injuries to the head and spine
DESCRIPTION
Chapter 29. Injuries to the Head and Spine. Case History. - PowerPoint PPT PresentationTRANSCRIPT

Slide 1Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Injuries to the Head and SpineInjuries to the Head and SpineChapter 29Chapter 29

Slide 2Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Case HistoryCase History
You respond to a 60-year-old man who fell while You respond to a 60-year-old man who fell while riding a motorcycle without a helmet. He has a riding a motorcycle without a helmet. He has a contusion on the left side of his forehead and fluid contusion on the left side of his forehead and fluid leaking from his nose, mouth, and ears. He is leaking from his nose, mouth, and ears. He is verbally combative but cannot move his upper and verbally combative but cannot move his upper and lower extremities.lower extremities.

Slide 3Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Central and Peripheral Central and Peripheral Nervous SystemNervous System

Slide 4Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
BrainBrain

Slide 5Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Layers of the BrainLayers of the Brain

Slide 6Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Blood Supply to the BrainBlood Supply to the Brain

Slide 7Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
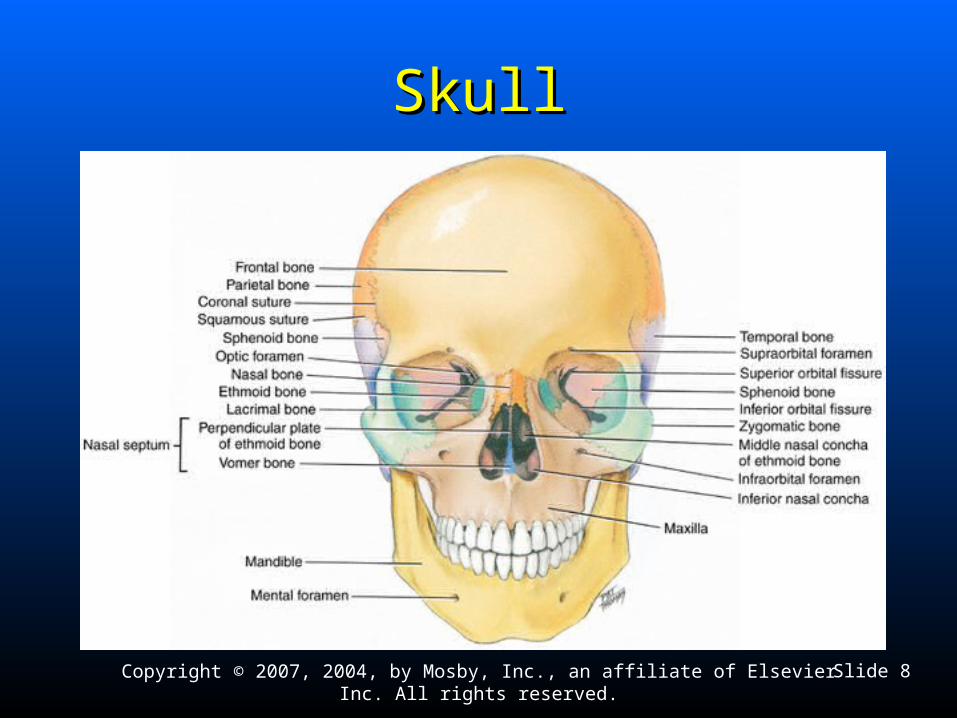
Skeletal SystemSkeletal System
Provides structure and supportProvides structure and support
Protects vital organsProtects vital organs
Allows movement, in conjunction with musclesAllows movement, in conjunction with muscles
Slide 8Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
SkullSkull

Slide 9Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Base of the SkullBase of the Skull

Slide 10Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Nerve Cells and PressureNerve Cells and Pressure
Nerve cells are very sensitive to pressure.Nerve cells are very sensitive to pressure.
When pressure is applied to nerve cells, function When pressure is applied to nerve cells, function becomes compromised.becomes compromised.
Determinants of injury from pressure:Determinants of injury from pressure: The amount of pressure applied on nerveThe amount of pressure applied on nerve The period of time over which it is appliedThe period of time over which it is applied

