disease
and inflammatory or metabolic conditions, and includes MRI and
EEG (D).
c) In the absence of MRI lesions related to seizures and definite
epileptic abnormalities on EEG following recovery from the seizure,
withholding of anti-epileptic drugs after a single seizure should be
considered. Long-term anti-epileptic therapy may be considered for
recurrent seizures (D).
d) For most patients without generalized disease activity,
immunosuppressive therapy is not indicated for prevention of
recurrences or control of refractory seizures (D, A).
e) Anti-coagulation may be considered in patients with anti-
phospholipidantibodies (D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – Seizure disorder
9. Movement disorders (Chorea)
a) In addition to symptomatic therapy for persistent symptoms,
anti-platelet agents may be considered in SLE patients with anti-
phospholipid antibodies (D).
b) Corticosteroids/immunosuppressive and/or anti-coagulation
therapy may be considered in severe cases when generalized
disease activity and/or thrombotic manifestations are present
(D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – Chorea
10. Acute confusional state
a) Lumbar puncture for CSF analysis and MRI should be
considered to exclude non-SLE causes, especially infection (D).
b) Corticosteroids and immunosuppressive therapy may be
considered in severe cases (D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – Acute confusion
1/24/2015
15
11. Major depression and psychosis
a) Major depression attributed to SLE alone is relatively
uncommon while psychosis is rare; although steroid-induced
psychosis may occur this is very rare (B).
b) There is no strong evidence to support the diagnostic utility
of serologic markers or brain imaging (D).
