infection in peritoneal dialysis
TRANSCRIPT
54
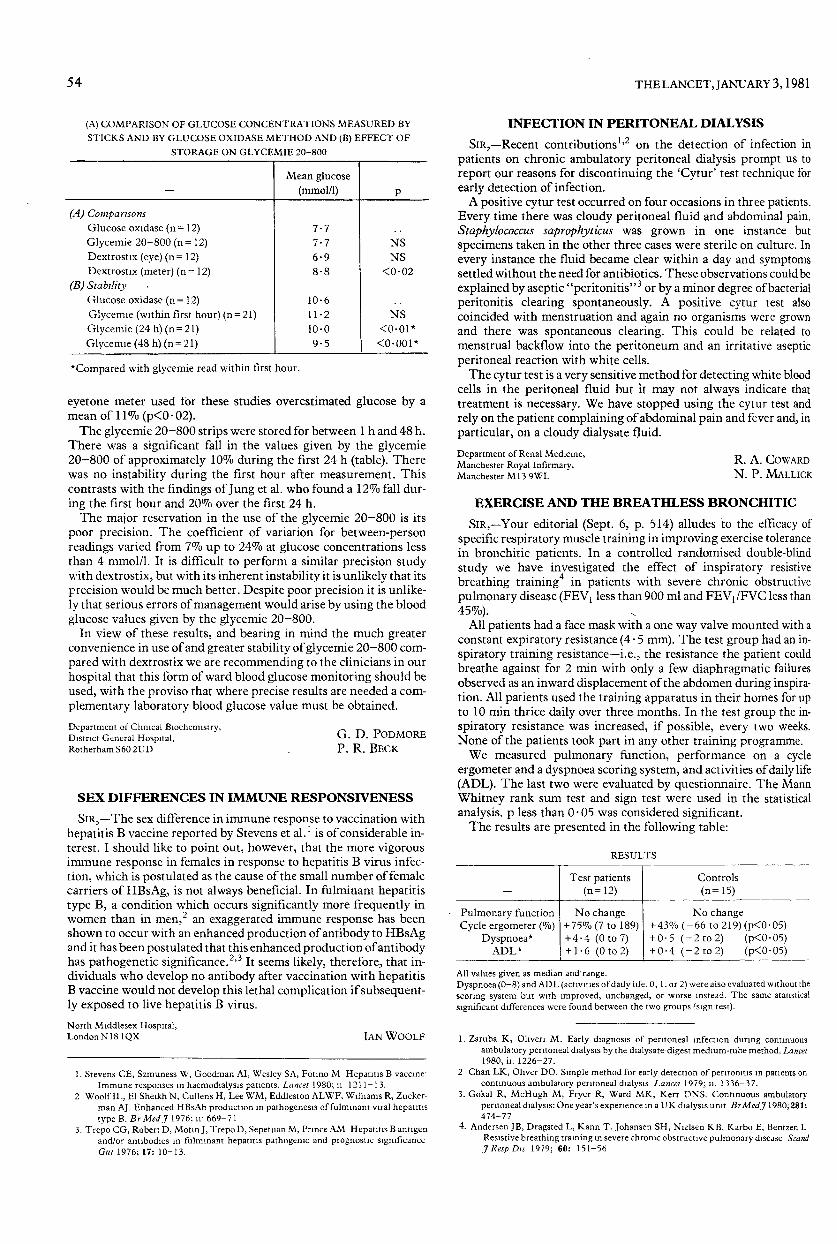
(A) COMPARISON OF GLUCOSE CONCENTRATIONS MEASURED BYSTICKS AND BY GLUCOSE OXIDASE METHOD AND (B) EFFECT OF
STORAGE ON GLYCEMIE 20-800
*Compared with glycemie read within first hour.
eyetone meter used tor these studies overestimated glucose by amean of 11 % (p<0 02).The glycemie 20-800 strips were stored for between 1 h and 48 h.
There was a significant fall in the values given by the glycemie20-800 of approximately 10% during the first 24 h (table). Therewas no instability during the first hour after measurement. Thiscontrasts with the findings of Jung et al. who found a 12% fall dur-ing the first hour and 20% over the first 24 h.The major reservation in the use of the glycemie 20-800 is its
poor precision. The coefficient of variation for between-personreadings varied from 7% up to 24% at glucose concentrations lessthan 4 mmol/1. It is difficult to perform a similar precision studywith dextrostix, but with its inherent instability it is unlikely that itsprecision would be much better. Despite poor precision it is unlike-ly that serious errors of management would arise by using the bloodglucose values given by the glycemie 20-800.
In view of these results, and bearing in mind the much greaterconvenience in use of and greater stability of glycemie 20-80b com-pared with dextrostix we are recommending to the clinicians in ourhospital that this form of ward blood glucose monitoring should beused, with the proviso that where precise results are needed a com-plementary laboratory blood glucose value must be obtained.