Slide 11Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Mechanism of Injury –Mechanism of Injury –Compression ForcesCompression Forces
Slide 12Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
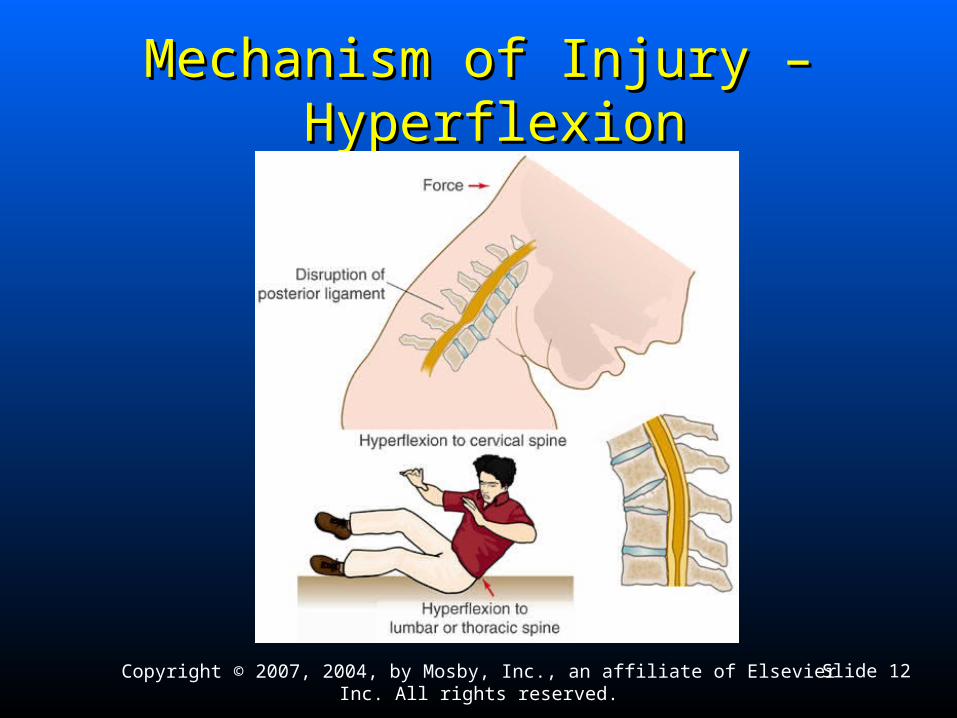
Mechanism of Injury –Mechanism of Injury – Hyperflexion Hyperflexion

Slide 13Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Mechanism of Injury – Mechanism of Injury – HyperextensionHyperextension
Slide 14Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Lateral BendingLateral Bending
DistractionDistraction Pulling apart of the spinePulling apart of the spine Example: HangingExample: Hanging

Slide 15Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
High Index of Suspicion for High Index of Suspicion for Spinal InjurySpinal Injury
Motor vehicle crashesMotor vehicle crashes
Pedestrian vs. vehicle collisionsPedestrian vs. vehicle collisions
FallsFalls
Blunt traumaBlunt trauma

Slide 16Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
High Index of Suspicion for High Index of Suspicion for Spinal InjurySpinal Injury
Penetrating trauma to head, neck, or torsoPenetrating trauma to head, neck, or torso
Motorcycle crashesMotorcycle crashes
HangingsHangings
Diving accidentsDiving accidents
Unconscious trauma victimsUnconscious trauma victims

Slide 17Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Spinal Injuries –Spinal Injuries –Signs and SymptomsSigns and Symptoms
Tenderness in the area of injury Tenderness in the area of injury
Pain associated with movingPain associated with moving Do not ask the patient to move to try to elicit a pain response.Do not ask the patient to move to try to elicit a pain response. Do not move the patient to test for a pain response.Do not move the patient to test for a pain response. Tell the patient not to move while you are asking questions.Tell the patient not to move while you are asking questions.
Normal function does not rule out spinal injury.Normal function does not rule out spinal injury.