c) In the absence of generalized disease activity,
immunosuppressive therapy is not indicated (D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – Psychiatric disease
12. Myelitis
a) The diagnostic work-up includes gadolinium-enhanced MRI
and CSF analysis (B, D).
b) Timely (as soon as possible) induction therapy with high-
dose corticosteroids followed by intravenous
cyclophosphamide should be instituted (A, D).
c) Maintenance therapy with less intensive immunosuppression
to prevent recurrence may be considered (D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – Myelitis
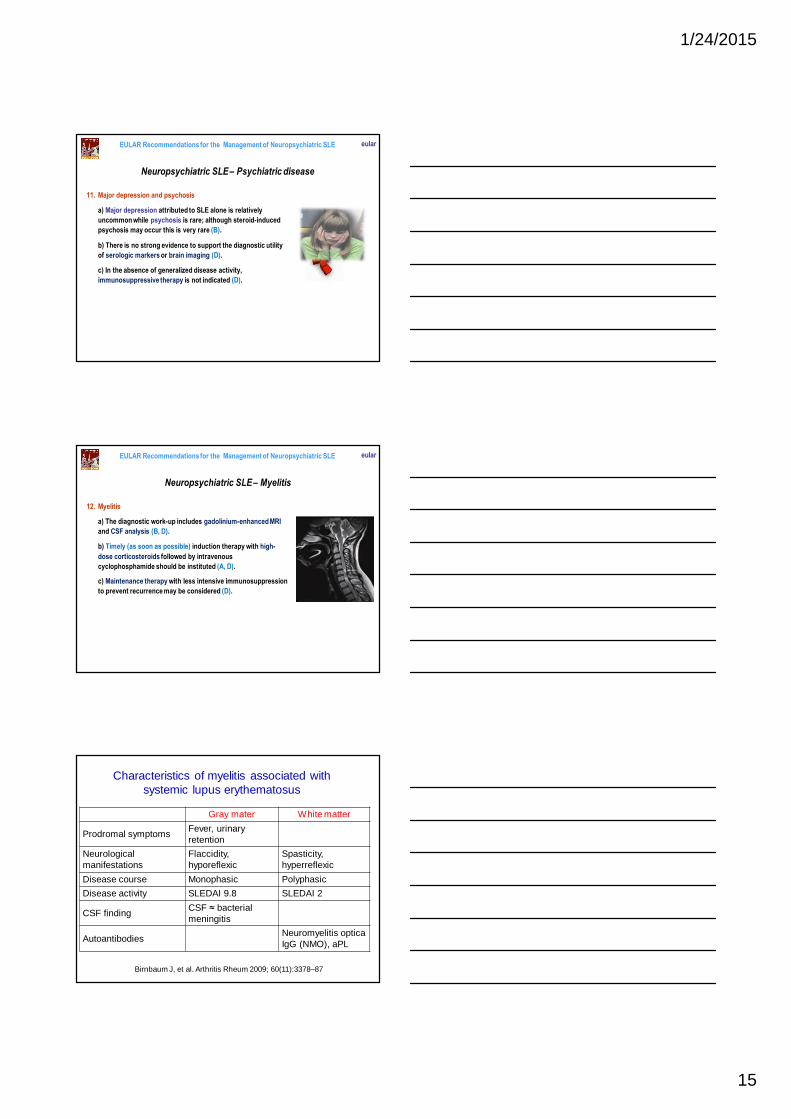
Characteristics of myelitis associated with systemic lupus erythematosus
Birnbaum J, et al. Arthritis Rheum 2009; 60(11):3378–87
Gray mater White matter
Prodromal symptomsFever, urinary retention
Neurological manifestations
Flaccidity,hyporeflexic
Spasticity, hyperreflexic
Disease course Monophasic Polyphasic
Disease activity SLEDAI 9.8 SLEDAI 2
CSF findingCSF ≈ bacterialmeningitis
AutoantibodiesNeuromyelitis opticaIgG (NMO), aPL
1/24/2015
16
13. Optic neuritis is commonly bilateral in SLE.
a) The diagnostic work-up should include ophthalmological
evaluation, MRI, and visual evoked potentials (B, D).
b) Needs to be distinguished from ischaemic optic
neuropathy, which is usually unilateral, especially in patients
with anti-phospholipid antibodies (D).
c) Corticosteroids (intravenous methylprednisolone) alone or
in combination with immunosuppressive agents should be
considered, but failures are common (A, D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – Optic neuritis
14. Peripheral neuropathy
a) It often co-exists with other neuropsychiatric
manifestations and is diagnosed with electromyography