Department of Clinical Biochemistry,District General Hospital,Rotherham S60 2UD
G. D. PODMOREP. R. BECK
SEX DIFFERENCES IN IMMUNE RESPONSIVENESS
SIR,-The sex difference in immune response to vaccination withhepatitis B vaccine reported by Stevens et al. 1 is of considerable in-terest. I should like to point out, however, that the more vigorousimmune response in females in response to hepatitis B virus infec-tion, which is postulated as the cause of the small number of femalecarriers of HBsAg, is not always beneficial. In fulminant hepatitistype B, a condition which occurs significantly more frequently inwomen than in men,z an exaggerated immune response has beenshown to occur with an enhanced production of antibody to HBsAgand it has been postulated that this enhanced production of antibodyhas pathogenetic significance.2,3 It seems likely, therefore, that in-dividuals who develop no antibody after vaccination with hepatitisB vaccine would not develop this lethal complication if subsequent-ly exposed to live hepatitis B virus.North Middlesex Hospital,London N18 1QX IAN WOOLF
1. Stevens CE, Szmuness W, Goodman AI, Wesley SA, Fotino M Hepatitis B vaccine:Immune responses in haemodialysis patients. Lancet 1980; ii: 1211-13.
2 Woolf IL, El Sheikh N, Cullens H, Lee WM, Eddleston ALWF, Williams R, Zucker-man AJ. Enhanced HBsAb production in pathogenesis of fulminant viral hepatitistype B. Br Med J 1976; ii: 669-71
3. Trepo CG, Robert D, Motin J, Trepo D, Sepetjian M, Prince AM Hepatitis B antigenand/or antibodies in fulminant hepatitis pathogenic and prognostic significanceGut 1976; 17: 10-13.
INFECTION IN PERITONEAL DIALYSIS
SiR,—Recent contributionsl,2 on the detection of infection inpatients on chronic ambulatory peritoneal dialysis prompt us toreport our reasons for discontinuing the ’Cytur’ test technique forearly detection of infection.A positive cytur test occurred on four occasions in three patients.
Every time there was cloudy peritoneal fluid and abdominal pain.Staphylococcus saprophyticus was grown in one instance but
specimens taken in the other three cases were sterile on culture. Inevery instance the fluid became clear within a day and symptomssettled without the need for antibiotics. These observations could be
explained by aseptic "peritonitis" or by a minor degree of bacterialperitonitis clearing spontaneously. A positive cytur test alsocoincided with menstruation and again no organisms were grownand there was spontaneous clearing. This could be related tomenstrual backflow into the peritoneum and an irritative asepticperitoneal reaction with white cells.The cytur test is a very sensitive method for detecting white blood
cells in the peritoneal fluid but it may not always indicate thattreatment is necessary. We have stopped using the cytur test andrely on the patient complaining of abdominal pain and fever and, inparticular, on a cloudy dialysate fluid.
Department of Renal Medicine,Manchester Royal Infirmary,Manchester M13 9WL
R. A. COWARDN. P. MALLICK
EXERCISE AND THE BREATHLESS BRONCHITIC
SIR,-Your editorial (Sept. 6, p. 514) alludes to the efficacy ofspecific respiratory muscle training in improving exercise tolerancein bronchitic patients. In a controlled randomised double-blindstudy we have investigated the effect of inspiratory resistive
breathing training in patients with severe chronic obstructivepulmonary disease (FEVlless than 900 ml and FEV; /FVC less than45%). ’-
All patients had a face mask with a one way valve mounted with aconstant expiratory resistance (4 - 5 mm). The test group had an in-spiratory training resistance-i.e., the resistance the patient couldbreathe against for 2 min with only a few diaphragmatic failuresobserved as an inward displacement of the abdomen during inspira-tion. All patients used the training apparatus in their homes for upto 10 min thrice daily over three months. In the test group the in-spiratory resistance was increased, if possible, every two weeks.None of the patients took part in any other training programme.We measured pulmonary function, performance on a cycle
ergometer and a dyspnoea scoring system, and activities of daily life(ADL). The last two were evaluated by questionnaire. The MannWhitney rank sum test and sign test were used in the statisticalanalysis. p less than 0’ 05 was considered significant.The results are presented in the following table:
All values given as median and range.Dyspnoea (0-8) and ADL (activities of daily life, 0, 1. or 2) were also evaluated without thescoring system but wnh improved, unchanged, or worse instead. The same statisticalsignificant differences were found between the two groups (sign test).
1. Zaruba K, Oliveri M. Early diagnosis of peritoneal infection during continuousambulatory peritoneal dialysis by the dialysate-digest medium-tube method. Lancet1980, ii: 1226-27.
2 Chan LK, Oliver DO. Simple method for early detection of peritonitis in patients oncontinuous ambulatory peritoneal dialysis Lancet 1979; ii: 1336-37.
3. Gokal R, McHugh M, Fryer R, Ward MK, Kerr DNS. Continuous ambulatoryperitoneal dialysis: One year’s experience in a UK dialysis unit Br Med J 1980; 281:474-77
4. Andersen JB, Dragsted L, Kann T, Johansen SH, Nielsen KB, Karbo E, Bentzen LResistive breathing training in severe chronic obstructive pulmonary disease ScandJ Resp Dis 1979; 60: 151-56