Slide 18Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Spinal Injuries –Spinal Injuries –Signs and SymptomsSigns and Symptoms
Pain independent of movement or palpationPain independent of movement or palpation Along spinal columnAlong spinal column Lower legsLower legs May be intermittentMay be intermittent
Obvious deformity of the spine on palpationObvious deformity of the spine on palpation
Soft tissue injuries associated with traumaSoft tissue injuries associated with trauma From head and neck to cervical spineFrom head and neck to cervical spine Shoulders, back, or abdomen (thoracic, lumbar region)Shoulders, back, or abdomen (thoracic, lumbar region) Lower extremities (lumbar, sacral region)Lower extremities (lumbar, sacral region)

Slide 19Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Motor and Sensory Function –Motor and Sensory Function –Upper ExtremitiesUpper Extremities

Slide 20Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Motor and Sensory Function –Motor and Sensory Function –Lower ExtremitiesLower Extremities

Slide 21Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Loss of Sensation and Function Loss of Sensation and Function Below Level of InjuryBelow Level of Injury
Loss of sensation and paralysisLoss of sensation and paralysis C4: claviclesC4: clavicles T4: nipple lineT4: nipple line T10: navelT10: navel L1: groinL1: groin
Level of injury – respiratory paralysisLevel of injury – respiratory paralysis Above C3, complete paralysis/respiratory arrestAbove C3, complete paralysis/respiratory arrest Below C5, intercostals and abdominals, diaphragmatic breathing onlyBelow C5, intercostals and abdominals, diaphragmatic breathing only
Upper or lower extremities Upper or lower extremities
IncontinenceIncontinence

Slide 22Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Assessment of Spine-Injured Assessment of Spine-Injured Responsive PatientResponsive Patient
Mechanism of injuryMechanism of injury
Questions to askQuestions to ask Does your neck or back hurt?Does your neck or back hurt? What happened?What happened? Where does it hurt?Where does it hurt? Can you move your hands and feet?Can you move your hands and feet? Can you feel me touching your fingers?Can you feel me touching your fingers? Can you feel me touching your toes?Can you feel me touching your toes?

Slide 23Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Assessment of Spine-Injured Assessment of Spine-Injured Unresponsive PatientUnresponsive Patient
Mechanism of injuryMechanism of injury
Initial assessmentInitial assessment
Inspect forInspect for Contusions Contusions Deformities Deformities Lacerations Lacerations Punctures/penetrationsPunctures/penetrations SwellingSwelling

Slide 24Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Assessment of Spine-Injured Assessment of Spine-Injured Unresponsive PatientUnresponsive Patient
Palpate for areas of tenderness or deformity.Palpate for areas of tenderness or deformity.
Obtain information from others.Obtain information from others. Mechanism of injuryMechanism of injury Mental statusMental status

Slide 25Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
ComplicationsComplications
Inadequate breathing Inadequate breathing efforteffort Prepare for positive-Prepare for positive-
pressure ventilation.pressure ventilation. Maintain manual inline Maintain manual inline
stabilization.stabilization.
ParalysisParalysis

Slide 26Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Emergency Medical CareEmergency Medical Care
Body substance Body substance isolationisolation Determined by Determined by
presenting problempresenting problem• GogglesGoggles
• GlovesGloves
• MaskMask
• GownGown

Slide 27Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Critically Injured PatientCritically Injured Patient
Perform a rapid extrication.Perform a rapid extrication.
Bring body into alignment.Bring body into alignment.
Transfer to long board without Transfer to long board without short spine board.short spine board.
Transport immediately.Transport immediately.

Slide 28Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Injuries to the Head –Injuries to the Head –StructuralStructural
Specific sections of the Specific sections of the brain are injured.brain are injured. Brain lacerationsBrain lacerations Brain contusionsBrain contusions Blockage of vessels Blockage of vessels
(stroke)(stroke)
Injuries can be Injuries can be traumatic or traumatic or nontraumatic.nontraumatic.

Slide 29Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Structural Injuries –Structural Injuries –Signs and SymptomsSigns and Symptoms
Result in localized Result in localized findings (unilateral)findings (unilateral) Unequal pupilsUnequal pupils One-sided paralysisOne-sided paralysis One-sided sensory lossOne-sided sensory loss

Slide 30Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Metabolic InjuriesMetabolic Injuries
Interruption of energy needed for cell lifeInterruption of energy needed for cell life
PoisoningPoisoning
HypoxiaHypoxia
Low blood sugarLow blood sugar