(EMG) and nerve conduction studies (B, D).
b) Combination therapy with corticosteroids and
immunosuppressive agents may be considered in severe
cases (D).
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Neuropsychiatric SLE – Peripheral neuropathy
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
Conclusions
• Recommendations regarding important aspects in diagnosis and management of SLE
patients with neuropsychiatric manifestations have been developed based on
systematic review of the literature and expert opinion
• These recommendations could facilitate medical care in lupus patients without
restricting the autonomy of the physicians providing the care
• Diagnostic and therapeutic algorithms based on the Recommendations
1/24/2015
17
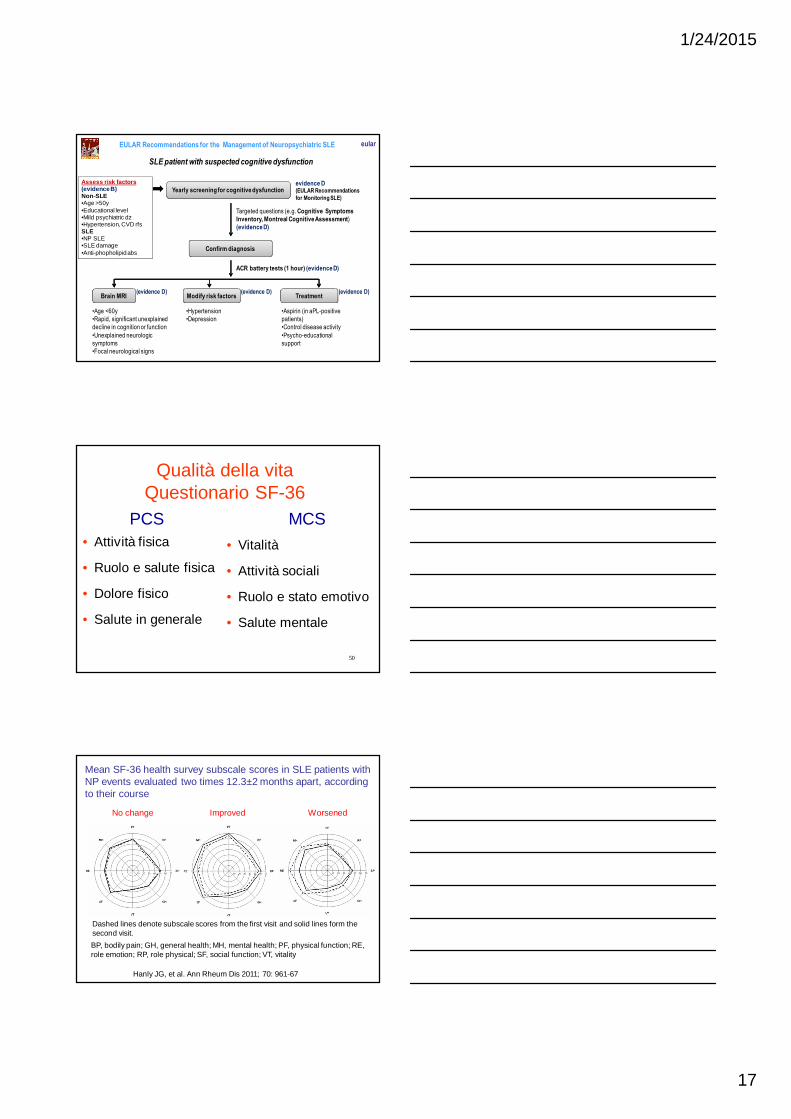
EULAR Recommendations for the Management of Neuropsychiatric SLE eular
SLE patient with suspected cognitive dysfunction
Yearly screening for cognitive dysfunctionevidence D (EULAR Recommendations
for Monitoring SLE)
Assess risk factors (evidence B)Non-SLE•Age >50y•Educational level•Mild psychiatric dz•Hypertension, CVD rfsSLE•NP SLE•SLE damage•Anti-phopholipid abs
Targeted questions (e.g. Cognitive Symptoms
Inventory, Montreal Cognitive Assessment)
(evidence D)
Confirm diagnosis
ACR battery tests (1 hour) (evidence D)
Brain MRI
•Age <60y
•Rapid, significant unexplained
decline in cognition or function
•Unexplained neurologic
symptoms
•Focal neurological signs
Modify risk factors
•Hypertension
•Depression
Treatment
•Aspirin (in aPL-positive
patients)
•Control disease activity
•Psycho-educational
support
(evidence D) (evidence D) (evidence D)
50
Qualità della vita Questionario SF-36
• Attività fisica
• Ruolo e salute fisica