Slide 31Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Metabolic Injuries – Metabolic Injuries – Signs and SymptomsSigns and Symptoms
Symmetrical findingsSymmetrical findings
General signs of CNS dysfunctionGeneral signs of CNS dysfunction

Slide 32Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Structural vs. Metabolic Structural vs. Metabolic FindingsFindings

Slide 33Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Secondary Complications of Secondary Complications of Brain InjuryBrain Injury
HypoxiaHypoxia
HypotensionHypotension
HypoglycemiaHypoglycemia
InfectionsInfections
Increased intracranial Increased intracranial pressurepressure

Slide 34Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Significance of Secondary Significance of Secondary ComplicationsComplications
Occur with direct brain injuryOccur with direct brain injury
Aggravate brain functionAggravate brain function
Management is important to overall care.Management is important to overall care.
Treatment prevents further injury to the brain.Treatment prevents further injury to the brain.

Slide 35Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Injuries to the Brain and SkullInjuries to the Brain and Skull
Most common cause of traumatic deathMost common cause of traumatic death May be immediateMay be immediate May occur over timeMay occur over time
Rapid recognition and management is key.Rapid recognition and management is key.
Access to surgical intervention is critical.Access to surgical intervention is critical.
Immobilization, airway, and ventilationImmobilization, airway, and ventilation Key to prehospital careKey to prehospital care
Slide 36Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Injuries to the Brain and SkullInjuries to the Brain and Skull
ScalpScalp
Skull fractureSkull fracture
ConcussionConcussion
Increased intracranial pressureIncreased intracranial pressure
Epidural hematomaEpidural hematoma
Subdural hematomaSubdural hematoma
Slide 37Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Related Nontraumatic ConditionsRelated Nontraumatic Conditions
Clots or hemorrhageClots or hemorrhage
Nontraumatic brain injuriesNontraumatic brain injuries Can be a cause of altered mental statusCan be a cause of altered mental status Signs and symptoms parallel those of traumatic injuriesSigns and symptoms parallel those of traumatic injuries No evidence of traumaNo evidence of trauma Lack of mechanism of injuryLack of mechanism of injury

Slide 38Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Skull Injury –Skull Injury –Signs and SymptomsSigns and Symptoms
Mechanism of traumaMechanism of trauma
Scalp injuriesScalp injuries ContusionsContusions LacerationsLacerations HematomasHematomas
Deformity to the skullDeformity to the skull

Slide 39Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.

Slide 40Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Skull Injury –Skull Injury –Signs and SymptomsSigns and Symptoms
Blood or fluid leakage from the Blood or fluid leakage from the ears or noseears or nose
Bruising around the eyesBruising around the eyes
Bruising behind the ears (mastoid Bruising behind the ears (mastoid process)process)

Slide 41Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.

Slide 42Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
ConcussionConcussion
Transient loss of consciousness or neurologic Transient loss of consciousness or neurologic functionfunction
Many degrees of injuryMany degrees of injury Least severeLeast severe
• Momentary loss of function immediately after injuryMomentary loss of function immediately after injury
• Short period of confusionShort period of confusion

Slide 43Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Concussion –Concussion –More SevereMore Severe
Brain contusionBrain contusion Vision lossVision loss ParalysisParalysis Sensory deficitsSensory deficits
Slide 44Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Signs of Signs of Increased Intracranial Pressure Increased Intracranial Pressure
Conscious patientsConscious patients HeadachesHeadaches NauseaNausea Vomiting (sometimes projectile)Vomiting (sometimes projectile)
Alterations in consciousness may occurAlterations in consciousness may occur SleepySleepy Responds to verbal stimuliResponds to verbal stimuli Responds to painful stimuliResponds to painful stimuli UnresponsiveUnresponsive

Slide 45Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Signs of Signs of Increased Intracranial Pressure Increased Intracranial Pressure
in Children in Children
Drowsiness, nausea, vomitingDrowsiness, nausea, vomiting Even after minor head injuryEven after minor head injury
Worsening may be due toWorsening may be due to HypoxiaHypoxia HypotensionHypotension Other causesOther causes

Slide 46Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Eye and Motor FindingsEye and Motor Findings
Unilaterally dilated pupilUnilaterally dilated pupil May not constrict with lightMay not constrict with light Eyelid may droopEyelid may droop
Unilateral weakness, paralysis, sensory loss, or a combination may be Unilateral weakness, paralysis, sensory loss, or a combination may be seen.seen.
As pressure increases, motor and sensory findings may affect both As pressure increases, motor and sensory findings may affect both sides.sides.
With further deterioration, abnormal postures or positions may be seen.With further deterioration, abnormal postures or positions may be seen.
Eventual flaccidityEventual flaccidity

Slide 47Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Abnormal PosturingAbnormal Posturing
Slide 48Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
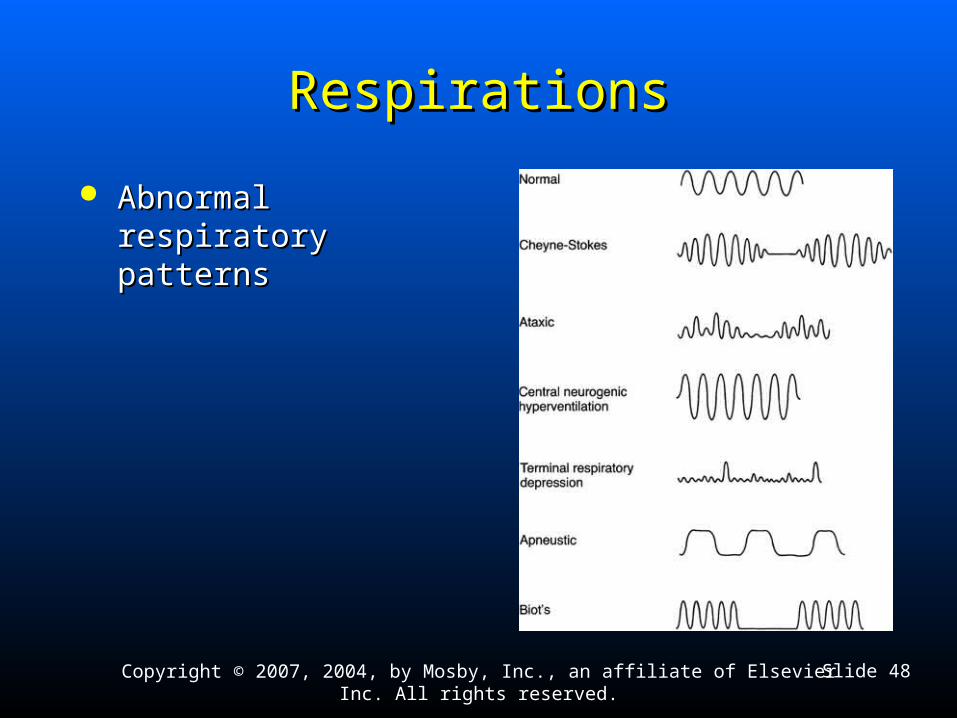
RespirationsRespirations
Abnormal respiratory Abnormal respiratory patternspatterns

Slide 49Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Pulse and Blood PressurePulse and Blood Pressure
Late sign of increased intracranial pressureLate sign of increased intracranial pressure
Pulse slows.Pulse slows.
Blood pressure increases.Blood pressure increases.

Slide 50Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Epidural HematomaEpidural Hematoma
Requires rapid recognition and early surgical interventionRequires rapid recognition and early surgical intervention
Usually presents with short period of unconsciousness after Usually presents with short period of unconsciousness after blunt trauma to head, fblunt trauma to head, followed by lucid interval, then decrease ollowed by lucid interval, then decrease in LOCin LOC Blown pupil on side of injuryBlown pupil on side of injury Weakness and sensory impairment on opposite side of bodyWeakness and sensory impairment on opposite side of body Abnormal respiratory patternAbnormal respiratory pattern Abnormal posturingAbnormal posturing Possible high blood pressure and slow pulsePossible high blood pressure and slow pulse If left untreated, death occurs.If left untreated, death occurs.

Slide 51Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Epidural HematomaEpidural Hematoma

Slide 52Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.

Slide 53Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Subdural HematomaSubdural Hematoma

Slide 54Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.

Slide 55Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.