• Dolore fisico
• Salute in generale
• Vitalità
• Attività sociali
• Ruolo e stato emotivo
• Salute mentale
PCS MCS
BP, bodily pain; GH, general health; MH, mental health; PF, physical function; RE, role emotion; RP, role physical; SF, social function; VT, vitality
Mean SF-36 health survey subscale scores in SLE patients with NP events evaluated two times 12.3±2 months apart, according to their course
Dashed lines denote subscale scores from the first visit and solid lines form the second visit.
Hanly JG, et al. Ann Rheum Dis 2011; 70: 961-67
No change Improved Worsened
1/24/2015
18
525252
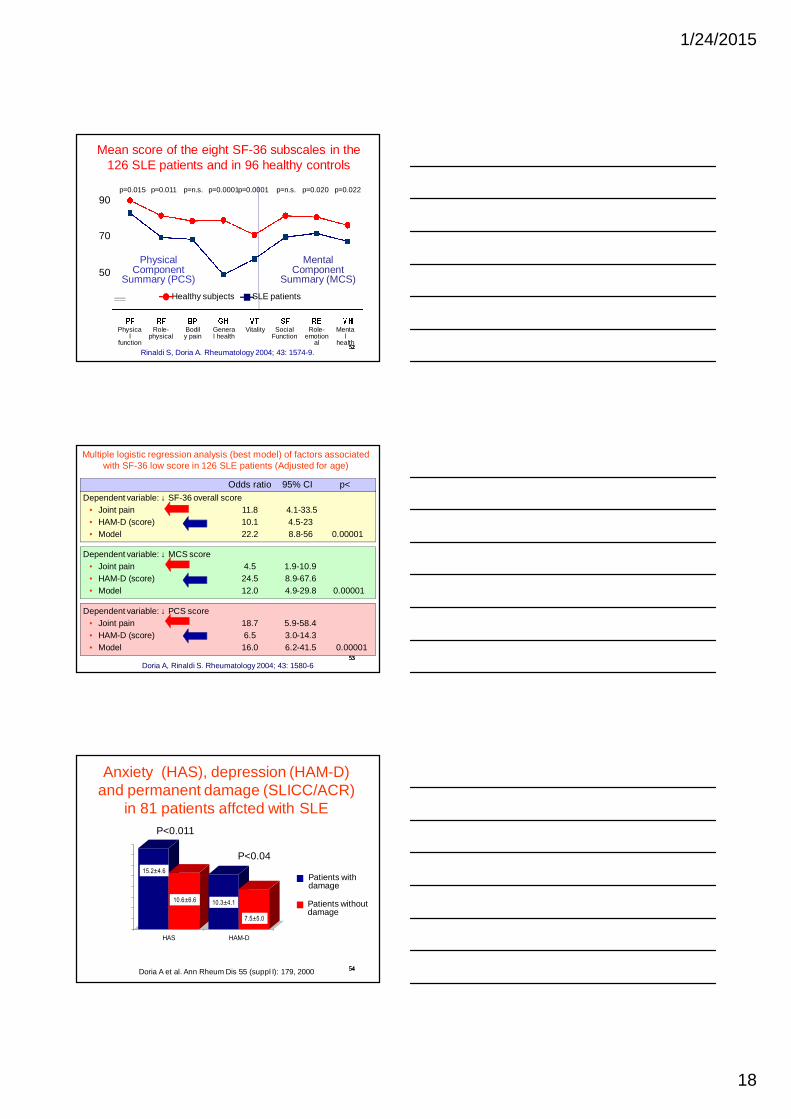
Mean score of the eight SF-36 subscales in the 126 SLE patients and in 96 healthy controls
p=0.015 p=0.011 p=0.0001p=0.0001 p=0.020 p=0.022p=n.s. p=n.s.
Physical
function
Role-physical
General health
Vitality Role-emotion
al
Mental
health
Bodily pain
Social Function
Healthy subjects SLE patients
Rinaldi S, Doria A. Rheumatology 2004; 43: 1574-9.
50
70
90
Mental Component
Summary (MCS)
Physical Component
Summary (PCS)
535353
Multiple logistic regression analysis (best model) of factors associated with SF-36 low score in 126 SLE patients (Adjusted for age)
Dependent variable: ↓ SF-36 overall score• Joint pain 11.8 4.1-33.5• HAM-D (score) 10.1 4.5-23• Model 22.2 8.8-56 0.00001
Dependent variable: ↓ MCS score• Joint pain 4.5 1.9-10.9• HAM-D (score) 24.5 8.9-67.6• Model 12.0 4.9-29.8 0.00001
Odds ratio 95% CI p<
Dependent variable: ↓ PCS score• Joint pain 18.7 5.9-58.4• HAM-D (score) 6.5 3.0-14.3• Model 16.0 6.2-41.5 0.00001
Doria A, Rinaldi S. Rheumatology 2004; 43: 1580-6
545454
Anxiety (HAS), depression (HAM-D) and permanent damage (SLICC/ACR)
in 81 patients affcted with SLE
0
2
4
6
8
10
12
14
16
HAS HAM-D
15.2±4.6
10.6±6.6 10.3±4.1
7.5±5.0
P<0.011
P<0.04
Doria A et al. Ann Rheum Dis 55 (suppl I): 179, 2000
Patients with damage
Patients without damage
1/24/2015
19
555555
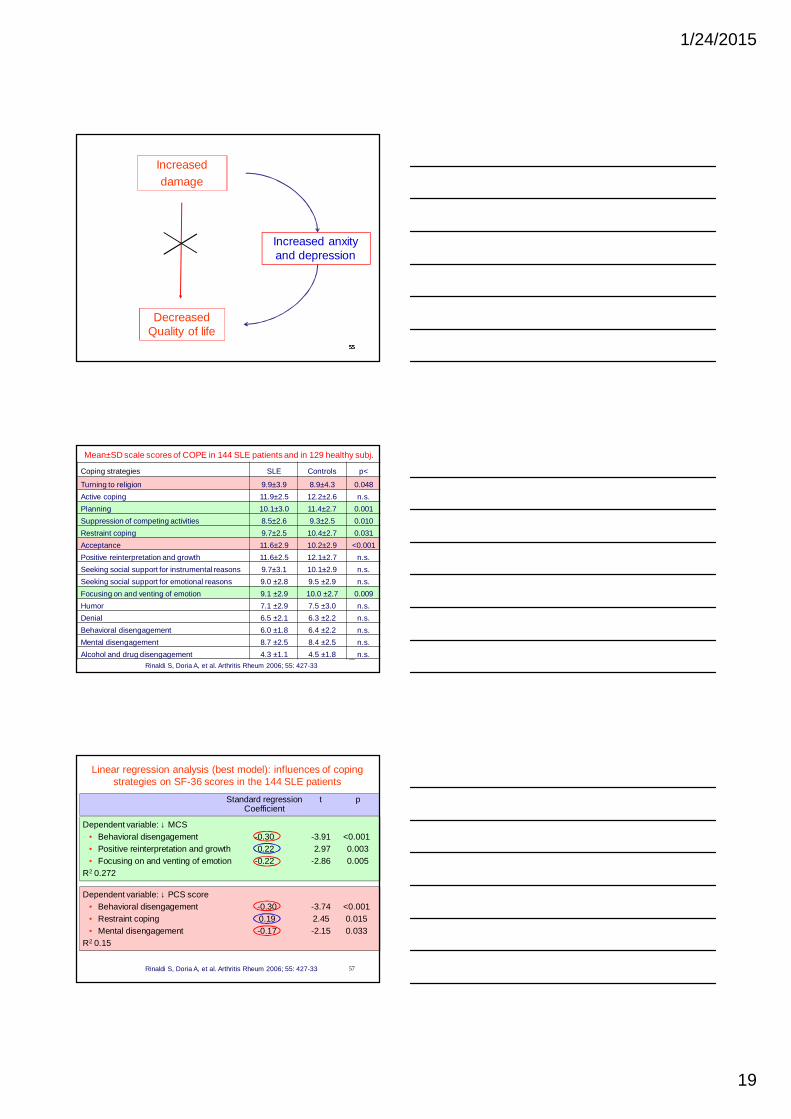
Increaseddamage
Increased anxity and depression
Decreased Quality of life
56
Coping strategies SLE Controls p<
Turning to religion 9.9±3.9 8.9±4.3 0.048
Active coping 11.9±2.5 12.2±2.6 n.s.
Planning 10.1±3.0 11.4±2.7 0.001
Suppression of competing activities 8.5±2.6 9.3±2.5 0.010
Restraint coping 9.7±2.5 10.4±2.7 0.031
Acceptance 11.6±2.9 10.2±2.9 <0.001
Positive reinterpretation and growth 11.6±2.5 12.1±2.7 n.s.
Seeking social support for instrumental reasons 9.7±3.1 10.1±2.9 n.s.
Seeking social support for emotional reasons 9.0 ±2.8 9.5 ±2.9 n.s.
Focusing on and venting of emotion 9.1 ±2.9 10.0 ±2.7 0.009
Humor 7.1 ±2.9 7.5 ±3.0 n.s.
Denial 6.5 ±2.1 6.3 ±2.2 n.s.
Behavioral disengagement 6.0 ±1.8 6.4 ±2.2 n.s.
Mental disengagement 8.7 ±2.5 8.4 ±2.5 n.s.
Alcohol and drug disengagement 4.3 ±1.1 4.5 ±1.8 n.s.
Mean±SD scale scores of COPE in 144 SLE patients and in 129 healthy subj.
Rinaldi S, Doria A, et al. Arthritis Rheum 2006; 55: 427-33
57
Linear regression analysis (best model): influences of coping strategies on SF-36 scores in the 144 SLE patients
Rinaldi S, Doria A, et al. Arthritis Rheum 2006; 55: 427-33
Dependent variable: ↓ MCS• Behavioral disengagement -0.30 -3.91 <0.001• Positive reinterpretation and growth 0.22 2.97 0.003• Focusing on and venting of emotion -0.22 -2.86 0.005
R2 0.272
Standard regression t pCoefficient
Dependent variable: ↓ PCS score• Behavioral disengagement -0.30 -3.74 <0.001• Restraint coping 0.19 2.45 0.015• Mental disengagement -0.17 -2.15 0.033
R2 0.15