Slide 56Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Brain Injury –Brain Injury –Signs and SymptomsSigns and Symptoms
Altered or decreasing mental statusAltered or decreasing mental status Confusion, disorientation, or repetitive questioningConfusion, disorientation, or repetitive questioning Best indicator of a brain injuryBest indicator of a brain injury
UnresponsiveUnresponsive Irregular breathing patternIrregular breathing pattern
Consideration of mechanism of injuryConsideration of mechanism of injury Deformity of windshieldDeformity of windshield Deformity of helmetDeformity of helmet

Slide 57Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Brain Injury –Brain Injury –Signs and SymptomsSigns and Symptoms
Contusions, lacerations, hematomas to scalpContusions, lacerations, hematomas to scalp Deformity to skullDeformity to skull Blood or fluid leakage from ears and noseBlood or fluid leakage from ears and nose Bruising around eyesBruising around eyes Bruising behind ears (mastoid process)Bruising behind ears (mastoid process) Neurologic disabilityNeurologic disability Nausea and/or vomitingNausea and/or vomiting Unequal pupil size with altered mental statusUnequal pupil size with altered mental status Seizure activity may be seenSeizure activity may be seen
Slide 58Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Open Head Injury –Open Head Injury –Signs and SymptomsSigns and Symptoms
Bruising around eyesBruising around eyes
Bruising behind ears (mastoid process)Bruising behind ears (mastoid process)
Nausea and/or vomitingNausea and/or vomiting
Brain injuryBrain injury Possible signs and symptoms of a closed head injuryPossible signs and symptoms of a closed head injury

Slide 59Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Glasgow Coma ScaleGlasgow Coma Scale
Objective assessment of mental statusObjective assessment of mental status
Three parametersThree parameters Eye openingEye opening Verbal responseVerbal response Motor abilityMotor ability

Slide 60Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Eye OpeningEye Opening
ScoresScores 4 – Open spontaneously (no stimuli)4 – Open spontaneously (no stimuli) 3 – Open to verbal stimuli3 – Open to verbal stimuli 2 – Open to painful stimuli2 – Open to painful stimuli 1 – Do not open1 – Do not open

Slide 61Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Verbal ResponseVerbal Response
ScoresScores 5 – Alert and oriented5 – Alert and oriented 4 – Confused (attention can be maintained)4 – Confused (attention can be maintained) 3 – Inappropriate (attention cannot be 3 – Inappropriate (attention cannot be
maintained)maintained) 2 – Incomprehensible sounds2 – Incomprehensible sounds 1 – No response1 – No response

Slide 62Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Motor AbilityMotor Ability
ScoresScores 6 6 –– Obeys verbal commands Obeys verbal commands
5 5 –– Localized to pain (reaches to source of pain) Localized to pain (reaches to source of pain)
4 4 –– Withdraws (rolls or moves from pain) Withdraws (rolls or moves from pain)
3 3 –– Flexion (flexes arms to pain) Flexion (flexes arms to pain)
2 2 –– Extension (extends arms to pain) Extension (extends arms to pain)
1 1 –– No response to pain No response to pain

Slide 63Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Emergency Medical CareEmergency Medical Care Use personal protection measures.Use personal protection measures.
Suspect spinal injury; immobilize spine.Suspect spinal injury; immobilize spine.
Maintain airway/artificial ventilation/oxygenation.Maintain airway/artificial ventilation/oxygenation.
Perform initial assessment.Perform initial assessment.
Immobilization spine.Immobilization spine.
Complete detailed physical examination en route.Complete detailed physical examination en route.

Slide 64Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Emergency Medical CareEmergency Medical Care
MonitorMonitor Airway, breathing, pulse, and mental statusAirway, breathing, pulse, and mental status
Control bleeding.Control bleeding. Do not apply pressure to open or depressed skullDo not apply pressure to open or depressed skull
Dress and bandage open wound.Dress and bandage open wound.

Slide 65Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Emergency Medical CareEmergency Medical Care
Nontraumatic injuryNontraumatic injury Place patient on the left side.Place patient on the left side.
Be prepared for changes in patient’s condition.Be prepared for changes in patient’s condition.
Transport immediately.Transport immediately.

Slide 66Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Cervical Spine Immobilization Devices –Cervical Spine Immobilization Devices –IndicationsIndications
Any suspected injury to the spine, based onAny suspected injury to the spine, based on Mechanism of injuryMechanism of injury HistoryHistory Signs and symptomsSigns and symptoms
Used in conjunction with short and long backboards.Used in conjunction with short and long backboards.

Slide 67Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Cervical Spine Immobilization Devices –Cervical Spine Immobilization Devices –PrecautionPrecaution
Cervical immobilization devices alone do not provide adequate Cervical immobilization devices alone do not provide adequate inline immobilization. Maintain manual immobilization until the inline immobilization. Maintain manual immobilization until the head is secured to the board.head is secured to the board.

Slide 68Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Long BackboardsLong Backboards
Several different types of long board immobilization devices Several different types of long board immobilization devices exist.exist.
Provide stabilization and immobilization to the head, neck and Provide stabilization and immobilization to the head, neck and torso, pelvis, and extremities.torso, pelvis, and extremities.
Use to immobilize patients found in a lying, standing, or sitting Use to immobilize patients found in a lying, standing, or sitting positionposition
Use in conjunction with short backboards.Use in conjunction with short backboards.

Slide 69Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Rapid ExtricationRapid Extrication
Unsafe sceneUnsafe scene
Unstable patient conditionUnstable patient condition
Patient blocking access to a seriously injured patientPatient blocking access to a seriously injured patient
Based on Based on TimeTime Patient conditionPatient condition Not the EMT’s preferenceNot the EMT’s preference

Slide 70Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Rapid ExtricationRapid Extrication
Apply CISD before move.Apply CISD before move.
Perform smoothly.Perform smoothly.
Coordination from lead person is key.Coordination from lead person is key.
Secure to long spine board after removal.Secure to long spine board after removal.
Slide 71Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Helmet Removal –Helmet Removal –Special Assessment NeedsSpecial Assessment Needs
• Ability to gain access to airway and breathingAbility to gain access to airway and breathing
Fit of the helmetFit of the helmet May prevent proper spinal immobilizationMay prevent proper spinal immobilization
Patient movement within the helmetPatient movement within the helmet

Slide 72Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Indications for Indications for Leaving Helmet in PlaceLeaving Helmet in Place
Fit of helmet is good with little or no movement of head.Fit of helmet is good with little or no movement of head.
Helmet does not impede airway or cause breathing problems.Helmet does not impede airway or cause breathing problems.
Removal would cause further injury to the patient.Removal would cause further injury to the patient.
Proper spinal immobilization could be performed with helmet in place.Proper spinal immobilization could be performed with helmet in place.
Helmet does not interfere with the ability to assess and reassess airway Helmet does not interfere with the ability to assess and reassess airway and breathing.and breathing.

Slide 73Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Indications for Indications for Helmet RemovalHelmet Removal
Inability to assess and/or reassess airway and breathingInability to assess and/or reassess airway and breathing
Restriction of adequate airway or breathing managementRestriction of adequate airway or breathing management
Improperly fitted helmetImproperly fitted helmet
Inability to perform proper spinal immobilization because of helmetInability to perform proper spinal immobilization because of helmet
Cardiac arrestCardiac arrest

Slide 74Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Types of HelmetsTypes of Helmets
SportsSports Typically open anteriorlyTypically open anteriorly Easier access to airway Easier access to airway
MotorcycleMotorcycle Full face guardFull face guard ShieldShield OtherOther

Slide 75Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
General Rules –General Rules –Helmet RemovalHelmet Removal
Technique depends on type of helmet.Technique depends on type of helmet.
Remove patient’s eyeglasses before removing the Remove patient’s eyeglasses before removing the helmet.helmet.

Slide 76Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.
Infants and ChildrenInfants and Children
Require same attention to spinal immobilization as adultsRequire same attention to spinal immobilization as adults
Pad spine boards from the shoulders to the heelsPad spine boards from the shoulders to the heels Accounts for larger head in proportion to rest of bodyAccounts for larger head in proportion to rest of body
If CSID does not fit properly, use rolled towel and tape.If CSID does not fit properly, use rolled towel and tape.
Transport in car seat if assessment, treatment, and Transport in car seat if assessment, treatment, and immobilization can be accomplished.immobilization can be accomplished.

Slide 77Copyright © 2007, 2004, by Mosby, Inc., an affiliate of Elsevier Inc. All rights reserved.